Embed Size (px)
Citation preview
Mind the Gaps: A Framework for
Inclusive Innovation
Kate Michi EtingerMural Institute
1st Ed 2008, 2nd Ed 2016
Mind the Gaps: A Framework for Inclusive Innovation 1
In 1994, the San Francisco Public Library launched a $34M capital campaign to build a new main library in the midst of a major recession. It began as large capital campaigns often do, chaired by San Francisco philanthropist Charlotte Maillard Swig; initial contributions poured in from expected donors, but stalled, first at $9M, then at $11M, and finally at $16M. With no more foundations and wealthy people to tap, it was a moment of crisis. The library foundation and capital campaign committee regrouped. Then, they did something unthinkable- unprecedented. They went to affinity groups that represented different communities of San Francisco—the Chinese, Latino, Gay-Lesbian, Environmental communities—as they sought input from these stakeholders about what each wanted in the new main library, they also asked each community to raise money within their communities for the new main library capital campaign. The affinity groups initiated fundraising within their communities; each community approached fundraising in a way that was tailored to their community’s giving style and interests. This unprecedented grassroots capital campaign raised over $10M toward the $34M goal—as an overwhelming success, it became a model for other cities. Importantly, it demonstrates the power of inclusive action.
– read more1
I. Engaging Change
Minding the gaps in our daily life and in our society enables us to create a just and inclusive society.2 This paper introduces Mind the Gaps, a framework to promote inclusive action, and demonstrates how this framework can be applied to facilitate inclusive innovation.
1 http://www.pps.org/reference/a-librarys-appeal-affinity-groups-as-a-new-means-of-fund-raising/2 This paper was originally submitted for the 2008 UNESCO Vesak Conference: Buddhist Contribution to Building a Just, Democratic and Civil Society. Meditation and mindfulness facilitate developing the capacity to recognize gaps within our daily life, to be present with these gaps to gain clarity, and to respond to these gaps with insight and wisdom.
Mind the Gaps: A Framework for Inclusive Innovation
“ ‘Mind the Gap’, a voice overhead calls out as the doors open for the Tube in London. That is precisely the same thing we aspire to in meditation,
to mind the gap between where we are in this moment -- before we act to get where we are going. If we can recognize that space, hold it open, we
then have a chance to transform our actions from blind habit to conscious action.”
– Soto Zen Priest Ingen Breen
2Mind the Gaps: A Framework for Inclusive Innovation
II. Mind the Gaps
The “Mind the Gaps” framework is applicable to a variety of issues—whether policy interventions, health care delivery, product design or philanthropy/development work. Ideally, the framework would be introduced early in the process of understanding a problem. Considering these gaps invites participation of voices not historically engaged in the problem solving process. When impacted parties have the opportunity to contribute their diverse perspectives and to engage in shaping a solution, it strengthens the acceptability and feasibility of the proposed action.
Often experts develop interventions. In these cases, the four-part framework can serve as a checklist to evaluate a proposed action before it is implemented.
To Mind the Gaps may seem intuitive, or it may feel new and uncomfortable. It is a practice; as we become more familiar with identifying these gaps, it becomes easier to build better solutions. Let’s explore how to Mind the Gaps with the following case study:
In December 2005, the Center for Disease Control (CDC) hosted a teleconference proposing that local governments throughout the United States adopt “Community Legal Preparedness for Public Health Emergency” that expands the public health authority for a possible serious infectious disease outbreak. Public Health Authority is the discretionary power that government has over the people to protect their health. The CDC’s proposed plan sought to broaden this discretionary authority by eliminating legal restrictions that had been placed after historical episodes of misuse of authority over certain vulnerable communities.
During the Questions & Answers, a participant inquired how this proposed scheme to broaden authority would address the needs and protect the rights of people from diverse communities, such as those who didn’t speak English. After a long pause, the presenter cited work done with a Native American tribe. Given that the example was not responsive to the question and none of the materials addressed these sub-communities, it prompted the question: What would an inclusive preparedness plan look like?
This case study applies the Mind the Gaps framework to identify who could fall into gaps with the CDC’s proposed preparedness plan and to determinate how the proposed plan could be more inclusive of marginalized communities.
Gaps of Geo-Political Socio-Economics (GPSE)
Gaps of Culture
Gaps of Systems
Gaps of Power Perspective
Mind the Gaps Applied: Public Health Preparedness Case Study
Mind the Gaps: A Framework for Inclusive Innovation 3
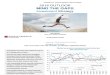
To assess Gaps of Culture asks that we cultivate the awareness that we are a fish swimming in water. We look to see the layers of assumptions that underpin the actions that we choose, the language that we use, the approach to problem solving we select, and the values that we promote. We do not need to challenge these assumptions; it is sufficient that we be aware of the assumptions. Then, we may begin to consider where and how diverging perspectives may also exist.
While this inquiry may include traditional concepts of ‘culture’ related to one’s customs, values, beliefs and identity. Gaps of Culture in this context may also prompt examining the assumptions implicit within our professional disciplines—such as, selected strategies, preferred methodologies, and presumed doctrines. To mind Gaps of Culture challenges us to look for unrecognized barriers based upon disciplinary assumptions and to invite different approaches to understand and to address a situation.
• How might the person/people I want to ‘help’ perceive my ‘help’? • What are my assumptions about providing care? • How does my health culture shape how I understand needs, service,
care and health? • Do I see the whole person beyond their health care need?
Health Care & Social Workers
• How does it feel for someone unfamiliar with this system to interact with me?
• What are my assumptions about justice, fairness, power, conflict resolution, peace?
• What do I assume about how respect is demonstrated and how reconciliation is achieved?
Legal Professionals& Mediators
• On what assumptions does the funding/program depend? • Who participates in defining focus, in designing interventions, and in
determining how our impact assessments? • What assumptions are embedded in our approach to impact? • What are our assumptions of “doing good” and how might our good
intentions yield bad outcomes?Funders, NPOs
& NGOs
Gaps of Culture
4Mind the Gaps: A Framework for Inclusive Innovation
The first step is to identify the different cultures operating as the CDC developed its community preparedness plan for dissemination to state departments of health. Cultures involved in the plan’s development: the federal government, the CDC, infectious disease, public health. Cultures involved in the plan’s adoption/execution: state government, health departments, city government, public health authority/law, public health interventions, medicine/infectious disease. Cultures involved in the implementation: health care, law enforcement, urban people, suburban people, rural communities, the sick, the well, fear, the media, people with access to care, people without access to care.
Questions that surface when looking at the situation from outside the culture of public health and outside the culture of government may include:
• What if, during an emergency, the public health authority’s good intentions to protect the public gets overrun by the politics of fear and discrimination?
• How does the public health authority intend to use their discretionary power?• Is there guidance on how to use discretionary power in difficult situations?• What if the public health authority is not as good as it presumes to be? • What protections exist for the public if the government fails to use its power well?• What if the public does not trust the public health authority and fails to respond to its
directives? • What accountability and/or incentives ensure that the public health authority’s good
intentions are realized?
An inclusive perspective might prompt considerations, such as:
• Given the history of public health’s treatment of vulnerable populations3 during infectious disease outbreaks, it is imperative to question whether the public health authority would be able to fulfill its intention to protect vulnerable populations amidst the heavy political and social pressures that often arise in the initial stages of a public health crisis--- when fear looms and science lags.
• How might those who do not trust the public health authority, or government in general, be affected during a public health emergency?
• What would be the implications for the public’s overall health if some sub-groups did not follow public health directives? What would be the burden on those communities for not adhering to the public health authority?
• Due to limited funding to support preventative or ongoing care for marginalized communities, these communities are often hard to reach, because they are conditioned not to have access to care. Who are these communities without access to care? How can they be reached effectively?
• Given the collective interest in having everyone engage with the system during an infectious disease outbreak, it should be a priority to fund inclusive policies that specifically outreach to and support the needs and interests of marginalized communities.
3 Ettinger, K. A Critical Legal History of Public Health’s Treatment of Vulnerable Populations during a Public Health Emergency. (Available from the author).
aav
Gaps of Culture Applied: Public Health Preparedness
Mind the Gaps: A Framework for Inclusive Innovation 5
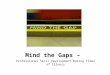
To assess the Gaps of GPSE, we consider how contextual factors -- geography, political context, and socio-economics -- impact communities differently, and as a result, how these factors might pose barriers to inclusiveness of a proposed action.
Gaps of GPSE are already well recognized as critical factors in ongoing disparities. For example, the public health term ‘social determinants of health’ recognizes how these factors strongly influence a person’s health, well being and access to care. In the legal system, Gaps of GPSE represent known barriers to accessing legal services and to receiving equitable remedies. Environmental justice addresses how these GPSE factors are associated with exposure to environmental hazards.
In philanthropy and non profit work, recent promising trends reflect greater inclusion arising from attention to Gaps of GPSE. Geographic: the focus and support for locally owned social businesses that solve challenges within their own community. Political: the inclusion of impacted communities in the problem definition and solution design process by methods such as human-centered design. Socio-economic: the shift away from development as solely charitable with a concurrent focus on solutions that enable financial empowerment and individual’s economic growth.
To take conscious, inclusive action, we reflect critically upon these GPSE factors and question who is not in this conversation due to GPSE factors. Then, we assess whether our proposed action may unintentionally exclude groups based on GPSE attributes.
• How might a patient’s socio-economic situation impact his/her ability to manage a diagnosis or to access recommended treatment?
• How might a patient’s distance from the clinic affect her care?• How might a patient’s political situation, e.g. documentation status,
impact his/her ability to access care?Health Care &
Social Workers
• How might geography or socio-economic status constrain a person’s ability to access and receive equitable justice?
• How might a person’s prior experience of justice influence whether s/he accesses the justice system?Legal Professionals
& Mediators
• How does our GPSE influence how we view whom to aid, how we understand the problem, and what kind of programs/solutions we choose to support?
• Does our understanding of a desirable solution match the view of the people we seek to help?
• Does our approach cultivate more equity between us and those we serve or does it maintain the GPSE difference between us?
Funders, NPOs& NGOs
Gaps of Geo-Political Socio-Economics (GPSE)
6Mind the Gaps: A Framework for Inclusive Innovation
To identify Gaps of GPSE for the CDC’s proposed plan begins with geography. In times of crisis, the personnel of transportation systems, e.g. bus drivers, flight crews or train conductors, become key players often overlooked. As well, considering the geographic needs to transport people (and supplies) to and away from a crisis zone, it is also important to consider who might go toward an outbreak. In addition to health professionals, the media and journalists represent a group of people who need to be included in Preparedness Plans.
The political context may surface different concerns. In the US, one needs to consider that a person’s legal residency and documentation status may adversely impact their willingness to seek needed care or to respond to directives to report for vaccinations or treatment. As well, a person’s experience historically with law enforcement and government authority may influence his/her willingness to comply with government regulations. Communities more conditioned to aggressive policing and brutality may react with mistrust to public health interventions, particularly if law enforcement participate alongside public health officials.
A historical review of marginalized communities and analysis of scenarios from past outbreaks yields identification of several groups at high risk of being overlooked in preparedness strategies: homeless, poor, persons with disabilities, persons who are institutionalized (prisons, nursing homes), children, elderly, undocumented people, recent immigrants (incl. people with limited English proficiency). These groups often have lower socio-economic status and thus, lack political power to advocate for their interests to be included in emergency preparedness plans or to protect themselves from overreaching government authority in times of crisis.4
An inclusive plan might address considerations, such as:
• How might people from different GPSE be affected during each critical stage? (awareness, prevention, screening, treatment, vaccination, quarantine)
• How will geography play a part in an epidemic – with regard to access to care, access to treatment and the spread of disease?
• How will political status influence public health efforts? What happens to non-English speakers or recent legal immigrants who are often scared to access public services in the US? What happens to people who are not legal residents? What happens to prisoners?
• What social factors will influence the epidemic? What happens to the elderly? What about the institutionalized elderly in nursing homes? What happens to a dependent child whose single parent requires quarantine?
• How might economic status impact the public health plans? How will the homeless be contacted? Will the narrow margins for the working poor (fear of job loss, need for money) impact those who need to work rather than stay home under quarantine?
4 This does not indicate the state of affairs at present. The purpose of this project in June 2005 was to raise awareness of the interests of marginalized communities in a time of a crisis and to promote inclusion of their interests in preparedness planning. Hurricane Katrina in Sept 2005 underscored the need to develop inclusive preparedness planning. The current situation varies by county and state.
aav
Gaps of GPSE Applied: Public Health Preparedness
Mind the Gaps: A Framework for Inclusive Innovation 7
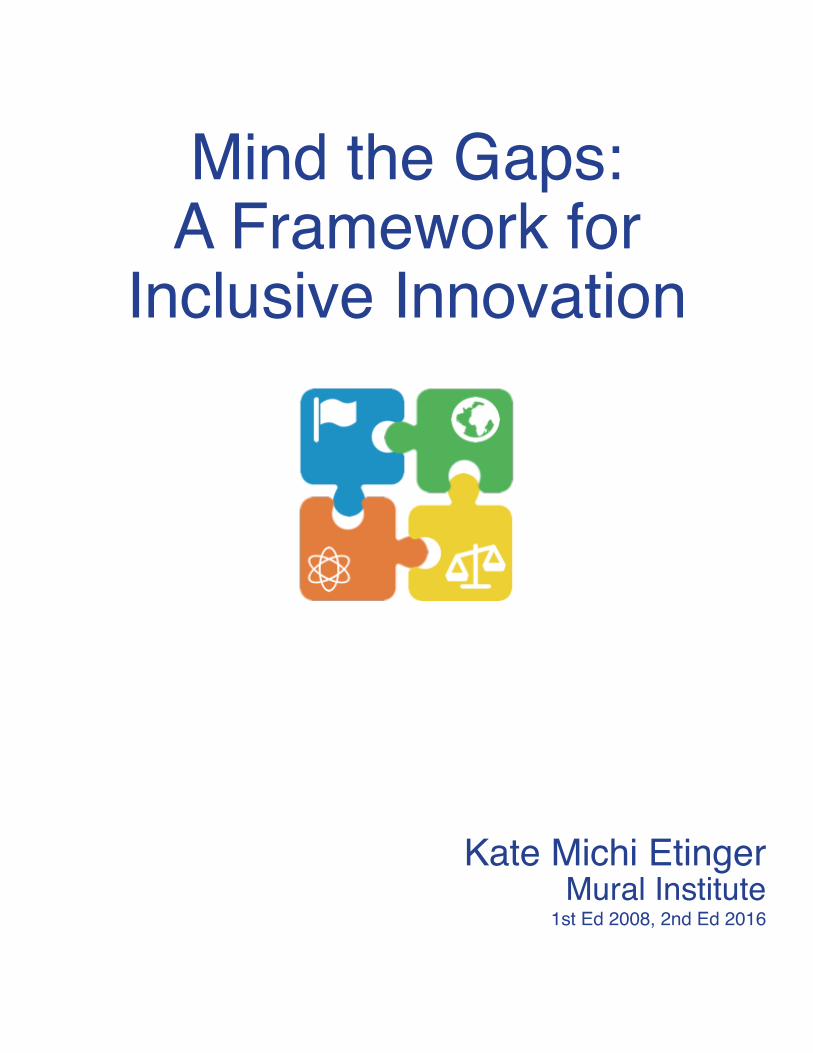
Assessing Gaps of Systems asks that we consider the inclusiveness of the systems upon which our proposed action depends and that we reflect critically upon the limitations of those systems. For example, if we propose to communicate a message – upon what systems does our message adepend? We must consider how we will reach people who do not speak our native language, who cannot hear/read, and to what extent there may be communities who lack access to this chosen media channel. Many young people no longer watch TV, etc.
Or, if we decide to locate a free mediation service at the court-house, we must consider whom our legal system serves and whom it fails to serve and determine whether our efforts to provide alternative methods for conflict resolution might be limited due to the legal system’s limitations in providing access to justice. Given the institutionalized racism in some urban police departments highlighted by the Black Lives Matter movement, it may be relevant to consider the implications for including a police presence in certain situations and to understand how to invite that presence in a way that does not alienate some communities.
Ultimately, Gaps of Systems challenge us to consider the systems that we rely on to implement our solution and to evaluate whether those systems work equally for all people. Gaps of Systems necessitate that we pay attention to the limitations of our existing systems, acknowledge where institutionalize injustices exist, and imagine how we can create more inclusive systems to accomplish our goals.
• If we rely on the existing system that delivers care to people, whom might we miss in our outreach?
• How does the system differ for someone with employer-based insurance differ from someone with individual payer insurance?
• How does systemic isolation impact the ability to have a voice in public policy that affects health and health care delivery?
Health Care Systems
• How do limitations of the justice systems impact our efforts to provide access to justice?
• How might systemic issues limit a person’s ability to access and to receive equitable justice?
• How does extensive legalese or lengthy arcane documents be a barrier for people who have only high school education?
• How does the documentation we require encumber rather than serve people who seek our services?
Justice Systems
• What systems do our funding/program strategies rely upon? • If we seek to provide alternative educational programming and offer it at
the local college, whom do we exclude as a result? • How do the people we aim to serve interact with system we want to
use?Funders, NPOs
& NGOs
Gaps of Systems

8Mind the Gaps: A Framework for Inclusive Innovation
Public health preparedness plans rely on three primary systems – public health authority/government, the health care system, and the media.
For people who have historically poor relationships with government, it is important to consider that they might ignore or be suspicious of government advisories. The government and health care system systemically alienate certain communities, particularly the poor and undocumented residents. Conditioned to fear that any contact with government will result in deportation, undocumented people fear government in a way that may cause them to ignore public health advisories to seek medical attention for surveillance at the first sign of symptoms. In public health emergencies, people who remain in the community until symptoms are definite may significantly increase the spread of the virus; thus, this historically adversarial relationship may have significant implications to the overall health of the public if not handled well. Thus, it is important to consider the manner and degree to which a community is alienated from the health care system and society and what may be necessary to promote trust in and compliance with public health directives. Other communities historically marginalized may react similarly—from homeless, those who have suffered from or fear religious persecution for health beliefs, communities unequally served by health/justice systems may be skeptical of interactions with government.
Most public health announcements are made through media channels. Traditionally radio and news, with the advent of the internet and other channels for rapid information dissemination, this changes how outreach strategies can be most effective. It remains important to continue to use traditional TV/radio outreach, especially to reach homebound older adults who may be isolated and who may not use new technology. As well, to consider what would happen to people who do not have media access. Homeless people who don’t have a radio/TV, deaf people who don’t listen to the radio, illiterate people who can’t read a flyer, and/or announcements made only in English would miss non-English speaking residents.
An inclusive plan might address considerations, such as:
• Who is not adequately or disparately served by the current health care system? [Includes homeless, poor, some religious communities with specific health beliefs (e.g. Jehovah Witness, Christian Scientists, etc), undocumented residents, people with limited English proficiency (LEP)] How might we reach these communities?
• Will undocumented residents fear deportation and other marginalized communities fear participation of law enforcement alongside public health authorities, and thus be afraid to come to the hospital when they have symptoms during a pandemic?
• Who will be overlooked if the strategy to promote awareness and prevention is through traditional media? How will people who don’t speak English learn of this? people who cannot read? people who are homeless? People without TV/Radio?
• Who will be overlooked if the strategy to promote awareness and prevention is through new media channels?
• How do public systems, such as public transit, affect who may come into contact with an infectious disease and how does it inform the way that disease may spread and how we may need to approach containment strategies?
aav
Gaps of Systems Applied: Public Health Preparedness
Mind the Gaps: A Framework for Inclusive Innovation 9
By assessing Gaps of Perspective, we consider how our power, privilege, and position shape our perspective on the proposed action. A power perspective unconsciously informs the strategies that we employ and it takes deliberate effort to understand that others do not enjoy the same power, privilege, and position. For example, some people may believe that exercising the right to peaceful protest is the most effective way to show their perspective publicly. Yet for others whose personal or community experience includes unequal justice, there may be hesitation to participate. These people may feel less security in exercising their civil rights and less confidence in the justice system to render a fair outcome if police get involved.
Many efforts to provide international aid failed due to a Gap of Perspective; the people who crafted the solutions—to build playpumps, to provide more bednets or to have one laptop per child—did not understand how their power, privilege and position shaped their view of the situation and acceptability of the solution.
We must learn how our power, privilege, and position shape our perspective in order to use our power perspective effectively. Cognitive dissonance and reactive devaluation impede people’s ability to hear and act upon the words from people perceived as “other”; thus, one effective way to use one’s power effectively is to address opportunities for inclusion with one’s peer group. If a peer says, let’s pay attention to this issue, then others are more likely to get involved. Ultimately, inclusive action is sharing our power and using our privilege and position well. Gaining a keen understanding of all three is critical to promoting inclusive action.
• How does the imbalance in power in this provider-patient relationship influence the interaction?
• What does my privileged position as a care provider afford in my relationship with the patient and the system?
• How can I, as a care provider, use my power, privilege, and position to benefit my patients and society?
Health Care Providers
• How does my position as someone familiar with navigating the legal system influence my view of the acceptability of this proposed program?
• How could this proposed program be more accessible to someone who is unfamiliar with, fearful of and/or intimidated by the law? Legal Professionals
& Mediators
• How does my power and privilege as the funder/aid worker inform this intervention?
• Would someone receiving this intervention find it appropriate and desirable?
• How can I use my power perspective most effectively - in this situation, is it optimal to ‘help’ others by intervening on their behalf or to invite them to have a seat at the table as problem solvers and co-creators of the solution?
Funders, NPOS& NGOs
Gaps of Power Perspective

10Mind the Gaps: A Framework for Inclusive Innovation
Gaps of Perspective in the preparedness plan arose from the power differential between the people who drafted it and the people who will be impacted by it. The plan was drafted by people who believe in the medical model, who trust in the government to “do the right thing” when given broad authority, and who are confident in the ability to handle a crisis with a public health approach. This view is the privilege of a particular kind of education, the privilege of understanding how public health interventions work, and the privilege of position to trust in broad government power. These privileges of perspective are to be expected— smart people who are highly educated in medicine and public health, who hold positions of power in our social hierarchy and who have good intentions to help people work at the CDC.
As the preparedness plan gets implemented, the broadened authority is exercised at a different level—state or city—by a different set of people who have a different power perspective. At this level, public health and government officials might be more sensitive to the marginalized communities within their constituencies. Since the CDC’s plan did not address these issues of inclusion, it was incumbent upon the local authorities to develop their own strategies. However, in a crisis, there is little time to go through the process of developing new oversight mechanisms or inclusion strategies because the focus is on the disease—treatment, prevention and education. Thus, the opportunity for inclusion would be to invite the identified groups into the problem solving process as the state department of health adopts the CDC’s recommended plan and to develop preventative policies with the power perspective of the impacted communities.
An effective way for the CDC to use its power would have been to include a directive for local governments to designed inclusion policies to supplement their preparedness plan.
An inclusive plan might address considerations, such as:
• How might this proposed action reflect assumptions of power?• What privileges informed the feasibility of the proposed action?• What power perspective influences the acceptability of the proposed action?• Where are there opportunities to share power in developing or implementing this
proposed action?• How will the impacted communities experience this proposed action- their autonomy,
their sense of power, their position? • Will everyone be impacted equally by this proposed action or will some communities
suffer greater burdens? If so, why and how can that be mitigated?• Does the proposed action empower the impacted communities? If not, how can it be
altered or implemented in a way that maximizes empowerment?• Where do I have power, privilege, and position in this situation and how can I use it most
effectively for inclusion?
aav
Gaps of Power Perspective Applied: Public Health Preparedness

Mind the Gaps: A Framework for Inclusive Innovation 11
III. Inclusive Action
To Mind the Gaps results in inclusive action. Inclusion changes the status quo. It disrupts current imbalances of power, and it introduces new methods for doing things—an innovation.
The Emergency Preparedness case study illustrates how applying Mind the Gaps to evaluate a proposed policy intervention identified opportunities for additional policies of inclusion. These opportunities for inclusive policies were presented in a poster5 at the CDC’s Public Health Law Conference in June 2005. Just three months later, Hurricane Katrina hit three months later, the groups identified and the issues anticipated in the poster became a part of tragic history. Hurricane Katrina underscored the devastating effects of neglecting marginalized communities by any level or department of government. While that tragedy resulted in increased attention to improve inclusion of diverse communities in policy development, there remains significant room for inclusive innovation.
This revision follows the recent Ebola crisis in West Africa. There disease spread due to many of these gaps—gaps of privilege due to authorities belief in the medical model and the public’s differing view about the illness, gaps of power arising from mistrust of the government, gaps of culture around health/sickness and death/burial, gaps of GPSE related to the socio-economics of livelihood and geographic distance to treatment centers. Many difficulties arose from the public’s response to public health advisories, which underscores that inclusive frameworks, such as Mind the Gaps, are applicable everywhere and remain important from global health to local public health initiatives.
Mind the Gaps Applied: Public Health Preparedness Case StudyProposed Inclusive Policies for Public Health Emergencies
5 Ettinger, KM. Vulnerable Populations During a Public Health Emergency, available at: www2a.cdc.gov/phlp/conferencecd2005/docs/kettinger.pdf
Immigrants• No request for immigration status during an intervention• No reporting of immigration status will be made for anyone contacted by the• public health service• Community programs to educate immigrant communities about confidentiality during
public health interventions and about public health, its role, and its services during a crisis:• Co-develop programs with community leaders• Establish culturally appropriate & language accessible manner
• Develop communication strategies to reach immigrant communities in the event of crisis:• Identify best possible means to disseminate information• Establish strategy to promote participation in vaccination/ detection/ treatment
measures
Poor & Homeless• Educate the public that no health insurance is necessary to receive screening and
treatment during intervention
aav

12Mind the Gaps: A Framework for Inclusive Innovation
Poor & Homeless• Develop appropriate communication strategies for:
• Homeless through helters• Substance users through street networks• People without access to traditional media (TV, radio, internet)• Illiterate
• For working poor, policies that provide assurances that measures will not have adverse economic consequences:
• No costs for screening and treatment• During Quarantine:
• Minimum wage and/or deferral of bill payments• Policy barring termination from employment/eviction• Programs to support child care
Institutionalized• Communication strategies to reach these isolated communities that depend on others for
their information:• Information needs to be provided in an understandable manner:• Acceptable and non threatening, if not understandable
• Develop advance policies for managing an outbreak within the institution• Institutions need to proactively develop infection control and screening protocols to be
used during an emergency for:• Staff• Visitors• People within the facilities
Persons with Disabilities• Develop appropriate communication strategies for disabled communities:
• Sensory impaired• Cognitively impaired• Psychiatric disabilities
• Establish policies that ensure emergency measures are accessible to and practicable for these communities:
• Physically accessible locations for the physically disabled• Home-based/separate area screening for immune-compromised• Procedures for surveillance and home management of disabled• Considerations regarding additional needs of immune compromised and of
chronically ill during quarantine• Layered confidentiality/privacy concerns for contact tracing• Complications and side effects of treatment or vaccination programs with immune
compromised population• Prevention of infection training for 1:1 caregivers
aav
Mind the Gaps Applied: Public Health Preparedness Case StudyProposed Inclusive Policies for Public Health Emergencies
Mind the Gaps: A Framework for Inclusive Innovation 13
IV. Inclusive Innovation
Bringing consideration of these gaps into the process of designing a new product or developing a new program will result inclusive innovation.
The appendix includes an example for how one might apply the Mind the Gaps framework for inclusive innovation in leadership.
After reviewing a proposed action, it may be determined that the initial approach is preferable even if it may not be fully inclusive. The process remains valuable because it facilitates deeper understanding of potential barriers, which enables identifying smart strategies to mitigate the barriers if/when they arise.
Applying the four-part framework diligently and consistently in personal and professional activities raises awareness of gaps in daily life and promotes more inclusive action.
AcknowledgementsVisual design by Rosamond Dunn. Icons licensed under creative commons from the Noun Project. ‘Culture’ by Adam Heller, GPSE by James Zamyslianskyj, ‘systems’ by Creative Stall, ‘power’ by Kristen Gee, ‘healthcare’ by To Uyen, ‘legal’ by Fraser Ferguson, ‘funders/NGOs’ by Thierry van Brenten.
14Mind the Gaps: A Framework for Inclusive Innovation
Apendix
Mind the Gaps Applied: Inclusive Leadership for School Administration
At a private elementary school in New York City6, an 8th grade student and her best friend gang up on a 5th grade student. They bind her hands with tape and plan to leave her in an area where students are not supposed to go without supervision. The terrified younger student complies with everything they say. Their plan is foiled when another 5th grade student discovers them; the 5th grade students tell their teacher. The school administrators hear from the two sets of girls and suspend the older students for two days and require them to write an essay reflecting on their actions. A week later, the school sends a letter to the parents indicating that two older girls had tied the hands of a younger student and then untied them and that the school had managed the situation. The victim’s parents are extremely distressed after hearing about this event from their daughter. As the principal of the private school where a bullying incident occurred, Mr. M considers how a response to the situation might be most inclusive.
Gaps of Culture: School LeadershipMr. M questions how he might approach a parent meeting to discuss the bullying situation. He considers how the discipline may appear to each set of parents. He decides to invite the parents of the children directly involved in the incident to meet with him. He deems that this approach fosters the kind of open dialogue that the school advocates and feels that he can manage these parents without difficulty.
Mr. M is bounded by the culture of “administrators” and approaches handling this situation in the delicate, political nature expected of someone in his position. However, to look beyond one’s “culture” of handling difficulty in a top down way, here are three approaches to support inclusive action in this conflict.
1. What is my disciplinary bias in how to approach conflict? Mr. M. does not consider whether the parents may think that he has a conflict of interest for economic reasons (e.g. his job may depend on parental donations to the school). If he considered these concerns, he might hire a mediator to have a neutral facilitator of dialogue, to level the playing field and to facilitate understanding. To be certain this strategy is acceptable, he would ask all sets of parents whether they are comfortable with having a mediator present to facilitate the dialogue.
2. What are my assumptions about who is impacted? Mr. M has not considered that other parents may have concerns about the situation, nor does he consider that other students not directly affected may have residual concerns from this event. Rather than narrowing the focus to whom he believes to be the impacted, Mr. M asks the community whether there are people who have unaddressed concerns.
3. Who solves the problem? Rather than a top down approach, an inclusive strategy for healing the community might be for Mr. M to invite the grades impacted 5th – 8th students and their teachers to an assembly to address healing this incident. This approach would enable students not directly involved but impacted an opportunity to express their concerns and needs for safety, and it would allow the entire community an opportunity to participate in the solution.
6 This is a fictional narrative for teaching any resemblance to a true story is purely coincidental.
v
Mind the Gaps: A Framework for Inclusive Innovation 15
Gaps of GPSE: School Leadership Mr. M does not see any geographic considerations in this case, but he recognizes political and socio-economic concerns. Mr. M is aware that the parents of the instigator and the victim have vastly different political outlooks, social status, and wealth. The instigator’s parents are wealthy, prominent business people with a lengthy lineage of family who have graduated from the school; the victim’s parents work in public health and government, and both are second generation immigrants of comfortable means but limited wealth.
To level the playing field in a situation of imbalance, having a neutral 3rd party facilitator may promote greater understanding of the differences and surface (mis)perceptions. For example, these parents may have different experiences of justice based on their personal GPSE histories, they may have different understandings of the event, and they may have different perspectives on what constitutes a just remedy of the situation.
Gaps of Systems: School LeadershipMr. M chose to use the school’s usual approach to handle this situation; critically considering this strategy, he might recognize that some might mistrust the school’s commitment to discipline justly arising from its dependence on parent financial contributions. To promote a sense of confidence in the school’s commitment to neutrality and justice, Mr. M might chose to use a mediator. If selecting a mediator, he would check with both parents to ensure they agreed to this process, as well he might consider whether the mediator has experience with multi-cultural conflicts and what qualifications the mediator might need to have to establish legitimacy with the parents in this conflict.
To inspire confidence in the fairness of handling this type of situation should it arise in the future, Mr. M might work with a coalition of teachers, parents, and students to identify and develop a way to handle any future similar incidents. This would provide consistency and transparency, while retaining flexibility and result from an inclusive problem solving team.
Gaps of Power Perspective: School Leadership Mr. M reflects on his power in this situation and feels confident that he can manage these parents based upon his authority at school. Yet, he does not have authority over the parents and in many ways, he is accountable to them.
Mr. M did not consider that his position could be perceived differently between the two families. While the instigator’s parents, wealthy patrons of the school, feel comfortable expressing their perspective and needs, the victim’s parents who do not have a strong economic relationship with the school do not feel equally entitled. He also did not consider that the victim’s parents might be concerned that pursuing a just outcome for their daughter could harm their relationship with the school. In contrast, the instigator’s parents are secure in their relationship with the school and do not even consider that stating their thoughts would have any implications for their daughter’s educational experience. These are differences arising out of the parents’ different power positions and the perspective of their privileges. Mr. M,who is not aware of his own privileged perspective, is insensitive to the ways that privilege shapes actions.
Mind the Gaps Applied: Inclusive Leadership for School Administration