Embed Size (px)
Citation preview
Assertive Continuing Care for Adolescents
Mark D. Godley, Ph.D., Susan H. Godley, Rh.D.,
Michael L. Dennis, Ph.D., Rod Funk, B.S., and
Lora L. Passetti, M.A.
Chestnut Health Systems
Bloomington, IL
This work is supported by grants from the National Institute on Alcoholism & Alcohol Abuse, the SAMHSA Center for Substance Abuse Treatment, and the Illinois Division of Alcoholism & Substance Abuse. The opinions are those of the author and do not reflect official positions of the government.
CollaboratorsSeveral colleagues at Chestnut served as co-
investigators or collaborators on this study. Their contributions made this work possible: Loree Adams, Becky Buddemeyer, Michael Dennis, Rod Funk, Susan Godley, Jen Hammond, Tracy Karvinen, Matt Orndorff, Lora Passetti, Laura Sloan, Ben Wells, Jen White, and Kelli Wright
And…Drs. H. Perl & J. Hough, NIAAA; R. Muck & J.
Buttler, CSAT; and M. Whitter, Illinois OASA
Questions Why is continuing care important? What have we learned about continuing
care in treatment programs? What is an “assertive” approach to
continuing care? What is the critical roll of supervision in
Assertive Continuing Care (ACC)? How does ACC compare to standard
practice in terms of implementation and outcome?
Why is Continuing Care Important?
Like many other illnesses, addiction is a chronic, relapsing condition.
Brown et al., 1989: 60% of youth relapsed in first 90 days after res. tx.
Dennis reports that most youth treated in the CYT outpatient study moved in and out of recovery.
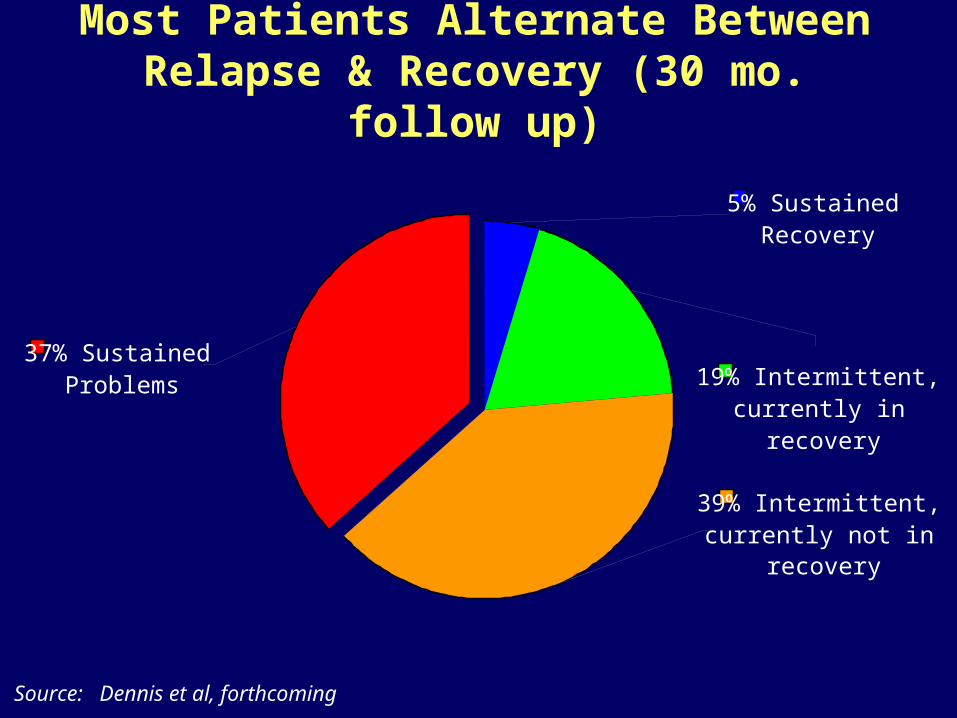
Most Patients Alternate Between Relapse & Recovery (30 mo. follow up)
Source: Dennis et al, forthcoming
37% Sustained Problems
5% Sustained Recovery
19% Intermittent, currently in
recovery
39% Intermittent, currently not in
recovery
Hypertension
Adherence to medication is less than 60%
Adherence to diet & exercise is less than 30%
Re-treated in 12 months: 50-60%
(McLellan, 2003; Treatment Research Institute)
Diabetes
Adherence to medication is less than 50%
Adherence to diet & exercise is less than 30%
Re-treated in 12 months: 30-50%
(McLellan, 2003; Treatment Research Institute)
Asthma
Adherence to medication is less than 30%
Re-treated in 12 months: 60-80%
(McLellan, 2003; Treatment Research Institute)
What Predicts Relapse in these Illnesses?
1. Poor adherence to behavior change requirements (diet, exercise, medication compliance)
2. Low Socioeconomic Status3. Low Family Support4. Psychiatric Co-Morbidity
(McLellan, 2003; Treatment Research Institute)
Why is Continuing Care Research in Addiction Treatment Important?
Existing studies reveal high levels of relapse after treatment
The evidence for continuing care is not yet clearly established (McKay, 2001)
Almost no continuing care studies of adolescents in the scientific literature
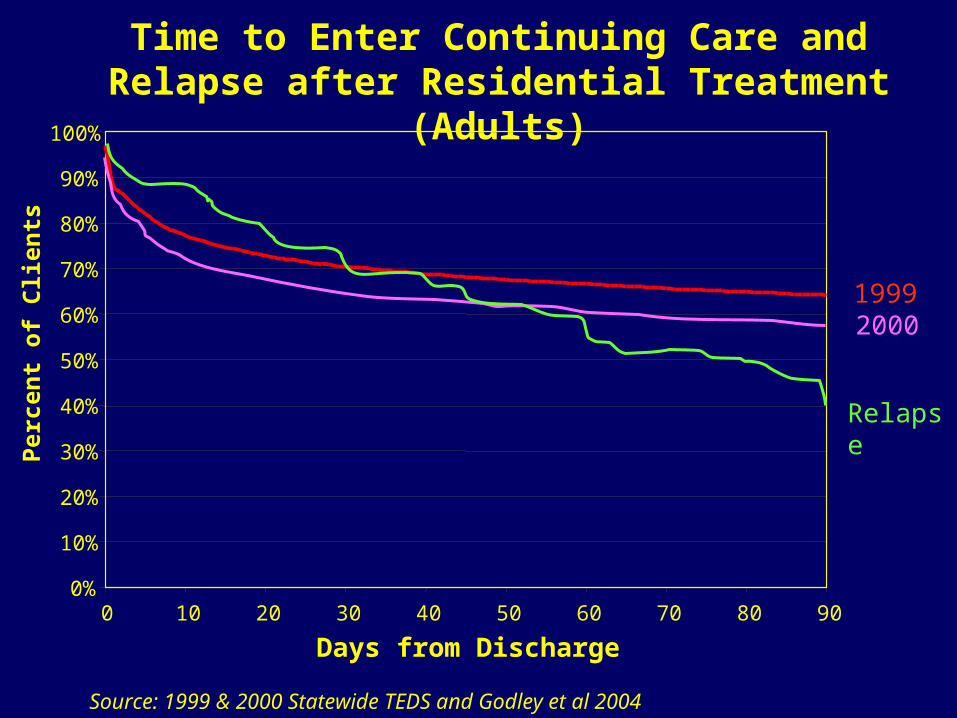
Time to Enter Continuing Care and Relapse after Residential Treatment (Adults)
Source: 1999 & 2000 Statewide TEDS and Godley et al 2004
1999
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 10 20 30 40 50 60 70 80 90
Days from Discharge
Per
cen
t o
f C
lien
ts
2000
Relapse
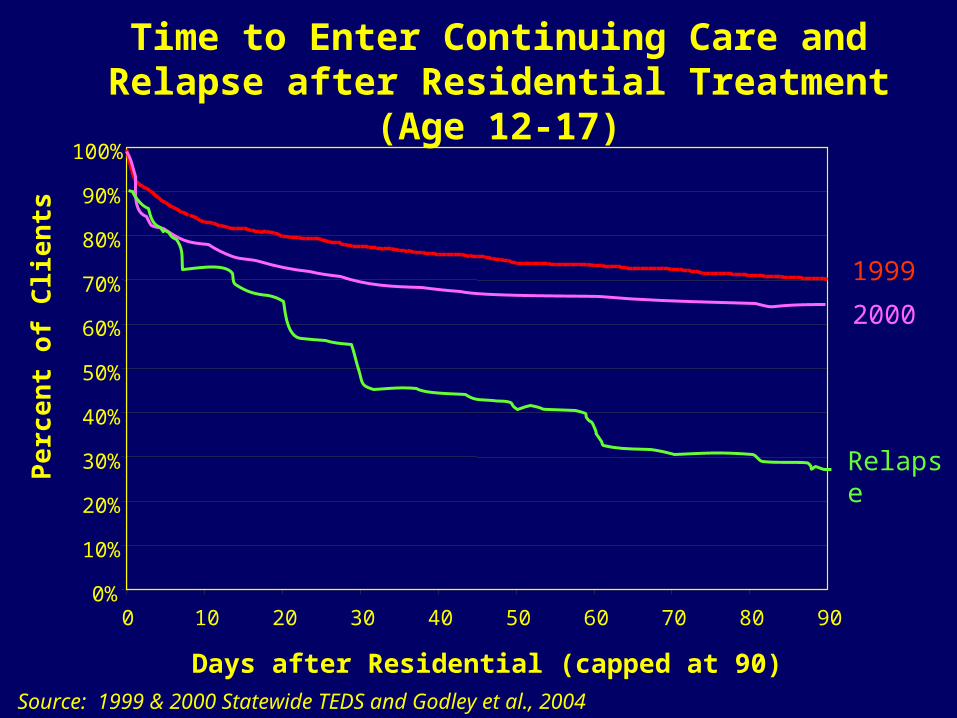
Time to Enter Continuing Care and Relapse after Residential Treatment (Age 12-17)
Source: 1999 & 2000 Statewide TEDS and Godley et al., 2004
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 10 20 30 40 50 60 70 80 90
Days after Residential (capped at 90)
Pe
rce
nt
of
Clie
nts
1999
2000
Relapse
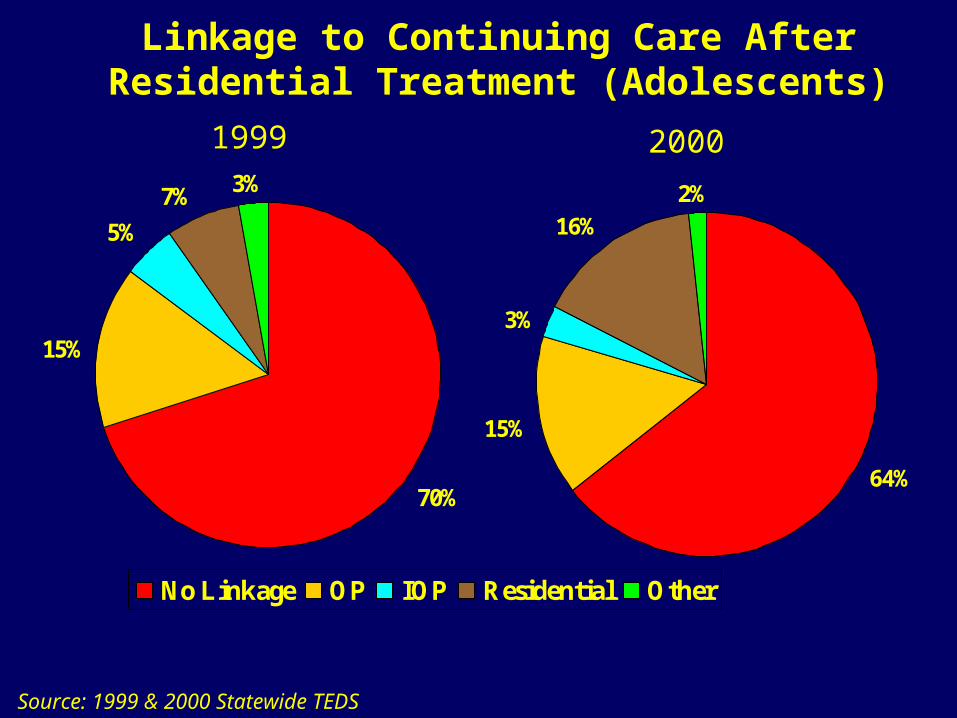
Linkage to Continuing Care After Residential Treatment (Adolescents)
Source: 1999 & 2000 Statewide TEDS
70%
5%
7% 3%
15%
64%
15%
3%
16%
2%
No Linkage OP IOP Residential Other
1999 2000
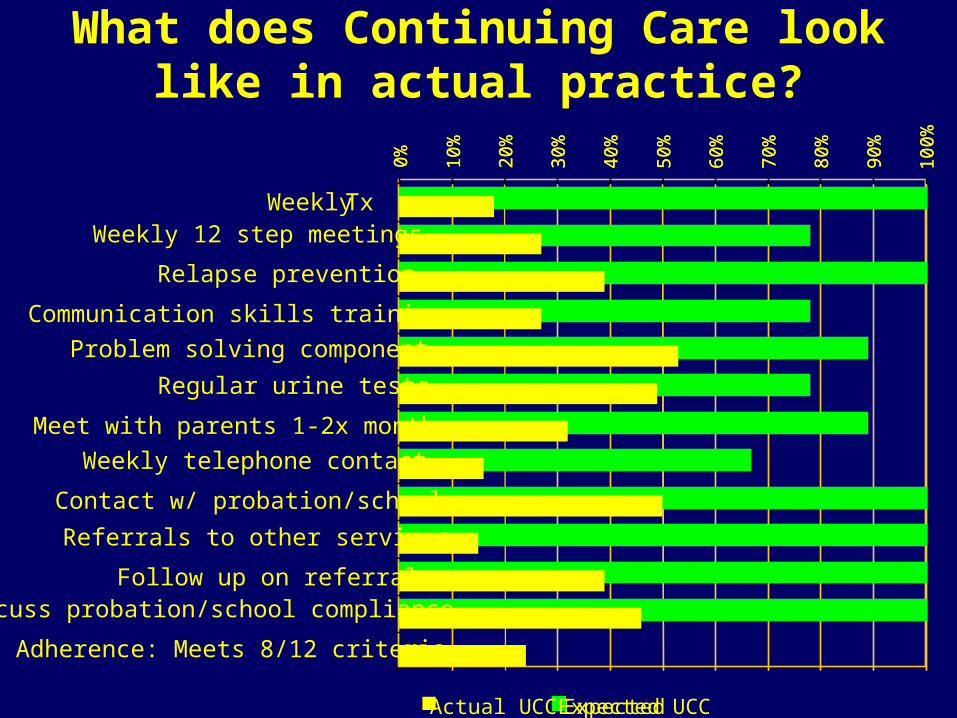
What does Continuing Care look like in actual practice?
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Expected
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Expected UCC
Weekly Tx Weekly 12 step meetings
Regular urine tests
Contact w/ probation/school
Follow up on referrals
Relapse prevention
Communication skills training
Problem solving component
Meet with parents 1-2x month
Weekly telephone contact
Referrals to other services
Discuss probation/school compliance
Adherence: Meets 8/12 criteria
Actual UCC
Barriers to Continuing Care
Typical referral process is passive, emulating medical clinics, and presumes the patient is motivated
Treatment Fatigue Reimbursement methods do little
to encourage continuing care Assertive approaches shift the
responsibility for linkage from the client to the provider
Examples of Assertive Approaches Recovery Management Check-ups
(Dennis, Scott, & Funk, 2003) Multisystemic Therapy (Henggeler, 1999) Tarrant Co. Juvenile Services-TCAP; Family
Preservation (Woods & Haene, 2002) Case Monitoring and Telephone Support
(Foote & Erfurt, 1991; Stout et al., 1999) Assertive Continuing Care Study (Godley
et al., 2002)
Suggested Goals of CC Encouraging and Priming Prosocial
Activities Reduce Social Risk Social Skill Development Monitoring to Prevent Relapse* Support* Linkage to Other Services Re-Intervention for Major Relapse**Essential CC Functions
A Controlled Study of the Effectiveness of Assertive Continuing Care
Research Questions
To determine the effectiveness of usual vs. assertive continuing care following residential treatment in:engaging and retaining youth in continuing care services
linking youth to additional services reducing AOD use and problems
Who was eligible to participate in the study?
Adolescents admitted to residential treatment (ASAM Level 3 care)
Length of stay of 7 days or longer (not required to have a successful discharge)
Reside in one of our “aftercare target counties”
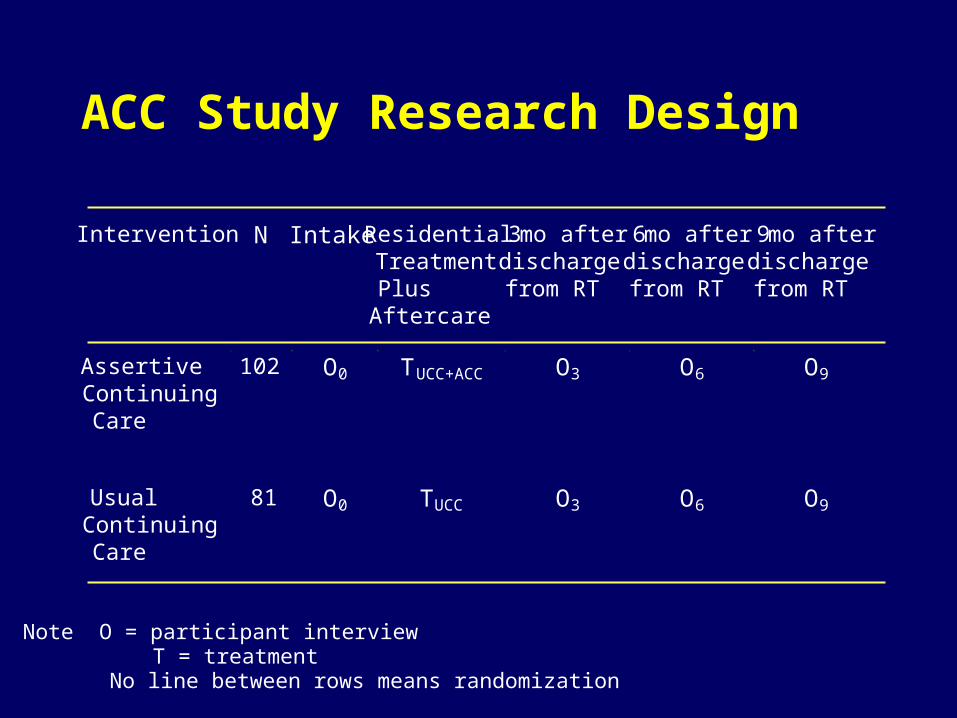
ACC Study Research Design
Intervention N Intake ResidentialTreatmentPlusAftercare
3 mo afterdischargefrom RT
6 mo afterdischargefrom RT
9 mo afterdischargefrom RT
AssertiveContinuingCare
102 O0 TUCC+ACC O3 O6 O9
UsualContinuingCare
81 O0 TUCC O3 O6 O9
Note O = participant interview T = treatment No line between rows means randomization
Core Measures
GAIN-I and GAIN M90 Form 90 TLFB BAC and Urine tests Collateral Assessment Form
Recruitment and Follow-up
81% of eligible clients agreed to participate
93% of all participants were interviewed at baseline, 3, 6, and 9 months
96% of all follow-up interviews were completed within two weeks of due date
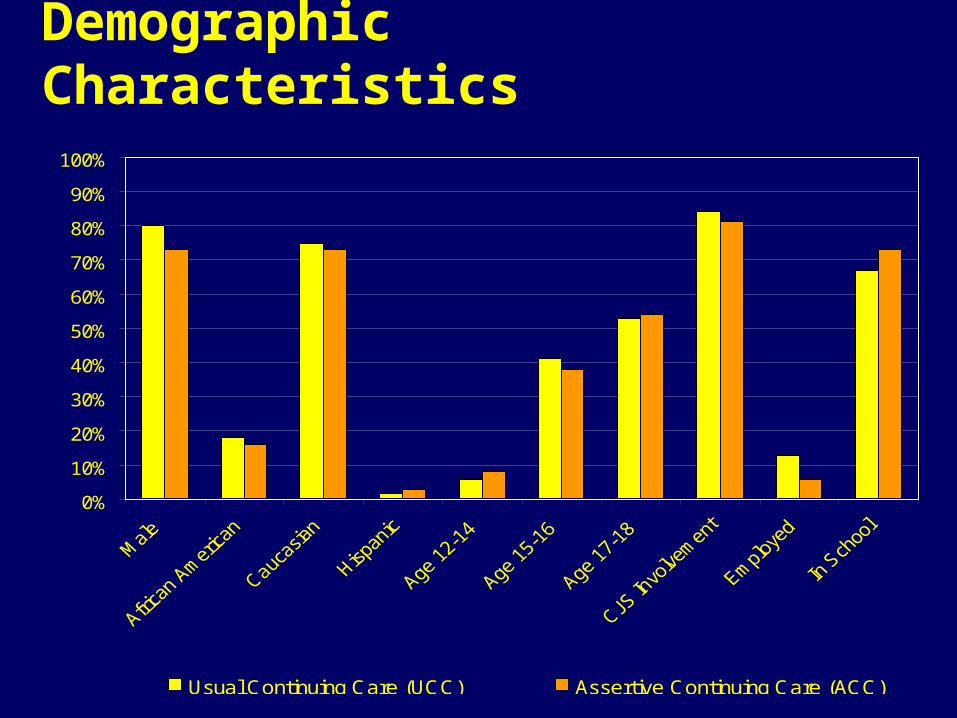
Demographic Characteristics
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Usual Continuing Care (UCC) Assertive Continuing Care (ACC)
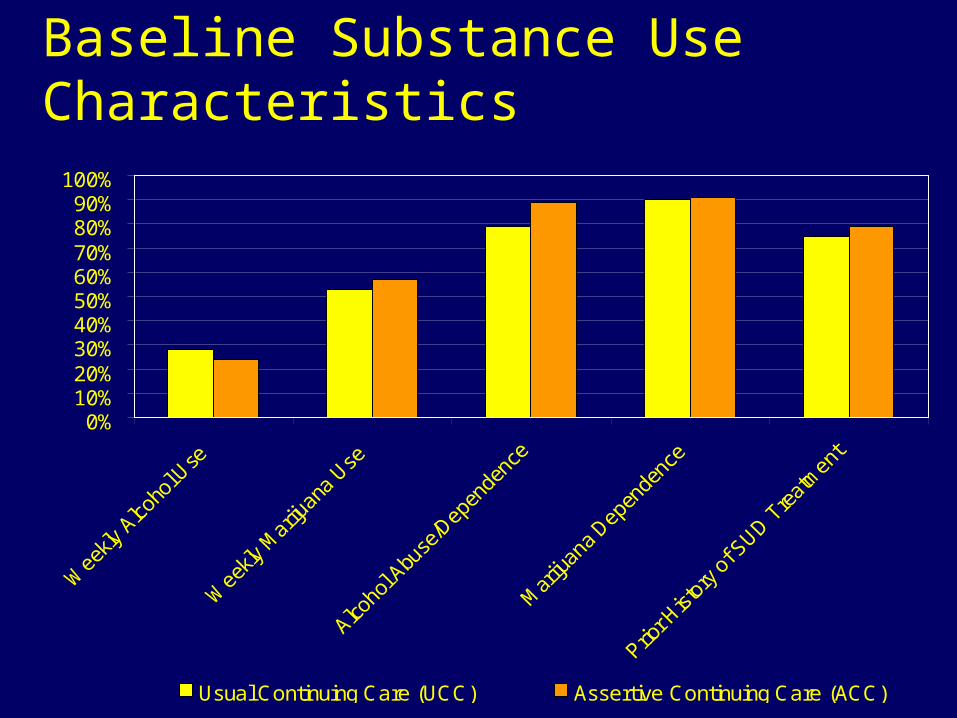
Baseline Substance Use Characteristics
0%10%20%30%40%50%60%70%80%90%
100%
Usual Continuing Care (UCC) Assertive Continuing Care (ACC)
Residential Treatment
Approach Length of Stay
Average LOS - 49 days for both groups
1- 3 weeks: 25% ACC - 28% UCC 4-12 weeks: 68% ACC - 71% UCC 13+ weeks: 6% ACC - 2% UCC
Rate of Successful Completion 50% ACC - 53% UCC
Features of the Assertive Continuing Care Intervention
Home Visits Sessions for patient, parents, and
together Sessions based on ACRA manual
(Godley, Meyers et al., 2001) Case Management based on ACC
manual (Godley et al, 2001) to assist with other issues (e.g., job finding, medication evaluation)
Monitoring ACC Implementation
Weekly Case Review Tracking Form Therapist Skillfulness Rating Form Procedure checklists completed
independently by therapist and supervisor
100% of sessions taped until certification
Monitoring Implementation
Simple monitoring systems work best
Monitor client contact and intervention procedures
Monitor total caseload weekly Weekly feedback on caseload
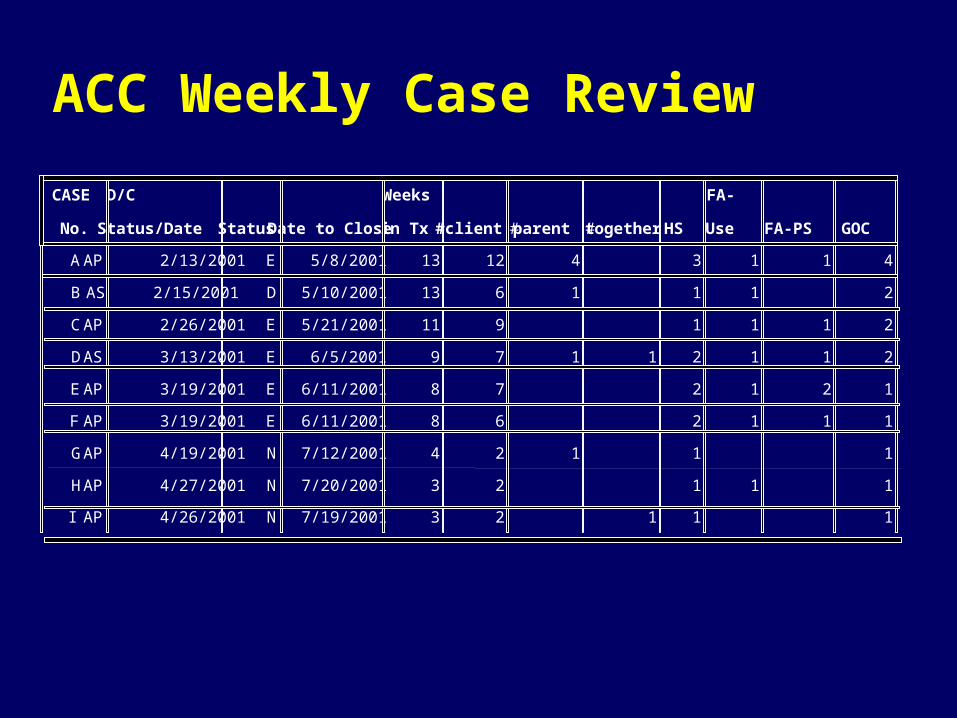
ACC Weekly Case Review
CASE
No.
D/C
Status/Date Status Date to Close
Weeks
in Tx #client #parent #together HS
FA-
Use FA-PS GOC
A AP 2/13/2001 E 5/8/2001 13 12 4 3 1 1 4
B AS 2/15/2001 D 5/10/2001 13 6 1 1 1 2
C AP 2/26/2001 E 5/21/2001 11 9 1 1 1 2
D AS 3/13/2001 E 6/5/2001 9 7 1 1 2 1 1 2
E AP 3/19/2001 E 6/11/2001 8 7 2 1 2 1
F AP 3/19/2001 E 6/11/2001 8 6 2 1 1 1
G AP 4/19/2001 N 7/12/2001 4 2 1 1 1
H AP 4/27/2001 N 7/20/2001 3 2 1 1 1
I AP 4/26/2001 N 7/19/2001 3 2 1 1 1
Engagement & Retention
94% of ACC vs. 54% of UCC group enrolled ACC averaged 14.1 aftercare sessions vs.
6.3 sessions for the UCC group ACC median sessions 10 compared to 2 for
UCC group No difference in average UCC sessions
between groups ACC significantly more likely to receive
referrals to other human service providers
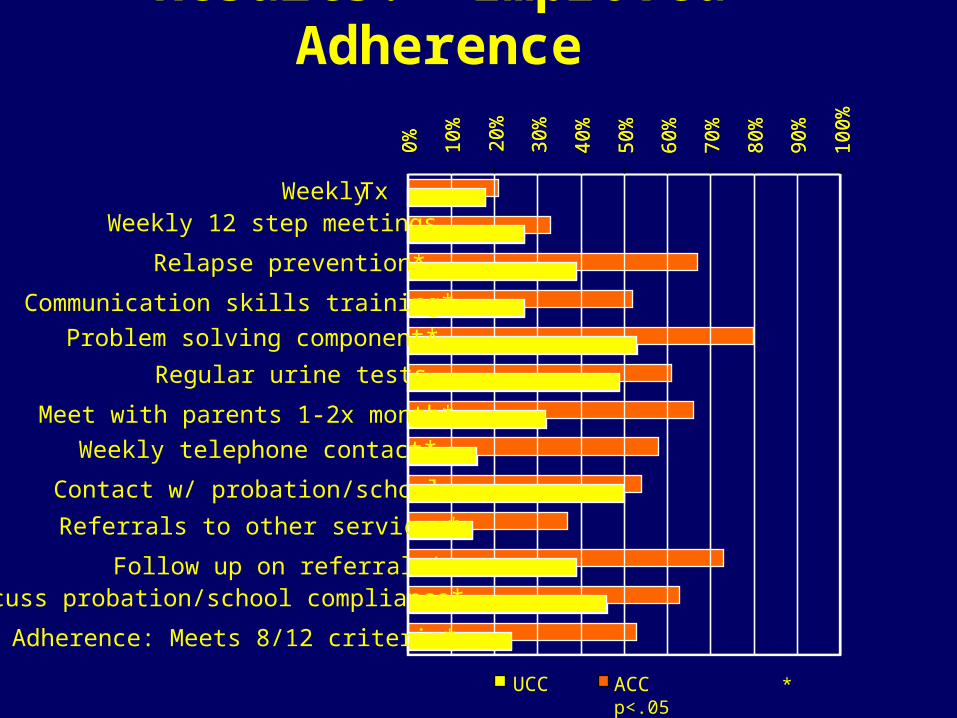
Results: Improved Adherence
ACC * p<.05
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Weekly Tx Weekly 12 step meetings
Regular urine tests
Contact w/ probation/school
Follow up on referrals*
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Relapse prevention*
Communication skills training*
Problem solving component*
Meet with parents 1-2x month*
Weekly telephone contact*
Referrals to other services*
Discuss probation/school compliance*
Adherence: Meets 8/12 criteria*
UCC
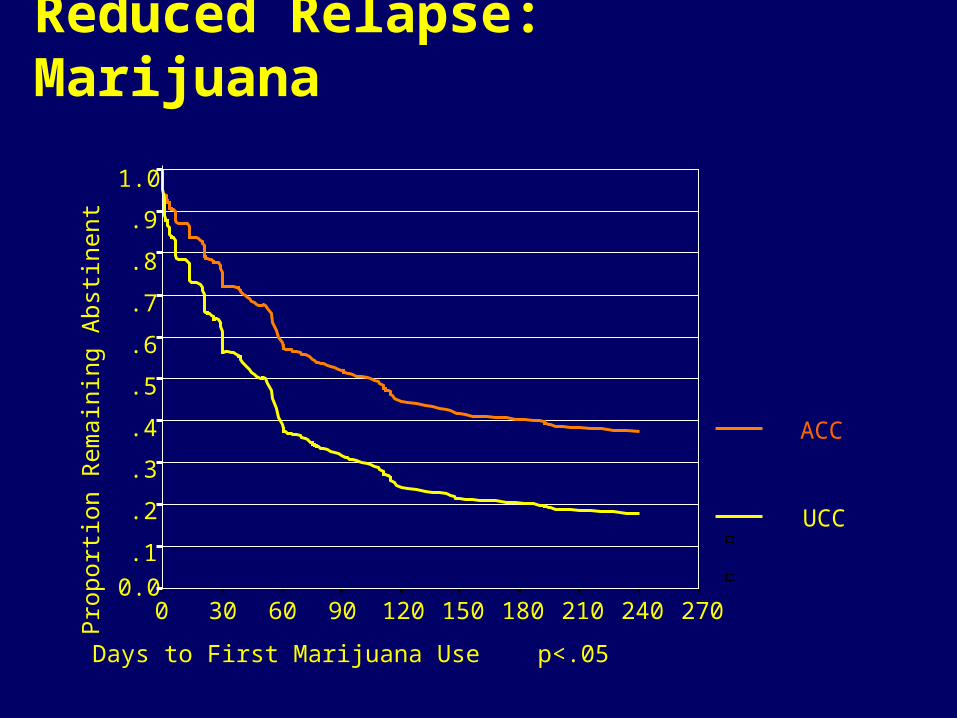
Reduced Relapse: Marijuana
Days to First Marijuana Use p<.05
2702402101801501209060300
Pro
port
ion
Rem
aini
ng A
bstin
ent
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
ACC
UCC
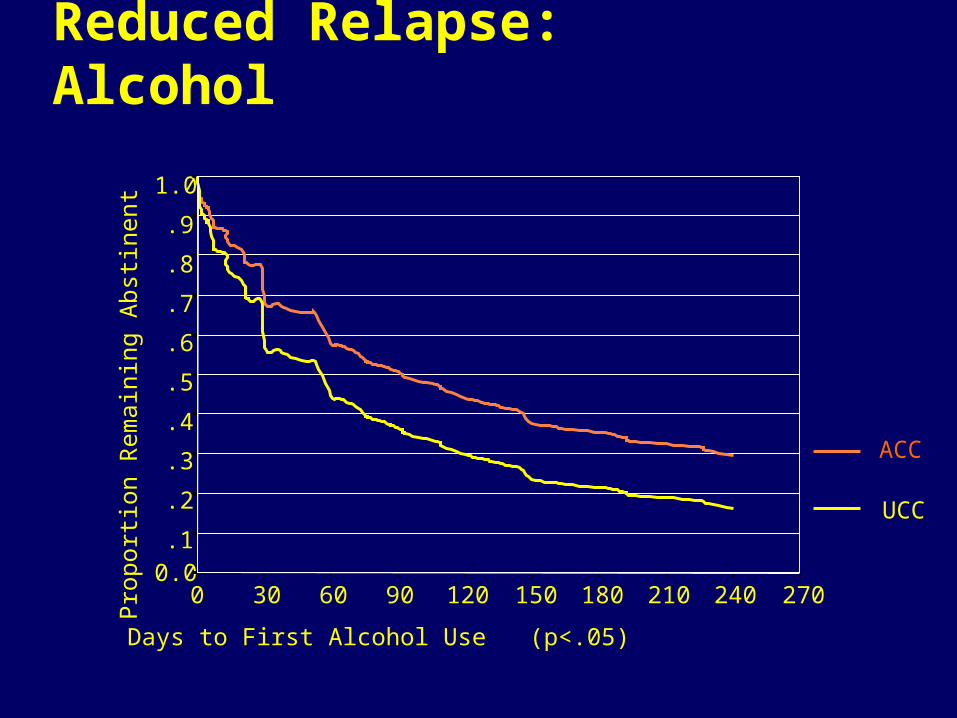
Reduced Relapse: Alcohol
Days to First Alcohol Use (p<.05)
2702402101801501209060300
Pro
port
ion
Rem
aini
ng A
bstin
ent
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.10.0
ACC
UCC
0
5
10
15
20
25
30
35
40
45
Pre-treatment ACC Phase Post ACC
Day
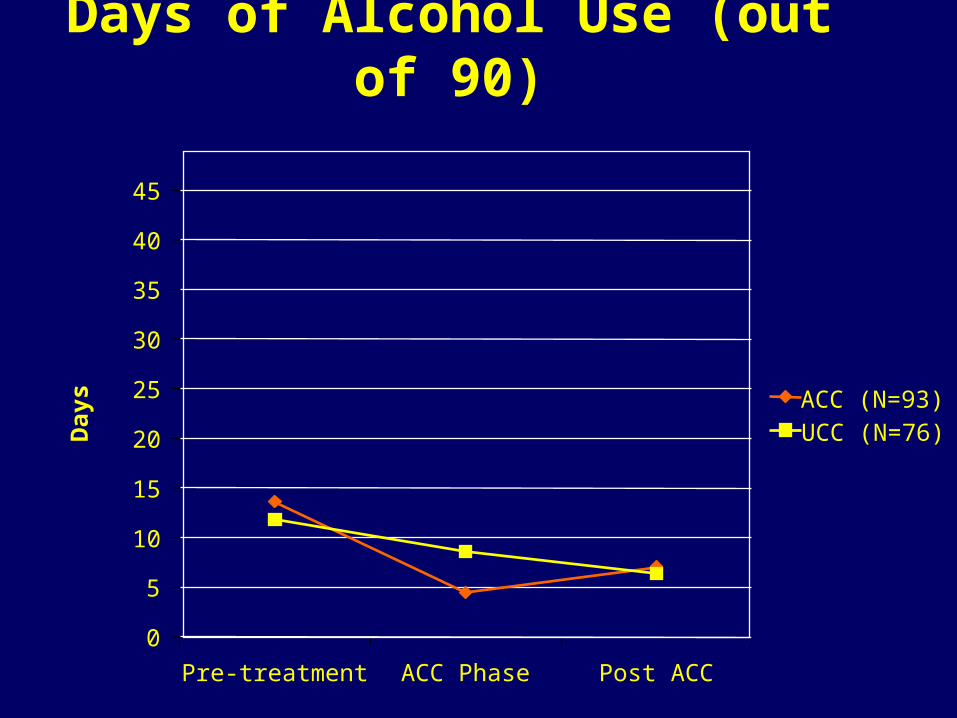
s ACC (N=93)UCC (N=76)
Days of Alcohol Use (out of 90)
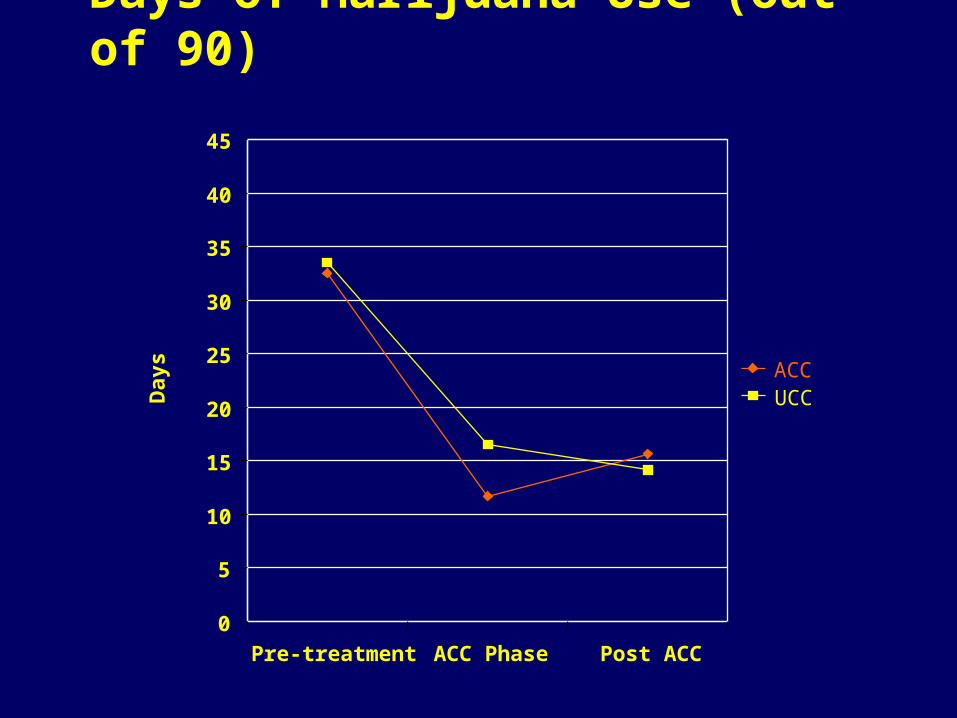
Days of Marijuana Use (out of 90)
0
5
10
15
20
25
30
35
40
45
Pre-treatment ACC Phase Post ACC
Day
s
ACCUCC
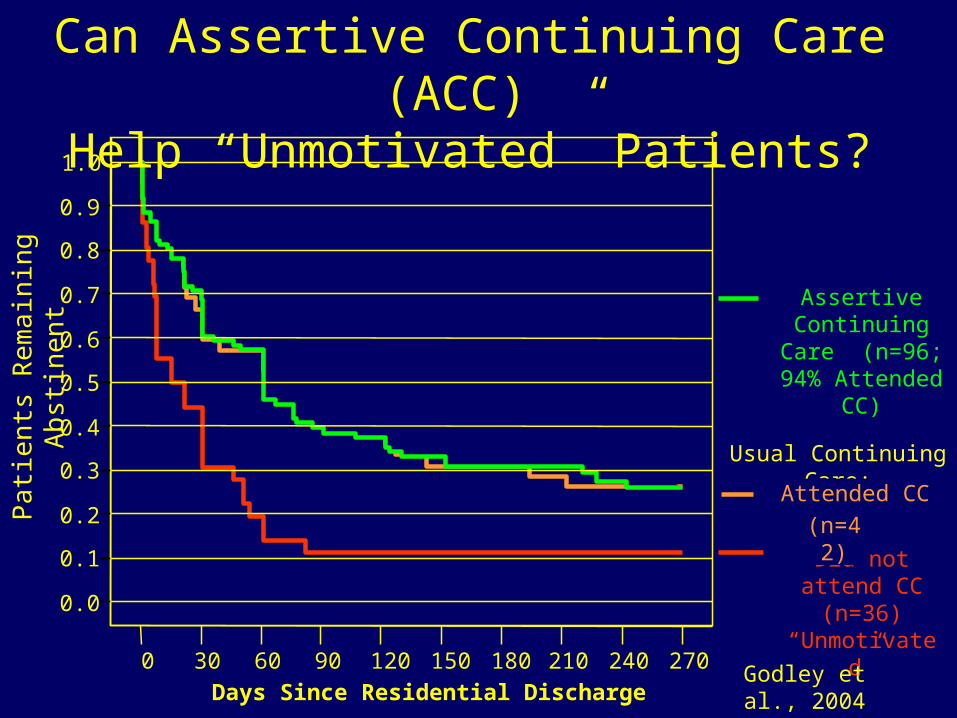
0 30 60 90 120 150 180 210 240 270
Days Since Residential Discharge
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Usual Continuing Care:
Did not attend CC (n=36)
“Unmotivated”
Attended CC
(n=42)
Assertive Continuing Care
(n=96; 94% Attended CC)
Pat
ient
s R
emai
ning
Abs
tinen
tCan Assertive Continuing Care (ACC)
Help “Unmotivated” Patients?
Godley et al., 2004
Conclusions Failure to link to CC is the norm in
actual practice For those who do link retention beyond
4 hours of service is less than 50% ACC is clearly superior to UCC in linking
and retaining youth in continuing care ACC clients receive more referrals to
ancillary services than UCC clients ACC was significantly better in
preventing relapse than UCC
Next Steps for Research Additional research is necessary to further
improve relapse prevention effectiveness We need to test models of continuing care
following outpatient treatment We need to test ways of improving 12 step
attendance among adolescents We need to better address the co-occurring
problems of adolescents Research is needed to test longer term
models of CC with adolescents-particularly decreasing levels of contact for monitoring, support, and re-intervention
Contact Information
Mark D. Godley, Ph.D.Chestnut Health Systems720 W. Chestnut St.Bloomington, IL 61704309.827.6026 [email protected]
Introduction
Our Background
Experience with adolescents involved in residential and outpatient treatment
Is it Aftercare or Continuing Care?