Embed Size (px)
Citation preview
THE HEARTBREAK KID, NÉ
An age-old tragedy in two parts
Dr Malcolm Davies
Division of Nephrology, Charlotte Maxeke Johannebsurg Academic Hospital
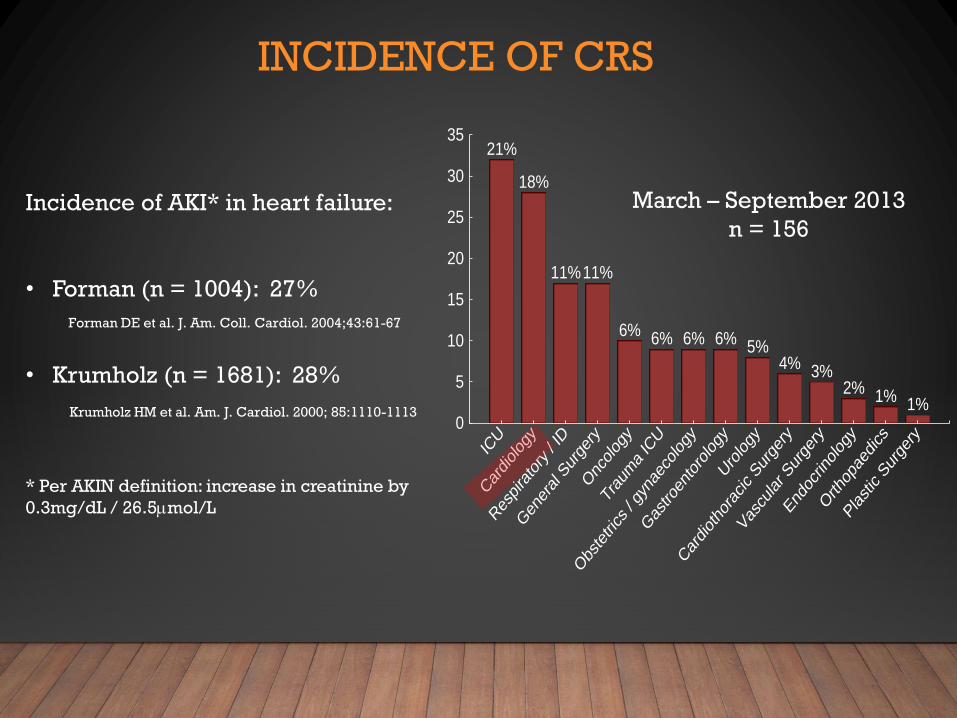
21%
18%
11%11%
6% 6% 6% 6% 5%4% 3%
2% 1% 1%
ICU
Car
diolog
y
Res
pira
tory / ID
Gen
eral S
urge
ry
Onc
olog
y
Trau
ma IC
U
Obs
tetrics
/ gy
naec
olog
y
Gas
troen
toro
logy
Uro
logy
Car
diotho
racic Sur
gery
Vas
cular S
urge
ry
End
ocrin
olog
y
Orth
opae
dics
Plastic S
urge
ry0
5
10
15
20
25
30
35
March – September 2013
n = 156Incidence of AKI* in heart failure:
• Forman (n = 1004): 27%
• Krumholz (n = 1681): 28%
* Per AKIN definition: increase in creatinine by
0.3mg/dL / 26.5mmol/L
INCIDENCE OF CRS
Forman DE et al. J. Am. Coll. Cardiol. 2004;43:61-67
Krumholz HM et al. Am. J. Cardiol. 2000; 85:1110-1113

www.nhlbi.nih.gov/research/reports/2004-cardiorenal
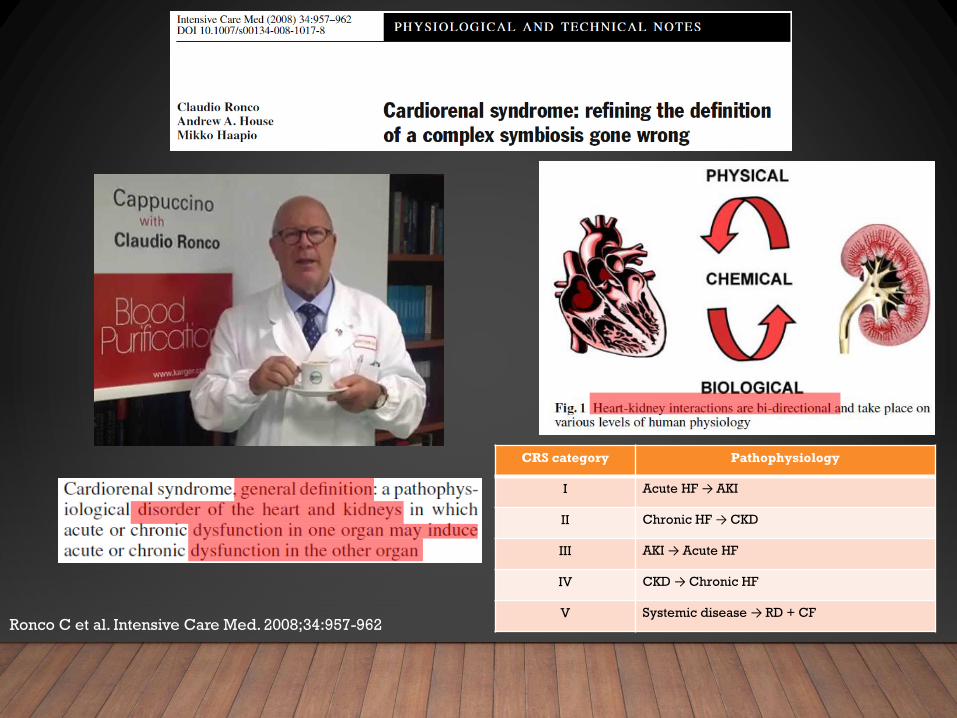
CRS category Pathophysiology
I Acute HF → AKI
II Chronic HF → CKD
III AKI → Acute HF
IV CKD → Chronic HF
V Systemic disease → RD + CFRonco C et al. Intensive Care Med. 2008;34:957-962
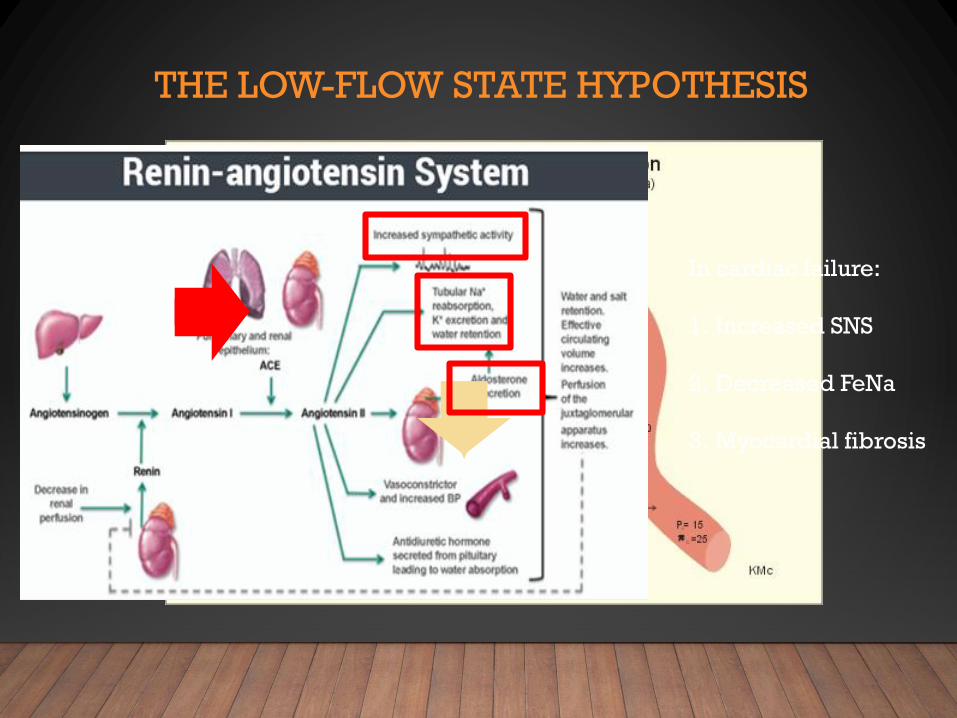
THE LOW-FLOW STATE HYPOTHESIS
In cardiac failure:
1. Increased SNS
2. Decreased FeNa
3. Myocardial fibrosis
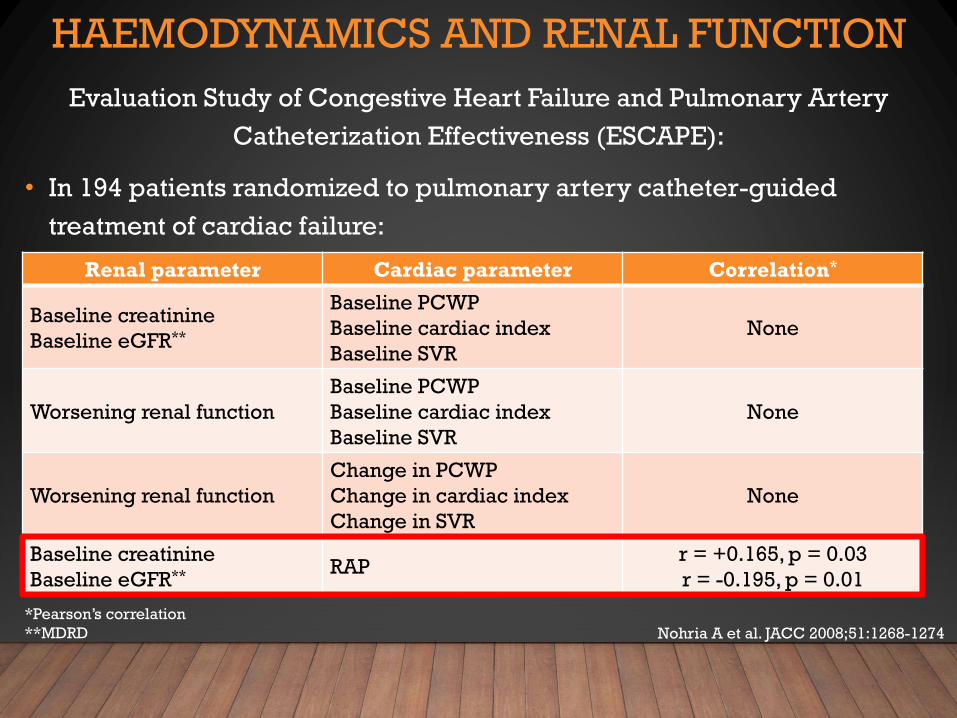
HAEMODYNAMICS AND RENAL FUNCTION
Evaluation Study of Congestive Heart Failure and Pulmonary Artery
Catheterization Effectiveness (ESCAPE):
• In 194 patients randomized to pulmonary artery catheter-guided
treatment of cardiac failure:
Renal parameter Cardiac parameter Correlation*
Baseline creatinine
Baseline eGFR**
Baseline PCWP
Baseline cardiac index
Baseline SVR
None
Worsening renal function
Baseline PCWP
Baseline cardiac index
Baseline SVR
None
Worsening renal function
Change in PCWP
Change in cardiac index
Change in SVR
None
Baseline creatinine
Baseline eGFR** RAPr = +0.165, p = 0.03
r = -0.195, p = 0.01
Nohria A et al. JACC 2008;51:1268-1274
*Pearson’s correlation
**MDRD
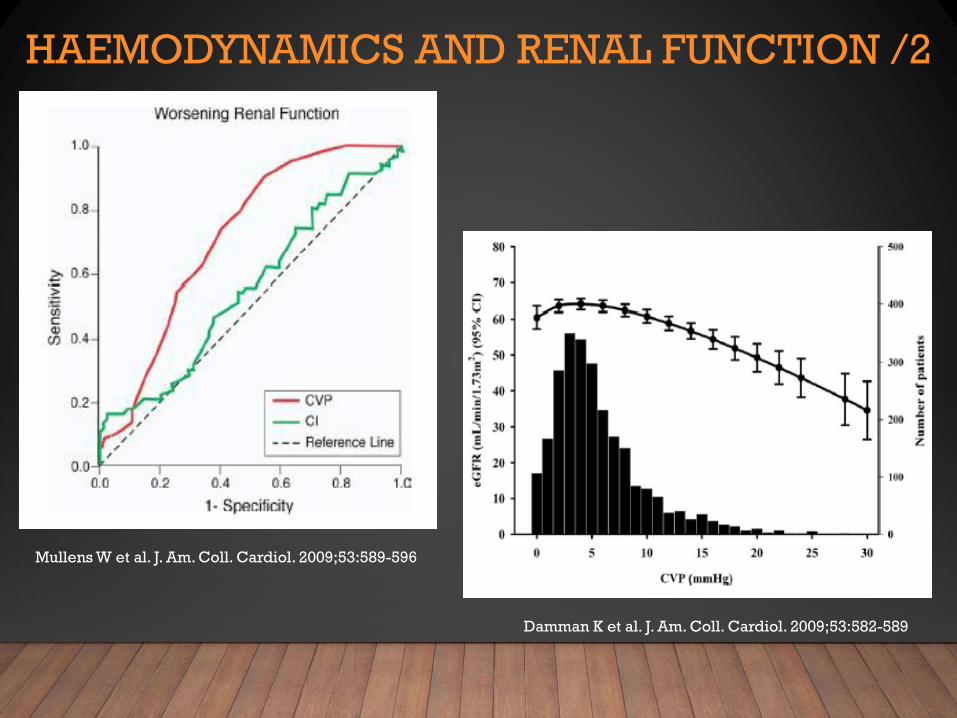
HAEMODYNAMICS AND RENAL FUNCTION /2
Mullens W et al. J. Am. Coll. Cardiol. 2009;53:589-596
Damman K et al. J. Am. Coll. Cardiol. 2009;53:582-589
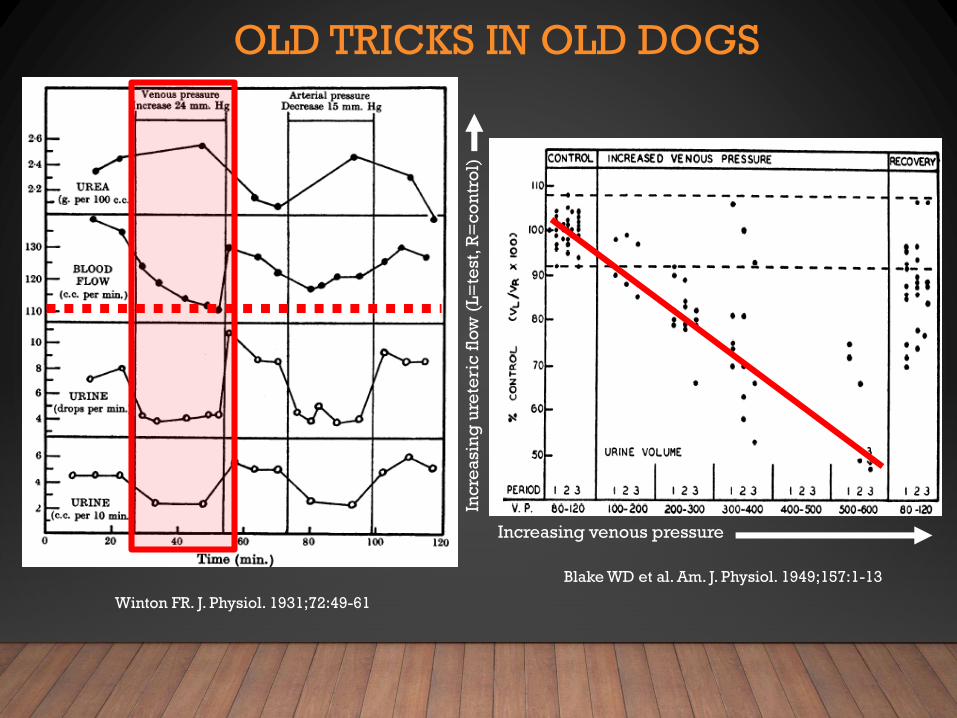
OLD TRICKS IN OLD DOGS
Winton FR. J. Physiol. 1931;72:49-61
Blake WD et al. Am. J. Physiol. 1949;157:1-13
Increasing venous pressure
Inc
rea
sin
g u
rete
ric
flo
w (
L=
test,
R=
co
ntr
ol)
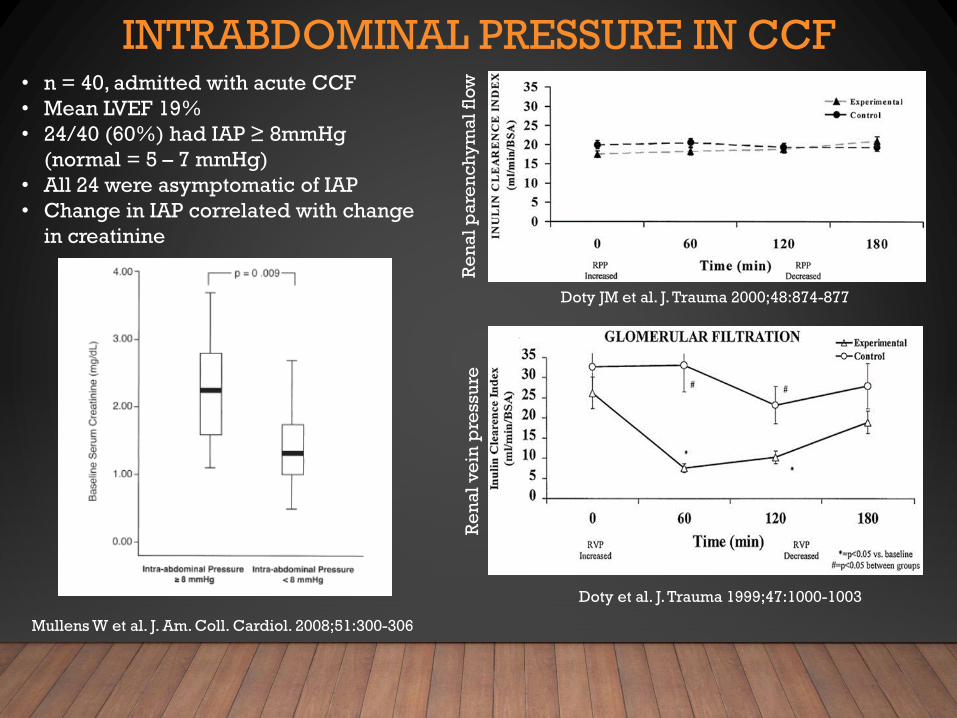
INTRABDOMINAL PRESSURE IN CCF• n = 40, admitted with acute CCF
• Mean LVEF 19%
• 24/40 (60%) had IAP ≥ 8mmHg
(normal = 5 – 7 mmHg)
• All 24 were asymptomatic of IAP
• Change in IAP correlated with change
in creatinine
Mullens W et al. J. Am. Coll. Cardiol. 2008;51:300-306
Doty JM et al. J. Trauma 2000;48:874-877
Doty et al. J. Trauma 1999;47:1000-1003
Re
na
l p
are
nc
hy
ma
l fl
ow
Re
na
l v
ein
pre
ssu
re
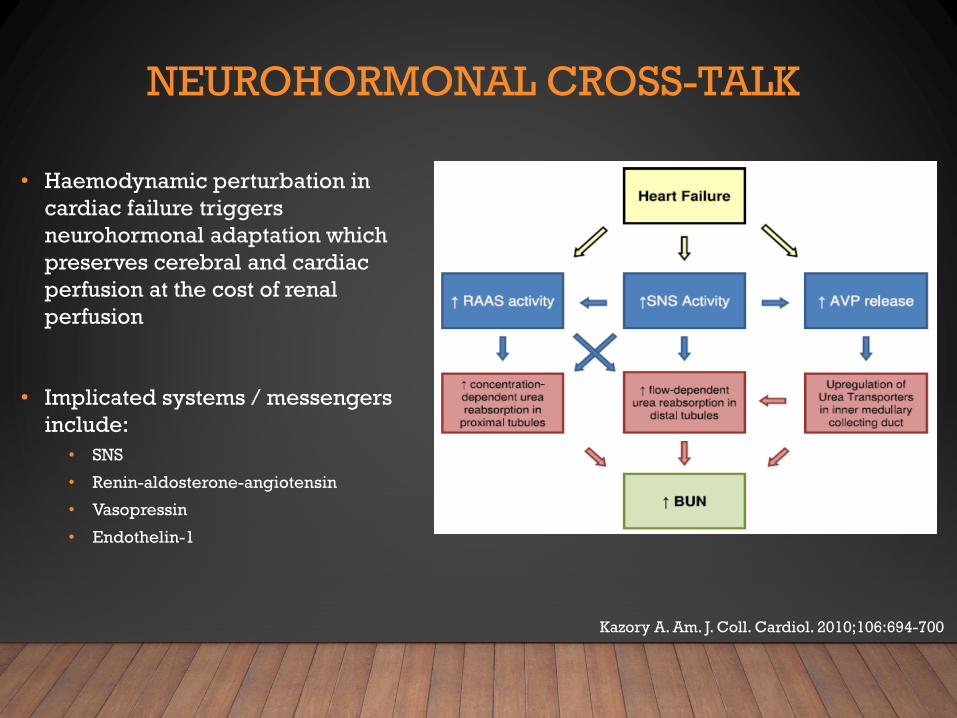
NEUROHORMONAL CROSS-TALK
• Haemodynamic perturbation in
cardiac failure triggers
neurohormonal adaptation which
preserves cerebral and cardiac
perfusion at the cost of renal
perfusion
• Implicated systems / messengers
include:
• SNS
• Renin-aldosterone-angiotensin
• Vasopressin
• Endothelin-1
Kazory A. Am. J. Coll. Cardiol. 2010;106:694-700
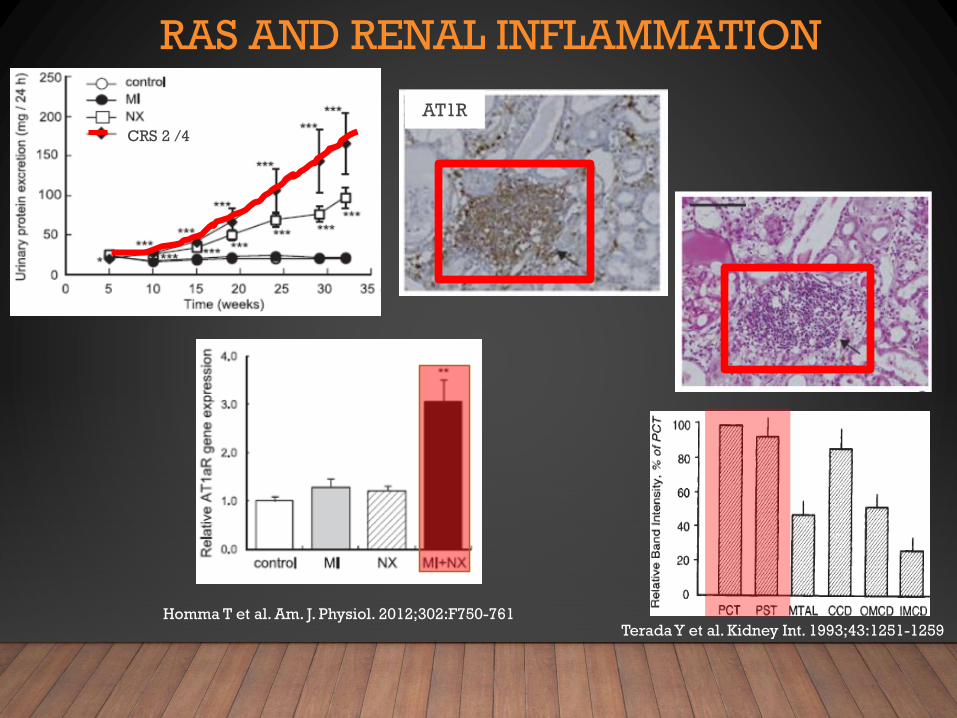
RAS AND RENAL INFLAMMATION
Homma T et al. Am. J. Physiol. 2012;302:F750-761Terada Y et al. Kidney Int. 1993;43:1251-1259
CRS 2 /4
AT1R

RAS AND RENAL INFLAMMATION /2
Li N et al. Clin. Chem. Acta 2010;411:1963-1968
Sham, CD4 AII, CD4
Crowley SD et al. Am. J. Physiol. Renal Physiol. 2008;295:F515-524
Madhur MS et al. Hypertens. 2010;55:500-507
Ruiz-Ortega et al. J. Immunol. 1998;161:430-439
IL-17
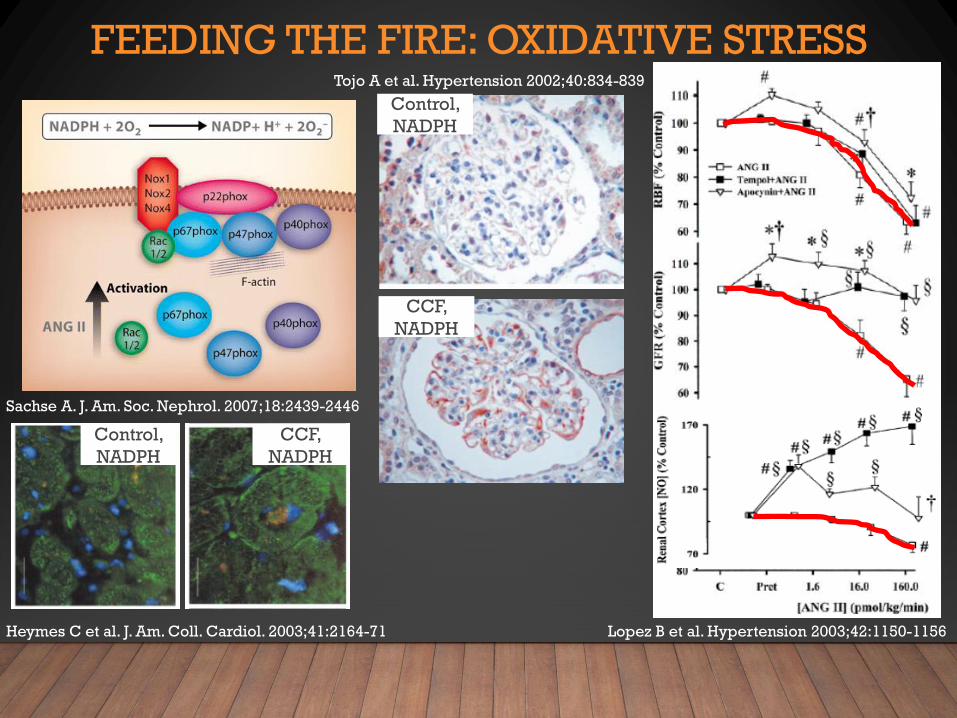
FEEDING THE FIRE: OXIDATIVE STRESS
Sachse A. J. Am. Soc. Nephrol. 2007;18:2439-2446
Lopez B et al. Hypertension 2003;42:1150-1156
Tojo A et al. Hypertension 2002;40:834-839
Heymes C et al. J. Am. Coll. Cardiol. 2003;41:2164-71
Control,
NADPH
CCF,
NADPH
CCF,
NADPH
Control,
NADPH
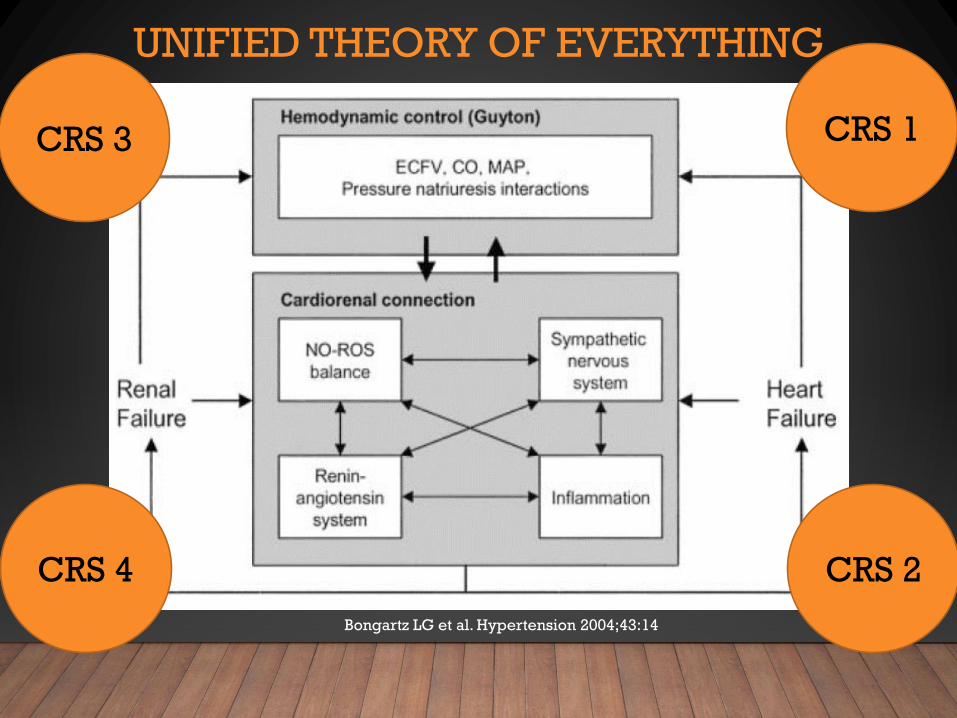
UNIFIED THEORY OF EVERYTHING
Bongartz LG et al. Hypertension 2004;43:14
CRS 1
CRS 2
CRS 3
CRS 4
THERAPY RATIONALES
1. Treat overload:
1. Reduce intra-abdominal and renal venous pressures to improve renal
perfusion
2. Reduce RV dilatation to improve LV filling and forward ejection
3. Improve LV stroke volume and decrease SVR
2. Improve cardiac function:
1. Improve renal perfusion to facilitate diuresis and clearance
3. Block activation of pro-inflammatory / pro-fibrotic
adaptive responses
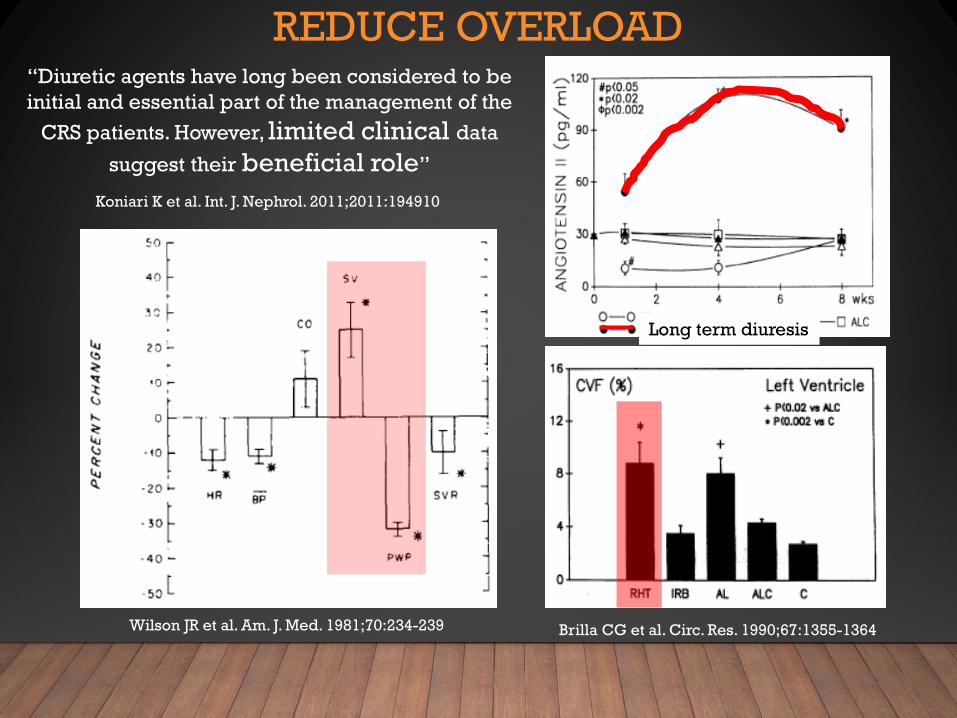
REDUCE OVERLOAD
Wilson JR et al. Am. J. Med. 1981;70:234-239 Brilla CG et al. Circ. Res. 1990;67:1355-1364
“Diuretic agents have long been considered to be
initial and essential part of the management of the
CRS patients. However, limited clinical data
suggest their beneficial role”
Koniari K et al. Int. J. Nephrol. 2011;2011:194910
Long term diuresis
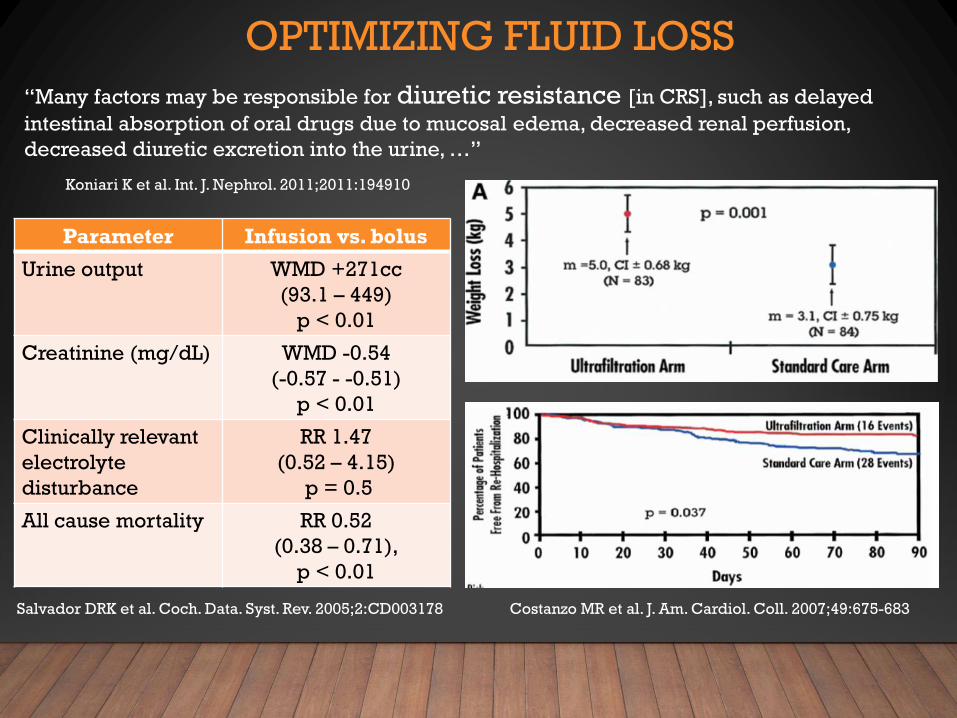
OPTIMIZING FLUID LOSS
“Many factors may be responsible for diuretic resistance [in CRS], such as delayed
intestinal absorption of oral drugs due to mucosal edema, decreased renal perfusion,
decreased diuretic excretion into the urine, …”
Koniari K et al. Int. J. Nephrol. 2011;2011:194910
Parameter Infusion vs. bolus
Urine output WMD +271cc
(93.1 – 449)
p < 0.01
Creatinine (mg/dL) WMD -0.54
(-0.57 - -0.51)
p < 0.01
Clinically relevant
electrolyte
disturbance
RR 1.47
(0.52 – 4.15)
p = 0.5
All cause mortality RR 0.52
(0.38 – 0.71),
p < 0.01
Salvador DRK et al. Coch. Data. Syst. Rev. 2005;2:CD003178 Costanzo MR et al. J. Am. Cardiol. Coll. 2007;49:675-683
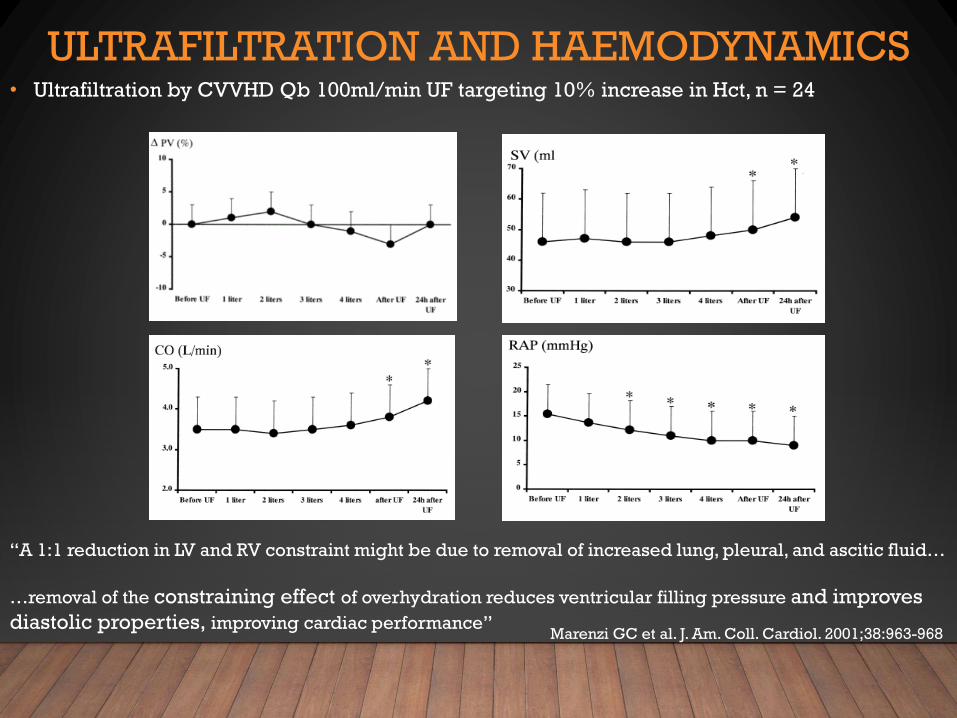
ULTRAFILTRATION AND HAEMODYNAMICS• Ultrafiltration by CVVHD Qb 100ml/min UF targeting 10% increase in Hct, n = 24
“A 1:1 reduction in LV and RV constraint might be due to removal of increased lung, pleural, and ascitic fluid…
…removal of the constraining effect of overhydration reduces ventricular filling pressure and improves
diastolic properties, improving cardiac performance”Marenzi GC et al. J. Am. Coll. Cardiol. 2001;38:963-968
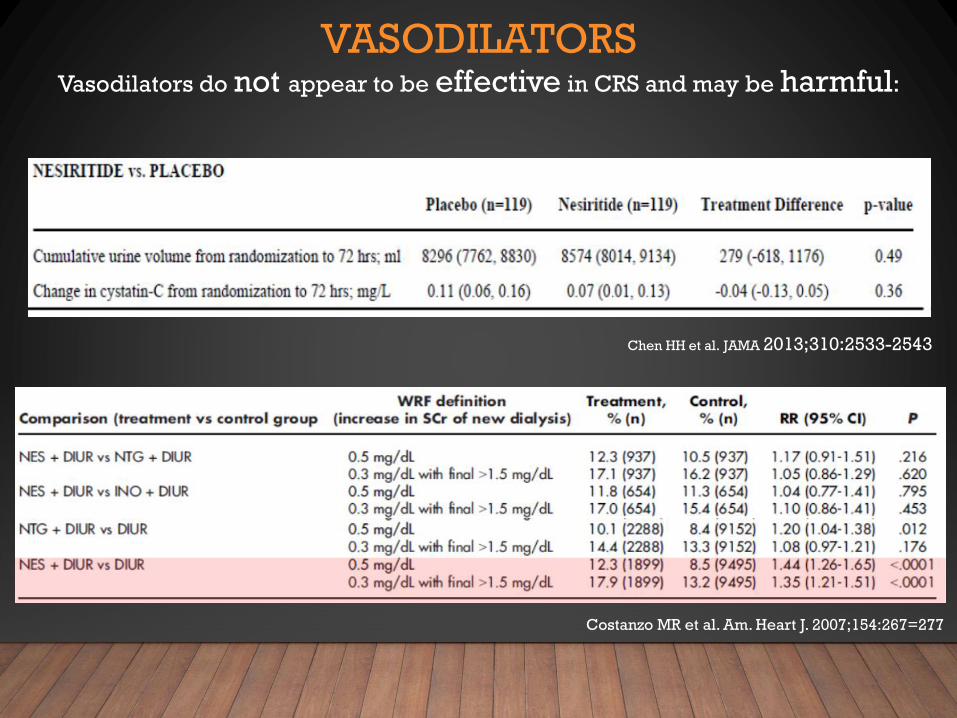
VASODILATORSVasodilators do not appear to be effective in CRS and may be harmful:
Costanzo MR et al. Am. Heart J. 2007;154:267=277
Chen HH et al. JAMA 2013;310:2533-2543
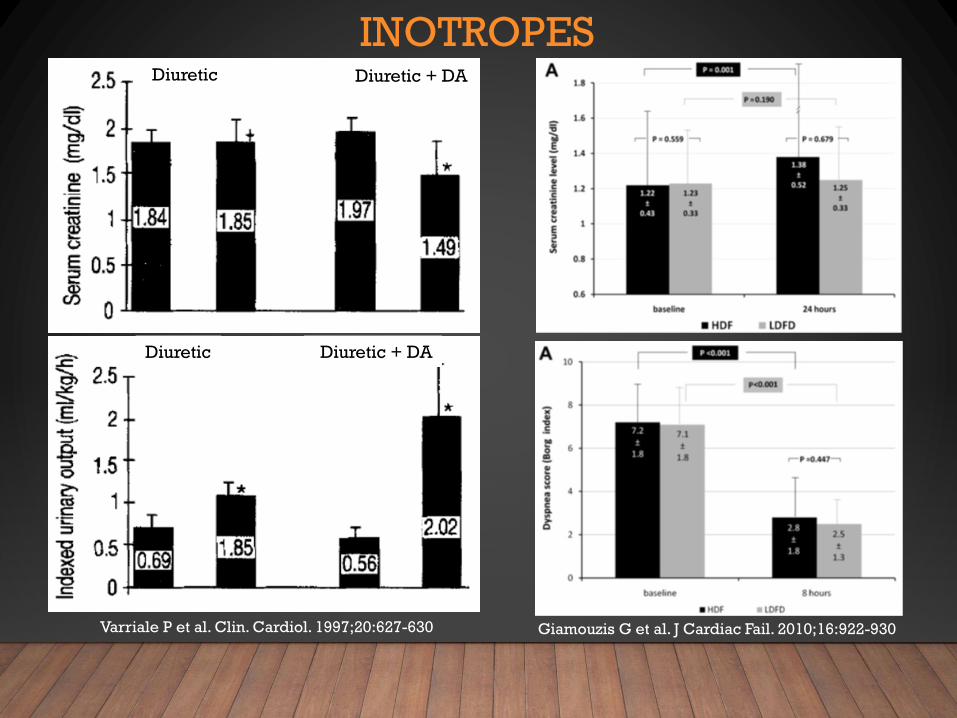
INOTROPESDiuretic
Diuretic
Diuretic + DA
Diuretic + DA
Varriale P et al. Clin. Cardiol. 1997;20:627-630 Giamouzis G et al. J Cardiac Fail. 2010;16:922-930
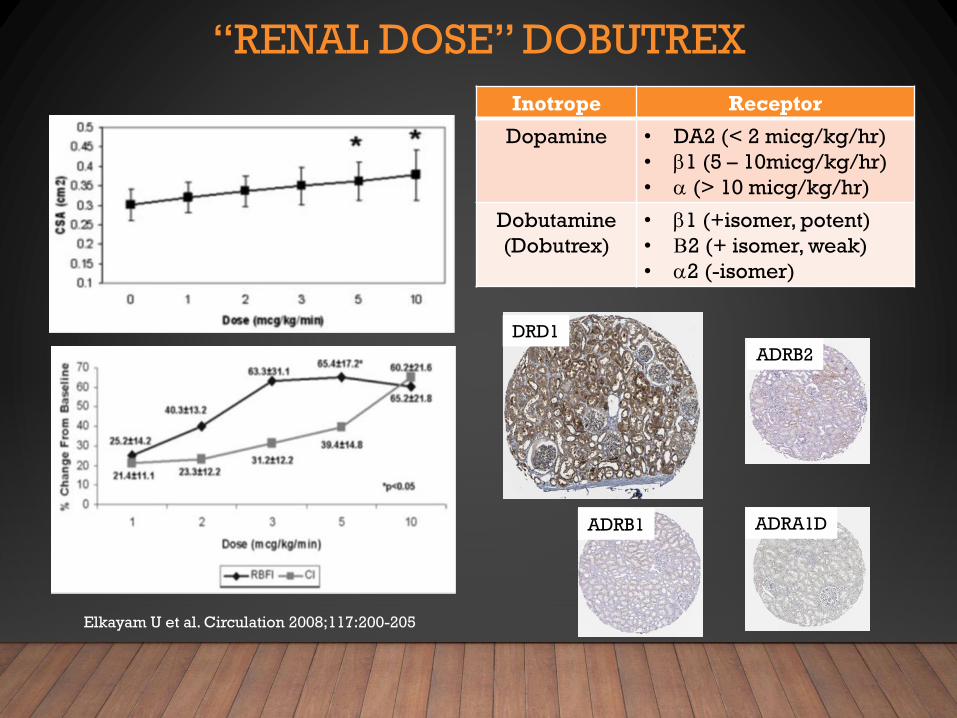
“RENAL DOSE” DOBUTREX
Inotrope Receptor
Dopamine • DA2 (< 2 micg/kg/hr)
• b1 (5 – 10micg/kg/hr)
• a (> 10 micg/kg/hr)
Dobutamine
(Dobutrex)
• b1 (+isomer, potent)
• B2 (+ isomer, weak)
• a2 (-isomer)
DRD1
ADRB2
ADRA1D
Elkayam U et al. Circulation 2008;117:200-205
ADRB1
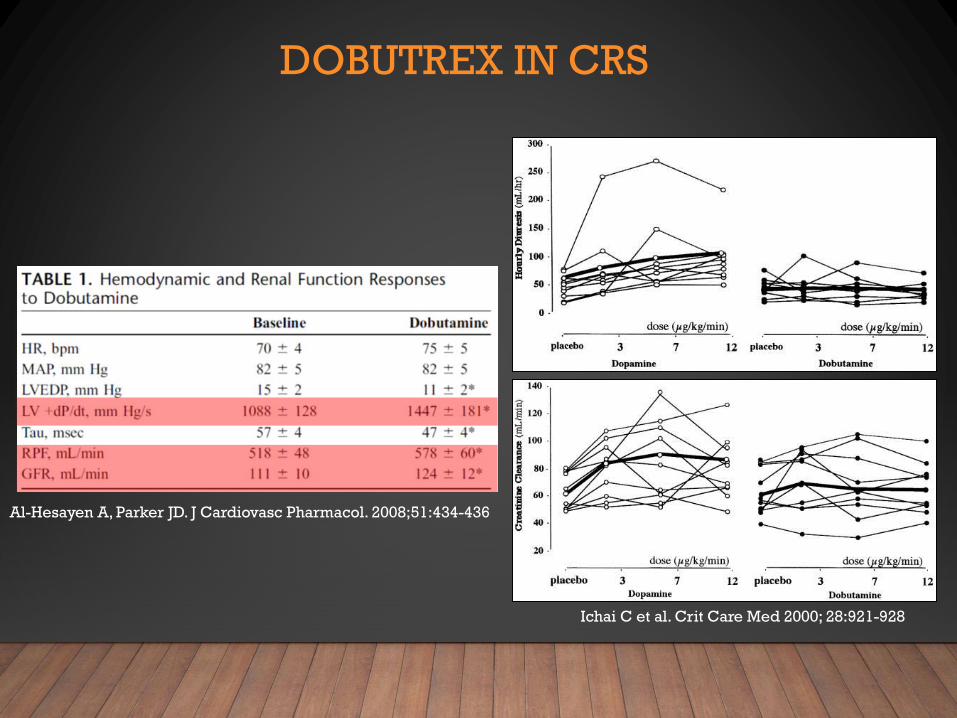
DOBUTREX IN CRS
Al-Hesayen A, Parker JD. J Cardiovasc Pharmacol. 2008;51:434-436
Ichai C et al. Crit Care Med 2000; 28:921-928
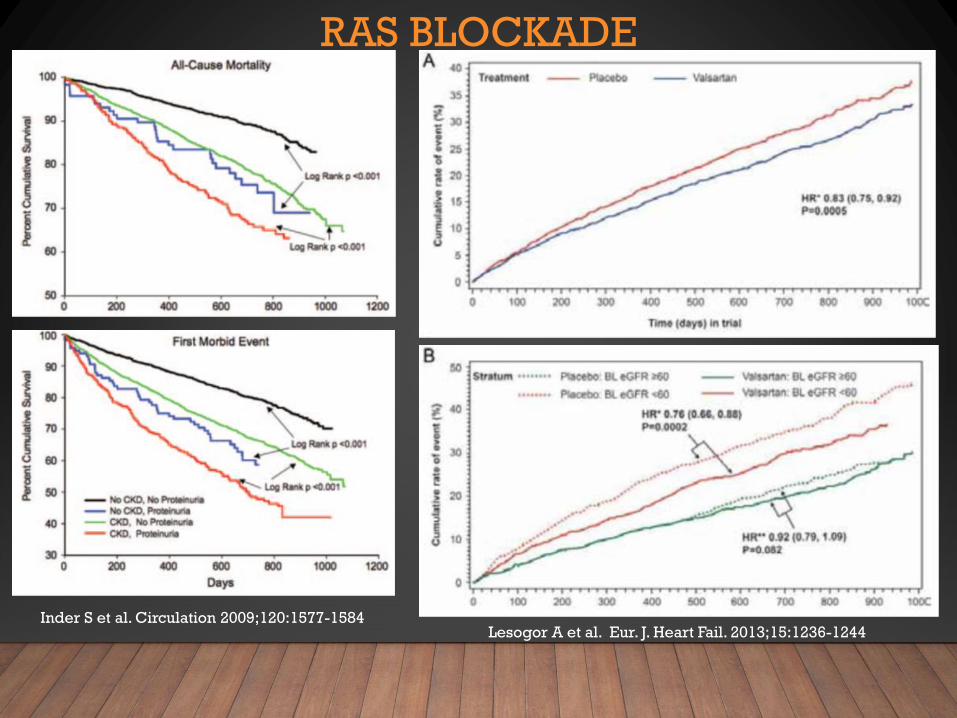
RAS BLOCKADE
Inder S et al. Circulation 2009;120:1577-1584Lesogor A et al. Eur. J. Heart Fail. 2013;15:1236-1244
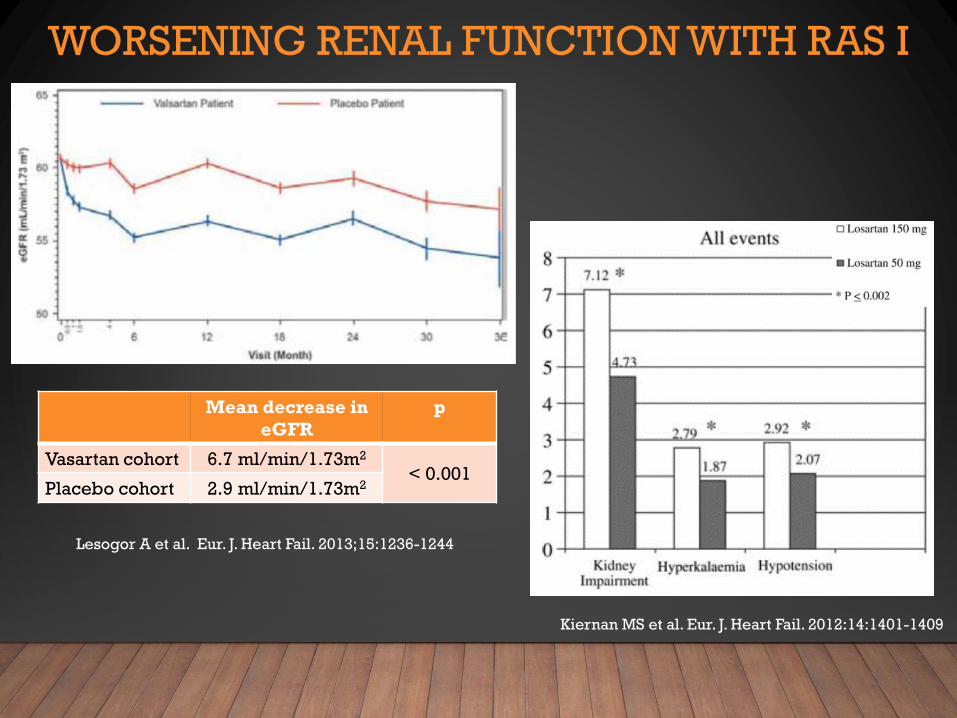
WORSENING RENAL FUNCTION WITH RAS I
Mean decrease in
eGFR
p
Vasartan cohort 6.7 ml/min/1.73m2
< 0.001Placebo cohort 2.9 ml/min/1.73m2
Lesogor A et al. Eur. J. Heart Fail. 2013;15:1236-1244
Kiernan MS et al. Eur. J. Heart Fail. 2012:14:1401-1409
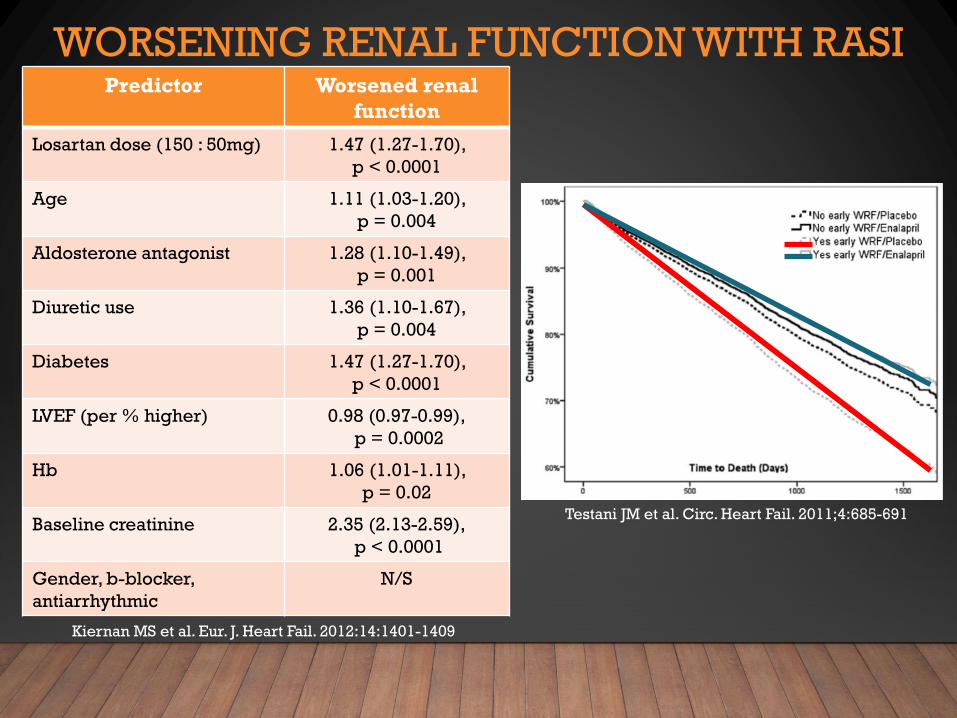
WORSENING RENAL FUNCTION WITH RASI
Kiernan MS et al. Eur. J. Heart Fail. 2012:14:1401-1409
Testani JM et al. Circ. Heart Fail. 2011;4:685-691
Predictor Worsened renal
function
Losartan dose (150 : 50mg) 1.47 (1.27-1.70),
p < 0.0001
Age 1.11 (1.03-1.20),
p = 0.004
Aldosterone antagonist 1.28 (1.10-1.49),
p = 0.001
Diuretic use 1.36 (1.10-1.67),
p = 0.004
Diabetes 1.47 (1.27-1.70),
p < 0.0001
LVEF (per % higher) 0.98 (0.97-0.99),
p = 0.0002
Hb 1.06 (1.01-1.11),
p = 0.02
Baseline creatinine 2.35 (2.13-2.59),
p < 0.0001
Gender, b-blocker,
antiarrhythmic
N/S
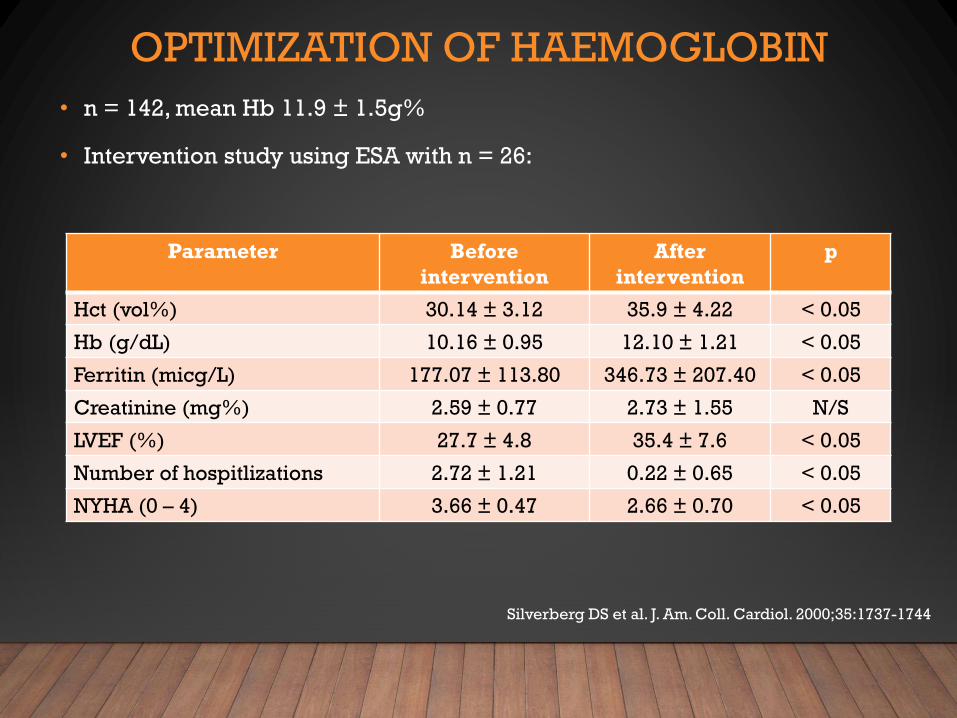
OPTIMIZATION OF HAEMOGLOBIN
• n = 142, mean Hb 11.9 ± 1.5g%
• Intervention study using ESA with n = 26:
Parameter Before
intervention
After
intervention
p
Hct (vol%) 30.14 ± 3.12 35.9 ± 4.22 < 0.05
Hb (g/dL) 10.16 ± 0.95 12.10 ± 1.21 < 0.05
Ferritin (micg/L) 177.07 ± 113.80 346.73 ± 207.40 < 0.05
Creatinine (mg%) 2.59 ± 0.77 2.73 ± 1.55 N/S
LVEF (%) 27.7 ± 4.8 35.4 ± 7.6 < 0.05
Number of hospitlizations 2.72 ± 1.21 0.22 ± 0.65 < 0.05
NYHA (0 – 4) 3.66 ± 0.47 2.66 ± 0.70 < 0.05
Silverberg DS et al. J. Am. Coll. Cardiol. 2000;35:1737-1744
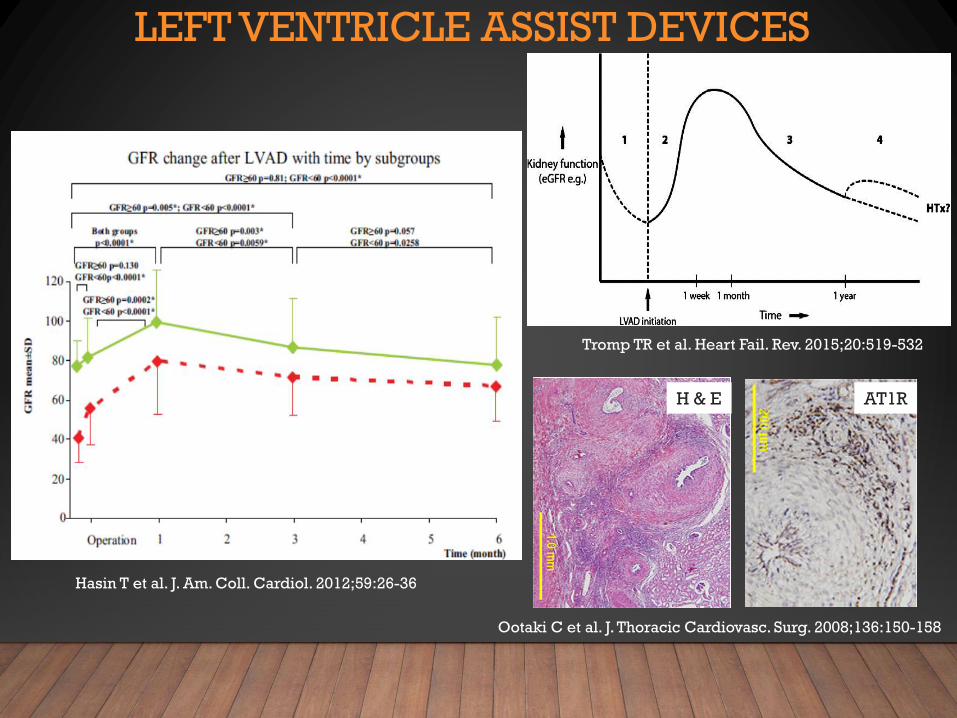
LEFT VENTRICLE ASSIST DEVICES
Tromp TR et al. Heart Fail. Rev. 2015;20:519-532
Hasin T et al. J. Am. Coll. Cardiol. 2012;59:26-36
Ootaki C et al. J. Thoracic Cardiovasc. Surg. 2008;136:150-158
H & E AT1R
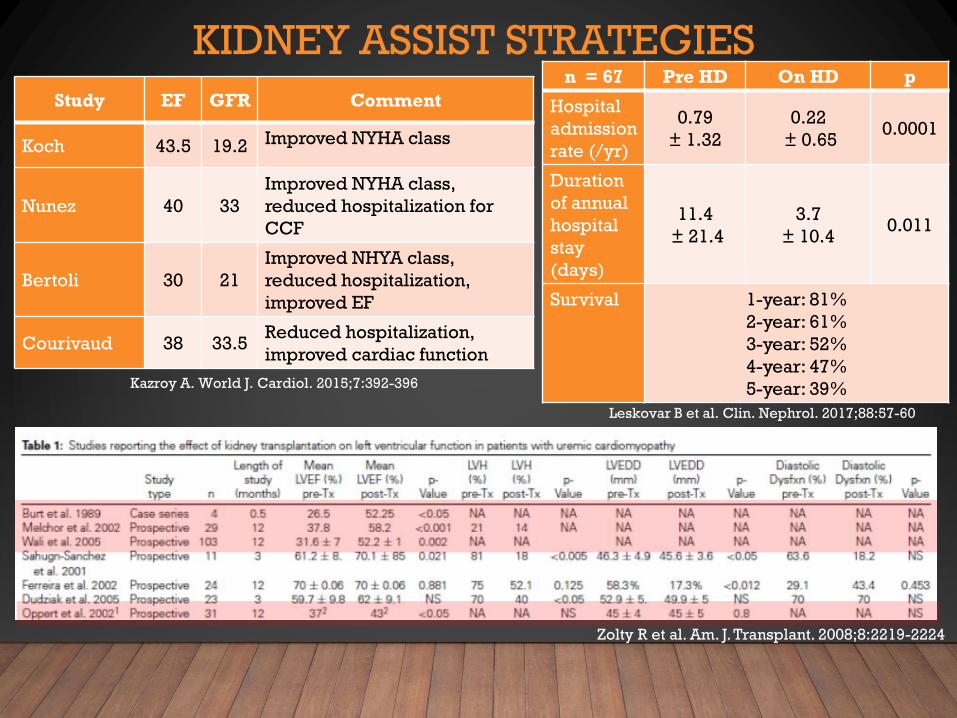
KIDNEY ASSIST STRATEGIES
Kazroy A. World J. Cardiol. 2015;7:392-396
Zolty R et al. Am. J. Transplant. 2008;8:2219-2224
n = 67 Pre HD On HD p
Hospital
admission
rate (/yr)
0.79
± 1.32
0.22
± 0.650.0001
Duration
of annual
hospital
stay
(days)
11.4
± 21.4
3.7
± 10.40.011
Survival 1-year: 81%
2-year: 61%
3-year: 52%
4-year: 47%
5-year: 39%
Leskovar B et al. Clin. Nephrol. 2017;88:57-60
Study EF GFR Comment
Koch 43.5 19.2 Improved NYHA class
Nunez 40 33
Improved NYHA class,
reduced hospitalization for
CCF
Bertoli 30 21
Improved NHYA class,
reduced hospitalization,
improved EF
Courivaud 38 33.5Reduced hospitalization,
improved cardiac function

SUMMARY
• Cardio-renal syndrome is not uncommon - ~ 1/3 of HF admissions will develop AKI
• The presence of CRS predicts a poorer long-term outcome
• The development of CRS results in activation of systems leading to chronic cardiac and renal injury
• In the context of anticipated poor outcome therapy is largely palliative:
• Diuresis relieves renal venous pressure and may improve renal function
• Long-term diuretic use when overload is corrected / improved will lead to further renal
injury
• Inotropes are only indicated in the context of cardiogenic shock
• “Renal dose dobutrex” has no scientific basis
• Vasodilators may be harmful
• RAS blockade is a rational therapy – accept MINOR GFR deterioration for long-term benefit
• Once CRS is established, cardiac / renal replacement therapies do not substantially alter
outcomes (? dual cardiac / renal transplant would be required)





























