Embed Size (px)
Citation preview

Ameloblastoma of the follicular, plexiform, andacanthomatous type in the maxillary sinus: A case reportBoris Gruica, Dr med dentVEdouartj Slauffer, Dr medVDaniel Buser, Prof Dr med denWMichael Bornstein, Dr med dent"
The amelcblastoma is a benign odontogenic tumor of epitheiiai origin, Histcpathoiogicaiiy, it occurs in sixpatterns: piexitorm, follicular, acanthomatous, granular celi, basai cell, and desmopiastic type. This reportpresents a rare case of an ameloblastoma in the maxillary sinus tbat consists of tbree types: foilicuiar,plexiform, and acantbomatcus. Ttie diagnostic procedure, surgicai therapy, and follow-up findings are de-scribed and discussed, (Quintessence Int 2003:34:31 J-314)
Key words: amelobiastoma, maxillary sinus, odontogenic tumor
The ameloblastotïia is a benign but locally invasiveneoplasm derived from odontogenic epithelium. It
is the most common odontogenic tumor but, even so,in most series only accounts for approximately P/o ofall oral tumors.' Usually the ameloblastomas are diag-nosed in the founh and fifth decades of life, except theunicystic type, which is usually found in the secondand third decades. There is no significant race or sexpredilection. Over 80% of ameloblastomas occur inthe mandible and the remainder in the maxilla. In themandible, about 70% are in the molar region and theascending ramus, 20% in the premolar region, and10% in the incisor region.̂
Clinically, three subtypes of ameloblastomas are rec-ognized: (1) policystic (common); (2) unicystic; and (3)peripheral. The last one is confined to the gingiva or
'Senior Leclurei, Department of Oral Surgery and Stomatology, School ofDental Medicine, University of Beine, Berne, Switzerland.
^Associate Professoi, Institute for Pathology, University of Berne, Berne,
Switzerland,
=Head and Chairman, Department of Oral S j rge iy and Stomatology,Seriool of Denial Medicine, Llniversity of Berne, Berne, Switzerland.
'Senior Lecturer, Department of Orai Surgery and Stornatology, School ofDental Medicine, Llniversity of Berne, Berne, Switzerland.
Reprint requests: Dr Michael Bornstein, Department of Oral Surgery andStomatology, Freiburgsfrasse 7, CH-3010 Berne, Switzeiland. E-mail:nircfiael.bornstein@zmk,unibe.ch
alveolar mucosa and does not invade the underlyingbone. It is a very rarely encoitntered type.̂ Radio-graphically, the typical picture of the policysticameloblastoma is of a multilocular destruction andgives the radiograph a "soap bubble" appearance,''Unicystic lesions are the most commonly seen anatomicform in Western children and are virtually only presentin the mandible (more than 90% of cases).^ Histo-logically there are two main patterns: follicular andplexiform. Other variations are acanthomatous. granu-lar cell, basal cell, and desmopiastic ameloblastomas,which are less common. Two additional rare histologietypes mentioned are the keratoameloblastoma and thepapilliferous keratoameloblastoma,^
CASE REPORT
In August 2000, a 75-year-old man was referred to theDepartment of Oral Surgery and Stomatology,University of Berne, for evaluation and further treat-ment of a swelling on the right maxilla. The patient re-ported that the swelling had been present for 9months, bled from time to time, and was painless. Thechief complaint was the misfit of the maxillary den-ture. He denied any significant medical history, had noknown drug allergies, and was not taking any medi-cine. He had been smoking cigars, three to five perday, for 40 years.
Quintessence International 311

• Gruica étal
Fig 1 Intraoial photograpin of Itie patient showingan exophytic, red-bluish soft-tissue neoplasm in thevestibule of the right maxilla
Fig 2 Panoramic radiograph showng a -fiKeci '^rliolucent-fadiopaqje lesionwith indistinct borders involving the right maxillary tuoerosity and the maxillarysinus.
Fig 3 Computer tomography soan showing a large expansile le-sion of the right maxilla involving the maxillary sinus and causingerosion of the lateral wall of the nose
Fig 4 Suigical specimen. Overview ot the ameloblastoma; Nestsand strands ot odontogenic epithelium (Hematoxylin-eosin stain;original magnification x2.5).
Extraoral examination revealed no abnormal find-ings in the cervical and submandibular lymph nodes.Intraoral examination sbowed a bard swelling of thebuccal-cortical bone of tbe right maxilla in tbe firstand second molar region, whicb was obliterating tbevestibule. Tbe middle of the swelling presented a per-foration, 15 X 20 mm, witb an exopbytic, red-bluishsoft-tissue neoplasm, wbieb immediately started tobleed after palpation (Fig 1). A panoramic radiographsbowed a mixed radiolucent-radiopaque lesion witbindistinct borders involving tbe right maxillarytuberosity and tbe maxillary sinus {Fig 2).
Two incisional biopsies were performed under localanestbesia on the border and the center of the lesion.Specimens from these materials showed well-differen-tiated palisaded cells around the periphery of nests,strands, and network of focally budding epitheliumwith small areas of squamous differentiation.
A computed tomography (CT) scan was ordered,which sbowed a large expansile lesion of the rigbt
maxilla involving tbe maxillary sinus and causing ero-sion of tbe lateral wall of tbe nose. The orbital floorwas intact (Fig 3).
The clinical and radiologie findings led to tbe finaldiagnosis of ameloblastoma. Therefore surgical man-agement was considered and the patient was referredto the Division of Craniomaxillofacial and Skull BaseSurgery, Department of Facial Plastic and Recon-structive Surgery at the University Hospitai in Berne.On October 4, 2000, a partial maxillectomy and a si-tnultaneous reeonstruetion using tbe tabula externawere performed after induction of general anesthesia.Postsurgical histopathologic examination revealed thesame histomorphology as in the incisional biopsies:nests and strands of odontogenic epitbelium and po-larization of cells around tbe proliferating nests witha sltTiilar pattern as enamel organ (Fig 4}, small andlarger central population of variably spaced stellate-shaped cells with focal cystic degeneration (foUicularpattern, Fig 5), anastomosing strands and cords of
312 Volume34, •1, 2003
• Gruica et ai
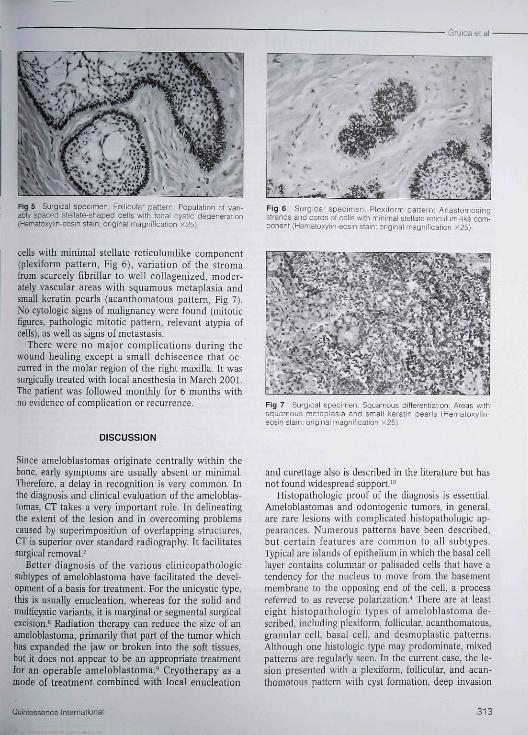
WxvT ' ' ' ^¿. -y-Ty 'vaf •• ' _̂ ' • -Fig 5 Surgicai specimen. Foiiicuiar pattern PopLJlatio-i ul vai,-abiy spaced sie i late-shaped ceils with tocal cystic degeneration(iHematcxylin-eosin stain; original magnitication x25).
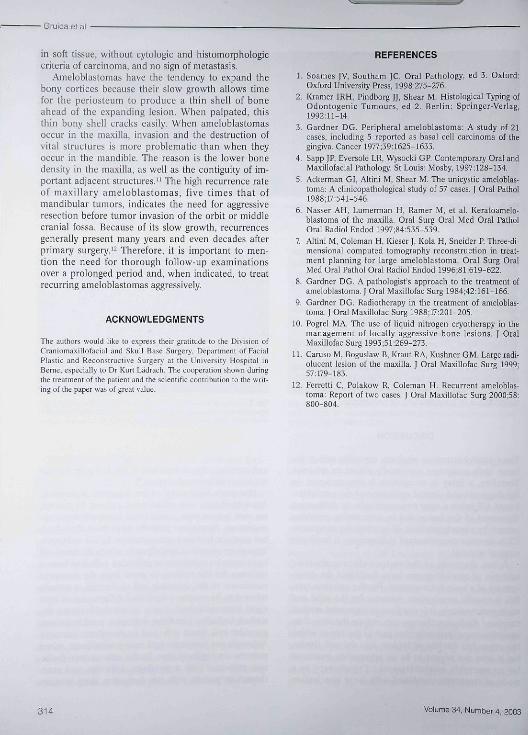
cells with minimal stellate reticuiumlike component(plexiform pattern. Fig 6), variation of the stromafrom scarcely fibrillar to well collagenized, moder-ately vascular areas with squamous metaplasia andsmall keratin pearls {acanthomatous pattern- Fig 7}.No cytologie signs of malignancy were found (miloticfigures, pathologic mitotic pattern, relevant atypia ofcells}, as well as signs of metastasis.
There were no major complications during thewound healing except a small dehiscence that oc-curred in the molar region of the right maxilla. It wassurgically treated with local anesthesia in March 2001.The patient was followed monthly for 6 months withno evidence of compficafion or recurrence.
DISCUSSION
Since ameloblastomas originate centrally within thebone, early symptoms are usually absent or minimal.Therefore, a delay in recognition is very common. Inthe diagnosis and clinical evaluation of the ameloblas-totnas, CT takes a very important role. In delineatingthe extent of the lesion and in overcoming problemscaused by superimposition of overlapping structures,CT is superior over standard radiography. It facilitatessurgicai removal.'
Better diagnosis of the various clinicopathologicsubtypes of ameloblastoma have facilitated the devel-opment of a basis for treatment. For the unicystic type,this is usually enucleation, whereas for the solid andmulticystic variants, it is marginal or segmental surgicalexcision.̂ Radiation therapy can reduce the size of anameloblastoma, primarily that part of the tumor whichhas expanded the jaw or broken into the soft tissues,but it does not appear to be an appropriate treatmentfor an operable ameloblastoma.^ Cryotherapy as amode of treatment combined with local enucleation
Fig 6 Surgicai specimen Piexiform pattern: Anastomosingstrands and cords of ceils with minimai steilate reticulum-ljke com-ponent (liematc>:yiin-eosin slain; original magnification X25).
Fig 7 Surgicai specimen Squamous öitferentiation; Areas withsquamous metapiasia and smaii keratin pearls (Hematcxylin-ecsir stain; onginal magnificaticn x25).
and curettage also is described in the literature but basnot found widespread support."*
Histopathologic proof of the diagnosis is essential.Ameloblastomas and odontogenic tumors, in general,are rare lesions with complicated histopathologic ap-pearances. Numerous patterns have been described,but certain features are common to all subtypes.Typical are islands of epithelium in which the basal celllayer contains columnar or palisaded cells that have atendency for the nucleus to move fi^om the basementmembrane to the opposing end of the cell, a processreferred to as reverse polarization."* There are at leasteight histopathologic types of ameloblastoma de-scribed, including plexiform, follicular, acanthomatous,granular cell, basal cell, and desmoplastlc patterns.Although one histologie type may predominate, mixedpatterns are regularly seen- In the current case, the le-sion presented with a plexiform, follicular, and acan-thomatous pattern witb cyst formation, deep invasion
Quintessence International 313
• Gruica et al
in soft tissue, witbout cytologie and bistomorpbologiccriteria of carcinoma, and no sign of metastasis,
Ameloblastomas have tbe tendency to expand thebony cortices because tbeir slow growtb allows timefor tbe periosteum to produce a tbin shell of boneabead of tbe expanding lesion, Wben palpated, tbistbin bony sbel! cracks easily, Wben ameloblastomasoceur in tbe maxilla, invasion and tbe destruction ofvital structures is more problematic tban wben tbeyoccur in the mandible, Tbe reason is tbe lower bonedensity in tbe maxilla, as well as tbe contiguity of im-portant adjacent structures." The high recurrence rateof maxillary ameloblastomas, five times that ofmandibular tumors, indicates the need for aggressiveresection before tumor invasion of tbe orbit or middlecranial fossa. Because of its slow growtb, recurrencesgenerally present tnany years and even decades afterprimary surgery,'̂ Therefore, it is important to men-tion tbe need for thorough foiiow-up examinationsover a prolonged period and, wben indicated, to treatrecurring ameloblastomas aggressively.
ACKNOWLEDGMENTS
The authors would like to e\pres,î their gratitude to ttie Division ofCraniomaxiilofaciai and Skull Base Surgery, Department of FacialPlastic and Reconstructive Surgery at the University Hospital inBeme, especially to Dr Kjrt Ladrach, The cooperation shown duringthe treatment of the patieni and the scientific contribution to the writ-ing of the paper wai of great value.
REFERENCES
1, Soames JV, Southam JC, Oral Pattiology, ed 3. Oxford:Oxford Utiiversity Press, 1998:275-276.
2, Iiramer lRH, Pindborg JJ, Shear M. Histological Typing ofOdontogenic Tumours, ed 2, Berlin: Springer-Vsrlag,1992:11-14,
3, Gardner DG, Peripheral anieloblastoma: A study of 21cases, including 5 reported as basal cell carcinoma of thegingiva. Cancer 1977;39:1625-1633,
4, Sapp ]P, Eversole LR, Wysocki GP, Contemporary Oral andMaxillofacial Pathology, St Louis: Mosby, 1997:128-134,
5, Ackerman GI, Altini M, Shear M, The unicystic ameloblas-toma: A clinicopathological study of 57 cases, | Oral Pathol1988;17:541-546,
6, Nasser AH, Lumertnan H, Ramer M, et al. Keratoamclo-blastoma of the maxilla. Oral Surg Oral Med Oral PatholOral Radioi Endod 1997;84:535-539.
7 Altini M, Colcmati H, Kiescr J, Kola H, Sncider P, Three-di-mensional computed tomography reconstmction in treat-ment planning for large ameloblastoma. Oral Surg OralMed Oral Pathol Oral Radioi Endod 1996;81:619-622,
8. Gardner DG. A pathologist's approach to tbe treatment ofameloblastoma, [ Oral Maxillofac Surg 1984;42:161-166,
9, Gardner DG, Radiotherapy in tbe treatment of ameloblas-toma. I Oral Maxillofac Surg 1988;17:201-205,
10, Pogrel MA, Tbe use of liquid nitrogen cryotberapy in themanagement of locally aggressive bone lesions, J OralMaxillofac Surg 1993;51:269-273,
11, Caniso M, Boguslaw B, Kraut RA, Kushner GM, Large radi-oiucent lesion of the maxilla, J Oral Maxillofac Sttrg 1999;57:179-183.
12, Ferretti C, Polakow R. Coleman H, Recurrent ameloblas-toma: Report of two cases, f Oral Maxillofac Surg 2000;58:
314 Volume 34, Number 4, 2003





























