Embed Size (px)
Citation preview

A validity study of the Washington Circle continuity of care performance measure
Mark D. GodleyBryan R. GarnerRodney R. FunkLora L. PassettiSusan H. Godley
Chestnut Health Systems Bloomington, IL
2008 Research Society on Alcoholism ConferenceWashington, D.C.

This work was supported by the National Institute of
Alcohol Abuse and Alcoholism (2 R01-AA010368) Dr. Margaret Mattson, Project Official
Dr. Peter Delany, Past Project Official
Acknowledgement

What is the Washington Circle?
• Formed in 1998 by the Center for Substance Abuse Formed in 1998 by the Center for Substance Abuse Treatment, the Washington Circle (WC) is a multi-Treatment, the Washington Circle (WC) is a multi-disciplinary group of providers, researchers, managed disciplinary group of providers, researchers, managed care representatives, and public policy representatives.care representatives, and public policy representatives.
• Goals of the WC were to:Goals of the WC were to:• Develop and pilot test performance measures for Develop and pilot test performance measures for
substance abuse treatment programssubstance abuse treatment programs• Promote adoption of these measures by public and Promote adoption of these measures by public and
private stakeholdersprivate stakeholders

What are the Washington Circle Performance Measures?
• IdentificationIdentification – number of individuals with a substance abuse – number of individuals with a substance abuse or dependence diagnosis who received a substance abuse or dependence diagnosis who received a substance abuse treatment service during the year among those who were treatment service during the year among those who were eligible for serviceseligible for services
• InitiationInitiation – number of individuals with an outpatient index – number of individuals with an outpatient index service (i.e., first treatment service preceded by a 60 day service (i.e., first treatment service preceded by a 60 day service-free period) during the year who received a second service-free period) during the year who received a second treatment service (other than detoxification or crisis service) treatment service (other than detoxification or crisis service) within 14 days after the index outpatient servicewithin 14 days after the index outpatient service
• EngagementEngagement – number of individuals with an outpatient index – number of individuals with an outpatient index service during the year who received two additional services service during the year who received two additional services (other than detoxification or crisis service) within 30 days after (other than detoxification or crisis service) within 30 days after initiation. initiation.

Washington Circle Continuity of Care Performance Measure
Continuity of care after…Continuity of care after…
• Assessment ServiceAssessment Service
• Detoxification Detoxification
• Short-term ResidentialShort-term Residential
• Long-term ResidentialLong-term Residential
• InpatientInpatient
Continuity of Care is defined as the number of Continuity of Care is defined as the number of individuals with an additional service within 14 individuals with an additional service within 14 days after discharge from the previous days after discharge from the previous service.service.
Source: Garnick, Lee, Horgan, & Acevedo (2007)

Current Research on the Relationship between Washington Circle Performance Measures and Outcomes
• Harris, Humphreys, & Finney (2006)Harris, Humphreys, & Finney (2006)• Used data from 5,723 patients who had received substance abuse Used data from 5,723 patients who had received substance abuse
treatment from one of 110 Veterans Affairs programs.treatment from one of 110 Veterans Affairs programs.• Found higher rates of initiation were significantly related to greater Found higher rates of initiation were significantly related to greater
improvements in reports of drug use (but not alcohol use).improvements in reports of drug use (but not alcohol use).• Neither identification nor engagement was significantly related to Neither identification nor engagement was significantly related to
improvements in either alcohol or drug use.improvements in either alcohol or drug use.
• Garnick et al., (2007)Garnick et al., (2007)• Used data from 5,169 outpatient clients included in the Oklahoma Used data from 5,169 outpatient clients included in the Oklahoma
Department of Mental Health and Substance Abuse Services Department of Mental Health and Substance Abuse Services (ODMHSAS) database.(ODMHSAS) database.
• Although initiation alone was not significantly associated with being Although initiation alone was not significantly associated with being arrested or incarcerations, clients who initiated and engaged were arrested or incarcerations, clients who initiated and engaged were significantly less likely to be arrested or incarcerated in the significantly less likely to be arrested or incarcerated in the following year. following year.

Study Goals
• Overall GoalOverall Goal: Conduct a validity test of the : Conduct a validity test of the Washington Circle performance measure for Washington Circle performance measure for Continuity of CareContinuity of Care
• Subgoals are to test whether:Subgoals are to test whether:• Assertive Continuing Care (ACC) approaches improve Assertive Continuing Care (ACC) approaches improve
compliance with the WC Continuity of Care measure compliance with the WC Continuity of Care measure regardless of whether they fail to successfully complete regardless of whether they fail to successfully complete residential treatment;residential treatment;
• Continuity of Care improves abstinence outcomes Continuity of Care improves abstinence outcomes regardless of residential discharge type.regardless of residential discharge type.

Why study continuity of care?
• Like many illnesses, alcohol or other drug Like many illnesses, alcohol or other drug dependence is characterized by periods of remission dependence is characterized by periods of remission and relapse (McLellan et al., 2000; Scott et al., 2005)and relapse (McLellan et al., 2000; Scott et al., 2005)
• 60-70% of youth relapse in first 90 days after res. tx. 60-70% of youth relapse in first 90 days after res. tx. (Brown et al., 1989; Godley et al., 2002) (Brown et al., 1989; Godley et al., 2002)
• Dennis et al., (2004) found that two thirds of youth Dennis et al., (2004) found that two thirds of youth treated in the CYT outpatient study moved in and out treated in the CYT outpatient study moved in and out of recovery during the post-treatment study phase.of recovery during the post-treatment study phase.
• McKay (2005) reports benefit from extended McKay (2005) reports benefit from extended interventions that provide care consistent with patient interventions that provide care consistent with patient need.need.

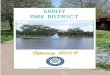
Source: 2000 Statewide DARTs
2000
Continuing Care Following Residential Treatment for Adolescents in Illinois
64%
15%
3%
16%2%
No Linkage OP IOP Residential Other

Why do so many patients fail to initiate continuing care?
May never get a referral if ASA/AD discharge type
Referral to another provider organization is “hit or miss”
Even transferring to another counselor within agency can be a problem.
Low Motivation/Treatment Fatigue - ready to be finished
Logistical/financial disincentives Providers view it as the patients’ responsibility

53% Have Unfavorable Discharges - Adolescents
Source: Data received through August 4, 2004 from 23 States (CA, CO, GA, HI, IA, IL, KS, MA, MD, ME, MI, MN, MO, MT, NE, NJ, OH, OK, RI, SC, TX, UT, WY) as reported in Office of Applied Studies (OAS; 2005). Treatment Episode Data Set (TEDS): 2002. Discharges from Substance Abuse Treatment Services, DASIS Series: S-25, DHHS Publication No. (SMA) 04-3967, Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from http://wwwdasis.samhsa.gov/teds02/2002_teds_rpt_d.pdf .
0% 20% 40% 60% 80% 100%
Outpatient(37,048 discharges)
IOP(10,292 discharges)
Detox(3,185 discharges)
STR(5,152 discharges)
LTR(5,476 discharges)
Total(61,153 discharges)
Completed Transferred ASA/ Drop out AD/Terminated

Who Links to Continuing Care?
Source: CSAT ART Grantees Wilcoxon (Gehen) statistic (df=2)=79.83, p < .001.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 10 20 30 40 50 60 70 80 90
Days from Residential Discharge
Per
cent
of C
lient
s Li
nked
Planned / transferwithin agency
Planned / Referred toother agency
Unplanned Discharge

Assertive Continuing Care Experiments
Samples: 183 adolescents in Study 1 and 342 in Study 2 meeting DSM IV dependence on alcohol, marijuana or other drug; meets ASAM Level 3 placement criteria, residential stay of 7+ days, returning to target
counties, not a ward of state.
Instruments: Global Appraisal of Individual Needs (GAIN);BAC and Urine tests for Cannabis and Cocaine; Collateral
Interviews
Design: Random Assignment to either UCC or different ACC conditions. Active CC phase was 90 days after residential discharge
Follow-up: Over 90% of all participants received a follow up interview at 3, 6, and 9 months after residential treatment

Features of Assertive Conditions
Meet once with client before res. discharge Clinician is responsible for initiating CoC within
14 days of discharge. Different conditions rec’d either A-CRA (Godley
et al., 2001), CM (Petry, 2000), or A-CRA+CM Sessions usually in the community
(home/school) Clinician helps patients comply with or obtain
needed services Limited transportation if needed to access
referral resources, job interviews, etc.

Compliance to WC Continuity of Care Standard
75%
55%
0%
20%
40%
60%
80%
100%
ACC UCC
22 = 19.17, = 19.17, pp < .001, d=.40 < .001, d=.40

Effect of CoC Compliance on Days of Abstinence
80%69%
0%
20%
40%
60%
80%
100%
Continuity of Care No Continuity ofCare
F F = 17.10, = 17.10, pp < .001, d=.44 < .001, d=.44
AlcoholAlcohol
70%
59%
Continuity of Care No Continuity of Care
F F = 10.74, = 10.74, pp < .001, d=.35 < .001, d=.35
MarijuanaMarijuana

Continuity of Care by Completion Status & Condition
84%
71%
0%
20%
40%
60%
80%
100%
ACC UCC
22 = 6.51, = 6.51, pp < .01, d=.31 < .01, d=.31
Residential CompletersResidential Completers
64%
33%
ACC UCC
Residential Non-CompletersResidential Non-Completers
22 = 17.71, = 17.71, pp < .001, d=.59 < .001, d=.59
Nearly Nearly
DoubledDoubled

79%
71%
79%
65%
0%
20%
40%
60%
80%
100%
Completers Non-Completers
Percent of Days Abstinent from Alcoholby Completion Status
82% 84% 78%
63%
Completers Non-Completers
Continuity ofCare
No Continuity ofCare
Interaction for Completion by CoCInteraction for Completion by CoCF F = 5.90, = 5.90, pp < .05, f-index=.14 < .05, f-index=.14
ACCUCCUCC
Main Effect for CoCMain Effect for CoC
F F = 5.18, = 5.18, pp < .05, d=.42 < .05, d=.42
N=62 N=27 N=22 N=40 N=134 N=25 N=89 N=50
23 of these 25 (93%) adolescents received
CoC more than 14 days after discharge
6 of these 27 (22%) adolescents received
CoC more than 14 days after discharge

69%
58%
69%
58%
0%
20%
40%
60%
80%
100%
Completers Non-Completers
Percent of Days Abstinent from Marijuanaby Completion Status
74%77%
64%
52%
Completers Non-Completers
Continuity ofCare
No Continuity ofCare
Interaction for Completion by CoC Interaction for Completion by CoC F F = 3.19, = 3.19, pp =.075, f-index=.11 =.075, f-index=.11
ACCACCUCCUCC
Main Effect for CoCMain Effect for CoC
F F = 4.11, = 4.11, pp < .05, d=.36 < .05, d=.36
N=62 N=27 N=22 N=40 N=134 N=25 N=89 N=50

Support for the WC CoC performance measure was found
Continuity of Care was significantly higher Continuity of Care was significantly higher among adolescents assigned to ACC, among adolescents assigned to ACC, regardless of residential treatment completion regardless of residential treatment completion status.status.
Continuity of Care was found to be significantly Continuity of Care was found to be significantly associated with higher rates of abstinence from associated with higher rates of abstinence from both Alcohol and Marijuana.both Alcohol and Marijuana.
Future research on continuing care should include patients who do not successfully complete treatment.
Conclusions

The outcome data is based on self-report Continuity of Care (CoC) within 14
days was imputed for a sub-sample of the UCC condition,
The sample is from two midwestern treatment sites, predominantly caucasian males, limiting generalizability
Study Limitations

Future Research Directions
Additional research is necessary to determine the clinical significance of these findings.
• Additional validity studies are necessary, Additional validity studies are necessary, especially to test whether CoC is robust especially to test whether CoC is robust even if the 14 day standard is not met.even if the 14 day standard is not met.
Similar research with adults is needed.• What patient subgroups do not seem to What patient subgroups do not seem to
need it (i.e., they do fine w/out CoC)?need it (i.e., they do fine w/out CoC)?• What patient subgroups appear to need What patient subgroups appear to need
CoC but do not benefit from it?CoC but do not benefit from it?

For More Information
To Download this presentation, go to:www.chestnut.org/LI/Posters/index.html
Mark D. Godley, Ph.D.Chestnut Health Systems720 W. Chestnut St.Bloomington, IL 61704309.827.6026 [email protected]