-
8/8/2019 06 Emergency Kuliah Emergency
1/67
EMERGENCYEMERGENCY
PEDIATRICPEDIATRIC
Dr. Idham Jaya Ganda, SpA(K)Dr. Idham Jaya Ganda, SpA(K)
PICU Subdiv. Child Health Dept
Medical Faculty, University of Hasanuddin
Dr. Wahidin Sudirohusodo HospitalMakassar
http://images.google.com/imgres?imgurl=http://www.pediatrics.ualberta.ca/emergency/images/Mask.jpg.jpg&imgrefurl=http://www.pediatrics.ualberta.ca/emergency/welcome.htm&h=1536&w=1028&sz=191&tbnid=j-DsWo7G15UJ:&tbnh=149&tbnw=100&start=43&prev=/images%3Fq%3Dpediatric%2Bemergency%26start%3D40%26hl%3Den%26lr%3D%26sa%3DNhttp://images.google.com/imgres?imgurl=http://www.pediatrics.ualberta.ca/emergency/images/Mask.jpg.jpg&imgrefurl=http://www.pediatrics.ualberta.ca/emergency/welcome.htm&h=1536&w=1028&sz=191&tbnid=j-DsWo7G15UJ:&tbnh=149&tbnw=100&start=43&prev=/images%3Fq%3Dpediatric%2Bemergency%26start%3D40%26hl%3Den%26lr%3D%26sa%3DNhttp://images.google.com/imgres?imgurl=http://www.pediatrics.ualberta.ca/emergency/images/Mask.jpg.jpg&imgrefurl=http://www.pediatrics.ualberta.ca/emergency/welcome.htm&h=1536&w=1028&sz=191&tbnid=j-DsWo7G15UJ:&tbnh=149&tbnw=100&start=43&prev=/images%3Fq%3Dpediatric%2Bemergency%26start%3D40%26hl%3Den%26lr%3D%26sa%3DNhttp://images.google.com/imgres?imgurl=http://www.pediatrics.ualberta.ca/emergency/images/Mask.jpg.jpg&imgrefurl=http://www.pediatrics.ualberta.ca/emergency/welcome.htm&h=1536&w=1028&sz=191&tbnid=j-DsWo7G15UJ:&tbnh=149&tbnw=100&start=43&prev=/images%3Fq%3Dpediatric%2Bemergency%26start%3D40%26hl%3Den%26lr%3D%26sa%3DNhttp://images.google.com/imgres?imgurl=http://www.pediatrics.ualberta.ca/emergency/images/Mask.jpg.jpg&imgrefurl=http://www.pediatrics.ualberta.ca/emergency/welcome.htm&h=1536&w=1028&sz=191&tbnid=j-DsWo7G15UJ:&tbnh=149&tbnw=100&start=43&prev=/images%3Fq%3Dpediatric%2Bemergency%26start%3D40%26hl%3Den%26lr%3D%26sa%3DN
-
8/8/2019 06 Emergency Kuliah Emergency
2/67
DENGUE SHOCKDENGUE SHOCK
SYNDROMESYNDROME
-
8/8/2019 06 Emergency Kuliah Emergency
3/67
ETIOLOGYETIOLOGY
Dengue VirusDengue Virus
UnclearUnclear
The Secondary HeterologousThe Secondary Heterologous
Infection HypothesisInfection Hypothesis
PATHOGENESISPATHOGENESIS
-
8/8/2019 06 Emergency Kuliah Emergency
4/67
CLINICALCLINICAL
MANIFESTASIONMANIFESTASION Fever: acute, high,
continuously,Fever: acute, high, continuously,
2-7 days2-7 days Bleeding manifestationBleeding
manifestation
Liver enlargementLiver enlargement
ShockShock
-
8/8/2019 06 Emergency Kuliah Emergency
5/67
-
8/8/2019 06 Emergency Kuliah Emergency
6/67
LABORATORIUMLABORATORIUM
Thrombocytopenia ( 100.000/mm Thrombocytopenia ( 100.000/mm33
oror
less)less)
Hem concentration ( Hct 20% or more)Hem concentration ( Hct 20%
or more)
-
8/8/2019 06 Emergency Kuliah Emergency
7/67
CLASSIFICATIONCLASSIFICATION
WHO CLASSIFICATION OF DHF (1975)WHO CLASSIFICATION OF DHF
(1975)
Grade IGrade I
Fever, Tourniquet test (+)Fever, Tourniquet test (+) Grade
IIGrade II
Grade I + spontaneous bleedingGrade I + spontaneous bleeding
Grade IIIGrade III
Grade II + Circulatory failureGrade II + Circulatory failure
Grade IVGrade IV
Profound shockProfound shock
Grade III & IVGrade III & IVDSSDSS
-
8/8/2019 06 Emergency Kuliah Emergency
8/67
TREATMENT DBD derajat III & IV
1. Oksigenasi (berikan O2 2-4 l/menit)
2. Penggantian volume plasma (cairan kristaloid isotonis)
Ringer laktat/NaCl 0,9 % / Asering
20 ml/kgBB secepatnya (bolus dalam 30 menit)
Evaluasi 30 menit, apakah syok teratasi ?
Syok teratasiSyok tidak teratasi
Kesadaran membaik
Nadi teraba kuat
Tekanan nadi > 20 mmHg
Tidak sesak nafas sianosis
Ekstremitas hangat
Diuresis cukup 1 ml/kgBB/jam
Kesadaran menurun
Nadi lembut / tidak teraba
Tekanan nadi < 20 mmHg
Distres pernafasan / sianosis
Kulit dingin dan lembab
Ekstremitas dingin
Periksa kadar gula darahCairan dan tetesan disesuaikan
10 ml/kgBB/jam
Pantau tanda vital tiap 10 menit
Catat balans cairan selama pemberian intravena
Lanjutkan cairan
20 ml/kgBB/jam
Evaluasi ketatTanda vital
Tanda perdarahan
Diuresis
Hb, Ht, trombosit
Tambahkan koloid/plasma
Dekstran/FPP
10-20 (max 30) ml/kgBB/jam
Stabil dalam 24 jam/Ht < 40
Tetesan 5 ml/kgBB/jam
Syok teratasi
Syok belum teratasi
Koreksi asidosis
Evaluasi 1 jam
Ht turun Ht tetap tinggi/ naikTetesan 3 ml/kgBB/jam
Infus stop tidak melebihi 48 jam
setelah syok teratasi
Tranfusi darah
Segar 10 ml/kgBB
diulang sesuai kebutuhan
Koloid 20 ml/kgBB
-
8/8/2019 06 Emergency Kuliah Emergency
9/67
MONITORINGMONITORING
Vital signsVital signs HctHct
-
8/8/2019 06 Emergency Kuliah Emergency
10/67
SEPTIC SHOCKSEPTIC SHOCK
-
8/8/2019 06 Emergency Kuliah Emergency
11/67
DEFINITIONDEFINITION
Septic syndromeSeptic syndrome
HypotensionHypotension
Responsive toResponsive to
treatmenttreatment
-
8/8/2019 06 Emergency Kuliah Emergency
12/67
ETIOLOGYETIOLOGY Neonates:Neonates: E. coliE. coli,,
StaphylococcusStaphylococcus
aureusaureus,, Streptococcus group BStreptococcus group B..
Child:Child: Streptococcus pneumonia, H.Streptococcus pneumonia,
H.
influenzae group B, Salmonella, S.influenzae group B,
Salmonella, S.aureus Stre tococcus rou A.
-
8/8/2019 06 Emergency Kuliah Emergency
13/67
Patofisiologi terjadinya syok septik
Infeksi Bakteri
Endorfin Produk Bakteri
mis. endotoksinAktivasi Komplemen
Makrofag
SitokinFaktor Jaringan
Aktivasi PMN.
Pelepasan PAF, produkArakidonat dan
Substansi toksik lainAktivasi
koagulasi
fibrinolisis
Aktivasi
kalikreinkinin
Vasodilatasi,
Kerusakan endotel
kapiler
Syok SeptikKebocoran kapiler,
kerusakan endotel
Kegagalan Organ Berganda
-
8/8/2019 06 Emergency Kuliah Emergency
14/67
CLINICALCLINICAL
MANIFESTATIONMANIFESTATION ChillingChilling
TachycardiaTachycardia
Hyperventilation/tachypneaHyperventilation/tachypnea
HypotensionHypotension ApateticApatetic AgitationAgitation
Bleeding manifestation (petechiae, purpura,Bleeding manifestation
(petechiae, purpura,
etc)etc) Neonates with immune disorder: unspecificNeonates with
immune disorder: unspecific
(lethargy, vomiting, abdominal pain,(lethargy, vomiting,
abdominal pain,h otermia h ertermiah otermia h ertermia
-
8/8/2019 06 Emergency Kuliah Emergency
15/67
DIAGNOSISDIAGNOSIS Clinical manifestationClinical
manifestation
Risk factorRisk factor Focus of infectionFocus of infection
Laboratory examination (bloodLaboratory examination (bloodsmear
culture
-
8/8/2019 06 Emergency Kuliah Emergency
16/67
TREATMENTTREATMENT
Infection control :Infection control : ampicillin &
aminoglycosideampicillin & aminoglycoside
Blood culture & sensitivity testBlood culture &
sensitivity test
Recovering tissue perfusion :Recovering tissue perfusion : fluid
resuscitation, acidfluid resuscitation, acid
base correction, cardiovascular medicines.base correction,
cardiovascular medicines. Respiratory function support :Respiratory
function support : oxygen/ ventilatoroxygen/ ventilator
Renal support :Renal support : diuretic medicines
(furosemide)diuretic medicines (furosemide)
CorticosteroidCorticosteroid
-
8/8/2019 06 Emergency Kuliah Emergency
17/67
DIARRHEA WITHDIARRHEA WITHDEHIDRATIONDEHIDRATION
-
8/8/2019 06 Emergency Kuliah Emergency
18/67
DEFINITIONDEFINITION
Watery stoolWatery stool
FrequencyFrequency 3X/ 243X/ 24
hours.hours.
-
8/8/2019 06 Emergency Kuliah Emergency
19/67
DEHYDRATION TYPESDEHYDRATION TYPES
IsotonicIsotonic
Na concentration 130-150meq/L orNa concentration 130-150meq/L
or
280 mosm/L280 mosm/L
Hypertonic:Hypertonic:
Na concentration > 150meq/L orNa concentration > 150meq/L
or
413 mosm/L413 mosm/L
Hypotonic:Hypotonic:
Na concentration
-
8/8/2019 06 Emergency Kuliah Emergency
20/67
DEHYDRATION GRADEDEHYDRATION GRADE
Cumulative losses (pwl, cwl, nwl)Cumulative losses (pwl, cwl,
nwl)
Mild : 5%Mild : 5%
Moderate : 5-10%Moderate : 5-10%Severe : >10%Severe :
>10%
Clinical manifestation ( scoring system)Clinical manifestation (
scoring system)
-
8/8/2019 06 Emergency Kuliah Emergency
21/67
Pemeriksaan
Angka Penilaian
1 2 3
Gambaran Klinik
Keadaan umum
Mata
MulutPernapasan
Turgor
Nadi
Baik
Normal
Normal20-30 per menit
Baik
Kuat / kurang
120 per menit
Lesu/haus
Cekung
Kering30-40 per menit
Kurang
120-140
per menit
Gelisah/renjatan
Sangat cekung
Sangat kering40-60 per menit
Jelek
Lebih 140
per menit
Derajat dehidrasi skor 6
diare tanpa
dehidrasi
skor 7-12
diare dehidrasi
ringan/sedang
skor 13 / lebih
diare dehidrasi
berat
-
8/8/2019 06 Emergency Kuliah Emergency
22/67
TREATMENTTREATMENT
Fluid therapy (Ringer Lactat orFluid therapy (Ringer Lactat
or
Ringer Asetat)Ringer Asetat)
Antibiotic therapyAntibiotic therapy
Acidosis therapyAcidosis therapy
-
8/8/2019 06 Emergency Kuliah Emergency
23/67
Umur
Cara Pemberian
Permulaan Lanjutan
Diare
Infantil
- PWL 125 ml
- NWL 100 ml
- CWL 25 ml250 ml
Kolera
PWL 100 ml/kg
4 jam pertama
60 ml/kg
1 jam pertama
30 ml/kg
20 jam berikut
190 ml/kg
7 jam berikut
70 ml/kg
PWL 100 ml/kg
Bayi kurang
12 bulan
Anak sama atau lebih 12
bulan
1 jam pertama
30 ml/kg
jam pertama
30 ml/kg
5 jam berikut
70 ml/kg
2 jam berikut
70 ml/kg
-
8/8/2019 06 Emergency Kuliah Emergency
24/67
ASTHMATICASTHMATIC
STATESTATE
-
8/8/2019 06 Emergency Kuliah Emergency
25/67
DEFINITIONDEFINITION
A severe asthma exacerbationA severe asthma exacerbation
which is not responsive to drugswhich is not responsive to
drugs
that are usually given for asthmathat are usually given for
asthma
exacerbation.exacerbation.
-
8/8/2019 06 Emergency Kuliah Emergency
26/67
ETIOLOGYETIOLOGY
MultifactorMultifactor
AllergenAllergen
RestlessnessRestlessness
EmotionEmotion
InfectionInfection
InheritedInherited
-
8/8/2019 06 Emergency Kuliah Emergency
27/67
PATHOGENESISPATHOGENESIS
Hyper responsiveness &Hyper responsiveness &
inflammation process of bronchusinflammation process of
bronchus
Hyper secretionHyper secretion EdemaEdema
BronchoconstrictionBronchoconstriction
-
8/8/2019 06 Emergency Kuliah Emergency
28/67
fication of Severity of Acute Asthma Exacerb
Parameters
Mild Moderate Severe Respiratory
Arrest
Imminent
Breathlessness Whilewalking
While talking While at rest
Talks Sentences Phrases Words
Position Can liedown Prefers sitting Sits upright
Alertness May beagitated
Usually
agitated
Always
agitated
Confused/
drowsy
Cyanotic - - + +++
Wheeze Moderate,often only
end
expiratory
Loud,
throughout
expiratory
inspiratory
Extremely loud,
can be heard
without
stethoscope
Absence of
wheeze
-
8/8/2019 06 Emergency Kuliah Emergency
29/67
Breathlessness Minimal Moderate Severe
Use of accessory
muscles
Usually not Commonly Always
Retractions Shallow,intercostals
Moderate, +
suprasternal
Deep, +
flare of alae
nasi
-
Respiratory rate Increased Increased Increased Decreased
Guide to rates of breathing in awake children:Age: Normal
rate:
< 2 month < 60 / minute2-12 months < 50 / minute
1-5 years < 40 / minute
6-8 years < 30 / minute
-
8/8/2019 06 Emergency Kuliah Emergency
30/67
Pulse Normal Tachycardia Tachycardia Bradycardia
Guide to normal pulse rates in children:
Age: Normal rate:
2-12 months < 160 / minute
1-2 years < 120 / minute3-8 years < 110 / minute
Pulsus
Paradoksus
None
< 10 mmHg
(+)
10-20 mmHg
(+)
> 20 mmHg
None
PEFR or FEV1
-before b.dilator-after b.dilator
(% pedicted
value)> 60%
> 80%
( % best value)
40-60%60-80%
< 40%
< 60 %respons < 2
jam
SaO2 > 95% 91-95% 90%
PaO2 Normal > 60 mmHg < 60 mmHg
PaCO2 < 45 mmHg < 45 mmHg > 45 mmHg
-
8/8/2019 06 Emergency Kuliah Emergency
31/67
CLINICALCLINICAL
MANIFESTATIONMANIFESTATION
CoughCough
WheezingWheezing
Tachypnea
Tachypnea
DyspneaDyspnea
Prolonged expirationProlonged expiration
RetractionRetraction
CyanosisCyanosis
TachycardiaTachycardia
-
8/8/2019 06 Emergency Kuliah Emergency
32/67
algorithmClinic/ER
Asses attack severity
1st managementnebulitation -agonis 3x, 20 min interval
3rd nebulitation + anticholinergic
Moderate attack(nebulization 2-3x,partial response)
give O2 asses: Moderate
ODC IV line
Mild attack(nebulization 1x,
complete response)
persist 1-2 hr:discharge
symptom reappear:Moderate attack
Severe attack(nebulization 3x,
no response)O2 from the startIV lineasses: Severe -
hospitalized CXR
-
8/8/2019 06 Emergency Kuliah Emergency
33/67
One Day Care (ODC)
Oxygen therapy Oral steroid Nebulized / 2 hour Observe 8-12
hours,if stabledischarge
Poor response in 12h,
admission
Admission room
Oxygen therapy Treat dehydration andacidosis
Steroid IV / 6-8 hours Nebulized / 1-2 hours Initial
aminophylline IV,
then maintenance Nebulized 4-6x good response per 4-6 h
If stable in 24 hours discharge Poor response ICU
Dischargegive -agonist(inhaled/oral)
routine drugs viral infection:oral steroid
Outpatient clinic in24-48 hours
Notes:In severe attack, directly use -agonist + anticholinergic
If nebulizers not available, use adrenalin SC 0.01 ml/kg/times with
maximal dose 0.3 ml/timesOxygen therapy 2-4 l/min should be early
treatment in moderate
and severe attack
-
8/8/2019 06 Emergency Kuliah Emergency
34/67
34
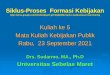
Figure. Jet nebulizerFigure. Jet nebulizer
-
8/8/2019 06 Emergency Kuliah Emergency
35/67
35
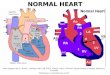
Figure. UltrasonicFigure. Ultrasonic
nebulizernebulizer
-
8/8/2019 06 Emergency Kuliah Emergency
36/67
-
8/8/2019 06 Emergency Kuliah Emergency
37/67
-
8/8/2019 06 Emergency Kuliah Emergency
38/67
38
DDrug dosage forrug dosage fornebulizernebulizer
DrugsNebulizer
Jet Ultrasound
NaCl 0.9% (ml) 5 10
2-agonist Alupent sol. 2% (gtt) Berotec 0.1% (gtt) Ventolin
nebule (mL)
Bricasma respule (mL)
3 5
5
1
1
3-5
5
1
1
Time (minutes) 10 - 15 3 - 5
-
8/8/2019 06 Emergency Kuliah Emergency
39/67
TREATMENT IN PICUTREATMENT IN PICU
Medicines atMedicines at
ward isward is
continuedcontinued
MechanicalMechanical
ventilatorventilator
-
8/8/2019 06 Emergency Kuliah Emergency
40/67
ACUTE RESPIRATORYACUTE RESPIRATORY
FAILUREFAILURE
-
8/8/2019 06 Emergency Kuliah Emergency
41/67
DEFINITIONDEFINITION
Respiratory system is unable toRespiratory system is unable
to
maintain its function hypoxia &maintain its function hypoxia
&
hypercapnea.hypercapnea.
-
8/8/2019 06 Emergency Kuliah Emergency
42/67
ETIOLOGYETIOLOGY
Increasing of coIncreasing of co22
Ventilated disorder without lungs dysfunctionVentilated disorder
without lungs dysfunction Ventilated disorder with lungs
dysfunctionVentilated disorder with lungs dysfunction
Ventilated disorder of death spaceVentilated disorder of death
space
C CCLINICAL
-
8/8/2019 06 Emergency Kuliah Emergency
43/67
CLINICALCLINICAL
MANIFESTATIONMANIFESTATION Symptoms of lungs disorderSymptoms of
lungs disorder ::
wheezing, grunting, flaring of alae nasi,wheezing, grunting,
flaring of alae nasi,
retraction, tachypnea, bradypnea, apnea,retraction, tachypnea,
bradypnea, apnea,
cyanosis.cyanosis. Signs of heart disorderSigns of heart
disorder ::
bradycardia/tachycardia,bradycardia/tachycardia,
hypotention/hypertention, cardiac
arrest.hypotention/hypertention, cardiac arrest.
Symptoms of CNS disorderSymptoms of CNS disorder ::
apatic, headache, convulsion, coma.apatic, headache, convulsion,
coma.
-
8/8/2019 06 Emergency Kuliah Emergency
44/67
TREATMENTTREATMENT
Airway (position, suction, ET)Airway (position, suction, ET)
Breathing (oxygen)Breathing (oxygen)
HumidificationHumidification
Bronchial washingBronchial washing PhysiotherapyPhysiotherapy
RehydrationRehydration Causal therapyCausal therapy Specific
therapy (mechanicalSpecific therapy (mechanical
ventilator)ventilator)
-
8/8/2019 06 Emergency Kuliah Emergency
45/67
EPILEPTIC STATUSEPILEPTIC STATUS
-
8/8/2019 06 Emergency Kuliah Emergency
46/67
DEFINITIONDEFINITION
Prolonged convulsion attackProlonged convulsion attack
(30 minutes or more)(30 minutes or more)
Recurrent convulsion in a short timeRecurrent convulsion in a
short time
as ifas ifno recoveryno recovery
-
8/8/2019 06 Emergency Kuliah Emergency
47/67
ETIOLOGYETIOLOGY Febrile convulsionFebrile convulsion
IdiopathicIdiopathic
SymptomaticSymptomatic
-
8/8/2019 06 Emergency Kuliah Emergency
48/67
PATHOFISIOLOGYPATHOFISIOLOGY CompensationCompensation
DecompensationDecompensation
-
8/8/2019 06 Emergency Kuliah Emergency
49/67
Age Type of epileptic state Features
Neo-
nates
Neonatal epileptic state
Neonatal syndromesepileptic
early infantile epilepticencephalopathy
neonatal myoclonicencephalopathy
benign familial neonatalseizures
- subtle, tonic,
clonic,myoclonic,apneic,fragmentary
- tonic- erratic, myoclonic- clonic
CLINICAL MANIFESTATIONCLINICAL MANIFESTATION
-
8/8/2019 06 Emergency Kuliah Emergency
50/67
Infant &
Child
Febrile epileptic state
Infantile spasms (westsyndromes)State in childhoodmyoclonic
syndromesState in benign partial
epilepsy
- convulsive or
hemiconvulsive (tonic-clonic)
- salaam attacks- myoclonic + absence- complex
partialseizures
Child &Adult
Tonic-clonic epileptic stateAbsence epileptic stateContinue
partially epilepticMyoclonic epileptic state in
comaMyoclonic epileptic statesyndromesComplex partial
epilepticstateEpileptic state in mental
retardation
- tonic-clonic, subtle- absence- simple partial- myoclonic
- myoclonic- complex partial- atypical absence, tonic,minor
motor
-
8/8/2019 06 Emergency Kuliah Emergency
51/67
TREATMENTTREATMENT
Initial treatment (stabilization)Initial treatment
(stabilization) PositionPosition ABCABC
Vital signs monitoringVital signs monitoring
Blood glucose & electrolyteBlood glucose &
electrolyte
AnticonvulsanAnticonvulsan Benzodiazepine ( diazepam,
midazolam)Benzodiazepine ( diazepam, midazolam)
PhenytoinPhenytoin
PhenobarbitalPhenobarbital
Cardiorespiratory & EEG monitoringCardiorespiratory &
EEG monitoring
Refracted treatmentRefracted treatment Barbiturate
(Phenobarbital, thiopental)Barbiturate (Phenobarbital,
thiopental)
Propofol & midazolamPropofol & midazolam
-
8/8/2019 06 Emergency Kuliah Emergency
52/67
INTUSSUSCEPTIONINTUSSUSCEPTION
-
8/8/2019 06 Emergency Kuliah Emergency
53/67
DEFINITIONDEFINITION
A condition where a section oA condition where a section of
intestine telescope into its selintestine telescope into its
self(proximal segment telescope into(proximal segment telescope
intodistal se ment of intestine .
PATHOFISIOLOGYPATHOFISIOLOGY
-
8/8/2019 06 Emergency Kuliah Emergency
54/67
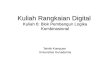
PATHOFISIOLOGYPATHOFISIOLOGY
IntussusceptionsIntussusceptions
-
8/8/2019 06 Emergency Kuliah Emergency
55/67
CLINICALCLINICAL
MANIFESTATIONMANIFESTATION ColicColic
VomitingVomiting Bloody stool , currant jelly stool &
terryBloody stool , currant jelly stool & terry
stoolstool
Sausage-shaped massSausage-shaped mass
Pseudo ortioPseudo ortio
-
8/8/2019 06 Emergency Kuliah Emergency
56/67
DIAGNOSISDIAGNOSIS ClinicalClinical
manifestationmanifestation
RadiologyRadiologyassessment:assessment:
Doughnut signDoughnut sign
Target signTarget sign Cu in si nCu in si n
-
8/8/2019 06 Emergency Kuliah Emergency
57/67
TREATMENTTREATMENT
Radiology reductionRadiology reduction
SurgerySurgery
-
8/8/2019 06 Emergency Kuliah Emergency
58/67
DIAPHRAGMATICDIAPHRAGMATIC
HERNIAHERNIA
-
8/8/2019 06 Emergency Kuliah Emergency
59/67
DEFINITIONDEFINITION
An abnormal opening in theAn abnormal opening in the
diaphragm that allow part odiaphragm that allow part of
abdominal organs to migrate into theabdominal organs to migrate
into the
chest cavit .chest cavit .
-
8/8/2019 06 Emergency Kuliah Emergency
60/67
-
8/8/2019 06 Emergency Kuliah Emergency
61/67
-
8/8/2019 06 Emergency Kuliah Emergency
62/67
-
8/8/2019 06 Emergency Kuliah Emergency
63/67
ETIOLOGYETIOLOGY Improper fusion of the canal ofImproper fusion
of the canal of
pleuroperitonealpleuroperitoneal MedicinesMedicines
Abnormal development of thoracicAbnormal development of
thoracicm sencime
CLINICALCLINICAL
-
8/8/2019 06 Emergency Kuliah Emergency
64/67
CLINICALCLINICAL
MANIFESTATIONMANIFESTATION DyspneaDyspnea
TachypneaTachypnea
CyanosisCyanosis
Asymmetry of the chest wallAsymmetry of the chest wall
TachycardiaTachycardia
Scapoid abdomenScapoid abdomen
Breath sound loosing at defectBreath sound loosing at
defectsideside
-
8/8/2019 06 Emergency Kuliah Emergency
65/67
DIAGNOSISDIAGNOSIS Clinical manifestationClinical
manifestation
Radiology examinationRadiology examination
-
8/8/2019 06 Emergency Kuliah Emergency
66/67
TREATMENTTREATMENT
Oxygen (ET), position, stop oralOxygen (ET), position, stop
oral
intakeintake SurgerySurgery
-
8/8/2019 06 Emergency Kuliah Emergency
67/67