Embed Size (px)
Citation preview

A Case Study and Exercise on How
To Use Lean Principles to Overcome
A Broken Paradigm
Cynthia Seaver, Director of Process Excellence
Mercy Health Muskegon
Certified Six Sigma Black Belt & Lean Expert

Case Study & Exercise
•Overview of Mercy Health’s Design of Consolidation New
Medical Tower
•Exercise…When you see this yellow guy, it is a discussion
point!

Healthcare Today…
• U.S. is most costly per person as compared
to all other countries
• Lower quality of health care outcomes
• U.S. hospital costs were $387.3 billion in
2011—a 63% increase since 1997 (inflation
adjusted).
• Costs per stay increased 47% since 1997,
averaging $10,000 in 2011.
• According to the World Health Organization
(WHO), total health care spending in the U.S.
was 17.9% of its GDP in 2011, the highest in
the world. 19.5% of GDP by 2017.
3 9/30/2014
Einstein put it this way:
“The significant problems we face cannot
be solved at the same level of thinking
we were at when we created them.”

Learner Objectives
• Define a paradigm
• Recognize there are paradigms in
healthcare today that are not working
• When/how to apply basic lean principles
and tools to see the paradigms in
healthcare today
• Learn how to use lean strategy to lead a
group to create a future state that will
break the paradigm of healthcare

Paradigm …is a distinct concept or thought pattern.
What are some “paradigms” in healthcare?

Paradigms Mercy Health Identified
1. Physician/provider focus
2. Design of facilities
support department silos
3. Patient hand-offs
4. Lack of collaborative
participation
5. Workflow encumbered
by the facility layout
6. Department silos - self-
contained
7

Result of Current Paradigms
• Our current “health” care model is broken.
• Current state based upon “push” thinking
• Patients are “pushed” through departments with separate
goals, budgets, and management.
•Push creates Waste:
• Unnecessary movement of patients, staff, materials and equipment
• Multiple, long queues
• Defects throughout
• Complexity of processes
• Imbalance of workloads
• Poor utilization of staff

Provided Current State
9 9/30/2014
CURRENT
Hospitals in community 3 locations + 1 Rural Acute
Hospital
Inpatient Room Sizes Undersized
Room Types Semi-Private
Total Bed Capacity 408
Patient Satisfaction – Facilities <90%
Physician Satisfaction – Facilities <90%
Quality Improvements Gradual-non scientific
Cost Efficiency Improvements Limited
Adaptability to Changing Environment Minimal

What would you do if you were presented this business case?

A Different Level & Pace of Change is Required
Time
Dramatic redefinition of value delivery, business models and business structures
Evolutionary incremental changes to increase value (Traditional Lean PI)
Mag
nit
ud
e o
f C
han
ge Transformational
Mercy Health…
“We Must Chart a New Course & Strengthen our Foundation”

Transformational Change
•Begins with a recognition that incremental
improvement is not enough
•Need to recognize that we need to change
•We need to stop doing the same things over and over
again expecting different (better) results
What Lean Strategies have we heard about in
healthcare that have been successful?

Learn from Toyota – 6 Ideas to Transformation
1. Create collaboration in the processes
2. Increase the relatedness of everyone in the process
3. Create commitment from all involved
4. Optimize the whole system, not the pieces
5. Couple action with learning
6. Reduce complexity of processes and underuse of staff
Lean, in healthcare, can best be understood as “value as defined by
our patients, pulled to our patients in search of perfection”
No one tool from lean strategies will produce
transformational results as well as these six BIG ideas

Plan for Success
• Create a balance of services
• Focus on creating patient flow
• Greatest error is not inviting
key stakeholders
Who needs to be invited to the
transformational workshops?

Create Guidance for the Teams
•Mercy Health Leadership created “guiding
principles” for transformational work
What Guiding Principles would you develop for
the teams?
•3P Participant Rights / Responsibilities
What Participant Rights would you recommend?

•Does it put the patients first?
•Does it add value to the patient experience?
•Does it empower patients to care for themselves?
• Is it safe?
• Is it convenient?
• Is it conducive to improve teamwork & patient flow?
• Is it adaptable and flexible?
•Can we afford it?
Mercy Health’s Guiding Principles
• Champion Guiding Principles • Challenge all assumptions about how work gets done • To be heard / To voice your thoughts • To disruptively innovate / To optimize the whole (not the parts) • To expect design requests to guide the plan / To seek clear explanations when
they don’t • To represent others doing similar work / To collaborate with others to
optimize the whole
Mercy Health’s 3P Participant Rights / Responsibilities

Participants? Ideas to Improve Patient Flow?
BLOW-UP &
REDEFINE
THE PROCESS
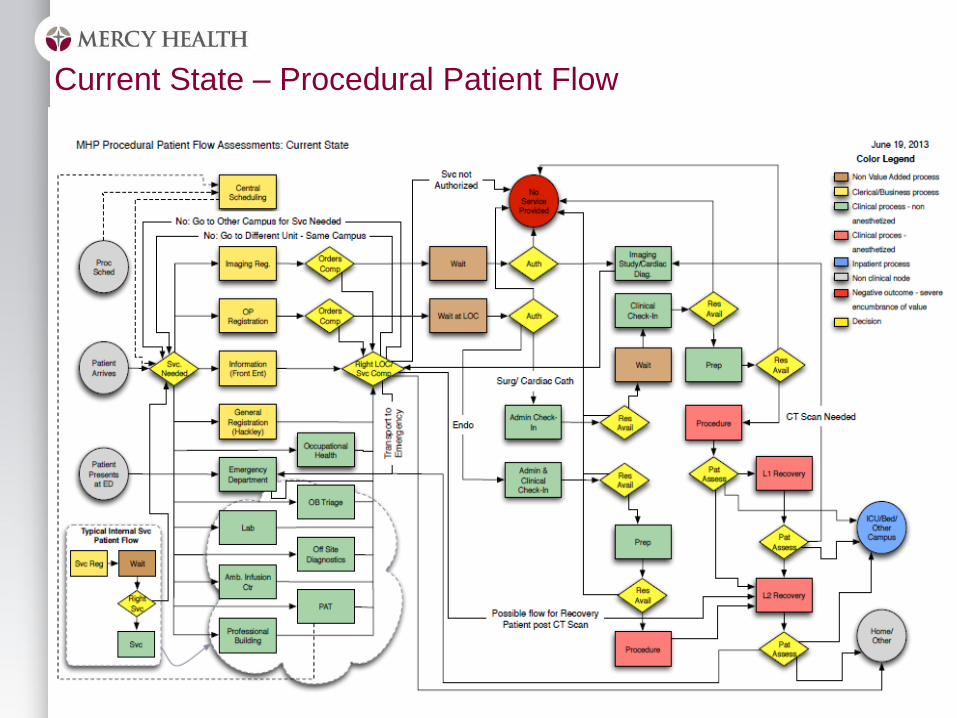
Current State – Procedural Patient Flow

Teach Strategies for Removing waste
Together we can begin to change everything!
1. Review the guiding principles
2. Discuss Team care principles
3. Simplify/standardize work and environments
4. Teach the 8 wastes of Lean – DOWNTIME
5. Combine knowledge from the Gemba & Value Stream in
search of perfection

Shared… Healthcare Strategies to Prepare for the Future
1. Operate more efficiently – pull rather than push
2. Focus on Outcomes
3. Embrace new technologies
4. Build right sized, adaptable sustainable facilities
5. Learn from manufacturing processes it can now evolve in
accordance with and even surpass current lean thinking)

Discussion: Team Care Vs Departments
Teams work together to produce value outcomes in the
care pathway
•Results in decreased cycle times for processes
•Results are based on optimization of the whole
•Multidisciplinary teams
•New team care model
•Reduces the size of the facility
Ideas you would have for future state?
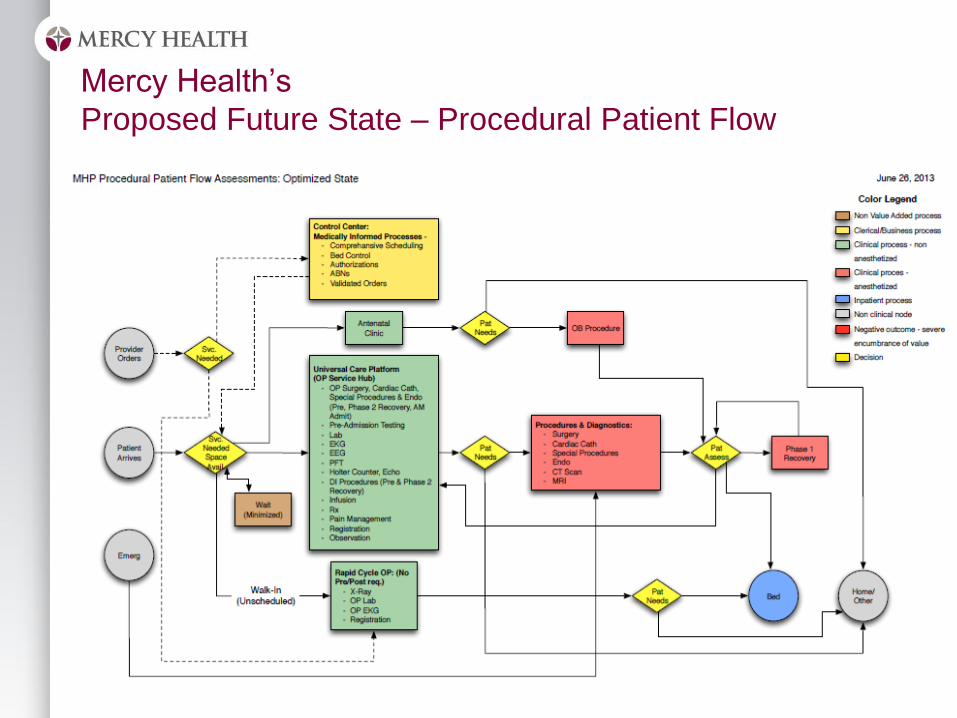
Mercy Health’s
Proposed Future State – Procedural Patient Flow

CASE STUDY 3P WORKSHOPS
Prepare for Facility Design

3P Preparation: Shell Selection
•7 Ways Shell Selection = 6 Various layouts +1 totally new
hospital

Picture of Selected Shell
Main Floor Tower
The Flow of a 3P: Preparation
• Multi-functional Teams:
– including those that designed the future state process
– Stakeholders in the “new” process
– Including physicians & representatives of ALL front line staff
– Participants are assembled in outcomes based teams
• Participants will identify a specific value stream & develop architecture
– Value Stream Maps with data
– Value vs Non-value
– Current state as well as an envisioned future state.

The Flow of a 3P: Five Day Workshop
• Day 1
– Leadership kicks off workshop & empowers team
– Lean Learning
– Review of Current State & envisioned future state
– Teams begin to resolve the program “7 Ways” using puzzle pieces
• Day 2
– Complete “7 Ways” of program & assess against patient values
– The teams then pull down all their to no more than 3
– Teams model up to three layouts by building ¼”=1’ three dimensional models.
– Teams then model their final version in a three dimensional model scaled at ½”=1’
• Day 3-4
– Full scale mock-ups of key rooms in the program, test and refine
– Identify rapid process improvement opportunities,
• Day 5
– PDSA
– Report to Senior Leaders & Physician Leaders
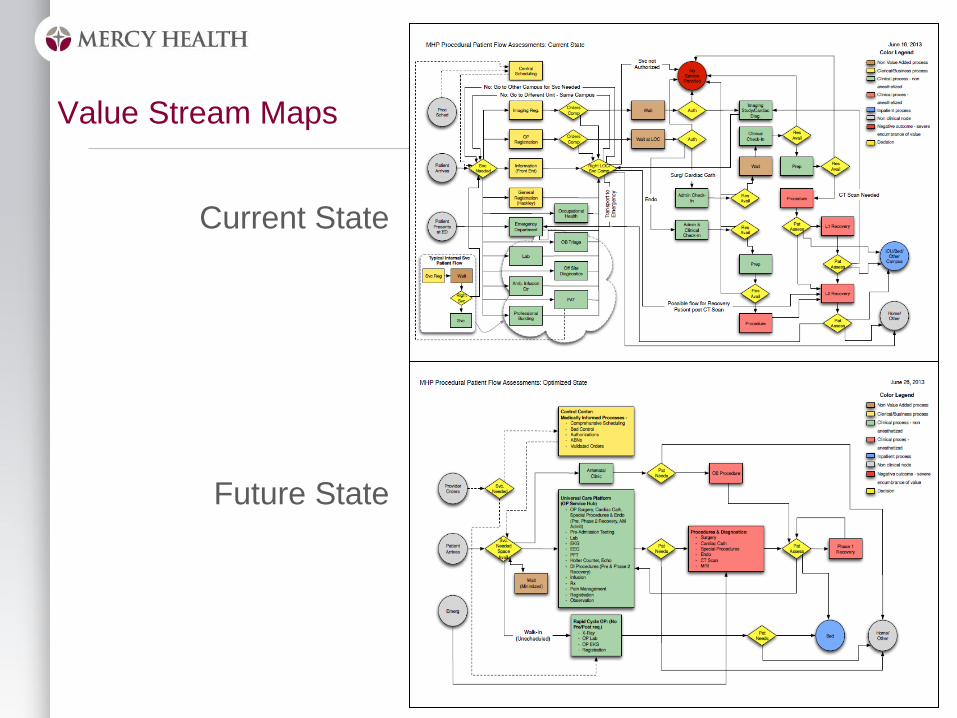
Value Stream Maps
Current State
Future State

7 Ways - Puzzle Design

¼” Metric Model

Full Size Models

3P Report Outs
•Leadership
•Departments
•Physicians
•Board Members
•Stakeholders

3P Follow Up
•Design of architecture based on new process
•Prioritize the rapid process improvement lists
•Participants bring their peers to review their work, facilitate
continued dialogue regarding the change that is coming
•Create a common understanding for the opportunity that
change promises
•Semi-permanent full scale mockups of unit sections are built to
provide simulation opportunities for teams to begin to envision
how they will accomplish better outcomes in less time with
fewer resources.
• 30/60/90 day reviews for design compliance with 3P Workshop
report outs
Time
Mag
nit
ud
e o
f C
han
ge
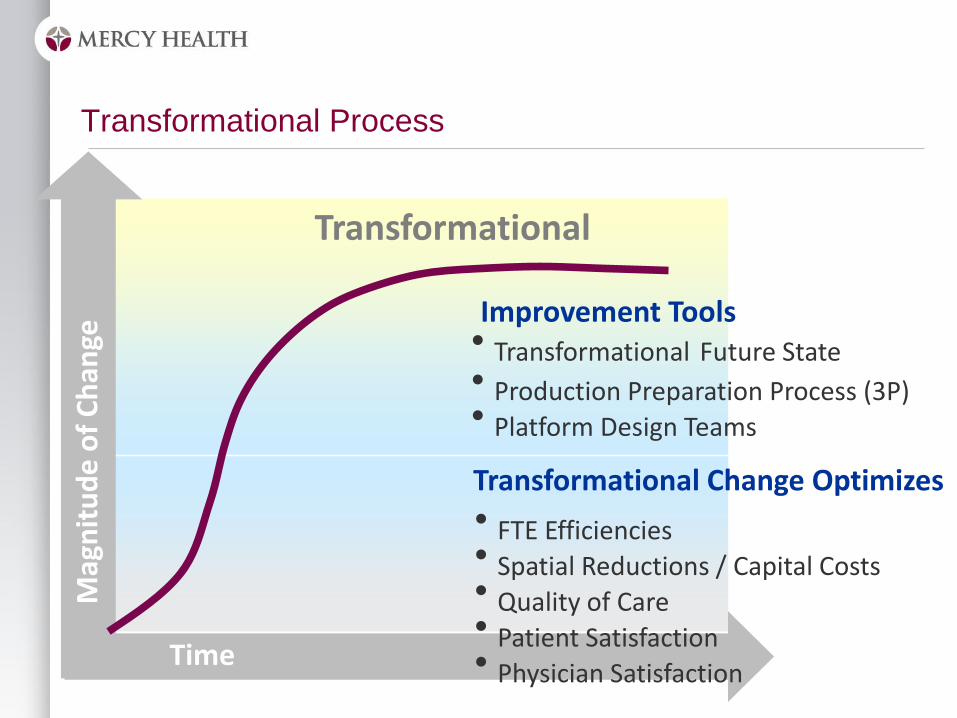
Transformational
Transformational Process
• Transformational Future State • Production Preparation Process (3P) • Platform Design Teams
Improvement Tools
• FTE Efficiencies • Spatial Reductions / Capital Costs • Quality of Care • Patient Satisfaction • Physician Satisfaction
Transformational Change Optimizes

Tips For Implementing for Transformation
• Engage stakeholders as multidisciplinary teams to participate in “kaikaku” or 3P
workshops
• Workshops can begin to identify/form new cultures in the workplace
• Envision the changes to the environment for optimizing the flows
• Greatest error in the implementation process is to error by deference –
consultants can never be as vested in the organization’s success as the
organization itself.
• The expertise must come from within, not some expert from outside.
• The quality of our answers is never greater than the quality of our questions
• Consultants can therefore “coach” successful implementations but should not
be considered the de facto leader of change
• The architect for a given project should never be the facilitator of a 3P
workshop for that project – they will already be too vested in one outcome.

Vision of Future Consolidated Mercy Health