Embed Size (px)
Citation preview

1129
Basilar Branch Pontine InfarctionWith Prominent Sensory Signs
Cathy M. Helgason, MD, and Andrew C. Wilbur, MD
We identified 10 patients with acute pontine infarction and specific sensory findings. Twopatients had pure sensory symptoms, two had sensory complaints of the hand and mouth, andthe other six had hemisensory loss referable to medial lemniscal or spinothalamic tractdysfunction but localized to one limb, to an arm and leg, or to the face, characteristic of strokelocalized to the cerebral hemisphere. All patients had magnetic resonance imaging showinginfarction of the medial or lateral pontine tegmentum and a patent basilar artery. No definitesource for cardiogenic thromboembolism was found. Infarcts in the midline extending from thebase of the pons posteriorly into the tegmentum suggested basilar branch occlusion, whileinfarcts involving only part of the tegmentum probably resulted from small penetrator branchocclusion. Vertigo, light-headedness, or cranial nerve dysfunction suggested a pontine locationof neurological dysfunction in these patients, but the nature of the sensory findings did notalways predict the lateral, medial, inferior, or superior extent of tegmental infarction. (Stroke1991^22:1129-1136)
Isolated reports suggest that a pure sensory syn-drome can be caused by pontine hemorrhage orinfarction. We describe 10 patients with pon-
tine infarction who presented with sensory com-plaints. All patients had ischemic changes localizedto the pontine tegmentum by magnetic resonanceimaging (MRI). Analysis of the symptoms and signsshould aid in the diagnosis of basilar branch diseaseand provide insight into the afferent sensory system.
Subjects and MethodsBetween June 1989 and June 1990 we identified 10
consecutive patients who had pontine infarction andacute sensory findings. Each patient was examined byone neurologist through the Stroke Service at one ofthe University of Illinois College of Medicine atPeoria hospitals, St. Francis Medical Center orMethodist Medical Center. All MRI scans wereinterpreted by a radiologist without knowledge of theclinical findings.
All patients had high-resolution cranial MRI witha 1.5 -T superconducting unit, using a 5-mm slicethickness and T2-weighted axial spin/echo imagingwith repetition times ranging from 2,000 to 3,000msec, first echo times of 20 or 25 msec, and secondecho times of 80 or 90 msec. Six patients also had
From the Departments of Neurology (C.M.H.) and Radiology(A.C.W.), University of Illinois College of Medicine at Chicago,Chicago, III.
Address for reprints: Dr. Cathy M. Helgason, Department ofNeurology (m/c 796), 912 South Wood Street, Room 855N NPI,Chicago, IL 60612.
Received August 24, 1990; accepted May 14, 1991.
T2-weighted coronal MRI scans with similar pulsesequence parameters.
All patients underwent neurological examination.Sensory testing included pinprick, touch, vibration,temperature, proprioception, and stereognosis. Onlythe abnormalities detected on examination are de-scribed in each case.
Case 1. A 53-year-old white man had the suddenonset of right leg tingling and numbness and aninability to place his foot on the ground correctlyduring ambulation. He became light-headed and haddifficulty writing, with tingling and numbness of hisright hand. On examination, bilateral carotid bruitswere noted. His blood pressure was 192/100 mm Hg,and his pulse was regular. There was right-sidedhyperreflexia and a right Babinski's sign. Clumsy,rapid, alternating movements of his right hand, in-tention tremor on right heel-to-shin testing, a wide-based gait, and veering to the right were noted. Hehad difficulty placing his right foot where he wanted.Perception of pinprick was decreased on his right legbelow the knee. A left hemisphere infarct was sus-pected. The MRI and test results are summarized inTable 1 and Figures 1 and 2. His gait improved.
Case 2. A 60-year-old white man had the suddenonset of numbness in his left arm and leg on a back-ground of congenital spina bifida, arrested hydroceph-alus, paraparesis, and incontinence. Examination re-vealed a blood pressure of 128/86 mm Hg and a regularpulse. Bilateral muscle wasting below the knees waspresent, with clubbing deformity of both feet and nomotion at the ankles or toes. Sensation was absent
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1130 Stroke Vol 22, No 9 September 1991
TABLE 1. Test Results and Risk Factors for Stroke in 6 Patients With Pontine Basilar Branch Occlusion
Case
1
2
3
4
NonspecificT2 changes
WM BG
— —
MRI
PontinePatent infarct
BA location
+ L sup posttegmenrum
+ R post lat lowtegmentum
+ L lat mid suptegmentum, Rmed low & midtegmentum
+ L mid sup base &tegmentum
Echocardiogram, chestroentgenogram
I LV compliance,global LV hypokinesis
LV apical hypokinesis,cardiomegaly
Severe mitral anuluscalcification, AVcalcification, stenosis ®urgitation, LVhypertrophy
Carotidduplex
sonogram
LICAbmoderateirregularity
Normal
Tight R ICA b,mild L ICA b,stenosis
Normal
Cerebral angiogram
ICA siphonirregularity, patentLVA
L ICA b mildstenosis (MRIangiography)
Other
HTN; peripheralvascular disease;tobacco, alcohol use;tchol
HTN; old myocardialinfarct; hx LOC;tchol
HTN; CABG; hx RICA occlusion, Rmiddle cerebral arteryinfarct; t chol, t TG
HTN; congestive heartfailure; hx LOC
5 + + L mid sup base & Normalmed tegmentum
Normal
10
R high midtegmentum
L mid base &med tegmentum,R low mid base& medtegmenrum
L mid low medtegmentum
Central & medmid suptegmentum
R low & mid lowbase & medtegmentum
Global LV, inferior L ICA bwall hypokinesis, aortic moderateinsufficiency, left atrial stenosisenlargement
L ICA b occlusion, HTN; t chol, TG;reconstituted via tobacco use; tthyrocervical trunk platelets
CABG; HTN; t chol,tLDL, 1HDL
Normal
Normal
Normal
Normal(transesophagealechocardiography)
Normal
Normal
Mild bilateralICA b stenosis
Normal
L ICA b moderatestenosis; patentVA & BA
Anteriorcommunicatingartery aneurysm
Normal VA & BA
HTN; tobacco use
T chol; HTN
Supraventriculartachycardia; t
Tobacco, drug abuse;t cerebrospinal fluidIgG & protein
MRI, magnetic resonance imaging; WM, white matter; BG, basal ganglia; BA, basilar artery; L, left; R, right; sup, superior; post, posterior;lat, lateral; med, medial; LV, left ventricle; AV, aortic valve; ICA, internal carotid artery, b, bifurcation; VA, vertebral artery; HTN,hypertension; chol, cholesterol; hx, history of; LOC, loss of consciousness; CABG, coronary artery bypass graft; TG, triglycerides; LDL, lowdensity lipoprotein; HDL, high density lipoprotein.
below the knees. He had a moderate intention tremoron finger-to-nose maneuver on the left. Marked de-creased perception of pinprick and vibration was notedon his left arm from the elbow to the dorsum of thehand, especially on the fourth and fifth digits. A rightthalamic infarct was suspected. The MRI and labora-tory results are given in Table 1 and Figures 1 and 3.His hospital course was unremarkable.
Case 3. A 59-year-old white man had a 3-weekhistory of intermittent right arm and leg numbnessand weakness, a feeling of right arm puffiness, andright leg tingling. On examination, his blood pressurewas 180/100 mm Hg and his pulse was regular. There
was constructional apraxia, left spastic hemiparesis,and depressed perception of pinprick in his left arm.Surprisingly, no right body signs were present. A lefthemisphere infarct was suspected. The MRI and testresults are given in Table 1 and Figure 1. The patientceased to have right body symptoms.
Case 4. An 80-year-old white woman lost con-sciousness for a brief period. When she regainedconsciousness she could not ambulate and she veeredto the right, slurred her speech, and described numb-ness in her right hand. On examination, her bloodpressure was 180/100 mm Hg and her pulse wasregular. She had left facial weakness. Her deep
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Helgason and Wilbur Pontine Infarct, Sensory Findings 1131
bO
a
Oe
Q goho
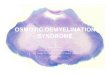
FIGURE 1. Location of pontine infarcts as interpreted bymagnetic resonance imaging for cases 1-10 (a through )),respectively.
tendon reflexes were brisk throughout. She veered tothe right on walking and had depressed fine motormotion of her right hand and bilateral intentiontremors on finger-to-nose testing (left limbs worsethan right). Sensory examination was normal. TheMRI and test results are given in Table 1 and Figure1. Her right hand control improved.
Case 5. A 50-year-old white woman developedright face and hand numbness followed by slurredspeech, the inability to grasp objects or write with herright hand, and loss of balance. On examination herblood pressure was 194/90 mm Hg and her pulse wasregular. She had bilateral carotid artery and leftvertebral artery bruits. She was dysarthric. She hadmild weakness of her right face and a decrease in finemotor motion of her right hand. Dorsiflexiort of herright foot was weak, and she fell to the right ontandem walk. Right hyperreflexia and Babinski's signwere present. The perception of pinprick was lost inher right hand. A left parietal infarct was suspected.The MRI and test results are given in Table 1 andFigure 1. Her symptoms improved.
Case 6. A 62-year-old white man reported suddennumbness and tingling in his arms and legs. He feltlight-headed, stumbled, and dropped back into achair. Afterward, he noted increased numbness in hisright arm with fine motor difficulty in his right hand.His right hand and leg were clumsy. On examination,his blood pressure was 206/104 mm Hg and his pulsewas regular. Mild left facial weakness and a right
FIGURE 2. Case 1. Axial (left) and sagittal (right) T2-weighted magnetic resonance images showing infarct in upper left pons(resonance time=2,500 msec; echo time=90 msec).
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1132 Stroke Vol 22, No 9 September 1991
FIGURE 3. Case 2 Axial T2-weighted magnetic resonanceimage showing infarct in lower right ports (resonance time-=2,500 msec; echo time=90 msec).
intention tremor on finger-to-nose testing were seen.He fell to the right when he ambulated. Perception ofpinprick was diminished in his right leg, trunk, andarm; perception of vibration and proprioception werediminished in his right arm and leg. A left thalamicinfarct was suspected. The MRI and test results aregiven in Table 1 and Figure 1. The patient's gaitnormalized, but he had residual tingling in his rightlimbs.
Case 7. A 57-year-old white woman noted right legweakness. The next day, she slurred her speech anddeveloped right hand, forearm, great toe, and dorsalpedal numbness. Examination revealed a blood pres-sure of 140/80 mm Hg and a regular pulse. Hertongue deviated to the right, and she had milddiffusely distributed arm and leg weakness. Her deeptendon reflexes were brisk, and there was a rightBabinski's sign. Months later she noted increaseddysarthria, difficulty swallowing, and left-sided clum-siness; her previous deficits had cleared. On exami-nation, her blood pressure was 182/100 mm Hg andher pulse was regular. She had marked dysarthria,uncontrollable bouts of laughter and crying, difficultyhandling her saliva, and weakness of her left face.Her reflexes were brisk. No Babinski's sign waspresent. Depressed perception of pinprick was foundon her left leg. She had an MRI and other tests (see
Table 1 and Figure 1). Over the following months,the patient remained pseudobulbar in affect. Herdysarthria and dysphagia cleared. She developed aprominent sensation of numbness in her fingertipsand around her mouth. Repeat MRI showed nochange.
Case 8. A 59-year-old black woman had light-headedness and right cheek and left arm volar sur-face numbness, followed by a burning sensation andbilateral cheek and lip numbness. There was ringingin her ears. Neurological examination showed de-creased perception of pinprick on her left face. Herblood pressure was 155/100 mm Hg, and her pulsewas regular. The MRI and test results are given inTable 1 and Figure 1. Her symptoms remainedunchanged.
Case 9. A 69-year-old white man developed leftgreater than right arm numbness. When he walked,he veered to the left. He felt light-headed. Hissymptoms lasted for several hours. Neurological ex-amination was normal. His blood pressure was 145/80mm Hg and his pulse was regular. His MRI and testresults are given in Table 1 and Figure 1. He re-mained asymptomatic.
Case 10. A 39-year-old male intravenous drugabuser had the sudden onset of left-sided weaknessand dysarthria followed by the inability to ambu-late. On examination, his blood pressure was 160/100 mm Hg and his pulse was regular. He had rightinternuclear ophthalmoplegia, weakness of his leftface, and nasal dysarthric speech. His limbs wereweak distally. Mild intention tremors were presentin his right arm and leg. There was left hyperreflexiaand bilateral Babinski's signs. Sensory examinationrevealed extinction on the left side of his bodyto double simultaneous stimulation. His MRI andtest results are given in Table 1 and Figure 1.He developed uncontrollable fits of laughter, andhis gait improved.
ResultsTen patients, six men and four women, aged 39-80
years, had new sensory complaints and pontine in-farction. The stroke was sudden and maximally man-ifest in four patients, progressed gradually in twopatients, and progressed intermittently or stutteredin four. One patient had a significant residual neu-rological deficit, and the others either improved orwere neurologically stable with minimal residual def-icit. All patients were functioning independently atthe time of discharge from the hospital.
The patients had infarcts ranging in size from 1.5to 1.8 cm3 and localized by MRI to the regionsdepicted in Table 1. Where the basis pontis wasinvolved, the infarcts extended posteriorly into thetegmentum (Figure 1). All patients had a patentbasilar artery defined by MRI.
Seven patients had hypertension prior to the onsetof infarction. No patient had diabetes mellirus or apathologically proven cardiogenic source for throm-boembolism. All but one patient had echocardiogra-
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Helgason and Wilbur Pontine Infarct, Sensory Findings 1133
phy and chest roentgenography performed. Fourpatients had evidence of cardiac disease. Findingssuggestive of a cardiac source for thromboembolismincluded cardiomegaly, global hypokinesis, focal walldyskinesia, and mitral anulus calcification. Five pa-tients had cerebrovascular extracranial or intracra-nial circulation atheroma defined by duplex scanningor cerebral angiography. Cerebral angiography per-formed in three patients failed to reveal vertebralbasilar artery abnormalities (Table 1).
Presenting symptoms included a light-headed sen-sation in four patients and loss of consciousness inone. Four patients had slurred speech, and one haddiplopia. Ataxia was found in seven patients whoveered when walking and had loss of balance orclumsiness. Hand and face numbness were the initialsymptoms in three patients. Two patients had peri-oral as well as hand numbness, and seven patientshad either numbness or tingling in the arm and leg orin the arm or hand alone. One patient had tinnitus,one a puffy feeling in the arm, and another a perioralburning sensation. In all but two patients (cases 4 and10), sensory complaints were either confirmed byexamination of the patient or distinguished by thepatient from motor signs at presentation.
DiscussionLacunar-sized (<, 1.5 cm in diameter) pontine infarc-
tion is associated with pure motor ataxic hemiparesis orthe clumsy hand-dysarthria syndrome.1 Basilar branchocclusion or basilar artery thrombosis may producelarger infarcts with combined sensory, motor, and cra-nial nerve dysfunction.2-3 Sensory complaints, whichoccur alone or in a facial/brachial distribution, resem-ble those of hemispheric stroke of a thalamic or parietallocation.4"6 Internal capsular posterior limb infarctionmay also cause hemisensory loss, and recent reportsattribute pure sensory findings to pontine stroke.7"10
Hommel et al8 described an infarct in the right para-median pons at the junction of the upper and lower twothirds of the tegmentum. This patient had a hemisen-sory complaint of numbness and tingling over the leftside of the body exacerbated by touch or rub, andfindings implicated medial lemniscus dysfunction andconsisted of loss of joint and position sense in bothlimbs. Stereognosis, pain, and temperature perceptionswere normal. Araga et al9 and Graveleau et al10 attrib-uted pure sensory complaints to pontine hemorrhagelocalized to the dorsal lateral pontine tegmentum.Their patients had dysesthesias and decreased percep-tions of touch, especially of the mouth and hand.Bilateral cheiro-oral syndrome due to unilateral para-median tegmental pontine hemorrhage was describedby Matsumoto et al.11 Usually the syndrome reflects athalamic or parietal lesion. The pontine location forthis symptom complex is unusual.12-14 Burning oral andmidfacial pain has been attributed to dysfunction of thetrigeminal nucleus or spinal tract after ventral pontineinfarction.15
Hemorrhage or infarct localized to the paramedianor lateral tegmentum may be associated with mixed
sensorimotor or combined sensory modality dysfunc-tion of medial lemniscal or spinothalamic tract dys-function. Caplan and Goodwin16 described threecases of lateral superior and inferior pontine tegmen-tal hemorrhage associated with severe contralateralsensory deficits to pinprick, position, or all sensorymodalities combined with motor and other neurolog-ical dysfunction. Kudo et al17 described a case ofdorsal lateral tegmental hemorrhage in which aster-ixis accompanied by mild hemiparesis was overshad-owed by profound contralateral hemisensory loss toall modalities and ataxia. A case of tetra-ataxichemiparesis associated with posterior pontine mid-line base lacunar-sized infarction was characterizedby a persistent and severe tingling sensation of bothhands despite normal sensory findings on clinicalexamination by Van Gijn and Vermeulen.18 Only twopatients of our series described pure sensory com-plaints (cases 2 and 8). Usually, sensory loss was apredominant component of a more complex array ofneurological dysfunction that included ataxia, hemi-paresis, reflex asymmetries, and dysarthria. One pa-tient had transient extraocular motility dysfunction(case 10), and others had vertigo or light-headednessat the onset of their stroke. Cases 1, 4, and 5resemble the ataxic hemiparesis or clumsy hand-dysarthria syndrome which, when localized to thepons, traditionally is not accompanied by sensoryfindings.1920 Cases 4 and 6 had loss of consciousnessand bilateral neurological signs suggesting dysfunc-tion of the reticular activating system or bilateralbrain stem dysfunction.
Hommel et al8 and others910 suggest that sensoryloss in pontine infarction runs true to tract type.When correlated with the anatomic site of the infarcton MRI, the sensory findings of the patients in ourseries did not always support this theory (Table 2).When pure sensory symptoms were the presenting orenduring complaint, one patient had lateral tegmen-tal and two had medial tegmental infarction (cases 2,7, and 8). All three patients noted "numbness." Thepatients with cheiro-oral complaints (cases 7 and 8)did not display findings or loss of proprioceptive orvibratory perception, even when the infarct on MRIappeared to involve the medial lemniscal tract. Case2 complained of "numbness" and had a lower pon-tine lateral tegmental infarct where the spinotha-lamic tract courses but sensory loss suggesting bothmedial lemniscal as well as spinothalamic tract in-volvement. In some instances, however, sensory find-ings correlated nicely with the anatomic site of theinfarct. Case 1 had decreased perception of pinprickconsistent with spinothalamic dysfunction and diffi-culty placing the same leg when ambulating, suggest-ing ataxia due to proprioceptive loss as might be seenwith medial lemniscal tract dysfunction. The mediallemniscal and spinothalamic sensory tracts approachone another anatomically as they ascend in the pons(Figure 4). Case l's infarct appropriately was in thesuperior lateral pontine tegmentum. Brodal21 sug-gests that the final definition of sensory representa-
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1134 Stroke Vol 22, No 9 September 1991
TABLE 2. Location by MRI of Pontine Infarcts and Clinical Sensory Complaints and Findings of Spinothalamlc or Medial Lemniscal Typein 10 Patients
Case
1
2
3
45
6
7
8
910
Medial
Puffiness, "numbness,"tingling
Spinothalamic sensorytype; ataxia,"numbness"
Spinothalamic sensorytype; "numbness"
Spinothalamic sensorytype; "numbness,"burning, ringing in ears
Ataxia, "numbness"Ataxia, extinction
Lateral
Spinothalamic, mediallemniscal sensorytype; ataxia,"numbness," tinglingSpinothalamic, mediallemniscal sensorytype; ataxia,"numbness"Puffiness,"numbness," tinglingAtaxia, "numbness"
Spinothalamic, mediallemniscal sensorytype; ataxia,"numbness," tingling
Tegmentum
Inferior
Spinothalamic,medial lemniscaisensory type; ataxia,"numbness"Puffiness,"numbness," tingling
Spinothalamicsensory type;"numbness"Spinothalamicsensory type;"numbness," burning,ringing in ears
Ataxia, extinction
Superior
Spinothalamic, mediallemniscal sensory type;ataxia, "numbness," tingling
Puffiness, "numbness,"tinglingAtaxia, "numbness"Spinothalamic sensory type;ataxia, "numbness"
Spinothalamic, mediallemniscal sensory type;ataxia, "numbness," tingling
Ataxia, "numbness"
tion in the spinothalamic and medial lemniscal tractshas yet to be clarified. Not only might spinothalamiccells be activated by rotation of the joints, butinformation about joint position may also be carriedin the spinothalamic tract. Information about tem-perature might be carried by the dorsal columns.
We encountered other difficulties with anatomiclocalization of the infarct for the patients in thisseries. Because somatotopic representation is com-pact in the long tracts, it was surprising that monoap-pendicular sensory loss would be attributable tostroke localized to the pons. The predominant handnumbness complained of by case 4 or the face andhand symptoms of cases 5, 7, and 8 were thereforeunexpected. Three of our patients (cases 6, 8, and 9),had infarcts of unexpected lateralization. Since thecases in this series were collected consecutively be-cause they had sensory complaints and infarcts local-ized to the pons, we included those patients. Case 9had a centrally located lesion, and case 6 had bilat-eral symptoms at onset. These facts suggest thepresence of lesions not seen on MRI. Case 8 hadbilateral findings but unilateral stroke delineated byMRI and symptoms of the cheiro-oral type similar tothe case of Matsumoto et al.n Biller et al22 noted thatMRI changes may not appear until up to 12 hoursafter the onset of symptoms of pontine infarction.Edema may also account for neuroanatomic dysfunc-tion and explain the findings of case 2 or otherpatients.
The MRI-defined pontine infarcts in this serieswere lacunar in size. There was no evidence forbasilar artery stenosis or occlusion. Biller et al22 andKnepper et al23 suggest that traditional axial andcoronal Tl- and T2-weighted MRI scans may be usedreliably to detect basilar artery thrombosis or occlu-sion. Finer details of basilar artery irregularity ordegree of stenosis would not be defined by thismethod. The etiologic role of thromboembolic oratheroembolic events with regard to small unilateralpontine infarcts has yet to be defined. Therefore, thesignificance of the presence of potential cardiacsources for thromboembolism in these patients isundefined. The near-universal presence of hyperten-sion, unilaterality of small pontine infarcts, and ab-sence of a definite thromboembolic source suggeststhe presence of intracranial atheromatous or lipohy-alinotic disease of the paramedian, circumferential,superior cerebellar, or anterior inferior cerebellarbranches of the basilar artery (Figure 4).24 The goodprognosis of these patients argues against progressivevertebral or basilar artery thrombosis, but not neces-sarily against embolism, as the etiology of stroke.
As shown by examination and MRI scans of thepresent series, pontine infarction may present withpure sensory dysfunction but most often is accompa-nied by other findings. Sensory complaints may sug-gest medial, lateral, inferior, or superior tegmentalinvolvement, but it may be difficult to distinguish theanatomic site of the infarct on clinical grounds alone.
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Helgason and Wilbur Pontine Infarct, Sensory Findings 1135
Circumferential artery
FIGURE 4. Courses ofspinotha-latnic (Sth) and medial lemniscal(ML) tracts (top) and arterialsupply (bottom) ofpons. Ports issupplied by paramedian branchesofbasilar artery in medial portionreaching posteriorly to ventraltegmentum. Short circumferentialarteries (Sh Cir Br) supply ante-rior lateral pontine surface; longcircumferential (L Cir Br) andanterior inferior cerebellar artery(AICA) branches supply caudaltegmentum; superior cerebellar ar-tery (SCA) and long circumferen-tial arteries supply rostral tegmen-tum. PICA, posterior inferiorcerebellar artery.
Although pathological proof is lacking, the etiology ofthe infarcts appears to be related to intracranialvascular occlusion due to intrinsic vascular disease.The isolated findings of a monoappendicular or facial/brachial distribution of sensory loss suggest cerebralhemispheric localized dysfunction. These patients,who had good prognoses, must be distinguished clin-ically from those with infarction due to large-vessel
occlusive or thromboembolic mechanisms. The capa-bility of MRI to accurately detect and localize pontineinfarction and suggest basilar artery patency mayallow this distinction to be made.25
AcknowledgmentsWe would like to thank Ms. Shari Clemons, RN,
for her time and devotion in helping collect the data
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

1136 Stroke Vol 22, No 9 September 1991
needed for case reviews. Ms. Jeanne Ward is thankedfor her invaluable technical assistance.
References1. Caplan LR, Stein RW: Stroke: A Clinical Approach. Boston,
Butterworths, 1986, pp 167-1772. Fisher CM, Caplan LR: Basilar artery branch occlusion: A
cause of pontine infarction. Neurology 1971;21:900-9053. Kubik C, Adams R: Occlusion of the basilar artery: A clinical
and pathologic study. Brain 1946;69:73-1214. Fisher CM: Pure sensory stroke and allied conditions. Stroke
1982;13:434-4475. Sacco RL, Bello JA, Traub R, Brust JCM: Selective proprio-
ceptive loss from a thalamic lacunar stroke. Stroke 1987;18:1160-1163
6. Derouesnd C, Mas J-L, Bolgert F, Castaigne P: Pure sensorystroke caused by a small cortical infarct in the middle cerebralartery territory. Stroke 1984;15:660-662
7. Derouesn6 C, Yelnik A, Castaigne P: Deficit sensitif isol6 parinfarctus dans le territoire de l'artere choroidienne artdrieure.RevNeurol (Paris) 1985;141:311-314
8. Hommel M, Besson G, Pollak P, Borgel F, Le Bas JF, PerretJ: Pure sensory stroke due to a pontine lacune. Stroke 1989;20:406-408
9. Araga S, Fukada M, Kagimoto H, Takahashi K: Pure sensorystroke due to pontine hemorrhage. JNeurol 1987;235:116-117
10. Graveleau PH, Decroix JP, Samson Y, Masson M, Cambier J:Deficit isol6 d'un h6micorps par Mmatome du pont. RevNeural (Paris) 1986;142:788-790
11. Matsumoto S, Kaku S, Yamasuki M, Imai T, Nabatame H,Kameyama M: Cheiro-oral syndrome with bilateral oralinvolvement: A study of pontine lesions by high resolutionmagnetic resonance imaging. / Neurol Neurosurg Psychiatry1989;52:792-794
12. Diaz-Calderon E, Gimeno-Alava A, Diaz A, Leiva C: Tuber-culoma of the pons (letter). / Neurol Neurosurg Psychiatry1981;44:266
13. Garcin RA, Lapresle J: Deuxifime observation personelle desyndrome sensitif de type thalamique et a topographie che'iro-orale par lesion localised du thalamus. Rev Neurol (Paris)1960;103:474-481
14. Garcin R, Lapresle R: Syndrome sensitif de type thalamiqueet a topographie chelro-orale par lesion localised du thalamus.Rev Neurol (Paris) 1954;99:121-129
15. Reutens DC: Burning oral and midfacial pain in ventralpontine infarction. Aust N ZJ Med 1990;20:249-250
16. Caplan LR, Goodwin JA: Lateral tegmental brainstem hem-orrhages. Neurology 1982;32:252-260
17. Kudo Y, Fukai M, Yamadori A: Asterixis due to pontinehemorrhage (letter). / Neurol Neurosurg Psychiatry 1985;48:487-488
18. Van Gijn J, Vermeulen M: Ataxic tetraparesis from lacunarinfarction in the pons. / Neurol Neurosurg Psychiatry 1983;46:669-670
19. Huang CY, Chan KH: Pontine ataxic hemiparesis, a lateralpenetrator syndrome? (letter). J Neurol Neurosurg Psychiatry1984;47:1046-1047
20. Glass JD, Levey AI, Rothstein JD: The dysarthria clumsyhand syndrome: A distinct clinical entity relative to pontineinfarction. Ann Neurol 1990;27:487-494
21. Brodal A: Neurological Anatomy in Relation to Clinical Medicine,ed 3. New York, Oxford University Press, Inc, 1981, pp 86-87
22. Biller J, Yuh WTC, Mitchell GW, Bruno A, Adams HP Jr:Early diagnosis of basilar artery occlusion using magneticresonance imaging. Stroke 1988;19:297-306
23. Knepper L, Biller J, Adams HP, Yuh W, Ryals T, Godersky J:MR imaging of basilar artery occlusion. / Comput AssistTomogr 1990;14:32-35
24. Caplan LR, Stein RW: Stroke: A Clinical Approach. Boston,Butterworths, 1986, pp 38-39
25. Solsberg MD, Founier D, Potts DG: MR imaging of theexcised human brainstem: A correlative neuroanatomic study.AJNR 1990;11:1003-1013
KEY WORDS • cerebral infarct • pons • spinothalamic tracts
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

C M Helgason and A C WilburBasilar branch pontine infarction with prominent sensory signs.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1991 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.22.9.1129
1991;22:1129-1136Stroke.
http://stroke.ahajournals.org/content/22/9/1129World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from