Embed Size (px)
Citation preview

Stephen Larsen
24th February, 2010
Lymphomas - classification and diagnosis

Two important references

http://apps.who.int/bookorders/anglais/detart1.jsp?sesslan=1&codlan=1&codcol=70&codcch=4002#$US122
http://www.amazon.com/Classification-Tumours-Haematopoietic-Lymphoid-Tissue/dp/9283224310$US104

Background

Thomas Hodgkin(1798-1866)
Thomas Hodgkin published in 1832 the first description of lymphoma, specifically of the form named after him, Hodgkin's lymphoma.
Name Hodgkin's Disease proposed in 1865 by Wiks.

History of Lymphoma Classification
Since Thomas Hodgkin’s first description of lymphoma in 1832, many other forms of lymphoma have been described, grouped under several proposed classifications.
1956, 1966 Rappaport’s Classification of NHL1966 Lukes-Butler (American) modern
classification of HL Kiel classification: in 1974, Karl Lennert
proposed a new system of classifying lymphomas based on cellular morphology and their relationship to cells of the normal peripheral lymphoid system.

The very popular 1982 Working formulation classification introduced the category Non-Hodgkin Lymphoma (NHL), itself divided into 16 different diseases.
REAL classification: In 1994 the Revised European-American Lymphoma (REAL) Classification attempted to apply immunophenotypic and genetic features in identifying distinct clinico-pathologic NHL entities.
The latest classification by the WHO (2001 updated in 2008) lists 43 different forms of lymphoma divided in four broad groups.

BLOOD, 1 DECEMBER 2008 VOLUME 112, NUMBER 12 p4384Classification of lymphoid neoplasms: the microscope as a tool for disease discovery

A practical way to think of lymphomaCategory Survival
of untreate
d patients
Curability
To treat or not to
treat
Non-Hodgkin lymphoma
Indolent Years Generally not curable
Generally defer Rx if asymptomatic
Aggressive
Months Curable in some
Treat
Very aggressive
Weeks Curable in some
Treat
Hodgkin lymphoma
All types Variable – months to years
Curable in most
Treat

Need for classification of Lymphomas
Classification is a language of medicine: diseases must be described, defined and named before they can be diagnosed, treated and studied.
A consensus on definitions and terminology is essential for both clinical practice and investigation.
A classification should contain diseases that are clearly defined, clinically distinctive, non-overlapping and that together comprise all known entities.

WHO classification of tumours of the haematopoietic and lymphoid tissues 4th edition, 2008 – true worldwide consensus classification of haematological malignancies:
WHO classification is based on the principles initially defined in REAL classification by the ILSG.
Guiding principle of the REAL and WHO classification is the attempt to define “real diseases” that can be recognised by available techniques and that appear to be distinct clinical entities.

Three important components to the process of developing classification of Hematological Malignancies:
First, recognising that the underlying causes of the neoplasm are often unknown and may vary. So, we use morphology, immunophenotype, genetic features, and clinical features to define diseases.
Second principle is that classification relies on building a consensus among as many experts as possible on the definition and nomenclature of the disease.
Third, while pathologists must take primary responsibility for developing a primary classification, involvement of clinicians is essential to ensure its usefulness and acceptance in daily practice.

There is no one “gold standard” by which all diseases are defined in the WHO classification.
So: 1. Morphology is always important. 2. Immuno-phenotype and 3. Genetic features are an important part of the definition of
haematologic tumors. Some diseases have a characteristic immunophenotype. Similarly in some lymphoid a specific genetic abnormality is the
key defining criteria, while others lack specific known genetic abnormality.
Some genetic abnormalities serve as prognostic factors.Most of the diseases in WHO classification are considered to be
distinct entities. However, some are not clearly defined and these are listed as provisional entities.

Conceptualizing lymphoma and its Classification
neoplasms of lymphoid origin, typically causing lymphadenopathy
leukemia vs lymphoma (extent of BM involvement)lymphomas as clonal expansions of cells at certain
developmental stages

Clinically useful classification
Diseases that have distinct• clinical features• natural history• prognosis• treatment
Biologically rational
classificationDiseases that have distinct• morphology• immunophenotype• genetic features• clinical features

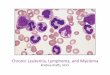
stemcell
lymphoidprogenitor
progenitor-B
pre-B
immatureB-cell
memoryB-cell
plasma cellplasma cell
DLBCL,FL, HL
ALL
CLL
MM
germinalgerminalcentercenterB-cellB-cell
maturenaiveB-cell

Diagrammatic representation of B-cell differentiation and relationship to major B-cell neoplasms.

Diagrammatic representation of T-cell differentiation and function.

Main Groups in WHO Classification of Lymphoid Malignancies
B Cell NeoplasmsPrecursor B Neoplasms Mature B Cell Neoplasms
T Cell and NK Cell NeoplasmsPrecursor T Cell NeoplasmsMature T Cell and NK Neoplasms
Hodgkins Lymphoma




DiagnosisRadiographic features
• Ultrasound• Chest-x-ray film: the mediastinal
lymphonodes• Computerized tomography(CT)
• Chest• Abdomen, • Pelvis
• Gallium-67 scintigraphy• Whole-body positron emission
tomography(PET)

DiagnosisBiopsy----Pathological DiagnosisHistopathological classificationImmunomarkers
eg: NHL, diffused large cell, B cellCytogenetic studies
E.g; Mantle Cell LymphomaMolecular Studies

Diagnosis depends on biopsy of lymph nodes or other involved organs
Need enough tissue to assess cells and architectureopen bx vs core needle bx vs FNA A fine needle biopsy is rarely sufficient!
Peripheral blood: Blood involvement. Usually no changes in WBC and Platelet count
BM: non-specific changesHD: R-S cell in smear and biopsyNHL: increased lymphocyte

Laboratory FindingsFlow cytometry. Immunophenotyping of
biopsy material is important in NHL.Establish clonalityPattern of surface protein expression can be
diagnosticImmunological tests:
NHL: M-protein(+) Coombs’ test(+) hypoglobulinemiaOther findings:
ESR ↑LDH ↑

Disorder Common Phenotype Comments/Variations Potentially Associated Genetic Abnormalities
Chronic lymphocytic leukemia/small cell lymphocytic lymphoma
DR, CD19, CD20, CD5, CD22(-), CD23, CD10(-), CD11c+/-, CD25+/-, CD43, clonal SIgM and SIgD weak CD20 dim
Abnormalities of 13q, 14q, 11q
BCL-2 overexpressed Bright SIg, CD20, FMC7
Mantle cell lymphoma
DR, CD19, CD20, CD5, CD22, CD23(-), CD10(-), CD43, moderate clonal SIg (IgM > IgD) Cyclin D1 overexpressed t(11; 14)
Follicular lymphoma
DR, CD19, CD20, CD5(-), CD22, CD23+/-, CD10, CD11c(-), CD43(-), very bright clonal SIg CD10 negative <20% t(14; 18)
Overexpression of BCL-2
Marginal zone and associated lymphomas
DR, CD19, CD20, CD5(-), CD22, CD23(-), CD10(-), CD11c, CD25(-), CD103(-), moderate clonal SIg SIgD rare Trisomy 3
Hairy cell leukemia
DR, CD19, CD20, CD5(-), CD22, CD23(-), CD10(-), CD11c, CD25, CD103, moderate clonal SIg
SIgD common, very bright CD22 and CD11c No consistent alteration
Plasma cell dyscrasias
DR(-), CD19(-), CD20(-), CD22(-), CD38, CD45, clonal cIg, clonal SIg-/+
Two color bright CD38 and dim CD45 sensitive marker No consistent alteration

Laboratory FindingsChromosome changes in NHL:
t(14;18): Follicular lymphoma t(8;14): Burkitt’s lymphoma t(11;14): Mantle-cell lymphoma t(2;5): Ki-1+(CD30 +) Anaplastic
large-cell lymphoma 3q27: Diffuse large B-cell
lymphoma

Laboratory Findings
Molecular Biology changes in NHL• bcl-2• TCR• IgH

Differential Diagnosis Lymph nodes enlargement Specific: TB Infection
Non-specific: bacteria, virus,
Maligancies: haematological (leukaemia,etc); solid tumor metastasis
Connective tissue diseases Kikuchi’s lymphadenitis in women with SLE
Sarcoidosis
Reactive!

Differential DiagnosisFever
Infection ( bacteria , virus, TB, etc )
Connective tissue disease
Malignant tumors
Malignancies in related organs
Gastrointestinal tumors, liver cancer, etc

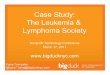
30%
22%8%7%
6%
6%
6%2%
14% Large B-cell
Follicular
Marginal zone
PTCL
Mantle cell
SLL/CLL
Mediastinal
Anaplastic L cell
Hodgkin’s
2002 SEER database. O’Connor

Three most common lymphomas
Follicular lymphomaDiffuse large B-cell lymphoma
Hodgkin lymphoma

Follicular lymphomamost common type of “indolent”
lymphomausually widespread at presentationoften asymptomaticnot curable (some exceptions)associated with BCL-2 gene
rearrangement [t(14;18)]cell of origin: germinal center B-cell

Follicular Lymphoma


defer treatment if asymptomatic (“watch-and-wait”)
several chemotherapy options if symptomatic
median survival: yearsdespite “indolent” label, morbidity and
mortality can be considerabletransformation to aggressive lymphoma can
occur

Diffuse large B-cell lymphoma
most common type of “aggressive” lymphoma
usually symptomaticextranodal involvement is commoncell of origin: germinal center B-cell or
activated B-like lymphomatreatment should be offeredcurable in ~ 40%

Diffuse Large B Cell Lymphoma


Hodgkin lymphoma
Classical Hodgkin lymphomas: Nodular sclerosisMixed cellularityLymphocyte-richLymphocyte depleted or not depleted
Nodular lymphocyte-predominant Hodgkin lymphoma

Hodgkin lymphomacell of origin: germinal centre B-cell Reed-Sternberg cells (or RS variants) in
the affected tissuesmost cells in affected lymph node are
polyclonal reactive lymphoid cells, not neoplastic cells

Reed-Sternberg cell

popcorn celllacunar cellclassic RS cell
(mixed cellularity) (nodular sclerosis) (lymphocytepredominance)

germinalcentreB cell
transformingevent(s)
loss of apoptosis
RS cellinflammatory
response
EBV?
cytokines

ConclusionThere are a large number of types of lymphoma.Therefore classification is important: a consensus on
definitions and terminology is essential for both clinical practice and clinical studies.
Classification has evolved as well learn more about the biology of distinct disorders.
Diagnosis requires an adequate biopsy. There are differing roles of flow cytometry, cytogenetics and moelcular studies for different disorders.