Embed Size (px)
DESCRIPTION
The presentation explains the different theories of DDH and the proper imaging ultrasound technique.
Citation preview

Dr/Ahmed Bahnassy
Consultant Radiologist
Riyadh Military hospital

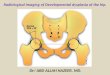
What is DDH
• The natural history of DDH dictates that this is not necessarily a simple task.
• DDH is composed of two elements:
• (1) instability and
• (2) abnormal morphology.

Assesment
• The technique for performing an infant hip sonogram may vary depending upon one's belief as to pathophysiology.
• Initial focus of hip sonography by Graf was on acetabular morphology, using a single static sonographic view.
• Harcke et al, on the other hand, emphasized assessment of instability in addition to morphology and advocated a dynamic sonographic technique.

• The current recommendation for sonographic examination of the infant hip incorporates assessment of both instability and morphology so the pathophysiology issue is resolved with respect to performance of the sonographic examination .

Hip sonographyTABLE 1 -- HIP SONOGRAPHY FOR DEVELOPMENTAL DYSPLASIA OF THE HIP
View Key Feature Comment
Coronal neutral* A Acetabular morphology Measurement optional
Coronal flexion A Acetabular morphology Measurement optional
Stability (if stressed) Stress optional
Used with Pavlik harness
Transverse flexion A Stability Stress required (except during treatment)
Used with Pavlik harness
Transverse neutral Femoral head position Optional view
Data from Harcke HT, Grissom LE: Performing dynamic sonography of the infant hip. AJR Am J Roentgenol 155:837-844, 1990; with permission.

Correct coronal view

Correct transverse view

I-Morphological assesment
• This system is based upon the appearance of the acetabulum in a coronal neutral position and describes measurement of acetabular slope (alpha angle) and position of the acetabular labrum (beta angle).

Benefits
• It is a well-recognized feature of DDH that the condition changes with time.
• It is greater at birth and decrease spontaneously in the first few months of life without treatment.

• Of particular relevance is the distinction of normal and abnormal in the first few weeks of life. It is recognized that a large number of newborns have a mild instability that has been described as physiologic laxity. In association with this is mild acetabular dysplasia consisting of a slightly increased angulation of the bony acetabulum as determined by Graf alpha angles (type 2A).

How to make good exam
• The proper coronal view, whether the femur is in neutral or in flexion, contains three elements .
• (1) The echoes from the bony ilium should be in a straight line parallel to the surface of the transducer.
• (2) The transition from the os ilium to the triradiate cartilage must be seen definitively.
• (3) Finally, the echogenic tip of the cartilage labrum needs to be present in the same plane that contains the other two elements.

Model view

Take your measurements


• Graf classification of infant hips based on the depth and shape of the acetabulum as seen on coronal ultrasonograms.
• Type I: normal; characterized by a well-formed acetabular cup with the femoral head beneath the acetabular roof.
• Type II: immature in infants less than three months of age and mildly dysplastic in infants older than three months; characterized by a shallow acetabulum with a rounded rim.
• Type III: subluxated; characterized by a very shallow acetabulum with some displacement of the femoral head.
• Type IV: dislocated; characterized by a flat acetabular cup and loss of contact with the femoral head.

Angle values

Dislocated Type III
• Lateral displacement of femoral head.
• Soft tissue between femoral haead and acetabulum
cross sectional view
normal

Dislocated hip type IV
coronal view

II- Stability assesment• The assessment of instability incorporates
dynamic technique in two views that include application of stress.
• Both views are performed with the hip flexed: the transducer orientation is coronal for one view and axial for the other.

Relax your patient
• Assessing the hip when the infant is not relaxed masks the presence of instability.
• To ensure a cooperative infant, it is recommended that a sonogram be performed in a quiet, semidarkened environment with a parent present and visible to the child.
• Bottle feeding the infant during the examination is helpful.

• Examination by ultrasound is modeled after the clinical examination and is based upon the provocative test for dislocation of an unstable hip (Barlow test) or the reduction of a dislocated hip (Ortolani test).

• With subluxation and lesser degrees of instability, the flexed hip tends to seat with abduction.
• Displacement is noted during adduction and stress.

• The key feature of instability is the lateral movement (toward the transducer) of the femoral head along the ischium. This results in increased echogenic soft tissue medially.
• Whereas a normal hip shows slight changes in the appearance of the medial tissues between abduction and adduction, with instability, the thickness more than doubles

Dynamic testing
• At rest :Normal.• With stress
subluxation occurs and B angle increases.

Summary• Ultrasonic evaluation of DDH includes:
• I-Morphology assesment (Graf angles)
• II-Stability assesment (dynamic exam )
• Acquired data depend on proper technique.




![Developmental Dysplasia of the Hip: [Print] - eMedicine … · 2017-07-13 · emedicine.medscape.com eMedicine Specialties > Orthopedic Surgery > Hip Developmental Dysplasia of the](https://img.pdfslide.us/doc/110x75/5e8dfff173e63d53604f5cb5/developmental-dysplasia-of-the-hip-print-emedicine-2017-07-13-emedicinemedscapecom.jpg)