Embed Size (px)
DESCRIPTION
Citation preview

395
Review
www.expert-reviews.com ISSN 1476-058410.1586/ERV.10.17
Every year, over half a million children under 5 years of age die from rotavirus diarrhea, the most common cause of severe, dehydrating diarrhea worldwide. More than 80% of these rotavirus-related deaths occur in developing countries of sub-Saharan Africa and south Asia (Figure 1) [1–3]. Moreover, rotavirus is responsible for 25–50% of all diarrheal hospitalizations in both developing and developed countries, and 23 million outpatient healthcare encounters annually in young children [1]. Almost all chil-dren by 5 years of age will have been infected with rotavirus (Figure 2).
Owing to the tremendous global burden of rotavirus disease, development of vaccines against this pathogen has been a priority for the past three decades. Two live, orally administered rotavirus vaccines, RotaTeq® (Merck and Co., Inc., PA, USA and Sanofi Pasteur MSD SNC, Lyon, France) and Rotarix™ (GSK Biologicals, Rixensart, Belgium), with good efficacy against severe rota-virus disease and reassuring safety profiles in clini-cal trials [4,5] have been licensed in many countries worldwide. In 2006, WHO’s Strategic Advisory Group of Experts (SAGE) reviewed the results of the pivotal safety and efficacy trials for these vaccines conducted in the Americas and Europe and strongly recommended their inclusion into national immunization programs of countries in these regions [6]. In April and October 2009, SAGE reviewed additional efficacy data from tri-als in Africa and Asia, and postlicensure studies in the Americas, and extended the recommendation for vaccination to all regions of the world [7–9].
In this review, we briefly review the epide-miology of rotavirus and the history of vaccine develop ment efforts. We then summarize early data on the effectiveness and impact of vaccin-ation from high- and middle-income countries that have adopted routine childhood immun-ization against rotavirus. Finally, we outline key outstanding questions and potential areas for further research, especially to optimize the ben-efits of vaccination in developing countries where vaccines are likely to have their greatest impact.
Epidemiology of rotavirusRotavirus is a nonenveloped, dsRNA virus with a segmented genome [10,11]. The genotypes (glyco-protein [G] and protease-cleaved [P] types) are defined by two structural viral proteins (VPs) in the outer capsid: VP4, the P protein; and VP7, the G protein. Natural fluctuations in genotype prevalence occur over time and by region of the world, with G1, G2, G3 and G4 being the most common genotypes worldwide. G9 emerged as a globally important strain in the 1990s and G12 strains have been documented in many countries over the last decade [12].
Rotavirus infects the proximal small intestine, resulting in destruction of the epithelial surface and blunting of the microvilli, leading to mal-absorption and diarrhea [11]. A nonstructural pro-tein (NSP4) of rotavirus acts as an enterotoxin in the mouse model and probably plays a role early in human disease pathogenesis [13]. The clinical spectrum of rotavirus disease in children ranges from mild, watery diarrhea of limited duration
Jacqueline E Tate†, Manish M Patel, A Duncan Steele, Jon R Gentsch, Daniel C Payne, Margaret M Cortese, Osamu Nakagomi, Nigel A Cunliffe, Baoming Jiang, Kathleen M Neuzil, Lucia H de Oliveira, Roger I Glass and Umesh D Parashar†Author for correspondenceNational Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention, 1600 Clifton Rd. NE, MS-A47, Atlanta, GA 30333, USA Tel.: +1 404 639 4559 Fax: +1 404 639 8665 [email protected]
The WHO has recently recommended the inclusion of rotavirus vaccine in the national immunization programs of all countries. In countries in the Americas, Europe and Australia that have adopted routine childhood immunization against rotavirus, significant reductions in the burden of severe childhood diarrhea have been observed. Besides protecting vaccinated children, disease rates also appear to be reduced in unvaccinated children, suggesting indirect benefits from vaccination (i.e., herd protection). Early clinical trial data from Africa and Asia are promising, and further efforts are needed to optimize the benefits of vaccination in developing countries where vaccines are likely to have their greatest impact.
Keywords: diarrhea • rotavirus • rotavirus vaccination • vaccine effectiveness
Global impact of rotavirus vaccinesExpert Rev. Vaccines 9(4), 395–407 (2010)
For reprint orders, please contact [email protected]

396
Review
Expert Rev. Vaccines 9(4), (2010)
to severe diarrhea with vomiting and fever that, in some children, can result in rapid dehydration with shock, electrolyte imbalance and death [14–17]. Natural rotavirus infections may commonly spread beyond the intestines into the blood stream, causing sys-temic viremia [18–22]. Rotavirus antigen has been detected in the serum of greater than 90% of rotavirus-positive children until approximately 5 days following symptom onset [18].
Although rotavirus infects virtually all children by 5 years of age in both developed and developing countries, there are significant differences between the two settings in terms of the age at which disease first occurs, the seasonality of rotavirus illness, the distribu-tion of serotypes and the proportion of severe outcomes, particularly mortality. In high-income countries, few children die from rota-virus and, globally, most children who die each year from rotavirus infection are from low-income countries [1]. The increased risk of mortality in low-income settings is probably due to a combination of factors, including limited access to healthcare (hydration therapy) and a greater prevalence of malnutrition and other comorbidities.
Rotavirus vaccinesImprovements in sanitation and hygiene have had a great impact on reducing diarrheal disease and deaths due to bacterial and parasitic agents that are spread primarily through contaminated
food or water, but these improvements have had a lesser impact on infection with rotavirus, which is most commonly spread from person to person [14,23–27]. Instead, early studies that followed cohorts of children in their first 2–3 years of life identified epi-demiologic features of rotavirus that indicated the disease might best be controlled through vaccination. Specifically, these studies demonstrated that children previously infected with rotavirus were protected against subsequent disease. Protection was great-est against moderate-to-severe disease and the level of protection increased with each new infection [23,28]. These data implied that an attenuated rotavirus vaccine that mimics natural infection could provide protection against disease and that multiple vaccine doses would probably be required to confer optimal protection.
HistorySince early animal models suggest that local intestinal immu-nity is important in protection from disease, rotavirus vaccine develop ment has focused on orally administered vaccines [29]. First-generation rotavirus vaccines used a ‘Jennerian’ approach where vaccines were developed using animal rotavirus strains that are naturally attenuated for humans and whose serotypes were hetero-typic compared with the most common human rotaviruses [30]. The performance of these vaccines was variable, with high efficacy
<10 deaths per 100,000
10–50 deaths per 100,000
50–100 deaths per 100,000
100–500 deaths per 100,000
Figure 1. Estimated rotavirus mortality rates in children under 5 years of age worldwide.Adapted with permission from [2].
Tate, Patel, Steele et al.

www.expert-reviews.com 397
Review
against severe rotavirus disease in Finland but little or no efficacy in developing coun-tries [31–40]. The best efficacy in a developing country setting of one such vaccine, a rhesus rotavirus vaccine, was observed for a clinical trial in Venezuela where the serotype of the predominate circulating G3 strain matched the serotype of the vaccine [41,42]. This find-ing suggested that serotype-specific immu-nity might be required to achieve optimal protection and led to efforts to develop second-generation multivalent vaccines.
Second-generation rotavirus vaccines used a ‘modified Jennerian’ approach where a naturally attenuated animal strain was used as the backbone for the vaccine and genes coding for the most common human rota-virus G types were substituted for the ani-mal rotavirus G type by reassortment in cell culture [30]. Pivotal clinical efficacy studies of the rhesus human rotavirus reassortant vaccine were conducted in Finland, the USA and Venezuela, where the vaccine showed 91, 82 and 88% efficacy against severe rotavirus gastroenteritis during the first year of follow-up, respectively [43–45].
In August 1998, a rhesus-based, tetravalent rotavirus vaccine (RRV-TV) with three of the four common human rotavirus G types (G1, G2 and G4) and the rhesus parent with G3 closely related to the human G3, the fourth common serotype, was introduced in the USA [46]. By May 1999, almost 1 million doses of the vaccine had been administered [46]. In July 1999, the vaccination program was suspended after the vaccine was associated with a rare adverse event, intussusception, a form of bowel obstruction in which one por-tion of the bowel telescopes into a distal portion [47,48]. In the first 3–14 days after receipt of the first dose of RRV-TV, risk of intus-susception was most elevated (>20-fold) and a smaller increased risk (~fivefold) was also observed within 3–14 days after the sec-ond dose [49]. Overall, the risk of intus susception was estimated as one case per 10,000 children vaccinated with RRV-TV [50].
Some researchers have suggested that the risk of intussusception associated with RRV-TV was age dependent and that the abso-lute number of intussusception events and possibly the relative risk of intus susception associated with the first dose of RRV-TV increased with increasing age at vaccination [51,52]. However, the WHO Global Advisory Committee on Vaccine Safety (GACVS), after reviewing all the available data, concluded that there was a high risk of RRV-TV-associated intus susception in infants immu-nized after day 60 and that insufficient evidence was available to conclude that the use of RRV-TV at any age under 60 days was associated with a lower risk [53]. The GACVS noted that the possibility of an age-dependent risk of intussusception should be taken into account in testing future rotavirus vaccines. RRV-TV vaccine was voluntarily withdrawn from the market and is not in use today. A Phase II trial to evaluate the safety, immunogenicity and potentially efficacy of two doses of RRV-TV administered to young infants under the age of 2 months is ongoing in Ghana [54].
Currently licensed pentavalent (RotaTeq, RV5) & monovalent (Rotarix, RV1) rotavirus vaccinesDespite the setback with the withdrawal of a licensed and recom-mended rotavirus vaccine, the burden of rotavirus disease was still deemed substantial by the public health community and develop-ment of other rotavirus vaccines continued. In 2006, results from clinical trials of two new rotavirus vaccines were published [4,5]. Both are live, attenuated, orally administered vaccines (Table 1). One, RotaTeq is a pentavalent, human–bovine reassortant vac-cine (RV5) that contains a bovine rotavirus backbone with single human rotavirus gene substitutions for each of the five common G and P human rotavirus genotypes (G1, G2, G3, G4 and P[8]) and is administered on a three-dose schedule [55]. The second vac-cine, Rotarix, is a monovalent, two-dose vaccine (RV1) based on a single rotavirus strain of the most common human genotype, G1P[8], observed globally [56,57]. Both of these vaccines have been evaluated in a variety of settings (Table 2).
Efficacy of RV5 & RV1 in pivotal prelicensure trialsIn clinical trials performed predominantly in the USA and Finland, RV5 reduced hospitalizations due to rotavirus gastro-enteritis by 96% (95% CI: 91–98%), emergency department visits by 94% (95% CI: 89–97%) and doctor’s office visits by 86% (95% CI: 74–93%) [5]. While the per-protocol analysis examined the efficacy against G1–G4 strains, the majority of cases in the clinical trial were G1. Only sufficient numbers of cases were enrolled to detect significant serotype-specific effi-cacy against G1 and G2 strains but significant reductions in rates of rotavirus hospitalizations and emergency department visits were detected for G1, G3, G4 and G9 [5]. The RV5 safety trial enrolled over 70,000 infants specifically to evaluate the risk of intussusception. No association with this adverse event was found within 42 days after any dose of RV5 (relative risk [RR]: 1.6; 95% CI: 0.4–6.4) [5].
527,000 deaths
2.3 million hospitalizations
23 million outpatient visits
114 million episodes
Figure 2. Global rotavirus disease burden. Adapted from [130].
Global impact of rotavirus vaccines

398
Review
Expert Rev. Vaccines 9(4), (2010)
RV1 was 85% (95% CI: 71–93%) efficacious in preventing severe (Vesikari score ≥11) rotavirus gastroenteritis during the first year of life in clinical trials in Latin America and 96% (95% CI: 90–99%) effective against severe disease in clinical trials in Europe [4,58]. No risk of intussusception in the 30 days post-RV1 vaccination was observed (RR: 0.85; 95% CI: 0.30–2.42) [4]. In Latin America, while fully heterotypic G2P[4] strains that share neither G nor P type with the RV1 vaccine strain were uncommon, protection appeared to be lower (44%; 95% CI: <0–84%) for severe disease (Vesikari score ≥11) against these strains [59]. However, in the sec-ond large efficacy trial conducted in Europe and in results of a meta-analysis integrating all previous trial results, RV1 provided statistically significant protection against severe rotavirus diarrhea caused by G2P[4] strains (86%; 95% CI: 24–99% and 67%; 95% CI: 15–87%, respectively) [58,60,61].
In 2006, based on the initial clinical trial data from Latin America, Europe and the USA, the SAGE recommended the use of rotavirus vaccines in countries where successful Phase III effi-cacy trials had been performed and where data from these trials suggested that the public health impact could be great [6]. This SAGE recommendation did not include countries in Africa and Asia, where rotavirus disease burden and mortality is high, because efficacy data were not available from these regions and the perfor-mance and efficacy of live, oral vaccines in these regions has been variable. Rather, the SAGE reiterated earlier recommendations that Phase III clinical trials be conducted in representative low-income countries of Asia and Africa to demonstrate vaccine efficacy in these settings. Following the 2006 SAGE recommendation, rotavirus
vaccines were subsequently introduced into numerous countries in the Americas, Europe and Australia, and Phase III clini-cal trials of both candidate vaccines were conducted in Africa and Asia.
Efficacy of RV5 & RV1 in Africa & AsiaPhase III clinical trials for RV1 were performed in South Africa and Malawi, and Phase II immunogenicity studies for RV1 were conducted in Bangladesh. Trials for RV5 were performed in Kenya, Ghana, Mali, Bangladesh and Vietnam. Vaccine performance with both vaccines was observed to be lower in these setting when compared with the pivotal studies described in previous sections. In South Africa, two doses of RV1 administered to infants at 10 and 14 weeks of age were 72% (95% CI: 40–88%) efficacious in prevent-ing severe rotavirus gastroenteritis and effi-cacy increased to 82% (95% CI: 55–94%) when a three-dose schedule administered at 6, 10 and 14 weeks was used [7,62]. In Malawi, the two- and three-dose schedules of RV1 yielded similar results with a two-dose vac-cine efficacy of 49% (95% CI: 11–72%)
and three-dose vaccine efficacy of 50% (95% CI: 11–72%) [7,62]. However, the background rates of rotavirus disease were much greater in Malawi than in South Africa, so despite a lower effi-cacy the vaccine was able to prevent 3.9 episodes of severe rotavi-rus gastroenteritis per 100 vaccinated children in Malawi versus 2.5 episodes per 100 vaccinated children in South Africa [7,62].
Preliminary results for the clinical trials for RV5 showed similar variability by setting as the RV1 trials although the methodology for assessing clinical efficacy varied for the two vaccines. In the three African RV5 clinical trial sites (Kenya, Ghana and Mali), a three-dose regimen of RV5 administered at 6, 10 and 14 weeks of age was 64% (95% CI: 40–79%) effective against severe rota-virus gastroenteritis during the first year of follow-up [8]. During the first year of follow-up in the Asian trial sites (Vietnam and Bangladesh), three doses of RV5 were 51% (95% CI: 13–73%) effective against severe rotavirus gastroenteritis [8].
Effectiveness & impact of RV5 & RV1 under routine use in the Americas, Australia & EuropeUSATo assess the impact and field effectiveness of rotavirus vaccin ation, post-introduction surveillance commenced in 2006 in the USA after the recommendation for routine use of rotavirus vaccine in all US infants [63]. In a case–control study of field effectiveness of vaccination conducted at a large pediatric hospital in Houston, TX, USA, RV5 was 85–89% effective in preventing severe rotavirus gastroenteritis, resulting in hospitalization or emergency depart-ment care, similar to the efficacy seen in prelicensure trials of
Table 1. Characteristics of available rotavirus vaccines.
Characteristic RV5 RV1
Manufacturer Merck & Co. (PA, USA) GlaxoSmithKline (Rixensart, Belgium)
Parent strain Bovine rotavirus strain WC3, type G6P7[5]
Human rotavirus strain 89–12, type G1P1A[8]
Formulation Five reassortants: G1xWC3, G2xWC3, G3xWC3, G4xWC3, P1A[8]xWC3
No reassortants
Vaccine titer ≥2.0–2.8 × 106 infectious units per strain, depending on serotype (1.15 × 107 infectious units per dose)
≥106 median cell culture infective dose after reconstitution, per dose
Method of attenuation Naturally attenuated (animal strain); passage varied by reassortant 7–69-times
Passaged 43-times
Cell culture substrate Vero cells Vero cells
Dose volume (ml) 2 1
Buffer Sodium citrate and phosphate Calcium carbonate
Dose regimen Three oral doses Two oral doses
Shedding following first dose (%)
9–21 35–80
RV: Rotavirus Adapted from [97].
Tate, Patel, Steele et al.

www.expert-reviews.com 399
Review
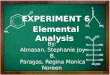
RV5 [64]. In addition, in a national network of sentinel clinical laboratories where results of rotavirus tests ordered by physicians were analyzed, the timing and magnitude of the first two rotavirus seasons following vaccine introduction were delayed by 6–15 weeks and decreased in peak magnitude by 42–60% (Figure 3) [65,66]. Similarly, declines in hospitalizations and doctor’s office visits for acute gastroenteritis were observed during the 2007–2008 season in many regions of the country [67]. Declines in disease were seen in all children under 5 years of age and not solely in age-eligible chil-dren suggesting possible indirect protection among unvaccinated populations who were still at risk [67].
AustraliaThe impact of the vaccination program in Australia has been similar to that in the USA. RV1 was introduced in Queensland, Australia, in July 2007 and the proportion of positive rotavirus tests in children under 2 years of age detected through laboratory surveillance declined by 45% in 2007 and 43% in 2008 compared with the prevaccine baseline [68]. Declines in the proportion of rotavirus-positive tests were also observed in older children who were in eligible to be vaccinated which also suggests that the vaccine may offer indirect benefits. In a post-introduction vaccine-effec-tiveness evaluation among indigenous children in central Australia in 2007, RV1 was 85% effective against confirmed rotavirus infec-tion (84% effective against G9P[8] strains), 83% effective against severe all-cause gastroenteritis and 78% effective against all-cause gastroenteritis of any severity [69]. In another similar study from the same population in 2009, RV1 was 86% effective against rotavirus hospitalization due to the G2P[4] strain [70].
AustriaA similar impact was also observed in Austria following the intro-duction of rotavirus vaccine into the universal mass vaccination program in 2007 [71]. In the first 18 months of the program, rates of hospitalization due to rotavirus fell 74% among age-eligible children. Vaccine effectiveness was estimated to be 61–98%.
BrazilIn March 2006, Brazil initiated universal immunization of infants with RV1. Since vaccine introduction, two cities in northeast Brazil (Aracaju and Recife), each with vaccine cov-erage of greater than 50%, have identified a predominance of G2P[4] strains in children with severe rotavirus diarrhea [72–74]. Although rotavirus now accounts for a substantially lower pro-portion of hospitalizations for diarrhea post vaccine introduc-tion compared with the prevaccine era [75], these findings have prompted debate about whether a possible lower effectiveness of RV1 against G2P[4] strains has led to their predominance for over 2 years [72–74,76]. Two recent evaluations have affirmed that RV1 is effective against severe rotavirus diarrhea caused by G2P[4] strains [75,77], although questions about effectiveness during the second year of life remain.
MexicoMexico introduced RV1 in a phased manner between February 2006 and May 2007. By May 2007, rotavirus vaccination was available for all Mexican infants. A recent investigation found that in 2008, when coverage for one or more doses among infants under 12 months of age exceeded 70%, there was a 42% decline in
Week of year
70
60
50
40
30
20
10
0
27 29 31 33 35 37 39 41 43 45 47 51 1 3 5 7 9 13 15 17 19 21 23 2549 11
2000–2006 maximum2000–2006 median2000–2006 minimum2007–2008 season2008–2009 season
% o
f te
sts
rota
viru
s p
osi
tive
Beginning/end of rotavirus season Peak week of activity
Week of year
Figure 3. Proportion of tests positive for rotavirus by week of year, USA, National Respiratory and Enteric Viruses Surveillance System (NREVSS), July 2000–June 2009.Adapted from [66].
Global impact of rotavirus vaccines

400
Review
Expert Rev. Vaccines 9(4), (2010)
all-cause diarrhea mortality among infants in this age group [78]. Moreover, a 23% reduction was also observed among older chil-dren 12–23 months of age who were largely ineligible for rotavi-rus immunization [78]. Sustained reduction in mortality among children under 2 years of age in 2009 and blunting of the sea-sonal peak in diarrhea deaths when rotavirus is most prevalent in Mexico provided further supporting evidence for vaccine effect as the major contributing factor towards this reduction in all-cause gastroenteritis mortality.
El SalvadorIn El Salvador, a low-to-middle-income country in Central America, a case–control evaluation of RV1 effectiveness found that this vaccine was 74% effective against severe rotavirus gas-troenteritis (Vesikari score ≥11) and 88% effective in preventing very severe rotavirus gastroenteritis (Vesikari score ≥15) [7]. The
impact of the vaccine in El Salvador was also observed through national surveillance data where cases of rotavirus diarrhea have declined by 79% following the introduction of RV1.
NicaraguaIn Nicaragua, one of the poorest countries in Latin America and eligible for support for vaccine purchase from the GAVI Alliance, a case–control evaluation found that RV5 was 52–63% effective in preventing severe rota-virus gastroenteritis (Vesikari score ≥11) and 73–86% effective in preventing very severe rotavirus gastroenteritis (Vesikari score ≥15) in the first year post vaccine introduction, during a season with G2P[4] rotavirus pre-dominance [79]. During the 2007 rotavirus season in Nicaragua when coverage with at least two doses among children under 12 months of age was still low at approxi-mately 26%, hospitalizations and health-care visits for diarrhea of any cause declined by 11 and 23%, respectively, compared with the prevaccine baseline [80].
Safety of rotavirus vaccinesAlthough neither RV5 nor RV1 were asso-ciated with intussusception during the clinical trials, post-introduction monitor-ing of vaccine safety is necessary as a low level of risk cannot yet be excluded. The USA has conducted postlicensure moni-toring since the introduction of RV5 in 2006 through the Vaccine Adverse Events Reporting System, a national passive sur-veillance system and through the Vaccine Safety Datalink, a cohort of children enrolled in a managed care network. To
date available data from these systems do not suggest a risk of intussusception after receipt of RV5 but continued monitoring is necessary as a low level of risk has not yet been excluded for RV5 and additional data are still needed for RV1 [81,82]. As more countries introduce rotavirus vaccines, continued monitoring is important. While there are no data to suggest that there would be regional differences in risk ratios for intussusception after vaccin ation, differences in background rates of intussusception could result in differences in attributable risk, if any risk after vaccin ation did exist [83].
Vaccine-acquired rotavirus disease after RV5 administration in three infants with severe combined immunodeficiency (SCID) has recently been reported suggesting that rotavirus vaccine may cause disease in severely immunocompromised children [84]. SCID is now included as a contraindications for RV5 [85]. Rotavirus vaccine is not contraindicated for children with other types of
Table 2. Vaccine efficacy and postlicensure effectiveness data for 1 year of follow-up by setting.
Setting Vaccine Type of study
VE† (%) (95% CI)
Severity Ref.
High and middle income
USA and Finland
RV5 Efficacy 98 (88–100) Clark score >16, efficacy against types G1–G4
[5]
USA and Finland
RV5 Efficacy 74 (67–80) Any severity; efficacy against types G1–G4
[5]
Finland RV1 Efficacy 90 (10–100) Vesikari score ≥11 [104]
Finland and Latin America
RV1 Efficacy 85 (75–92) Vesikari score ≥11 [4]
Europe RV1 Efficacy 87 (80–92) Any severity [58]
Finland RV1 Efficacy 73 (27–91) Any severity [104]
USA RV5 Effectiveness 88 (68–96) Hospitalization and ED visit
[64]
Australia RV1 Effectiveness 85 (23–97) Hospitalization in indigenous population
[69]
Brazil RV1 Effectiveness 79 (74–82) Hospitalization and ED visit; efficacy against G2P[4]
[75]
Brazil RV1 Effectiveness 85 (54–95) Hospitalization; efficacy against G2P[4]
[77]
Middle-low and low income
Asia (Vietnam, Bangladesh)
RV5 Efficacy 51 (13–73) Vesikari score ≥11 [8]
Africa (Kenya, Ghana, Mali)
RV5 Efficacy 64 (40–79) Vesikari score ≥11 [8]
Africa (South Africa, Malawi)
RV1 Efficacy 62 (44–73) Vesikari score ≥11 [7]
Nicaragua RV5 Effectiveness 46 (18–64) Hospitalization [79]
El Salvador RV1 Effectiveness 76 (64–84) Hospitalization [7]
†VE stands for vaccine efficacy or vaccine effectiveness, depending on the type of study.ED: Emergency department; RV: Rotavirus.
Tate, Patel, Steele et al.

www.expert-reviews.com 401
Review
immuno deficiencies but few data are available [85]. HIV-infected and -exposed infants were included in the RV1 clinical trials and no significant safety concerns were identified [62].
Global introduction of rotavirus vaccinesThe 2009 global recommendation by the WHO for the inclusion of rotavirus vaccines in the routine childhood vaccine programs in all countries, and specifically in countries where the diarrheal proportion of under-5-year-old mortality is 10% or more [7,9], is a significant step towards fully utilizing these vaccines. Several other important developments have occurred which will enhance the global impact of these rotavirus vaccines on childhood mortality as they are introduced more widely.
First, the efficacy of RV5 and RV1 vaccines in developing coun-tries, although moderate, has demonstrated that the vaccines have a substantial public health impact on disease in these settings where the highest rates of rotavirus mortality occur. Rotavirus vaccines significantly reduced serious rotavirus gastroenteritis in resource-poor settings in Africa and Asia, where the attack rate for severe and fatal rotavirus diarrhea is high. The protection occurred in settings where multiple G and P types circulated, where nonvaccine strains predominated, and where vaccine was administered to children under ‘real world conditions’ – concomi-tant administration with oral polio vaccine (OPV), no restric-tions on breastfeeding and inclusion of children exposed to HIV infection [62]. Significantly, the vaccines do not interfere with the immune response to OPV vaccines [86,87]. These results are very encouraging about the potential for rotavirus vaccines to reduce the significant morbidity and mortality due to rotavirus diarrhea in the world’s poorest children.
Second, the currently available vaccines have been shown to be safe with respect to intussusception and other serious adverse events. Recent recommendations by SAGE and the WHO GACVS have relaxed the restriction on the age window for vac-cine administration. The SAGE recommendations extend the administration of the first dose of vaccine up to 15 weeks of age, similar to the US Advisory Committee on Immunization Practices (ACIP) recommendations and the last dose of either the two-dose RV1 or the three-dose RV5 vaccine should be admin-istered by 32 weeks of age [7,63]. This expanded age recommen-dation would increase vaccine coverage in developing countries where children often present late for their routine childhood vaccinations [88,89].
Third, GAVI approved the inclusion of rotavirus vaccines for vaccine subsidy in GAVI-eligible countries and has requested ‘let-ters of interest’ from countries wanting rotavirus vaccines. Several African and Asian countries submitted proposals to GAVI for review in late 2009. While subsidization by GAVI will make it financially feasible for early adopter countries to use the current rotavirus vaccines, the long-term sustainability of vaccine pur-chase for all GAVI-eligible countries cannot be guaranteed. The GAVI subsidy of rotavirus vaccine means that the UNICEF will be able to negotiate lower prices for low-income countries, but this support for the vaccines ends in 2015, and countries will be expected to cover the whole cost once the GAVI subsidy closes.
Coordinated efforts with GAVI, the manufacturers and other international partners are needed to ensure the affordability of rotavirus vaccines for low and lower middle-income countries, both now and in the future.
Rotavirus vaccines are poised to make a significant public health impact on rotavirus-associated mortality in developing countries, and as funding subsidies are made available and effectiveness data are generated in early adopter countries showing the impact of the vaccines, continued introduction of the vaccines in additional countries is probable.
Evaluating & improving performance of rotavirus vaccines in developing countriesWhile rotavirus vaccines are likely to have a tremendous impact on rotavirus disease in developing countries, live, oral vaccines have had an inconsistent history in the developing world. For example, OPV is less immunogenic and more doses are required to protect children in India and other developing countries com-pared with children in the developed world [90–92]. Similarly, an oral cholera vaccine was found to be less immunogenic and a higher titer of the vaccine was needed to offer protection against disease in developing countries in Asia and Latin America [93,94]. Early rotavirus vaccines also faced challenges in the developing world, and several candidate rotavirus vaccines (RIT4237, WC3, RRV and RRV-TV) had lower or no measurable efficacy in clini-cal trials in South America and Africa than in Europe and North America [37–40,95]. Even in clinical trials and in routine use in immunization programs, the effectiveness of current rotavirus vaccines has been inversely correlated with the childhood mortal-ity level in the country where the trial was conducted. Similarly, immune response to RV1, which has been more widely tested in the developing world, appears to decrease with decreasing income level of the country [96].
The reasons why live, oral rotavirus vaccines are less effica-cious in developing countries are not clear and are probably multi faceted [97]. First, children in these countries often have distinct medical conditions from those typically seen among children in the developed world. For example, a higher preva-lence of co morbid infections in young children – HIV, malaria, tuberculosis and intestinal infections with other microorganisms – may adversely affect vaccine performance. Second, malnutri-tion is more common and may influence vaccine effectiveness. Third, in these developing country settings, levels of maternal rotavirus anti bodies are passively transferred to babies during gestation and still present in infancy. Furthermore, rotavirus-vaccine neutralizing activity of breast milk is usually higher than in developed countries, and may reduce vaccine titer and adversely affect vaccine take; however, further studies are needed to confirm this [98,99]. Also, rotavirus vaccine is almost always administered on the same schedule as OPV, and some data sug-gest that the immune response to the first dose of rotavirus vaccine in particular could be somewhat reduced when given concomitantly with the first dose of OPV [86,100]. Finally, the diversity of circulating strains in Africa and Asia is substantial and different from that seen in the Americas and Europe [101,102].
Global impact of rotavirus vaccines

402
Review
Expert Rev. Vaccines 9(4), (2010)
Globally, G1P[8] is the most predominant strain causing over 70% of rotavirus infections in North America, Europe and Australia but causes only 30% of rotavirus infections in South America and Asia, and 23% in Africa [101]. In parts of Asia and Africa, G9 strains have emerged as the predominantly circulat-ing strain and G8 strains are isolated with increasing frequency in Africa as well [103]. While the vaccines have demonstrated pro-tection against the most commonly circulating strains (G1–G4 and G9), effectiveness against less common strains has not been fully evaluated [5,58,59,104].
Thus, despite the promising efficacy data from the clinical tri-als in Africa and Asia, many unanswered questions about vac-cine effectiveness and how to improve vaccine performance in these settings remain. As vaccines are introduced into the routine immunization programs in Africa and Asia, ongoing monitoring is critical since vaccine performance varied by setting in clinical trials. Thus, to fully understand the impact of rotavirus vaccine introduction in developing countries, several key epidemiologic issues should be monitored including vaccine performance against severe disease during routine use, vaccine impact on rotavirus disease epidemiology, including changes in burden of severe dis-ease and death, age distribution of cases, seasonality and sero-type distribution, indirect benefits for unvaccinated children, and duration of protection [105].
Careful consideration of these issues prior to vaccine introduc-tion will enable development of surveillance systems capable of capturing the full impact of the vaccine program. Initiation of population-based surveillance in a variety of high-disease-burden settings prior to vaccine introduction will enable calculation of baseline rates of disease, hospitalization, and death due to all-cause diarrhea and rotavirus gastroenteritis, and documentation of currently circulating strains. After vaccine introduction, these surveillance platforms will enable monitoring of changes in rates of mortality and morbidity, and any shifts in circulating strains as well as serve as a basis for vaccine effectiveness evaluations. Furthermore, these platforms can be used to explore reasons for lower efficacy of rotavirus vaccines in developing countries in contrast to middle- and high-income countries, and to examine the usefulness of potential ways to improve vaccine performance, such as delaying age at first vaccination by 4–6 weeks to reduce interference by maternal antibodies, offering neonatal vaccina-tion to target early disease, increasing the number of doses, alter-ing breastfeeding practices immediately preceding and following immunization, and using zinc or probiotic supplementation to improve the mucosal response to vaccination.
The long-term impact of vaccines on circulating strains is unknown and continuous surveillance will be needed to address this issue [12,106]. Studies in countries that have introduced rota-virus vaccines have, in some cases, reported higher prevalence of G2P[4] where RV1 is being used and an increase in G3P[8] where RV5 is in use. However, information to date suggests that these trends may simply reflect natural strain variation rather than escape from vaccine immunity [75,107–113]. Long-term vaccine effectiveness studies could provide a good platform to continuously assess levels of protection against individual serotypes to determine whether
strain evolution leads to reduced vaccine effectiveness. Since the rate at which potential strains that evade immunity evolve in an immune population is unknown, conducting such investigations over a period of years after high vaccine uptake has been achieved may be important. Accompanying genetic characterization of rota-viral strains from effectiveness studies will be important to assess possible immune escape mechanisms.
To have optimal public health impact, vaccines should protect against severe rotavirus disease during the period when most severe disease occurs, the first 2 years of life in developing coun-tries and the first 3 years of life in developed countries. Data from Europe and Latin America suggest that there is a slight decrease in efficacy from the first to the second rotavirus season of follow-up, but overall protection was sustained at reasonable levels [5,58,59,104]. This decrease in efficacy might be greater in the developing world but further data are needed. Effectiveness of partial vaccination is also important as some severe disease occurs prior to completion of the full series and protection against breakthrough disease is important.
Several additional rotavirus vaccines are currently in various stages of development including vaccines based on neonatal rota-virus strains in India [114,115] and Australia [116,117]; a neonatal dosing schedule of the previously withdrawn RRV-TV to address the intussusception issue [118]; and a designer vaccine based on a bovine strain that could include additional serotypes such as G8 and G9, which are common in some developing countries [119], and that has been licensed to vaccine manufacturers in Brazil, China and India. These vaccines may offer less expensive alternatives to the currently available vaccines. Neonatal rotavirus strains have been found in nosocomial outbreaks of asymptomatic infections in newborn units. However, neonatal rotavirus strains usually do not cause disease in infants and have been shown to protect against severe rotavirus disease on reinfection [120,121]. A live, oral vaccine based on a lamb rotavirus strain has been used in China since 2001 but only limited data on safety, immunogenicity and effectiveness of this vaccine are available, which limits its wider use in other immunization programs [122,123]. In addition to these potential new oral vaccines, alternative approaches to rotavirus vaccine administration such as rotavirus antigens for parenteral delivery are also being explored so as to avoid a theoretical risk of intussusception [124–129]. A parenterally administered vaccine is not susceptible to risk factors (e.g., breastfeeding and interference from other floras in the gut) associated with live oral vaccines and thus could be equally immunogenic and effective in children in low-income countries.
Expert commentaryTwo live, oral rotavirus vaccines are currently available. These vaccines have shown high postlicensure effectiveness in high- and middle-income countries. Furthermore, increasing vaccine cover-age has been correlated with decreases in diarrhea and rotavirus morbidity in these settings. Early data from clinical trials in Africa and Asia suggest that vaccines will have moderate effi-cacy in these settings, but even a moderately effective vaccine would have a substantial public health impact in these settings
Tate, Patel, Steele et al.

www.expert-reviews.com 403
Review
Key issues
• Two live, orally administered rotavirus vaccines are currently available for use.
• The WHO recommends the inclusion of rotavirus vaccines in the national immunization programs of all countries.
• Clinical trials and postlicensure monitoring in high- and middle-income countries have found rotavirus vaccines to be highly effective against rotavirus gastroenteritis and demonstrate substantial public health impact.
• Studies of rotavirus vaccines in low-income countries have shown moderate efficacy, but even a moderately effective vaccine will have substantial public health benefit in these high-burden settings.
• Further study of rotavirus vaccines in low-income countries is needed to determine the potential impact of immunization against rotavirus in these settings and identify ways to improve impact.
ReferencesPapers of special note have been highlighted as:• of interest
1 Parashar UD, Gibson CJ, Bresse JS, Glass RI. Rotavirus and severe childhood diarrhea. Emerg. Infect. Dis. 12(2), 304–306 (2006).
2 Parashar UD, Burton A, Lanata C et al. Global mortality associated with rotavirus disease among children in 2004. J. Infect. Dis. 200(Suppl. 1), S9–S15 (2009).
3 Glass RI, Bresee JS, Turcios R, Fischer TK, Parashar UD, Steele AD. Rotavirus vaccines: targeting the developing world. J. Infect. Dis. 192(Suppl. 1), S160–S166 (2005).
4 Ruiz-Palacios GM, Perez-Schael I, Velazquez FR et al. Safety and efficacy of an attenuated vaccine against severe rotavirus gastroenteritis. N. Engl. J. Med. 354(1), 11–22 (2006).
• PresentsresultsfromlargePhaseIIIclinicaltrialsindevelopedcountries
showingthatthemonovalentrotavirusvaccineisefficaciousagainstsevererotavirusdisease.
5 Vesikari T, Matson DO, Dennehy P et al. Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N. Engl. J. Med. 354(1), 23–33 (2006).
• PresentsresultsfromlargePhaseIIIclinicaltrialsindevelopedcountriesshowingthatthepentavalentrotavirusvaccineisefficaciousagainstsevererotavirusdisease.
6 Conclusions and recommendations from the Immunization Strategic Advisory Group. Wkly Epidemiol. Rec. 81(1), 2–11 (2006).
7 Meeting of the immunization Strategic Advisory Group of Experts, April 2009 – conclusions and recommendations. Wkly Epidemiol. Rec. 84(23), 220–236 (2009).
8 Rotavirus vaccines: an update. Wkly Epidemiol. Rec. 84(51–52), 533–540 (2009).
• PresentsrecommendationoftheWHOtoincluderotavirusvaccineinthenationalimmunizationprogramsofallcountries.
9 Meeting of the Strategic Advisory Group of Experts on immunization, October 2009 – conclusions and recommendations. Wkly Epidemiol. Rec. 84(50), 517–532 (2009).
10 Estes MK, Cohen J. Rotavirus gene structure and function. Microbiol. Rev. 53(4), 410–449 (1989).
11 Estes MK, Kapikian AZ. Rotaviruses. In: Field’s Virology (5th Edition). Knipe DM, Howley PM (Eds). Lippincott, Williams and Williams, PA, USA, 1917–1958 (2007).
12 Gentsch JR, Parashar UD, Glass RI. Impact of rotavirus vaccination: the importance of monitoring strains. Future Microbiol. 4, 1231–1234 (2009).
13 Ball JM, Tian P, Zeng CQ, Morris AP, Estes MK. Age-dependent diarrhea induced by a rotaviral nonstructural glycoprotein. Science 272(5258), 101–104 (1996).
with high disease burden. Thus, the WHO has recommended that rotavirus vaccines be introduced into the national immuni-zations programs of all countries worldwide. To improve vac-cine performance and achieve the greatest public health impact, additional research is needed to ensure that these vaccines reach their fullest potential.
Five-year viewPostlicensure data showing high effectiveness of rotavirus vaccines in routine use in high- and middle-income countries and promis-ing efficacy data from clinical trials in Africa and Asia suggest that rotavirus vaccine will have substantial impact on global rotavirus morbidity and mortality as these vaccines are introduced into countries’ national immunization programs. However, to reap the full benefit of rotavirus vaccination, further study of rotavi-rus vaccines in developing countries should continue to explore ways to improve vaccine performance in settings where rota-virus morbidity and mortality is highest. Specifically, these studies could examine the impact that delaying age at first vaccination, offering neonatal vaccination, increasing the number of doses, altering breastfeed-ing practices, and using zinc or probiotic supplementation will have on vaccine per-formance. In addition, new data will enable us to further understand the impact of the introduction of rotavirus vaccine on key epidemiological issues including vaccine performance against severe disease during routine use, vaccine impact on rotavirus disease epidemiology, including changes
in burden of severe disease and death, age distribution of cases, seasonality and serotype distribution, herd protection for unvac-cinated children, and duration of protection. This information will enable us to use vaccines to their fullest potential.
Financial & competing interests disclosureNigel A Cunliffe has received research grant support and lecture fees from GSK Biologicals and SPMSD. Osamu Nakagomi has received research grants from GlaxoSmithKline and Banyu Pharmatheuticals. Jacqueline E Tate, Manish M Patel, A Duncan Steele, Jon R Gentsch, Daniel C Payne, Margaret M Cortese, Baoming Jiang, Roger I Glass and Umesh D Parashar do not have any relevant disclosures. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Global impact of rotavirus vaccines

404
Review
Expert Rev. Vaccines 9(4), (2010)
14 Rodriguez WJ, Kim HW, Brandt CD et al. Longitudinal study of rotavirus infection and gastroenteritis in families served by a pediatric medical practice: clinical and epidemiologic observations. Pediatr. Infect. Dis. J. 6(2), 170–176 (1987).
15 Glass RI, Kilgore PE, Holman RC et al. The epidemiology of rotavirus diarrhea in the United States: surveillance and estimates of disease burden. J. Infect. Dis. 174(Suppl. 1), S5–S11 (1996).
16 Gurwith M, Wenman W, Hinde D, Feltham S, Greenberg H. A prospective study of rotavirus infection in infants and young children. J. Infect. Dis. 144(3), 218–224 (1981).
17 Carlson JA, Middleton PJ, Szymanski MT, Huber J, Petric M. Fatal rotavirus gastroenteritis: an analysis of 21 cases. Am. J. Dis. Child. 132(5), 477–479 (1978).
18 Blutt SE, Matson DO, Crawford SE et al. Rotavirus antigenemia in children is associated with viremia. PLoS Med. 4(4), e121 (2007).
19 Blutt SE, Kirkwood CD, Parreno V et al. Rotavirus antigenaemia and viraemia: a common event? Lancet 362(9394), 1445–1449 (2003).
20 Chiappini E, Azzari C, Moriondo M, Galli L, de Martino M. Viraemia is a common finding in immunocompetent children with rotavirus infection. J. Med. Virol. 76(2), 265–267 (2005).
21 Chitambar SD, Tatte VS, Dhongde R, Kalrao V. High frequency of rotavirus viremia in children with acute gastroenteritis: discordance of strains detected in stool and sera. J. Med. Virol. 80(12), 2169–2176 (2008).
22 Ray P, Fenaux M, Sharma S et al. Quantitative evaluation of rotaviral antigenemia in children with acute rotaviral diarrhea. J. Infect. Dis. 194(5), 588–593 (2006).
23 Velazquez FR, Matson DO, Calva JJ et al. Rotavirus infections in infants as protection against subsequent infections. N. Engl. J. Med. 335(14), 1022–1028 (1996).
24 Black RE, Lopez de Romana G et al. Incidence and etiology of infantile diarrhea and major routes of transmission in Huascar, Peru. Am. J. Epidemiol. 129(4), 785–799 (1989).
25 Mrukowicz J, Szajewska H, Vesikari T. Options for the prevention of rotavirus disease other than vaccination. J. Pediatr. Gastroenterol. Nutr. 46(Suppl. 2), S32–S37 (2008).
26 Simhon A, Mata L, Vives M et al. Low endemicity and low pathogenicity of rotaviruses among rural children in Costa Rica. J. Infect. Dis. 152(6), 1134–1142 (1985).
27 Zaki AM, DuPont HL, el Alamy MA et al. The detection of enteropathogens in acute diarrhea in a family cohort population in rural Egypt. Am. J. Trop. Med. Hyg. 35(5), 1013–1022 (1986).
28 Bishop RF, Barnes GL, Cipriani E, Lund JS. Clinical immunity after neonatal rotavirus infection. A prospective longitudinal study in young children. N. Engl. J. Med. 309(2), 72–76 (1983).
29 Snodgrass DR, Wells PW. Rotavirus infection in lambs: studies on passive protection. Arch. Virol. 52(3), 201–205 (1976).
30 Midthun K, Kapikian AZ. Rotavirus vaccines: an overview. Clin. Microbiol. Rev. 9(3), 423–434 (1996).
31 Vesikari T, Isolauri E, D’Hondt E, Delem A, Andre FE, Zissis G. Protection of infants against rotavirus diarrhoea by RIT 4237 attenuated bovine rotavirus strain vaccine. Lancet 1(8384), 977–981 (1984).
32 Vesikari T, Isolauri E, Delem A et al. Clinical efficacy of the RIT 4237 live attenuated bovine rotavirus vaccine in infants vaccinated before a rotavirus epidemic. J. Pediatr. 107(2), 189–194 (1985).
33 Ruuska T, Vesikari T, Delem A, Andre FE, Beards GM, Flewett TH. Evaluation of RIT 4237 bovine rotavirus vaccine in newborn infants: correlation of vaccine efficacy to season of birth in relation to rotavirus epidemic period. Scand J. Infect. Dis. 22(3), 269–278 (1990).
34 Vesikari T. Clinical trials of live oral rotavirus vaccines: the Finnish experience. Vaccine 11(2), 255–261 (1993).
35 Vesikari T, Ruuska T, Delem A, Andre FE. Neonatal rotavirus vaccination with RIT 4237 bovine rotavirus vaccine: a preliminary report. Pediatr. Infect. Dis. J. 6(2), 164–169 (1987).
36 Vesikari T, Ruuska T, Delem A, Andre FE, Beards GM, Flewett TH. Efficacy of two doses of RIT 4237 bovine rotavirus vaccine for prevention of rotavirus diarrhoea. Acta Paediatr. Scand. 80(2), 173–180 (1991).
37 Hanlon P, Hanlon L, Marsh V et al. Trial of an attenuated bovine rotavirus vaccine (RIT 4237) in Gambian infants. Lancet 1(8546), 1342–1345 (1987).
38 De Mol P, Zissis G, Butzler JP, Mutwewingabo A, Andre FE. Failure of live, attenuated oral rotavirus vaccine. Lancet 2(8498), 108 (1986).
39 Lanata CF, Black RE, del Aguila R et al. Protection of Peruvian children against rotavirus diarrhea of specific serotypes by one, two, or three doses of the RIT 4237 attenuated bovine rotavirus vaccine. J. Infect. Dis. 159(3), 452–459 (1989).
40 Georges-Courbot MC, Monges J, Siopathis MR et al. Evaluation of the efficacy of a low-passage bovine rotavirus (strain WC3) vaccine in children in Central Africa. Res. Virol. 142(5), 405–411 (1991).
41 Flores J, Perez-Schael I, Gonzalez M et al. Protection against severe rotavirus diarrhoea by rhesus rotavirus vaccine in Venezuelan infants. Lancet 1(8538), 882–884 (1987).
42 Perez-Schael I, Garcia D, Gonzalez M et al. Prospective study of diarrheal diseases in Venezuelan children to evaluate the efficacy of rhesus rotavirus vaccine. J. Med. Virol. 30(3), 219–229 (1990).
43 Pérez-Schael I, Guntiñas MJ, Pérez M et al. Efficacy of the rhesus rotavirus-based quadrivalent vaccine in infants and young children in Venezuela. N. Engl. J. Med. 337, 1181–1187 (1997).
44 Joensuu J, Koskenniemi E, Pang XL, Vesikari T. Randomised placebo-controlled trial of rhesus-human reassortant rotavirus vaccine for prevention of severe rotavirus gastroenteritis. Lancet 350(9086), 1205–1209 (1997).
45 Bernstein DI, Glass RI, Rodgers G, Davidson BL, Sack DA. Evaluation of rhesus rotavirus monovalent and tetravalent reassortant vaccines in US children. US Rotavirus Vaccine Efficacy Group. JAMA 273(15), 1191–1196 (1995).
46 Rotavirus vaccine for the prevention of rotavirus gastroenteritis among children. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 48(RR-2), 1–20 (1999).
47 Withdrawal of rotavirus vaccine recommendation. MMWR Morb. Mortal. Wkly Rep. 48(43), 1007 (1999).
48 Intussusception among recipients of rotavirus vaccine – United States, 1998–1999. MMWR Morb. Mortal. Wkly Rep. 48(27), 577–581 (1999).
49 Murphy TV, Gargiullo PM, Massoudi MS et al. Intussusception among infants given an oral rotavirus vaccine. N. Engl. J. Med. 344(8), 564–572 (2001).
Tate, Patel, Steele et al.

www.expert-reviews.com 405
Review
50 Peter G, Myers MG. Intussusception, rotavirus, and oral vaccines: summary of a workshop. Pediatrics 110(6), e67 (2002).
51 Simonsen L, Viboud C, Elixhauser A, Taylor RJ, Kapikian AZ. More on RotaShield and intussusception: the role of age at the time of vaccination. J. Infect. Dis. 192(Suppl. 1), S36–S43 (2005).
52 Rothman KJ, Young-Xu Y, Arellano F. Age dependence of the relation between reassortant rotavirus vaccine (RotaShield) and intussusception. J. Infect. Dis. 193(6), 898; author reply 898–899 (2006).
53 Global Advisory Committee on Vaccine Safety, 1–2 December 2005. Wkly Epidemiol. Rec. 81(2), 15–19 (2006).
54 International Medica Foundation. Milestone in Phase II Clinical Trial for Rotavirus Vaccine Reached. International Medica Foundation, MN, USA (2009).
55 Heaton PM, Goveia MG, Miller JM, Offit P, Clark HF. Development of a pentavalent rotavirus vaccine against prevalent serotypes of rotavirus gastroenteritis. J. Infect. Dis. 192(Suppl. 1), S17–S21 (2005).
56 Bernstein DI, Smith VE, Sherwood JR et al. Safety and immunogenicity of live, attenuated human rotavirus vaccine 89–12. Vaccine 16(4), 381–387 (1998).
57 De Vos B, Vesikari T, Linhares AC et al. A rotavirus vaccine for prophylaxis of infants against rotavirus gastroenteritis. Pediatr. Infect. Dis. J. 23(10 Suppl.), S179–S182 (2004).
58 Vesikari T, Karvonen A, Prymula R et al. Efficacy of human rotavirus vaccine against rotavirus gastroenteritis during the first 2 years of life in European infants: randomised, double-blind controlled study. Lancet 370(9601), 1757–1763 (2007).
59 Linhares AC, Velazquez FR, Perez-Schael I et al. Efficacy and safety of an oral live attenuated human rotavirus vaccine against rotavirus gastroenteritis during the first 2 years of life in Latin American infants: a randomised, double-blind, placebo-controlled Phase III study. Lancet 371(9619), 1181–1189 (2008).
60 Keating GM. Rotavirus vaccine RIX4414 (Rotarix). Paediatr. Drugs 8(6), 389–395; discussion 396–387 (2006).
61 De Vos B, Han HH, Bouckenooghe A et al. Live attenuated human rotavirus vaccine, RIX4414, provides clinical protection in infants against rotavirus strains with and without shared G and P genotypes: integrated analysis of randomized controlled trials. Pediatr. Infect. Dis. J. 28(4), 261–266 (2009).
62 Madhi SA, Cunliffe NA, Steele AD et al. Impact of human rotavirus vaccine on severe gastroenteritis in African infants: a multicentre clinical trial. N. Engl. J. Med. 362(4), 289–298 (2010).
• PresentsresultsfromPhaseIIIclinicaltrialsintwoAfricancountriesshowingthatthemonovalentrotavirusvaccineisefficaciousagainstsevererotavirusdiseaseandpreventssubstantialdiseaseburden.
63 Cortese MM, Parashar UD. Prevention of rotavirus gastroenteritis among infants and children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 58(RR-2), 1–25 (2009).
64 Boom JA, Tate JE, Sahni LC et al. Effectiveness of Pentavalent rotavirus vaccine in a large, urban US population. Pediatrics 125(2), e199–e207 (2010).
65 Tate JE, Panozzo CA, Payne DC et al. Decline and change in seasonality of US rotavirus activity after the introduction of rotavirus vaccine. Pediatrics 124(2), 465–471 (2009).
66 Reduction in rotavirus after vaccine introduction – United States, 2000–2009. MMWR Morb. Mortal. Wkly Rep. 58(41), 1146–1149 (2009).
67 Cortese MM, Tate JE, Simonsen L, Edelman L, Parashar UD. Reduction in gastroenteritis in children and correlation with early rotavirus vaccine uptake from a national medical claims database. Pediatr. Infect. Dis. J. (2010) (In Press).
68 Lambert SB, Faux CE, Hall L et al. Early evidence for direct and indirect effects of the infant rotavirus vaccine program in Queensland. Med. J. Aust. 191(3), 157–160 (2009).
69 Snelling TL, Schultz R, Graham J et al. Rotavirus and the indigenous children of the Australian outback: monovalent vaccine effective in a high-burden setting. Clin. Infect. Dis. 49(3), 428–431 (2009).
70 Snelling TL, Andrews RM, Kirkwood CD, Carapetis JR. Evaluation of the monovalent human rotavirus vaccine RIX4414 following a G2P[4] outbreak. Presented at: 26th meeting of the 49th Annual Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC). San Francisco, CA, USA, 12–15 September 2009.
71 Paulke-Korinek M, Rendi-Wagner P, Kundi M, Kronik R, Kollaritsch H. Universal mass vaccination against rotavirus gastroenteritis: impact on
hospitalization rates in austrian children. Pediatr. Infect. Dis. J. DOI: 10.1097/INF.0b013e3181c18434 (2009).
72 Gurgel RQ, Cuevas LE, Vieira SC et al. Predominance of rotavirus P[4]G2 in a vaccinated population, Brazil. Emerg. Infect. Dis. 13(10), 1571–1573 (2007).
73 Gurgel RQ, Correia JB, Cuevas LE. Effect of rotavirus vaccination on circulating virus strains. Lancet 371(9609), 301–302 (2008).
74 Nakagomi T, Cuevas LE, Gurgel RG et al. Apparent extinction of non-G2 rotavirus strains from circulation in Recife, Brazil, after the introduction of rotavirus vaccine. Arch. Virol. 153(3), 591–593 (2008).
75 Gurgel RQ, Bohland AN, Vieira SA et al. Incidence of rotavirus and all-cause diarrhea in northeast brazil following the introduction of a national vaccination program. Gastroenterology 137, 1970–1975 (2009).
76 Patel MM, de Oliveira LH, Bispo AM, Gentsch J, Parashar UD. Rotavirus P[4]G2 in a vaccinated population, Brazil. Emerg. Infect. Dis. 14(5), 863–865 (2008).
77 Correia JB, Patel MM, Nakagomi O et al. Effectiveness of monovalent rotavirus vaccine (rotarix) against severe diarrhoea caused by serotypically-unrelated G2P[4] strains in Brazil. J. Infect. Dis. 201(3), 363–369 (2010).
78 Richardson V, Hernandez-Pichardo J, Quintanar-Solares M et al. Reduction in childhood diarrhea deaths after rotavirus vaccine introduction in Mexico. N. Engl. J. Med. 362(4), 299–305 (2010).
79 Patel M, Pedreira C, De Oliveira LH et al. Association between pentavalent rotavirus vaccine and severe rotavirus diarrhea among children in Nicaragua. JAMA 301(21), 2243–2251 (2009).
80 Orozco M, Vasquez J, Pedreira C et al. Uptake of rotavirus vaccine and national trends of acute gastroenteritis among children in Nicaragua. J. Infect. Dis. 200(Suppl. 1), S125–S130 (2009).
81 Belongia EA, Irving SA, Shui IM et al. Real-time surveillance to assess risk of intussusception and other adverse events after pentavalent, bovine-derived rotavirus vaccine. Pediatr. Infect. Dis. J. 29(1), 1–5 (2010).
82 Haber P, Patel M, Izurieta HS et al. Postlicensure monitoring of intussusception after RotaTeq vaccination in the United States, February 1, 2006, to September 25, 2007. Pediatrics 121(6), 1206–1212 (2008).
Global impact of rotavirus vaccines

406
Review
Expert Rev. Vaccines 9(4), (2010)
83 Patel MM, Haber P, Baggs J, Zuber P, Bines JE, Parashar UD. Intussusception and rotavirus vaccination: a review of the available evidence. Expert Rev. Vaccines 8(11), 1555–1564 (2009).
84 Patel NC, Hertel PM, Estes MK et al. Vaccine-acquired rotavirus in infants with severe combined immunodeficiency. N. Engl. J. Med. 362(4), 314–319 (2010).
85 RotaTeq® (Package Insert). Merck & Co., Inc., NJ, USA (2009)
86 Zaman K, Sack DA, Yunus M et al. Successful co-administration of a human rotavirus and oral poliovirus vaccines in Bangladeshi infants in a 2-dose schedule at 12 and 16 weeks of age. Vaccine 27(9), 1333–1339 (2009).
87 Ciarlet M, Sani-Grosso R, Yuan G et al. Concomitant use of the oral pentavalent human-bovine reassortant rotavirus vaccine and oral poliovirus vaccine. Pediatr. Infect. Dis. J. 27(10), 874–880 (2008).
88 Patel MM, Clark AD, Glass RI et al. Broadening the age restriction for initiating rotavirus vaccination in regions with high rotavirus mortality: benefits of mortality reduction versus risk of fatal intussusception. Vaccine 27(22), 2916–2922 (2009).
89 Clark A, Sanderson C. Timing of children’s vaccinations in 45 low-income and middle-income countries: an analysis of survey data. Lancet 373(9674), 1543–1549 (2009).
90 John TJ. Antibody response of infants in tropics to five doses of oral polio vaccine. Br. Med. J. 1(6013), 812 (1976).
91 John TJ, Jayabal P. Oral polio vaccination of children in the tropics. I. The poor seroconversion rates and the absence of viral interference. Am. J. Epidemiol. 96(4), 263–269 (1972).
92 Patriarca PA, Wright PF, John TJ. Factors affecting the immunogenicity of oral poliovirus vaccine in developing countries: review. Rev. Infect. Dis. 13(5), 926–939 (1991).
93 Suharyono, Simanjuntak C, Witham N et al. Safety and immunogenicity of single-dose live oral cholera vaccine CVD 103-HgR in 5–9-year-old Indonesian children. Lancet 340(8821), 689–694 (1992).
94 Gotuzzo E, Butron B, Seas C et al. Safety, immunogenicity, and excretion pattern of single-dose live oral cholera vaccine CVD 103-HgR in Peruvian adults of high and low socioeconomic levels. Infect. Immun. 61(9), 3994–3997 (1993).
95 Linhares AC, Gabbay YB, Mascarenhas JD et al. Immunogenicity, safety and efficacy of tetravalent rhesus-human, reassortant rotavirus vaccine in Belem, Brazil. Bull. World Health Organ. 74(5), 491–500 (1996).
96 Patel M, Shane AL, Parashar UD, Jiang B, Gentsch JR, Glass RI. Oral rotavirus vaccines: how well will they work where they are needed most? J. Infect. Dis. 200(Suppl. 1), S39–S48 (2009).
97 Glass RI, Parashar UD, Bresee JS et al. Rotavirus vaccines: current prospects and future challenges. Lancet 368(9532), 323–332 (2006).
98 Rennels MB. Influence of breast-feeding and oral poliovirus vaccine on the immunogenicity and efficacy of rotavirus vaccines. J. Infect. Dis. 174(Suppl. 1), S107–S111 (1996).
99 Moon KB. Differential rotavirus antibody profiles in breast milk specimens from mothers with infants in developed and developing countries. Presented at: American Society for Virology Conference. Vancouver, BC, Canada, 11–15 July 2009.
100 Steele AD, De Vos B, Tumbo J et al. Co-administration study in South African infants of a live-attenuated oral human rotavirus vaccine (RIX4414) and poliovirus vaccines. Vaccine DOI:10.1016/j.vaccine.2008.08.034 (2008) (Epub ahead of print).
101 Santos N, Hoshino Y. Global distribution of rotavirus serotypes/genotypes and its implication for the development and implementation of an effective rotavirus vaccine. Rev. Med. Virol. 15(1), 29–56 (2005).
102 Sanchez-Padilla E, Grais RF, Guerin PJ, Steele AD, Burny ME, Luquero FJ. Burden of disease and circulating serotypes of rotavirus infection in sub-Saharan Africa: systematic review and meta-analysis. Lancet Infect. Dis. 9(9), 567–576 (2009).
103 Steele AD, Ivanoff B. Rotavirus strains circulating in Africa during 1996–1999: emergence of G9 strains and P[6] strains. Vaccine 21(5–6), 361–367 (2003).
104 Vesikari T, Karvonen A, Puustinen L et al. Efficacy of RIX4414 live attenuated human rotavirus vaccine in Finnish infants. Pediatr. Infect. Dis. J. 23(10), 937–943 (2004).
105 Patel MM, Parashar UD. Assessing the effectiveness and public health impact of rotavirus vaccines after introduction in immunization programs. J. Infect. Dis. 200(Suppl. 1), S291–S299 (2009).
106 Matthijnssens J, Bilcke J, Ciarlet M et al. Rotavirus disease and vaccination: impact of genotype diversity. Future Microbiol. 4(10), 1303–1316 (2009).
107 Kirkwood C, Boniface C, Barnes G, Bishop R. Rotavirus genotype distribution in Australian children – what has happened during the first 18 months after introduction of RotaTeq™ and Rotarix™. Presented at: Vaccines for Enteric Diseases Meeting. Malaga, Spain, 9–11 September 2009.
108 Gurgel RQ, Correia JB, Cuevas LE. Effect of rotavirus vaccination on circulating virus strains [comment]. Lancet 371(9609), 301–302 (2008).
109 Leite JP, Carvalho-Costa FA, Linhares AC. Group A rotavirus genotypes and the ongoing Brazilian experience: a review. Mem. Inst. Oswaldo Cruz. 103(8), 745–753 (2008).
110 Nakagomi T, Cuevas LE, Gurgel RG et al. Apparent extinction of non-G2 rotavirus strains from circulation in Recife, Brazil, after the introduction of rotavirus vaccine. Arch. Virol. 153(3), 591–593 (2008).
111 Patel MM, de Oliveira LH, Bispo AM et al. Rotavirus P[4]G2 in a vaccinated population, Brazil [comment]. Emerg. Infect. Dis. 14(5), 863–865 (2008).
112 Hull J, Teel E, Kerin T et al. Report of the U.S. rotavirus strain surveillance (1996–2008). Presented at: American Society for Microbiology Meeting. BC, Canada, 17–21 July 2009.
113 Payne DC, Szilagyi PG, Staat MA et al. Secular variation in United States rotavirus disease rates and serotypes: implications for assessing the rotavirus vaccination program. Pediatr. Infect. Dis. J. 28(11), 948–953 (2009).
114 Bhandari N, Sharma P, Taneja S et al. A dose-escalation safety and immunogenicity study of live attenuated oral rotavirus vaccine 116E in infants: a randomized, double-blind, placebo-controlled trial. J. Infect. Dis. 200(3), 421–429 (2009).
115 Bhandari N, Sharma P, Glass RI et al. Safety and immunogenicity of two live attenuated human rotavirus vaccine candidates, 116E and I321, in infants: results of a randomised controlled trial. Vaccine 24(31–32), 5817–5823 (2006).
116 Barnes GL, Lund JS, Adams L et al. Phase 1 trial of a candidate rotavirus vaccine (RV3) derived from a human neonate. J. Paediatr. Child Health 33(4), 300–304 (1997).
Tate, Patel, Steele et al.

www.expert-reviews.com 407
Review
117 Barnes GL, Lund JS, Mitchell SV et al. Early Phase II trial of human rotavirus vaccine candidate RV3. Vaccine 20(23–24), 2950–2956 (2002).
118 Ruiz LP Jr. Rotavirus vaccines. N. Engl. J. Med. 354(16), 1747–1751; author reply 1747–1751 (2006).
119 Kapikian AZ, Simonsen L, Vesikari T et al. A hexavalent human rotavirus-bovine rotavirus (UK) reassortant vaccine designed for use in developing countries and delivered in a schedule with the potential to eliminate the risk of intussusception. J. Infect. Dis. 192(Suppl. 1), S22–S29 (2005).
120 Bhan MK, Lew JF, Sazawal S, Das BK, Gentsch JR, Glass RI. Protection conferred by neonatal rotavirus infection against subsequent rotavirus diarrhea. J. Infect. Dis. 168(2), 282–287 (1993).
121 Vethanayagam RR, Ananda Babu M, Nagalaxmi KS et al. Possible role of neonatal infection with the asymptomatic reassortant rotavirus (RV) strain I321 in the decrease in hospital admissions for RV diarrhea, Bangalore, India, 1988–1999. J. Infect. Dis. 189(12), 2282–2289 (2004).
122 Mohan KV, Kulkarni S, Glass RI, Zhisheng B, Atreya CD. A human vaccine strain of lamb rotavirus (Chinese) NSP4 gene: complete nucleotide sequence and phylogenetic analyses. Virus Genes 26(2), 185–192 (2003).
123 Fu C, Wang M, Liang J, He T, Wang D, Xu J. Effectiveness of Lanzhou lamb rotavirus vaccine against rotavirus gastroenteritis requiring hospitalization: a matched case-control study. Vaccine 25(52), 8756–8761 (2007).
124 Ciarlet M, Crawford SE, Barone C et al. Subunit rotavirus vaccine administered parenterally to rabbits induces active protective immunity. J. Virol. 72(11), 9233–9246 (1998).
125 Jiang B, Estes MK, Barone C et al. Heterotypic protection from rotavirus infection in mice vaccinated with virus-like particles. Vaccine 17(7–8), 1005–1013 (1999).
126 Herrmann JE, Chen SC, Fynan EF et al. Protection against rotavirus infections by DNA vaccination. J. Infect. Dis. 174(Suppl. 1), S93–S97 (1996).
127 Coffin SE, Klinek M, Offit PA. Induction of virus-specific antibody production by lamina propria lymphocytes following intramuscular inoculation with rotavirus. J. Infect. Dis. 172(3), 874–878 (1995).
128 Conner ME, Crawford SE, Barone C, Estes MK. Rotavirus vaccine administered parenterally induces protective immunity. J. Virol. 67(11), 6633–6641 (1993).
129 Jiang B, Gentsch JR, Glass RI. Inactivated rotavirus vaccines: a priority for accelerated vaccine development. Vaccine 26(52), 6754–6758 (2008).
130 Parashar UD, Hummelman EG, Bresee JS, Miller MA, Glass RI. Global illness and deaths caused by rotavirus disease in children. Emerg. Infect. Dis. 9(5), 565–572 (2003).
Affiliations• Jacqueline E Tate, PhD
National Center for Immunization and Respiratory Diseases, US CDC, 1600 Clifton Rd. NE, MS-A47, Atlanta, GA 30333, USA Tel.: +1 404 639 4559 Fax: +1 404 639 8665 [email protected]
• Manish M Patel, MD, MSc National Center for Immunization and Respiratory Diseases, US CDC, Atlanta, GA, USA
• A Duncan Steele, PhD Rotavirus Vaccine Program, PATH, Seattle, WA, USA
• Jon R Gentsch, PhD National Center for Immunization and Respiratory Diseases, US CDC, Atlanta, GA, USA
• Daniel C Payne, PhD, MSPH National Center for Immunization and Respiratory Diseases, US CDC, Atlanta, GA, USA
• Margaret M Cortese, MD National Center for Immunization and Respiratory Diseases, US CDC, Atlanta, GA, USA
• Osamu Nakagomi, MD, PhD Department of Molecular Microbiology and Immunology, Graduate School of Biomedical Sciences, Nagasaki University, Nagasaki, Japan
• Nigel A Cunliffe, MBChB, PhD Department of Medical Microbiology and Genitourinary, Medicine, University of Liverpool, Liverpool, UK
• Baoming Jiang, PhD National Center for Immunization and Respiratory Diseases, US CDC, Atlanta, GA, USA
• Kathleen M Neuzil, MD, MPH Rotavirus Vaccine Program, PATH, Seattle, WA, USA
• Lucia H de Oliveira Immunization Unit, Family and Community Health, Pan American Health Organization, 525 23rd Street NW, Washington, DC 20037, USA
• Roger I Glass, MD, PhD Fogarty International Center, NIH, Bethesda, MD, USA
• Umesh D Parashar, MBBS, MPH National Center for Immunization and Respiratory Diseases, US CDC, Atlanta, GA, USA
Global impact of rotavirus vaccines