Embed Size (px)
Citation preview
AN ANALYSIS OF THE BURDEN OF SCHIZOPHRENIA AND RELATED
SUICIDE IN AUSTRALIA
Access Economics Report for Sane Australia 2002 An Analysis for Cost Benefit Literature Review with
some Updated Information
PURPOSE OF REVIEW
• Summarise and comment on content and methodology of 2001 Access Economics report into schizophrenia and suicide
• Update some of the information in the report to as recent as possible, such as graphs and tables
2
WHAT IS THIS REPORT ABOUT?
• 2001 report written for SANE• Specifically about schizophrenia and suicide• Costs is the focus of the report• Financial costs and effects for individuals• Health costs in particular
3
Location On Web
Sane Australia. (2002). Schizophrenia: costs: an analysis of the burden of schizophrenia and related suicide in Australia. An Access Economics report.
http://www.aftercare.com.au/wp-content/uploads/2012/11/Schizophrenia-Costs.pdf
4
TOPICS
• Overview of report (executive summary)• Schizophrenia and Suicide Issues• Prevalence and Direct Health Costs• Indirect Costs and Burdens• Conclusions• Methodology
5
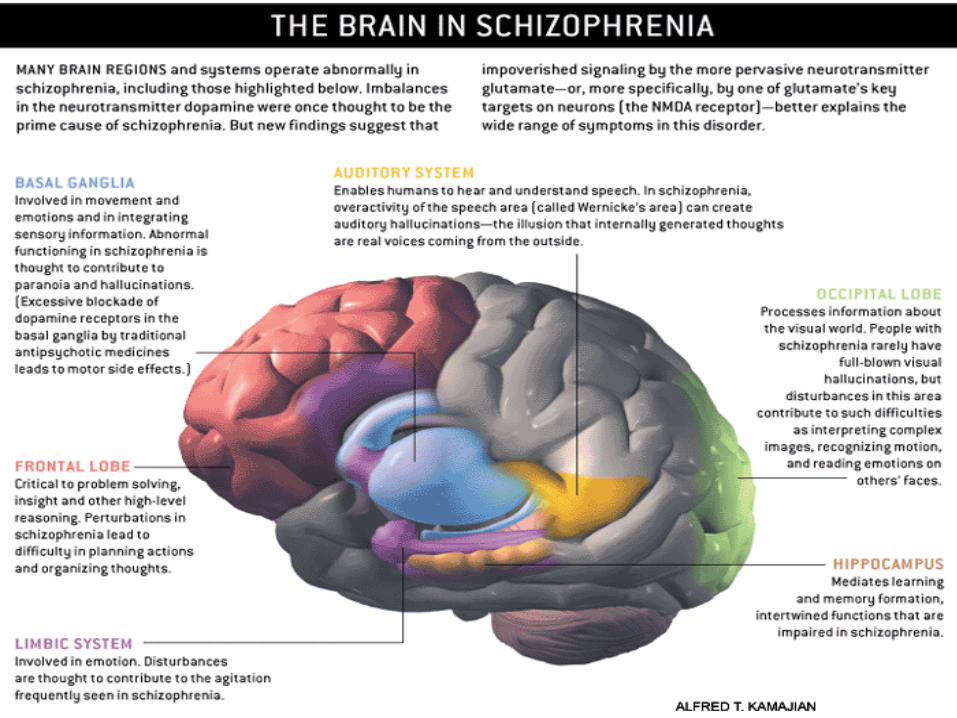
BRIEFLY ABOUT SCHIZOPHRENIA
6
WHAT IS SCHIZOPHRENIA?
A long-term mental disorder of a type involving a breakdown in the relation between thought, emotion, and
behaviour, leading to faulty perception, inappropriate actions and feelings, withdrawal from reality and personal
relationships into fantasy and delusion, and a sense of mental fragmentation. 7
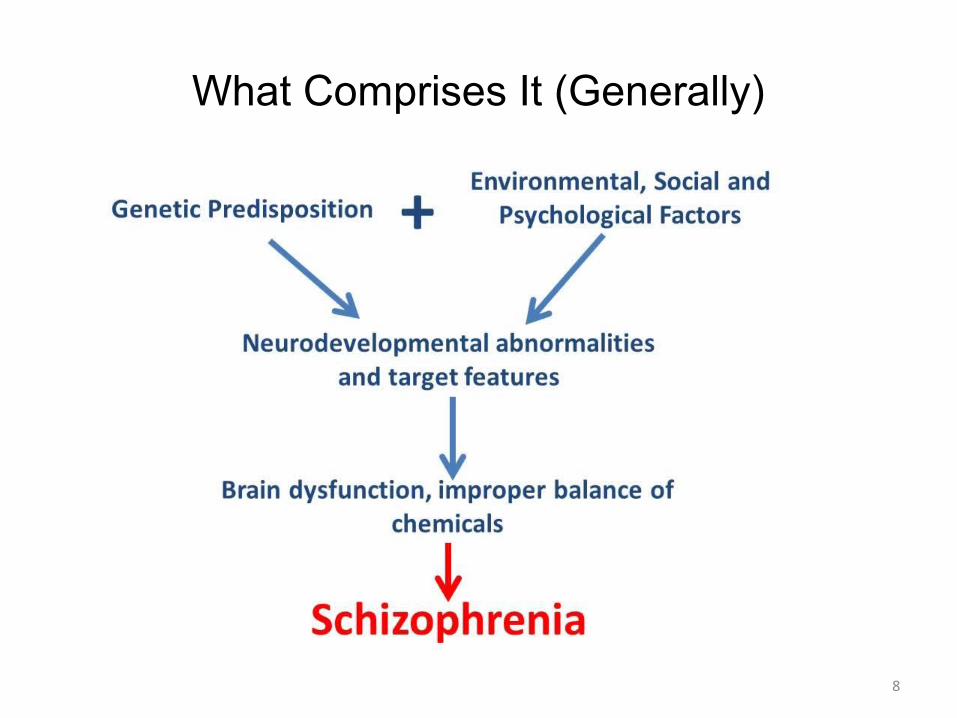
What Comprises It (Generally)
8
9
TOPIC 1
OVERVIEW
(EXECUTIVE SUMMARY)
10
EXECUTIVE SUMMARY
• Schizophrenia is cost
• Direct and indirect costs are enormous
• Real financial costs of illness - $1.85 Billion, 0.3% of GDP
• $50,000 on average for each of more 37,000 Australians with schizophrenia
11*2001 figures
EXECUTIVE SUMMARYDIRECT COSTS
• Direct health system costs 2001 - $661 million
• 60% Hospital Costs
• 22% Community Mental Health Services
• 6% Medical Costs (GP’s and Specialists)
• 4% Nursing Homes
• 2% Pharmaceuticals12
$18,000 per person with schizophrenia
1.2% of national health spending
6 times spending on average Australian’s health care
13
EXECUTIVE SUMMARY INDIRECT COSTS
• Total $722 million
• $488 million lost earnings from not being able to work
• $94 million premature deaths
• $88 million carer costs
• $52 million prison, police legal costs
14
EXECUTIVE SUMMARY TRANSFER COSTS
• $190 million of lost tax revenue (patients and carers)
• $274 million in welfare payments – mostly disability support pensions
15
EXECUTIVE SUMMARY THE BURDEN OF DISEASE
• 22,616 years of healthy life lost to do schizophrenia in 2001
• 3.323 years lost due to suicide and self-inflicted injury
• 55% mostly males
• 74% young people 15-34
• 129 Australians in 2001 suicided because of it
• 2.5 times risk of death than the average Australian 16
One-year prevalence is low (1.92 per 1000 globally in range of 1 to 7.5), lifetime prevalence is around 10 per 1000
Direct costs are likely to be underestimated for pharmaceuticals
Burden of disease does not estimate suffering of families as they care for those with it
Public health spending in Australia is low as Australians with schizophrenia are missing out on effective treatments
17
EXECUTIVE SUMMARYCOST-EFFECTIVE INTERVENTIONS THAT NEED
INVESTMENT
• Prevention and early intervention programs
• Newer improved medications
• Career education and training• Psychosocial rehabilitation strategies• Treatment of co-existing substance abuse
• Research into causes and more effective treatments
18
TOPIC 2
Schizophrenia and Suicide
19
SCHIZOPHRENIA – CLINICAL PICTURE
• Diagnosis is complex based on observations of behaviours and one’s thinking process (DSM-IV OR ICD-10 classification)
• Symptoms vary for every person but may be:
Hallucinations – Especially voices, tactile and visual Delusions – False beliefs, ideas of grandiosity or persecution Disordered Thinking – Abnormalities in language Abnormal Affect – Depressed mood, low motivation, withdrawal
• Onset of it is either acute (days or weeks) or insidious (gradual transition)
• Onset is earlier in males especially in 20’s, females early 30’s20
SCHIZOPHRENIA IS THE MOST COMMON TYPE OF PSYCHOSIS, REPRESENTING OVER HALF OF ALL
PSYCHOTIC PATIENTS.
According to ICD-10 criteria*:
1.53.8% of people with psychoses had schizophrenia
2.10.8% Schizoaffective Disorder
3.11.8% Bi Polar and/or mania
4.8.4% depressive psychosis
5.15.3% other psychosis
21* International Statistical Classification of Diseases and Related Health Problems (ICD)
SCHIZOPHRENIA – CLINICAL PICTUREAetiology (Cause/s of Disease)
• It is a group of brain disorders
• Strong evidence that genetic and environmental factors impact on early brain development leading to an increased risk of development of it
22
SCHIZOPHRENIA – CLINICAL PICTURE - FACTORS
• Heredity/Genetics
• Physical Abnormality of the Brain
• Chemical Imbalance
• Environment
• Note: it is not considered a stress-related illness but stressful life events and use of drugs can precipitate a psychotic episode or first onset of it
23
SCHIZOPHRENIA – CLINICAL PICTURE – ILLNESS PROGRESSION
• 45% of patients have complete or partial recovery after one or more episodes
• 20% poor outcomes and 35% varying degrees of remission and exacerbation
• World Health Organisation based categories
24
SCHIZOPHRENIA – MORBIDITY
• Disability is experienced by those with it
• Self-care is particularly of concern especially hygiene
• 30% in Low Prevalence Disorders Study (LPDS) suffered impairment with 3.6% self-neglect
• Occupational performance – study, housework, employment) is largely affected
25
Morbidity - refers to the state of being diseased or unhealthy within a population.
SCHIZOPHRENIA – MORBIDITY – WORK AND EDUCATIONAL LIMITATIONS, SOCIAL-ECONOMIC
DISADVANTAGE• People with schizophrenia are socio-economically
disadvantaged with over 70% of people with psychosis in Australia not working at all
• Nearly half have no school or tertiary education
• People with schizophrenia who had employment experience high rates of losing it with 53% had lost nearly 15% of their work-weeks during the due due to illness-related absence
26
SCHIZOPHRENIA – MORBIDITY – SOCIAL STIGMA
• This is referred to as social mistreatment
• Many forms with de-stigmatizing psychotic illness as a challenge
• Includes negative labelling, pejorative language
• Barriers to housing, employment, social services, social interactions, friendships with lower self-esteem and reluctance to obtain treatment
27
SCHIZOPHRENIA – MORBIDITY – SOCIAL ISOLATION
• Tend to want to be isolated
• 31% live alone
• 59% have an impaired ability to socialise
• 35% have no face-to-face contact with close relative
• 39% have no ‘best’ friend, 12% no friends at all, 64% single
28
SCHIZOPHRENIA – VIOLENCE AND CRIMINALITY
• Rate of violence can be more if substance abuse or previous criminal activity are present
• Medications being discontinued is also a risk
• More people in the prison system worldwide of those with psychotic illness – 3.7% males, 4.0% females
• Also those with schizophrenia more likely to be victims of crime
29
SCHIZOPHRENIA – CO-MORBIDITIES
• Higher risk of other mental illnesses – 25%-30% chance of clinical depression
• More anxiety, paranoia of being attacked due to persecutory delusions or worry about having an episode
• Can also be prone to physical disorders due to unhealthier lifestyles and effects of anti-psychotic drugs
30
SCHIZOPHRENIA – OTHER ISSUES AND HIGH RISK OF MORTALITY
• Substance abuse – Alcohol (30%), and/or Drugs (25%)
• Makes symptoms worse and treatment plans become ineffective
• Lifetime diagnosis of alcohol and drug abuse is higher than the general population
• Smoking is a common form of substance abuse with a risk of associated health issues, one study suggests 80% of people with schizophrenia smoke
31
SUICIDE ISSUES
• The World Health Organisation (WHO) calculates lifetime risk of suicide for people with schizophrenia as 10-13%, 12 times population risk
• Higher in men 20%, women 17%
32
SCHIZOPHRENIA – MORBIDITY
33
SCHIZOPHRENIA – MORBIDITY
34
SCHIZOPHRENIA – MORBIDITY
35
SCHIZOPHRENIA – MORBIDITY
36
SCHIZOPHRENIA – MORBIDITY
37
SCHIZOPHRENIA – MORBIDITY
38
SCHIZOPHRENIA – MORBIDITY
39
SCHIZOPHRENIA – MORBIDITY
40





























