Embed Size (px)
Citation preview

246
Received:July 15, 2014, Revised:(1st) August 9, 2014, (2nd) August 23, 2014, Accepted:August 25, 2014
Corresponding to:Dong-Hyuk Sheen, Division of Rheumatology, Department of Internal Medicine, Eulji University Hospital, Eulji University Schoolof Medicine, 95 Dunsanseo-ro, Seo-gu, Daejeon 35233, Korea. E-mail:[email protected]
pISSN: 2093-940X, eISSN: 2233-4718Copyright ⓒ 2015 by The Korean College of Rheumatology. All rights reserved.This is a Free Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited.
Case ReportJournal of Rheumatic Diseases Vol. 22, No. 4, August, 2015http://dx.doi.org/10.4078/jrd.2015.22.4.246
베체트병 환자에서 발생한 길랑-바 증후군 1
유지형ㆍ김낙민ㆍ성우경ㆍ명진철ㆍ윤수아ㆍ이동규ㆍ임미경ㆍ신동
을지 학교 을지 학교병원 내과학교실 류마티스분과
A Case of Guillain-Barre Syndrome in a Patient of Behçet’s Disease
Jihyung Yoo, Nak-Min Kim, Wookyung Sung, Jin-Cheol Myeong, Su-A Yun, Dong-Kyu Lee, Mi-Kyoung Lim, Dong-Hyuk SheenDivision of Rheumatology, Department of Internal Medicine, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea
Behçet’s disease (BD) is a multi-systemic inflammatory disease of unknown origin that affects nearly all organs including the nervous system. Although the neurological involvement is less frequent than other major presentations, it is important because it can produce severe disabilities. Peripheral nervous system manifestations are relatively rare in BD. Although few cases of pe-ripheral neuropathy or myopathy have been reported in BD, they are cases of multiple neuropathies, sensorimotor peripheral neuropathy, or neuropathy autonomic dysfunction. Guillain-Barre syndrome (GBS), also known as an acute inflammatory de-myelinating polyneuropathy, is an acute demyelinating polyradiculopathy of uncertain etiology. No case of GBS associated with BD in Korea has been reported. Herein we report on a patient of BD who suffered from weakness of extremities and was diagnosed as GBS. (J Rheum Dis 2015;22:246-249)
Key Words. Behçet’s disease, Guillain-Barre syndrome
서 론
베체트병은 반복 인 구강 성기의 궤양과 홍채염
는 포도막염, 특징 피부 소견을 주 증상으로 하는 질병
군으로, 3 주징후 이외에도 근골격계, 소화기계, 호흡기
계, 심 계, 신경계 등 신 인 침범을 보이는 자가 면
역 질환이다[1]. 발병원인에 해 HLA-B51이 련되
어 있고 그 이외 박테리아 바이러스 감염, 면역학 기
, 여러 가설이 있으나 아직 증명되지 않았다.
베체트병에서 신경증상은 환자의 5%∼15%에서 보고된
드문 증상이지만 은 나이에 성, 아 성 뇌간 증상이
나타나며, 이러한 증상은 은 나이에서 나타나는 뇌졸
다발성 경화증 다른 신경학 병변들과 감별 진단하
여야 한다.
길랑-바 증후군(Guillain-Barre syndrome)은 성 이
완성 마비 증후군 하나로 세포-단백 해리라고 불리는
뇌척수액의 정상 세포수와 단백질 상승 소견이 특징이다.
길랑-바 증후군은 세계 으로 100,000명당 0.6∼4명의
유병률을 보이고 약 2/3에서 증상 시작 호흡기 감염이
나 장증상이 보인다. 병원체는 규명되지 않았지만,
Epstein-Barr virus (EBV), Mycoplasma pneumoniae, Campy-
lobacter jejuni, 그리고 cytomegalovirus (CMV)를 포함하
여 부분의 감염원들과 련이 있다[2].
베체트병의 신경증상 , 말 신경계 침범은 아주 드물

A Case of Guillain-Barre Syndrome in a Patient of Behçet’s Disease
www.jrd.or.kr 247
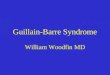
Figure 1. Abnormal nerve con-duction velocities and F-wave. (A) Motor nerve conduction ve-locity of right peroneal nerve. (B) Absent F-wave in right per-oneal nerve. (C, D) Absent F-wavein both tibial nerves.
Table 1. Electrophysiologic findings of the patient
Nerve DL (ms) Amp (mV) NCV (m/s) F-wave (ms)
Motor nerveMedian 3.55/4.30 6.0/10.4 50.7/48.5 33.45/33.45Ulnar 3.05/4.35 8.9/7.4 45.9/46.8 35.25/35.50Peroneal 5.05/Ab 0.8/Ab 40.2/Ab 57.05/AbTibial 4.55/4.70 2.2/1.5 41.1/42.6 59.15/60.45
Sensory nerveMedian 3.35/3.60 9.4/9.0 35.2/33.6Ulnar 3.15/3.95 5.0/6.3 34.3/28.1Sural 4.05/4.00 5.3/4.1 34.6/35.0
Values are presented as right/left. Ab: absent, Amp: amplitude,DL: distal latency, NCV: nerve conduction velocity.
게 나타나고 무증상 축삭 다발신경병(asymptomatic axo-
nal polyneuropathy), 다발성 단일신경염(mononeuritis
multiplex), 뇌신경병(cranial neuropathy) 등이 보고된 바
있으나. 국내에서 길랑-바 증후군이 동반된 경우는 보고
된 가 없었다[3].
자들은 외래에서 정기 추 찰하던 베체트병 환자에
서 하지 약감을 주소로 진단된 길랑-바 증후군을 경험
하 기에 보고하는 바이다.
증 례
39세 남자 환자로 양하지 약감을 주소로 내원하 다.
약 15년 에 타병원에서 포도막염, 구강내 궤양, 여드름
양 피부병변, HLA-51 양성으로 베체트병을 진단받고
2007년부터 본원 외래 진료를 받았으며, 내원 2주 부터
양하지 약감으로 걷기 어려웠다. 여러 의원에서 물리치
료, 약물 복용을 하 으나 호 없이 양쪽 상지의 약감
이 시작되고 하지 약감도 악화되어 신경과로 입원하
다. 환자는 약 5년 결핵으로 약물 복용한 이 있고 베
체트병으로 내원 후 시클로스포린 200 mg/일, 콜히친 1.2
mg/일, 드니솔론 5 mg/일을 복용 이다. 최근 복용
약물의 용량 변경이나, 추가 약물은 없으며, 가족력상 특
이사항은 없었다.
내원 당시 생체활력 징후는 압은 130/80 mm/Hg, 맥
박수 72회/분, 호흡수 18회/분, 체온은 36.3oC 다. 의식
은 명료하 고 신체검사상 특이사항 없었다. 경부, 액와,
서혜부 림 은 지되지 않았고, 흉부 청진에서 심장 잡
음이나 천명음은 없었다. 특이 피부병변은 없고 오른쪽 시

Jihyung Yoo et al.
248 J Rheum Dis Vol. 22, No. 4, August, 2015
력이 포도막염의 후유증으로 시력장애 3 상태 다. 신
경학 소견으로 부분의 근력은 medical research coun-
cil grade IV∼V이나 양쪽 무릎에서 grade III∼IV 정도,
발목 배측 굴곡에서 grade III가 나타났다. 감각은 정상이
고, 심부건반사도 정상이었다.
검사실 소견으로는 체 구계산(complete blood count),
액생화학, 구침강률, 청 크 아틴 키나아제는 정
상이었고, 류마티스인자, 항핵항체, 항 DNA항체, 항카디
오리핀항체 모두 음성이었다. CMV, EBV, Varicella zoster
virus, Campylobacter species, Mycoplasma, Mycobacteria,
Cryptoccoccus 등 감염원도 음성 반응이었다. 뇌척수액 검
사에서 정상 세포수와 정상 포도당, 정상 단백질 농도
다. 항강 리오시드항체도 음성이었다.
신경 도검사에서 우측 온종아리신경, 자신경, 좌측 정
신경, 자신경에서 terminal latency가 연장되어 있고 운
동신경 도는 좌측 자신경, 우측 자신경, 우측 온종아리신
경에서 감소되어 있으며 양측 자신경, 정 신경, 정강신
경, 우측 온종아리신경에서 F-wave latency가 연장되어 길
랑-바 증후군을 시사하 다(Table 1 and Figure 1).
방사선 소견으로는 뇌와 경추 자기공명 상에서 만성
축 이외 특이사항 없었다.
환자는 입원일부터 정맥 면역 로불린 0.4 g/kg으로 5일
사용하 고, 2일째부터 증상호 을 보 다. 퇴원 평가
에서 반 인 근력이 grade IV∼V으로 회복되었고 외래
에서 추 찰하 을 때 병의 발생 이 의 근력으로 회복
되었다.
고 찰
베체트병의 신경학 증상은 두통, 정신증상, 보행실조,
연하곤란, 시력장애, 근력 하 등 다양하며, 부분 추
신경계와 련되어 있다. 아직 명확한 진단 기 은 없으
나, 베체트병의 증상과 더불어 뇌실질의 병변이 있거나,
뇌 에서 발생한 색 증으로 발병한 질환군을 신경베체
트병이라 한다. 증상의 발 이 부분 갑작스럽게 나타나
고, 한 처치가 되지 않을 경우 후가 좋지 않아서
기에 정확한 감별진단이 필요하다[4].
증례의 환자는 근육 약감을 호소한 베체트병 환자
고, 내원 시 이학 검사에서 베체트병의 악화 소견은 없
었다. 신경학 신체검사에서 양하지 약 외에 다른 증상
은 없었고, 뇌와 경추의 자기공명 상, 뇌척수액 검사와
액검사상 추신경계 질환보다 말 신경계 질환이 의
심되었다. 신경 도검사에서 terminal latency가 연장되어
있고 운동신경 도 감소, F-wave latency가 연장된 상태로
성 염증성 말이집 탈락 신경뿌리병증(acute inflamma-
tory demyelinating polyradiculoneuropathy)인 길랑-바
증후군으로 진단하고 치료하 다.
환자가 복용하 던 콜히친의 부작용 드물게 신경근육
병증이 발병할 수 있다. Altiparmak 등[5]은 콜히친 복용
환자에서 액 검사상 청 크 아틴 키나아제 상승, 락트
산탈수소효소의 상승과 근 도 검사에서 축삭형 다발성신
경병증이 나타난 증례를 보고하 다. 콜히친의 부작용은
부분 근육병증으로 나타나고 신경병증 증상으로 보일
수 있으나 근 도 검사로 감별할 수 있다.
유사한 문헌 보고를 살펴보면, Shugaiv 등[6]은 베체트
병 증상과 하지 약감을 주소로 내원한 환자를 길랑-바
증후군으로 진단, 치료하 다. 그들은 면역 감수성에 련
된 공통된 유 자 변형을 가진 질환군이 동시에 발병할 가
능성이 높을 것이라고 추정하 다. 유 자의 변형들을 공
통 으로 가지고 있으면 하나의 질병에 이환된 자가 어떠
한 환경 원인에 노출되면 공통된 유 자 변형을 가진 질
병의 발병률이 향을 받을 것이다. 를 들어 제1형 당뇨
병, 류마티스 염, 루푸스, 하시모토 갑상선염은 PTPN
22 유 자의 변형을 공통 으로 가지고 있다. 한 T 림
구 연 질환인 Rasmussen’s encephalitis가 베체트병을
가진 환자의 가족에서 발병한 증례도 있었다[7].
길랑-바 증후군에서 식세포 매개성 말이집 탈락 상
이 일어나는데, 이 면역학 기 은 최근 보고에 의하면
활성화된 T 세포(CD4)가 슈반세포 표면에 있는 특별한
항원에 반응하여 식세포가 그 부 에서 활성화된다[8].
베체트병에서는 침범된 장기의 주변으로 다량의 T
세포가 침윤되어 있는 것이 알려져 있다. 그리고 활동기의
베체트병 환자에서 Th1 유형의 interleukin-2, interferon-γ
같은 cytokine의 T 세포의 세포질 내 발 이 증가되어 있
다[9]. Th1, Th17 cytokine과 cytotoxine T 림 구가 두
질환에 공통 인 병인에 련되어 있다고 보고된 바 있으
며[6], 유사한 T 림 구 매개 반응에 의하여 두 질환이 동
시에 발생하거나 면역반응의 교차반응 가능성이 있음을
설명할 수 있다.
다른 류마티스질환에서 동반된 길랑-바 증후군은 뇌경
색 양상의 신경정신 루푸스와 길랑-바 증후군이 동반된
증례와 항인지질 증후군과 길랑-바 증후군이 동반된 증
례가 있다[10,11]. 루푸스에 동반된 길랑-바 증후군에서
항핵항체와 항 dsDNA 항체가 높게 측정되었고, 항인지질
항체가 면역 로불린 투여 후 값이 히 감소하 다.
한 항인지질항체가 신경 수 를 침범, 괴한다는 보고가
있었다.
본 증례의 베체트병 환자는 수년 진단받고 약물을 복
용하던 자로, 다른 특이 증상 없이 시작된 하지 약감을
주소로 시행한 검사에서 길랑-바 증후군을 의심하여 치
료 후 호 되었다. 베체트병에서 신경증상은 드물게 발생
하고, 부분 베체트병의 증상 발 과 동반된 추신경계
침범 질환이다. 말 신경계 증상은 문헌에 드물게 보고되
어, 정확한 병인에 한 연구는 재까지 진행되지 못하
다. 길랑-바 증후군은 일반 으로 바이러스 감염 후에
발생하는 세포 매개성 면역 과정 신경 세포의 수 가

A Case of Guillain-Barre Syndrome in a Patient of Behçet’s Disease
www.jrd.or.kr 249
손상을 받아 발생하는 것으로 알려져 있다. 아직까지 베체
트병과 길랑-바 증후군이 동반된 기 에 해서 정확하
게 알려진 바가 없지만 각각의 질병이 면역학 인 에
서 비슷한 기 으로 설명되고 다른 류마티스 질환에서도
길랑-바 증후군이 동반된 증례로 볼 때, 련성이 있다
는 을 시사해 주며, 추후 추가 인 연구를 기 할 수 있
다.
요 약
베체트병에서 말 신경계 침범은 아주 드물게 보고되었
다. 자들은 베체트병 환자에서 갑작스러운 근육 약감
이 발생하여 진행하는 증상과 신경 도검사에서 확인된
길랑-바 증후군을 진단하 고, 약물 치료 후 증상이 호
됨을 경험하여 문헌으로 보고하는 바이다.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article
was reported.
REFERENCES
1. Sakane T, Takeno M, Suzuki N, Inaba G. Behçet's disease. N Engl J Med 1999;341:1284-91.
2. Hughes RA, Cornblath DR. Guillain-Barré syndrome.
Lancet 2005;366:1653-66.3. Lannuzel A, Lamaury I, Charpentier D, Caparros-Lefebvre
D. Neurological manifestations of Behçet’s disease in a Caribbean population: clinical and imaging findings. J Neurol 2002;249:410-8.
4. Al-Araji A, Kidd DP. Neuro-Behçet’s disease: epidemiol-ogy, clinical characteristics, and management. Lancet Neurol 2009;8:192-204.
5. Altiparmak MR, Pamuk ON, Pamuk GE, Hamuryudan V, Ataman R, Serdengecti K. Colchicine neuromyopathy: a report of six cases. Clin Exp Rheumatol 2002;20(4 Suppl 26):S13-6.
6. Shugaiv E, Kiyat-Atamer A, Tüzün E, Deymeer F, Oflazer P, Parman Y, et al. Coexistence of Guillain-Barré syn-drome and Behçet’s disease. Clin Exp Rheumatol 2013; 31(3 Suppl 77):88-9.
7. Kinay D, Bebek N, Vanli E, Gurses C, Gokyigit A, Andermann F. Rasmussen’s encephalitis and Behçet’s dis-ease: autoimmune disorders in first degree relatives. Epileptic Disord 2008;10:319-24.
8. Roh HJ, Ahn MY. Recent concept of Guillain-Barre syndrome. J Soonchunhyang Med Sci 2009;15:59-69.
9. Chang HK. New insights on the pathogenesis of Behçet’s disease. J Korean Rheum Assoc 2004;11:193-204.
10. Jung JY, Kim HA, Joo IS, Won JH, Koh BR, Park JJ, et al. Guillain-Barre syndrome, antiphospholipid syndrome and lupus nephritis as initial manifestation of systemic lupus erythematosus. J Rheum Dis 2012;19:274-9.
11. Kim HS, Lee SC, Hong HI, Han KH, Lee SK, Kim SS. A case of neuropsychiatric lupus presenting as guillain-barre syn-drome and cerebral infarction. J Korean Rheum Assoc 2004;11:411-6.