Embed Size (px)
DESCRIPTION
Article about real time US in hip dysplasia evaluation
Citation preview

406 THE JOURNAL OF BONE AND JOINT SURGERY
REAL-TIME ULTRASOUND IN THE DIAGNOSIS OF CONGENITAL
DISLOCATION AND DYSPLASIA OF THE HIP
N. M. P. CLARKE. H. THEODORE HARCKE, PETER McHUGH, MYUNG 500 LEE, PATRICIA F. BORNS,
G. DEAN MAcEWEN
From the Alfred I. duPont Institute, Wilmington, Delaware
A technique of examining the infant hip joint with real-time ulfrasound is described. Since the
cartilaginous femoral head is clearly imaged by ultrasound, anatomical structures and their relationships can
be accurately determined. Dislocated hips are easily detected and subluxations also can be visualised.
We report our experience with 131 examinations in 104 patients, comprising 259 single hip studies. Of
83 patients who were previously untreated, there were 178 hip studies with three false-negative and four false-
positive ulfrasound results. No dislocations were missed. Twenty-seven patients who were already being
treated were examined to assess hip location, comprising a total of 81 hip studies. In some cases the patients
were examined while in an abduction device, cast, or Pavlik harness. In one case a disloction was not detected.
The method of examination using real-time ultrasound is considered to be reliable, accurate, and a useful
adjunct to radiography. The advantages are that it is non-invasive, portable, and involves no exposure to
radiation.
The diagnosis of instability and dysplasia in the hip of
the newborn infant remains difficult. Although clinical
examination is recognised as an effective screening
method for dislocations, there remains a small popula-
tion of neonates in whom a confirmatory image is
desirable. Radiographs are, of course, helpful in the
assessment of unstable hips (Bertol, Macnicol and
Mitchell 1982) or frankly dislocated hips. However, the
exact indications for and limitations of radiographic
examination of the neonatal hip are still unclear. Un-
certainties arise in the interpretation of radiographs of
the immature pelvis, regardless of the intended position
of the hip; indeed, position may be an important cause of
simulated abnormality (Blank 1981).
Misinterpretation arises because the only structures
imaged by radiographs are the ossified portions of the
pelvis. It therefore becomes necessary to extrapolate the
image of the cartilaginous structures. Clearly this has
disadvantages, and a radiograph only contributes signifi-
cantly to the diagnosis and management ofthe hip ifit is
N. M. P. Clarke, FRCS. Senior RegistrarRoyal Orthopaedic Hospital, Woodlands, Northfield, BirminghamB3l 2AP, England.
H. T. Harcke. MD, Director, Department of Medical ImagingP. McHugh, Research StudentM. S. Lee, MD, Radiologist. Department of Medical Imagingp. F. Borns, MD, Radiologist, Department of Medical ImagingG. D. MacEwen, MD, Medical DirectorAlfred I. duPont Institute, P0 Box 269, Wilmington, Delaware19899, USA.
Requests for reprints should be sent to Mr N. M. P. Clarke.
�,i_�) 1985 British Editorial Society of Bone and Joint Surgery0301-620X/85/3051 $2.00
definitely abnormal. At present, clinical and radio-
graphic examinations are used to complement each
other. A single examination by itself may be unsatis-
factory, and invasive arthrography may, in some
patients, be the only means of obtaining a clear image
of the developing hip joint.
Since Kleinberg and Lieberman (1936) introduced
the acetabular index as a possible means of identifying
abnormal hips, confusion and controversy have existed
and many attempts to clarify the exact radiographic
indices for dysplasia have been made (Caffey et a!. 1956;
Laurenson 1959). In some methods of evaluation,
complicated calculations are required (Tonnis I 976;
Wientroub 1981).
In the context of this diagnostic dilemma, ultra-
sound has obvious potential for examining the infant
hip. It requires no exposure to radiation and clearly
images the cartilaginous structures that are so poorly
delineated by radiography.
Graf(1983) was the first to realise this potential. He
used a fixed-arm B-scanning unit to obtain sonographic
images ofinfant hipjoints. His technique was necessarily
complicated because of the equipment he used, and it
took considerable expertise and time to obtain a satis-
factory examination. Real-time ultrasound is much
simpler to operate and is portable, and the ultrasound
image changes rapidly enough to portray movement.
Images are obtained by placing a transducer on the skin
and scanning a specific sector of the anatomy. The sector
is varied by moving the transducer, allowing simulta-
neous images to be viewed on a screen. Novick, Ghelman
and Schneider (1983) examined a small number of infant
hips using real-time ultrasound and were encouraged by

Number of Repeatexaminations examinations
10 218 29 012 125 0
5 14 0
83 6
Totalnumberof hips
244018265012
8
I 78Total
Treated (27t patients)Pavlik harness�NilIn castIn braceIn traction
18 97 1l� 2I I0 2�
15
5416
542
Total 27 81
Exclusions (18 patients) 18 38
* Positive Barlow or Ortolani signst 6 patients originally examined before treatment were examined again
after treatment started, 4 once and 2 patients three times� Only 16 examinations in 10 patients were performed with the baby
actually in the harness§ Signifies only one hip examined
REAL-TIME ULTRASOUND IN DIAGNOSING CONGENITAL HIP DISLOCATION AND DYSPLASIA 407
VOL. 67-B, No. 3, MAY 1985
the views that they obtained. This led us to undertake a
prospective study of a group of infants referred for hip
evaluation.
The aims of this study were: to establish that real-
time ultrasound was a reliable method of identifying
anatomical structures and their relationships; to develop
a technique for routine examination; and to ascertain
whether ultrasound could differentiate between normal
and abnormal hips.
MATERIALS AND METHODS
A total of 122 patients referred to the Alfred I. duPont
Institute for evaluation of their hips have been studied.
All were examined clinically by an orthopaedic surgeon
for instability or dislocation of the hip. A conventional
anteroposterior radiograph was then obtained, followed
by real-time ultrasound examination of the hips. The
ultrasound studies were performed without knowledge
of the preceding clinical and radiographic findings. In
those instances where the infant was already being
treated, or had returned for a follow-up visit, it was
obvious that there was some clinical problem. However,
at the time of ultrasound examination, the examiner was
not aware of either the side or the type of involvement
which had been diagnosed.
Table I details the patient population. At review, 19
examinations in I 8 patients were excluded: one patient
(two examinations) had had multiple previous surgical
procedures; in I 5 there were no radiographs available for
comparison; in one patient there was a technical failure;
and in one osteogenesis imperfecta prohibited a satis-
factory examination. There remained I 31 examinations
in 104 patients (259 individual hip studies) which form
the basis of this report. Twenty-seven patients were
already being treated, most of them in a Pavlik harness.
Eighty-three patients were referred either for confirma-
tion of a diagnosis of hip dislocation or dysplasia, or for
initial assessment. The average age at examination was
22 weeks (range 4 days to 2 years 6 months). There were
37 boys and 67 girls. The ultrasound findings were
compared with the clinical examination and with the
radiographic appearance (which was reported indepen-
dently by a radiologist). A computer was employed to
analyse the information.
Patients being actively treated were assessed only
for hip location. In untreated patients, the sonogram was
studied for evidence of hip dislocation or subluxation
and for acetabular dysplasia. This was compared with
radiographic evidence of dislocation, subluxation, lateral
displacement and dysplasia. Clinical examination was
used to identify any limitation of abduction, and to
distinguish subluxatable, dislocatable and dislocated
hips.
Ulfrasound technique. The sonographic examinations
were performed using an Advanced Technology Labora-
tory M K I 00 sector scanner and were recorded on
videotape. Both 3 MHz and 5 MHz transducer frequen-
cies were tried, but most examinations were performed
with the 3 MHz scan head. The technique that was
developed has been reported elsewhere (Harcke et a!.
1984) but it is appropriate to describe it briefly here.
Studies were first performed on the hip joint of an
anaesthetised infant pig. Simultaneous fluoroscopic and
sonographic examinations allowed correlation of ana-
tomical landmarks. This was facilitated by the insertion
of a needle into key points within the joint, such as the
ossific nucleus. We established that the femoral head
appears as an area of few echoes while the bony ilium is a
bright echogenic structure except where the triradiate
cartilage is present and produces few echoes. The gap
created by the cartilage allows the transmission of sound
into the pelvis in the zone where bone has produced
acoustic shadowing.
Table 1. Analysis of patients examined by ultrasound
Reason for evaluation
Untreated (83 patients)Hip clickSubluxationDislocation*Hip checkFoot disordersTorsional deformityMultiple
abnormalities
With children, several views of the infant hip were
obtained by placing the transducer in different positions.
A combination of two views was eventually selected as
being most reliable in the identification of the anatomical
structures. This involved a series of two-plane examina-
tions which, when considered together, yielded a three-
dimensional representation of the hip. Displacement of
the femoral head in any direction could therefore be
determined.
In both views, the images are obtained by placing
the transducer laterally in the region of the greater
trochanter. In the view designated as “transverse-
neutral” the infant is supine and the hip is in the neutral
position. The image is effectively a transverse section of

Fig. I
LAT.
Fig. 2
P0�1
Acetabulum Femoral Head
Fig. 4
LA T.
INF.
Fig. 6
Figures I to 6 are reproduced with permission from Harcke et al. J U/trasound Med 1984;3: 13 1-7.
ANT.
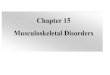
Figures 1 to 3
Figure I-The “transverse-neutral view.” Thesector scanned by the ultrasound is a transversesection of the hip joint which is in the neutralposition. Figures 2 and 3-The image obtainedfrom the “transverse-neutral” view of a left hipwith a corresponding diagram to identify the
anatomical landmarks.
Triradiate Cartilage
Pelvis
sup.
Fig. 3
Figures 4 to 6
Figure 4-The “coronal-flexion” view. Theultrasound sector effectively scans a coronalsection of the hip joint. The femur is in theflexed position and the transducer is rotatedthrough 90 when compared with the“transverse-neutral” view. Figures 5 and 6-The image obtained from the “coronal-flexion” view with a corresponding diagram to
identify the anatomical landmarks.

True Truenegative* positivet
False Falsenegative� positive� ConflictsL
REAL-TIME ULTRASOUND IN DIAGNOSING CONGENITAL HIP DISLOCATION AND DYSPLASIA 409
VOL. 67-B. No. 3. MAY 1985
the hip joint, femoral head and neck (Fig. 1). Figure 2
shows the actual image obtained, with a corresponding
diagram of the anatomical landmarks (Fig. 3). The
femoral head lies against the bony acetabular floor with
the triradiate cartilage clearly seen as a defect in the
bright echoes. The concentric relationship of the femoral
head to the triradiate cartilage in this view is crucial,
since failure to visualise it is indicative of displacement.
The femoral shaft serves as a reference point for the
examiner. By moving the transducer in a cephalad
direction, the femoral head is revealed. Lateral displace-
ment is seen as a gap between the femoral head and the
acetabular floor. Superior displacement will cause the
acetabulum to be obscured by echoes from the femoral
shaft and the triradiate cartilage will not be visualised.
In the second view, known as the “coronal-flexion”
view, the infant remains supine, the hip is flexed to 90#{176}
and the transducer is also rotated through 90#{176}.The area
scanned is effectively a coronal section of the flexed hip
joint (Fig. 4). Figure 5 shows the actual image obtained
and Figure 6 is the corresponding diagram. The position
view. In. a few cases infants who were being treated in
casts were examined after cutting a lateral window
through the plaster.
RESULTS
Of the 83 patients being evaluated for the first time, 89
examinations were performed comprising 178 individual
hip studies. These studies were evaluated by comparison
with both clinical and radiographic examinations (Table
II). There were I 36 true-negative and 22 true-positive
results.
Of the true positives there were eight subluxations,
10 dislocations, and four hips with acetabular dysplasia.
For the purposes of this study, a false-negative ultra-
sound result was deemed to have occurred when ultra-
sound missed an abnormal hip detected by both clinical
examination and radiography. Similarly, a false-positive
ultrasound result occurred when ultrasound was inter-
preted as showing an abnormal hip when clinical and
radiographic examinations were both normal. There
were three false-negative and four false-positive results
Table II. Hip evaluations in previously untreated patients
Reason for evaluation
Hipclick 19 2 1 1 1
Subluxation 26 6 1 1 6
Dislocation 7 8 0 1 2
Hipcheck 18 3 1 1 3
Foot disorder 48 2 0 . 0 0
Torsional deformity 12 0 0 0 0
Multiple abnormalities 6 1 0 0 1
Total 136 22 3 4 13
* Normal clinical, radiographic, and ultrasound examinations
t Abnormal clinical, radiographic, and ultrasound examinations� Abnormal clinical and radiographic examinations; normal ultrasound examination§ Normal clinical and radiographic examinations; abnormal ultrasound examinationU Inconsistent clinical and radiographic results
of the bright echoes of the ilium superiorly reflect
acetabular depth and, therefore, coverage of the femoral
head. The greater the cover, the less the radiographic
acetabular index, thus enabling an assessment to be
made ofacetabular dysplasia. Again, the femoral shaft is
a reference point. It lies anteriorly because of the flexed
position ofthe hip. By moving the transducer posteriorly,
the femoral head and acetabulum will come into view.
Femoral head displacement will again cause the acet-
abulum to be obscured by the echogenic femoral shaft.
Most ultrasound examinations in this series were
performed using a combination of the two views de-
scribed. Evaluation of infants in the Pavlik harness,
however, was based only upon the “coronal-flexion”
(Table III). No frank dislocations were missed. Ultra-
sound missed a unilateral dysplastic hip in one patient; in
two other patients, each with bilateral subluxation,
ultrasound diagnosed only unilateral subluxation. No
dislocations were falsely diagnosed. In three of the false-
positive results, clinical or radiographic examinations
had suggested unilateral abnormality, but ultrasound
demonstrated bilateral involvement.
Table II also details the 13 hip studies in which the
clinical and radiographic examinations did not agree;
these are categorised as “conflicts” . In seven hips, the
radiographic and ultrasound examinations were ab-
normal but clinical examination was normal; in five the
radiographic results were abnormal but both clinical and

Radiograph
Bilateral hip clicksPossible subluxation
Bilateral lateraldisplacement
99 Subluxation Bilateralpositive Barlow test
Normal Bilateral subluxation
410 N. M. P. CLARKE, H. T. HARCKE, P.McHUGH, M. S. LEE, P. F. BORNS, G. D. MACEWEN
THE JOURNAL OF BONE AND JOINT SURGERY
Table III. False-negative and false-positive evaluations in untreated patients (178 hips examined)
Patient Reason fornumber evaluation Clinical examination
False negatives5 Hip click
83 Hip check Left adduction Left dysplasiacontracture
False positivesI 3 Dislocation Left positive Barlow test
Bilateral lateral displace-ment with abnormalacetabula
39 Subluxation Normal Right lateral displace-ment
89 Hip check Normal Normal
1 18 Hip click Normal Left dysplasia
Classification
Ultrasound Left hip Right hip
Left-not concentrically True positive False negativereducedRight-normal
Normal bilaterally False negative True negative
Left-subluxated True positive False negativeRight-normal
Conflict False positive
Bilateral dysplasia False positive Conflict
Left not concentrically False positive True negativereduced
Left-subluxated Conflict False positiveRight-not concentricallyreduced
ultrasound examinations were normal; and in one, clini-
cal and ultrasound examinations were abnormal although
radiographs were normal. Excluding these “conflicts”,
the specificity* for ultrasound in the untreated
group was 97% and the sensitivity* was 88%.
In the group of 27 patients already receiving
treatment at the time of initial ultrasound examination,
42 examinations were made, comprising 81 individual
hip studies. There were 75 true-negative studies (showing
that the hip was normally located), and four true-
positives. Three of these true-positives were hip disloca-
tions (one in an abduction brace and two in the Pavlik
harness) and one was a severely dysplastic hip being
treated in a Pavlik harness. There were no false-positives
in the treated group, but one false-negative result and
one “conflict” did occur. The “conflict” was in a patient
being followed for unilateral hip dysplasia in whom
ultrasound was interpreted as normal but the radio-
graphic appearances were equivocal. The only false-
negative study was in a patient in an abduction brace
with a dislocation that was missed by ultrasound. In this
patient, initial radiographs had been reported as normal,
but suspicion led to confirmation of the diagnosis by
computerised tomography.
. . True negatives* Specificity = ___________________________
True negatives + false positives
. . . True positivesSensitivity = .
True positives + false negatives
DISCUSSION
We have established that real-time ultrasound can, in
fact, be used to image the infant hip. Anatomical
structures and their relationships are clearly visualised,
and the capacity for imaging the cartilaginous femoral
head offers an important advantage over conventional
radiography. The technique for ultrasound examination
that we have described is reliable for hips in infants up to
the age of about one year.
Our experience has shown that one limiting factor
for accurate interpretation of the image is the size of the
ossific nucleus of the femoral head. When the bony
nucleus is present, a zone of acoustic shadowing appears
medially and may be mistaken for the triradiate car-
tilage. The crucial sector in the transverse-neutral view is
one which demonstrates concentric reduction of the
femoral head against the acetabular floor while at the
same time imaging for the triradiate cartilage. It is clearly
important that any artefactual triradiate cartilage is not
mistaken for the actual triradiate cartilage. When the
ossific nucleus is less than 10 mm in its transverse
diameter, the ultrasound beam can be directed at an
angle that bypasses this nucleus and enables the triradi-
ate cartilage to be viewed. However, larger bony nuclei
will obscure medial structures by virtue of the diminished
cartilaginous space between the nucleus and the femoral
metaphysis (Fig. 7).
The combination of two views-the transverse-
neutral and the coronal-flexion--was chosen because
easily identifiable landmarks were consistently visible.
These landmarks could not be misrepresented by a
change in projection, hence normality was always quickly
and reliably established. These two views allow dis-
placement in any direction to be detected, and acetabular

Fig. 7
Transverse-neutral view of a right hip illustrating how a large ossificnucleus may obscure medial structures by virtue ofacoustic shadowing
(arrow).
Fig. 8
REAL-TIME ULTRASOUND IN DIAGNOSING CONGENITAL HIP DISLOCATION AND DYSPLASIA 411
VOL. 67 B. No. 3. MAY 1985
dysplasia can be diagnosed by studying the coronal
section. The flexed posture of the hip in the coronal-
flexion view reflects the position used during the clinical
examination; this view also permits infants to be
examined while retained in a Pavlik harness or abduction
brace, when proper location of the hip is of prime
interest.
We have found that an adduction contracture of the
hip makes the examination easier, in that the ultrasound
“aperture” is effectively enlarged; an abduction contrac-
ture closes the “aperture” and makes the examination
more difficult.
Several aspects of our results merit further dis-
cussion. First, the standards by which we judged the
accuracy of ultrasound-clinical and radiographic
examination-are themselves open to question. The
subtleties of the lax or clicking hip on physical examina-
tion have long been recognised as complicating the
definitive diagnosis of hip dislocation. Likewise, radio-
graphic studies do not always reveal mild degrees of
dislocation, subluxation or, even more obscure, sub-
luxatability. Hence the ultrasound “false-positive” re-
suits may conceivably reflect true pathology, particularly
when consideration is given to the fact that three patients
with false-positive ultrasound studies each had a con-
tralateral hip in which the clinical and radiographic
results were in conflict (Table III).
Those examinations classified as “conflicts”, in
which the clinical and radiographic assessments differed,
are a testimony to the difficulties that may be encoun-
tered in diagnosing hip dislocation and dysplasia. We
have not included these results in our final calculations
because we cannot, except in extreme cases, objectively
determine whether the clinical or radiographic results are
actually correct.
The ability of ultrasound to image the cartilaginous
femoral head-rather than the ossified femoral
metaphysis-in relation to the acetabulum makes it a
very attractive imaging tool. However, its sensitivity
must be viewed with caution. Barlow (1962) has stated
that more than 60% of unstable hips recover sponta-
neously in the first week of life. We have seen several
instances in which ultrasound images of neonatal hips
have displayed slight subluxation of the femoral head
(Fig. 8) which shows as a gap between the head and the
acetabular floor. We have performed an insufficient
number of hip studies in such patients to establish
whether this appearance resolves spontaneously at the
same time as the clinical laxity, or whether it is a true
pathological entity. Clearly, before ultrasound can be
used with certainty as a screening tool for congenital hip
dislocation or dyspiasia, the natural history of this type
of appearance will have to be defined.
In our series, 27 infants were examined while
retained in either a brace or a cast. Those in casts were
examined through a lateral window, using the landmarks
of the coronal-flexion view to assess hip location. Hips
retained in a brace were subject to the difficulties of
examination caused by abduction. The one missed
dislocation was such a case: the femoral head was very
small, the acetabulum very shallow, and the posterior
dislocation was only clearly seen with the aid of com-
puterised tomography.
Transverse-neutral view ofa right hip in a neonate. The femoral head isnot concentrically seated, as evidenced by a gap between the head andacetabular floor medially (arrow). There is also slight posterior
displacement of the femoral head.
No mention has yet been made of the potential for
dynamic examination offered by real-time ultra-
sonography. One dislocatable hip was examined in such
a way that the hip could be viewed in both the located
and the dislocated positions. While this case effectively
demonstrated the possibility of dynamic study, the real
value of such an examination lies in its ability to image

412 N. M. P. CLARKE, H. T. HARCKE, P.McHUGH, M. S. LEE, P. F. BORNS, G. D. MAcEWEN
THE JOURNAL OF BONE AND JOINT SURGERY
hips with less distinct abnormalities. Ultrasound offers
great advantages over conventional radiographs in the
detection of hip abnormalities, certainly as an adjunct to
radiographic evaluation (both diagnostic and follow-up
studies), and possibly even as a screening tool. Ultra-
sound could also eventually replace some of the multiple
radiographs required to assess relocation during treat-
ment, thus reducing exposure to radiation. Ultrasound
may be a non-invasive alternative to the measurement of
angles or distances on a radiograph, since the relation-
ships of the cartilaginous femoral head are defined in
three dimensions. As such, sonographic imaging may
contribute significantly to the understanding of the
natural history and pathological anatomy of the spec-
trum ofjoint abnormality encompassing congenital hip
dislocation and dysplasia.
REFERENCES
Barlow TG. Early diagnosis and treatment of congenital dislocation ofthe hip. J Bone Joint Surg [BrJ l962;44-B:292.-301.
Bertol P, Macnicol MF, Mitchell GP. Radiographic features ofneonatal congenital dislocation of the hip. J Bone Joint Surg [Brl1982;64-B: 176-9.
Blank E. Some effects of position on the roentgenographic diagnosis ofdislocation at the infant hip. Skeletal Radiol 198 1 ;7(l): 59-61.
Caffey J, Ames R, Silverman WA, Ryder Cl’, Houaji G. Contradictionof the congenital dysplasia-predislocation hypothesis of con-genital dislocation of the hip through a study of the normalvariation in acetabular angles at successive periods in infancy.Pediatrics 1956; 17:632-40.
Graf R. New possibilities for the diagnosis of congenital hip jointdislocation by ultrasonography. J Pediatr Orthop l983;3:354-9.
Harcke HT, Clarke NMP, Lee MS, Bores PF, NiacEwen GD.Examination of the infant hip with real-time ultrasound. JUltrasound Med 1984:3: 13 1-7.
Kleinberg S, Lieberman HS. The acetabular index in infants in relationto congenital dislocation of the hip. Arch Surg l936;32: 1049-54.
Laurenson RD. The acetabular index: a critical review. J Bone JointSurg [Br] 1959;4l-B:702-lO.
Novick G, Ghelman B, Schneider M. Sonography of the neonatal andinfant hip. AJR l983;141(4):639-45.
T#{212}nniSD. Normal values ofthe hipjoint for the evaluation ofx-rays inchildren and adults. C/in Orthop 1976; 1 19: 39-47.
Wientroub S, Tardiman R, Green 1, Salama R, Weissman SL Thedevelopment of the normal infantile hip as expressed by radio-logical measurements. mt Orthop 1981 ;4(4):239-41.







![Developmental Dysplasia of the Hip: [Print] - eMedicine … · 2017-07-13 · emedicine.medscape.com eMedicine Specialties > Orthopedic Surgery > Hip Developmental Dysplasia of the](https://img.pdfslide.us/doc/110x75/5e8dfff173e63d53604f5cb5/developmental-dysplasia-of-the-hip-print-emedicine-2017-07-13-emedicinemedscapecom.jpg)