Embed Size (px)
Citation preview

Urine Formation by the Kidneys : TubularReabsorption and Secretion

Tubular reabsorption is quantitatively large and highly selective
Tubular reabsorption includes passive and active mechanisms

Na+ REABSORPTION
Normally about 60% of the filtered Na+ is reabsorbed in the proximal tubule, primarily by Na–H exchange.
Another 30% is absorbed via the Na–2Cl–K cotransporter in the thick ascending limb of the loop of Henle.
In both of these segments of the nephron, passive paracellular movement of Na+ also contributes to overall Na+ reabsorption.
In the distal convoluted tubule 7% of the filtered Na+ is absorbed by the Na–Cl cotransporter.
The remainder of the filtered Na+, about 3%, is absorbed via ENaC channels in the collecting ducts


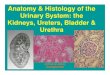
Transport proteins involved in the movement of Na+ across the apical membranes of renal tubular cells

GLUCOSE REABSORPTION
Glucose, amino acids, and bicarbonate are reabsorbed along with Na+ in the early portion of the proximal tubule
It is filtered at a rate of approximately 100 mg/min (80 mg/dL of plasma × 125mL/min)
The amount reabsorbed is proportional to the amount filtered
Essentially all of the glucose is reabsorbed, and no more than a few milligrams appear in the urine per 24 h
The transport maximum (TmG) is about 375 mg/min in men and 300 mg/min in women

the actual renal threshold is about 200 mg/dL of arterial plasma, which corresponds to a venous level of about 180 mg/dL

The transport maximum is the maximum rate at which glucose can be reabsorbed from the tubules.
The threshold for glucose refers to the filtered load of glucose at which glucose first begins to be excreted in the urine

Sodium glucose co transporters (SGLT2 and SGLT1) are located on the brush border of proximal tubular cells and carry glucose into the cell cytoplasm against a concentration gradient
Approximately 90 percent of the filtered glucose is reabsorbed by SGLT2 in the early part of the PCT (S1 segment) and the residual 10 percent is transported by SGLT1 in the latter segments (S3 segment) of the PCT
On the basolateral side of the membrane, glucose diffuses out of the cell into the interstitial spaces with the help of glucose transporters GLUT2, in the S1 segment and GLUT1 in the S3 segment of the PCT


Reabsorption and Secretion Along Different Parts of the Nephron

PROXIMAL CONVOLUTED TUBULE
The entire proximal tubule reabsorbs 65% of the filtered Na+ and water
The tight coupling between Na+ and water reabsorption is called isosmotic reabsorption




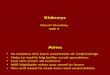
Changes in concentrations of different substances in tubular fluid along the PCT relative to the concentrations of these substances in the plasma and in the glomerular filtrate

LOOP OF
HENLE

The descending part of the thin segment is highly permeable to water and moderately permeable to most solutes, including urea and sodium.
The ascending limb, including both the thin and the thick portions, is virtually impermeable to water, a characteristic that is important for concentrating the urine.
About 20 percent of the filtered water is reabsorbed in the loop of Henle, and almost all of this occurs in the thin descending limb.
About 25 percent of the filtered loads of sodium, chloride, and potassium are reabsorbed in the loop of Henle, mostly in the thick ascending limb.

In the thick ascending loop, movement of Na+ across the luminal membrane is mediated primarily by a 1Na-2Cl-1K co transporter. Also there is a Na-H counter-transport mechanism membrane that mediates Na+ reabsorption and H+ secretion

Distal Tubule




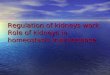
Cellular mechanism of action of antidiuretic hormone in the principal cell of the late distal tubule and collecting duct


Medullary Collecting Duct

Hormones That Regulate Tubular Reabsorption

Direct effects of angiotensin II (Ang II) to increase proximal tubular sodium reabsorption.
Ang II stimulates sodium-hydrogen exchange (NHE) on the luminal membrane and the sodium-potassium ATPase transporter as well as sodium-bicarbonate co-transport on the basolateral membrane. These same effects of Ang II likely occur in several other parts of the renal tubule, including the loop of Henle, distal tubule, and collecting tubule

Q1. approximate % of sodium absorbed in DCT is:
a) 15%b) 7%c) 3%d) Nil

Q2. in DCT sodium is reabsorbed via:
a) Na+-K+-2Cl- exchangerb) Na+-H+ cotransporterc) Both (a) and (b)d) None

Q3. considering plasma glucose level to be 150 mg/dl and GFR to be 133 ml/min, what should be the glucose filtration rate?
a) 100 mg/minb) 150 mg/minc) 200 mg/mind) 250 mg/min

Q4 . Splay is:
a) Difference between actual and observed renal threshold for glucose reabsorption
b) Difference between actual and observed transport maximum of glucose
c) Difference between transport maximum and renal threshold for glucose reabsorption
d) None

Q5. Transport maximum for glucose is around:
a) 100 mg/dlb) 180 mg/dlc) 360 mg/dld) 425 mg/dl

Q6. true about SGLT2 is:
a) Situated on brush border of PCTb) Present on segment 3 (later segment) of PCTc) Absorbs 10% of glucosed) All of the above

Q7. isosmotic reabsorbtion in PCT refers to:
a) Osmolarity remains almost constant in PCTb) Tight coupling between water and sodium reabsorbtionc) Both (a) and (b)d) None

Q8. Thin descending limb of Henle is:
a) Impermeable to waterb) Impermeable to solutesc) Moderately permeable to solutesd) None

Q9. in thick ascending loop of Henle, urine becomes:
a) Hyper osmolarb) Hypo osmolar c) Remains iso osmolard) Depends on aldosterone

Q10. Intercalated cells in DCT, are concerned with:
a) Na+ reabsorptionb) H+ reabsorptionc) HCO3
- reabsorptiond) None

Q11. effect of aldosterone on collecting duct is:
a) Increased sodium secretionb) Increased potassium secretionc) Increased water secretiond) None

Q12. true about ADH is:
a) Acts via cAMP mediated mechanismb) Increases water reabsorption in collecting duct via aquaporin 1c) Increases water reabsorption in DCT via aquaporin 1d) All of the above