Embed Size (px)
Citation preview

TERAPIA DIRIGIDA POR METAS EN CIRUGÍA MAYOR NO CARDIACA
SERGIO OCHOA CASTRILLÓNRESIDENTE DE ANESTESIOLOGÍA
TERCER AÑOTUTOR
DR JAVIER BENÍTEZ

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

CONTENIDODEFINICIÓN
CAMBIOS FISIOPATOLÓGICOS EN CIRUGÍA MAYOR
CONCEPTOS, BENEFICIOS Y RIESGOS DE LA TERAPIA DIRIGIDA POR METAS
MONITORIA IDEAL
INTERVENCIONES Y ALGORITMO
CONCLUSIONES

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012
GENERALIDADES
• Cirugía mayor: 230 millones/año• 18% complicaciones POP– Compromiso funcionalidad– Mayor mortalidad a mediano plazo
• 3 – 5% mortalidad antes del egreso• Papel terapia dirigida por metas • ¿Por qué no la usamos?
Marik P. Perioperative hemodynamic optimization: a revised approach. Journal of Clinical Anesthesia (2014)

DEFINICIÓN
• Uso apropiado fluidos, inotrópicos y vasoactivos
Intervenciones terapéuticas para lograr una meta determinada
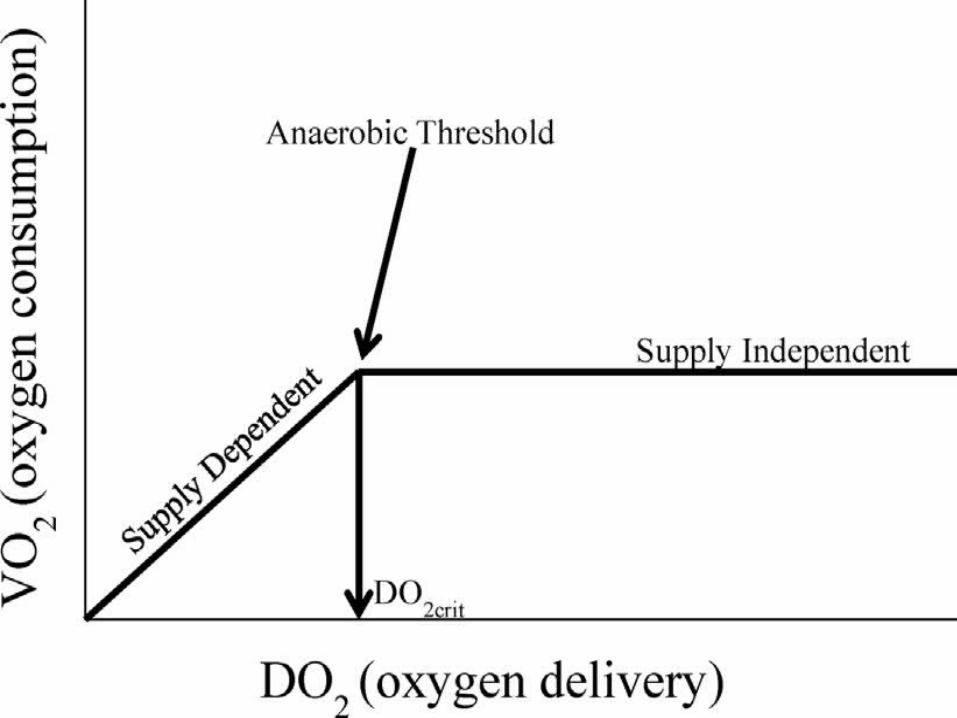
• Evitar disoxia tisular – Relación DO₂/VO₂• Garantizar perfusión orgánica durante cirugía
Satisfacer aumento en la demanda de oxígeno
• Subutilización Reducción morbimortalidad POP
Independientemente del monitor hemodinámico
utilizado Clinical review: Goal-directed therapy - what is the evidence in surgical patients? The eff ect
on diff erent risk groups. Critical Care 2013

CAMBIOS FISIOPATOLÓGICOS EN CIRUGÍA MAYOR
• Directa: acceso quirúrgico y remoción de órgano • Indirecta: pérdidas hemáticas, perfusión, técnica
anestésica
Lesión primaria
• Consecuencia• Mediada directamente: citoquinas, hormonal,
neural
Lesión secundaria
RESPUESTA AL ESTRÉS
Scott M. Pathophysiology of Major Surgery and the Role of Enhanced Recovery Pathways and the Anesthesiologist to Improve Outcomes. Anesthesiology Clin. 2015

Scott M. Pathophysiology of Major Surgery and the Role of Enhanced Recovery Pathways and the Anesthesiologist to Improve Outcomes. 2015

LESIÓN PRIMARIA INDIRECTA
• Pérdidas hemáticas – Reducción DO₂– Causa SIRS
• Hipoperfusión local– Disfunción celular secundaria – Riesgo infecciones – Compromiso anastomosis
• Papel del anestesiólogo – Tono vasomotor – Fluidoterapia Scott M. Pathophysiology of Major Surgery and the Role of Enhanced Recovery Pathways
and the Anesthesiologist to Improve Outcomes. Anesthesiology Clin. 2015
Joosten A. Defining Goals of Resuscitation in the critically I ll Patient. Crit Care Clin. 2015

Joosten A. Defining Goals of Resuscitation in the critically I ll Patient. Crit Care Clin. 2015

HIPOVOLEMIA
“Sacrificio órganos no vitales”Activación SNS y eje RAAAumento respuesta inflamatoriaConlleva a mayor dosis de vasopresores
Joosten A. Defining Goals of Resuscitation in the critically I ll Patient. Crit Care Clin. 2015

HIPERVOLEMIA
Extravasación fluidos (edema secundario)Mayor demanda miocárdicaDisminución oxigenación tisular Hemodilución (coagulopatía)Mayor mortalidad (balance positivo)
Joosten A. Defining Goals of Resuscitation in the critically I ll Patient. Crit Care Clin. 2015

ORIGEN DEUDA DE OXÍGENO
Marik P. Perioperative hemodynamic optimization: a revised approach. Journal of Clinical Anesthesia (2014)

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

HISTORIA TERAPIA DIRIGIDA POR METAS (GDT)
• Shoemaker (1988)• CAP: metas suprafisiológicas (IC ≥ 4.5
L/min/m², DO₂ ≥ 600 ml/min)• Disminución mortalidad en pacientes de alto
riesgo • Relación < IC e hipoperfusión mucosa
intestinal• Optimización volumen y uso inotrópicos
Waldron N. Perioperative Goal-DirectedTherapy. Journal of Cardiothoracic and Vascular Anesthesia. 2014
Cirugía mayor
Complicaciones POP
prevenibles
Morbimortalidad a largo
plazo
Clinical review: Goal-directed therapy - what is the evidence in surgical patients? The eff ect on diff erent risk groups. Critical Care 2013


BENEFICIOS TERAPIA DIRIGIDA POR METAS
Menor estancia hospitalaria
• Balance perfusión y edema intersticial
Menor estancia en UCI
Menores complicaciones gastrointestinales
Disminución incidencia injuria renal aguda
Mayor sobrevida a largo plazo (15 años)
Menor íleo y PONV
¿Riesgo sobrecarga hídrica y descompensación cardiaca?Waldron N. Perioperative Goal-DirectedTherapy. Journal of Cardiothoracic and Vascular
Anesthesia. 2014

• Revisión sistemática • MEDLINE – EMBASE – COCHRANE• 32 ensayos clínicos controlados • 2.808 pacientes (1.438 GDT – 1.370 controles)• 1988 – 2011
Clinical review: Goal-directed therapy - what is the evidence in surgical patients? The eff ect on diff erent risk groups. Critical Care 2013

MORTALIDADGrupo riesgo intermedio(mortalidad 0 – 4.9%)
Grupo riesgo alto(mortalidad 5 – 19.9%)
Grupo riesgo extremadamente alto(mortalidad ≥ 20%)

MORBILIDADGrupo riesgo intermedio(mortalidad 0 – 4.9%)
Grupo riesgo alto(mortalidad 5 – 19.9%)
Grupo riesgo extremadamente alto(mortalidad ≥ 20%)

RESULTADOSOptimización de metas demostró mejores desenlaces
Uso combinado de fluidos e inotrópicos fue superior
No hay duda del beneficio de la terapia dirigida por metas
Se requiere un protocolo claramente definido
¿POR QUÉ NO LA UTILIZAMOS?
Clinical review: Goal-directed therapy - what is the evidence in surgical patients? The eff ect on diff erent risk groups. Critical Care 2013

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

¿CUÁL ES LA MONITORIA IDEAL EN GDT?
• Monitor ideal • Representativo de perfusión
tisular • Disponible• Continua • Reproducible • No invasivo• Bajo costo
Waldron N. Perioperative Goal-DirectedTherapy. Journal of Cardiothoracic and Vascular Anesthesia. 2014

Frecuencia cardiaca Tensión arterial Gasto urinario
Waldron N. Perioperative Goal-DirectedTherapy. Journal of Cardiothoracic and Vascular Anesthesia. 2014
• Medidas insensibles del estado de volemia
• Monitoria indiscutible
PVCPCCP
• Utilidad limitada demostrada como medida de precarga

CATÉTER ARTERIA PULMONAR
• Gran papel histórico • Controversial• Errores en interpretación • No se ha demostrado mejoría en desenlaces
en GDT• Papel importante en poblaciones especiales:– Estado hemodinámico complejo– Pacientes ancianos
Isbell J. Impact of hemodynamic monitoring on clinical Outcomes. Best Practice & Research Clinical Anaesthesiology 2014
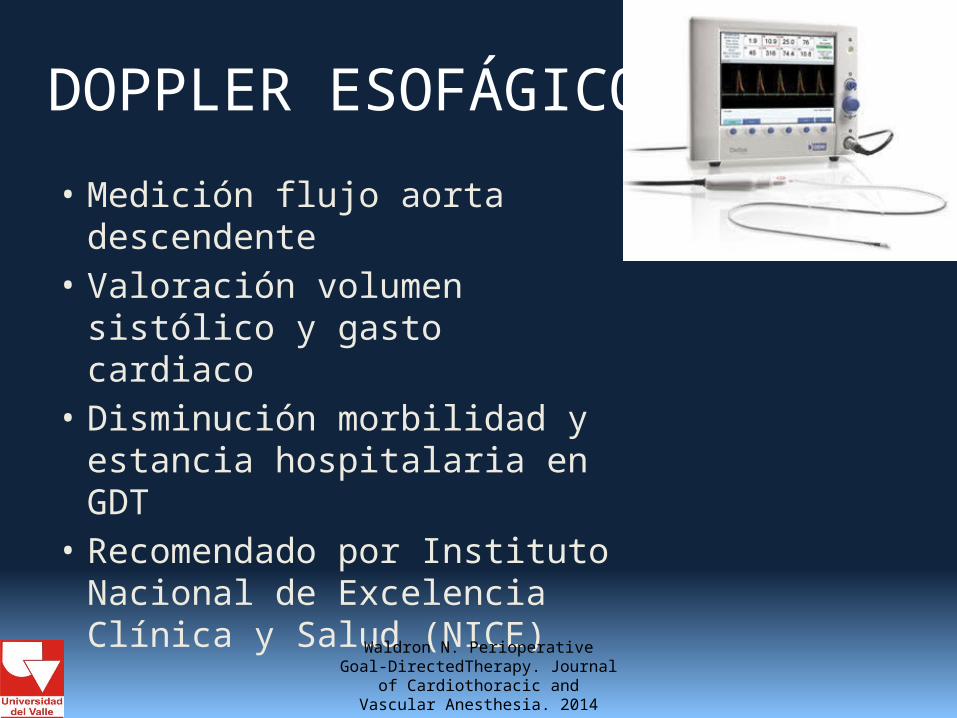
DOPPLER ESOFÁGICO
• Medición flujo aorta descendente
• Valoración volumen sistólico y gasto cardiaco
• Disminución morbilidad y estancia hospitalaria en GDT
• Recomendado por Instituto Nacional de Excelencia Clínica y Salud (NICE)
Waldron N. Perioperative Goal-DirectedTherapy. Journal of Cardiothoracic
and Vascular Anesthesia. 2014
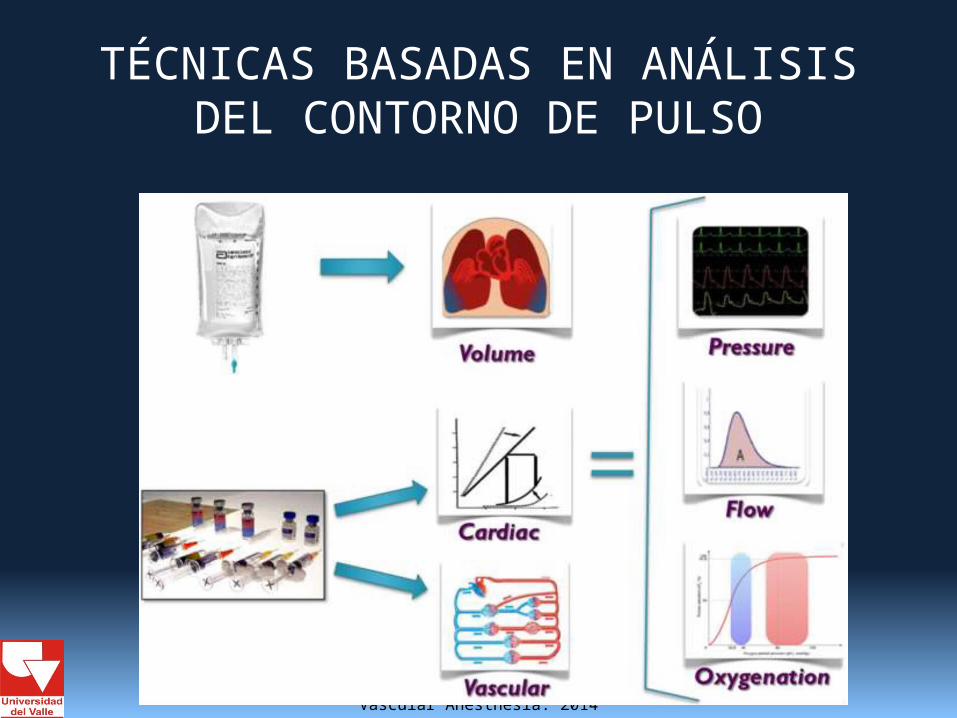
TÉCNICAS BASADAS EN ANÁLISIS DEL CONTORNO DE PULSO
Waldron N. Perioperative Goal-DirectedTherapy. Journal of Cardiothoracic
and Vascular Anesthesia. 2014

UTILIDAD MEDIDAS DINÁMICAS
Variación de ondas de presión arterial depende de la volemia
• Año 1998: 1%• Año 2012: 45%
Predice respuesta a fluidos
No son marcadores de volemia ni precarga
Mejores predictores que medidas de presión de llenado
% utilización:
¿Mejora desenlaces?
The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Critical Care 2014

UTILIDAD MEDIDAS DINÁMICAS
Meta-análisis
• Variabilidad volumen sistólico (SVV)• Variabilidad presión de pulso (PPV)• Variabilidad presión sistólica (SPV)• Índice de variabilidad pletismográfica (PVI)
Desenlace primario: morbilidad POP
14 artículos: 961 pacientes
2007 – 2013
Europa – China – USA – India – Brasil
The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Critical Care 2014

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

Reducción significativa en morbilidad global
The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Critical Care 2014
Reducción significativa en estancia en UCI, morbilidad infecciosa, cardiovascular y abdominal
Tendencia a la reducción de complicaciones respiratorias
No diferencias en complicaciones renales

UTILIDAD MEDIDAS DINÁMICAS
Beneficios de parámetros dinámicos similar a parámetros de flujo
Método más simple, no requiere cálculos
Costo-eficiente
Sin embargo tiene limitaciones:
The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Critical Care 2014

MARCADORES DE BIENESTAR TISULAR
Complemento a dispositivos de monitoria continua
Indicadores de aporte/consumo O₂
Medida intermitente
Beneficio en desenlaces clínicos
No hay clara superioridad de alguna en GDT (lactato – BE - SVO₂ - ERO₂ - P(v a)CO₂)
Isbell J. Impact of hemodynamic monitoring on clinical Outcomes. Best Practice & Research Clinical Anaesthesiology 2014
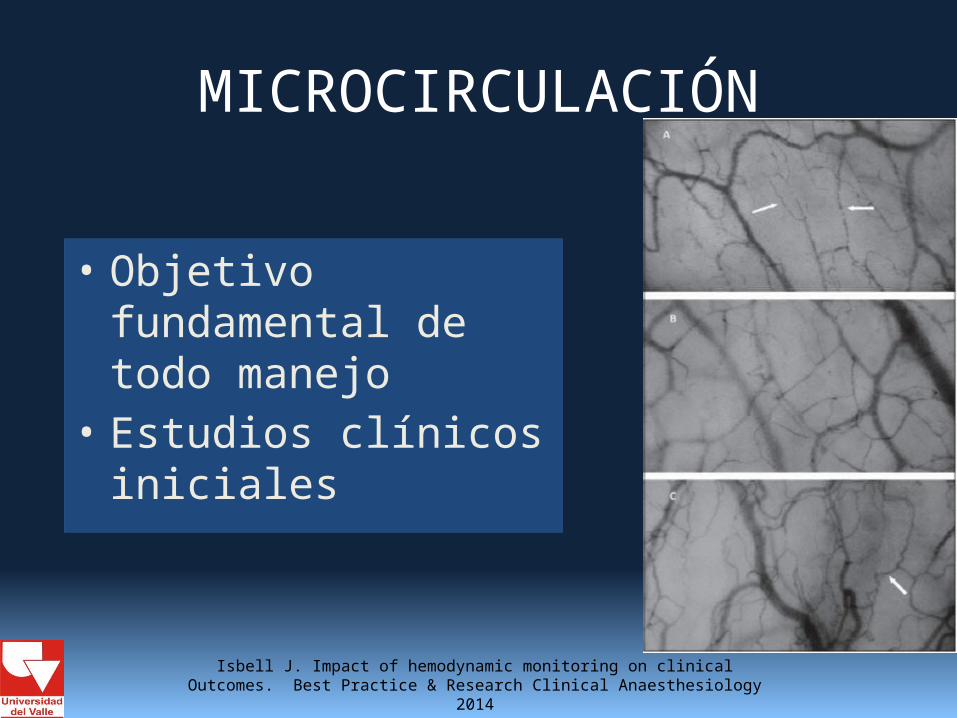
MICROCIRCULACIÓN
• Objetivo fundamental de todo manejo
• Estudios clínicos iniciales
Isbell J. Impact of hemodynamic monitoring on clinical Outcomes. Best Practice & Research Clinical Anaesthesiology 2014

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

PRESIÓN CONT
MANEJO ÁCIDO BASE
MANEJO VENT
OXIGEN
MEDIDA DESEMPEÑO
CARDIACO
VALORACIÓN DEPENDENCIA
VOLUMEN
PVC O SVCO₂
PCCP O SVMO₂
CVC SI
LÍNEA ARTERIAL
SI SI SI SI
CONTORNO PULSO
SI SI SI SI SI
CAP SI SI SI SI
DOPPLER ESOFAGICO
SI SI
BIOIMPED SI SI

FLUIDO IDEAL
Coloides no reducen riesgo de complicaciones ni muerte Hidroxietil starch aumenta riesgo de muerte (RR 1 IC95% 1.02 – 1.09)Coloides costo mucho mayor a cristaloides
Perel P. Colloids versus crystalloids for fluid resuscitation in critically ill patients (Review) The Cochrane Collaboration. 2013
No hay gran evidencia en cuanto al inotrópico o vasoactivo ideal en GDT

FLUIDO IDEAL
• ¿Cristaloides balanceados o no?• Revisión sistemática 706 pacientes • No diferencias en morbimortalidad entre
grupos• Cristaloides no balanceados: – Mayor hipercloremia y acidosis metabólica – Mayor necesidad de trasfundir plaquetas
Burdett E. Perioperative buffered versus non-buffered fluidadministration for surgery in adults (Review) The Cochrane Collaboration. 2013

FLUIDO IDEAL
Rusell L. The ideal fluid. Curr Opin Crit Care 2014, 20.

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

¿Existe riesgo de complicaciones cardiacas en pacientes de alto riesgo?

RIESGOS TERAPIA DIRIGIDA POR METAS
• Metaanálisis • 22 RCT • 2129 pacientes • Reducción complicaciones cardiovasculares (OR:
0.54 (0.38 – 0.76) y arritmias (OR: 0.54 (0.35 – 0.85)• No diferencias en desarrollo de edema pulmonar
agudo ni isquemia miocárdica• Mayor beneficio con monitoria mínimamente
invasiva
Arulkumaran N. Cardiac complications associated with goal directed therapy in high-risk surgical patients: a meta analysis. British Journal of Anaesthesia. 2014

TERAPIA DIRIGIDA POR METASElegir monitoria según contexto del paciente
Control periódico medidas de bienestar tisular
VVS < 12%
IC ≥ 2.5 l/min/m²
TAM en metas
Revalorar cada 15 minutos
Cristaloide balanceado (si ↓ IC considerar dobutamina)
Dobutamina
Norepinefrina
NO
NO
NO

CONCLUSIONES
• Es fundamental lograr una adecuada perfusión tisular en el paciente llevado a cirugía mayor
• La terapia dirigida por metas basada en fluidos, inotrópicos y vasoactivos ha demostrado claramente un beneficio a corto, mediano y largo plazo
• La elección del monitoreo depende del contexto de cada paciente

CONCLUSIONES
La pregunta que queda por resolver es….
¿POR QUÉ NO LA USAMOS?

Joosten A. Defining Goals of Resuscitation in the critically I ll Patient. Crit Care Clin. 2015

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012
MUCHAS GRACIAS

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012

Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012


Anesthetic considerations for the patient with liver disease. Curr opin anesth 2012
• Un hermano puede no ser un amigo, pero un amigo será siempre un hermano Demetrio de Falero





























