Embed Size (px)
Citation preview
8/6/2019 Acute Leukemia and Lymphoma R
http://slidepdf.com/reader/full/acute-leukemia-and-lymphoma-r 1/6
Acute Leukemia + Malignant Lymphoma ( 2011 )
1 4th
year – female
Leukemia
Acute Chronic
Myeloid Acute myeloid leukemia Chronic myeloid leukemia
Lymphoid Acute lymphoblastic
leukemia
Chronic lymphoid leukemia
Acute Leukemia
It occurs abruptly ( suddenly )
In normal individuals there are 2 % of primitive cells (blasts) inside their B.M
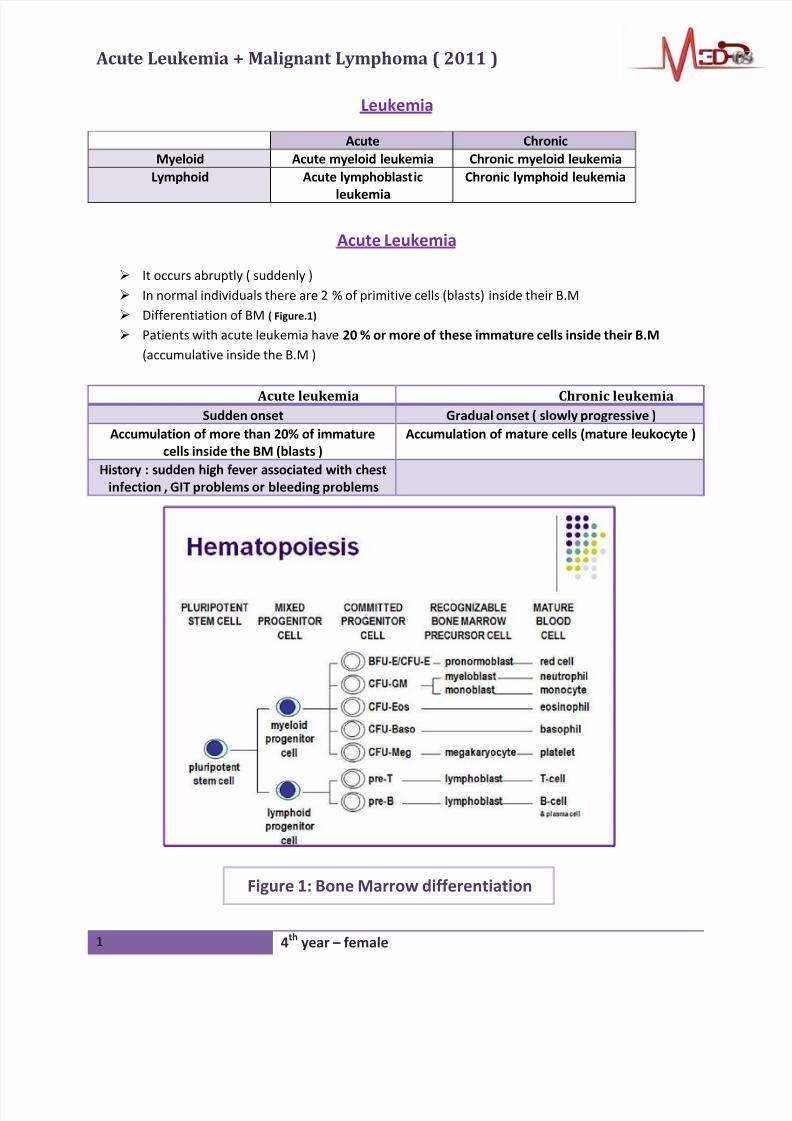
Differentiation of BM ( Figure.1)
Patients with acute leukemia have 20 % or more of these immature cells inside their B.M
(accumulative inside the B.M )
Acute leukemia Chronic leukemiaSudden onset Gradual onset ( slowly progressive )
Accumulation of more than 20% of immature
cells inside the BM (blasts )
Accumulation of mature cells (mature leukocyte )
History : sudden high fever associated with chest
infection , GIT problems or bleeding problems
Figure 1: Bone Marrow differentiation
8/6/2019 Acute Leukemia and Lymphoma R
http://slidepdf.com/reader/full/acute-leukemia-and-lymphoma-r 2/6
Acute Leukemia + Malignant Lymphoma ( 2011 )
2 4th
year – female
• Predisposing Factors:
AL is a multi system hypothesis. Could occur in uterine life or acquired during the life .possible causes
that may contribute in the developing of the disease :
1-
Ionizing radiation ( even the therapeutic doses )
2- Chemicals , e.g. : benzene
3- Viruses .e.g. : EBV , CMV , HIV
4- Exposure to environmental hazards & air pollution
5- Genetic predisposition , e.g.: translocation , mutations
• Incidence :
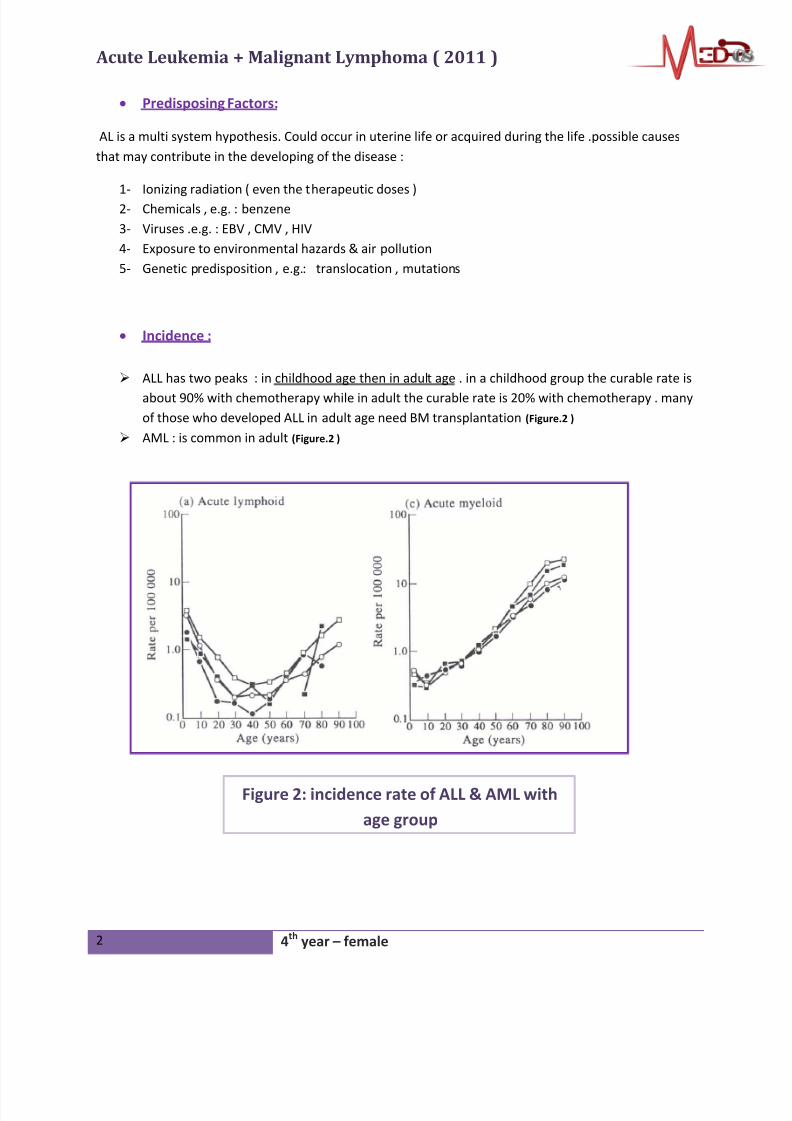
ALL has two peaks : in childhood age then in adult age . in a childhood group the curable rate is
about 90% with chemotherapy while in adult the curable rate is 20% with chemotherapy . many
of those who developed ALL in adult age need BM transplantation (Figure.2 )
AML : is common in adult (Figure.2 )
Figure 2: incidence rate of ALL & AML with
age group
8/6/2019 Acute Leukemia and Lymphoma R
http://slidepdf.com/reader/full/acute-leukemia-and-lymphoma-r 3/6
Acute Leukemia + Malig
3 4th
Classification 1- T-lymphoc
2- B-lymphoc
3- precursors
Cli
General • Bone
a- An
b- Ne
c- Th
Organ infiltration
(MCQs)
Santury sites o
because of its
lymphoblasts c
tend to have C
also infiltrate t
the testis and
Patients usuall
lymphadenop
splenomegaly
testicular mas
Hypervicosity
syndrome
It is more com
cause of hyper
sludge togethe
1- Luckostasis
2- CNS proble
, confusion
3- Kidney (wh
4- Ear : tinnit
A
ant Lymphoma ( 2011 )
year – female
ALL & AML
ALL AM
tes
te
According to the FAB cla
M0 = no differentiation
M1 = >3% MPO; 20% AMM2= inc gran; Auer rods
M3= inc promyelocytes
M4= myelomono
M5= monoblastic
M6= erythroleukemia
M7= megakaryocytic
ical presentations( classical Finding )
arrow failure
emia(normochromic normocytic) : fatigue , pallor ,h
utropenia : recurrent infection ( form his/her own f
omopcytopenia : bruise , purpra , bleeding tenden
f lymphoblsats:
mall sizes ,
an cross the BBB and
S infiltration . it can
e coporacavernosa in
roliferate there.
y present with
thy ,hepato-
CNC complains or
es
M3 (promylocytic)
and patient in most o
with DIC( lymphoblas
tissue factors that ov
coagulation cascade
M4 & M5 (monocytic
tissues . patient may
hyperplasia or subcu
Patients may present wi
manifestations except in
M5 leuckemiaOther Finding
on in AML than ALL because of the large size of ce
iscosity refers to the increase in number of blasts c
r .as a result the following complications may occur
: heart pushes now against high resistance HF
ms : due to inadequate O2 saturation ( blood flow v
, syncopic attack , loss of consciousness
ich has very fine blood supply): hematoriua , acute
s , HL ( may be the 1st
complication )
Figure
of pati
A- gum
B- Chlo
B
L
sification :
L
eadache
lora)
cy
tends to over bleed
f the time presents
ts in M3 release
er activate the
)
) tend to infiltrate
present with gum
taneous nodules
h no specific
case of M3 , M4 or
lls in AML. The actual
ell which are tend to
:
ery slow) delusion
renal shut down
: Clinical presentations
nt with AML
hyperplasia
romas
8/6/2019 Acute Leukemia and Lymphoma R
http://slidepdf.com/reader/full/acute-leukemia-and-lymphoma-r 4/6
Acute Leukemia + Malignant Lymphoma ( 2011 )
4 4th
year – female
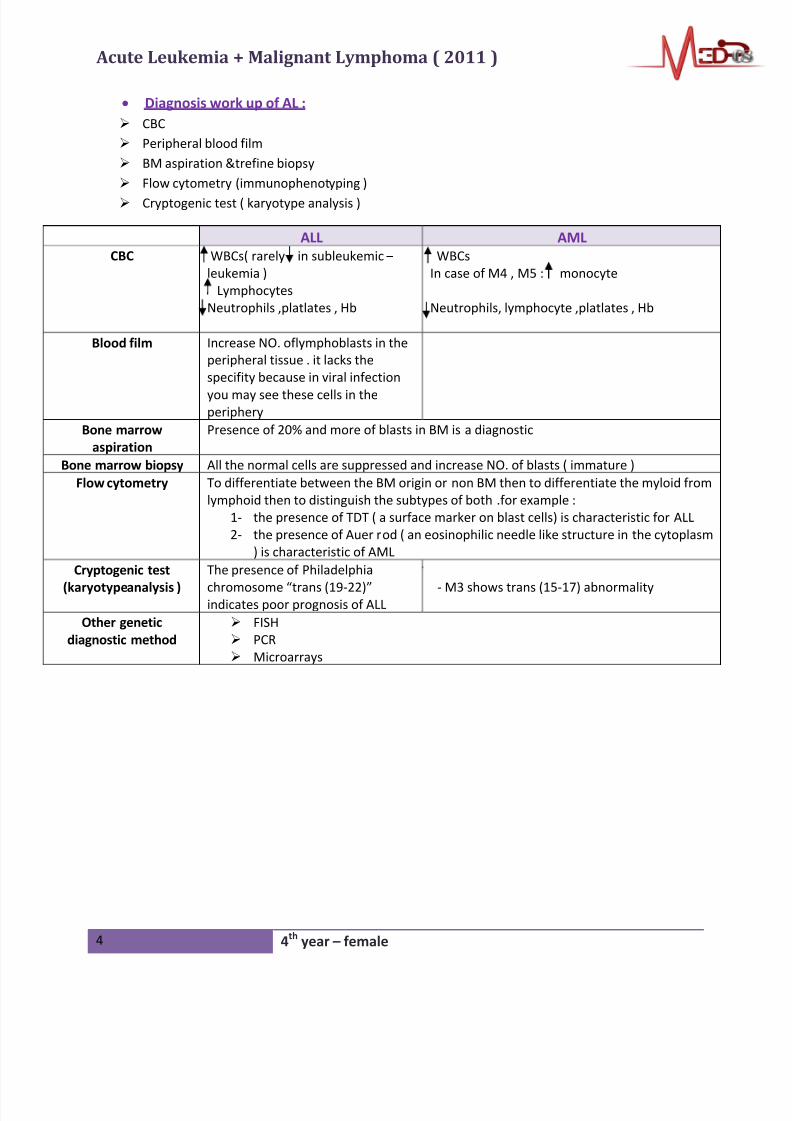
• Diagnosis work up of AL :
CBC
Peripheral blood film
BM aspiration &trefine biopsy
Flow cytometry (immunophenotyping )
Cryptogenic test ( karyotype analysis )
ALL AML
CBC WBCs( rarely in subleukemic –
leukemia )
Lymphocytes
Neutrophils ,platlates , Hb
WBCs
In case of M4 , M5 : monocyte
Neutrophils, lymphocyte ,platlates , Hb
Blood film Increase NO. oflymphoblasts in the
peripheral tissue . it lacks the
specifity because in viral infection
you may see these cells in theperiphery
Bone marrow
aspiration
Presence of 20% and more of blasts in BM is a diagnostic
Bone marrow biopsy All the normal cells are suppressed and increase NO. of blasts ( immature )
Flow cytometry To differentiate between the BM origin or non BM then to differentiate the myloid from
lymphoid then to distinguish the subtypes of both .for example :
1- the presence of TDT ( a surface marker on blast cells) is characteristic for ALL
2- the presence of Auer rod ( an eosinophilic needle like structure in the cytoplasm
) is characteristic of AML
Cryptogenic test
(karyotypeanalysis )
The presence of Philadelphia
chromosome “trans (19-22)”indicates poor prognosis of ALL
- M3 shows trans (15-17) abnormality
Other genetic
diagnostic method
FISH
PCR
Microarrays
8/6/2019 Acute Leukemia and Lymphoma R
http://slidepdf.com/reader/full/acute-leukemia-and-lymphoma-r 5/6
Acute Leukemia + Malignant Lymphoma ( 2011 )
5 4th
year – female
Lymphoma
A-Hodgkin’s lymphoma :
Bimodal age distribution : young & old age
It is a curable disease by chemotherapy
• Predisposing factors :
EBV
HCV
House hold probe : more than one member in a family + environmental causes
HIV : through immunosuppression
• Clinical presentation :
It has to start in L.N L.N enlargement ( superficial – intra-thoracic – intra-abdominal )
intra-abdominal L.N may lead to pressure manifestation : bowel obstruction
The enlargement L.Ns are rubbery in consistency , firm , big in size & non-tender (painless)
B-symptoms : fever , wt loss ( > 10% / 6 months) , night sweats (drenching > 38 ) Itching is one of the symptoms and it is due to presence of basophilia and eosinophilia
• Pathognemonic cells :
Owl eyes “ Reed- sternberng “ cells – muted B-cell
Big nucleus , 2 big inclusions
• Investigation :
1- Hx& Ex
2- L.N BIOPSY ( excesional biopsy ) : the best form cervical
In patients with shortness of breath , take it from the thoracic with CT-guided
DON’T take FNA
3- Cytology
a- Reed- sternberng cells with inflammatory background
b- Types : according to WHO classification :
Nodular sclerosis ( young age & female )
Mixed cellurity( older age)
Lymphocytic depleted
Lymhphocytic –predominant
c- Staging : an arble staging system :
Stage I : 1 L.N gp.
Stage II : 2 L.N gp. above the diaphragm
Stage III : 2 L.N above & below the diaphragm
Stage IV : distant metastasis
Each stage further subdivided into :
A lack of B cells
B present of B cells
X L.N larger than 10 cm

8/6/2019 Acute Leukemia and Lymphoma R
http://slidepdf.com/reader/full/acute-leukemia-and-lymphoma-r 6/6
Acute Leukemia + Malignant Lymphoma ( 2011 )
6 4th
year – female
4- CT scan of the neck – chest – abdomen – pelvic : to stage correctly to give appropriate
treatment
5- BM aspiration &trephinebiopsy : to see BM involvement
• Always remember : Hodgkin’s lymphoma is a disease of primary L.N involvement and it isspread in ordinary fashion ( contiguity )
B- Non-Hodgkin’s lymphoma :
- Hetergenousdisease : can involve extra-lymphatic system from the beginning
- L.N enlargement is haphazard
• Predisposing factors :
- Same as Hodgkin’s lymphoma
- Patients with autoimmune disease ( Celiac disease or UC ) or those who are immune
compromised have more tendency to develop Non-Hodgkin’s lymphoma
• Investigation :
- Take skin biopsy in Mycosis fungoides(sézarýssyndrome )or from the lung (pleural effusion ) or
from L.N
- NHL is difficult to staging
• Specific types :
1- H.pylori : it causes peptic ulcer disease or gastritis but some cases developMALT lymphoma
( mucosa –associtiated –lymphoid tissue lymphoma )
2- EBV related : can lead to Burkitt’s Lymphomapatient presents with jaw lesion
Done by
Scientific Committee – female – 2011