Upload
sebastianpaez8
View
27
Download
0
Embed Size (px)
Citation preview
Leukemia andLymphomaR. Paul Guillerman, MDa,*, Stephan D. Voss, MD, PhDb,Bruce R. Parker, MDa
into future applications of imaging in the man-agement of pediatric leukemia and lymphomapatients.
for 80% to 85% of childhood ALL. About 12% ofALL is T-cell lineage, which is associated with olderage, male gender, leukocytosis, and a mediastinal
annin Street, Suite 470, Houston, TX
b Department of Radiology, Childrens Hospital Boston, Harvard Medical School, 300 Longwood Avenue,
KEYWORDS
Lymphoma Leukemia Hodgkin lymphomaleu
iologic.thec
linics
.comRadiol Clin N Am 49 (2011) 767797Boston, MA 02115, USA* Corresponding author.E-mail address: [email protected] Department of Pediatric Radiology, Texas Childrens Hospital, 6701 F77030, USAsearch into cancer cooperative group studyprotocols are also discussed to provide insights
ALL is subtypedby theWorldHealthOrganization(WHO)by immunophenotypeasB-lymphoblastic orT-lymphoblastic.4 Precursor B-cell ALL accountsLeukemiaand lymphomaare themostcommonandthirdmost commonpediatricmalignancies, respec-tively, and together account for nearly half of allcases of childhood cancer. Although childhoodleukemia and lymphoma share similar cell lineageorigins and both are treated with risk-stratifiedprotocols entailing cytotoxic chemotherapy, theclinical manifestations and imaging indications forthese malignancies vary substantially, with someoverlap.Advances in imaginghaveplayedaparticu-larly important role in improving the assessment oflymphoma at the time of diagnosis, during treat-ment, and following therapy. Imaging has alsohelped guide the design of clinical trials evaluatingnovel treatment strategies.Along with providing relevant details on current
classification, epidemiology, and treatment, thisarticle reviews the current roles of imaging in themanagement of pediatric patients with leukemiaand lymphoma, with attention to diagnosis, stag-ing, risk stratification, therapy response assess-ment, and surveillance for disease relapse andadverse effects of therapy. Advances in functionalimaging and integration of clinical imaging re-
Non-Hodgkin lymphoma Acute lymphoblastic Acute myeloid leukemiadoi:10.1016/j.rcl.2011.05.0040033-8389/11/$ see front matter 2011 Elsevier Inc. AllLEUKEMIAClassification and Epidemiology
Leukemia is the most common childhood malig-nancy, accounting for one-quarter to one-third ofchildhood malignancy cases. Nearly all childhoodleukemia cases are the acute form. Acuteleukemia is classified by the morphology, immuno-phenotype, and cytogenetics of the leukemic cellsinto acute lymphoblastic leukemia (ALL) and acutemyeloid leukemia (AML). ALL and AML accountfor three-quarters and one-fifth of childhood leu-kemia cases, respectively. Chronic myelogenousleukemia (CML) accounts for less than 5% ofcases of childhood leukemia, whereas juvenilemyelomonocytic leukemia (JMML), a myelodys-plastic-myeloproliferative syndrome, accounts forless than 1% of cases of childhood leukemia.1
There is a sharp peak in ALL incidences amongchildren 2 to 3 years of age, with evidence thatALL initiates in utero2 AML rates are highest inthe first 2 years of life, decline to a nadir at 6 yearsof age, and slowly increase during the adolescentyears.3
kemiarights reserved. rad
dren with leukemia so that those children who
diffuse demineralization. Lytic bone lesions are
Guillerman et al768have a good outcome with modest therapy canbe spared more intensive and toxic treatment,whereas a more aggressive, and potentially moretoxic, therapeutic approach can be provided forpatients who have a lower probability of long-term survival. The 10-year event-free survival(EFS) rate is 67% to 78% for standard and higherrisk childhood ALL with risk-adapted combinationchemotherapy and central nervous system (CNS)prophylactic therapy (intrathecal chemotherapywith or without cranial radiation).6 More intensivechemotherapy regimens or hematopoietic stemcell transplantation (HSCT) may be pursued forcertain high-risk ALL groups and marrow relapse.Children with AML have a wide range in outcome
depending on specific biologic factors, with a 5-year EFS rate of 40% to 58%.7 Infection, severehemorrhage, hyperleukocytosis-related leukosta-sis, and resistant leukemia lead to thehighmortality.The mainstay of AML treatment is systemic combi-nation chemotherapy, with some form of CNS-directed therapy incorporated into most protocols.Induction of profound bone marrow aplasia isgenerally necessary to achieve remission, andleukocyte growth factors such as G-CSF or GM-CSF are often administered to reduce the durationmass. T-cell lineage ALL may be regarded asa disseminated form of T-cell lymphoblasticlymphoma in terms of malignant phenotype,approach to therapy, andpatterns of relapse. About2% of ALL is mature B-cell and the disseminatedform of Burkitt or Burkitt-like lymphoma.1 AML hastraditionally been subtyped into M0 to M7 formsaccording to the French-American-British (FAB)Cooperative Group morphologic-immunohisto-chemical classification system. Acute promyelo-cytic leukemia (APL), the M3 subtype of AML, isnotable for bleeding complications related to severecoagulopathy. A newer classification of AML by theWHO incorporates cytogenetic abnormalities andspecific gene mutations and provides more reliableprognostic information.4
An increased risk of leukemia is associated withcertain genetic disorders, including trisomy 21,monosomy7, andneurofibromatosis type 1 (partic-ularly JMML), and DNA repair disorders such asataxia-telangiectasia. Of special interest to theradiologist is the reported increased risk ofleukemia fromprenatal or postnatal radiation expo-sure, although the magnitude of the risk is subjectto considerable uncertainty and debate.5
Treatment
Risk-based treatment assignment is used in chil-of neutropenia, but have no significant effect onusually metadiaphyseal and geographic or perme-ative. Subperiosteal resorption of the medial cortexof the proximal humerus is commonly visible onchest radiographs at the time of presentation, butis nonspecific and can also be observed in thesetting of Gaucher disease, sickle cell disease,mortality. The duration of remission is prolongedby chemotherapy intensification and/or HSCT,although HSCT may not be necessary in thosewith complete remission and favorable prognosticfactors.8,9
Imaging Features
Fever, petechiae, lethargy, and pallor caused bybone marrow suppression by leukemic cells arecommon at presentation. These symptoms andsigns often prompt a chest radiograph. Chest radi-ography may reveal a mediastinal mass (especiallyfrom thymic infiltration in T-cell ALL), cardiomegalyand pulmonary vascular plethora (related toanemia), pulmonary air space opacification (relatedto infection, hemorrhage, or leukostasis), pleuralthickening (especially in JMML), splenomegaly(present in 75%), or skeletal abnormalities.10
More than a third of children with leukemiapresent with limping, bone pain, arthralgia, or othercomplaints referable to the extremities or spine.Approximately 40% of children presenting withacute leukemia have at least 1 radiographic skeletalabnormality.11,12 The number of bones involved onradiographs correlates with bone pain severity,but symptoms correlate poorly with the location ofskeletal lesions on radiographs and asymptomaticinvolvement is common, especially in nonweight-bearing areas.12,13 Findings of leukemia on skeletalradiographs include transverse lucent metaphysealbands, diffuse demineralization, subperiostealcortical bone erosion, periosteal reaction, lyticbone lesions, osteosclerosis, and pathologic frac-tures. Transverse metaphyseal lucent bands, alsoknown as leukemic lines, are attributable to distur-bance of endosteal mineralization resulting inabnormally small trabeculae adjacent to the zoneof provisional calcification. In preschool-aged chil-dren, transverse lucent metaphyseal bands aremore specific for leukemia than for other diseasesand are most conspicuous at sites of rapid skeletalgrowth such as the distal femur, proximal tibia,proximal humerus, and distal radius (Fig. 1).12
Diffuse demineralization is common, particularlyafter therapy,whereasosteosclerosis is uncommonand usually a late manifestation after therapy. Path-ologic fractures are most commonly observed asvertebral compression deformities in the setting ofneuroblastoma, or lymphoma (Fig. 2).14
Technetium (Tc)-99m phosphonatebased bonescintigraphy is abnormal in 75% of patients withALL at diagnosis. The most common abnormalityis symmetric increased uptake in the metadiaphy-ses of the lower limbs (Fig. 3). Other patternsinclude diffuse increased uptake in a superscanpattern with accentuation of the long bone meta-physes, focal increased uptake at sites of corticalbone destruction or pathologic fracture, and focaldecreased uptake at sites of osteonecrosis.15 Theaddition of early phase whole-body scintigraphymay increase the sensitivity for detection ofabnormal uptake from leukemia in the long bonemetadiaphyses, spine, and pelvis compared withthat of delayed-phase whole-body scintigraphyalone.16 The number of regions with abnormaluptake is positively correlated with age. There isonly modest correlation between the sites ofabnormal uptake, radiographic abnormalities, andclinical signs and symptoms.17
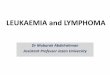
Fig. 1. An ankle radiograph from a 7-year-old girlwith precursor B-cell ALL shows transverse lucentbands (leukemic lines) along the distal tibial andfibular metaphyses just proximal to the zones ofprovisional calcification.
Fig. 2. Anteroposterior (A) and lateral (B) chest radiograpsubperiosteal resorption of the medial cortex and subtlehumeri, as well as diffuse demineralization of the vertebr
Leukemia and Lymphoma 769On magnetic resonance (MR) imaging, malig-nant infiltration of the bone marrow by leukemiatypically manifests as increased signal intensityon fat-suppressed T2-weighted and short-tauinversion recovery (STIR) sequences and de-creased signal intensity on T1-weighted images.18
Prolongation of the T1 relaxation time correlateswith the proportion of blast cells in the marrow.19
The infiltration is usually diffuse, including involve-ment of the epiphyses (Fig. 4). The findings areless conspicuous in hematopoietic marrow thanin fatty marrow and consequently are more difficultto appreciate in younger children before the phys-iologic conversion of hematopoietic to fattymarrow.20 ALL and AML cannot be reliably
hs of a 7-year-old boy with precursor B-cell ALL revealtransverse lucent metaphyseal bands of the proximal
al bodies.
Leukemic involvement of the solid viscera,especially the spleen and thymus, is common,and manifests as organomegaly from diffuse infil-tration or as focal masses. Diffuse infiltration ofthe thymus is characteristic of T-cell ALL (Fig. 5).Splenomegaly and a mediastinal mass fromthymic infiltration at presentation of childhoodALL are independent predictors of tumor lysissyndrome.22 The constellation of splenomegaly,hepatomegaly, lymphadenopathy, and skin rashis characteristic of JMML.23 Nephromegaly atpresentation is usually caused by leukemic cellinfiltration, but can also be caused by renal veinthrombosis from intravascular leukostasis.24 Focalrenal leukemic masses at presentation are usuallymultifocal, bilateral, low attenuation on computedtomography (CT), and hypoechoic on ultrasound,and must be differentiated from lymphoma,nephroblastomatosis, and infection. Renal infiltra-tion is most frequent with T-cell ALL and the M4and M5 subtypes of AML, and is often accom-panied by extramedullary involvement at other
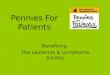
Fig. 3. A delayed-phase Tc-99m methylene diphosph-onate bone scintigraphy image of the lower extremi-ties of a child with precursor B-cell ALL depictssymmetric increased radiopharmaceutical uptake inthe long bone metadiaphyses.
Guillerman et al770distinguished from MR imaging or MR spectros-copy. The MR imaging appearance associatedwith marrow infiltration by acute leukemia is notspecific and can also be seen in settings of hema-
topoietic marrow hyperplasia and infiltrativemetastases from solid tumors such as neuroblas-toma, rhabdomyosarcoma, and Ewing sarcoma.21
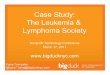
Fig. 4. An MR imaging examination of the lower extremitishows diffuse abnormal low signal intensity of the bonabnormal high intensity of the bone marrow on a STIR (B-cell ALL.sites.25 Leukemic infiltration of the kidneys israrely associated with acute renal failure or renaltubular dysfunction at presentation.26,27 Pancre-atic enlargement from leukemic infiltration isunusual.28
Brain atrophy, at least borderline in degree andof unclear cause, can be seen by CT in 40% ofchildren with ALL at diagnosis.29 Even in the pres-ence of neurologic symptoms, CNS imaging find-ings other than atrophy are uncommon. Head CTor MR imaging can reveal hemorrhage or infarction
es performed on a 3-year-old boy with refusal to walke marrow on a T1-weighted image (A) and diffuseB) image caused by marrow infiltration by precursor
associated with AML and is rare, occurring as anisolated finding in less than 1% of cases of AMLand in 11% of cases along with marrow diseaseat the time of diagnosis.36
A definitive diagnosis of leukemia is usually es-
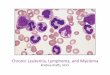
imaging examination in an 11-year-old girl withAML shows a soft tissue mass of the right maxillarysinus, zygoma, and inferior orbit that is isointense tothe marrow of the diploe of the skull, consistentwith a chloroma.
Leukemia and Lymphoma 771caused by intravascular leukostasis or throm-bocytopenia.30 Cerebral hemorrhage is morecommon than subdural or subarachnoid hemor-rhage. Abnormal enhancement of the meningesor nerve roots in a child with leukemia suggestsleptomeningeal involvement, even if CSF cytologicstudies are negative. As many as half of all casesof acute leukemia involve ocular manifestations,and the most frequent finding is retinal hemor-rhage. Retinal hemorrhages related to leukemiaare usually bilateral and located in the posteriorpole.31
A potential diagnostic pitfall is aleukemic or sub-leukemic leukemia. From one-quarter to one-thirdof cases of leukemia present with anemia andthrombocytopenia but no leukocytosis or leukemic
Fig. 5. A coronal chest CT image of 13-year-oldpatient with T-cell ALL shows a characteristic medias-tinal mass from diffuse leukemic infiltration of thethymus.blasts on peripheral blood smear.11,32,33 Many ofthese patients have bone or joint pain that canmasquerade clinically as osteomyelitis or arthritisfor several months and prompt referral for muscu-loskeletal MR imaging examinations. Appropriaterecognition of bone marrow infiltration on MRimaging can suggest the correct diagnosis ofleukemia before leukocytosis or blasts in theperipheral blood are noted.34
Extramedullary leukemia (EML), also known asgranulocytic sarcoma or chloroma, describesa mass of leukemic cells outside the bone marrow.EML is more common in infants than in older chil-dren and can precede the blast phase by up to 4years.35 The skin, orbits, CNS, and spine are themost common sites, and symptoms relate tomass effect. On CT, EML masses show variableenhancement and can be confused with otherneoplasms, hematoma, or abscess. On MR ima-ging, EMLmasses show isointensity to hypercellu-lar bone marrow (Fig. 6). EML is most commonlyFig. 6. A coronal T1-weighted image from an MRtablished by bone marrow aspiration or biopsyrevealing malignant cells of myeloid or lymphoidlineage. Definitive diagnosis can also be estab-lished by biopsy of an extramedullary mass ofleukemic cells.
Staging and Risk Stratification
Leukemia is conceptualized as a disseminatedmalignancy of the hematopoietic system and thereis no role for traditional staging based on imagingfindings as for lymphoma and solid tumors, evenfor children with isolated EML whomust be treatedas if there is systemic disease. ALL is classified aslow risk, standard risk, high risk, and very high riskfrom clinical and biologic features and early treat-ment response. Higher risk ALL groups includeinfants, adolescents, those with high leukocytecounts, those with CNS disease, those with initialinduction failure or high levels of end-inductionminimal residual disease (MRD), and those with
Nephromegaly at the time of presentation is
several weeks before relapse is detected by iliac
Guillerman et al772reportedly an adverse prognostic factor forALL.41 Nephromegaly in childhood ALL is alsocorrelated with subsequent renal damage detect-able by renal MAG-3 or dimercaptosuccinic acid(DMSA) scintigraphy.42 Overt testicular involve-ment at diagnosis has been considered anadverse prognostic factor for ALL, but this mayno longer be the case with aggressive initialtherapy. Neither the presence of a mediastinalmass at the time of diagnosis nor an incompleteresponse with a residual mediastinal mass onchest radiograph at day 35 or 70 of therapypredicts a worse prognosis in T-cell ALL.43
Therapy Response Evaluation
Imaging is not currently relied on to evaluateresponse to therapy for childhood leukemia.However, some trends may be observed onskeletal radiographs. The transverse metaphyseallucent bands usually resolve quickly with treat-ment, whereas periostitis, cortical erosion, andlytic bone lesions resolve more slowly, and osteo-penia may worsen, related to steroids. Bone scle-rosis and osteonecrosis may also develop aftertherapy.The high sensitivity of MR imaging for bone
marrow abnormalities has led to investigation ofMR imaging as a method for therapy responseevaluation. During chemotherapy for leukemia,the bone marrow becomes hypocellular and ede-matous. Following chemotherapy, there is progres-sive regeneration of normal hematopoietic cellsand fat. Marked increase in the marrow fat fractionis observed by chemical shift MR imaging in theT-cell lineage, hypodiploidy or certain chromo-some translocations.37 In AML, risk category defi-nitions are in evolution. Adolescent and obesepatients are in a poorer outcome group and leuko-cyte count at diagnosis is inversely related tosurvival, whereas trisomy 21, APL subtype, andearly response to therapy are favorable factors.38
The prognostic significance of radiographic andscintigraphic bone abnormalities is uncertain, relat-ing to conflicting reports in the literature. It has beenreported that multiple bone involvement on radio-graphs portends a shorter duration of remissionand survival39; that there is no correlation of radio-logical or scintigraphic extent of bone disease andduration of remission or survival13,17; that childrenwithout radiographic abnormalities have an aggres-sive form of leukemia, whereas those with a fewbone lesions have an indolent form40; and that thosewith radiographic bone lesions represent a subsetwith a better prognosis.33marrow of patients responding to chemotherapy,bone marrow aspirate or biopsy, reflecting thepatchy nature of relapsed leukemia and effectsof sampling bias.50 Unlike the diffuse marrowabnormality typical of leukemia on MR imaging atpresentation, early relapsed ALL can manifest aswell-defined nodules of low signal intensity onT1-weighted sequences and high signal intensityon T2-weighted and STIR sequences. In thissetting, directed marrow lesional biopsy may berequired to avoid false-negative iliac marrowsampling.51 Although time to relapse is an impor-tant predictor of outcome, evidence that earlydetection of relapse by frequent surveillanceimproves outcome is lacking.52
Extramedullary involvement is more common atrelapse than at presentation. Sanctuary sites forleukemic cells during therapy, where relapse canoccur even in the presence of bone marrow remis-whereas a low marrow fat fraction persists in thesetting of unresponsive disease. In children withALL who enter remission, marrow T1 relaxationtime normalizes, whereas the marrow T1 relaxa-tion time remains prolonged in those who do notenter remission. However, the specificity of MRimaging is limited by the difficulty in differentiatingviable neoplasm from effects of therapy, includinghematopoietic marrow regeneration (particularlywith G-CSF or GM-CSF therapy), hematopoieticmarrow reconstitution following stem cell trans-plantation, marrow iron overload from transfu-sional hemosiderosis, and marrow infarction andfibrosis.4446 Because of these limitations, MRimaging has not replaced marrow aspirate orbiopsy for assessment of therapeutic response inleukemia.47
Surveillance for Relapse
The most common site of ALL relapse is themarrow, followed by the CNS and testes. Isolatedmarrow involvement occurs in 48% of cases ofrelapsed ALL in children at a median time of 26months, whereas the incidence of isolated CNSrelapse is less than 5% and the incidence of iso-lated testicular relapse is less than 2%. Outcomeof ALL is poorer with early relapse and with iso-lated bone marrow relapse than with later relapseand combined marrow and testicular or CNSrelapse.48 Most AML relapses occur in themarrow, with CNS relapse being uncommon.Survival is substantially lower in those with shorterremissions, and relapsed leukemia is still theprimary cause of death in patients with AML.49
In some instances, relapse of leukemia in thevertebral marrow can be detected by MR imagingsion, include the CNS, testes, and kidneys. CNS
prophylaxis has greatly reduced the incidence ofCNS relapse, and surveillance imaging of theCNS is not warranted. A possible exception isEML, for which relapse is extramedullary in nearly40% of cases and most often in the CNS.36
Patients with suspected testicular relapse gener-ally go to biopsy without imaging, but occasionallyultrasound is requested and may show hypoe-choic, enlarged testicles with or without focallesions (Fig. 7). Isolated testicular relapse is rareand testicular biopsy at the end of therapy hasfailed to show a survival benefit for patients withearly detection of occult disease,53 arguingagainst a role for surveillance imaging of thetestes.
incidence begins to equilibrate between thegenders and patients older than 15 years of age
childhood and adolescent/young adult forms ofHL.54,55
HL is characterized by a variable number of char-acteristic clonal multinucleated giant cells (Reid-Sternberg [RS] cells) in an inflammatory milieu.The WHO classification separates the uncommonnodular lymphocyte-predominant form of HL(NLPHL) from the common form, designatedclassicHL.WHOsubtypesof classicHLarenodularsclerosis (NS), lymphocyte rich (LR), mixed cellu-larity (MC), and lymphocyte depleted (LD).56 TheNS subtype of HL accounts for greater than 85%ofpediatricHLand is characterizedby lymphnodesthat have thickened capsules and dense collage-nous bands that separate the nodes into macro-
-ye
Leukemia and Lymphoma 773have an approximately equal incidence betweenboys and girls.54 There are some studies suggest-ing an association between chronic Epstein-Barrvirus (EBV) and HL and this has led some investi-gators to propose a distinction between the
Fig. 7. Testicular relapse of precursor B-cell ALL in a 3Surveillance chest radiographs are sometimesobtained to evaluate for mediastinal relapse inpatients with T-cell ALL with a prior mediastinalmass. However, a beneficial impact of this prac-tice on outcome has not been established.
LYMPHOMAClassification and Epidemiology
Pediatric lymphoma, including Hodgkin lymphoma(HL) and non-Hodgkin lymphoma (NHL), is thethird most common malignant neoplasm in child-hood and adolescence. HL is unusual in patientsyounger than 4 years of age, and typically occursin older children and adolescents.3 In patientsyounger than 10 years of age, there is a malepredominance of HL; beyond this age the relativedefined masses on ultrasonography.nodules. The presence of collagen and fibrousstroma contributes to the presence of residualmediastinal soft tissue that is commonly seen earlyafter completion of therapy, even after no viabledisease remains. The MC subtype accounts for30% of the cases in young children and can beconfused for NHL.The characteristic RS cell in classic HL is
believed to arise from preapoptotic germinalcenter B-cells that cannot synthesize immuno-globulin and show constitutive activation of thenuclear factor k-B pathway, conferring resistanceto apoptotic stimuli. EBV is associated with 15%to 25% of HL in developed countries and up to90% in developing countries, most commonly inyounger patients with MC histology. Despite this,EBV serologic status does not seem to be a prog-nostic factor in pediatric patients with HL,57 incontrast with patients with NHL.NHL of childhood is a heterogeneous collection
of lymphoid neoplasms that are not classified asHL. Although a large number of forms of NHL arerecognized, the 4 most commonly occurring inchildren include Burkitt lymphoma (BL), diffuselarge B-cell lymphoma (DLBCL), anaplastic large
ar-old boy manifests as testicular enlargement by ill-
HL, NHL is more common in children younger than
Guillerman et al77410 years of age. There is also a male predomi-nance, particularly in older patients.58 Age-specific incidence also varies according to diseaseclassification, with LL occurring with a fairlyconstant rate across all age groups, whereasALCL and DLBCL predominate in older adoles-cents. Although the cause of NHL is uncertain,there is an increased incidence of lymphomas inimmunosuppressed patients. Other studies haveshown a role for EBV in the pathogenesis of lym-phoproliferative disease and NHL. Taken together,these findings suggest that disordered immuno-regulation, with resultant clonal proliferation ofimmature cells that have failed to differentiate,contributes to malignant transformation in NHL.59
Each NHL subtype has characteristic pathologicfeatures, and recent molecular and translationalinvestigations have led to new understanding ofthe pathobiology of NHL.54,59 BL and DLBCL arebelieved to derive from lymph nodegerminal centerregions where proliferating B-cell lymphoblastsnormally differentiate. The activation of proto-oncogenes and/or disruption of tumor suppressorgenes or hypermutation of proto-oncogenes arebelieved to result in the malignant transformationof these germinal center lymphoblasts. Consistentwith this interpretation, B-lineage cell surfaceantigen CD20 shows increased expression onboth BL and DLBCL. ALCL shows expression ofCD30 and is characterized by overexpression ofthe anaplastic lymphoma kinase (ALK) tyrosinekinase, which is believed to play a role in ALCLtumor genesis. LL, in contrast with the other pedi-atric NHL subtypes, predominantly arises fromimmature T-cells, corresponding to defined stagesof thymocyte differentiation. Less than 10%of LL isof B-cell origin.58 When greater than 25% of thebone marrow is infiltrated with lymphoblasts, thedisease is termed ALL rather than LL. Posttrans-plant lymphoproliferative disease (PTLD) is seenin the setting of both solid organ and bone marrowtransplantation, and results directly from hostimmunosuppression.60,61 PTLD, which is usuallyEBV-related, is not initially classified as amalignantlymphoma and frequently responds to reduction inimmunosuppression. However, the lymphoproli-ferative disease may progress to an aggressiveB-cell lymphoma, resulting in widespread malig-nant disease.62
Treatment
With current treatment approaches, the 5-yearcell lymphoma (ALCL), and precursor T-cell and B-cell lymphoblastic lymphoma (LL). In contrast withsurvival rate for children and adolescentsdiagnosed with HL is around 95%.7 This highcure rate has led to renewed interest in the rolethat treatment-related toxicities and long-termconsequences of therapy play in overall morbidityand mortality.63,64 The risk of death caused bydisease at 20 years from diagnosis almost equalsthe risk of death from other causes, includingtreatment-related effects.63
In the 1960s and 1970s, extended field radiationtherapy improved disease-free and overall survivalrates amongst patients with HL.55 However, thisso-called mantle radiation resulted in significantlate effects in the irradiated tissues. Subsequentdevelopment of a combination of chemotherapyregimens showed that disease-free survival couldbe improved with lower dose radiation therapyregimens, and, in certain patients with HL, elimina-tion of radiation therapy altogether. In patients withlow-stage HL, overall survival was no different forpatients whose initial therapy was chemotherapyalone, because of effective salvage regimens.65,66
In patients with advanced-stage HL, EFS washigher for those who received initial chemotherapyand radiation therapy compared with those withchemotherapy alone.54,67 As with current standardregimens, these early treatment regimens wererisk adapted: those with favorable-risk disease,defined by low stage and low bulk disease,typically receive 2 to 4 cycles of multiagent che-motherapy with either low-dose involved field radi-ation or no radiation, whereas those patients withhigher risk disease are stratified to receive moreintensive chemotherapy before involved fieldradiotherapy.55
These risk-adapted approaches do not take intoaccount initial disease response, in contrast withresponse-adapted approaches, in which the over-all treatment intensity is modulated during thecourse of therapy based on initial response. Thislatter approach is emerging as a potential meansof further reducing therapy and potentially reduc-ing late effects for those patients with HL inwhom cure is likely, while maintaining high curerates and aggressive treatment of those patientsat higher risk of relapse.64,67
Patients with NHL have lower overall survivalrates compared with HL. With current treatmentapproaches, more than 85% of children and 75%of adolescents with NHL survive at least 5 years.7
Treatment of childhood NHL depends on localizedversus disseminated disease. Localized disease istypically defined as stage I or II disease, whereasstage III or IV disease is generally considered tobe disseminated. In most children, NHL is widelydisseminated from the outset, and systemic treat-ment with aggressive combination chemotherapy
is usually recommended for most patients.54,58
Children with refractory or relapsed NHL havea worse outcome than newly diagnosed patients,and thus aggressive up-front therapy and earlyremission remain the goal of new treatmentregimens.68
The outcome for LL is excellent, with longer leu-kemialike therapy consisting of induction, consoli-dation, and maintenance therapy. In contrast,nonlymphoblastic NHL has superior outcomewith short, intensive pulse therapy. For recurrentor refractory B-lineage NHL or LL, survival is low(10%20%), emphasizing the importance ofachieving cure during the initial therapy. For recur-rent or refractory ALCL, as many as 60% ofpatients can ultimately be salvaged and achievelong-term survival.69 PTLD can involve multipleorgans and systems, and responds variably toconventional lymphoma therapies.6062
Radiation therapy plays little role in the routinemanagement of pediatric NHL, in contrast withHL.58 Mediastinal radiation is not commonly used
Leukemia and Lymphoma 775for patients with mediastinal masses, except in theemergent treatment of symptomatic superior venacava obstruction or airway obstruction. Even inthis instance, low-dose radiation is usually used.
Imaging Features
In HL, chest radiographs obtained for upper respi-ratory symptoms and/or vague constitutionalsymptoms, such as fever or night sweats, oftenprompt the initial diagnosis. At the time of diag-nosis, a mediastinal mass is present in more thantwo-thirds of patients with HL (Figs. 8 and 9).70
Fig. 8. An 18-year-old patient with HL. On the uprightposteroanterior (PA) chest radiograph, the transversewidth of the mediastinal mass exceeds one-third ofthe thoracic diameter, meeting the criterion for bulk
disease.The diagnostic evaluation should always includeimaging of the chest and neck up to the level ofthe Waldeyer ring. Large neck and mediastinalmasses may compress the airway and centralvascular structures. Care must therefore be takenin sedating these patients before imaging.71 Aftera careful physiologic and radiographic evaluationof the patient has been performed, the least inva-sive procedure should be used to establish thediagnosis. If possible, peripheral lymph nodebiopsy is preferable. Aspiration cytology is notsufficient because of the absence of stromaltissue, and core needle biopsies are necessary.Surgical staging has been largely replaced byimaging; however, mediastinoscopy or thoraco-scopy may be needed when other modalities failto establish the diagnosis or if questionable areasof involvement result in upstaging the patient andhistologic confirmation is required.Lung involvement is seen in less than 5% of chil-
dren younger than 10 years of age and 15% ofadolescents with HL.70,72 Nodules greater than 1cm are the most common pulmonary finding duringstagingof patientswithHL, althoughdiffuse intersti-tial thickening and lobar or segmental consolidationare other pulmonary manifestations of disease. Thepresence of pulmonary disease usually occurs inassociation with ipsilateral hilar or mediastinallymphadenopathy (Fig. 10). The most commonmechanisms of disease spreading into the lungsare hematogenous and lymphangitic spread, andless frequent, direct invasion. Pleural andpericardialeffusions are infrequent findings in HL and usuallyresult from lymphatic obstruction.70 Pleural effu-sions are typically transudative and usually negativefor malignant cells. Pericardial effusion, whenpresent,maysuggest tumor involvement of theperi-cardium fromdirect extension of the adjacentmedi-astinal mass. Where pericardial involvement issuspected, MR imaging may be superior to CT,particularly with the advent of respiratory andcardiac gated MR imaging.Liver involvement by HL is almost always
associated with splenic involvement, and splenicinvolvement without associated para-aortic lym-phadenopathy is unusual (Fig. 11). Splenic in-volvement occurs in 30% to 40% of Hodgkindisease (HD). Splenic size is unreliable for predict-ing splenic HD involvement.73
At diagnosis, bone marrow involvement isunusual in HL. MR imaging and [18F]fluorodeoxy-glucose (FDG)positron emission tomography(PET) are more sensitive than conventional CT fordetecting bone marrow involvement.72 Corticalbone involvement is similarly rare in HL. Whenpresent, lesions are typically lytic and may have
accompanying periosteal reaction.70
Historically, gallium (67Ga) scintigraphy was themainstay of functional imaging in lymphoma buthas now usually been replaced by FDG-PET.FDG-PET has been shown to be more sensitivethan gallium scintigraphy for determining lung,bone, and nodal involvement and has amuch lowerradiation dose than gallium scintigraphy.7476
Gallium has prolonged retention in the bowel,further limiting its usefulness in evaluating intra-abdominal disease. Although gallium scintigraphyapproaches the sensitivity of FDG-PET for diag-nosis and staging of neck and mediastinal/chest
Fig. 9. Chest CT images of an 18-year-old girl (see chesconglomerate lobular mediastinal lymphadenopathy.
Guillerman et al776nodal disease in pediatric HL, nearly all institutionsFig. 10. A 14-year-old girl with HL. CT images showpulmonary,mediastinal, andbilateralhilar involvement.have access to FDG-PET scanning and there iscurrently little justification for gallium scanning.FDG-PET has been studied extensively in adult
lymphoma77 and, to a lesser extent, in pediatricpopulations.72,78 The overall consensus frommultiple studies is that FDG-PET is more sensitivethan CT for involvement of normal-sized lymph no-des and extranodal disease, including the spleen,liver, and bone marrow (see Fig. 11; Fig. 12).7984
Combined FDG-PET/CT imaging retains the highsensitivity of FDG-PET for detecting disease, butimproves the specificity, with coregistered fusedimages resulting in the highest sensitivity andspecificity at detecting disease and correlatingsites of abnormal FDG uptake with specificanatomic regions.80,82,85,86
False-positive FDG uptake is well recognizedand can result from rebound thymic hyperplasia,hypermetabolic brown fat, muscle, hyperplastic/recovering marrow and/or spleen, gonadal andbreast cyclic hormonal stimulation, and sites ofrecent surgery or infection (Fig. 13).87,88 The char-acteristic patterns of nonspecific uptake are wellrecognized by experienced radiologists and nu-clear medicine physicians and the use of coregis-tered FDG-PET/CT has proved invaluable for
t radiograph in Fig. 8) with HL depict characteristicidentifying and eliminating areas of false-positiveuptake from the diagnostic evaluation.88 In someinstances, background uptake can be reduced.For example, brown fat uptake can be largely elim-inated by warming the patient, and, in challengingcases, premedicating the patient with fentanyland/or benzodiazepines.89
Among pediatric NHL, BL most commonlypresents with intra-abdominal visceral disease,and widespread extranodal involvement is oftenpresent. The initial imaging evaluation is usuallydirected at assessment of symptoms referable toabdominal involvement. Involvement of the perito-neum, solid abdominal organs, and bowel withcomplicating intussusception can be seen (Figs.14 and 15).
Leukemia and Lymphoma 777Asmany as 75% of patients with LL present witha mediastinal mass and dyspnea, wheezing,stridor, or dysphagia.58 The mediastinal enlarge-ment in LL is attributable to diffuse thymic involve-ment and does not show the typical nodularheterogeneous appearance more characteristicof HL and other forms of NHL (Fig. 16). Thesetumors grow rapidly and patients with LL maydeteriorate quickly because of airway compres-sion and impairment of venous return, particularlywhen patients are placed supine or sedated. In thispopulation of patients, diagnostic imaging may notbe possible because of the tenuous clinical statusof the patient, and pleural fluid and/or bonemarrow aspiration may be the only means of accu-rately diagnosing these patients.ALCL is often associated with systemic symp-
toms and signs such as fever and weight loss,and a prolonged waxing and waning course beforediagnosis. A mediastinal mass may be seen in upto 40% of patients with ALCL, and, when present,is often accompanied by large pleural and pericar-dial effusions. ALCL can also involve lung, skin,
Fig. 11. Axial and coronal contrast-enhanced CT images omediastinal mass with accompanying diffuse splenic invothis patient with HL. The accompanying FDG-PET imageboth the chest and abdomen.and bone,54 and often presents with extensivemultifocal disease (Figs. 17 and 18).DLBCL has a less characteristic clinical pattern
compared with other NHL subtypes. Most patientswith DLBCL present with localized disease. Anteriormediastinal and/or bulky cervical/supraclavicularlymphadenopathyaremorecharacteristicofDLBCLthan of the other NHL subtypes. Up to 70%of thesepatients have a mediastinal mass, which mayproduce airway obstruction and superior venacava syndrome (Fig. 19).54,72 In general, thesetumors are more aggressive than HL and malignantpericardial effusions resulting fromdirect pericardialinvasion, malignant pleural effusions, and pulmo-nary involvement may be seen (Fig. 20). Patientswith DLBCL with disease localized to the medias-tinum may be difficult to distinguish from HL basedon imaging (see Fig. 19).54 The presence of meta-chronous peripheral lymphadenopathy or boneinvolvement makes DLBCL the more likely diag-nosis. About 20% of pediatric patients with DLBCLpresent with primary mediastinal disease (primarymediastinal B-cell lymphoma).90 This presentation
f the chest and abdomen, respectively, show a largelvement and mesenteric lymph node enlargement inshows diffuse FDG uptake throughout the mass in
Guillerman et al778is more common in older children and adolescents.These tumors are more aggressive and are associ-ated with a worse outcome compared with otherpediatric large B-cell lymphomas. Growth into adja-cent structures is common and there is a character-istic tendency for focal involvement of the kidneys(see Fig. 20).PTLD can involve multiple organs or have focal
involvement. The use of FDG-PET to stage theextent of disease and assess response to therapyin PTLD is increasingly advocated (Fig. 21).62,91
Staging and Risk Stratification
The Ann Arbor system for staging of HL was devel-oped to classify anatomic sites of disease basedon a combination of clinical, surgical, and imagingfindings. The Cotswold modifications of the AnnArbor staging system incorporated the prognosticimplications of tumor bulkiness and number ofdisease sites into the staging system.92 The revisedAnn Arbor staging system is shown in Box 1.Staging is largely based on identifying diseaseabove or below the diaphragm and at identifyingnoncontiguous involvement of extralymphatic sites
Fig. 12. Axial CT, coronal FDG-PET, and fused axial PET/CTnode involvement was shown by FDG-PET and PET/CT fusiohave been interpreted as unopacified bowel. This patient ihad extensive pulmonary nodules, confirmed as FDG-avidof disease that indicate hematogenous spread.Unique to HL is the designation of extralymphaticdisease that results from direct extension of aninvolved lymph node region, which can be chal-lenging at the time of staging. For example, contig-uous involvement of lung adjacent to a largemediastinal mass may be considered stage IIErather thanstage IVdisease.However, thepresenceof a malignant pleural effusion that is cytologicallypositive for HL would be considered stage IV. Forareas of questionable noncontiguous extralym-phatic involvement, pathologic confirmation maybe requiredbeforeassignment tostage IV.Thepres-ence of B symptoms (fever, night sweats, weightloss) is included in the staging of the patient, andinfluences whether the patient is assigned to a lowor intermediate/high-risk treatment regimen.The posteroanterior (PA) upright chest radio-
graph is still used for determining the presence ofbulk disease (mediastinal mass > one-third of themaximal transthoracic diameter) (see Fig. 8).55
However, the Cotswolds modification of the AnnArbor classification also defines lymph nodesgreater than 10 cm in maximal dimension on CTimaging as bulky. Despite various attempts, the
show extensive FDG-avid HL. Retroperitoneal lymphn, whereas the same site shown on the CT alone coulds the same 14 year old who is shown in Fig. 9, who alsosites of disease.
Fig. 13. A 15-year-old patient with stage IV HL. Baseline FDG-PETand CT show extensive disease, including pulmo-nary lesions. At the end of therapy, FDG uptake has resolved, except for presumed background brown fat uptakein the neck. Residual CT abnormalities were interpreted as scar tissue in view of the negative FDG-PET scan. By 4months after completion of therapy the patients pulmonary relapse was obvious by CT and confirmed by FDG-PET. Rx, treatment.
Fig. 14. Sporadic BL has a proclivity for widespread extranodal involvement, as illustrated by the presence ofmasses in the pancreas and right kidney on an abdominal CT image (A), proximal right tibial bone marrow onan T1-weighted MR image (B), and lumbosacral epidural space on a sagittal STIR MR image (C) in this 8-year-old boy.
Leukemia and Lymphoma 779
Guillerman et al780current definitions of bulky disease are not stan-dardized and frequently depend on the clinical trialprotocol and the cooperative group from whichthe protocol derives. For example, bulky disease,
Fig. 15. An 8-year-old girl with BL. Coronal CT reconstruc(arrows). Two days later, the patient presented with abdintussusception. A contrast enema confirmed the intussuintussusception recurred, she was taken to the operating
Fig. 16. Diffuse infiltration of the thymus resulting ina smoothly marginated homogeneous anterior medias-tinal mass that compresses the airway and occludes theleft brachiocephalic vein or superior vena cava isa common presentation of T-cell lymphoblastic lym-phoma, as shown in this chest CT image.as defined by PA chest radiograph and CT of nodaldisease, is still recognized in the risk stratification ofpatients enrolled in Childrens Oncology Grouptrials and St Jude Consortium trials. However,results from the German-Austrian Pediatric Multi-center trial suggest that bulk disease alone is nota prognostic factor for outcome with a risk-adapted treatment strategy.93 Contrast-enhancedCT and FDG-PET imaging complete the contribu-tion of imaging to staging and risk stratification.There is currently no role for bone scintigraphy inthe routine staging evaluation.94 Increasingly,particularly in Europe, the use of MR imaging,including diffusion-weighted imaging, is beingadvocated to reduce radiation exposure in theseheavily imaged and treated patients.95,96
Combined FDG-PET/CT imaging provides themost sensitive and specific means of accuratelystaging patients with HL (see Figs. 1113). Forexample, in one study of children and adolescentswith HL, FDG-PET changed the staging in 15% ofthe patients, most of whom were upstaged. Mostof the false negatives not detected by FDG-PET
tion shows thickening of the distal ileum and cecumominal pain. An ultrasound examination showed ansception, which was successfully reduced. When theroom where the diagnosis of BL was established.
ang a
Leukemia and Lymphoma 781Fig. 17. An 11-year-old patient with paraspinal ALCL. CTtion and invasion of the spinal canal. An MR imaginhad tiny pulmonary nodules shown by chest CT.97
Most discordance between CT and FDG-PEToccurs at extranodal sites, such as the lung, inwhich CT is superior for tiny nodules, and thespleen and bone marrow, in which FDG-PET issuperior.98 The highest diagnostic accuracy istherefore achieved using a combination of FDG-PET and CT.Despite these advances in functional imaging,
staging with conventional imaging modalities (CTand/or MR imaging) alone as the standard initialstaging procedure for risk and treatment stratifica-tion has historically been sufficient to achieve curerates greater than 90% in pediatric HL. Therefore,the ultimate impact of additional whole-bodyimaging with either MR imaging or FDG-PET,although promising, may be modest in terms ofchanging overall cure rates of pediatric HL.However, the incorporation of FDG-PET/CT find-ings into radiation treatment planningmaybe signif-icant in treatment-related toxicity, by guidingtreatment dose and target treatment volume.55,63,99
Onestudy found that involved field radiation therapy(IFRT) volumes needed to be adjusted from FDG-PET findings in 70%of pediatric patients with HL.98
The St Jude (Murphy) classification is used forthe staging of pediatric NHL (Box 2). This system
therapy showed a decrease in size of the mass. Althougthe presence of FDG uptake after completion of consolidaRx, treatment.dMR images show paraspinal mass with bone destruc-nd FDG-PET scan obtained while the patient was onis based on tumor burden, and has served clini-cians well for many years. In the past, even withless effective chemotherapy, the St Jude systemprovided a sound basis for treatment stratification.Children with NHL, in contrast with HL, frequentlypresent with disseminated disease. As with HL,CT scanning is most commonly used for the initialstaging of NHL. For specific sites of bone or CNSdisease, MR imaging is used. FDG-PET detectsadditional disease in a small proportion of pedi-atric patients with NHL (see Figs. 17, 18 and 20;Figs. 22 and 23), but it has not been shown todetect additional sites of disease that would resultin frequent alterations of patient stage, nor has itbeen generally shown to result in any modificationof treatment.100 High cure rates result from risk-adapted intensive chemotherapy without radiationtherapy, and it has not been necessary to mapprecisely every small site of nodal disease, be-cause patients are being treated intensively andsystemically.58 As a result, in contrast with theadult situation, FDG-PET is not routinely includedin the diagnostic staging of childhood NHL.101
However, NHL is often disseminated at the timeof initial disease presentation and, in this setting,early response assessment may be more usefulin predicting ultimate patient outcome rather than
h the patient did not have a baseline FDG-PET scan,tion chemotherapy suggested residual active disease.
Guillerman et al782extent of disease and overall tumor burden atdiagnosis (see Fig. 23). For these patients, diag-nostic FDG-PET imaging is obtained to providea baseline for subsequent response assessment.ALCL is an example of disease distribution not
fitting well into the St Jude NHL staging system
Fig. 18. A 12-year-old boy with ALCL. He initially presenenlargement. Ultrasonography (not shown) revealed hetetesticular biopsy was negative for malignancy. The CT scpain, reveals diffuse mesenteric and retroperitoneal lympobliteration of the left renal vein likely accounted for theuptake in the primary mass, as well as a left supraclavicul
Fig. 19. Primary mediastinal large B-cell lymphomaoften assumes a lobular morphology like HL and tendsto occlude the superior vena cava, as shown on thischest CT image.(see Figs. 17 and 18). Sites of involvement that areunusual in childhood lymphoma, such as skin,lung, and bone, are common in ALCL. LL is anotherexample of the limitations of the NHL stagingsystem. Most patients are stage III, with few pre-senting with either stage I or stage II disease.Furthermore, the outcome of patients with stageIV disease (usually the result of bone marrowinvolvement), differs little from those with stage IIIdisease. Because of the overall excellent responseof these patients, features such as tumor bulk,pleural effusion, and respiratory obstruction donot ultimately influence overall outcome.54,58 Aswith LL, BL responds rapidly to aggressive che-motherapy.58 Patients with localized disease haveanexcellent outcomeaftera short courseofaggres-sive chemotherapy, and, with improvements intreatment, even patients with advanced-stagedisease at diagnosis have an excellent overalloutcome. AlthoughFDG-PETscanningmaybeper-formed during staging of patients with BL, given thespeed with which these tumors grow and enlarge,there is little evidence that functional imagingaffects staging or outcome in this population ofpatients.101
ted with testicular pain, swelling, and left testicularrogeneous testicular echogenicity, but no focal mass;an shown here, obtained for subsequent abdominalhadenopathy. Occlusion of the inferior vena cava andinitial left testicular complaints. FDG-PET scan shows
ar site. No uptake was present in the scrotum.
Leukemia and Lymphoma 783Therapy Response Evaluation
Initial efforts to develop objective measurementcriteria for assessing solid tumors were putforward by the WHO and used bidirectionalmeasurement techniques.102 These measurementtechniques focused primarily on disease staging
Fig. 20. (A) Axial CT images in a patient with mediastinal Dbrachiocephalic vein, tracheal narrowing, pulmonary metuptake in the mediastinal mass, pulmonary lesions, and rof disease in the pancreas that are difficult to resolve byand determining initial disease bulk in an effort tostratify patients into treatment groups. Earlycriteria for response were also developed, andled to categories ranging from complete response(CR) to progressive disease, and included stable/no change or partial response (PR) in the classifi-cation scheme, depending on the estimates of
LBCL, showing mediastinal mass, near occlusion of theastases, and bilateral renal lesions. (B) FDG-PET showsenal lesions. In addition, FDG-PET clearly shows 2 fociCT.
eveulatoapy
Guillerman et al784change in tumor size. The WHO criteria presentedmany challenges, particularly for tumors such as
Fig. 21. A 12-year-old heart transplant recipient with fnode enlargement in the retroperitoneum, supraclavicment, consistent with PTLD. Disease did not respondextensive FDG-avid PTLD. One month after chemotherHL, which frequently leave measurable residualposttreatment scar tissue. Minimum lesion sizeand numbers of lesions to be recorded were notspecified and, depending on the location of tumor,size measurements of lymph nodes may havebeen based on physical examination estimates.In addition, these methods were devised beforethe advent of the multiplanar cross-sectionalimaging techniques that are in common use today(CT and MR imaging), and underestimates ofdisease burden and the choice of measurementtechnique often led to errors in establishingdisease progression or response.Developing objective measures of treatment
response is essential to having evaluable prospec-tive end points in early phase clinical trials anddetermining whether new agents warrant furthertesting. The challenge is developing surrogateend points that accurately reflect the diseaseprocess and response to therapy at a time whenother indicators of response (eg, change in clinicalstatus) may not reflect treatment response. Forexample, a brisk response to chemotherapy is anindirect determinant of biologic homogeneitywithin the tumor, which, in turn, translates intomore uniform chemosensitivity across the entiretumor volume. As a result, changes in FDG uptakethat occur soon after the initiation of therapy serveas an in vivo chemosensitivity test, even whensignificant changes in tumor volume or complete
r and increased EBV titers. CT showed extensive lymphr regions, and mediastinum, as well as splenic involve-reduction in immunosuppression. FDG-PET confirmedthere is no residual disease.resolution of the tumor mass are not yet seen onmorphologic imaging (Fig. 24). Studies showingthat significant reductions in tumor volume andFDG-PET negativity are associated with favorableoutcome in both pediatric HL and NHL suggestthat rapid and homogeneous cytotoxic chemo-therapy responsiveness may lead to improveddisease-free survival.103
Several studies of FDG-PET for response as-sessment in pediatric lymphoma have beenreported.86,104107 The use of FDG-PET in assess-ing response during therapy for tumors that areFDGavidat the timeof staging isbeing investigated.In one study of pediatric and young adult patientswith HL or NHL, the negative predictive value ofFDG-PET during therapy was 96%, whereas thepositive predictive value was 100%.86 This obser-vation, substantiated by other studies, suggeststhat interim FDG-PET scanning during therapy isan excellent prognostic indicator for predicting clin-ical outcome.An ongoing major European study in childhood
and adolescent HL is evaluating the role of interimFDG-PET in determining the need for involved fieldradiotherapy in patients who have a good earlyresponse to induction chemotherapy (ie, thosepatients who are in complete remission or in partialremission based on CT, but FDG-PET negative).100
Leukemia and Lymphoma 785Box 1Modified Ann Arbor staging system forchildhood HL
Stage I: involvement of single lymph node region (I) orlocalized involvement of a single extralymphaticorgan or site (IE)
Stage II: involvement of 2 or more lymph node regionson the same side of the diaphragm (II) or localizedcontiguous involvement of a single extralymphaticorgan or site and its regional lymph node(s) withinvolvement of 1 or more lymph node regions onthe same side of the diaphragm (IIE)
Stage III: involvement of lymph node regions on bothsides of the diaphragm (III), which may also beaccompanied by localized contiguous involvement ofan extralymphatic organ or site (IIIE), by involvementof the spleen (IIIS), or both (IIIE1S)This represents an early effort to incorporate aresponse-based treatment algorithm into ongoingclinical trials of pediatric lymphoma patients. Mostof the data have been obtained after 2 cycles ofchemotherapy, although there is no evidence tosuggest that a response evaluation after 2 or 3cycles is either superior or inferior to that performedafter 1 cycle. A very early response to therapy after 1cycle may be more predictive than responsesmeasured after more prolonged therapy.As noted earlier, the use of two-dimensional
measurement techniques does not account forfunctional and metabolic changes in the tumor.The International Harmonization Project (IHP)was convened to address this issue in adultlymphoma and issued revised criteria in 2007 forcomplete remission, partial remission, progressivedisease, and stable disease (SD) both for HL and
Stage IV: disseminated (multifocal) involvement of 1or more extralymphatic organs or tissues, with orwithout associated lymph node involvement, orisolated extralymphatic organ involvement withdistant (nonregional) nodal involvement
Anatomic lymph node regions for the purpose of HLstaging are Waldeyer ring, cervical/supraclavicular/occipital/preauricular, infraclavicular, axillary/pectoral,epitrochlear/brachial, mediastinal, hilar, splenic/splenichilar, mesenteric, para-aortic/celiac/periportal/retro-crural,iliac, inguinal/femoral, and popliteal.
The designation A is for asymptomatic disease and B isfor the presence of unexplained fever, weight loss, ornight sweats. The designation E is for minimal extra-lymphatic disease from direct extension of an involvedlymph node region, originally devised to indicate ex-tralymphatic disease limited enough to be subjectedto definitive treatment by radiation therapy. Thedesignation E is not appropriate for cases of wide-spread or diffuse extralymphatic disease (eg, a largepleural effusion that is cytologically positive), whichshould be considered stage IV.NHL.77,108 Although the focus of this project wasadult lymphoma, the criteria proposed can, forthe most part, be applied to pediatric lymphomas.A summary of these criteria is shown in Table 1. Asbefore, measurable extranodal disease should beassessed in a manner similar to that for nodaldisease. For HL, the spleen is still considereda site of nodal disease (see Fig. 11). Disease locithat are assessable but not measurable (eg,pleural effusions and bone lesions) are recorded
Box 2St Jude staging system for childhood NHL
Stage I: a single tumor (extranodal) or single anatomicsite (nodal), excluding mediastinum or abdomen
Stage II: a single tumor (extranodal) with regionalnode involvement; 2 or more nodal sites on the sameside of the diaphragm; 2 single (extranodal) tumorswith or without regional node involvement on thesame side of the diaphragm; a primarygastrointestinal tract tumor, with or withoutassociated mesenteric nodes, grossly completelyresected
Stage III: 2 single tumors (extranodal) on oppositesides of the diaphragm; 2 or more nodal areas aboveand below the diaphragm; primary intrathoracictumors (mediastinal, pleural, thymic); extensiveprimary intra-abdominal disease, unresectable;paraspinal or epidural tumors
Stage IV: any of stages IIII with initial CNS or bonemarrow involvement (1.5 cm in greatest transverse diameter, ornot more than 1.0 cm in short axis for lymph nodesless than 1.5 cm in size at diagnosis). These
Guillerman et al786criteria have been developed for adults but shouldbe applicable for most pediatric patients, althoughsome clinical judgment is necessary in cases withborderline enlarged lymph nodes. Splenic and/orliver involvement, either as diffuse enlargementor focal nodules, should return to normal sizeand nodules should disappear. However, thedetermination of splenic involvement may be chal-lenging and multiple imaging modalities may beused to unequivocally establish the presence orabsence of residual abdominal visceral disease(see Fig. 24). Bone marrow involvement, if present,must have cleared based on repeat bone marrowbiopsy. Residual bone marrow abnormalities byimaging (ie, FDG-PET or MR imaging) should beconfirmed by biopsy in order for a patient to beconsidered in CR.PR is defined by the IHP as regression of
measurable disease with no new sites of disease.There must be at least a 50% decrease in the sumof the product of the diameters of up to 6 largestdominant nodes or nodal masses, which shouldbe clearly measurable in 2 dimensions. Thereshould be no increase in size of other nodes, liver,
Fig. 22. A 16-year-old patient with DLBCL. Axial CT andmultiple diaphragmatic lymph nodes. An additional focuwould not have been detected without the use of FDG-PEand spleen. Splenic/hepatic nodules must regressby not less than 50% in size. If bone marrow wasinvolved before therapy and clinical CR was ac-hieved by other criteria, but there is persistentmarrow involvement, the patient is still considereda partial responder. For partial responders, post-treatment FDG-PET should be positive in at least1 previously involved site. If FDG avidity at base-line is unknown, then the CT criteria are used.SD is defined by the IHP as failure to attain either
CR or PR, but not meeting criteria for progressivedisease. For FDG-avid lymphomas, the FDG-PETscan should be positive at prior sites of diseasewith no new areas of involvement on the posttreat-ment CT or FDG-PET. If FDG-PET is not available,there must be no change in the size of the previouslesions on the posttreatment CT scan.The appearance of any new lesion at the end of
therapy should be considered relapsed (after CR)or progressive disease (after PR or SD) accordingto the IHP unless otherwise confirmed by histo-logic evaluation. Increased FDG uptake at a previ-ously unaffected site or at a previously involvedsite that had responded should also be considered
FDG-PET show uptake in the mediastinal mass ands of disease in a small aortocaval lymph node (arrow)T.
Fig. 23. An 8-year-old patient with hip pain. MR imaging shows diffuse marrow replacement on T2-weighted andT1-weighted images. CT shows extensive visceral and intra-abdominal involvement. FDG-PET confirms diffuseabnormal uptake throughout the abdomen and bone marrow. Bone marrow aspirate showed greater than25% infiltration of the marrow by Burkitt cells, indicating Burkitt leukemia.
Fig. 24. This patient with HL received 2 4-week cycles of therapy. Compared with the baseline examination (seeFig. 11) there is still residual mediastinal soft tissue abnormality, although decreased from the baseline examina-tion. The spleen is now normal in size; however, punctate hypodensities are still present in the spleen. Despitethese residual CT findings, the accompanying FDG-PET shows complete resolution of abnormal FDG uptake inthe mediastinal mass and in the abdomen.
Leukemia and Lymphoma 787
Guillerman et al788Table 1Summary of new Harmonization Projectcriteria for PET and CT in determiningresponse in lymphomaa
Response Criteriarelapsed or progressive disease (see Fig. 13).Lymph nodes are considered abnormal if theirshort axis is greater than 1.0 cm. In most patientswith prior pulmonary nodules, new lung nodulesidentified by CT are typically benign and shouldbe histologically confirmed to establish relapse/progressive disease. Sites of relapse or progres-sive disease should be FDG avid unless the lesion
CR FDG-PET completely negativeResidual lymph nodes/nodalmasses allowed, if FDGnegative
Bone marrow biopsy negativeSplenic/liver involvement mustdisappear
No new sites of disease
PR PDG positivity should bepresent in at least 1previously involved site
Regression of measurabledisease; no new sites ofdisease
50% decrease in SPD of 6dominant LNs/nodal masses
50% reduction in splenic/hepatic nodules, if present
Even if CR by other criteria,positive bone marrowbiopsy is considered PR
SD Failure to achieve PR, but notmeeting PD criteria
PD/relapse Any lesion increased in size by50% from nadir
Any new lesionPET should be positive in new/progressed lesions if1.5 cm
Notes: New criteria include PET in definition of CR. PETconsidered positive if uptake is greater than mediastinalblood pool (lesions >2 cm), or more than local background(lesions
Fig. 25. (A) PET/CT showing increased FDG uptake in the mediastinal nodal masses of a patient with HL at diag-nosis. The uptake is clearly greater than in the mediastinal blood pool or liver. (B) After 2 cycles of therapy, a medi-astinal soft tissue mass persists. There is low-level FDG uptake in the mass, as great as in the mediastinal bloodpool but less than in the liver, which emphasizes the challenge in interpreting residual FDG uptake in patientscompleting their up-front chemotherapy.
Leukemia and Lymphoma 789
unclear whether radiation treatment can be re-duced to initial involved sites of nodal activity oreliminated entirely for those patients with HL whohave no residual nodal activity early after responseto therapy.55 One approach, for example, would berestricting radiation to sites of residual FDGuptake.The goal would be to titrate therapy using the prog-nostic value of early treatment response to reducetreatment intensity in thosepatientswith rapid earlyresponses and thereby reduce toxicity while, at thesame time, intensifying treatment of those withslowearly responses in aneffort to improvedisease
normal tissues compared with involved field radia-
presents as an enlarging thymic mass within 6to 8 months of completion of chemotherapy(Fig. 26). Rebound thymic hyperplasia can showavidity for FDG, usually in a pattern of mild, diffuseuptake, in contrast with the intense, discreteuptake usually associatedwith lymphoma. If a childor adolescent has imaging findings compatiblewith rebound thymic hyperplasia, continued sur-veillance is advised rather than biopsy, especiallyif there is no other evidence of recurrence or priorneoplastic involvement of the thymus.112
In a recent pediatric intermediate-stage and
madia
Guillerman et al790tion and, coupledwith functional imaging responseassessment, could produce significant reductionsin radiation-related late effects.
Surveillance for Relapse
Relapse occurs in approximately 20% of pediatricpatients with HL.63 Most of these occur within thefirst 3 years. It has been suggested that relapsesoccurring beyond 1 year after the completion oftherapy have a favorable prognosis relative tothose occurring early after completion of therapyand therefore surveillance imaging and identifica-tion of relapse has remained an important goal ofobservation of therapy.Rebound thymic hyperplasia, a potential mimic
of mediastinal relapse, most characteristically
Fig. 26. A chest CT image (A) obtained in an asymptotherapy for HL shows enlargement of an anterior mecontrol.These approaches, all of which require confirma-
tion in clinical trial settings, are intended to developresponse-adapted therapy to identify patients withfavorable chemotherapy-sensitive disease whocan be treated with abbreviated chemotherapyand low-dose IFRT or no radiation therapy at all.Alternatively, rather than entirely eliminating radia-tion therapy, radiation therapy volumes may berestricted to lymph node regions that were initiallyinvolvedwith disease rather than the entire regionalnodal group.55,99 Such an approach has the poten-tial to significantly reduce the irradiated volume ofimage (B) obtained at the end of therapy, representing readvanced-stage HL study, relapses occurred in10.6%of thepatients,with amedian time to relapseof 7 months.113 Most of these relapses occurredwithin 18 months after completion of therapy andmost of these relapses were local, at original sitesof disease. Nearly two-thirds of these relapsesweredetectedbasedonclinical symptoms, labora-tory tests, or physical examination findings. Only17% of the patients, all of whom relapsed morethan 1 year after therapy, were asymptomatic andhad disease detected solely from surveillanceimaging. A review of the number of imaging studiesperformed to identify these relapses revealed thatmore than 400 CT scans were mandated byprotocol to detect these asymptomatic relapses.Based on this, it has been suggested that CT, andimaging of any kind, is overused in the routine post-treatment surveillance of patients with HL, andmodifications in surveillance protocol are indicatedfor routine long-term surveillance. A recent reporthas further emphasized the considerable increasein radiation exposure to these patients attributableto routine surveillance imaging.114
As has been reported in adult studies, mostrelapses occur in areas of initial disease and withinthe first year after completionof therapy,which indi-cates that the frequency of screening should begreatest in the early posttherapy years. The role ofFDG-PET as a surveillance tool to detect relapsein asymptomatic patientshasnot beenestablished.In particular, the problem of false-positive findings
tic 15-year-old patient 5 months after completion ofstinal soft tissue structure compared with a chest CT
bound thymic hyperplasia.
in evaluating pediatric lymphoma is becoming
Leukemia and Lymphoma 791TREATMENT-RELATED COMPLICATIONS
Overall survival rates are excellent for ALL,HL, local-ized low-stage NHL, and even for some advanced-stage NHL and AML. The goal of reducing toxiceffects of therapy is now a focus of the next genera-tion of treatment protocols.55,115 Imaging playsan important role in diagnosing treatment-relatedcomplications of leukemia and lymphoma. Many ofthe complications associated with leukemia andlymphoma are shared because of the treatment ofboth with cytotoxic chemotherapy with associatedmarrow suppression. The complications can beacute or late in onset, and can involve virtually anyorgan system. Among the complications amenableto diagnosis by imaging are opportunistic infecti-ons, cerebral hemorrhage/infarction, methotrexate-induced leukoencephalopathy, venous thrombosis,anthracycline-induced cardiomyopathy, bleomycin-induced pulmonary fibrosis, bronchiolitis obliterans,radiation pneumonitis, radiation pericarditis, typhli-tis, asparaginase-associated pancreatitis, hepaticveno-occlusive disease, graft-versus-host disease,hemorrhagic cystitis, posttransplant lymphoprolifer-ative disorder, osteonecrosis, and osteoporosis. Adetailed discussion of the imaging of these compli-cations is beyond the scope of this article.Second malignant neoplasms, including AML,remains and current recommendations do notinclude the use of FDG-PET for routine surveil-lance.77 However, if sites of disease are detectedby other imaging modalities or are suspected clini-cally, there may be a role for FDG-PET imaging inconfirming relapse, but not as an integral part ofroutine surveillance in either HL or NHL.100 In onestudy, the use of FDG-PET/CT to identify recurrentdisease in asymptomatic patients with HL andNHLled to false-positive results in 63% and 41% ofpatients, respectively, for a positive predictivevalue of only 53%.106 Although the negative predic-tive value was greater than 99% in this study, thehigh frequency of false positives does not allowappropriate treatment decisions to be confidentlymade based solely on FDG-PET surveillanceimaging.There will be understandable reluctance to
reducing the intensity of surveillance imaging ata time when treatment intensity and duration oftherapy are also being reduced. Nonetheless, allof the available evidence suggests that aggressivemonitoring early after therapy combined with judi-cious imaging and close physical examination andlaboratory monitoring during the surveillanceperiod is the most effective means of followingthese patients.NHL, and malignancies of breast, lung, and thyroidfeasible (Fig. 27). Whole-body MR imaging hasshown good agreement with FDG-PET/CT forboth nodal and extranodal staging of lymphoma.116
MR imaging false negatives occur with normal-sized involved lymph nodes and spleen, diseasethat is detectable by FDG-PET. MR imaging pro-vides an alternative imaging method to CT foranatomic disease assessment at staging and re-staging without ionizing radiation exposure. Fur-thermore, surveillance by MR imaging may be theimaging modality of choice, particularly in patientswith lymphoma in whom sustained PR or CR hasoccurred.Because of high tumor cellularity and highwithin radiation fields, are all of concern.55Historicaltreatment regimens for lymphoma,which used highradiation doses and intense chemotherapy regi-mens, had well-established rates of secondarymalignancy.54 The risk of secondary malignancyafter low-dose radiation is not well described,because this became the standard treatment ofchildren only in the mid 1980s and for adolescentsin the early 1990s. With unknown latency periodsfor developing second malignancies after low-dose radiation exposure and reduced chemo-therapy, there is noclear role for routine surveillanceimaging in these patients.
FUTURE DIRECTIONS
With isotropic voxel acquisition of cross-sectionalimaging data, the ability to generate three-dimensional tumor representations has improvedand accurate tumor volume calculations are nowfeasible, although automated measurement tech-niques remain elusive. Nonetheless, changes in tu-mor volume, particularly with extensive multifocalsites of bulky lymphoma, may be an important vari-able to correlate with FDG-PET response. It seemsoverly simplistic to assume that all patients whobecome FDG negative after 2 cycles of therapy,even in the presence of large residual masses, willbe uniformly free of disease progression or relapse.The ability to provide other criteria for response todevelop a multivariant array of imaging criteriashould allow us to best identify those patients trulymanifesting a good response to chemotherapy,without overlooking those patients in whom moreaggressive treatment is mandated.In the past, MR imaging of the thoracic and
abdominal cavity has been limited by motion arti-fact and long examination times. However, withincreasing availability of faster MR imaging scan-ning techniques and respiratory and cardiac gat-ing capabilities, a more routine role of MR imagingnuclear/cytoplasm ratios,most forms of lymphoma
entation with cough led to discovery of an anterior medi-isteiumt a
Guillerman et al792Fig. 27. A 16-year-old boy with stage IIA HL. Initial presastinal mass, for which a broad differential diagnosis exPET scan show an FDG-avid mass that abuts the pericard(not shown) sequences showed that the mass was noexcised, confirming the diagnosis of HL.that have been studied have high signal intensity(ie, restricted diffusion) on diffusion-weighted MRimages.95,96 In one study, diffusion-weighted MRimaging matched FDG-PET/CT findings in 94% ofthe lymph node regions studied.117 Furthermore,changes in diffusion characteristics may providean additional means of evaluating residual nodalmasses, because nodal apparent diffusion coeffi-cient has been shown to increase followingsuccessful chemotherapy.118 The use of whole-body MR imaging with diffusion-weighted imagingwith background signal suppression sequenceshas also been shown to provide better tissuecontrast in detecting malignant nodal involvementcompared with conventional MR imaging se-quences.119 As these techniques are incorporatedinto the evaluation of pediatric lymphoma patients,it seems likely that changes in tumor characteris-tics as manifested by changes in diffusion orchanges in enhancement may provide additionalsurrogates of response to help further developa response assessment profile. Whole-body MRimaging with diffusion-weighted imaging mayalso serve as a more sensitive method to rapidlyevaluate leukemic infiltration of the bone marrowfor therapeutic response to cytotoxic chemo-therapy.120 However, widespread interindividualvariation and restricted diffusion as a normald. Chest CT, T2-weighted chest MR imaging, and FDG-, consistent with neoplasm. Gated cardiac MR imagingdherent to pericardium. The mass was subsequentlyfinding in the pelvis and spine of children limit thespecificity of this technique, raising the risk offalse-positive interpretations.121
SUMMARY
As the most common childhood malignancy,leukemia is frequently encountered as an under-lying condition in subjects of pediatric imagingstudies. The most frequent indication for imagingof childrenwith leukemia is to evaluate for complica-tions of treatment. Occasionally, imaging findingssuggest a previously unsuspected diagnosis ofleukemia, particularly in children with nonspecificmusculoskeletal complaints or unexplained fever.There is no current routine role of imaging in riskstratification, therapy response assessment, or re-lapse surveillance for childhood leukemia.The use of imaging in guiding diagnostic
procedures, risk stratification, therapy responseassessment, and relapse surveillance in childhoodlymphoma has evolved in the last 20 to 30 years.From a time when nearly all patients with lym-phoma were surgically staged to a time whennearly all patients have multiple imaging studies,each of which provides complimentary informa-tion, current lymphoma management requires theintegration of imaging at all phases of treatment.
6. GaynonPS,Angiolillo AL,CarrollWL, et al. Long-term
results of theChildrens CancerGroup studies for chi-
ldhood acute lymphoblastic leukemia 19832002:
Leukemia and Lymphoma 793a Childrens Oncology Group Report. Leukemia
2010;24:28597.
7. Smith MA, Seibel NL, Altekruse SF, et al. Outcomes
for children and adolescents with cancer: chal-
lenges for the twenty-first century. J Clin Oncol
2010;28:262534.
8. Creutzig U, Reinhardt D. Current controversies:
which patients with acute myeloid leukaemia
should receive a bone marrow transplantation?A
European view. Br J Haematol 2002;118:36577.
9. Lange BJ, Smith FO, Feusner J, et al. Outcomes in
CCG2961, a childrens oncology group phase 3
trial for untreated pediatric acute myeloid leukemia:
a report from the childrens oncology group. BloodCurrent approaches should include a combinationof anatomic and functional imaging techniques topredict which patients will benefit from less toxictreatment regimens and which patients will requireaugmented therapy. Patient-specific and disease-specific imaging biomarkers to provide specificindicators of disease activity are needed to guidethe evolution from risk-adapted therapy toresponse-based therapy. The ongoing challengeis to optimize available imaging techniques anddevelop a reproducible set of validated biomarkersand image-processing tools to best accomplishthese goals.
REFERENCES
1. Smith MA, Ries LAG, Gurney JG, et al. Leukemia.
In: Ries LA, Smith MA, Gurney JG, editors. Cancer
incidence and survival among children and adoles-
cents: United States SEER Program 19751995.
Bethesda (MD): National Cancer Institute; 1999.
p. 1734.
2. Greaves M. In utero origins of childhood
leukaemia. Early Hum Dev 2005;81:1239.
3. Altekruse SF, Kosary CL, Krapcho M, et al. SEER
cancerstatistics review, 19752007,NationalCancer
Institute. Bethesda (MD), based on November 2009
SEER data submission, posted to the SEER Web
site, 2010. Available at: http://seer.cancer.gov/csr/
1975_2007/. Accessed September 7, 2010.
4. Swerdlow SH, Campo E, Harris NL, et al. WHO
classification of tumours of haematopoietic and
lymphoid tissues. 4th edition. Lyon (France): Inter-
national Agency for Research on Cancer; 2008.
5. Dainiak N. Hematologic consequences of expo-
sure to ionizing radiation. Exp Hematol 2002;30:
51328.2008;111:104453.10. Siegel MJ, Shackelford GD, McAlister WH. Pleural
thickening.Anunusual featureofchildhood leukemia.
Radiology 1981;138:3679.
11. Abbas AA, Baker DL, Felimban SK, et al. Musculo-
skeletal and radiological manifestations of child-
hood acute leukaemia: a clinical review. Haema
2004;7:44855.
12. Sinigaglia R, Gigante C, Bisinella G, et al. Musculo-
skeletal manifestations in pediatric acute leukemia.
J Pediatr Orthop 2008;28:208.
13. Hann IM, Gupta S, Palmer MK, et al. The prognostic
significance of radiological and symptomatic bone
involvement in childhood acute lymphoblastic
leukaemia. Med Pediatr Oncol 1979;6:515.
14. Melhem RE, Saber TJ. Erosion of the medial cortex
of the proximal humerus. A sign of leukemia on the
chest radiograph. Radiology 1980;137:779.
15. Bernard EJ, Nicholls WD, Howman-Giles RB, et al.
Patterns of abnormality on bone scans in acute
childhood leukemia. J Nucl Med 1998;39:19836.
16. Shalaby-Rana E, Majd M. (99m)Tc-MDP scinti-
graphic findings in children with leukemia: value
of early and delayed whole-body imaging. J Nucl
Med 2001;42:87883.
17. Clausen N, Gotze H, Pedersen A, et al. Skeletal
scintigraphy and radiography at onset of acute
lymphocytic leukemia in children. Med Pediatr On-
col 1983;11:2916.
18. Moulopoulos LA, Dimopoulos MA. Magnetic reso-
nance imaging of the bone marrow in hematologic
malignancies. Blood 1997;90:212747.
19. Moore SG, Gooding CA, Brasch RC, et al. Bone
marrow in childrenwith acute lymphocytic leukemia:
MR relaxation times. Radiology 1986;160:23740.
20. Babyn PS, Ranson M, McCarville ME. Normal bone
marrow: signal characteristics and fatty conver-
sion. Magn Reson Imaging Clin N Am 1998;6:
47395.
21. Ruzal-Shapiro C, Berdon WE, Cohen MD, et al. MR
imaging of diffuse bonemarrow replacement in pedi-
atricpatientswithcancer.Radiology1991;181:5879.
22. Truong TH, Beyene J, Hitzler J, et al. Features at
presentation predict children with acute lympho-
blastic leukemia at low risk for tumor lysis syndrome.
Cancer 2007;110:18329.
23. Niemeyer CM, Arico M, Basso G, et al. Chronic
myelomonocytic leukemia in childhood: a retro-
spective analysis of 110 cases. European Working
Group on Myelodysplastic Syndromes in Child-
hood (EWOG-MDS). Blood 1997;89:353443.
24. Murray JC, Dorfman SR, Brandt ML, et al. Renal
venous thrombosis complicating acute myeloid
leukemia with hyperleukocytosis. J Pediatr Hematol
Oncol 1996;18:32730.
25. Hilmes MA, Dillman JR, Mody RJ, et al. Pediatric
renal leukemia: spectrum of CT imaging findings.Pediatr Radiol 2008;38:42430.
Guillerman et al79426. Sato A, Imaizumi M, Chikaoka S, et al. Acute renal
failure due to leukemic cell infiltration followed by
relapse at multiple extramedullary sites in a child
with acute lymphoblastic leukemia. LeukLymphoma
2004;45:8258.
27. Hayek M, Srinivasan A. Acute lymphoblastic
leukemia presenting with lactic acidosis and renal
tubular dysfunction. J Pediatr Hematol Oncol 2003;
25:48890.
28. Rausch DR, Norton KI, Glass RB, et al. Infantile
leukemia presenting with cholestasis secondary
to massive pancreatic infiltration. Pediatr Radiol
2002;32:3601.
29. Jankovic M, Zanetto F, Conter V, et al. Cranial
computed tomography findings in children with
acute lymphoblastic leukemia at diagnosis. Am J
Pediatr Hematol Oncol 1989;11:3279.
30. Vazquez E, Lucaya J, Castellote A, et al. Neuroi-
maging in pediatric leukemia and lymphoma:
differential diagnosis. Radiographics 2002;22:
141128.
31. Ulu EM, Tore HG, Bayrak A, et al. MRI of central ner-
vous system abnormalities in childhood leukemia.
Diagn Interv Radiol 2009;15:8692.
32. Shackelford GD, Bloomberg G, McAlister WH. The
value of roentgenography in differentiating aplastic
anemia from leukemia masquerading as aplastic
anemia. Am J Roentgenol Radium Ther Nucl Med
1972;116:6514.
33. Kai T, Ishii E, Matsuzaki A, et al. Clinical and prog-
nostic implications of bone lesions in childhood
leukemia at diagnosis. Leuk Lymphoma 1996;23:
11923.
34. Guillerman RP. Normal and abnormal bone marrow.
In: Slovis T, editor. Caffeys pediatric diagnostic
imaging. 11th edition. Philadelphia: Elsevier; 2008.
p. 297096.
35. Bulas RB, Laine FJ, Das Narla L. Bilateral orbital
granulocytic sarcoma (chloroma) preceding the
blast phase of acute myelogenous leukemia: CT
findings. Pediatr Radiol 1995;25:4889.
36. Dusenbery KE, Howells WB, Arthur DC, et al. Extra-
medullary leukemia in children with newly diag-
nosed acute myeloid leukemia: a report from the
Childrens Cancer Group. J Pediatr Hematol Oncol
2003;25:7608.
37. Schultz KR, Pullen DJ, Sather HN, et al. Risk-
and response-based classification of childhood B-
precursoracute lymphoblastic leukemia:acombined
analysis of prognostic markers from the Pediatric
Oncology Group (POG) and Childrens Cancer
Group (CCG). Blood 2007;109:92635.
38. Creutzig U, Zimmermann M, Ritter J, et al. Defini-
tion of a standard-risk group in children with
AML. Br J Haematol 1999;104:6309.
39. Masera G, Carnelli V, Ferrari M, et al. Prognosticsignificance of radiological bone involvement inchildhood acute lymphoblastic leukaemia. Arch
Dis Child 1977;52:5303.
40. Heinrich SD, Gallagher D, Warrior R, et al. The
prognostic significance of the skeletal manifesta-
tions of acute lymphoblastic leukemia of childhood.
J Pediatr Orthop 1994;14:10511.
41. DAngelo P, Mura R, Rizzari C, et al. Prognostic
value of nephromegaly at diagnosis of childhood
acute lymphoblastic leukemia. Acta Haematol
1995;94:849.
42. Yetgin S, Olgar S, Aras T, et al. Evaluation of kidney
damage in patients with acute lymphoblastic leu-
kemia in long-term follow-up: value of renal scan.
Am J Hematol 2004;77:1329.
43. Attarbaschi A, Mann G, Dworzak M, et al. Medias-
tinal mass in childhood T-cell acute lymphoblastic
leukemia: significance and therapy response.
Med Pediatr Oncol 2002;39:55865.
44. Vande Berg BC, Lecouvet FE, Michaux L, et al.
Magnetic resonance imaging of the bone marrow
in hematological malignancies. Eur Radiol 1998;8:
133544.
45. Fletcher BD, Wall JE, Hanna SL. Effect of hemato-
poietic growth factors on MR images of bone
marrow in children undergoing chemotherapy.
Radiology 1993;189:74551.
46. EmyPY,LevinTL,ShethSS,etal. Ironoverload in retic-
uloendothelial systems of pediatric oncology patients
who have undergone transfusions: MR observations.
AJR Am J Roentgenol 1997;168:10115.
47. Benz-Bohm G, Gross-Fengels W, Bohndorf K, et al.
MRI of the knee region in leukemic children. Part II.
Follow up: responder, non-responder, relapse. Pe-
diatr Radiol 1990;20:2726.
48. Gaynon PS, Qu RP, Chappell RJ, et al. Survival
after relapse in childhood acute lymphoblastic
leukemia: impact of site and time to first relapse
the Childrens Cancer Group experience. Cancer
1998;82:138795.
49. Webb DK. Management of relapsed acute myeloid
leukaemia. Br J Haematol 1999;106:8519.
50. Jensen KE, Thomsen C, Henriksen O, et al.
Changes in T1 relaxation processes in the bone
marrow following treatment in children with acute
lymphoblastic leukemia. A magnetic resonance
imaging study. Pediatr Radiol 1990;20:4648.
51. Kan JH, Hernanz-Schulman M, Frangoul HA, et al.
MRI diagnosis of bone marrow relapse in children
with ALL. Pediatr Radiol 2008;38:7681.
52. Rubnitz JE, Hijiya N, Zhou Y, et al. Lack of benefit of
early detection of relapse after completion of
therapy for acute lymphoblastic leukemia. Pediatr
Blood Cancer 2005;44:13841.
53. Trigg ME, Steinherz PG, Chappell R, et al. Early
testicular biopsy in males with acute lymphoblastic
leukemia: lack of impact on subsequent event-freesurvival. J Pediatr Hematol Oncol 2000;22:2733.
Leukemia and Lymphoma 79554. Reiter A, Ferrando AA. Malignant lymphomas
and lymphadenopathies. In: Orkin SH, Fisher DE,
LookAT, et al, editors.Oncologyof infancyandchild-
hood. Philadelphia: Elsevier; 2009. p. 417508.
55. Hodgson DC, Hudson MM, Constine LS. Pediatric
Hodgkin lymphoma: maximizing efficacy and mini-
mizing toxicity. SeminRadiatOncol2007;17:23042.
56. Jaffe ES, Harris NL, Stein H, et al. Pathology and
genetics of tumours of hematopoietic and lymphoid
tissues. World Health Organization Classification of
Tumours of Haemtopoietic and Lymphoid Tissues.
Lyon (France): IARC Press; 2001.
57. Claviez A, Tiemann M, Luders H, et al. Impact of
latent Epstein-Barr virus infection onoutcome in chil-
dren and adolescents with Hodgkins