Embed Size (px)
DESCRIPTION
Repaso enarm reumatologia, les deseo exito
Citation preview

REUMATOLOGIA
ENARM



CASO CLINICO• A 57-year-old man presents with a swollen, painful left knee. He fell on the
knee 3 days ago while hurrying up the stairs. On examination, there is a swollen knee with palpable effusion and decreased range of motion. Adiagnostic tap is preformed and 5 cc of transparent fluid is removed. The WBC count is 1000/mL (20% polymorphonuclear neutrophils [PMNs]), glucose is equal to plasma, viscosity is high, and lactate dehydrogenase (LDH) is low.
(A) normal synovial fluid(B) noninflammatory effusion(C) inflammatory effusion(D) septic arthritis(E) hemorrhagic effusion

(B) This man has a noninflammatory effusion likely from the trauma caused by the fall. In the
noninflammatory category, the fluid is transparent,
WBC 200–2000/mL (<25% PMNs), glucoseis normal, and LDH is low. Another causefor a noninflammatory effusion is osteoarthritis.(Kasper, p. 2032)

CASO CLINICO• A77-year-old woman presents with a swollen, painful right knee. She
fell on the knee 3 days ago while hurrying up the stairs. On examination, there is a swollen knee with palpable effusion and decreased range of motion. A diagnostic tap is preformed and 5 cc of opaque fluid is removed. The WBC count is 20,000/Ml (50% PMNs), glucose is lower than plasma, viscosity is low, and the LDH is high.
(A) normal synovial fluid(B) noninflammatory effusion(C) inflammatory effusion(D) septic arthritis(E) hemorrhagic effusion
(C) This woman has an inflammatory categoryof effusion in view of the opaque color, highWBC 2000–10,000 (>50% PMNs), low glucose,and high LDH. Common causes for this includecrystal induced arthritis, SLE, and RA. In septicarthritis, WBC is usually 50,000/mL or moreand often >100,000/mL with >75% PMNs.Other important tests on synovial fluid includeGram stain and culture when an inflammatoryeffusion is suspected clinically.

ARTRITIS REUMATOIDE• 1.- En que enfermedades suelen ser positivos los ANA +? R = LES, esclerodermia, Sjogren y enfermedad del tejido conectivo
• 2. El FR que anticuerpo lo compone? R = IgM dirigida contra el fragmento fc de IgG
• 3. En que enfermedades se presenta comúnmente la trombocitosis? R = Vasculitis, enfermedad de Still y AR.
• 4. En que enfermedades se presenta comúnmente la trombocitopenia? R = LES y Sx antifosfolipido
• 5. Que tratamiento se utiliza en el fenómeno de Raynaud? R = Nifedipino

• 6. Cuales manifestaciones clínicas y de lab sugieren AR?
R = Artritis de MAS DE 3 ARTICULACIONES, RIGIDEZ MATUTINA, nódulo reumatoide y FR positivo lo sugieren.
• 7. Cual es el HLA implicado en la AR?
R = HLA DR4
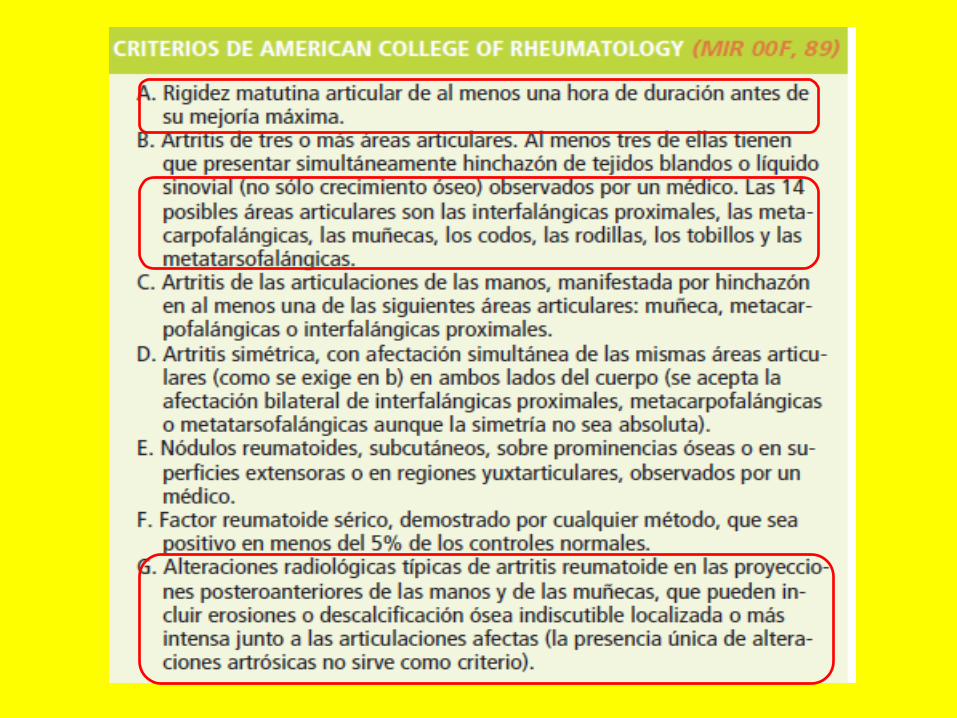
• 8. Cuales son los criterios revisados en 1987 para la clasificación de la AR?
1) Rigidez matutina MAYOR A 30 MINUTOS2) Artritis de 3 O MAS articulaciones3) Artritis de las manos4) Artritis SIMÉTRICA5) NÓDULOS reumatoides6) FR positivo en suero7) Cambios radiológicos
• 9. Cual es el órgano blanco más afectado en la AR? R = La membrana SINOVIAL
• 10. Cuales son las manifestaciones extrarticulares más comunes de la AR? R = ANEMIA NORMO-NORMO por uso de AINES con STDB, TROMBOCITOSIS, nódulos subcutáneos y
SEQUEDAD DE MUCOSAS (Sx Sjogren secundario)

• 11. Cuales son las manifestaciones provocadas por la AR en las glándulas exocrinas y mucosas?
R = Principalmente en las PARÓTIDAS, LAGRIMALES, mucosa y serosa de la VRS y CUELLO UTERINO produciendo DOLOR Y AUMENTO DEL VOLUMEN
• 12. Cuales son las manifestaciones oftalmológicas de la AR? R = EPIESCLERITIS y ESCLEROMALACIA (adelgazamiento).
• 13. Cuales son las manifestaciones cardiovasculares de la AR?1) VALVULARES: MITRAL Y AORTICA. 2) VASCULARES: Vasculitis y ateroesclerosis.
• 14. Cuales son las manifestaciones renales de la AR? R = MICROALBUMINURIA o MICROHEMATURIA.
• 15. Que manifestación pulmonar da la AR? R = FIBROSIS pulmonar manifestada en RX COMO PANAL DE ABEJA.

• 16. En que consiste el Síndrome de FELTY? R = AR, ESPLENOMEGALIA y LEUCOPENIA a expensas de neutrófilos.
• 17. En que consiste el síndrome de CAPLAN? R = AR, NODULOSIS reumatoide pulmonar y NEUMOCONIOSIS.
• 18. Que anticuerpos en la AR tienen la mas alta especificidad diagnostica?
R = ANTICUERPOS ANTIPEPTIDOS CITRULINADOS ANTI- CCP
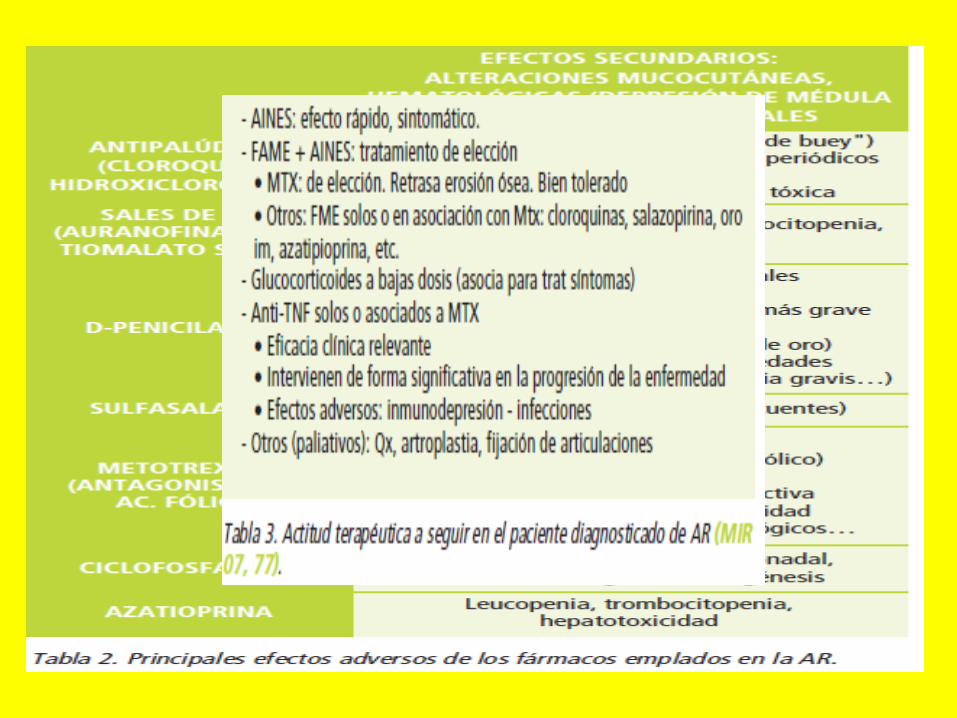
• 19. Cual es el manejo de la AR?1) Los FAME (fármacos moduladores de la enfermedad) deben utilizarse cuando
se hace el dx y antes de que aparezcan los cambios erosivos. 2) La CLOROQUINA y el METOTREXATE son INDUCTORES DE REMISIÓN en AR.
• 20. Cual es el efecto secundario mas común de la CLOROQUINA, la cual es un inductor de la remisión de AR?
R = Musculopatia (miopatía).

ARTRITIS CRONICA JUVENIL



CASO CLINICO• A 25-year-old woman develops painful swelling of both hands and
wrists. She is also very stiff in the morning. Physical examination reveals erythema, swelling and joint line tenderness of the proximal interphalangeal, MCP, and wrists joints. Her RF is positive, ANA is negative, and x-rays of the hands show early erosive joint changes. Which of the following medications is most likely to prevent progression of disease?
(A) D-penicillamine(B) antimalarial(C) methotrexate(D) NSAID or aspirin(E) gold

(C) Methotrexate, 7.5–20 mg once weekly, isthe most commonly recommended diseasemodifying drug, because its effect is more rapidand patients are able to tolerate it for longerperiods of time. Maximum improvement withmethotrexate occurs after 6 months of therapy.Toxicity includes GI upset, oral ulceration, andliver function abnormalities. GI upset in particularmay be ameliorated by concurrent folicacid administration. Pneumonitis has also beenreported.
CASO CLINICO• A 29-year-old woman develops symptoms of painful swelling,
and stiffness of both hands. Physical examination reveals involvement of the proximal interphalangeal joints and MCP joints. Aclinical diagnosis of rheumatoid arthritis is made. Which of the following is the most likely cause of the inflammation in her joints?
(A) activated T cells(B) antineutrophil antibodies(C) microvascular injury(D) interleukin-4 (IL-4)(E) precipitated RF

(A) Numerous mediators of inflammation arefound in the synovium of patients withrheumatoid arthritis (RA). The evidence favoringactivated T cells as the initiators of theinflammation include the predominance ofCD4+ T cells in the synovium, the increase insoluble interleukin-2 (IL-2) receptors (a productof T-cell activation), and amelioration of symptoms by T-cell
removal.
CASO CLINICO• A 63-year-old man is worried that he has RA because his RF serology
is positive in a low titer. He has pain in his left hand and right knee, which usually bother him in the evening. He has not noticed any inflammation or swelling and there is no history of morning stiffness. On examination, there are no active joints. Which of the following statements regarding the presence of RF is correct?
(A) is positive in 10–20% of people over age 65(B) is positive in almost 100% of “classical” RA(C) is seen only in RA(D) is always abnormal(E) is frequently present in osteoarthritis

(A) The presence of RF has little predictivepower in determining the diagnosis of RA.However, it is useful in determining prognosis,as high titers of RF are associated with moresevere and progressive disease, as well as withextra-articular manifestations.

CASO CLINICO• A 30-year-old woman develops painful swelling of her hands, pleuritic chest
pain, and shortness of breath on exertion. She is also very stiff in the morning. Physical examination reveals involvement of the proximal interphalangeal joints and MCP joints. Air entry is decreased to the right lower lobe and the area is dull on percussion. Her RF is elevated and a CXR reveals a pleural effusion. A diagnostic tap is performed, and 500 cc of a straw-colored fluid is removed. Which of the following biochemical patterns is consistent with a pleural effusion due to her primary condition?
(A) exudate protein and LDH ratios with low glucose(B) exudate protein and LDH ratios with high glucose(C) transudate protein and LDH ratios with high glucose(D) transudate protein and LDH ratios with low glucose(E) normal pleural fluid

(A) Pleuritis is common at autopsy in patientswith RA but is not usually symptomatic.Typically, the pleural fluid shows increasedpleural fluid: serum protein and LDH ratios(exudate pattern), and low glucose and lowcomplement levels. Pleuropulmonary
manifestations are more common in men with
CASO CLINICO• A 54-year-old woman with rheumatoid arthritis (RA) presents with
fatigue and low white count (white blood cells [WBC] 2500/mL) on routine blood work. She has no active joint symptoms and her RA is controlled on low dose methotrexate and NSAIDs. On examination, she has chronic joint deformities of her hands and a palpable spleen, which is a new finding. Which of the following is the most likely diagnosis for her low white count?
(A) methotrexate therapy(B) rheumatoid nodules disrupting bone marrow architecture(C) Felty’s syndrome(D) normal variation(E) myelofibrosis

• (C) The triad of chronic RA, splenomegaly, and neutropenia is called Felty’s syndrome. It is associated with high titers of RF and extraarticular disease. The increased susceptibility to infections is secondary to both decreased neutrophil number and function. Felty’s syndrome is rare in African Americans.

CASO CLINICO• A 29-year-old woman develops painful swelling of both hands.
She is also very stiff in the morning. Physical examination reveals involvement of the proximal interphalangeal joints and metacarpophalangeal (MCP) joints. Her RF is positive and ANA is negative. Which of the following medications is most likely to improve her joint pain symptoms?
(A) D-penicillamine(B) an antimalarial(C) methotrexate(D) NSAID or aspirin(E) gold
• (D) This patient has RA and aspirin or other nonsteroidal agents are effective medications for relieving the signs and symptoms of disease. They do little to modify the course of the disease, however. The new generation of NSAIDs that are more specific inhibitors of cyclooxygenase 2 cause less GI toxicity. Glucocorticoids are very powerful at suppressing signs and symptoms of disease and may alter disease progression. Methotrexate is an important disease modifying drug (DMRD) used to prevent joint destruction. Gold and antimalarials were important DMRDs in the past before the use of methotrexate and newer “biological” agents.

CASO CLINICO• A 50-year-old man develops fatigue and painful swelling of both
hands. He is also very stiff in the morning and requires longer time to get ready for work. Physical examination reveals erythema, swelling, and tenderness on palpation of the proximal interphalangeal joints and MCP joints. Plain x-rays of the hand are taken. Which of the following x-ray findings is characteristic of this condition?
(A) loss of articular cartilage and bone erosion(B) normal(C) osteolytic changes(D) osteosclerotic changes(E) osteolytic and osteosclerotic changes together

(A) This patient has features of rheumatoidarthritis, and early in RA there may not be anybony changes seen, except nonspecific findingsof soft tissue swelling and joint effusions. Withlonger active inflammation of the joints, loss ofcartilage and bony erosions can be seen. Thevalue of x-rays is to determine the extent ofbone and cartilage damage.

CASO CLINICO• A 40-year-old woman complains of being very “stiff” in the morning, in
addition to having sore hands and wrists. The symptoms have come on very gradually and she can not recall exactly when they started. Her only other complaint is that of being fatigued. Physical examination reveals involvement of the proximal interphalangeal joints, MCP joints, and wrist joints in a symmetrical fashion. She also has nodules over both elbows. Which of the following is predictive of developing extraarticular features of her condition?
(A) her knees are involved early(B) there is a poor articular response to disease-suppressing medication(C) humoral immunity is suppressed(D) cellular immunity is suppressed(E) she develops an antibody to her own immunoglobulin (RF)

(E) Extra-articular manifestations of RA generallydevelop in patients with high titers ofautoantibody to the Fc component of IgG (alsoknown as rheumatoid factor (RF).

CASO CLINICO• A 67-year-old man has a long history of symmetrical small joint
arthritis with deformities. He now develops shortness of breath on exertion with a dry cough, but no sputum or chest discomfort. His heart sounds have a loud P2, and the lungs have fine bibasilar crackles. Which of the following is the most likely diagnosis of the pulmonary condition associated with his arthritis?
(A) pleuritis(B) cavitating lesions(C) intrapulmonary nodules(D) interstitial fibrosis(E) diffuse pneumonitis

(D) In RA, pleural involvement is very commonat autopsy but infrequently causes symptoms.Interstitial lung disease (ILD) is the mostcommon manifestation of rheumatoid lung disease.RA associated interstitial lung disease(RA-ILD) is usually similar to idiopathic pulmonaryfibrosis (IPF) in terms of its clinical presentation,pathology, disease spectrum, andpathogenesis. Presentation is more common atage 50–60 years, in men (M:F = 2–3:1), and inassociation with seropositive and erosive jointdisease. If pleural fluid is present, glucose levelsare very low.
OSTEOARTROSIS
• 21. Cual es la causa de dolor e incapacidad mas frecuente en ancianos?
R = La OSTEOARTROSIS
• 22. Los nódulos de Heberden (distales) y de Bouchard (proximales) en que enfermedad se manifiestan?
R = Osteoartrosis
• 23. Cual es el órgano blanco de la OA?R = CARTÍLAGO ARTICULAR con distribución asimétrica

• 24. Cual es el cuadro clínico y radiologico de la OA? R = Dolor articular, RIGIDEZ MATUTINA DE NO >30 MIN después de haber realizado una
actividad leve-moderada una noche antes, perdida de la funcionabilidad, CRECIMIENTO DE OSTEOFITOS, micro fracturas, irritación de terminales nerviosas.
• 25. Como diagnosticas OA?1) HC, no se necesitan pruebas de laboratorio. 2) Radiográficamente: DISMINUCIÓN DEL ESPACIO ARTICULAR, presencia de osteofitos o
quistes subcondrales e incremento de la densidad ósea sub condral, lo que se le llama esclerosis subcondral.
• 26. Cual es el tx de elección de la OA? R = ACIDO HIALURONICO, PARACETAMOL y demás AINES. El TRAMADOL se utiliza en
pacientes que no toleran AINES, inhibidores de la COX-2 o déficit renal grave.
• 27. Cual es el tx de la OA utilizado en pacientes intolerantes a AINES o con daño renal? R = TRAMADOL, GLUCOSAMINA, GLUCOCORTICOIDES INTRARTICULARES en caso de
proceso agudo, HIALURONATO el cual restaura las propiedades elásticas y de viscosidad del liquido sinovial, CIRUGÍA.

CASO CLINICO• A 60-year-old man has pain in his left hand and right knee, which is interfering
with his work. The pain came on gradually, first in his hand 6 months ago and now in his knee. It is usually fine when he wakes up, but gets worse as the day progresses. There is no history of any trauma, and he is otherwise well. Taking over-the-counter NSAIDs usually relieves the pain. On examination, there is bony soft tissue swelling of his second and third DIP joints in the left hand and crepitus over the right knee with flexion. There is no erythema or joint effusion. Which of the following characteristics is a risk factor for this condition?
(A) being Chinese(B) being African(C) being male(D) being overweight(E) hyperthyroidism
CASO CLINICO• A 67-year-old woman has pain in her left hand and right knee, which is
interfering with her activities. The pain came on gradually, first in her hand 6 months ago and now in her knee. It is usually fine when she wakes up, but gets worse as the day progresses. There is no history of any trauma, and she is otherwise well. Taking over-the-counter NSAIDs usually relieves the pain. On examination, there is bony soft tissue swelling of his second and third DIP joints in the left hand and crepitus over the right knee with flexion. There is no erythema or joint effusion. Which of the following best describes this disease condition?
(A) disease of the synovial membrane(B) disease of the articular cartilage(C) disease of the entire joint(D) disease of the subchondral bone(E) disease of the ligaments

CASO CLINICO
• Which of the following is the most commonlocation for osteoarthritis?
(A) hip(B) base of thumb(C) knee(D) spine(E) DIP joints of hand

(E) Heberden’s nodes, bony enlargement of theDIP joints of the hand, are the most commontype of osteoarthritis. Although they can presentacutely with pain and inflammation, theyare frequently slow in developing and relativelyasymptomatic.
CASO CLINICO• A 60-year-old man has pain in his left hand and right knee, which is interfering
with his work. The pain came on gradually, first in his hand 6 months ago and now in his knee. It is usually fine when he wakes up, but gets worse as the day progresses. There is no history of any trauma, and he is otherwise well. Taking over-the-counter NSAIDs usually relieves the pain. On examination, there is bony soft tissue swelling of his second and third DIP joints in the left hand and crepitus over the right knee with flexion. There is no erythema or joint effusion. Which of the following characteristics is a risk factor for this condition?
(A) being Chinese(B) being African(C) being male(D) being overweight(E) hyperthyroidism
(D) There are numerous diseases and risk factorsassociated with the development ofosteoarthritis. People of Chinese and Africanheritage have a lower risk than Caucasians,while Native Americans have a higher risk.Women are more affected than men, and obesityis a significant risk factor. Hyperthyroidismis not one of the many metabolic/endocrinedisorders associated with osteoarthritis.

CASO CLINICO• A 57-year-old man has pain in his left hand and right knee, which is interfering
with his work. The pain came on gradually, first in his hand 6 months ago and now in his knee. It is usually fine when he wakes up, but gets worse as the day progresses. There is no history of any trauma, and he is otherwise well. Taking over-the-counter NSAIDs usually relieves the pain. On examination, there is bony soft tissue swelling of his second and third distal interphalangeal (DIP) joints in the left hand and crepitus over the right knee with flexion. There is no erythema or joint effusion. Which of the following is the initial change noticed in the pathogenesis of osteoarthritis?
(A) abnormal chondrocyte function(B) a defect in the extracellular matrix of cartilage(C) inflammatory changes in subchondral bone(D) ligament inflammation(E) synovial inflammation
• (B) It is most likely that the primary change in osteoarthritis occurs in the cartilage. It is possible that there is a disruption of the collagen network of the cartilage, specifically a disruption of the “glue” holding together adjacent fibers.

CASO CLINICO• A 74-year-old woman has pain in her left hand and right knee, which started
months ago, and is now interfering with her activities. The pain gets worse as the day progresses. There is no history of any trauma, and she is otherwise well. Taking over-the-counter acetaminophen usually relieves the pain. On examination, there is bony soft tissue swelling of her second and third DIP joints in the left hand and crepitus over the right knee with flexion. There is no erythema or joint effusion. Which of the following is the most likely explanation for the joint pain of osteoarthritis?
(A) synovial inflammation is not the cause(B) ligament inflammation is a common cause(C) clinically visible (via plain x-ray) fractures are a common cause of pain(D) osteophytes can cause pain(E) muscles are not involved

• (D) Osteophytes can cause pain by stretchingperiosteal nerve endings. Synovial inflammationis frequently seen in osteoarthritis, but notin ligament inflammation. Microfractures, butnot macrofractures, commonly cause pain.Muscle spasm can be an important factor inthe joint pain.

Policondritis recidivante
• A 45-year-old man has had intermittent swelling and pain in the superior part of his auricles for several years. Mild arthritis usually accompanies these episodes. Last year he also had redness, pain, and swelling over the bridge of his nose. Which of the following is the most likely diagnosis?
(A) psoriatic arthritis(B) Behçet’s syndrome(C) Wegener’s granulomatosis(D) relapsing polychondritis(E) rheumatoid arthritis

(D) The disease is relapsing polychondritis andis characterized by frequent remissions andexacerbations of lesions and is rarely fatal.Auricular chondritis and nasal chondritis arethe most common manifestations. It can also besecondary to SLE, RA, Sjögren’s syndrome, andvasculitis.

GOTA• 28. Cual es el cc de la gota?1) Los primeros ataques suelen afectar una sola articulación siendo la mas frecuente LA PRIMERA
MTF (podagra), tobillos, RODILLAS (gonagra), tarsos, muñecas y dedos de las manos, cursa con FIEBRE.
2) La cetoacidosis diabética, anemia hemolítica, síndrome de lisis tumoral y psoriasis cursan con hiperuricemia.
• 29. Menciona algunos fármacos uricosuricos y cuando se trata la gota asintomática?
1) PROBENECID, benzobromarona, LOSARTAN y sulfinpirazona.2) La gota asintomática se trata en casos de litiasis renal, acido úrico > 11, ataques de gota
reiterados y gota crónica.
• 30. Que birrefringencia te indica la identificación de cristales de urato sódico en el liquido sinovial?
R = Birrefringencia NEGATIVA intensa, tienen FORMA DE AGUJA.
• 31. Que característica macroscópica tiene el liquido sinovial en un px con ataque agudo de gota?
R = Apariencia PURULENTA con predominio de PMN
• 32. Que medicamento esta contraindicado en el ataque agudo de gota? R = ALOPURINOL que es un inhibidor de la Xantina-oxidasa
• 33. Cual es el efecto adverso más importante de los uricosuricos?
R = Pueden causar NEFROLITIASIS


• 34. Que causa la pseudogota? R = Cristales de PIROFOSFATO DE CALCIO
• 35. Que etiología tiene la Pseudogota? R = Hemocromatosis, hiperparatiroidismo, hipofosfatasia e hipomagnesemia.
• 36. Cual es el cuadro clínico de la pseudogota? R = Ataque MONOARTICULAR u oligoarticular, PSEUDOPODAGRA, rodillas
(gonagra) y DEDOS DE MANOS (queiagra).
• 37. Cual es la birrefringencia de la pseudogota? R = Birrefringencia POSITIVA pero débil, tienen FORMA DE BASTONES O
ROMBOS.
• 38. Cual es el tratamiento de elección de la pseudogota? R = PARACETAMOL
• 39. Cual es el tratamiento profiláctico de la pseudogota? R = COLCHICINA .6 mg c/12


CASO CLINICO
• A 72-year-old man injures his right knee in a car accident, and now it is swollen and extremely painful to bend the knee. X-rays of the knee rule out a fracture, and joint fluid aspiration reveals an opaque-colored fluid containing rhomboid crystals with weak-positive birefringence. Which of the following is the most appropriate next step in management?
(A) oral prednisone(B) intravenous antibiotics(C) oral NSAIDs(D) acetaminophen(E) allopurinol

(C) In traumatic arthritis, swellings, ecchymoses, muscular spasms, and tenderness tend to be present, but fractures must be excluded. This man has calcium pyrophosphate (CPPD) crystalinduced monoarthritis, so called “pseudogout.” It is most common in the elderly and can be precipitated by minor trauma. The crystals have a rhomboid shape, and the clinical presentation can mimic that of gout. It can be associated with metabolic abnormalities such as hyperparathyroidism or hemochromatosis. Treatment is with an NSAID for 7–10 days. If there are multiple joints involved, then steroids can be considered. An alternative to oral NSAIDs is intra-articular steroids for single joint disease. Allopurinol is not effective in CPPD. Synovial fluid is bloody, but the fluid is of normal viscosity, so a “string” test is usually positive.

CASO CLINICO
• A63-year-old man develops pain and swelling in his knee. It appears warm, red, and swollen with decreased range of movement. A diagnostic aspiration is performed. Which of the following will most likely distinguish pseudogout from gout?
(A) positive birefringent crystals(B) acute onset(C) involvement of single joints(D) involvement of large joints(E) association with diabetes

• (A) Pseudogout (calcium pyrophosphatecrystals—CPPD) is distinguishable from goutby positive birefringent crystals. CPPD areshort, blunt rhomboids, and urate crystals (seenin gout) are needle-shaped with negative
birefringence.

CASO CLINICO
A 63-year-old man with an 8-year history ofrecurrent severe arthritis in his large toes has anelevated creatinine level. Which of the following
mechanisms is the most likely explanation forhis renal impairment?
(A) GN(B) vascular injury
(C) uric acid kidney stones(D) distal tubular atrophy
(E) renal parenchymal uric acid crystals

(E) The typical renal lesions in gout are uratecrystals in the medulla or pyramids, with surroundingmononuclear and giant cell reaction.The degree of renal impairment, however, doesnot correlate with hyperuricemia, and thedecline in renal function correlates with aging,hypertension, renal calculi, or unrelatednephropathy. (Kasper, p. 1704)
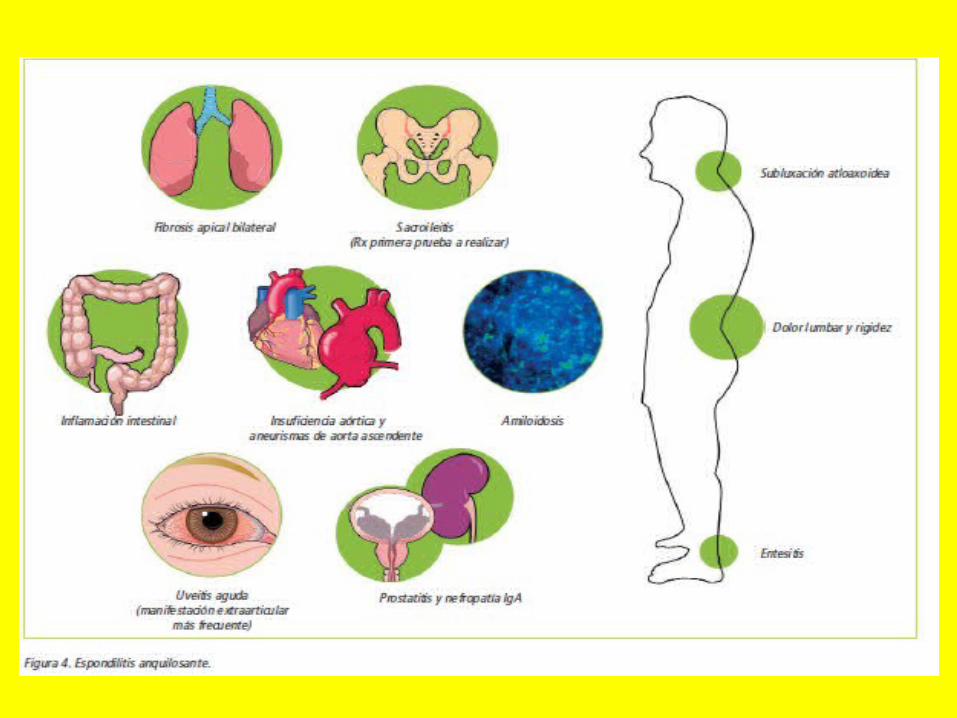
ESPONDILITIS ANQUILOSANTE• 40. Que espondiloartropatias se asocian al HLA-B27? R = ESPONDILITIS ALQUILOSANTE, ARTRITIS REACTIVA, ESPONDILOARTROSIS PSORIASICA,
uveítis anterior aguda.
• 41. Cual es el síntoma inicial de la espondilitis alquilosante (EA)? R = DOLOR en regiones SACROILIACAS Y LUMBARES. En la ex fis HAY DISMINUCIÓN DE LA MOVILIDAD DE
LA COLUMNA LUMBAR, dolor al presionar las regiones sacroiliacas y disminución de la expansión del tórax.
• 42. Cual es la manifestación extrarticular mas frecuente de la EA? R = UVEITIS ANTERIOR, 2/3 de px tiene CAMBIOS EN LA MUCOSA Y SUBMUCOSA DEL COLON E ÍLEON
TERMINAL
• 43. Cuales son los hallazgos más comunes en imagen obtenidas en la espondilitis anquilosante? R = Erosiones y esclerosis sacroiliacas, IMAGEN EN COLUMNA DE BAMBU
• 44. Cual es el manejo de la EA? R = AINES, COX-2, Infliximab, Etanercept mas terapia física. Indometacina, INFLIXIMAB que disminuye el FNTa.



CASO CLINICO• A 22-year-old man has symptoms of low back pain and stiffness.
After several months of mild symptoms, he notes more severe stiffness at night and hip pain. On physical examination, there is paravertebral muscle tenderness and limited flexion of the lumbar spine. Figure shows an x-ray of the lumbar spine. Which of the following is the most likely diagnosis?
(A) Reiter syndrome(B) Marfan syndrome(C) ankylosing spondylitis (AS)(D) RA(E) pseudogout

CASO CLINICO• A 27-year-old man has a history of low back pain and stiffness. After
several months of mild symptoms, he notes more severe stiffness at night and hip pain. On physical examination, there is paravertebral muscle tenderness and limited flexion of the lumbar spine. X-ray of the lumbar spine shows sacroiliitis. In addition to recommending physiotherapy and exercise, which of the following is the most appropriate next step in management?
(A) NSAID therapy(B) phenylbutazone(C) azathioprine(D) acetaminophen(E) prednisone
• (A) All NSAIDs are probably equally effectivein the treatment of this man’s ankylosingspondylitis. Options include indomethacin ornaproxen, but not phenylbutazone since it cancause aplastic anemia. Exercise and maintainingproper posture are very important.

CASO CLINICO• A 27-year-old man has a history of low back pain and stiffness. Recently, he
has noticed more severe stiffness at night and hip pain. The symptoms improve in the morning after doing some “stretching” exercises. On physical examination, there is paravertebral muscle and sacroiliac joint tenderness with limited flexion of the lumbar spine. A2/6 diastolic murmur is also heard at the left sternal border radiating to the apex. Which of the following is the most likely diagnosis for the diastolic murmur?
(A) mitral stenosis(B) tricuspid stenosis(C) aortic insufficiency(D) pulmonic insufficiency(E) tetralogy of Fallot
(C) The frequency of aortic insufficiency hasbeen about 4% in ankylosing spondylitis (AS).Other cardiac valve anomalies are not increasedin incidence. Rarely, congestive heart failure orthird degree heart block can occur as well.(Kasper, p. 1994).

CASO CLINICO• A23-year-old man notices new low back pain, stiffness, and left eye
discomfort. Sunlight also bothers his eyes. The back pain is worse at night and described as a dull ache in the back and buttock area. On physical examination, there is paravertebral muscle, iliac crest, and ischial tuberosity tenderness with limited flexion of the lumbar spine. His eye is inflamed and the pupil is constricted. Pelvic x-rays show sacroiliitis. Which of the following is the most likely diagnosis for his eye symptoms (it is the most common extra-articular manifestation of this condition)?
(A) glaucoma(B) acute anterior uveitis(C) keratitis(D) conjunctivitis(E) episcleritis

(B) Acute anterior uveitis is the most commonextra-articular manifestation of ankylosingspondylitis (AS). Pain, photophobia, andincreased lacrimation are the usual symptoms.Attacks are unilateral and tend to recur, oftenin the other eye. Cataracts and secondary glaucomaare not uncommon sequelae. The iritis isusually managed with local glucocorticoidadministration in association with a mydriaticagent.

ENFERMEDAD DE REITER• 45. Cuales son los datos más comunes de ARTRITIS REACTIVA o
enfermedad de Reiter? R = Ligado al HLA B27, oligoartritis, CONJUNTIVITIS, URETRITIS,
CERVICITIS, ULCERAS ORALES x un CUADRO INFECCIOSO PREVIO.
• 46. Que precede a una manifestación de ARTRITIS REACTIVA o síndrome de Reiter?
R = Alguna INFECCIÓN por SALMONELLA, SHIGELLA, YERSINIA,
CLAMYDIA TRACHOMATIS +++ o CAMPYLOBACTER que PRECEDE a la MANIFESTACIÓN ARTICULAR 3-4 semanas después.
• 47. Cual es el estudio de laboratorio o gabinete de elección del
síndrome de Reiter? R = CULTIVO CON ANTIBIOGRAMA, se puede encontrar también Ac anti
bacteriano en el suero o liquido sinovial o DNA bacteriano.

ARTRITIS SORIASICA• 48. Que es la artritis soriasica? R = Ligado al HLA B27. Se define como una ARTRITIS usualmente
SERONEGATIVA que se ASOCIA A SORIASIS.
• 49. Cual es el cuadro clínico de la artritis soriasica? R = PRECEDE PSORIASIS A ARTRITIS, ARTRITIS ASIMÉTRICA con DEDOS EN
APARIENCIA DE SALCHICHA (DACTILITIS) de los dedos de manos y pies.
• 50. Como diagnosticas artritis soriasica? R = HC, y RX con evidencia de SACROILEITIS ASIMÉTRICA, alteraciones de la
conformación de hueso nuevo con IMAGEN DE PUNTA DE LÁPIZ EN UNA COPA.
• 51. Cual es el manejo de la artritis soriasica? R = AINES E INFLIXIMAB. Tratamiento de soriasis.


CASO CLINICO• A 19-year-old man has a chronic papulosquamous skin disorder
involving his knees and elbows. He now has dull low back pain and morning stiffness that lasts a few hours. On examination, forward flexion at the lumbar spine is reduced but neck movements are normal. There is stress tenderness of both sacroiliac joints. Which of the following is the most likely diagnosis?
(A) RA(B) ankylosing spondylitis (AS)(C) psoriatic arthritis(D) reactive arthritis(E) PMR

(C) This patient has a sacroiliac form of arthritisseen in patients with psoriasis. Patients withpsoriasis can develop five different patterns ofmusculoskeletal symptoms. These includearthritis of the DIP joints; asymmetric oligoarthritis;symmetric polyarthritis similar to RA; spineand sacroiliac type; and arthritis mutilans, ahighly destructive form. Most patients withpsoriatic arthritis also have nail involvement.Only about a quarter actually develop a progressive,destructive disease. Uric acid may beelevated because of high tissue turnover but isnot part of the pathogenesis of joint disease.

ARTRITIS GONOCOCICA
• 52. Cual es el cuadro clínico de la artritis gonococcica?
R = Poliartritis, tenosinovitis (60%) y monoartritis purulenta en la rodilla 40%
• 53. Como diagnosticas y tratas la artritis
gonococcica?R = Cultivo de liquido sinovial, CEFTRIAXONA iv o
LEVOFLOXACINO a los alérgicos a penicilina.
HLA B27
• Cuales patologías están ligadas al HLA B27?1) Espondilitis anquilosante2) Artritis reactiva o Síndrome de Reiter3) Artritis soriasica

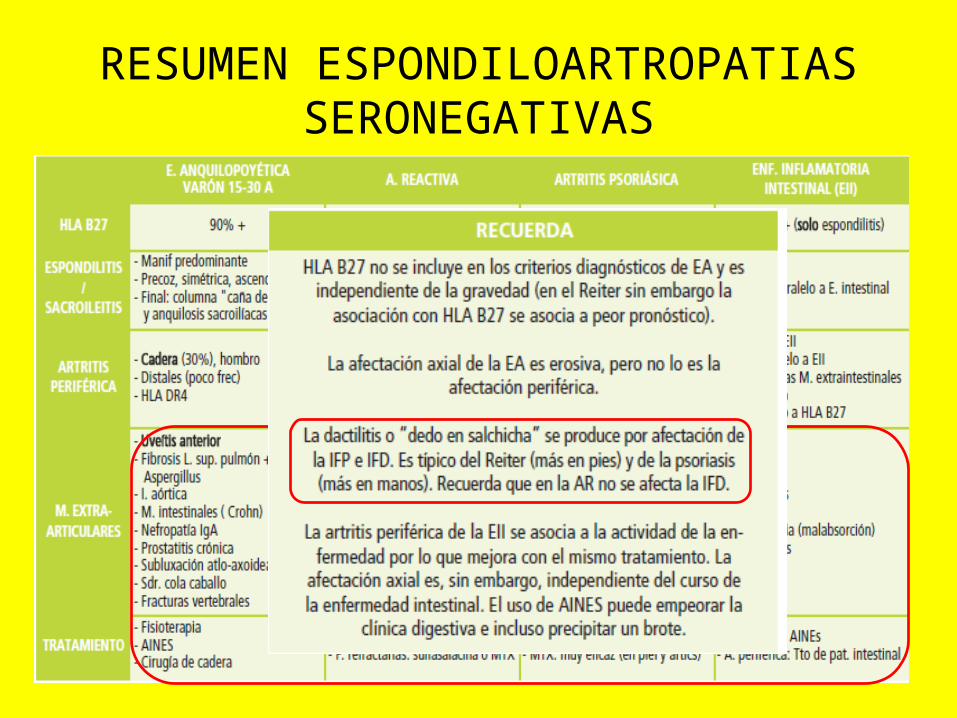
RESUMEN ESPONDILOARTROPATIAS SERONEGATIVAS

CUCI Y CHRON
• 54. Cuales son los 2 tipos de artropatía en px con enfermedad de Chron y CUCI?
R = ESPONDILITIS ANQUILOSANTE y ARTRITIS PERIFÉRICA.
• 55. Cual es el cc de la enfermedad de CHRON? R = DOLOR ABDOMINAL, FIEBRE, diarrea, ULCERAS ORALES,
anorexia, hipersensibilidad de vientre al tacto, masa abdominal, disminución de peso y SANGRE EN EVACUACIONES.
• 56. Cual es el cc de CUCI? R = Diarrea, HEMATOQUEZIA, DOLOR ABDOMINAL con
hipersensibilidad y LEUCOS AUMENTADOS EN LAS EVACUACIONES.

CASO CLINICO• A 32-year-old woman has a long history of intermittent bloody diarrhea
and crampy abdominal pain. Recently, her bowel symptoms have increased and she is having 4–6 bowel movements a day with mucus and blood in the stool. She now has a low-grade fever, loss of appetite, and new musculoskeletal symptoms. Which of the following is the best description of this patient’s accompanying arthritis?
(A) asymmetric migratory polyarthritis involving the large joints of the arms and legs
(B) not usually associated with disease flares(C) a progressive, crippling course(D) symmetrical small joint involvement(E) seropositive
(A) In inflammatory bowel disease, there aretwo common types of arthritis involvement.The first is an asymmetric, migratory polyarthritisthat affects the large joints of thelower and upper extremities and is closelyrelated to the activity of bowel disease.Spondylitis is also common (though not alwayssymptomatic) and is not always related toactivity of bowel disease.

ESPONDILOARTROPATIA INDIFERENCIADA
• 57. Que caracteriza a las espondiloartropatias indiferenciadas? R = TODOS AQUELLOS CC QUE REÚNEN CRITERIOS DE CLASIFICACIÓN
de las espondiloartropatias PERO NO LOS CRITERIOS ESPECÍFICOS o cc característicos de c/u de ellas.
• 58. Cuales son las manifestaciones clínicas mas comunes de las espondiloartropatias indiferenciadas?
R = 60-75% desarrolla datos de espondilitis alquilosante o artritis soriasica.
• 59. Cuales son los medicamentos utilizados en las espondiloartropatias indiferenciadas?
R = AINES, COX-2, infliximab


FIBROMIALGIA• 60. Como se define a la fibromialgia? R = Dolores difusos, presentes por > 3 MESES y que involucran los 4 CUADRANTES
DEL CUERPO Y ESQUELETO AXIAL, NO HAY SUEÑO REPARADOR y AMANECEN CANSADOS + la presencia a la PALPACIÓN DIGITAL DE 11 PUNTOS DOLOROSOS DE LOS 18.
• 61. Que estudio auxiliar te ayuda a diagnosticar fibromialgia? R = No hay estudio que pueda ayudar
• 62. Cual es el tratamiento de la fibromialgia?
1) AMITRIPTILINA antes de dormir,
2) FLUOXETINA para el dolor, no hay tratamiento especifico
• 63. Cual es el pronóstico de la fibromialgia? R = DESFAVORABLE ya que el 25% desarrolla incapacidad importante.

SX ANTIFOSFOLIPIDO• 65. Cuales son los criterios laboratoriales diagnósticos de SAF?
R = Anticuerpos ANTICARDIOLIPINAS y anticoagulante LUPICO.
• 66. Cual es la etiología del SAF? R = Se desconoce. Los linfocitos T.
• 67. Cuales son los mecanismos por los cuales se presenta trombosis en el SAF? R = INHIBICIÓN de la actividad ANTICOAGULANTE, inhibición de FIBRINÓLISIS y respuesta mediada por
células aumentada
• 68. Cual es el cc característico del SAF? R = TROMBOSIS, livedo reticularis, ABORTOS FRECUENTES.
• 69. Que es el SAF catastrófico? R = Resulta de una forma acelerada que produce falla organica multiple
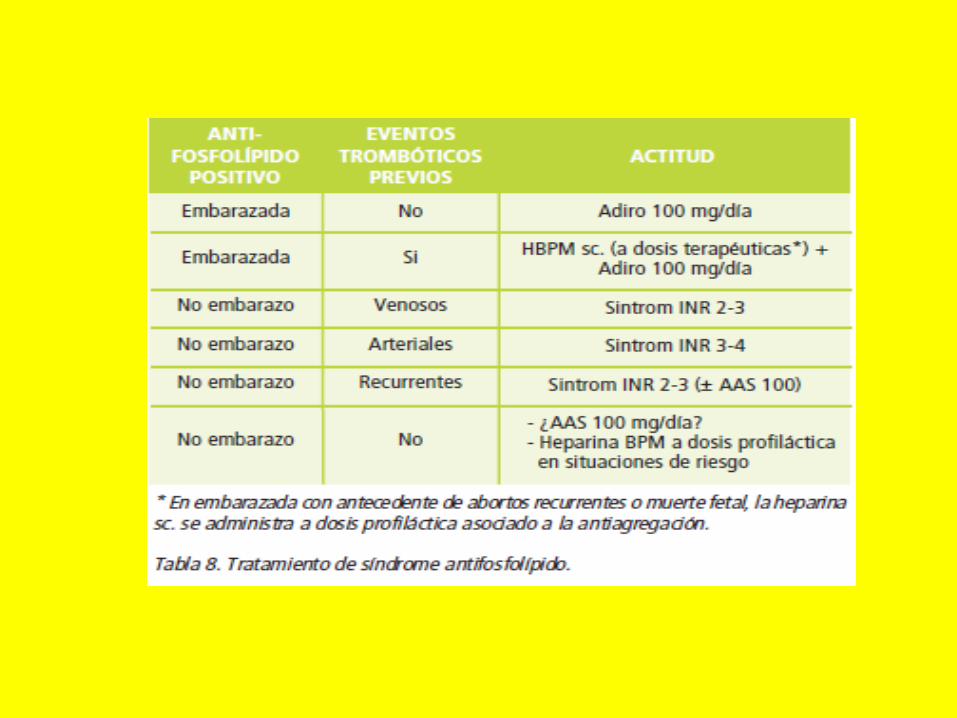
• 70. Cual es el manejo del SAF? R = PREDNISONA ELIMINA ANTICOAGULANTE. ASA 100 mg cada 24 hrs, estatinas, HEPARINA EN
EMBARAZADAS y WARFARINA DESPUÉS DEL EMBARAZO.


FIEBRE REUMATICA
• 71. En la fiebre reumática, dentro de las manifestaciones cardiacas, que podemos encontrar?
R = NÓDULOS/cuerpos de ASCHOFF (que son una confluencia de monocitos y macrófagos rodeados por fibrosis) y CARDITIS (Infiltrado inflamatorio que abarca las 3 capas del corazón). Se utilizan LOS CRITERIOS DE JONES para su diagnostico.
• 72. Cual es el tratamiento de elección para la fiebre reumática?
R = PENICILINA, ASA y HALOPERIDOL EN CASO DE COREA.

LUPUS ERITEMATOSO SISTEMICO• 73. Que HLA tienen relación con el LES?
1) HLA B8, HLA DR2 y DR3.
2) Los alelos de HLA están en el brazo corto del CROMOSOMA 6.
• 74. Que fármacos inducen la producción de anticuerpos antinucleares y LES? R = HIDRALAZINA, procainamida, clorpromazina, ISONIAZIDA y diversos anticonvulsivantes.
• 75. Cual es el cc del LES en cada aparato – sistema y con que padecimientos se relaciona? 1. Se relaciona con: PTI, ANEMIA HEMOLITICA Y TIROIDITIS. 2. Constitucionales: la FATIGA es lo mas común 3. Mucocutaneas: 80%, LESIONES DISCOIDES observándose en cara, pabellones auriculares y el AREA DE
V DEL ESCOTE. Eritema malar o en ALAS DE MARIPOSA QUE ES FOTOSENSIBLE. EL neonatal QUE SE PRESENTA EN LOS HIJOS DE PX CON LES POR EL PASO DE IgG CARACTERIZÁNDOSE POR LESIONES CUTÁNEAS Y BLOQUEO CARDIACO CONGÉNITO EN LOS PRIMEROS 6 MESES DE EDAD. ALOPECIA.
4. Musculoesqueletico: ARTRALGIAS con artritis. Osteonecrosis en la cabeza femoral, humeral, cóndilos femorales, carpo, tarso manifestándose clínicamente con dolor que mejora con el reposo.
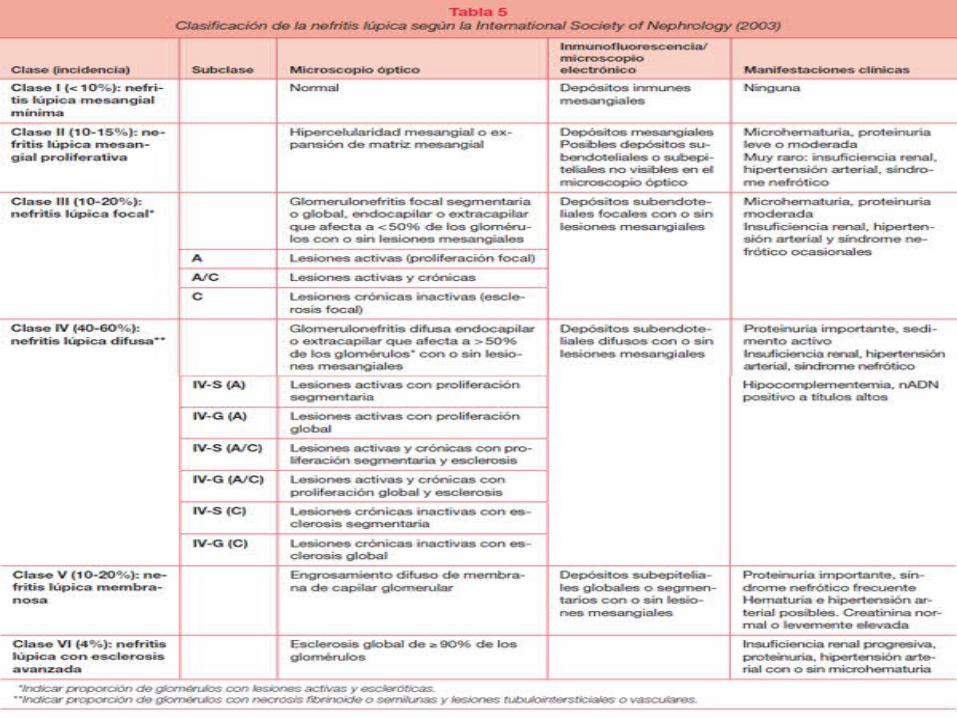
5. Renal: nefritis lupica siendo la mas común la TIPO IV ¨GLOMERULONEFRITIS PROLIFERATIVA DIFUSA¨. 6. SNC: Meningitis aséptica, EVC, síndromes desmielinizantes y cefaleas. 7. Cardiopulmonar: En corazón con VEGETACIONES ENDOCARDICAS de LIBMAN-SACKS, en pleura lo
mas común es pleuritis con o sin derrame pleural con niveles altos de proteínas DHL, complejos inmunes, ANA y células LE. LA VALVULA MAS AFECTADA ES LA MITRAL.
8. Gastrointestinal: Se puede presentar con SEROSITIS, disfagia y dispepsia muy a menudo. 9. Hematológico: PANCITOPENIA Y >TTP. Anemia por deficiencia de hierro MICROCITICA-HIPOCROMICA.

• 76. Cual es el inmunosupresor de elección para la nefritis lupica y cual es el de elección en caso de serositis.?
1) Nefritis lupica: CICLOFOSFAMIDA2) Serositis: METOTREXATO
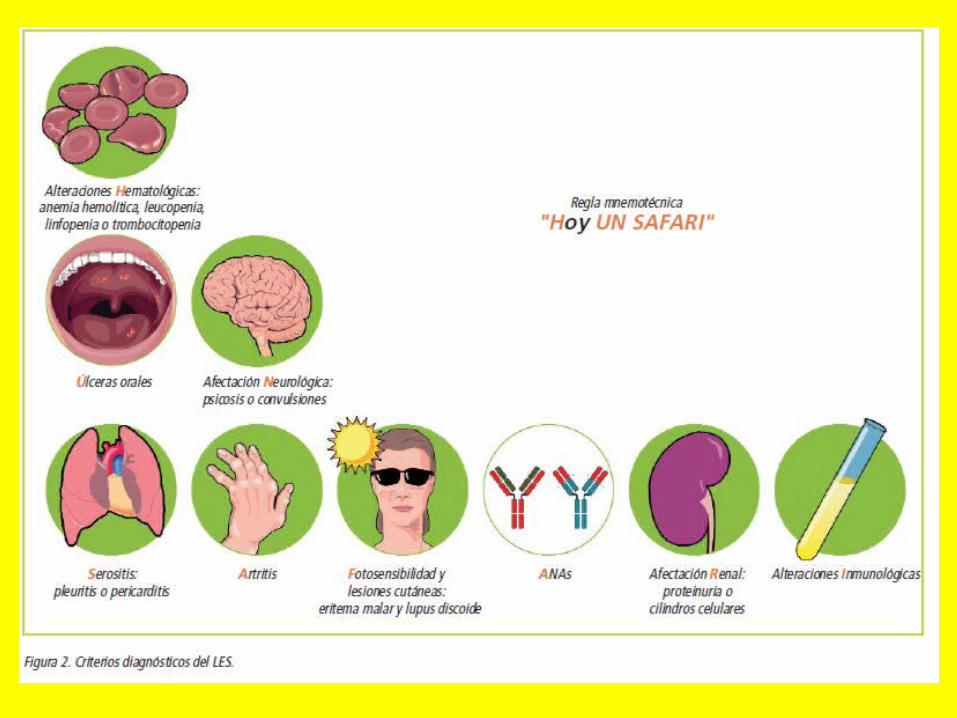
• 77. Cuantos criterios se revisaron en 1997 para dx de lupus? 11 criterios entre los cuales están: 1. Eritema malar 2. Lupus discoide 3. Foto sensibilidad 4. Ulceras orales 5. Artritis no erosiva 6. Serositis 7. Afección renal 8. Afección neurológica 9. Afección hematológica 10. Afección inmunológica 11. ANA + y se requieren de 4 criterios para el diagnostico.
• 78. Que medicamentos han mejorado la supervivencia en pacientes con nefropatía lupica?
R = GLUCOCORTICOIDES + CICLOFOSFAMIDA



CASO CLINICO
• A22-year-old woman develops a red rash over her cheeks, and pain and swelling in both knees as well as several small joints in her hands. Medical evaluation reveals oral ulceration and 3+ proteinuria. Which of the following is the most sensitive test for the diagnosis of this condition?
(A) LE cells(B) ANAs(C) anti-Sm(D) anti-Ro(E) antiphospholipid

(B) ANAs are present in 98% of patients withSLE. Repeatedly negative tests make the diagnosisof SLE very unlikely. Unfortunately, thetest is not specific and may be positive innormal people (especially in older individuals),or secondary to infections, drugs, or otherautoimmune disorders.

CASO CLINICO• A 25-year-old woman with SLE notices increasing fatigue and shortness of
breath on exertion. Her usual SLE symptoms of joint discomfort, chest pain, and fevers are not present. On examination, there are no active joints, but she is jaundiced. Laboratory studies show hemoglobin 9 g/dL, WBC 5000/mL, platelets 150,000/mL, reticulocyte count 4%, direct antiglobulin test: positive, total bilirubin 4 g/dL, direct 0.5 mg/dL, aspartate amino transferase (AST) 20 U/L, alanine amino transferase (ALT) 15 U/L, LDH 300 U/L. Which of the following is the most likely diagnosis?
(A) autoimmune hepatitis(B) hemolytic anemia(C) viral hepatitis(D) acute blood loss(E) Gilbert syndrome

(B) This patient with SLE has developed autoimmunehemolytic anemia. Treatment consists ofhigh-dose oral steroids. The positive Coombs’test (direct antiglobulin test), high indirect bilirubin,high LDH, and high retic count are all supportiveof hemolytic anemia. Anormal AST and
ALT rule out hepatitis.

CASO CLINICO• A30-year-old woman develops a rash over her cheeks, nose, and
ears. She also has pain and swelling in her wrists as well as several small joints in her hands. Medical evaluation reveals oral ulceration and 3+ proteinuria. Her ANAis positive. Which of the following is the most likely cardiac manifestation of her disease?
(A) pericarditis(B) myocarditis(C) aortic regurgitation(D) nonbacterial endocarditis(E) myocardial vasculitis with infarction

(A) This patient has SLE and pericarditis, sometimesleading to tamponade, is the most commonmanifestation of cardiac disease. Myocarditisdoes occur and can cause arrhythmias, suddendeath, or heart failure. Libman-Sacks endocarditisis associated with thrombotic eventsor, less commonly, valvular regurgitation.Myocardial infarction is more commonly aresult of atherosclerotic disease than vasculitis.

CASO CLINICO• A 24-year-old is referred for assessment of a low white cell count. She has
no past medical history and is not on any medications. Her only symptoms are of joint discomfort in her hands, and occasional sharp chest pains that change with breathing. On examination, there is inflammation of some MCP and DIP joints in both hands, and the rest of the examination is normal. Her WBC is 3500/mL and the lymphocytes are low (15%) and PMNs are normal. Which of the following is the most likely diagnosis?
(A) periarteritis nodosa(B) SLE(C) scleroderma(D) DM(E) osteoarthritis
(B) Leukopenia occurs in almost two-thirds ofthe SLE patients, and the differential count isusually normal. Lymphocytes and platelets canalso be reduced.

CASO CLINICO• A 26-year-old woman develops a red rash over her cheeks and
pain, and swelling in both wrists as well as several small joints in her hands. The rash gets worse on sun exposure and involves her cheeks, nose, ears, and chin. Medical evaluation reveals oral ulceration and 3+ proteinuria. Which of the following is the most specific test for diagnosis of this condition?
(A) lupus erythematosus (LE) cells(B) antinuclear antibody (ANA)(C) anti-Sm antibody(D) anti-Ro antibody(E) antiphospholipid antibody

• (C) Anti-Sm detects a protein complexed to six species of small nuclear ribonucleic acid (RNA). It is believed to be very specific for SLE. However, only 30% of patients have a positive test. In the case presented, there are enough clinical criteria (four) to confirm the diagnosis of SLE with 98% specificity and 97% sensitivity.

CASO CLINICO• A young woman presents with a facial rash, arthralgias, and
fatigue. The rash on her face is erythematous and raised, her heart and lungs are normal, and wrists are swollen and tender on palpation. She has mild thrombocytopenia (90,000/mL). Which of the following is the most appropriate initial autoantibody test?
(A) anti-double-stranded (ds) deoxyribonucleic acid (DNA)(B) anti-Sm(C) anti-Ro or La(D) ANA(E) antiphospholipid antibodies (lupus anticoagulant)
• (D) ANA is the most important diagnosticautoantibodies in patients being evaluated forSLE. It is rare to have ANA negative SLE. Theother antibodies can occur in SLE but not assensitive for the diagnosis as ANA. AntidsDNAand anti-SM are specific for SLE butnot sensitive.

CASO CLINICO• A34-year-old woman develops a red rash over her cheeks,
frequent oral ulcers, and pain and swelling in both wrists as well as in severalsmall joints in her hands. Medical evaluation reveals a positive ANA, and 3+ proteinuria. Which of the following organ involvement will cause the most symptoms during the course of this disease?
(A) renal pathology(B) cardiopulmonary pathology(C) musculoskeletal pathology(D) thrombotic events(E) skin changes
(C) About 95% of patients will develop musculoskeletal symptoms during the course of SLE.
Arthralgias and myalgias predominate, butarthritis, hand deformities, myopathy, and avascularnecrosis of bone also occur. About 85% ofpatients will have hematologic disease and 80%will have skin manifestations.
CASO CLINICO• A27-year-old woman presents with a red rash over her cheeks, and
pain and swelling in both knees as well as several small joints in her hands. She notes that the rash is worse with sun exposure. Medical evaluation reveals oral ulceration, positive ANA, and 3+ proteinuria. Which of the following is the most likely mechanism for the renal damage in this condition?
(A) vasculitis(B) microemboli(C) antibasement membrane antibodies(D) deposition of circulating immune complexes(E) primary tubular atrophy

(D) Renal disease is usually secondary to deposition of circulating immune complex. Although most patients with SLE have such deposits, only half have clinical nephritis as defined by proteinuria. Renal biopsy can provide both prognostic and therapeutic information.

ENFERMEDAD DE STILL• 79. Que caracteriza clínicamente a la enfermedad de Still?
R = VARIANTE DE LA ARTRITIS REUMATOIDE en la cual hay FIEBRE DE MAS DE
40 y con precipitación posterior varios grados debajo, odinofagia y poliadenopatias. LO PRECEDE FARINGITIS.
• 80. Cual es una manifestación característica de la enfermedad de still?
R = EXANTEMA NO PRURIGINOSO, maculopapular de COLOR SALMÓN en TÓRAX Y ABDOMEN.
• 81. Cual es el laboratorio distintivo de la enfermedad de Still?
R = LEUCOCITOSIS > 40, VSG AUMENTADA, hipergamaglobulinemia IgG y anemia. NO se detectan AUTOANTICUERPOS NI FR.
• 82. Cual es el manejo de la enfermedad de Still? R = AINES

CASO CLINICO• An 18-year-old man has had fever for several weeks. The fever
occurs on an almost daily basis and is associated with an evanescent salmon-colored truncal rash. He has diffuse arthralgias, and an extensive investigation for infections and malignancy is negative. Which of the following is diagnostic of this condition?
(A) high-titer rheumatoid factor (RF)(B) positive ANA(C) response to steroid therapy(D) response to nonsteroidal antiinflammatory drug (NSAID) therapy(E) lymph node biopsy

• (D) Still’s disease (juvenile RA) in an adultmay present as fever of unknown origin.Unfortunately, RF is often negative, and aresponse to NSAIDs along with exclusion ofother diseases confirms the diagnosis.

ESCLEROSIS SISTEMICA O ESCLERODERMIA
• 83. Como se define la enfermedad llamada esclerosis sistémica o esclerodermia? R = Es una enfermedad que se caracteriza por la aparición de fibrosis difusa de la piel y órganos internos
• 84. Que es el síndrome de CREST en esclerosis sistémica o esclerodermia? R = Calcinosis cutánea, fenómeno de Raynaud, trastorno de la motilidad Esofágica, eSclerodactilia y
Telangectasia
• 85. Cuales son las variantes de esclerosis sistémica o esclerodermia y sus principales afecciones?
1) LIMITADA 80%: en la que hay ENDURECIMIENTO DE LA PIEL, manos o cara.
2) DIFUSA: afecta tronco y extremidades, muñecas, tobillos, rodillas, RIÑÓN (GLOMERULOESCLEROSIS DIFUSA) y corazón con CARDIOPATÍA RESTRICTIVA. La principal CAUSA DE MUERTE ES PULMONAR POR HIPERTENSIÓN O FIBROSIS.
• 86. Cuales son las manifestaciones cutáneas de la esclerodermia? R = La piel se ve brillante , con PERDIDAS DE PLIEGUES Y ATROFIA DE FOLÍCULOS PILOSOS, se siente
ACARTONADA, la afección facial provoca una cara afilada.
• 87. Cuales son las manifestaciones vasculares de la esclerodermia? R = Fenómeno de Raynaud en dedos de manos, pies, nariz, oídos y lengua.

• 88. Cuales son las manifestaciones pulmonares de la esclerodermia? R = Enfermedad pulmonar INTERSTICIAL EN LA DIFUSA CON PATRÓN RESTRICTIVO. Hipertensión pulmonar y
cor pulmonale. En la TAC se puede ver si hay actividad (imagen en vidrio despulido) o solo fibrosis (imagen en panal de abejas)
• 89. Cuales son las manifestaciones GI de la esclerodermia? R = La mayoría tiene AFECCIÓN ESOFÁGICA CARACTERIZADA POR ERGE, pirosis y dificultad para el paso de
alimentos sólidos siendo de preferencia los líquidos.
• 90. Cual es la manifestación renal de la esclerodermia? R = Crisis renal esclerodermica (HAS MALIGNA) que conlleva a una IR rápidamente progresiva.
• 91. Cuales son los laboratorios de esclerosis sistémica o esclerodermia? R = ANA +, depende del órgano afectado, AC VS ESCLERODERMIA SCL-70. En la BIOPSIA aparece EXCESO DE
DEPOSITO DE COLÁGENO EN PIEL, TCS Y VASOS SANGUÍNEOS que puede aparecer de manera lineal (esclerosis lineal) o en parches hipocromicos. DIFUSA: ANA y TOPOISOMERASA I, SX CREST: AC ANTICENTROMERO.
• 92. Cual es el manejo de la esclerosis sistémica o esclerodermia?
R = D- PENICILAMINA. Para el FENÓMENO DE RAYNAUD se da NIFEDIPINO o losartan. Iloprost que es análogo de la prostaciclina para ulceras digitales. CICLOFOSFAMIDA, corticoides, SINDENAFIL para ENFERMEDAD INTERSTICIAL PULMONAR. PIEL (morfea del tronco hipocromica) luz UV, CORTICOIDES TÓPICOS, si se generaliza se da metotrexate o CORTICOIDES SISTÉMICOS. CALCINOSIS diltiazem o NIFEDIPINO. DAÑO RENAL IECAS. TELANGIECTASIAS ESCLEROSIS. GI PROCINETICOS Y ERITROMICINA por que ESTIMULA LA MOTILINA, NO CISAPRIDA (QUE PUEDE PRODUCIR SX QT LARGO, TAQUICARDIA VENTRICULAR Y DESENLACES FATALES). ARTRALGIAS acetaminofen, PERICARDITIS AINES, corticoides o CICLOFOSFAMIDA.




CASO CLINICO• A39-year-old woman complains of developing painful pale fingers on
cold exposure for the past 5 years. Recently, she has noticed swollen fingers and tight skin, which limit flexion and extension. She also has new abdominal symptoms that are bothersome. On examination, the skin on the fingers is smooth and shiny with associated edema. The rest of the examination is normal. Which part of the gastrointestinal (GI) tract is most frequently involved in this condition?
(A) esophagus(B) stomach(C) duodenum(D) ileum(E) colon

• (A) This patient has scleroderma andesophageal symptoms are present in more than50% of patients. They are due to the reducedtone of the gastroesophageal sphincter anddilation of the distal esophagus. Gastric andsmall intestinal motility problems can alsooccur. Vascular ectasia in the GI tract can resultin bleeding.

CASO CLINICO
• A22-year-old woman develops color change in her fingers with cold exposure. The fingers turn white, then blue, and finally red. Which of the following statements regarding this condition is incorrect?
(A) may lead to gangrene of the fingers(B) may precede the onset of scleroderma(C) symptoms can be brought on by vibration or stress(D) pallor (white color) associated with coldness and numbness
while rubor (red color) associated with pain and tingling(E) affects the sexes equally

(E) Raynaud’s phenomenon may lead to gangreneof the fingers. It can be primary(Raynaud’s disease) or secondary to other diseases,especially scleroderma, in which it can bethe presenting symptom. In women, the primaryform is common (over 50%), and the phenomenonis generally much more frequent inwomen. Digital infarction is much morecommon in relationship to scleroderma than itis in primary Raynaud’s disease.
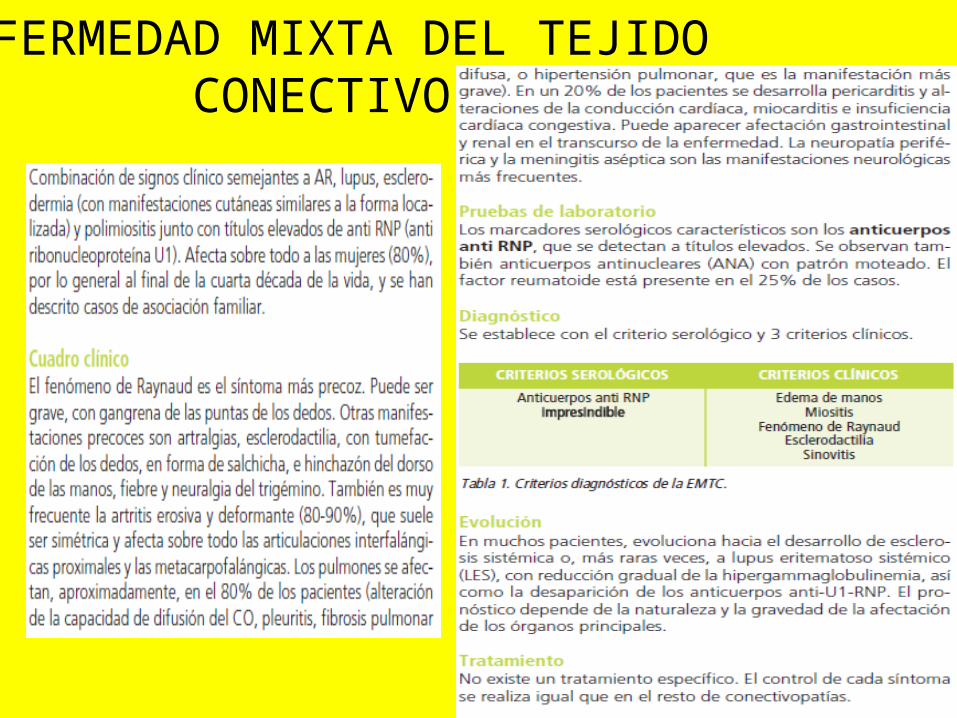
ENFERMEDAD MIXTA DEL TEJIDO CONECTIVO

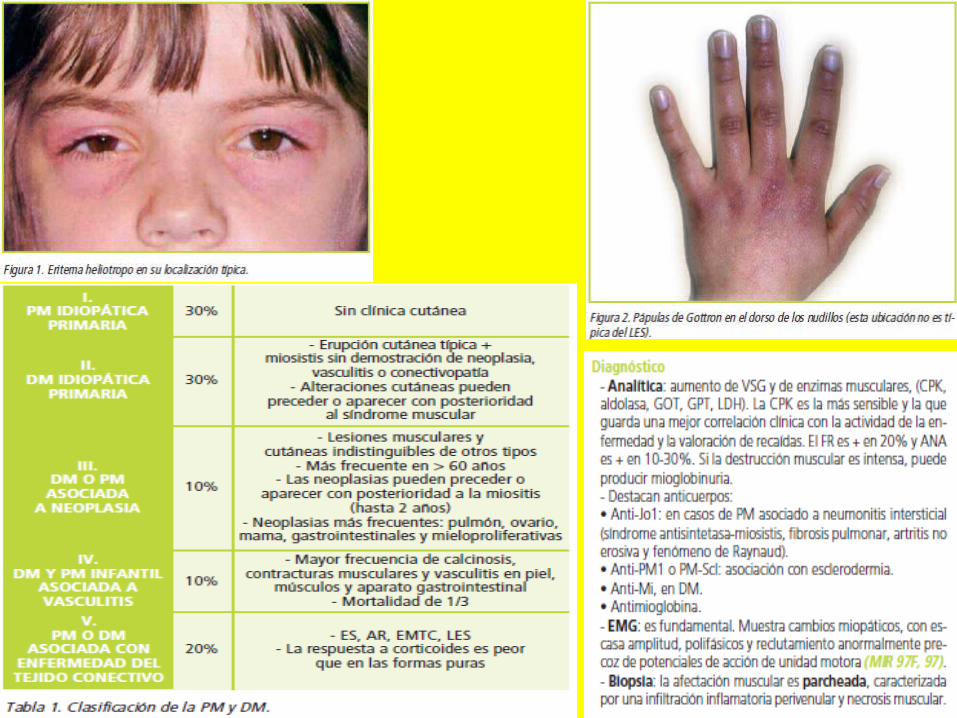
MIOSITIS Y DERMATOMIOSITIS• 93. Que tipo de padecimientos son la miositis y dermatomiositis? R = Etiologia desconocida y se caracterizan por DEBILIDAD MUSCULAR PROXIMAL GRADUAL
Y PROGRESIVA.
• 94. Que células predominan en la biopsia con DERMATOMIOSITIS?
R = Infiltrado de CÉLULAS B Y T CD4
• 95. Que células predominan en la biopsia con POLIMIOSITIS?
R = Predominan las células T CD8 A NIVEL ENDOMICIAL.
• 96. Cuales son los datos clínicos de la miositis y dermatomiositis?1) Dificultad para la deglución por afección de musculo estriado, EXANTEMA COLOR ROJO
OBSCURO CARACTERÍSTICO CON DISTRIBUCIÓN MALAR PARECIDO A LES QUE PUEDE ESTAR EN CARA, CUELLO Y ESPALDA.
2) EDEMA PERIORBITARIO AMORATADO (heliotropo) SOBRE LOS PARPADOS. 3) Fiebre, DISMINUCIÓN DE LA FUERZA PROXIMAL y V del cuello.

• 97. El SIGNO DE GOTTRON es patognomónico de miositis y dermatomiositis, que lo caracteriza?
R = ERITEMA PERIUNGUEAL, PLACAS ERITEMATO-ESCAMOSAS SOBRE DORSO DE LAS ARTICULACIONES INTERFALANGICAS Y METACARPOFALANGICAS.
• 98. Según los criterios de Bohan y Peter como diferencias la dermatomiositis de la miositis-polimiositis?
R = 1) DERMATOMIOSITIS: 3 de 4 criterios MAS ERITEMA. 2) MIOSITIS: 4 criterios SIN ERITEMA.
• 99. Cuales son los datos de laboratorio de miositis y dermatomiositis?
R = DHL Y CPK ELEVADA, AC ANTI RO-LA, AC ANTI JO y BIOPSIA MUSCULAR CON INFILTRADO LINFOCITARIO
• 100. Cual es el manejo de la polimiositis y dermatomiositis? R = PREDNISONA, la cual puede o no combinarse con inmunosupresores.

CASO CLINICO• A 64-year-old woman presents with fatigue, and musculoskeletal
symptoms. She reports of no headache, jaw discomfort, or visual disturbance. Her physical examination is normal, and laboratory testing reveals an elevated ESR of 75 mm/h. She is started on prednisone 10 mg/day and notices a dramatic improvement in her symptoms after 1 week. Which of the following are the most typical symptoms of this disorder?
(A) heliotrope rash(B) proximal muscle weakness(C) painful peripheral neuropathies(D) stiffness and pain of proximal muscles(E) hematuria

(D) This patient has PMR. It is characterized bystiffness, aching, and pain in proximal musclegroups in the neck, shoulders, back, hips, andthighs. It is considerably more common thantemporal arteritis. Both diseases are almostexclusively seen in the over 50 age group.

CASO CLINICO• A 64-year-old man is having difficulty getting out of a chair. He has
lost 15 lb and feels tired all the time. On examination, there is a blue purple rash on his eyelids and knuckles, and muscle strength in his proximal muscles is rated 4 out of 5. His creatinine kinase (CK) level is elevated and he is started on prednisone. Which of the following is the most important in monitoring response to therapy?
(A) testing of muscle strength(B) sedimentation rates(C) urine transaminase enzymes(D) EMG(E) alkaline phosphatase

(A) The course of muscle necrosis in dermatomyositiscan be best followed by repeated CKdeterminations. Repeated muscle biopsies arerarely required. However, the goal of therapy isto increase muscle strength and function, so followingmuscle strength is the key clinical assessmentof response to therapy.

CASO CLINICO• A 63-year-old man presents with weakness and hemoptysis, but no
fever, cough, or sputum. He has a 60-pack-per-year history of smoking. The chest x-ray (CXR) reveals a lung mass with mediastinal widening. On examination, there is a blue purple discoloration of the upper eyelids and erythema on his knuckles. He has proximal muscle weakness rated 4+/5, normal reflexes, and sensation. Which of the following is the most likely diagnosis for his muscle weakness?
(A) SLE(B) scleroderma(C) dermatomyositis (DM)(D) polyarteritis(E) Weber-Christian disease

(C) This man has dermatomyositis, a paraneoplasticphenomenon of many cancers. The mostcommon tumors associated with DM have beenbronchogenic carcinomas, ovarian cancers, breastcancers, and melanoma but many others haveoccurred. The malignancy may antedate or postdatethe myositis. Older age makes malignancymore likely. The extent of the workup for malignancy,if DM is the presentation, depends onclinical circumstances, but history and physicalexamination, not x-rays, are the cornerstones ofevaluation.

SX SJOGREN• 101. Cual es el cc del síndrome de Sjogren? R = XEROSTOMIA, XEROFTALMIA Y ATROFIA PAPILAR LINGUAL. Los síntomas
aumentan con la aplicación de ANTICOLINERGICOS, ANTIDEPRESIVOS Y DIURÉTICOS.
• 102. Cuales son los datos de laboratorio de laboratorio sugerentes de Sx de Sjogren?
R = ANA 95% y ANTI RO-LA, SSA Y SSB. Prueba de SCHRIMER MENOR A 5 MM cuando lo normal es mayor a 10 después de 5 min.
• 103. Cual es el manejo del Sx de Sjogren?1) SALIVA Y LAGRIMAS ARTIFICIALES. 2) PILOCARPINA.



CASO CLINICO
• A 32-year-old woman develops symptoms secondary to a dry mouth and dry eyes. She has enlarged salivary glands. Studies forautoantibodies to Ro (SS-A) are positive. Asalivary gland biopsy reveals lymphocytic infiltration. Which of the following is the most likely diagnosis?
(A) sarcoidosis(B) primary Sjögren’s syndrome(C) human immunodeficiency virus (HIV) infection(D) lymphoma(E) amyloidosis

• (B) The sicca syndrome is a recognized feature of Sjögren’s syndrome. It can be primary or secondary to other autoimmune disorders such as RA, SLE, scleroderma, or vasculitis. Primary Sjögren’s syndrome is most common in middle-aged women; sicca symptoms can also occur as a complication of HIV infection or in sarcoidosis. Sjögren’s syndrome is more likely to have positive serology, while the serology in sarcoid or HIV is negative. Both HIV and Sjögren can have lymphocytic infiltration, but in HIV it is predominantly by CD8+ lymphocytes, whereas in Sjögren’s syndrome, the infiltration is by CD4+ lymphocytes. In sarcoidosis, biopsy reveals granulomas.
RABDOMIOLISIS
• 104. En que consiste la rabdomiolisis?R = Consiste en la NECROSIS de musculo esquelético,
relacionado comúnmente a traumatismo.
• 105. Por que se produce IRA en rabdomiolisis?R = Daño tubular por filtración de MIOGLOBINA
• 106. Cual es el manejo de la rabdomiolisis?R = AUMENTO DE LIQUIDOS de 4-6 litros y vigilar función
renal.
POLIARTERITIS NODOSA• 107. Cuales son los signos y síntomas de poliarteritis nodosa? R = DOLOR EN EXTREMIDAD POR ARTRALGIA, MIALGIA QUE AFECTA PANTORRILLAS, puede
afectar riñón causando HAS, IRA O HEMORRAGIA POR MICROANEURISMAS. MONONEURITIS MÚLTIPLE (PIE CAÍDO), corazón con IAM. Livides reticular, nódulos subcutáneos, y ulceras en piel. Son necesarios 3 de 10 criterios para su diagnostico.
• 108. Cuales son las pruebas de laboratorio en la poliarteritis nodosa y con que otro virus se relaciona habitualmente?
R = DESCARTAR VHB QUE SE ASOCIA EN 20-30%. ANCA (-) Y ANA (-) .Anemia, leucocitosis y trombocitosis. Se confirma diagnostico con toma de BIOPSIA DE LA LESIÓN.
• 109. Que datos se obtienen al tomar la biopsia en la poliarteritis nodosa? R = BIOPSIA DE ARTERIA de mediano o pequeño calibre con PRESENCIA DE INFILTRADO
GRANULOCITICO, PMN Y CÉLULAS MONONUCLEARES EN LA PARED DEL VASO.
• 110. Cual es el manejo de la poliarteritis nodosa? R = ESTEROIDES, pero SI SE ASOCIA CON VHB SE AGREGAN RETROVIRALES.


CASO CLINICO• A 39-year-old man has had several weeks of fever, abdominal pain,
weight loss, and lack of energy. Three days prior to assessment, he developed a left foot drop. Physical examination confirms left peroneal nerve damage and a bilateral sensory peripheral neuropathy in both legs. Laboratory evaluation reveals ESR of 105 mm/h, WBC of 14,000/mL, and a negative serologic test for ANCA. The eosinophil count is normal. Which of the following is a reasonable method of establishing a diagnosis?
(A) testicular biopsy(B) skin biopsy(C) spiral computerized tomography (CT) of chest(D) further serologic testing(E) abdominal angiography

(E) This patient likely has PAN. ANCA andother serology are usually negative in PAN;positive serology suggests another diagnosis.The optimal diagnostic strategy is the biopsy of an
affected organ. However angiography tolook for aneurysms of small- and medium sizedarteries generally has higher yield thanblind biopsy of unaffected organs. The lungsare not a characteristic site of involvement.

CASO CLINICO• A 45-year-old man has had several weeks of fever, abdominal pain, weight
loss, and lack of energy. Three days prior to assessment, he developed a left foot drop. His blood pressure is 160/90 mm Hg, pulse 80/min, and physical examination confirms left peroneal nerve damage and a bilateral sensory peripheral neuropathy in both legs. There are no skin rashes. Laboratory evaluation reveals ESR of 105 mm/h, WBC of 14,000/mL, and negative serologic tests for ANCA and ANA. Eosinophil count is normal. Which of the following chronic viral infections is sometimes associated with this?
(A) high cytomegalovirus (CMV) titers(B) herpesvirus material in circulating immune complexes(C) hepatitis B material in circulating immune complexes(D) epidemiologic relationship to Coxsackie B virus(E) triggering of symptoms following viral gastroenteritis secondary to
rotavirus infection

(C) About 20–30% of patients with PAN havehepatitis B antigenemia. Circulating immunecomplexes containing hepatitis B antigen andimmunoglobulin have been detected, andimmunofluorescence of blood vessel wallshave also demonstrated hepatitis B antigen.Antiviral therapy has been used in these cases.

CASO CLINICO• A 42-year-old woman has had several weeks of fever, abdominal pain, weight loss,
and lack of energy. Three days prior to assessment, she developed a left foot drop and rash on her legs. Her blood pressure is 160/90 mm Hg, pulse 80/min, and physical examination confirms left peroneal nerve damage and a bilateral sensory peripheral neuropathy in both legs. The rash looks like livedo reticularis. Laboratory evaluation reveals ESR of 105 mm/h, WBC of 14,000/mL, and negative serologic tests for ANCA and ANA. Eosinophil count is normal, and urinalysis is negative for casts, protein, and red cells. Biopsy of the skin rash shows inflammation of the small blood vessels. Which of the following is the most appropriate next step in management?
(A) plasmapheresis(B) steroid therapy alone(C) combination therapy with steroids and cyclophosphamide(D) cyclophosphamide therapy alone(E) combination therapy with steroids and methotrexate

(C) Current treatment for polyarteritis nodosa(PAN) mimics that of Wegener’s granulomatosisin the initial treatment with combinationsteroid and cyclophosphamide therapy. Thiswill result in up to a 90% long-term remissionrate even after discontinuation of therapy. Incases associated with hepatitis B infection,plasmapheresis is sometimes used as initialtherapy.

CASO CLINICO• A 55-year-old woman has had several weeks of fever, abdominal pain, weight
loss, and lack of energy. Three days prior to the assessment, she developed a left foot drop. Her blood pressure is 160/90 mm Hg, pulse 80/min, and physical examination confirms left peroneal nerve damage and a bilateral sensory peripheral neuropathy in both legs. There are no skin rashes. Laboratory evaluation reveals ESR of 105 mm/h, WBC of 14,000/mL, and negative serologic tests for antineutrophil cytoplasmic antibody (ANCA) and ANA. The eosinophil count is normal, and urinalysis is negative for casts, protein, and red cells. Which of the following is the most likely mechanism for renal injury in this condition?
(A) nephrotic syndrome(B) diffuse glomerulonephritis(C) granuloma formation(D) necrotizing vasculitis of vessels(E) exclusively small vessel involvement

(D) This patient has polyarteritis nodosa (PAN)and in classic PAN, unlike microscopicpolyangiitis, both small and medium vesselsare involved. The renal lesions are ischemicsecondary to fibrinoid necrosis of the vessels. Inmicroscopic polyangiitis, a diffuse glomerulonephritisis frequently present. The mostcommon organ systems involved are the kidneys,musculoskeletal system, and peripheralnervous system.
POLIMIALGIA REUMATICA/ ARTERITIS DE CELULAS GIGANTES
• 111. Cual es la diferencia entre polimialgia reumática y arteritis de células gigantes?
R = LA POLIMIALGIA REUMÁTICA SOLA NO PRODUCE CEGUERA y responde a la terapéutico
con prednisona y la ARTERITIS DE CÉLULAS GIGANTES OCASIONA CEGUERA y necesita mayores dosis de prednisona.
• 112. Cuales son los datos clínicos de polimialgia reumática? R = DOLOR Y RIGIDEZ DE HOMBRO y región de la cintura acompañado de fiebre y
disminución de peso.
• 113. Cuales son los datos clínicos de arteritis de células gigantes? R = Cefalea, SENSIBILIDAD DE CUERO CABELLUDO, síntomas visuales, CLAUDICACIÓN
MANDIBULAR.
• 114. Cuales son los datos de la biopsia y USG en ACG de la arteria temporal? R = INFILTRADO en túnica ½ y adventicia con linfocitos y células plasmáticas. USG CON SIGNO
DEL HALO con sensibilidad 62% y especificidad 82%
• 115. Que dato se encuentra en la biopsia de la arteria temporal en ACG?
R = Fragmentación de la lamina elástica e infiltrado por linfocitos y macrófagos, células gigantes en la lamina elástica interna.
• 116. Cual es el manejo de la polimialgia reumática? R = PREDNISONA POR 1ª
• 117. Cual es el manejo de la ACG? R = PREDNISONA Y PREVENCIÓN DE CEGUERA
PERMANENTE

CASO CLINICO• A 74-year-old man presents with a history of increasing frequency of
headaches, fatigue, and weight loss for 3 months. He has had migraine headaches in the past, but these are differentfrom them. He is also experiencing back, shoulder, and hip discomfort, which is worse in the morning. His head and neck examination is normal. Range of motion in the shoulders and hips is reduced because of discomfort but there is no active inflammation. Which of the following signs or symptoms is most helpful in the diagnosis?
(A) throat pain on swallowing(B) pain in the jaw when chewing(C) malaise(D) fatigue(E) sweating

(B) Although malaise, fatigue, and sweatingare common in temporal arteritis, they are toononspecific to help in making the diagnosis.Claudication of the jaw and tongue, while notvery sensitive for temporal arteritis, are morespecific than the constitutional symptoms.Odynophagia is not a characteristic of this
disease.

CASO CLINICO• A 69-year-old man comes to the office complaining of fatigue, and weight loss for 3
months. He also reports having frequent headaches, which are new for him. There are no other constitutional symptoms of fever, chills or night sweats. He does have chronic lower back pain but lately he has noticed pain in his shoulder, and hip as well. The muscle and joint symptoms are worse in the morning, and the stiffness lasts for 1 hour. His jaw also hurts when he is chewing food. Head and neck examination is normal, there is no lymphadenopathy and fundoscopy is normal. Range of motion in theshoulders and hips is reduced because of discomfort but there is no active inflammation. Which of the following is the most feared complication in patients with this condition?
(A) blindness(B) cortical stroke(C) limb claudication(D) renal infarction(E) aortic aneurysm

(A) Although all these complications have beenreported in giant cell arteritis, the only one witha significant likelihood is blindness secondaryto ischemic optic neuropathy. Thus, if the diseaseis suspected, urgent diagnosis and treatmentis required.

CASO CLINICO• A 67-year-old man complains of frequent headaches that are new for him.
They are usually not very severe, and relieved with acetaminophen. He also has some back, shoulder, and hip discomfort, which is worse in themorning as well he feels quite fatigued and does not have his usual energy level. On examination, his neck is supple to flexion, fundi and thyroid examination are normal. Range of motion in the shoulders and hips is reduced because of discomfort but there is no active inflammation. There are no focal deficits on screening neurologic examination. Which of the following is the most appropriate initial diagnostic test?
(A) immunoelectrophoresis(B) c-ANCA levels(C) ESR(D) creatine phosphokinase (CPK)(E) hemoglobin and red cell indices

(C) Almost all patients with temporal arteritiswill have an elevated ESR. Although a high ESR cannot
make the diagnosis, a normal ESRhelps in excluding the diagnosis. C-ANCA is adiagnostic tool for Wegener’s granulomatosis.Elevated CPK is not seen in temporal arteritis,even with associated PMR. Normochromic, orslightly hypochromic, anemia often seen intemporal arteritis is too nonspecific to be ofmuch diagnostic help.

CASO CLINICO• A 57-year-old woman is complaining of frequent headaches and scalp
tenderness. She also has arthralgias, fatigue, and discomfort in her jaw when she chews. On examination, her head and neck is normal, but the right temporal artery is tender on palpation. Her erythrocyte sedimentation rate (ESR) is 50 mm/h and hemoglobin 10.5 g/dL. Atemporal artery biopsy is obtained for diagnostic confirmation. Which of the following is the most appropriate next step in management?
(A) intravenous high-dose steroids(B) acetylsalicylic acid(C) indomethacin(D) low-dose (prednisone 40 mg/day) steroids by mouth(E) topical steroid creams

• (D) The response of pain, stiffness, and headaches to 40–60 mg of prednisone is dramatic in giant cell arteritis. The duration of treatment is not known but most patients require treatment for more than 2 years. ESR is used to monitor response to therapy. Patients need treatment and evaluation for the complications of long-term steroid use such as osteoporosis and diabetes.

CASO CLINICO
• A 75-year-old woman has abrupt onset of soreness, and severe stiffness of the shoulders and upper thighs with low grade fever. Physical examination is entirely normal, but ESR is over 100 mm/h. Which of the following is the most likely diagnosis?
(A) dermatomyositis (DM)(B) osteoarthritis(C) polymyalgia rheumatica (PMR)(D) midline granuloma(E) sarcoidosis

• (C) This patient has PMR. Proximal arm and hipmuscle/joint discomfort is the hallmark of thisdisorder. Difficulty in getting out of bed or risingfrom a chair may suggest polymyositis, but themuscles are normal when muscle strength isassessed. In general, PMR causes painful muscles,not weak muscles. However, pain may leadto profound disuse atrophy and apparent muscleweakness. In these cases, normal CK and nonspecificmuscle biopsy still allow accurate differentiationfrom polymyositis.

CASO CLINICO• A71-year-old woman comes to the office with a history of headaches, fatigue,
and weight loss for 3 months. The headaches are new for her, and usually not very severe. Her jaw also hurts when she is chewing food. Two days prior, she had briefly lost partial vision in her left eye. There were no other neurologic symptoms at the time. On examination, her neck is supple to flexion, fundi and neurologic examinations are normal. She is started on prednisone 60 mg/day and a biopsy is performed to confirm the diagnosis. Which of the following is the most likely change seen on the biopsy to confirm the diagnosis?
(A) immune complex deposition(B) arteritis with giant cells(C) lymphocytic infiltration(D) type II muscle fiber atrophy(E) polyphasic potentials on electromyography (EMG)

(B) Temporal artery biopsy is required fordefinitive diagnosis of giant cell arteritis,because of the relatively nonspecific nature ofthe presenting symptoms, signs, and routinelaboratory tests. The arteritis can be segmental,however, and great care must be taken in thepathologic assessment.

GRANULOMATOSIS DE WEGENER• 118. Cuales son las vasculitis asociadas a ANCA?
R = Granulomatosis de WEGENER, SX DE CHURG-STRAUSS y POLIANGEITIS
MICROSCÓPICA. • 119. En que consiste la granulomatosis de Wegener? R = VASCULITIS de arterias pequeñas, LESIONES GRANULOMATOSAS NECROSANTES de VÍAS AÉREAS
SUPERIORES E INFERIORES Y GLOMERULONEFRITIS. Se sospecha en personas con AFECCIONES RESPIRATORIAS RECURRENTES.
• 120. Cuales son los datos clínicos de la granulomatosis de Wegener? R = RINITIS crónica o SINUSITIS CRÓNICA. PULMONAR: 96% con ESPUTO SANGUINOLENTO, dolor
torácico y disnea. SÍNTOMAS DE VÍAS AÉREAS SUPERIORES E INFERIORES CON REBELDÍA AL TRATAMIENTO 90%. Afección RENAL: con GLOMERULOESCLEROSIS FOCAL Y SEGMENTARIA que puede evolucionar a IR rápidamente progresiva.
• 121. Cuales son los datos de gabinete de la granulomatosis de Wegener? R = ANCAc. ANCAp .Biopsia renal con GLOMERULONEFRITIS FOCAL Y SEGMENTARIA NECROSANTE.
TAC de tórax con infiltrados, nódulos, granulomas y calcificaciones. Histologicamente vasculitis, inflamación granulomatosa, necrosis.
• 122. Cual es el manejo de granulomatosis de Wegener? R = CICLOFOSFAMIDA, prednisona, metotrexate.

CASO CLINICOA 28-year-old woman presents with a recent
episode of coughing up some blood, frequentnosebleeds, and now decreased urine output.A nasal mucosa ulcer was seen on inspection.Her urinalysis is positive for protein and redcells consistent with a GN. The CXR shows
two cavitary lesions and her serology is positivefor antineutrophil cytoplasmic antibodies
(ANCA). Which of the following is the mostlikely diagnosis?
(A) Wegener’s granulomatosis(B) bacterial endocarditis
(C) Goodpasture’s syndrome(D) lupus erythematosus
(E) poststreptococcal disease

(A) Numerous diseases are associated withrenal and pulmonary manifestations, includinglupus, Goodpasture’s syndrome, andWegener’s granulomatosis. Wegener’s is typicallyassociated with antineutrophil cytoplasmicantibodies. (Kasper, p. 2005)
SX DE CHURG STRAUSS• 123. Como se define el síndrome de Churg-Strauss?
R = Como una VASCULITIS necrosante sistémica y tiene una gran ASOCIACIÓN CON ASMA 98-100%
• 124. Cual es el cc del síndrome de Churg-Strauss? FASE I: ASMA o RINITIS alérgica con meses o años de duración. FASE II: INFILTRACIÓN TISULAR EOSINOFILICA con cuenta arriba de 1000 por ml. FASE III: Vasculitis sistémica que afecta corazón, pulmones, piel, nervios periféricos
• 125. Cuales son los datos de gabinete y biopsia en el síndrome de Churg-Strauss? R = ANCAp Y EOSINOFILIA. Biopsia con GRANULOMA EOSINOFILO extravascular con zona de
necrosis central rodeada de infiltrado celular mixto.
• 126. Cual es el manejo del síndrome de Churg-Strauss? R = El tratamiento para el síndrome de Churg-Strauss incluye GLUCOCORTICOIDES como la
prednisolona y otras drogas inmunosupresoras como la azatioprina y ciclofosfamida. La enfermedad es crónica y de por vida.

POLIANGEITIS MICROSCOPICA• 127. Cuales son los datos clínicos de la poliangeitis microscópica?
R = RIÑÓN con GLOMERULONEFRITIS de rápida progresión y PULMÓN con
HEMORRAGIA difusa.
• 128. Que se observa en la biopsia renal en un paciente con poliangeitis microscópica?
R = Demuestra GLOMERULONEFRITIS NECROSANTE FOCAL Y SEGMENTARIA pauciinmune,
con PROLIFERACIÓN CAPILAR EN FORMA DE MEDIAS LUNAS.
• 129. Que datos radiológicos y sintomáticos tiene un paciente a nivel pulmonar en un paciente con poliangeitis microscópica?
R = La HEMORRAGIA PULMONAR se documenta al observar un infiltrado o sombras alveolares en un paciente con HEMOPTISIS, disnea (hipoxemia) y anemia en ausencia de edema pulmonar o infección.
• 130. Cual es el diagnostico diferencial en un paciente con poliangeitis microscópica? R = SX DE GOODPASTURE que también presenta un síndrome pulmón-riñón pero NO PRESENTA
VASCULITIS NI AFECCIÓN MULTISISTEMICA.
• 131 Cual es el manejo de la poliangeitis microscópica? R = GLUCOCORTICOIDES Y CICLOFOSFAMIDA. Sin tratamiento la mortalidad a 5 años es del 85%.


PURPURA DE HENOCH SCHONLEIN• 132. En que consiste la purpura de Henoch Schonlein? R = Vasculitis sistémica de pequeño calibre mas común en niños
• 133. Cuales son los rasgos típicos de la purpura de Henoch Schonlein?1) ANTECEDENTE DE ENFERMEDAD VIRAL.
2) TRIADA CLÁSICA DE PURPURA, DOLOR ABDOMINAL TIPO CÓLICO Y
ARTRITIS. 3) Purpura palpable NO TROMBOPENICA en región glútea y miembros pelvicos, dolor
abdominal, artritis, hematuria. 4) Lesiones en la piel de forma clásica en extremidades inferiores pero pueden
manifestarse en cualquier zona. 5) GI: Dolor tipo cólico, nausea y vomito. 6) RENAL: Glomerulonefritis o síndrome nefrótico.
• 134. Cuales son lo hallazgos patológicos en la biopsia y gabinete de la purpura de Henoch Schonlein?
R = Depósitos de IgA EN BIOPSIA y análisis sanguíneo SIN TROMBOPENIA ni alteración de la coagulación.


SÍNDROME DE BECHET• 135. Que caracteriza al síndrome de Bechet? 1) ULCERA ORAL, ENCIA Y LABIOS: Ulcera dolorosa redonda (aftosa), borde
eritematoso y cubierta por pseudomembrana amarillento. 2) ULCERAS GENITALES: Pene, escroto o vulva similares a las orales. 3) OFTALMICAS: Hipopion, epiescleritis, vasculitis retineana e UVEÍTIS con dolor,
ojo rojo y visión borrosa.
• 136. Que pruebas diagnostica existe para el diagnostico de síndrome de Bechet? R = PATERGIA + que consiste en puncionar con una aguja estéril el antebrazo del
paciente y si aparece un nódulo eritematoso aséptico o una pústula mayor a 2 mm es positivo.
• 137. Cual es el manejo del síndrome de Bechet?1) GLUCOCORTICOIDES.
2) TALIDOMIDA para ULCERAS ORAL Y VAGINAL

ARTERITIS DE TAKAYASU• 138. Que tipo de alteración es la arteritis de Takayasu? R = Es una vasculitis que afecta a la aorta y sus ramas así como a las arterias pulmonares
produciendo síntomas isquémicos principalmente.
• 139. Cuales son los datos clínicos de la arteritis de Takayasu?
1) SISTEMICOS: FIEBRE, pérdida de peso, astenia, artralgias. 2) Manifestaciones isquémicas como frialdad de una o mas extremidades, cefalea, amaurosis,
diplopía y la PRESIÓN EN AMBOS BRAZOS DIFIERE 10 MM/HG.
• 140. Cuales son los datos de laboratorio y gabinete principales en la arteritis de Takayasu?
1) LABORATORIO: VSG AUMENTADA, trombocitosis, ANEMIA NORMO-NORMO.2) ANGIOGRAFIA: estrechamientos con adelgazamientos progresivos, oclusiones y aneurismas.
• 141. Cual es el manejo de la arteritis de Takayasu?
1) PREDNISONA2) ANGIOPLASTIA

CASO CLINICO• A 24-year-old woman notices pain in her left arm, made worse with use.
She also has fatigue, fever, night sweats, and arthralgias. On examination, there are no palpable lymph nodes, and the joints and muscle strength are normal. The left radial pulse is absent, and there is a bruit over the left subclavian and common carotid arteries. Preliminary laboratory investigations reveal an elevated ESR and mild anemia. Which of the following vascular findings is most likely to be found in her?
(A) high pressure in the legs and low pressure in the arms(B) low pressure in the legs and high pressure in the arms(C) high-pitched diastolic murmur(D) a relentless course to death(E) hypotension

(A) High pressure in the legs and low pressurein the arms characterize Takayasu’s syndrome.Clinical manifestations include easy fatigabilityof the arms and atrophy of the soft tissues of theface. The course is variable, and spontaneousremissions can occur. The disease predominantlyaffects young women.
ENFERMEDAD DE KAWASAKY
• 142. Cual es el cc de la enfermedad de Kawasaky?R = Enfermedad FEBRIL generalmente EN <5ª y se
caracteriza por eritema en mucosa oral, EROSIONES EN LOS LABIOS, LENGUA EN FRESA, vasculitis coronaria.
• 143. Cual es el manejo de la enfermedad de Kawasaky?
R = GAMAGLOBULINA IV + ASA por 14 días.


OSTEOMIELITIS TB O MAL DE POTT• 145. En un paciente con ANEMIA DE CÉLULAS FALCIFORMES, que agente causal es mas
común de provocar osteomielitis? R = Salmonella
• 146. Cual es el tratamiento de elección para todas las lesiones óseas causadas por coccidioides inmitis?
R = ITRACONAZOL
• 147. Cual es el cc de la osteomielitis tuberculosa? R = DOLOR DORSAL Y LUMBAR con dificultad para sentarse, ponerse de pie o flexionar el
cuerpo, con dolor a la palpación y contracción muscular protectora, se aprecia malestar general crónico y manifestaciones pulmonares de tb.
• 148. Cuales son los hallazgos radiológicos de la osteomielitis tuberculosa o mal de Pott? R = LESIONES OSTEOLITICAS EN LA COLUMNA, ASÍ COMO PERDIDA DE LA ALTURA DEL
ESPACIO INTERVERTEBRAL.

• 149. Cual es la complicación mas grave de la osteomielitis tb en la columna vertebral (espondilitis tuberculosa o enfermedad de Pott)?
R = Paraplejia
• 150. Cual es el régimen de tx en la osteomielitis tuberculosa? R = I, R Y P durante 6 MESES
• 151. Cual es el cc de la artritis tuberculosa?• R = La artritis periférica se manifiesta como MONOARTRITIS EN MAS DEL
90% de los casos, siendo las ARTICULACIONES GRANDES COMO LA RODILLA O LA CADERA LAS MAS AFECTADAS. El dolor o limitación funcional son síntomas tardíos.
• 152. Cual es la triada clásica de Phemister radiológico en la osteomelitis tuberculosa o mal de Pott?
• R = OSTEOPENIA PERIARTICULAR, EROSIONES ARTICULARES PERIFÉRICAS Y DISMINUCIÓN GRADUAL DEL ESPACIO ARTICULAR. El diagnostico definitivo se realiza mediante la biopsia de tejido sinovial, con cultivos y tinciones demostrando el bacilo.

OSTEOSARCOMA• 153. Cuales son los tumores benignos de los huesos y cual es su tratamiento de elección? R = OSTEOMAS OSTEOIDES y el tratamiento de elección es la FOTOCOAGULACIÓN CON LASER
• 154. Que es una atropatia neurogena o articulación de Charcot? R = Consiste en la DESTRUCCIÓN ARTICULAR resultante de la PERDIDA o disminución en la
PROPIOSEPCION DEL DOLOR Y TEMPERATURA. LA INYECCIÓN INTRARTICULAR DE HIDROCORTISONA PUEDE OCASIONARLO
• 155. Que lugar ocupa en frecuencia el osteosarcoma? R = 2do lugar después del mieloma y es maligno, ataca principalmente a niños, adolescentes y adultos
jóvenes CRECIENDO GENERALMENTE EN ZONAS DE DESARROLLO EPIFISIARIO.
• 156. Cual es el cc del osteosarcoma? R = Es una neoplasia que crece con rapidez y altamente destructiva metastatiza al pulmón
rápidamente. El síntoma principal es el DOLOR con afección articular, AUMENTO DE LA TEMPERATURA LOCAL.
• 157. Cuales son los hallazgos de gabinete en el osteosarcoma? R = La FA esta aumentada. La RM es de elección. En la radiografía simple presenta una IMAGEN EN
¨SOL NACIENTE¨.
• 158. Cual es el manejo del osteosarcoma? R = QUIMIOTERAPIA neoadyuvante mas RESECCIÓN con supervivencia de un 90%

TUMOR DE EWING• 159. Donde se localiza frecuentemente el tumor de Ewing?1) El sarcoma de Ewing es una neoplasia maligna de crecimiento rápido, que NACE DE
LAS CÉLULAS PRIMITIVAS DE LA MEDULA ÓSEA, normalmente en la cavidad medular de HUESOS LARGOS.
2) Inicia creciendo en el interior de la cavidad medular, perforando el hueso cortical de la diáfisis y elevando el periostio que da el signo RADIOGRÁFICO EN CAPAS DE CEBOLLA.
• 160. Cual es el cc del tumor de Ewing? R = DOLOR, SENSIBILIDAD LOCAL, manifestaciones sistémicas. DEBIDO AL CENTRO
NECRÓTICO HAY FEBRÍCULA, LEUCOCITOSIS y elevación de la VSG.
• 161. Cual es el pronóstico del tumor de Ewing?1) MALO CON UNA MORTALIDAD DEL 95% pese al tratamiento debido a METÁSTASIS
PULMONARES. 2) El tratamiento temprano reduce la mortalidad a 50% y se hace con quimio y
radioterapia.

OSTEOMIELITIS AGUDA• 162. Cual es el microorganismo mas frecuente de la osteomielitis aguda?1) STAPHYLOCOCCUS AUREUS, la puerta de entrada suele ser la piel a través de erosiones,
abrasiones, pústulas o quemaduras. 2) En LACTANTES los agentes mas frecuentes son los ESTREPTOCOCOS (NEUMOCOCO) O
HAEMOPHILUS INLUENZAE.
• 163. Cual es el cc característico de la osteomielitis aguda? R = Existe el ANTECEDENTE DE TRAUMA O INFECCIÓN recurrente de VÍAS RESPIRATORIAS O PIEL. El
primer síntoma es el dolor, acompañado de anorexia y FIEBRE. La TUMEFACCIÓN de partes blandas es un signo tardío.
• 164. Que estudios de gabinete son útiles para el diagnostico de osteomielitis aguda? R = La radiografía demuestran cambios solo en etapas tardías, pero el CAMBIO MAS PRECOZ DE
ESTA ES UNA REACCIÓN PERIOSTICA. LA RESONANCIA Y LA GAMAGRAFIA SON MAS ESPECIFICAS DE MANERA TEMPRANA.
• 165. Cual es el estándar de oro para el dx de osteomielitis aguda? R = LA BIOPSIA DE HUESO, a la que se le realiza CULTIVO CON ANTIBIOGRAMA.
• 166. Cual es el manejo de la osteomielitis aguda? R = Manejo empírico con PENICILINA G Y CLINDAMICINA DE 4-6 SEMANAS y ESCARIFICACIÓN para
aumentar el flujo sanguíneo y promover la formación de vasos nuevos en el hueso.

OSTEOMIELITIS CRONICA• 167. Cual es el cc de la osteomielitis crónica? R = EL paciente PERSISTE CON UNA LESIÓN RESIDUAL DOLOROSA
después de la resolución de la fase aguda, acompañada de tumefacción, dolor a la palpación e impotencia.
• 168. Cuales son los hallazgos de gabinete en la osteomielitis crónica? R = Se encuentra un SECUESTRO CLARO EN EL HUESO QUE SE
OBSERVAN COMO CAVIDADES RADIOLUCIDAS CON TEJIDO DE GRANULACIÓN EN SU INTERIOR, con aumento de volumen de tejidos blandos y posteriormente OSTEOPENIA y LISIS ÓSEA POR DESTRUCCIÓN TRABECULAR.
• 169. Cual es el manejo de la ostemielitis crónica? R = RETIRAR TODO EL HUESO NECRÓTICO, y antibióticos partiendo de
los resultados de la biopsia de hueso.

ARTRITIS SEPTICA PIOGENA• 171. Cuales son los factores de riesgo para la artritis séptica piógena (gonocócica o no)? R = Abuso de drogas IV, jóvenes sexualmente activos, enfermedades concomitante como DM, AR o lupus,
antecedentes de cirugía o prótesis.
• 172. Cual es el cc de la artritis séptica piógena gonocócica o no? R = Es una entidad de inicio agudo y progresivo caracterizado por dolor e inflamación local (salvo en el primer año
de vida donde es similar a la sepsis). El dolor es moderado a intenso con limitación funcional, aumento de la temperatura local y rubor es monoarticular, cuando es poliarticular es en paciente inmunocomprometido siendo la rodilla la mas afectada.
• 173. Cuales son los hallazgos radiológicos en la artritis séptica piógena? R = Edema de tejidos blandos y derrame articular. EN AFECCIÓN POR ANAEROBIOS SE VE GAS EN TEJIDOS BLANDOS.
El gamagrama óseo con tecnecio (valora flujo) o con galio (valora actividad inflamatoria) pueden utilizarse de manera temprana.
• 174. Cual es el manejo de la artritis séptica piógena?1) Consiste en la administración de antibióticos y drenaje de la articulación afectada. En caso de ARTRITIS PIÓGENA
debe administrarse de 3 A 4 SEMANAS y en caso de ARTRITIS GONOCÓCICA DE 7 A 14 DÍAS.2) En menores de 2M: DICLOXACILINA mas CEFOTAXIMA3) En LACTANTES: DICLOXACILINA mas CEFOTAXIMA4) En niños MAYORES DE 3ª: DICLOXACILINA5) Artritis séptica GONOCÓCICA: 1g por via IM o IV cada 24 hrs.6) Artritis séptica en DROGADICTOS por via IV: DICLOXACILINA mas GENTAMICINA7) Artritis séptica en INMUNOCOMPROMETIDOS: CEFTAZIDIMA mas AMIKACINA8) Artritis séptica POSTOPERATORIA: VANCOMICINA mas AMIKACINA9) Artitis séptica en FRACTURA ABIERTA: AMOXICILINA con ACIDO CLAVULANICA


RESUMEN DE LAS ENFERMEDADES METABOLICAS OSEAS
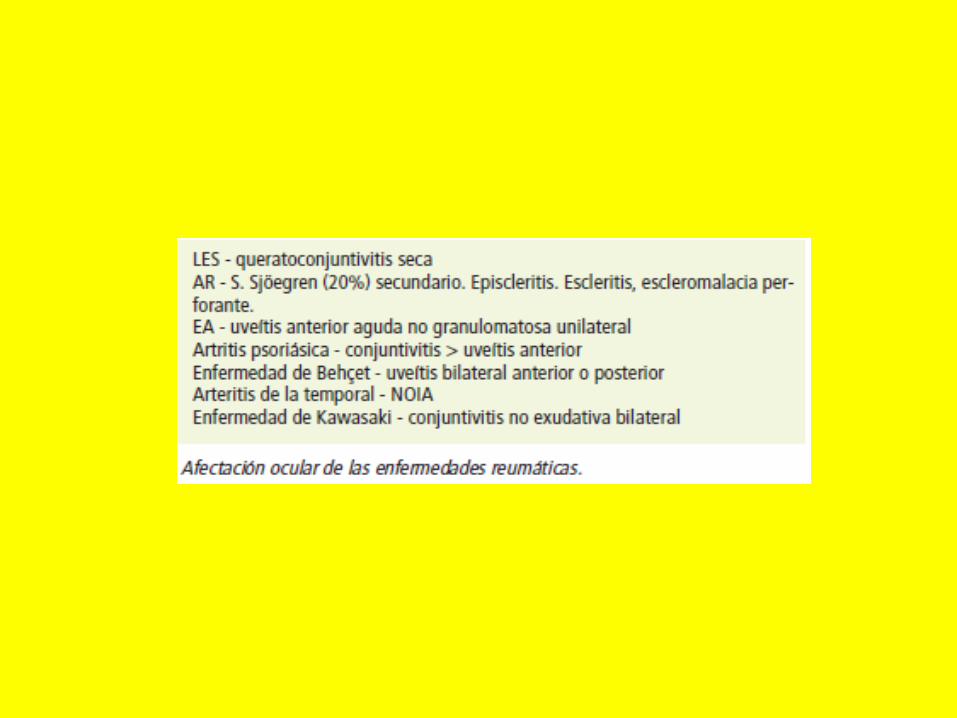

ENFERMEDAD DE PAGET• Figure shows an x-ray of a 40-year-oldCaucasian man with symptoms of sinusitis andan incidental finding in the skull. Which of thefollowing is the most likely diagnosis?
(A) normal variant(B) osteomyelitis(C) Paget’s disease(D) hemangioma(E) metastatic disease

• (C) This is a rarefied area involving the frontal and parietal bones, and it is an early stage of Paget’s disease in which calvarial thickening and foci or radiopacity are not present within the radiolucent area. At this stage of the disease, a cross-section through the margin of the lesion reveals a compact inner and outer table in the normal portion, whereas the diploe widens and extends to the outer and inner surfaces of the calvarium without a change in the calvarial thickness in the lesion.
• El tratamiento incluye AINES, bifosfonatos y calcitonina.

CPK
• Las siguientes patologías cursan con aumento de la CPK
1) HIPOTIROIDISMO2) RAZA NEGRA3) POLIMIOSITIS Y4) DERMATOMIOSITIS

Consejos
1. Leer diariamente y en bloques
2. Adiós Partys un tiempo
3. Has ejercicio y come bien durante el estudio
4. Toma algún curso bueno si tienes la posibilidad
5. Ten Fe.

BIBLIOGRAFIA
• EXARMED• PAPADAKIS• CTO• HARRISON• AMIR• USMLE STEPS



![Clínica Universitária de Reumatologia – Faculdade de ...§ões_Reumatologia_CHUC... · Apr 30. [Epub ahead of print] • Pigmented Villonodular Synovitis: a recurrent case with](https://img.pdfslide.us/doc/110x75/5c65198c09d3f2916e8c4235/clinica-universitaria-de-reumatologia-faculdade-de-oesreumatologiachuc.jpg)























![Manual de Reumatologia Cajigas[Librosmedicospdf.net].pdf](https://img.pdfslide.us/doc/110x75/577c78591a28abe0548fb3fe/manual-de-reumatologia-cajigaslibrosmedicospdfnetpdf.jpg)

