Embed Size (px)
DESCRIPTION
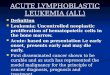
Acute lymphoblastic leukemia/lymphoma (ALL). A group of neoplasms of B or T lymphoblasts Pre-B cell (85%): childhood acute leukemias Pre-T cell: lymphomas in adolescent males, 50~70% with mediastinal (thymic) masses B & T : similar histology, immunophenotype - PowerPoint PPT Presentation
Citation preview

Acute lymphoblastic leukemia/lymphoma (ALL)
• A group of neoplasms of B or T lymphoblasts• Pre-B cell (85%): childhood acute leukemias• Pre-T cell: lymphomas in adolescent males,
50~70% with mediastinal (thymic) masses• B & T : similar histology, immunophenotype• Chromosome anomaly (90%): hyperdiploidy,
pseudodiploid, t(12;21), t(9;22), and t(4;11)

Diagnosis Cell of Origin
Genotype Salient Clinical Features
Precursor B-cell acute lymphoblastic leukemia/lymphoma
Bone marrow precursor B-cell expressing TdT and lacking surface Ig
Diverse chromosomal translocations; t(12;21) involving CBFαand ETV6 most common rearrangement
Predominantly children with symptoms relating to pancytopenia secondary to marrow involvement; aggressive

Precursor T-cell acute lymphoblastic leukemia/lymphoma
Precursor T-cell (often of thymic origin) expressing TdT
Diverse chromosomal translocations, many involving T-cell receptor loci; rearrangements of TAL1 most common
Predominantly adolescent males with thymic masses; variable splenic, hepatic, and bone marrow involvement; aggressive

BM smear: lymphoblasts

Flow cytometry immunophenotype

Clinical features of ALL
• Blasts in BM suppress hematopoiesis by physical crowding: anemia, neutropenia, thrombocytopenia
• Abrupt stormy onset• Bone pain and tenderness• Generalized lymphadenopathy (LAP),
splenomegaly, hepatomegaly• CNS manifestations• Treatment (Tx) & prognosis (Px)

Myeloid Neoplasms• This heterogeneous group of neoplasms is an
origin in a progenitor cell that normally gives rise to terminally differentiated cells of the myeloid series (erythrocytes, granulocytes, monocytes, and platelets).
• Bone marrow (BM) and other MPS• AML: immature myeloid cells in the BM• MDS: ineffective hematopoiesis & cytopenia• MPD: increased production of terminally
differentiated myeloid cells

Acute myelogenous leukemia (AML)
• Primarily in adult: peak age, 15~39 y/o• Pathophysiology: acquired genetic alteration
inhibition of terminal differentiation physical replacement pancytopenia
• Tx: clear the BM leukemic clone (cytotoxic drugs), overcome the block in differentiation
• Classification • Diagnosis: >20% myeloid blasts in BM, variable
number of leukemic cells in PB (aleukemic leukemia)

Revised FAB Classification of AML
ClassIncidence (%
of AML) Marrow Morphology/Comments
M0 Minimallydifferentiated
AML
2-3% Blasts lack definitive cytologic and cytochemical markers of myeloblasts (e.g., myeloperoxidase negative) but express myeloid lineage antigens and resemble myeloblasts ultrastructurally.
M1 AML without Differentiation
20% Very immature, but =3% of blasts are peroxidase positive; few granules or Auer rods and little maturation beyond the myeloblast stage.
M2 AML with maturation
30-40% Full range of myeloid maturation through granulocytes; Auer rods present in most cases; often associated with the t(8;21).

M3 Acute promyelocytic leukemia
5-10% Most cells are hypergranular promyelocytes, often with many Auer rods per cell; patients are younger (median age 35 to 40 years); high incidence of DIC; strong association with the t(15;17).
M4 Acute myelomonocytic leukemia
15-20% Myelocytic and monocytic differentiation evident; myeloid elements show range of maturation; monoblasts are positive for nonspecific esterases; subset associated with the inv(16).

M5 Acute monocytic leukemia
10% In M5a subtype, monoblasts (peroxidase-negative, nonspecific esterase-positive) and promonocytes predominate in marrow and blood;
In M5b subtype, mature monocytes predominate in the peripheral blood; M5a and M5b occur in older patients; characterized by high incidence of organomegaly, lymphadenopathy, and tissue infiltration.

M6 Acuteerythroleukemia
5% Dysplastic erythroid precursors (some megaloblastoid, others with giant or multiple nuclei) predominate, and within the non-erythroid cells, >30% are myeloblasts; seen in advanced age; makes up 1% of de novo AML and 20% of therapy-related AML.
M7 Acutemegakaryocytic leukemia
1% Blasts of megakaryocytic lineage predominate; blasts react with platelet-specific antibodies directed against GPIIb/IIIa or vWF; myelofibrosis or increased marrow reticulin seen in most cases.

Proposed WHO Classification of AML
Class Prognosis
I. AML with Recurrent Chromosomal Rearrangements
AML with t(8;21)(q22;q22); CBFα/ETO fusion gene
Favorable
AML with inv(16)(p13;q22); CBFβ/MYH11 fusion gene
Favorable
AML with t(15;17)(q22;11-12); RARα/PML fusion gene
Intermediate
AML with t(11q23;v); diverse MML fusion genes
Poor

II. AML with Multilineage Dysplasia
With prior myelodysplastic syndrome Very poor
Without prior myelodysplastic syndrome Poor
III. AML, Therapy Related
Alkylating agent related Very poor
Epipodophyllotoxin related Very poor
IV. AML, not Otherwise Specified
Sub-classes defined by extent of differentiation and FAB classification (e.g., M0-M7)
Intermediate

BM smear: myeloblasts (M1)

Flow cytometry immunophenotype

Acute promyelocytic leukemia (M3)

Acute monocytic leukemia (M5b)

Chromosomal Abnormalities of AML
• 90% AML, with prognostic implication• Ch 5 or 7 deletion: AML after MDS of CT/RT• AML M3 (APL): t(15;17) RAR-α/PML fused g
ene hybrid mRNA abnormal retinoic acid receptor block myeloid cell differentiation => all-trans-retinoic acid causing neoplastic promyelocytes neutrophils (differentiation therapy), but all patients ultimately relapse

Clinical Features of AML
• Weeks or a few months of the onset of symptoms with findings related to pancytopenia, similar to that of ALL
• APL: DIC (disseminated intravascular coagulation)
• M4 &M5: infiltration of the skin (leukemia cutis) and the gingiva
• localized mass composed of myeloblasts: granulocytic sarcoma (myeloblastoma, chloroma)

Myelodysplastic Syndrome (MDS)• A group of clonal stem cell disorders
characterized by maturation defects resulting in ineffective hematopoiesis and an increased risk of transformation to AML
• BM replaced by the clonal progeny of a mutant multipotent stem cell that retains the capacity to differentiate into RBC, WBC, PLT, but in an ineffective and disordered manner
• BM: hyper-/normo-cellular, PB: pancytopenia• Idiopathic (primary) or therapy-related (t-MDS)

MDS• Pathogenesis: unknown (? Stem cell damage)• monosomy 5/7, 5q/7q deletions, trisomy 8, 20q
deletion• MF: dysplastic differentiation & <30% blasts
–BM: ring sideroblasts, megaloblastoid maturation, nuclear budding; pseudo-Pelger-Huet cells, hypo- or hyper-lobated nucleated megakaryocytes– PB: pseudo-Pelger-Huet cells, giant PLT, macrocyte, poikilocyte, monocytosis

BM smear: myelodysplasia

Clinical Course of MDS• Adult >60 y/o• S/S: pancytopenia, asymptomatic (half)• multiple chromosomal abnormalities and severity
of cytopenia• median survival: 9~29 months (may >5 yrs)• 10~40%: AML transformation• t-MDS: 4~8 months, more grim prognosis• Tx: allogeneic BMT for younger patients;
supportive treatment for the older

Chronic Myeloproliferative Disorders (MPD)
• A group of disorders of multipotent progenitor cell capable of terminal differentiation => hypercellular BM and increased hematopoiesis & PB counts, extramedullary hematopoiesis & splenomegaly, later in spent phase (may progress to AML, especially in CML)
• CML, PCV (PV), ET, IM• non-specific pathologic findings, overlap with one
another and some reactive hyperplasia• Dx: clinical+morphologic+cytogenetic

Chronic Myelogenous Leukemia• Age: 25~60 y/o (peak 30+~40+y/o)• Genetics: Philadelphia chromosome (Ph1)>90%• MF: hypercellular BM with sea-blue histiocytes;
leukocytosis, eosinophilia, and basophilia in PB; neoplastic extramedullary hematopoiesis (splenomegaly)
• S/S: anemia, hypermetabolism, LUQ distension or pain, lack of leukocyte alkaline phosphatase
• Course: slow progression (median survival 3 yrs); accelerated phase (50%) 6-12 m blast crisis 70% AML, 30% ALL (most early B lineage)
• Tx: low-dose CT, allogeneic BMT (75% cure)

Fluorescence in situ hybridization (FISH)

FISH

FISH

PB smear: chronic myeloid leukemia

Spleen in CML

PCV: polycythemia vera• A multipotent myeloid stem cell neoplasm• absolute increase in red cell mass (Hb, Hct…)• serum erythropoietin: virtually undetectable• BM: hyperplasia fibrosis (spent phase)• Age: 60 y/o; S/S: increased red cell mass
hematocrit total blood volume vascular stasis (hypertensive, cyanotic, pruritus, gout…)
• risk of bleeding and thrombotic episodes• Px: 10 yrs, spent phase (M with MM), 2~15% to
AML; Tx: phlebotomy

Spleen in PCV

ET: essential thrombocytosis
• The least common form of MPD• Megakaryocytic hyperplasia: PLT>600K• Dx: by exclusion of other MPDs or reactive• BM: mild to moderate hyperplasia with marked
megakaryocytic hyperplasia• PB: giant PLT, mild leukocytosis• S/S: thrombosis and hemorrhage• Px: indolent disorder, long asymptomatic periods,
median survival: 12~15 yrs

PB smear: ET

IM: myelofibrosis with myeloid metaplasia (MMM)
• Hallmark: early marrow fibrosis (myelofibrosis)• neoplastic megakaryocytes release PDGF & TGF-
fibrosis hematopoietic stem cells seed the spleen, liver, LNs EMH (MM)
• BM: early hypercellularity, megakaryocytic hyperplasia and dysplasia, minimal fibrosis hypocellularity, diffuse fibrosis or osteosclerosis
• Spleen: huge, EMH with large, clustered megaK• PB: leukoerythroblastosis, dacryocytes

PB smear: normoblast & dacryocytes

Clinical Course of MMM
• Age: 60 y/o or more• S/S: progressive anemia or huge spleen,
hyperuricemia and secondary gout• Lab: moderate to severe anemia (normochromic
and normocytic) with leukoerythroblastosis, WBC (variable) & PLT (N or elevated, then decreased)
• median survival: 1~5yrs, complication: infection, thrombosis, bleeding, 5~20% to AML

Langerhans cell histiocytosis (Histiocytosis X)
• Clonal proliferation of the antigen-presenting dendritic cells (normal in the skin and others)
• Three categories:- Letterer-Siwe disease: acute disseminated- Hand-Schuller-Christian disease: calvarial defects, diabetes insipidus, and exophthalmos- Eosinophilic granuloma
• EM: HX bodies (Birbeck granules)


Spleen

Splenic infarcts

Thymoma, benign

Thymoma, invasive