-
7/31/2019 Arrutmias en Pediatria
1/12
Pediatric Arrhythmias
Debra Hanisch, RN, MSN, CPNP
During the past decade, our awareness and understanding of
arrhythmias in children has expanded immensely. This
reportdiscusses the more commonly encountered pediatric rhythm
disturbances, including sinus node dysfunction, the various formsof
supraventricular tachycardia, ventricular tachycardia, long QT
syndrome, and the atrioventricular blocks. The
electrocar-diographic characteristics, electrophysiological
mechanisms, clinical presentation, and current acute and chronic
managementoptions for each are described.Copyright 2001 by W.B.
Saunders Company
N
ORMAL CONDUCTION IS characterized by
an impulse that is initiated by the sinoatrial(SA) node, located
in the right atrium near the
superior vena cava junction, propagated through
the cardiac conduction system across the atria,
converging at the atrioventricular (AV) node, pro-
ceeding down the His bundle to the right and left
bundle branches, and finally spreading through-
out the Purkinje fibers to depolarize the ventricles
(Figure 1). Characteristic electrocardiographic
(ECG) findings of normal sinus rhythm include
upright P-waves and QRS complexes in leads I and
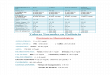
aVF. Age-appropriate parameters for heart rate, PR
interval, and QRS duration are presented in Table
1 (Liebman, 1982).
The majority of children who are diagnosed with
arrhythmias have structurally normal hearts. For
children with complex congenital heart disease,
advances in surgical and medical management
have resulted in improved survival. However,
these children may be at risk for developing early
and late postoperative arrhythmias. This report dis-
cusses the more common pediatric arrhythmias
found in both structurally normal hearts and in
patients with congenital heart disease. ECG char-
acteristics, electrophysiological mechanisms, clin-
ical presentation, and acute and chronic manage-ment options for
each rhythm abnormality are
described.
SINUS NODE DYSFUNCTION
Sinus node dysfunction (SND) encompasses a
number of arrhythmias including sinus bradycar-
dia, sinus pauses or arrest, sinoatrial exit block,
escape rhythms, and brady-tachy syndromes. On
the ECG, sinus bradycardia has the appearance of
sinus rhythm, but at a slower rate than expected for
age (Table 2). Sinus pauses, sinus arrest, and exit
block produce electrical pauses in the rhythm.Junctional escape
rhythms occur when the atrial
rate slows to the point where the AV nodes auto-
maticity takes over. Slow heart rates may predis-
pose the heart to certain tachyarrhythmias, such as
atrial flutter.
Typically, SND occurs as a result of surgical
injury to the sinoatrial node or its arterial supply.
Surgical procedures associated with a higher inci-
dence of SND include the Mustard or Senning
procedures for d-transposition of the great arteries,
the Fontan procedure for single ventricle physiol-
ogy, closure of atrial septal defects, and repair oftotal
anomalous pulmonary venous return. How-
ever, whenever cannulation for cardiopulmonary
bypass is done near the superior vena cavaright
atrial junction, there is a risk for SND.
Nonsurgical causes of SND include right atrial
dilation due to pressure or volume overload. SND
may be seen in cardiomyopathies or inflammatory
conditions, such as myocarditis, pericarditis, and
rheumatic fever. Increased vagal tone and certain
drugs, especially antiarrhythmic agents, may result
in SND as well. In anorexia nervosa, resting heart
rates tend to be 20 beats/min slower than inmatched controls
(Panagiotopoulos, McCrindle,
From the Lucile Packard Childrens Hospital at Stanford,
Palo Alto, CA.
Address reprint requests to Debra Hanisch, RN, MSN,
CPNP, Pediatric Cardiology, Lucile Packard Childrens Hos-
pital at Stanford, 750 Welch Rd., Suite #305, Palo Alto, CA
94304.
Copyright 2001 by W.B. Saunders Company
0882-5963/01/1605-0008$35.00/0
doi:10.1053/jpdn.2001.26571
351Journal of Pediatric Nursing, Vol 16, No 5 (October),
2001
-
7/31/2019 Arrutmias en Pediatria
2/12
Hick, & Katzman, 2000). Conditioned athletes also
have slower-than-average resting heart rates. Mod-
ified criteria are used to diagnose SND in these
latter two populations.
Sinus node dysfunction may occur at any age.As a surgical
complication, SND may occur im-
mediately after surgery or may not manifest for up
to 10 years or longer after surgery. Most children
with SND are asymptomatic. Of those who are
symptomatic, the most common symptoms appear
to be fatigue, exercise intolerance, dizziness, and
syncope. Sudden death is rare.
Acute management of the bradycardic child with
hemodynamic instability includes adequate venti-
lation, oxygenation, and administration of epineph-
rine (0.01 mg/kg) or, if the bradycardia is vagally
mediated, atropine (0.02 mg/kg; minimum dose 0.1mg). If there is
no response to these medications,
temporary pacing should be instituted (Hazinski,
Cummins, & Field, 2000).
For long-term management, permanent pace-
maker therapy for SND is indicated when symp-
toms are associated with bradycardia or chrono-
tropic incompetence (Gregoratos et al., 1998).
Pacing may also be warranted in individuals with
brady-tachy syndrome, in which slowing of the
heart rate may mediate the onset of tachycardia. In
this situation, antibradycardia pacing either alone
or in combination with antitachycardia pacing maybe used.
Prophylactic permanent pacing is a con-
sideration for patients with SND who are placed on
antiarrhythmic agents that prolong the QT interval,
such as amiodarone, to prevent further slowing of
the heart rate and/or pause-dependent torsades de
pointes (Martin & Kugler, 1999).
SUPRAVENTRICULAR TACHYCARDIA
Supraventricular tachycardia (SVT) refers to a
sustained tachyarrhythmia that originates above
Table 1. Normal Heart Rates, PR Intervals, and QRS Durations
in Children
Age
Heart Rate (bpm)PR Interval
(ms)QRS Duration
(ms)M Range
1 day 119 94-145 70-120 50-841-7 days 133 100-175 70-120
40-793-30 days 163 115-190 70-110 40-731-3 months 154 124-190
70-130 50-803-6 months 140 111-179 70-130 60-806-12 months 140
112-177 80-130 50-801-3 years 126 98-163 80-150 50-803-5 years 98
65-132 90-150 60-845-8 years 96 70-115 100-160 50-808-12 years 79
55-107 100-170 50-84
12-16 years 75 55-102 110-160 40-80
Adapted and reprinted with permission (Liebman, 1982).
Figure 1. Normal conductionsystem.
352 DEBRA HANISCH
-
7/31/2019 Arrutmias en Pediatria
3/12
the bundle of His. SVT is the most common ab-
normal tachyarrhythmia in children, with an esti-
mated incidence in the pediatric population of
0.1% to 0.4% (Ludomirsky & Garson, 1990). The
rhythm typically appears with an abrupt onset as a
regular, narrow QRS tachycardia. Rates vary from
130 to 300 beats/min depending on the patients
age and the SVT mechanism. On the ECG, the
QRS complex is usually normal in configuration,but in less than
10% of cases the QRS is wide due
to aberrant conduction to the ventricles (Ludomir-
sky & Garson, 1990).
Several SVT mechanisms have been identified.
The more common ones are described here (Figure
2). The vast majority of SVT rhythms are either
due to a re-entrant circuit, with or without an
accessory pathway, or an automatic ectopic focus.
Triggered activity accounts for a very small per-
centage of SVT.
Atrioventricular reciprocating tachycardia
(AVRT) is a common type of SVT that relies on at
least two electrical connections between the atriaand
ventricles: the AV node and an accessory
pathway (more than one accessory pathway may
be present). Conduction proceeds antegrade down
one pathway and retrograde up the other to form a
Table 2. Sinus Bradycardia
ECG Criteriaa 24-Hour Ambulatory ECG Criteriaa
Age Group Heart Rate Age Group Heart Rate
Infants to 3 years 100 bpm Infants to 1 year of age 60 bpm
sleeping; 80 bpm awakeChildren 3-9 years 60 bpm Children 1-6 years
60 bpmChildren 9-16 years 50 bpm Children 7-11 years 45 bpm
Adolescents 16 years 40 bpm Adolescents , young adu lts 40
bpmHighly trained athletes 30 bpm
aBased on data from Kugler, JD (Kugler, 1990).
Figure 2. Common mechanisms of SVT.
353PEDIATRIC ARRHYTHMIAS
-
7/31/2019 Arrutmias en Pediatria
4/12
re-entrant circuit. Nearly 75% of the SVT rhythms
in children are mediated by accessory pathways.
The most common form of AVRT is orthodromic
reciprocating tachycardia, which involves ante-
grade conduction down the AV node to the ventri-
cles and retrograde conduction up the accessory
pathway to the atria. Antidromic reciprocating
tachycardia (down the accessory pathway, up the
AV node) occurs in less than 10% of patients.
Wolff-Parkinson-White (WPW) syndrome is a
frequently encountered type of AVRT. WPW is
characterized by a manifest pathway that is evident
on a 12-lead ECG during sinus rhythm. Pre-exci-
tation of the ventricle through the accessory path-
way (Kent bundle) appears as a delta wave, or
slurred upstroke into the QRS complex, along with
a shortened PR interval (Figure 3). There is an
increased incidence of WPW in patients with Eb-
steins anomaly, tricuspid atresia, double-outletright ventricle,
and hypertrophy cardiomyopathy
(Van Hare, 1999). Among patients with AVRT,
about half have a concealed accessory pathway,
meaning that pre-excitation is not evident on the
12-lead ECG (Deal, 1998).
The permanent form of junctional reciprocating
tachycardia (PJRT) is a type of AVRT in which
the retrograde conduction through the accessory
pathway is slow, producing retrograde (inverted)
P-waves with a longer RP interval than is seen
in other types of AVRT. This slow conduction
through the accessory pathway contributes to theincessant nature
of this form of SVT.
AV nodal re-entrant tachycardia (AVNRT) is
distinguished from AVRT in that, instead of an
accessory pathway, dual pathways exist within the
AV node. Typically, conduction proceeds ante-
grade down a slow pathway and retrograde up a
fast pathway to create a re-entrant circuit. On the
ECG, retrograde P-waves are buried within the
QRS complex. AVNRT accounts for nearly 15%
of SVT in the pediatric population, but rarely ap-
pears before the age of two years (Ko, Deal, Stras-
burger, & Benson, 1992). AVNRT is not associ-
ated with congenital heart disease (Deal, 1998).
Intra-atrial re-entrant tachycardia (IART),
commonly referred to as atrial flutter, is a re-
entrant tachycardia that is confined to the atria.
Propagation of IART relies on an electrical path-
way within the atria with both an area of slow
conduction and an anatomic obstruction that re-
sults in unidirectional block. This milieu for IART
exists after atrial surgery for congenital heart dis-
ease, such as the Mustard/Senning operation for
transposition of the great arteries, the Fontan pro-
cedure for single ventricle physiology, repair of
total anomalous pulmonary venous return, and
atrial septal defect closure. In fact, almost 95% of
atrial flutter diagnosed beyond infancy is associ-
ated with structural heart disease (Deal, 1998). On
ECG, characteristic saw-tooth waves (flutter
waves) are seen at rates of 200 to 400 bpm withvariable AV
conduction (Figure 4).
Atrial ectopic tachycardia (AET) is a primary
atrial tachycardia that arises from an automatic
focus in the atria but outside the sinus node. Atrial
rates may range from 90 to 330 bpm with variable
AV block (Sokoloski, 1999). On ECG, distinct
P-waves are seen with a morphology that is differ-
ent from the normal sinus P-wave. AET is present
in only a small percentage of children with SVT
but has proven to be quite resistant to medical
management. As a rapid, incessant tachycardia,
AET may lead to a dilated cardiomyopathy that isusually
reversible with successful abolition of the
automatic focus.
Junctional ectopic tachycardia (JET) is an au-
tomatic tachycardia that originates in the AV junc-
tion or His bundle. The ventricular rates generally
range from 150 to 300 bpm. The ECG may reveal
AV dissociation with the ventricular rate being
faster than the atrial rate (Figure 5). However, in
some cases, 1:1 VA conduction occurs, with the
retrograde P-wave superimposed on the QRS com-
plex. JET is encountered more frequently as a
Figure 3. Wolff-Parkinson-White (WPW).
354 DEBRA HANISCH
-
7/31/2019 Arrutmias en Pediatria
5/12
postoperative arrhythmia. The heart rate may start
out more slowly but then rapidly increases within a
few hours after cardiopulmonary bypass. Hemody-namic compromise
occurs as a result of the fast
heart rate and loss of the atrial contribution to
ventricular filling (atrial kick). If not adequately
controlled, JET is associated with a high mortality
in the postoperative patient. Infrequently, JET may
present as a congenital arrhythmia with a familial
predilection.
The relative incidence of these different types of
SVT varies with age (Table 3). AVRT has a rela-
tively high incidence among newborns and infants,
with male patients affected more than female pa-
tients. In many of these infants SVT will sponta-neously resolve
by 6 to 12 months of age, but over
30% will have recurrence later in life (Perry &
Garson, 1990). AVNRT is virtually unseen in ne-
onates but occurs more frequently with increasing
age. AVNRT represents over 50% of the SVT in
adults. The incidence of primary atrial tachycardias
remains fairly constant across all age groups.
Infants with SVT tend to present with nonspe-
cific symptoms such as irritability, lethargy, poor
feeding and, after 24 to 48 hours, signs of conges-
tive heart failure (CHF) (Table 4). In the presence
of associated congenital heart disease, CHF may
develop more quickly. In severe cases, hemody-namic compromise
may occur and lead to respira-
tory distress, hypotension, and shock. The older
child with SVT may describe palpitations, a fast
heart rate, chest discomfort, or dizziness. In rare
instances, syncope or cardiac arrest may ensue.
Acute management of SVT depends on the pa-
tients age and condition. In the presence of shock
or cardiovascular collapse, immediate synchro-
nized cardioversion with 0.5 to 1.0 joule/kg is
warranted. In the more stable patient, 0.1 to 0.2
mg/kg of adenosine may be administered intrave-
nously by rapid bolus to induce transient AV block(Hazinski et
al., 2000). If the SVT is a re-entrant
tachycardia that uses the AV node as part of its
circuit, adenosine will break the tachycardia. If not,
adenosine may at least be helpful in unveiling the
tachycardia mechanism during the brief time AV
conduction is interrupted (Figure 4). IART re-
sponds to either DC cardioversion or atrial over-
drive pacing. Automatic tachycardias (AET, JET)
do not respond to DC cardioversion or overdrive
pacing. Intravenous amiodarone has proven to be
Figure 4. Atrial flutter with 2:1 block.
Figure 5. Junctional ectopic tachycardia (JET).
355PEDIATRIC ARRHYTHMIAS
-
7/31/2019 Arrutmias en Pediatria
6/12
the most effective agent for the acute management
of these challenging automatic tachycardias. For
JET, atrial or dual-chamber pacing at a rate above
the JET rate can improve hemodynamics by estab-
lishing AV synchrony. Maintaining normothermia,
or even mild hypothermia, may lower the JET rate
to facilitate pacing therapy. For the very stable
pediatric patient with SVT, vagal maneuvers may
be attempted initially to terminate the tachycardia,
such as placing a bag of ice water over the face to
elicit the diving reflex, inducing rectal stimulation
with a thermometer (infants), or performing a Val-
salva maneuver (older child).
Chronic management of SVT also varies de-
pending on the patients age, symptoms, frequency
of tachycardia episodes, presence of structural
heart disease, and risk for sudden death. Most SVT
in infants involves an accessory pathway and can
usually be controlled with oral digoxin or propran-
olol to slow conduction across the AV node. If the
SVT is refractory to these agents, flecainide, so-
talol, or amiodarone may be effective but carry agreater risk of
adverse effects. Combinations of
drugs may be needed in some cases. More than
90% of infants diagnosed with SVT before two
months of age will have spontaneous resolution of
their arrhythmia by eight months of age (Perry &
Garson, 1990). These patients are usually weaned
off their antiarrhythmic medications after 6 to 12
months of therapy but are monitored for late re-
currence. In the older child with infrequent epi-
sodes and mild symptoms, a management option
may be to do nothing. For others with more prob-
lematic tachycardia, chronic antiarrhythmic drug
therapy may be indicated. Radiofrequency (RF)
catheter ablation becomes a reasonable therapeutic
option in the school-aged child or adolescent. RF
ablation is performed in the cardiac catheterization
or electrophysiology laboratory with percutane-
ously inserted electrode catheters to map the elec-
trical pathways and an ablation catheter to create
strategically placed thermal lesions to interrupt im-
pulse conduction. The success rate with RF abla-
tion varies according to the type of SVT and insti-
tutional experience, but has been reported to be
83% to 96% (Kugler et al., 1994; Kugler, Danford,
Houston, & Felix, 1997). RF ablation has been
performed successfully in infants with SVT refrac-
tory to medical management but, because of theirsmall size, is
associated with a much greater risk
for complications, such as AV block or perforation
of the heart.
VENTRICULAR TACHYCARDIA
Ventricular tachycardia (VT) is defined as three
or more consecutive premature ventricular com-
plexes (PVCs) at a rate greater than 120 beats/min
but usually less than 250 beats/min. The QRS
complexes are typically wide with AV dissociation
or, in rare cases, 1:1 retrograde VA conduction. VT
may be nonsustained (lasting less than 10 seconds)or sustained
(lasting 10 seconds or longer). Mono-
morphic VT refers to tachycardia in which all the
QRS complexes have a similar morphology, in
contrast to polymorphic VT with multiform com-
plexes. Torsades de pointes (twisting of the
points) is a type of polymorphic VT characterized
by rapid, wide, undulating QRS complexes that
appear to be spiraling around an axis (Figure 6).
Table 3. Age-Related Incidence of SVTa
Age AVRT AVNRTPrimary Atrial Tachycardia
(IART, AET)
Prenatal/Neonate 80-85% 0% 15-20%Infant 80% 5% 15%1-5 years 65%
20-25% 10-15%
6-10 years 60% 30% 10-15%Adolescent 65-70% 20% 15%
aBased on data from Ko et al. (Ko et al., 1992).
Table 4. Differentiating Supraventricular Tachycardia From Sinus
Tachycardia
Supraventricular Tachycardia Sinus Tachycardia
History Nonspecific; lethargy or i rritabi lity, poorfeeding,
tachypnea, diaphoresis, pallor
Suggestive of volume loss, vomiting,diarrhea, blood loss, or
febrile illness
Examination Signs of congestive heart failure: tachypnea,moist
crackles, increased respiratoryeffort, poor perfusion,
hepatomegaly
Consistent with dehydration, fever, or bloodloss; clear lungs,
normal liver; may bedue to CHF in congenital heart disease
ECG Abrupt onset, heart rate 220 bpm,regular R-R intervals,
P-waves seen in50-60% with abnormal axis, narrowQRS in 90% of
SVTs
Gradual onset, heart rate usually less than200 bpm, variable R-R
intervals, normalP-wave axis, narrow QRS
Chest radiograph May have an enlarged heart, signs ofpulmonary
edema
Small or normal heart, clear lung fields(unless congenital heart
disease present)
Echocardiogram May have ventricular dilat ion or dysfunction
Usual ly normal
Adapted and reprinted with permission from Hanisch, D. (Hanisch
& Perron, 1992).
356 DEBRA HANISCH
-
7/31/2019 Arrutmias en Pediatria
7/12
Mechanisms for VT are not as well described as
for SVT, but appear to include re-entry (similar to
IART), abnormal automaticity, and triggered ac-
tivity.
The incidence of VT in the pediatric population
is unknown, but accounts for about 6% of patients
followed for tachyarrhythmia (Dick & Russell,
1998). The causes of VT in children are similar tothose for
PVCs. VT may be associated with severe
electrolyte or metabolic abnormalities, hypoxia,
hypothermia, or drug toxicity. Cardiac conditions
such as cardiomyopathy, myocarditis, arrhythmo-
genic right ventricular dysplasia, and ventricular
tumors (rhabdomyomas, hamartomas) may create a
substrate for VT. Surgery for congenital heart dis-
ease, particularly procedures that involve a ventric-
ulotomy (i.e., tetralogy of Fallot repair) have been
associated with an increased risk for early and late
postoperative VT. Another recognized cause of VT
is congenital or acquired long QT syndrome.VT may present at any
age and with varying
degrees of symptoms. Some children may present
with minimal symptoms despite their tachycardia;
however, most children will be symptomatic. In-
fants may be lethargic, tachypneic, and pale, and
may feed poorly. Mottling or cyanosis may be
present as well. Older children report palpitations,
chest discomfort, dizziness, nausea, or syncope. In
many instances, the child initially presents after
resuscitation from sudden cardiac death.
Acute management of VT in the unstable patient
should be focused on rapid termination of the
arrhythmia with synchronized cardioversion (0.5 to
1.0 joules/kg) or, if pulseless, defibrillation (2 to 4
joules/kg) (Hazinski et al., 2000). Intravenous li-
docaine, procainamide, or amiodarone may be
used to supress PVCs and further occurrences of
VT. Careful attention to maintaining normal elec-
trolyte values is necessary in the postresuscitation
period. In extreme cases of uncontrollable inces-
sant VT, extracorporeal membrane oxygenation(ECMO) support or a
ventricular assist device may
be required.
Chronic management options for VT are based
on the childs age and clinical condition. Antiar-
rhythmic drug therapy may be successful in sup-
pressing ventricular ectopy in postoperative pa-
tients; however, the potential for proarrhythmia
and depression of ventricular function must be
recognized. An implantable pacemaker/cardio-
verter-defibrillator (ICD) device, with or without
concomitant drug therapy, is indicated for selected
patients with cardiomyopathy, long QT syndrome,life-threatening
VT, and resuscitated sudden car-
diac death. RF ablation has been employed suc-
cessfully in some patients with discrete arrhythmo-
genic foci (Silka & Garson, 1999). For others,
surgical intervention either cryoablation, revi-
sion of previous congenital heart surgery, removal
of a cardiac tumor, or cardiac transplantmay be
necessary (Dick & Russell, 1998).
LONG QT SYNDROME
Congenital long QT syndrome (LQTS) is an
inherited disorder that affects the ion channels in
the heart, resulting in abnormal ventricular repo-
Figure 6. Torsades de pointes.
Figure 7. Mobitz I AV block (Wenckebach).
357PEDIATRIC ARRHYTHMIAS
-
7/31/2019 Arrutmias en Pediatria
8/12
larization and an increased risk for life-threatening
arrhythmias. LQTS is characterized by prolonga-
tion of the QT interval on ECG, usually measuring
greater than 440 to 460 ms. The diagnosis of
LQTS, however, is not based solely on the pres-
ence of a prolonged QT interval, but on additional
ECG findings, clinical presentation, and family
history. Typically on ECG, abnormal T-wave mor-
phology is present and may reflect the specific ion
channel that is affected. Patients with LQTS tend
to have abnormally low resting heart rates for their
age. A documented episode of torsades de pointes
lends further support to the diagnosis of LQTS.
Clinically, 60% of patients present with symptoms.
These symptoms include syncope or presyncope
(often associated with exercise, noise, or stress),
palpitations, seizure activity, and cardiac arrest.
Also, in 60% of cases, the family history is positive
for either a family member diagnosed with LQTSor a sudden,
unexplained premature death.
The incidence of LQTS is estimated to be 1 in
5,000 to 10,000, with a higher prevalence in female
patients in the adult age group, but a nearly equal
gender distribution in children. Male patients tend
to present at an earlier age and more often with
sudden cardiac death (Locati et al., 1998). Several
clinical associations have been identified with
LQTS, including congenital AV block (5%), con-
genital deafness (4.5%), congenital heart disease
(12%), and syndactyly (Garson et al., 1993; Marks,
Trippel, & Keating, 1995). Jervell and Lange-Nielson
syndrome represents the autosomal reces-
sive form of LQTS and is associated with congen-
ital deafness. Romano-Ward syndrome refers to the
autosomal dominant form of LQTS. The specific
types of LQTS that have been identified are listed
in Table 5. Approximately 50% of patients have
LQT1, 45% have LQT2, and 5% have LQT3. The
remaining types are relatively rare.
Management of LQTS is individualized, with
consideration given to the patients age and risk
factors. Typically, drug therapy with beta blocking
agents (propranolol, atenolol) is instituted. The use
of sodium channel blockers (mexiletine, pheny-
toin) for patients with identified LQT3 has been
advocated (Schwartz et al., 1995). Limited success
has been reported with potassium supplements and
spironolactone in selected patients with LQT2
(Compton et al., 1996). Pacemaker therapy is use-
ful in combination with beta blockade to pre-
vent bradycardia and pause-dependent torsades de
pointes. Increasing the heart rate with pacing also
helps to shorten the QT interval in these patients.
ICD placement is indicated for those who have
experienced a previous cardiac arrest or have failed
drug therapy. Tiered therapy consisting of beta
blockade and implantation of a pacemaker/ICD is
considered appropriate for high-risk patients. In
addition, the LQTS patient is instructed to avoid
triggers such as competitive athletics (LQT1), loudnoises
(LQT2), hypokalemia, and drugs that cause
QT prolongation.
ATRIOVENTRICULAR BLOCKS
Atrioventricular (AV) block describes delayed or
incomplete conduction of impulses through the AV
node. Three degrees of AV block are recognized.
First-degree AV block is defined as prolonged
conduction through the AV node; this produces a
prolonged PR interval on the ECG, but there is
consistent 1:1 AV conduction. Second-degree AV
block has two forms: Mobitz I and Mobitz II.Mobitz type I AV
block, also known as Wencke-
bach, is recognized on the ECG by its characteris-
tic pattern of a gradually lengthening PR inter-
val followed by a nonconducted P-wave (dropped
beat) (Figure 7). In Mobitz type II AV block, there
is intermittent failure of the P-wave to be con-
ducted, but wherever measurable PR intervals oc-
cur, they are consistent and do not lengthen. Gen-
erally, Mobitz II AV block produces a fixed ratio
of P-waves to QRS complexes (2:1 or 3:1), but
occasionally the AV block is variable. Third-de-
gree AV block is defined as complete failure of the
atrial impulses to be conducted to the ventricles.On the ECG, AV
dissociation is seen in which the
atrial rate is faster than the ventricular rate.
AV block may be congenital or acquired. Con-
genital AV block is estimated to have an incidence
of 1 in 22,000 live births (Ross & Gillette, 1999).
Approximately 25% to 30% of these children have
associated congenital heart disease, most com-
monly 1-transposition of the great arteries with
ventricular inversion. In addition, there appears to
be a strong association between SS-A/Ro or SS-
Table 5. Genes Associated With Low QT Syndrome
(Ackerman, 1998)
LQTS Gene Chromosome Ion Channel
LQT1 KVLQT1 11p15.5 K
LQT2 HERG 7q35-36 K
LQT3 SCN5A 3q21-24 Na
LQT4 Unknown 4q25-27 UnknownLQT5 KCNE1 (MinK) 21q22.1-22.2 K
LQT6 MiRPI 21 KaJLN1 KVLQT1 11p15.5 KaJLN2 KCNE1 (MinK)
21q22.1-22.2 K
Data from Ackerman, 1998.aAssociated with congenital
deafness.
358 DEBRA HANISCH
-
7/31/2019 Arrutmias en Pediatria
9/12
Table 6. Nursing Care of the Pediatric Arrhythmia Patient
Arrhythmia Clinical Symptoms Acute Management Chronic Management
Parent/Patient Education
Sinus nodedysfunction
Slow heart rateIrregular heart beatFatigueExercise
intolerance
DizzinessSyncope
Monitor rhythm andhemodynamic status
If unstable:Ventilate, oxygenate
EpinephrineAtropineIsoproterenololTemporary pacing
Pacemaker How to check pulse rateReport symptoms to
cardiologistPacemaker education if device
is implanted
Supraventriculartachycardia
Infant:Irritability,
lethargyPoor feedingPallorSweatingCHF
Monitor rhythm andhemodynamic status
If stable:Vagal maneuversOverdrive pacing
Adenosinemay be diagnosticand/or therapeutic (0.1-0.2 mg rapid
IV bolus)
Medications:Digoxin for non-WPW
onlyPropranololAtenololFlecainideSotalolAmiodarone
How to check pulse rateReport symptoms to cardiologistHow to
perform vagal
maneuvers (check withcardiologist first)
If symptomatic, go toemergency room
Older child:PalpitationsFast heart rate
Chest discomfortDizziness
If unstable:Synchronized cardioversion
(0.5-1.0 joule/kg)For JET,
IV amiodarone Overdrive pacing
RF ablation Medication teaching as neededProcedural teaching if
RF
ablation is planned
Ventriculartachycardia
Cardiac arrest Monitor rhythm andhemodynamic status
Medications:Amiodarone
How to check pulse rateHow to perform CPR
Infant:LethargyTachypneaPallorPoor feeding
CPR if neededSynchronized cardioversion
(0.5-1.0 joules/kg)If pulseless, defibrillation (2-4
joules/kg)
Beta-blockersVerapamil (in Verapamil-
sensitive VT)
Call 911 in the event ofsyncope or arrest
Medication teaching as neededAvoid medications that cause
QT prolongationOlder child:
PalpitationsChest discomfort
DizzinessNauseaSyncope
IV medications:AmiodaroneLidocaine
ProcainamideCorrect electrolyte imbalanceECMO or VAD for
uncontrolled
incessant VT
RF ablationICD
Procedural teaching if ICD isplanned
Activity restrictions as
prescribed by cardiologist
Long QTsyndrome
Syncope/presyncopeoftenassociated withexercise, noise,or
stress
PalpitationsSeizuresCardiac arrest
Monitor rhythm andhemodynamic status
For Torsades de Pointes:Initiate CPRSynchronized
cardioversionAdminister IV beta blocker
(Esmolol)Temporary overdrive pacing
to suppress VT
Medications:Beta blockers
PropranololAtenolol
?Alpha blockers?Na or Ca2 ion-channel
blockersPacemakerICD
How to check pulse rateHow to perform CPRCall 911 in the event
of
syncope or arrestFamily members need ECGs to
measure QT (hereditary)Medication teachingProcedural teaching
if
pacemaker or ICD isplanned
Avoid triggers:Competitive athleticsLoud noises
(LQT2)HypokalemiaMedications that cause QT
prolongation
AV block(2 or 3)
CHFFatigueExercise intoleranceDizzinessSyncope
Temporary pacemaker Pacemaker How to check pulse rateHow to
perform CPR if
pacemaker dependentProcedural teaching for
pacemaker implantPacemaker education,
emphasize no contactsports
Call 911 in the event ofsyncope or arrest
359PEDIATRIC ARRHYTHMIAS
-
7/31/2019 Arrutmias en Pediatria
10/12
B/La autoantibodies in the mother (present in col-
lagen vascular diseases such as lupus erythemato-
sis) and the development of congenital AV block
in the child (Waltuck & Buyon, 1994). Surgical
AV block occurs as a complication in congenital
heart surgery because of injury to the AV node or
His bundle. Certain procedures, such as closure of
an AV septal defect or ventricular septal defect,
tetralogy of Fallot repair, subaortic resection oraortic valve
replacement, carry a higher risk for
surgical AV block. In the current era of congenital
heart surgery, the incidence of permanent AV
block is 3% or less for these procedures (Friedman,
1998). Inflammation, as seen with myocarditis,
rheumatic fever, or Lyme disease, is another cause
for acquired AV block.
Symptoms seen in children with AV block de-
pend on the ventricular rate. Children with first-
degree or second-degree Mobitz I AV block are
generally asymptomatic. However, the fetus with
complete AV block may present with hydrops and
necessitate early delivery and intervention. CHFmay be seen in
infants with slow ventricular rates,
especially in the presence of associated congenital
heart defects. Older children may complain of fa-
tigue, exercise intolerance, dizziness, or, in some
cases, syncope. Sudden death has been reported. A
chest radiograph may reveal cardiomegaly in pa-
tients with long-standing AV block due to the
chronically slow hearts attempt to compensate by
augmenting the stroke volume.
Pacemaker therapy is clearly indicated for
symptomatic children with second-degree Mobitz
II and third-degree complete AV block. In postop-
erative patients, the AV block may be transient, so
temporary pacing is employed for the first 10 to 14
days. If the AV block persists beyond this period,
permanent pacing is warranted. Much controversy
exists over the proper time to intervene with pacing
in the asymptomatic child with congenital AV
block (Friedman, 1995). With advances in devicetechnology and
pacing lead design, implanting
pacemakers in young infants and children has be-
come much safer and more practical.
NURSING RESPONSIBILITIES
The bedside nurse is in a crucial position to
identify rhythm disturbances in pediatric patients.
Quick determination of the childs hemodynamic
status at the onset of an abnormal rhythm with
ongoing assessments throughout the course of the
arrhythmia is key to guiding therapy. Monitoring
the ECG and obtaining clear rhythm strips to doc-
ument both normal and abnormal rhythms contrib-ute to making an
accurate arrhythmia diagnosis.
When antiarrhythmic drugs are used, the nurse
must be aware of possible adverse effects, includ-
ing the potential for proarrhythmia. An awareness
and understanding of newer treatment modalities,
including RF ablation techniques and device ther-
apy, has important implications for patient care as
well (Tables 6 and 7).
Patient education is a vital component of the
nurses role in caring for these children and their
Table 7. Internet Resources
Organization Website Comments
American Heart Association (AHA) www.americanheart.org
Professional and lay information on manycardiac conditions,
including arrhythmias
North American Society of Pacingand Electrophysiology
(NASPE)
www.NASPE.org Professional and lay information on arrhythmias,RF
ablation, medications, and device therapy
The Heart of PediatricElectrophysiology (HOPE)
www.rhythmsofhope.org Organization was formed in 1999 to
provideeducation and support to families and
healthprofessionals.
Website not yet available.Toll-free phone number:
877-394-HOPE
SADS Foundation (SuddenArrhythmic Death Syndrome)
www.sads.org Nonprofit organization provides information onLong
QT Syndrome, including acomprehensive listing of medications
thatcause QT prolongation
Cardiac Arrhythmia Research andEducation Foundation, Inc.
(CARE)
www.longqt.com Nonprofit organization provides information
onLong QT Syndrome
The Childrens Health InformationNetwork
www.tchin.org Internet resource for professionals and
familiesproviding information on various aspects ofcongenital heart
disease, includingarrhythmias
Physicians Desk Reference PDR.net Professional and lay
information on medications,including antiarrhythmic drugs
360 DEBRA HANISCH
-
7/31/2019 Arrutmias en Pediatria
11/12
families. Parents and patients need to learn how to
check a pulse rate, how to recognize signs and
symptoms associated with arrhythmias and side
effects of prescribed antiarrhythmic agents, what
to do if signs or symptoms occur, what types of
activity should be restricted, and, in some cases,
how to perform cardiopulmonary resuscitation
(CPR). Patients at risk for syncope or cardiac arrest
should be encouraged to obtain a MedicAlert
bracelet (MedicAlert, Turlock, CA). Psychosocial
issues need to be addressed as well. Parents and
patients may be afraid of a cardiac arrest, espe-
cially if there is pacemaker-dependency or a family
history of sudden cardiac death. Children and ad-
olescents with implanted pacemakers or defibrilla-
tors often express concerns related to repeated sur-
gical procedures and the resultant scars and
visibility of the implanted device. These patients
frequently express a need to be accepted by their
peers and be treated normally (Zeigler & Corbett,
1995). In some cases, referral to professional coun-
seling may be beneficial. Effective and safe man-
agement of young patients with arrhythmias is
contingent upon a comprehensive team approach
that includes not only the health care professionals,
but also the caretakers of these special children.
REFERENCESAckerman, M.J. (1998). The long QT syndrome: Ion
channel
diseases of the heart. Mayo Clinic Proceedings, 73(3),
250-269.Compton, S.J., Lux, R.L., Ramsey, M.R., Strelich, K.R.,
Sanguinetti, M.C., Green, L.S., Keating, M.T., & Mason,
J.W.
(1996). Genetically defined therapy of inherited long-QT
syn-drome: Correction of abnormal repolarization by potassium.
Circulation, 94(5), 1018-1022.Deal, B.J. (1998).
Supraventricular tachycardia mechanisms
and natural history. In B.J. Deal, G.S. Wolff, & H.
Gelband(Eds.), Current Concepts in Diagnosis and Management of
Arrhythmias in Infants and Children (pp. 117-143). Armonk,NY:
Futura Publishing.
Dick, M.I., & Russell, M.W. (1998). Ventricular
tachycardia.
In B.J. Deal, G.S. Wolff, & H. Gelband (Eds.), Current
Con-cepts in Diagnosis and Management of Arrhythmias in Infantsand
Children (pp. 181-222). Armonk, NY: Futura Publishing.
Friedman, R.A. (1995). Congenital AV block: Pace me now
or pace me later? Circulation, 92(3), 283-285.Friedman, R.A.
(1998). Sinus and atrioventricular conduction
disorders. In B.J. Deal, G.S. Wolff, & H. Gelband
(Eds.),
Current Concepts in Diagnosis and Management of Arrhyth-mias in
Infants and Children (pp. 89-116). Armonk, NY:
FuturaPublishing.
Garson, A.J., Dick, M.I., Fournier, A., Gillette, P.C.,
Ham-ilton, R., Kugler, J.D., Van Hare, G.F.I., Vetter, V., &
Vick,
G.W.I. (1993). The long QT syndrome in children: An interna-
tional study of 287 patients. Circulation, 87(6),
1866-1872.Gregoratos, G., Cheitlin, M., Conill, A., Epstein, A.,
Fellows,
C., Ferguson, T.J., Freedman, R., Hlatky, M., Naccarelli,
G.,Saksena, S., Schlant, R., & Silka, M. (1998). ACC/AHA
Guide-
lines for implantation of cardiac pacemakers and
antiarrhythmiadevices: A report of the American College of
Cardiology/
American Heart Association task force on practice
guidelines(committee on pacemaker implantation). Journal of the
Amer-ican College of Cardiology, 31, 1175-1209.
Hanisch, D.G., & Perron, L. (1992). Complex dysrhythmias
in infants and children. AACN Clinical Issues in Critical
CareNursing, 3(1), 255-269.
Hazinski, M.F., Cummins, R.O., & Field, J.M. (Eds.).
(2000).
2000 Handbook of Emergency Cardiovascular Care for Health-care
Providers. Dallas: American Heart Association.
Ko, J.K., Deal, B.J., Strasburger, J.F., & Benson,
D.W.J.(1992). Supraventricular tachycardia mechanisms and their
age
distribution in pediatric patients. American Journal of
Cardiol-ogy, 69(12), 1028-1032.
Kugler, J.D. (1990). Sinus node dysfunction. In P. Gillette
&A.J. Garson (Eds.), Pediatric Arrhythmias:
Electrophysiologyand Pacing (pp. 250-300). Philadelphia: WB
Saunders.
Kugler, J.D., Danford, D.A., Deal, B.J., Gillette, P.C.,
Perry,
J.C., Silka, M.J., Van Hare, G.F., & Walsh, E.P. (1994).
Ra-
diofrequency catheter ablation for tachyarrhythmias in
children
and adolescents. The New England Journal of Medicine,330(21),
1481-1487.
Kugler, J.D., Danford, D.A., Houston, K., & Felix, G.
(1997).
Radiofrequency catheter ablation for paroxysmal
supraventric-
ular tachycardia in children and adolescents without
structuralheart disease. American Journal of Cardiology, 80(11),
1438-1443.
Liebman, J. (1982). Tables of normal standards. In J. Lieb-
man, R. Plonsey, & P.C. Gillette (Eds.), Pediatric
Electrocar-diography (pp. 82-133). Baltimore: Williams &
Wilkins.
Locati, E.H., Zareba, W., Moss, A.J., Schwartz, P.J.,
Vincent,
G.M., Lehmann, M.H., Towbin, J.A., Priori, S.G., Napolitano,
C., Robinson, J.L., Andrews, M., Timothy, K., & Hall,
W.J.
(1998). Age- and sex-related differences in clinical
manifesta-
tions in patients with congenital long-QT syndrome: Findings
from the international LQTS registry. Circulation,
97(22),2237-2244.
Ludomirsky, A., & Garson, A. (1990). Supraventricular
tachycardia. In P.C. Gillette & A.J. Garson (Eds.),
PediatricArrhythmias: Electrophysiology and Pacing (pp.
380-426).
Philadelphia: W.B. Saunders Company.Marks, M.L., Trippel, D.L.,
& Keating, M.T. (1995). Long
QT syndrome associated with syndactyly identified in
females.
American Journal of Cardiology, 76(10), 744-745.Martin, A.B.,
& Kugler, J.D. (1999). Sinus node dysfunction.
In P.C. Gillette & A.J. Garson (Eds.), Clinical Pediatric
Ar-rhythmias (2nd ed., pp. 51-62). Philadelphia: W.B.
SaundersCompany.
Panagiotopoulos, C., McCrindle, B.W., Hick, K., & Katz-
man, D.K. (2000). Electrocardiographic findings in
adolescents
with eating disorders. Pediatrics, 105(5), 1100-1105.Perry,
J.C., & Garson, A.J. (1990). Supraventricular tachy-
cardia due to Wolff-Parkinson-White syndrome in children:
early disappearance and late recurrence. Journal of the
Ameri-can of College Cardiology, 16(5), 1215-1220.
Ross, B.A., & Gillette, P.C. (1999). Atrioventricular
block
and bundle branch block. In P.C. Gillette & A.J. Garson
(Eds.),Clinical Pediatric Arrhythmias (2nd ed., pp. 63-77).
Philadel-phia: W.B. Saunders Company.
Schwartz, P.J., Priori, S.G., Locati, E.H., Napolitano, C.,
Cantu, F., Towbin, J.A., Keating, M.T., Hammoude, H., Brown,
A.M., Chen, L.-S.K., & Colatsky, T.J. (1995). Long QT
syn-
drome patient with mutations of the SCN5A and HERG gene
have differential responses to Na channel blockade and to
increases in heart rate: Implications for gene-specific
therapy.
Circulation, 92(12), 3381-3386.Silka, M.J., & Garson, A.J.
(1999). Ventricular arrhythmias.
In P.C. Gillette & A.J. Garson (Eds.), Clinical Pediatric
Ar-rhythmias (2nd ed., pp. 121-145). Philadelphia: W.B.
SaundersCompany.
361PEDIATRIC ARRHYTHMIAS
-
7/31/2019 Arrutmias en Pediatria
12/12
Sokoloski, M.C. (1999). Tachyarrhythmias confined to theatrium.
In P.C. Gillette & A.J. Garson (Eds.), Clinical Pediatric
Arrhythmias (2nd ed., pp. 78-96). Philadelphia: W.B.
SaundersCompany.
Van Hare, G. (1999). Supraventricular tachycardia. In
P.C.Gillette & A.J. Garson (Eds.), Clinical Pediatric
Arrhythmias(2nd ed., pp. 97-120). Philadelphia: W.B. Saunders
Company.
Waltuck, J., & Buyon, J. (1994).
Autoantibody-associatedcongenital heart block: Outcome in mothers
and children. An-nals of Internal Medicine, 120(7), 544-551.
Zeigler, V.L., & Corbett, K.S. (1995). Psychosocial
aspectsof caring for pediatric pacemaker recipients and their
families.In P.C. Gillette & V.L. Zeigler (Eds.), Pediatric
Cardiac Pac-ing (pp. 181-203). Armonk, NY: Futura Publishing.
362 DEBRA HANISCH