Embed Size (px)
Citation preview

Journial of Neurology, Neurosurgery, anid Psychiatry 1981:44:983-990
Autonomic dysfunction in Guillain-Barre syndromeRR TUCK, JG McLEOD
From the Department of Medicine, the University of Sydney, and the Department of Neurology, The RovalPrince Alfred Hospital, Camperdown, NSW, Australia
SUMMARY The following tests of autonomic function were performed on seven patients with theGuillain-Barre syndrome and compared with controls: (1) measurement of heart rate and bloodpressure in the supine and erect positions, (2) measurement of baroreflex sensitivity, (3) Valsalva'smanoeuvre, (4) sweat test. In two patients the heart rates were fixed and greater than 100/min and inthree there was postural hypotension. The baroflex sensitivity of four patients was abnormal andheart rate response to Valsalva's manoeuvre was impaired in two of the three patients who were
able to perform the manoeuvre. Areas of anhidrosis were found in all seven patients. These abnorm-alities probably reflect pathological alterations of the sympathetic and parasympathetic componentsof the autonomic nervous system of patients with Guillain-Barre syndrome. The severity of autonomicinvolvement is not related to the degree of sensory and motor disturbance which is consistent with thepatchy distribution of lesions throughout the peripheral and autonomic nervous systems.
Autonomic dysfunction may occur in the Guillain-Barre syndrome and account for some of thefatalities in the condition. Manifestations ofautonomic involvement are disturbances of sweat-ing,' heart rate and rhythm,2 3 blood pressurecontrol,3-6 and sphincter, visceral and pupillaryfunction.' 6The baroreceptor-heart rate reflex has not pre-
viously been studied in a group of patients withGuillain-Barre syndrome, as it has been in patientswith peripheral neuropathy due to diabetes, alcoholand porphyria.7-9 In view of the potentially fataldisturbances of autonomic function that can occur inthe Guillain-Barre syndrome, it seemed appropriateto investigate the abnormalities of sweating andbaroflex control of heart rate and blood pressure inpatients with this condition. A brief account of thisstudy has already been published.10
Materials and methods
Tests of autonomic function were performed on fivehealthy subjects and seven patients with Guillain-Barresyndrome after informed consent had been obtained.
Address for reprint requests: J G McLeod, Departnment ofMedicine, The University of Sydney, Sydney, New SouthWales 2006, Australia.
Accepted 21 July 1981
Control subjectsThe control subjects were five healthy males whose agesranged from 20 to 49 years (mean 38; SD 8). They werefree of hypertension, heart disease and neurologicaldisease and were taking no medication.
PatientsThe ages of seven patients (five males, two females) withGuillain-Barre syndrome ranged from 33 to 55 years(mean 43; SD 9). None suffered from hypertension orheart disease. The interval between the onset of weaknessand the time of maximum disability ranged from 12 hoursto three weeks. Six patients had a presumed viral illnessat an interval ranging from three days to seven weeksbefore the onset of neurological symptons. The patientsdisability at the time of testing was graded on a scale from0 to 5 (table 1). None of the patients required assistedventilation. In five patients, the CSF protein concen-tration was greater than 04 g/l. Abnormalities ofperipheral nerve conduction were demonstrated in allpatients. Serum B12, serum folate and glucose tolerance
Table I Disability status of patients with GBS at timeofautonomic testing
Status Criteria
O NormalI Symptoms but no signs2 Mild motor and sensory symptoms andl signs3 Moderate disability4 Assistance needed with walking5 Unable to walk
983
Protected by copyright.
on April 3, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.11.983 on 1 Novem
ber 1981. Dow
nloaded from

984
tests were normal and urinary porphyrins were notdetected.The interval between the onset of weakness and the
autonomic tests ranged from one to nine weeks. Threepatients were being treated with oral corticosteroids atthe time of the investigations; one patient (Case 5) wasreceiving amitriptyline 75 mg at night and diazepam15 mg/day, but no other patient was being treated withdrugs which affected autonomic function.
Measurement of heart rate and heart periodHeart rate and heart period (R-R interval) were measuredfrom the patients' electrocardiogram with a Grass EKGTachograph preamplifier (Model 7P4D) and recordedusing a Grass (Model 7B) pen recorder.
Measurement of arterial blood pressureThe arterial blood pressure was measured througha cannula inserted into the left brachial artery usinga pressure transducer (Statham Model P23AC) placed atthe approximate level of the aortic valve, a Grass (Model7P1B) preamplifier and Model 7DAE driver amplifierand was recorded on another channel of the pen recorder.
Alteration ofpostureThe subjects lay quietly on a tilt table until the pulse andblood pressure remained steady. The subjects and patientswere then tilted until either they were vertical or theirsystolic blood pressure fell below 90 mmHg. Except whenpostural hypotension was severe, subjects were tilted forfive minutes before being returned to the horizontalposition. Heart rate and blood pressure during tiltingwere recorded continuously.
Measurement of baroreceptor-heart-rate reflexsensitivityThe sensitivity of the baroreceptor-heart rate reflex wasmeasured by comparing changes in the heart period withchanges in systolic blood pressure. Transient elevations ofarterial blood pressure were produced with intravenousinjections of phenylephrine, an alpha-adrenergic agentthat raises blood pressure by causing peripheral vaso-constriction while having little direct effect on heart rate.The drug was given intraveneously over 10-30 seconds indoses ranging from 25-300,g. Up to six injections weregiven to each subject, at least two minutes being allowedbetween each injection. The baroflex sensitivity wascalculated according to the method described by Smythet al.11 Each heart period was plotted against the systolicblood pressure of the preceding heart beat from the startof the rise in blood pressure to the peak, and the slope ofthe linear regression of these points so obtained was usedas an estimate of baroreflex sensitivity (ms/mmHg).
Valsava's manoeuvreThe manoeuvre was performed with the subjects on thetilt table elevated to an angle of 300. The subjects wereasked to maintain a column of mercury in a manometerat a height of 40 mm for ten seconds using a mouthpiecewhich consisted of a syringe barrel. After several trialattempts the heart period and blood pressure wererecorded before, during and 30 seconds after three
Tuck, McLeod
successive manoeuvres. Approximately two minuteswere allowed between each. The Valsalva ratio was calcu-lated by dividing the longest heart period occurring afterthe manoeuvre by the shortest during the manoeuvre.12The highest ratio from the three attempts was recorded.7
The sweat testSweating was assessed by mapping the areas of skinwhich sweated in response to body heating. Each subjectlay supine while a powder (alizarine red 35 G, rice starch60 G and sodium carbonate 20 G) that changed colourfrom pale pink to deep purple when wet was dusted overall of the visible skin surface except the face. A heatingcradle was placed over the subject's chest and abdomenand heat was applied until oral temperature had risenI C or until sweating began to occur on the face when theareas over which sweating occurred were recorded.
Statistical methodsMeans are expressed with standard deviations and werecompared using the two-tailed Student's t test.13 Thesample variances were compared using the VarianceRatio Test (Snedecor's 'F' test). If there was a significantdifference between variances (p < 0-05) the means werecompared using t', instead of t.13 Data which differed bymore than two standard deviations from the control meanwere regarded as abnormal. The data relating heartperiod and systolic blood pressure were stored on papertape. The linear regressions of the heart period and bloodpressure were calculated with the aid of a PDP 11/40computer using the method of least squares.13 Thesignificance of the regression coefficient was calculated.'3
Results
The disability status of the seven patients withGuillain-Barre syndrome and the individualpooled results of autonomic function tests performedon the five control subjects and the seven patientsare shown in Table 2.
HEART RATEThe resting heart rates of five control subjects rangedfrom 57 to 68 beats/min (mean 64 ± 4). Heart ratesof the seven patients ranged from 73 to 118 beats/min(mean 92 ± 16). The differences are significant(p < 002). In two patients (Cases 1 and 5) theresting pulse rates were greater than 100/minute.
BLOOD PRESSUREThe resting arterial blood pressures of the fivecontrol subjects ranged from 115/65 to 160/95 mmHg(mean 132/77 ± 19/12). The resting arterial pressuresin the seven patients, none of whom were known tobe hypertensive prior to their illness, ranged from122/66 to 175/92 (mean 153/87 + 21/14). There wasno significant difference in the mean systolic ordiastolic blood pressures in the two groups, althoughin Cases I and 7 systolic blood pressures were
Protected by copyright.
on April 3, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.11.983 on 1 Novem
ber 1981. Dow
nloaded from

Autonomic dysfunction in Guillain-Barre syndrome
Table 2 Summary ofresults of autolnioic tests performed on five healthy subjects and seven patients with GBS
ANumtiber Age Sex DisabilitY Tiineftronz Heart rate In(rease Arterial blood pressuee Va/salva Baroreflexstatus oniset of Supilie Erect % Supine Erect Change ratio sensitivity
GBS to (beats/mninute) nnzHg minnHg °' tis/lnmHg(/ate oftests (dlay)
125 118S -5 6 2-4 15Control 1. 34 M 0 - 57 77 35
12 15 75subjects 160 155 -3.1 2-3 14
2. 45 M 0 - 63 71 13 95 98 3 2
115 112 -2-6 229 9.13. 34 M 0 - 67 893 33 65 70 - 77
118 110 -6-8 2-1 6-34. 49 M 0 - 65 73 12 73 68 -69
140 130 -7-1 27 115. 293 M 0 - 68 85 25 83 80 -3 6
Mean 38 - - - 64 79 24 132 125 -[6 r-084;n =2919 18 -1 0r3-
SD 8 - - - 4 8 11 12 12 6 5
Patients 1. 48 F 5 30 118 120 1-7 92 90 2-2 016
135 130 -3-7 2-9 172. 35 M 2 20 83 100 21 77 73 -5-2
3. 44 M 5 32 88 112 27 66 66 -0- 1-5 5 6
140 136 -2-9 1-7 8-44. 54 M 5 17 83 9)2 11 75 71 -53
168 100 -41 - 0-415. 55 F 5 63 1 10 1 12 1-8 ,98 65 -34
155 112 -28 - 3-06. 33 M 2 13 86 104 21 loo 65 -35
173 121 -30 - 5-17. 32 M.i 5 7 73 95 30 100 80 - 20
Mean 43 - - - 92 105 16 87 123 -14 r 050;2n-054221 18 IS - -
SD 10 - - - 16 10 12 14 98 15p >005 <0 02 >005 --005 -0-05 <001
0-05 0-05
(*Slope of regression of pooled dat..)
abnormal (table 2). In one patient (Case 5), the bloodpressure fluctuated during the course of the illnessto levels as high as 230/120.
EFFECT OF POSTURE ON HEART RATE AND
BLOOD PRESSUREThe heart rate was measured immediately beforetilting and as soon as tilting was complete. The meanincrease in control subjects was 240% (± 11 %) and inpatients it was 16% ( ± 12 %). There was no significantdifference in the two groups, although in Cases Iand 5 the heart rate increased only 1-7% and 1.80%respectively, both of which are abnormal.The systolic blood pressures of all control subjects
fell slightly on tilting, the mean fall being50 (± 2 1 %). The mean fall in the systolic bloodpressure of patients was 18% ( ± 15%) which did notdiffer significantly from the control mean. In allpatients the systolic blood pressure fell on tiltingand in Cases 1, 5, 6 and 7 the percentage fall wasabnormal.The diastolic blood pressures fell in three and
increased in two of the control subjects when tilted,the mean change being -1 6% (±6 5%). Thediastolic blood pressure fell on tilting in six of thepatients and remained unchanged in the seventh.The mean change was - 14% ( ± 15%) which was notsignificantly different from the control mean but inCases 5, 6 and 6 the fall in diastolic blood pressurewas abnormal.The changes in heart rate and the blood pressure
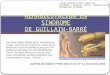
responses to tilting in a control subject and in twopatients are shown in fig 1.
BAROFLEX SENSITIVITYThe range of sensitivity of the baroreceptor-heart-rate reflex was 6-3 to 15 ms/mmHg in five controlsubjects (mean 12 ms/mmHg; r = 0-84; N = 29).In the seven patients the range of baroreflex sensi-tivity was 0 16 to 17 ms/mmHg; r = 0 50; n = 42).The difference was significant (p < 0-01) (figs 2 and3). When the data for each patient were comparedwith the pooled control data, the baroreflex sensi-tivities of Cases 2, 3 and 4 did not differ significantly
985
Protected by copyright.
on April 3, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.11.983 on 1 Novem
ber 1981. Dow
nloaded from

Tuck, McLeod
Control
A 90]
BP 12i n_75_
1001HR70 ' /-J p ~ V
Case 5
HR 120i100
Case 6
A 90]0
150 1
BP_50-
R100]HR 8]<---
1 minute
Fig I Records obtainedfrom one control subject andtvo patients with GBS (Cases 5, 6) showing the changesin heart-rate and blood pressure in response to tiltinig.Postural hypotension is pr-esent in both patients and inCase 5, the heart-r-ate is fixed at 110 per minute (Aangle of tilt; BP =-- arterial blood pressure, mtnnHg;HR = heart rate, beats/minute).
from the control sensitivity. The sensitivity wassignificantly less than the control value in Case 7(p < 0 05) and in Cases 1, 5 and 6 (p < 0-01). Twoof the patients (Cases I and 5) had baroreflexsensitivities of only 016 and 0-41 ms/mmHg,respectively (fig 3). Thus, their heart rates remainedalmost unchanged despite increases of up to30 mmHg in systolic blood pressure. Both of thesepatients had fast resting heart-rates (.1 18 and110 beats/min respectively) and one (Case 5) hadpostural hypotension.
VALSALVA'S MANOEUVRE
When the five healthy subjects performed Valsalva'smanoeuvre there was an initial transient increase inthe arterial blood pressure (Phase I) which then fellto a level less than the resting value at which itremained until forced expiration ceased (Phase It).At that moment, there was a transient fall in arterial
0 5 10 15 20Increase in systolic blood pressure (mmHg)
25
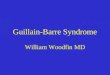
Fig 2 The relationship between the increase in he(altper-iod and the incr ease in systolic blood pressur e
following intravenous injections ofphenylephrine. Theclosed circles represent the means of the pooled datafrom the 5 control subjects and the open circles r-epresent
the means of the pooled data from the 7 patients withGBS. Vertical bars epresent + I SE. The slopes of ther-egression lines are 12 ms/mmHg for the control subjects(r = 0-84, n - 29) and 5-7 (ms/mmHg) for the patientswith GBS (r 0 50, n = 42). The difference betweenthe slopes was significant (p < 0-01).
blood pressure (Phase III). The blood pressure thenrapidly increased to a level above the resting valueto which it returned over the subsequent 15-40seconds (Phase IV). The mean ratio of the shortestR-R interval (Valsalva ratio) was 2 5 + 0-3).
Facial and respiratory weakness prevented fourpatients from performing Valsalva's manoeuvre. Inthe other three the blood pressure changes duringand after the manoeuvre were normal. In Case 2 theValsalva ratio was in the control range while inCases 3 and 4 the ratios were 1-5 and 1-7 which were
below the normal range.
SWEAT TEST
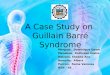
A sweat test was attempted on all seven patients.One patient (Case 5) was unable to tolerate the testbut she had not demonstrated any signs of sweatingafter her oral temperature had risen from 35 8° to36-4 OC. The other six patients were all able to tolerateheating, and all had some areas of anhidrosis(fig 4). Two patients (Cases 3 and 7) had completeanhidrosis of the lower limbs and three patients(Cases 1, 3 and 6) had areas of anhidrosis on theirabdominal walls.
A 90
150BP
50-
4001
E1300-
.0
200-
a 10S
O-A
986
Protected by copyright.
on April 3, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.11.983 on 1 Novem
ber 1981. Dow
nloaded from

Autonomic dysfunction in Guillain-Barre syndromne
Controls GBS
15
Baroref lex sensitivity(ms/mmHg) 10
Fig 3 The baroreflex sensitivities of 5 healthy subjectsanid 7 patients with GBS. The baroreflexv sensitivity ofthe control group was 12 ms/mmHg (r = 0-84, n = 29)and of the patient group was 5 7 ms!mmHg (r = 0 50,n = 42). The difference between the two sensitivities was
significant (p < 0-01).
Discussion
The results of the present investigation have shownthat in patients with Guillain-Barre syndrome thereare abnormalities of control of heart rate, bloodpressure and sweating. Although only five controlsubjects were studied in detail, the values obtainedwere similar to those of other workers for the meanresting heart rate7 14 and change in heart rate'5 andblood pressure with tilt.16 The increased mean restingheart rate in the seven patients, in two of whom(Cases 1 and 5) it remained relatively fixed through-out the study at greater than 100/minute, is consistentwith the observations of previous investigators whonoted tachycardia in this condition.1-3 Increasedresting heart rates have been observed in patientswith diabetes mellitus7 and acute intermittentporphyria.17 In both these conditions the tachycardiahas been attributed to lesions of the vagus or
glossopharyngeal nerves or both.'7 18 A fixedtachycardia also occurs when the autonomic nerve
supply to the heart is blocked pharmacologically.15Therefore, it is likely that the relatively fixed rapidheart rate of Cases 1 and 5 was a result of involve-ment of the cardiac autonomic nerve supply. In
I
2 3
Ff 4- 4,+ C Ad
4
.I
Fig 4 Patterns of sweat production in 6 patients withGBS. Black areas indicate regions of normal sweatproduction while the spotted areas are those in whichsweating was patchY.
cases 1 and 7 supine systolic blood pressures were
greater than two standard deviations above thecontrol mean and in Case 5 the blood pressure
fluctuated considerably during the course of theillness reaching levels as high as 230/130. Elevated or
fluctuating arterial blood pressure has been docu-mented previously in Guillain-Barre syndromel 2 5and may be caused by lesions of the glossopharyngealnerves which contain afferent fibres from the arterialbaroreceptors. The hypothesis that lesions of theafferent nerves from arterial baroreceptors are
responsible for hypertension, fluctuating arterialblood pressure and tachycardia is consistent withstudies on experimental animals and human sub-jects with lesions of these nerves.19-2' It is significantthat the patient who had fluctuating arterial bloodpressure and tachycardia (Case 5) had left-sidedpalatal weakness, dysphagia and dysphonia, clinicalfeatures that are consistent with a lesion of the leftvagus nerve.A significant fall in both the systolic and diastolic
arterial blood pressures occurred on tilting three ofthe seven patients with Guillain-Barre syndrome.
0
0
0
0
0~~
0
Sq
0 J X -
987
II
I..-I 1)
1% p
Protected by copyright.
on April 3, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.11.983 on 1 Novem
ber 1981. Dow
nloaded from

988
Orthostatic hypotension has been found in patientswith Guillain-Barre syndrome by other investi-gatorsl 45 and is also a common finding in patientswith diabetic autonomic neuropathy.7 It does notnormally occur in healthy subjects because of thecontrol of arterial blood pressure by the baroreflexes.On assuming the upright position there is an increasein splanchnic vascular resistance which contributessubstantially to the overall vascular resistance.22The decrease in splanchnic blood flow is attributed toarteriolar constriction which is mediated by thesympathetic nervous system.23 It has been shown bydirect intraneural recording of sympathetic nervousactivity from muscle nerves in man that changingposition from supine to sitting or standing increasesmuscle sympathetic nerve activity.24 The veins mayalso play some part in maintaining arterial bloodpressure in the upright position.25 The distensibilityof superficial veins decreases in normal subjectsduring the performance of Valsalva's manoeuvre26but in some patients with Guillain-Barre syndromethis response has been found to be absent presumablydue to involvement of their sympathetic nervesupply.27 The postural hypotension of patients in thepresent study was probably related to lesions of thesympathetic nervous supply to the arterioles andveins or of the afferent fibres from the arterialbaroreceptors. Of the three patients in the presentstudy with marked orthostatic hypotension, therewas evidence in two (Cases 6 and 7) that the baro-receptor afferent fibres were partially intact becausethe changes in their heart rate with increases in bloodpressure were qualitatively normal. The third patientwith postural hypotension (Case 5) had a fixed heartrate as well as severe postural hypotension whichmay have been caused by lesions of the sympatheticand vagus nerves on the efferent side of the baro-reflex arc and/or lesions of the afferent fibres fromthe baroreceptors. In this patient there was clinicalevidence of involvement of one vagus nerve in whichafferent fibres from the aortic arch baroreceptors andefferent fibres to the heart could also have beenaffected. However from the present study it isimpossible to determine exactly the site of theautonomic lesions. The absence of postural hypo-tension in one (Case 1) of the two patients who hada resting tachycardia is evidence that the baro-receptor afferent and sympathetic efferent fibres wereintact but that the vagal efferent fibres to the heartwere affected.The sensitivity of the heart-rate-baroreceptor
reflex was measured in one patient with Guillain-Barre syndrome by Davidson and Jellinek28 but thepresent study is the first in which changes in thesensitivity of the reflex have been documented ina group of such patients. The method used measures
Tuck, McLeod
rapid changes in heart rate which are mediatedlargely by the parasympathetic nervous system inresponse to changes in arterial pressure." 14 23 Themethod has been used to demonstrate impairmentof baroreflex sensitivity in patients with diabeticneuropathy.29 It is simpler than that devised byKorner et al,14 which measures the steady statecharacteristics of the baroreflex and which has beenused previously in our laboratory.7 8 Lesions in theafferent nerve fibres in the glossopharyngeal andvagus nerves from the carotid sinus and aortic archbaroreceptors and/or efferent fibres in the vagusnerves may reduce the sensitivity of the baroreflexwhich was found in four of the patients in the presentstudy and in the patient of Davidson and Jellinek.28The glossopharyngeal and vagus nerves are known tobe affected both clinically6 and pathologically30 inGuillain-Barre syndrome although in the presentstudy only one (Case 5) of the four patients with anabnormal baroreceptor heart rate reflex had obviousclinical evidence of involvement of these cranialnerves.
Impaired function of the baroreflexes could be dueto a lesion or lesions in the vasomotor centres of themedulla. This explanation is unlikely in a disease ofthe peripheral nervous system in which pathologicalchanges within the brainstem are usually minimal orabsent.3 30 However, extensive changes in the brain-stem involving the vagal nuclei have been described3land physiological studies32 provide some evidencethat central autonomic pathways maybe involved.None of the patients in the present study suffered
from heart disease and the only ECG abnormalitywas sinus tachycardia. However, pathologicalchanges have been found in the hearts of somepatients who died with Guillain-Barre syndrome3although Bredin2 could find no abnormalities in thehearts of two patients who died apparently as a resultof cardiac complications of the syndrome.
Abnormalities of the heart rate and blood pressureresponses to Valsalva's manoeuvre have beenreported in Guillain-Barre syndrome,5 27 but thethree patients in the present study who were able toperform the manoeuvre had normal responses,although in two, the Valsalva ratio was below thecontrol range of the present study. None of the threepatients had orthostatic hypotension or abnormalbaroreflex sensitivities and it was concluded that theyhad minimal disturbance of reflex autonomiccardiovascular control. It is probable that the patientswith postural hypotension and impaired baroreflexsensitivities would have had an abnormal Valsalvaresponse if they had been able to perform themanoeuvre.The sweat test was abnormal in six patients in
whom it was performed satisfactorily. Absent or
Protected by copyright.
on April 3, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.11.983 on 1 Novem
ber 1981. Dow
nloaded from

Aiutoniomic dvflitnion iti Guillci,i-Barre sYndrome
impaired sweating was found on the abdominal wallof three patients-two of whom had posturalhypotension (Cases 6 and 7). Since surgical resectionof the lower thoracic sympathetic ganglia andsplanchnic nerves cause postural hypotension33 andanhidrosis of the abdominal wall,34 it is suggestedthat the anhidrosis and postural hypotension inCases 6 and 7 was due to involvement of the lowerthoracic and upper lumbar segments of the sym-pathetic chains or splanchnic nerves or both. Posturalhypotension in patients with diabetes mellitus hasbeen attributed in part to pathological changes thatoccur in the greater splanchnic nerves.7The present investigations have demonstrated
varying degrees of impairment of autonomic nervoussystem function in all seven patients. The findingssuggest that lesions may occur in the afferent fibresfrom the arterial baroreceptors in the vagus andglossopharyngeal nerves, in the efferent para-sympathetic fibres in the vagus nerves which inner-vate the heart and in the sympathetic fibres whichcontrol sweating and vasomotor tone. Pathologicalstudies have demonstrated demyelinating lesions inthe glossopharyngeal and vagus nerves30 31 and inthe sympathetic chains and white rami.35 The severityof involvement of the autonomic nervous systemdoes not appear to be related to the degree of motorand sensory disturbance. The consequences ofinvolvement of the autonomic nervous system inGuillain-Barre syndrome are negligible in manypatients but on occasion they can be life threatening.Postural hypotension may lead to syncope andirreversible brain damage in a paralysed patient whois inadvertently left in a sitting position or whorequires an anaesthetic.36 Sudden cardiovascularcollapse may be the terminal event. Although themechanism is uncertain involvement of theautonomic nervous system has been implicated notonly in Guillain-Barre syndromes1 2 5 26 but also indiabetic autonomic neuropathy.37
Dr Roger R Tuck was in receipt of a NationalHealth and Medical Research Council MedicalPostgraduate Research Scholarship.
References
Lichtenfeld P. Autonomic dysfunction in the Guillain-Barre syndrome. Am J Med 1971;50:772-80.
2 Bredin CP. The Guillain-Barre syndrome. The unsolvedcardiovascular problems. 11 JIMed Sci 1977;146:273-9.
3 Haymaker W, Kernohan JW. The Landry-Guillain-Barre syndrome. Medicine (Baltimore) 1949 ;28:59-141.
Barraclough MA, Sharpey-Schafer EP. Hypotension
3*
989
from absent circulatory reflexes. Lancet 1963;1:1121-6.
5Birchfield RI, Shaw CM. Postural hypotension in theGuillain-Barre syndrome. Ar-ch Neurol 1964;10:149-57.
6 Marshall J. The Landry-Guillain-Barre syndrome.Brain 1963;86:55-66.
Low PA, Walsh JC, Huang CY, McLeod JG. Thesympathetic nervous system in diabetic neuropathy-a clinical and pathological study. Br-ain 1975 ;98:341-56.
'Low PA, Walsh JC, Huang CY, McLeod JG. Thesympathetic nervous system in alcoholic neuropathy-a clinical and pathological study. Brain 1975;98:357-64.
Stewart PM, Hensley WJ. An acute attack of variegateporphyria complicated by severe autonomic neuro-pathy. Aust NZJ Med 1981 ;1 1:82-3.
l Tuck RR, McLeod JG. Autonomic dysfunction in theLandry-Guillain-Barre syndrome. Clin Exp Neurol1978 ;15 :197-203.
Smyth HS, Sleight P, Pickering GW. Reflex regulationof arterial pressure during sleep in man. A quanti-tative method of assessing baroreflex sensitivity.Circ Res 1969;24:109-21.
12 Levin AB. A simple test of cardiac function based uponthe heart rate changes induced by the Valsalvamanoeuvre. Am J Cardiol 1976;18:90-9.
13 Snedecor GW, Cochran WG. Statistical method.s.6th ed, Ames, Iowa: Iowa State University Press,1967.
14 Korner P1, West MJ, Shaw JB, Uther JB. "Steady-state" properties of the baroreceptor-heart ratereflex in essential hypertension in man. Clin E-ApPharmacol P/hYvsiol 1974;1 :65-76.
15 Robinson BF, Epstein SE, Beiser GD, Braunwald E.Control of the heart rate by the autonomic nervoussystem. Studies in man on the interrelation betweenbaroreceptor mechanisms and exercise. Cir-c Res1966;19:400-1 1.
16 Currens, JH. A comparison of the blood pressure in thelying and standing positions: a study of five hundredmen and five hundred women. Am Heart J 1948;35:646-54.
17Ridley A, Hierons R, Cavanagh JB. Tachycardia andthe neuropathy of porphyria. Lancet 1968;2:708-10.
18 Wheeler T, Watkins PJ. Cardiac denervation indiabetes. Br- Med J 1973 ;4:584-6.
19 Guz A, Noble MIM,Widdicombe JG, Trenchard D,Mushin WW, Makey AR. The r6le of vagal andglossopharyngeal afferent nerves in respiratorysensation, control of breathing and arterial pressureregulation in conscious man. Clin Sci 1966 ;30 :161-70.
20 Heymans C, Neil C. Reflexogenic areas of the cardio-vascular system. London: J & A Churchill, 1958.
21 Ripley RC, Hollifield JW, Nies AS. Sustained hyper-tension after section of the glossopharyngeal nerve.Am J Med 1977;62:297-302.
22 Rowell LB, Detry JM, Blackman JR, Wyss C. Import-ance of the splanchnic vascular bed in human bloodpressure regulation. J Appl PhYsiol 1972;32:213-20.
23 Kirschheim HR. Systemic arterial baroreceptor re-
Protected by copyright.
on April 3, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.11.983 on 1 Novem
ber 1981. Dow
nloaded from

Tuck, McLecod
flexes. Physiol Rev 1976;56:100-76.24 Burke D, Sundlof G, Wallin BG. Postural effects on
muscle nerve sympathetic activity in man. J ofPhysiol (London) 1977;272:399-414.
25 Shepherd JT. R6le of veins in circulation. Circulation1966 ;33 :484-91.
26 Watson WE. Venous distensibility of the hand duringValsalva's manoeuvre. Br Heart J 1962;24:26-30.
27 Watson WE. Some circulatory responses to Valsalva'smanoeuvre in patients with polyneuritis and spinalcord disease. J Neurol Neurosurg Psychiatry 1962;25:19-23.
28 Davidson DLW, Jellinek EH. Hypertension andpapilloedema in the Guillain-Barre syndrome. JNeurol Neurosurg Psychiatry 1977 ;40 :144-8.
29 Bennett T, Hosking DJ, Hampton JR. Baroreflexsensitivity and responses to the Valsalva manoeuvrein subjects with diabetes mellitus. J Neurol NeurosurgPsychiatry 1976;39:178-83.
30 Asbury AK, Arnason BG, Adams RD. The in-flammatory lesion in idiopathic polyneuritis. Itsr6le in pathogenesis. Medicine (Baltimore) 1969;48:173-215.
31 Roseman E, Aring CD. Infectious polyneuritis.Medicine (Baltimore) 1941 ;20 :463-94.
32 Appenzeller 0, Marshall J. Vasomotor disturbance inLandry-Guillain-Barre syndrome. Arch Neurol 1963;9 :368-72.
33 White JC, Smithwick RH. The autonomic nervous
system anatomy, physiology and surgical application.2nd ed. London: Macmillan, 1944.
34 List CF, Peet MM. Sweat secretion in man. II Anatomicdistribution of disturbances in sweating associatedwith lesions of the sympathetic nervous system.Arch Neurol 1938;40:27-43.
3 Matsuyama H, Haymaker W. Distribution of lesionsin the Landry-Guillain-Barre syndrome, withemphasis on involvement of the sympathetic system.Acta Neuropathol (Berl) 1967;8:230-41.
36 Perel A, Reches A, Davidson JD. Anaesthesia in theGuillain-Barre syndrome. Anaesthesia 1977 ;32 :357-260.
3 Page M McB, Watkins PJ. Cardiorespiratory arrestand diabetic autonomic neuropathy. Lancet 1978;1:14-16.
990
Protected by copyright.
on April 3, 2022 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.11.983 on 1 Novem
ber 1981. Dow
nloaded from