Embed Size (px)
DESCRIPTION
plexi
Citation preview

34 Indian Journal of Oral Sciences Vol. 6 Issue 1 Jan-Apr 2015
Introduction
The ameloblastoma is a benign odontogenic tumor of epithelial origin, which is thought to represent 10% of all tumors of the jaw bones.[1] The name “ameloblastoma” implies a resemblance to cells of the enamel-forming organ.[2] This lesion was first designated as an “Adamantinoma” by Malassez in 1885, while the term ameloblastoma was coined by Ivy and Churchill in 1930.[3]
There are three different clinico-radiographic types: The conventional solid/multicystic intra-osseous ameloblastoma, the unicystic ameloblastoma and the peripheral ameloblastoma. In addition, the desmoplastic ameloblastoma is regarded as a fourth subtype of ameloblastoma because of its mixed radiolucent-radiopaque radiographic appearance (resembling a fibro-osseous lesion) and unique histology.[4] These tumor types differ in biological behavior and rate of recurrence. Therefore, each type of ameloblastoma requires different forms of treatment.[5]
Histological ly, ameloblastomas are classified into follicular, plexiform, acanthomatous, granular cell, desmoplastic and basal cell types, with the follicular and plexiform patterns being the most common.[5] Other rare histologic types mentioned include the papilliferous, clear cell and keratoameloblastoma. These variants may exist singly or as a combination of two or more types.[6] However, there is no relationship between the individual patterns and the behavior of the tumor or its prognosis.[4]
This paper reports a distinctive case of an ameloblastoma presenting as a unilocular radiolucency in the angle and ramus region on the right side of the mandible in a 20-year-old female patient, which showed histopathological features of both the acanthomatous and plexiform patterns.
Case Report
A 20-year-old female patient reported to our out-patient department with a chief complaint of swelling in the lower right
Date of Submission: 11-02-2014Date of Acceptance: 10-03-2015
Address for correspondence: Dr. Nigel R Figueiredo, House No. 685, Santerxette, Aldona, Bardez - 403 508, Goa, India. E-mail: [email protected]
ABSTRACT
The ameloblastoma is an odontogenic tumor of epithelial origin, which is persistent and locally invasive, and has aggressive but benign growth characteristics. There are three major clinico‑radiographic types: Conventional solid/multicystic intra‑osseous, unicystic and peripheral ameloblastoma, with the conventional solid intra‑osseous type being the most common. Histopathologically, it occurs in six patterns: Plexiform, follicular, acanthomatous, granular cell, basal cell, and desmoplastic types. This report describes a case of an ameloblastoma in the angle and ramus region of the mandible, which radiographically appeared as a unilocular radiolucency mimicking a dentigerous cyst or unicystic ameloblastoma, but showed features of both the acanthomatous and plexiform patterns of a conventional/solid ameloblastoma on histopathological analysis.
Ameloblastoma of the acanthomatous and plexiform type in the mandible presenting as a unilocular radiolucency
Nigel R Figueiredo, Manoj Meena, Ajit D Dinkar, Manisha KhorateDepartment of Oral Medicine and Radiology, Goa Dental College and Hospital, Bambolim, Goa, India
Case Report
Key words: Acanthomatous, ameloblastoma, plexiform, unilocular
Access this article online
Website: www.indjos.com
DOI: 10.4103/0976-6944.154608
Quick Response Code:
[Downloaded free from http://www.indjos.com on Wednesday, October 21, 2015, IP: 202.43.93.11]
Figueiredo, et al.: Ameloblastoma of the acanthomatous and plexiform type in the mandible
35Indian Journal of Oral Sciences Vol. 6 Issue 1 Jan-Apr 2015
posterior region since 2 months. The patient gave a history of progressive increase in the size of the swelling with occasional pain in the area. On extra-oral examination, a diffuse swelling was seen over the right side of the face, over the posterior body and angle of the mandible, extending superiorly to involve the ramus and inferiorly to the posterior submandibular region, measuring around 5 × 4 cm [Figure 1].
The overlying skin was normal with no evidence of any discharge. On palpation, the swelling was firm in consistency, tender, non-pulsatile and non-compressible, with no local rise in temperature. Intra-oral examination revealed a diffuse swelling in the right retromolar region and buccal vestibule in region of 47-48 [Figure 2]. A single, subcentimetric, firm and mobile right submandibular lymph node was palpable.
Panoramic radiography showed a large, well-defined unilocular radiolucency with thin corticated borders in the right angle of mandible, extending superiorly to involve the entire ramus and anteriorly up to the 47 region. The internal structure was completely radiolucent. An impacted developing 48 was seen, which was displaced inferiorly to the angle of mandible [Figure 3].
An incisional biopsy was carried out, which showed strands of odontogenic epithelium proliferating irregularly in a sparse connective tissue stroma. A cystic lining was seen, which was flattened in one area and 7-10 layers thick in other areas. There was palisading of basal cells with reverse polarity, hyperchromasia, and presence of stellate-reticulum like cells. The findings of the incisional biopsy, correlated with the clinico-radiographic findings, were suggestive of a dentigerous cyst with secondary changes of an ameloblastoma.
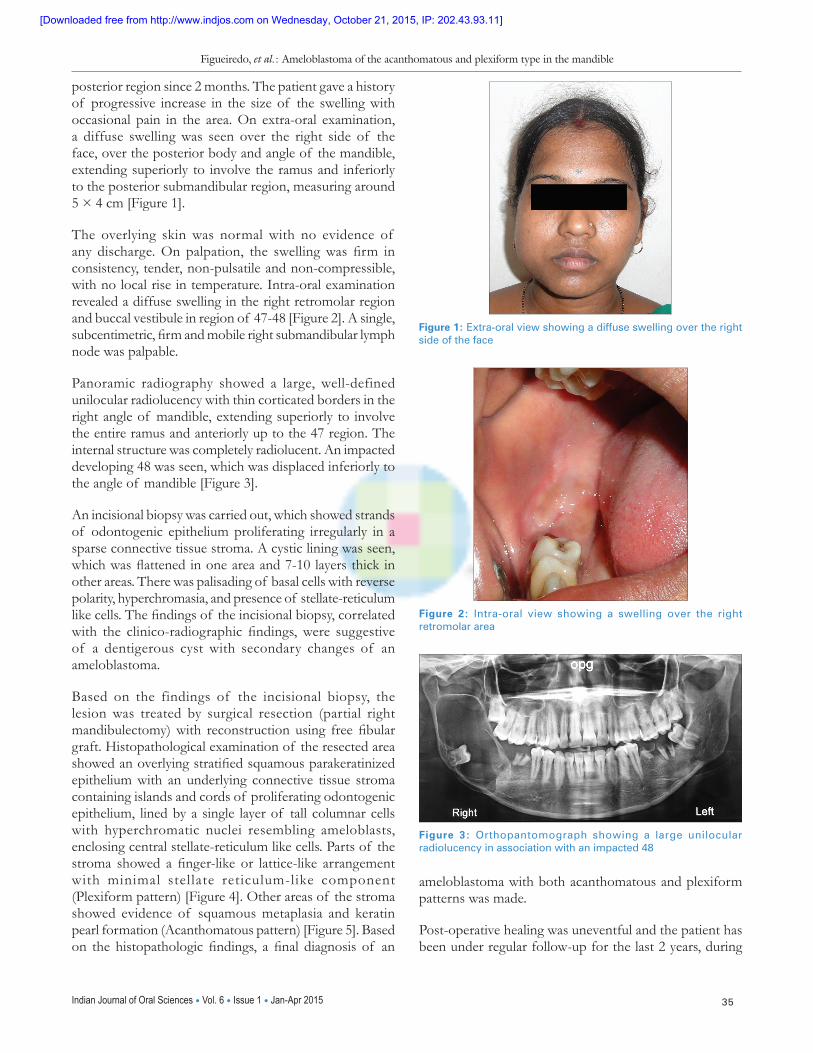
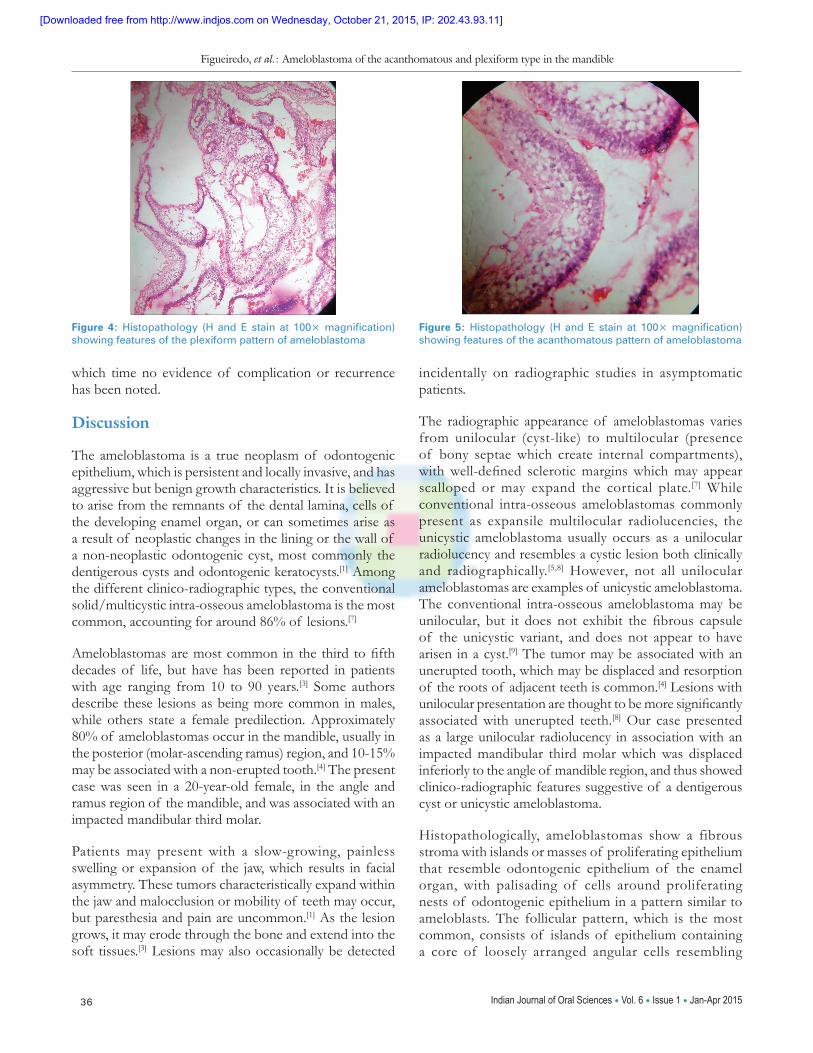
Based on the findings of the incisional biopsy, the lesion was treated by surgical resection (partial right mandibulectomy) with reconstruction using free fibular graft. Histopathological examination of the resected area showed an overlying stratified squamous parakeratinized epithelium with an underlying connective tissue stroma containing islands and cords of proliferating odontogenic epithelium, lined by a single layer of tall columnar cells with hyperchromatic nuclei resembling ameloblasts, enclosing central stellate-reticulum like cells. Parts of the stroma showed a finger-like or lattice-like arrangement with minimal stellate reticulum-like component (Plexiform pattern) [Figure 4]. Other areas of the stroma showed evidence of squamous metaplasia and keratin pearl formation (Acanthomatous pattern) [Figure 5]. Based on the histopathologic findings, a final diagnosis of an
ameloblastoma with both acanthomatous and plexiform patterns was made.
Post-operative healing was uneventful and the patient has been under regular follow-up for the last 2 years, during
Figure 1: Extra‑oral view showing a diffuse swelling over the right side of the face
Figure 2: Intra‑oral view showing a swelling over the right retromolar area
Figure 3: Orthopantomograph showing a large unilocular radiolucency in association with an impacted 48
[Downloaded free from http://www.indjos.com on Wednesday, October 21, 2015, IP: 202.43.93.11]
Figueiredo, et al.: Ameloblastoma of the acanthomatous and plexiform type in the mandible
36 Indian Journal of Oral Sciences Vol. 6 Issue 1 Jan-Apr 2015
which time no evidence of complication or recurrence has been noted.
Discussion
The ameloblastoma is a true neoplasm of odontogenic epithelium, which is persistent and locally invasive, and has aggressive but benign growth characteristics. It is believed to arise from the remnants of the dental lamina, cells of the developing enamel organ, or can sometimes arise as a result of neoplastic changes in the lining or the wall of a non-neoplastic odontogenic cyst, most commonly the dentigerous cysts and odontogenic keratocysts.[1] Among the different clinico-radiographic types, the conventional solid/multicystic intra-osseous ameloblastoma is the most common, accounting for around 86% of lesions.[7]
Ameloblastomas are most common in the third to fifth decades of life, but have has been reported in patients with age ranging from 10 to 90 years.[3] Some authors describe these lesions as being more common in males, while others state a female predilection. Approximately 80% of ameloblastomas occur in the mandible, usually in the posterior (molar-ascending ramus) region, and 10-15% may be associated with a non-erupted tooth.[4] The present case was seen in a 20-year-old female, in the angle and ramus region of the mandible, and was associated with an impacted mandibular third molar.
Patients may present with a slow-growing, painless swelling or expansion of the jaw, which results in facial asymmetry. These tumors characteristically expand within the jaw and malocclusion or mobility of teeth may occur, but paresthesia and pain are uncommon.[1] As the lesion grows, it may erode through the bone and extend into the soft tissues.[3] Lesions may also occasionally be detected
incidentally on radiographic studies in asymptomatic patients.
The radiographic appearance of ameloblastomas varies from unilocular (cyst-like) to multilocular (presence of bony septae which create internal compartments), with well-defined sclerotic margins which may appear scalloped or may expand the cortical plate.[7] While conventional intra-osseous ameloblastomas commonly present as expansile multilocular radiolucencies, the unicystic ameloblastoma usually occurs as a unilocular radiolucency and resembles a cystic lesion both clinically and radiographically.[5,8] However, not all unilocular ameloblastomas are examples of unicystic ameloblastoma. The conventional intra-osseous ameloblastoma may be unilocular, but it does not exhibit the fibrous capsule of the unicystic variant, and does not appear to have arisen in a cyst.[9] The tumor may be associated with an unerupted tooth, which may be displaced and resorption of the roots of adjacent teeth is common.[4] Lesions with unilocular presentation are thought to be more significantly associated with unerupted teeth.[8] Our case presented as a large unilocular radiolucency in association with an impacted mandibular third molar which was displaced inferiorly to the angle of mandible region, and thus showed clinico-radiographic features suggestive of a dentigerous cyst or unicystic ameloblastoma.
Histopathologically, ameloblastomas show a fibrous stroma with islands or masses of proliferating epithelium that resemble odontogenic epithelium of the enamel organ, with palisading of cells around proliferating nests of odontogenic epithelium in a pattern similar to ameloblasts. The follicular pattern, which is the most common, consists of islands of epithelium containing a core of loosely arranged angular cells resembling
Figure 4: Histopathology (H and E stain at 100× magnification) showing features of the plexiform pattern of ameloblastoma
Figure 5: Histopathology (H and E stain at 100× magnification) showing features of the acanthomatous pattern of ameloblastoma
[Downloaded free from http://www.indjos.com on Wednesday, October 21, 2015, IP: 202.43.93.11]

Figueiredo, et al.: Ameloblastoma of the acanthomatous and plexiform type in the mandible
37Indian Journal of Oral Sciences Vol. 6 Issue 1 Jan-Apr 2015
stellate-reticulum, surrounded by a single layer of tall columnar cells with nuclei showing reverse polarity. The plexiform pattern shows long anastomosing cords or sheets of odontogenic epithelium, while the acanthomatous type shows extensive squamous metaplasia and keratin formation in the central portion of the islands.[5] The present case resembled a dentigerous cyst/unicystic ameloblastoma radiographically, but the histopathological analysis showed separate areas of both the plexiform and acanthomatous patterns of a conventional solid intra-osseous ameloblastoma.
Although ameloblastomas may arise from dentigerous cysts by ameloblastic transformation of the cyst lining, this remains a point of controversy. Two reasons for this include: Firstly, an ameloblastoma may involve an unerupted tooth, particularly a third molar at the angle of mandible and may thus radiographically resemble a dentigerous cyst; secondly, a biopsy of an ameloblastoma may often be taken from an expanded locule lined by a thin layer of epithelium, and may histologically appear as a dentigerous cyst—when the tumor is entirely removed, a diagnosis of ameloblastoma is made, which may be misinterpreted as arising from a dentigerous cyst.[10] This was evident in the present case where the findings of an incisional biopsy, correlated with the radiographic findings, suggested a dentigerous cyst with secondary changes of an ameloblastoma, while histopathological examination following removal of the entire tumor revealed features suggestive of an ameloblastoma.
The treatment of ameloblastomas depends on the clinico-radiologic variant, anatomic location and clinical behavior of the tumor. The age and the general state of health of the patient are also important factors.[11] Conventional ameloblastomas are locally invasive with a high rate of recurrence if not adequately removed. Surgical treatment of ameloblastoma may be either conservative or radical. The conservative approach is usually carried out for unicystic/small unilocular lesions and includes enucleation, curettage or surgical excision with peripheral osteotomy.[12] Radical treatment measures are advocated for large lesions, which include marginal or segmental resection of the diseased section of the jaw and inclusion of about 1 or 2 cm of apparently uninvolved bone.[6] Supra-periosteal resection of the bone is necessary when extensive thinning or perforation of the cortical plates is noted. In the mandible, either full-thickness resection or resection with preservation of the lower border is done, while resection of maxillary lesions is defined by the anatomic extension of the excision in partial or total maxillectomy.[12] Therapeutic irradiation should not be used in the treatment of ameloblastomas as it can
lead to osteonecrosis and has a potential for inducing post-radiation malignancies.[9]
Conventional solid intra-osseous ameloblastomas have a well-documented tendency for recurrence, especially if treated by conservative procedures like curettage. This is because the lesion characteristically infiltrates between the trabeculae of cancellous bone of the jaws, and thus extends beyond its radiographically apparent margin.[13] Because of their slow growth, recurrence of these lesions may be long-delayed, and hence a long-term post-operative follow up is essential for all patients.
Acknowledgment
Dr. Anita Spadigam, Professor and Head, and Dr. Anita Dhupar, Asst. Professor, Department of Oral and Maxillofacial Pathology, Goa Dental College and Hospital, Bambolim, Goa - India, for the histopathological analysis and photographs.
References
1. Kashyap B, Reddy PS, Desai RS. Plexiform ameloblastoma mimicking a periapical lesion: A diagnostic dilemma. J Conserv Dent 2012;15:84‑6.
2. Kim SG, Jang HS. Ameloblastoma: A clinical, radiographic, and histopathologic analysis of 71 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:649‑53.
3. More C, Tailor M, Patel HJ, Asrani M, Thakkar K, Adalja C. Radiographic analysis of ameloblastoma: A retrospective study. Indian J Dent Res 2012;23:698.
4. Bachmann AM, Linfesty RL. Ameloblastoma, solid/multicystic type. Head Neck Pathol 2009;3:307‑9.
5. Lee SK, Kim YS. Current concepts and occurrence of epithelial odontogenic tumors: I. Ameloblastoma and adenomatoid odontogenic tumor. Korean J Pathol 2013;47:191‑202.
6. Gruica B, Stauffer E, Buser D, Bornstein M. Ameloblastoma of the follicular, plexiform, and acanthomatous type in the maxillary sinus: A case report. Quintessence Int 2003;34:311‑14.
7. White SC, Pharoah MJ, editors. Oral radiology: Principles and interpretation. 5th ed. St. Louis, Missouri: Mosby (Elsevier); 2004. p. 419‑22.
8. MacDonald‑Jankowski DS, Yeung R, Lee KM, Li TK. Ameloblastoma in the Hong Kong Chinese. Part 2: Systematic review and radiological presentation. Dentomaxillofac Radiol 2004;33:141‑51.
9. Pilch BZ, editor. Head and Neck Surgical Pathology. Philadelphia: Lippincott Williams and Wilkins; 2001. p. 212‑4.
10. Shear M, editor. Cysts of the Oral Regions. 3rd ed. Oxford: Butterworth‑Heinemann Limited; 1992. p. 92‑3.
11. Gümgüm S, Hoşgören B. Clinical and radiologic behaviour of ameloblastoma in 4 cases. J Can Dent Assoc 2005;71:481‑4.
12. Rastogi V, Pandilwar PK, Maitra S. Ameloblastoma: An evidence based study. J Maxillofac Oral Surg 2010;9:173‑7.
13. Gardner DG. Some current concepts on the pathology of ameloblastomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:660‑9.
How to cite this article: Figueiredo NR, Meena M, Dinkar AD, Khorate M. Ameloblastoma of the acanthomatous and plexiform type in the mandible presenting as a unilocular radiolucency. Indian J Oral Sci 2015;6:34-7.Source of Support: Nil, Conflict of Interest: None declared
[Downloaded free from http://www.indjos.com on Wednesday, October 21, 2015, IP: 202.43.93.11]





























