Embed Size (px)
Citation preview
fetal echocardiography
Fetal Echocardiography
fetal echocardiography
• INTRODUCTION• TIMING OF FETAL ECHOCARDIOGRAPHY• EQUIPMENT • LATERALITY OF FETAL BODY AND IMAGE
ORIENTATION• VISCEROATRIAL ARRANGEMENT(SITUS)• CARDIAC POSITION AND AXIS ORIENTATION• SEGMENTAL ANALYSIS• ECHOCARDIOGRAPHIC PROJECTIONS
fetal echocardiography
• Malformations of the heart and arterial trunks are the most common form of congenital anomalies found in humans.
fetal echocardiography
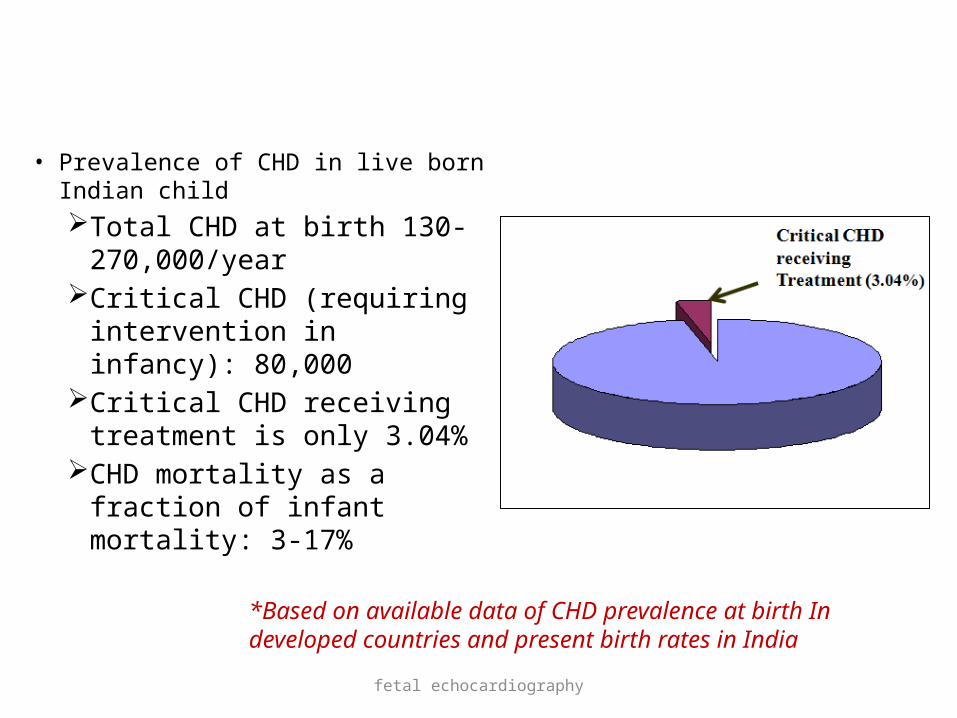
• Prevalence of CHD in live born Indian childTotal CHD at birth 130-
270,000/year Critical CHD (requiring
intervention in infancy): 80,000
Critical CHD receiving treatment is only 3.04%
CHD mortality as a fraction of infant mortality: 3-17%
*Based on available data of CHD prevalence at birth In developed countries and present birth rates in India
fetal echocardiography
• Importance in developing world
Limited resources to treat complex heart problems. Relatively few centres in public sector offering
treatment for complex CHD. Very limited infrastructure for transporting sick
neonates with critical CHDs which are correctable.
Early diagnosis is a solution for this
Antenatal Cardiac Diagnosis

fetal echocardiography
• The incidence of CHD is much higher in the fetal population.
• A good number of fetuses with complex cardiac anomalies succumb in the first trimester itself, even before the cardiac anomaly is suspected;
• some parents opt for termination of pregnancy after the diagnosis is made in the mid-trimester; and some cardiac anomalies are progressive and end in intrauterine death.
• Thus, the incidence quoted above may be only the tip of the iceberg.
fetal echocardiography
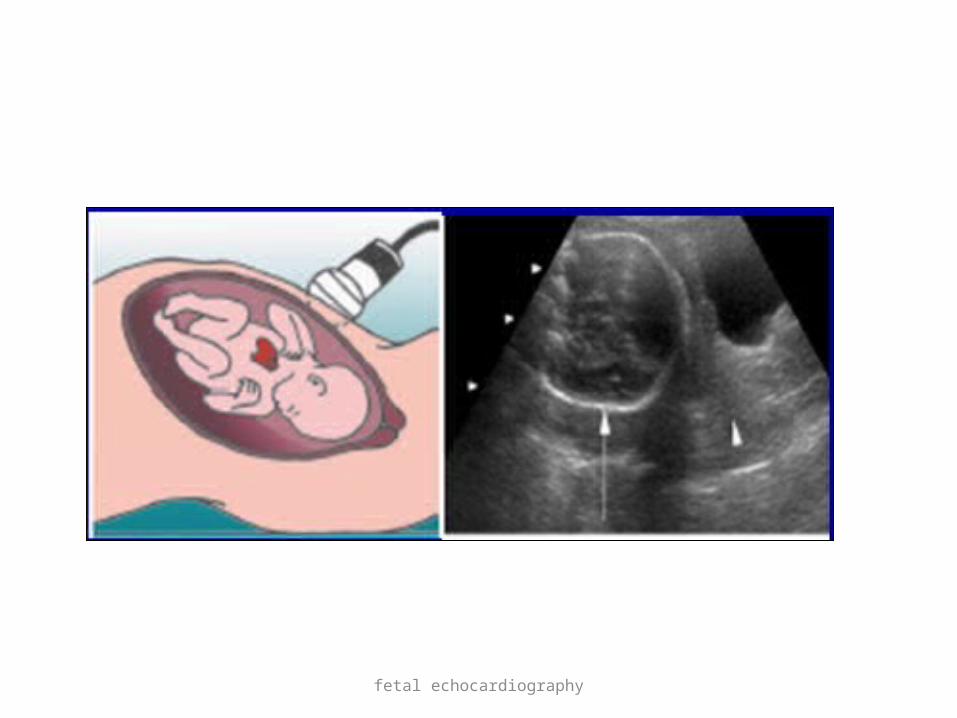
• Fetal echocardiography, or the use of ultrasonic technologies to evaluate the fetal cardiovascular system, enables diagnosis of structural heart defects, and offers a way to observe complex physiological processes prior to birth
fetal echocardiography
Indications for fetal echocardiography
A. Maternal indicationsCongenital heart diseaseCardiac teratogens
Isotretinoin ,lithium, ethanol, phenytoin etcMaternal metabolic disorders
Diabetes, phenylketonuria , gestational diabetesAutoimmune disorders
Sjogrens syndrome , SLEIntrauterine infections
Rubella

fetal echocardiography
B. Fetal indications: Extra cardiac anamolies
Chromosomal and Anatomic(increased NT , GIT , RENAL , CNS ) Fetal cardiac arrythmias
Irregular rhythm , tachycardia(absence of amnionitis) , bradycardia Non immune hydrops Abnormal fetal situs Suspected fetal heart anomaly by screening ultrasound Chromosomal abnormalities Monochorionic twin gestation
Twin twin transfusion syndrome, conjoint twins
fetal echocardiography
• Familial indications :History of CHD
Previous sibling , paternalMendalian syndromes
Williams syndrome , Digeorge syndromeConsanguinity
fetal echocardiography
Indications for converting a routine scan into fetal echocardiography1. Chamber asymmetry2. Altered cardiac axis3. Altered position of the fetal heart4. Enlarged fetal heart5. Arrhythmia
fetal echocardiography
TIMING OF FETAL ECHOCARDIOGRAPHY
• Fetal echocardiography is best performed between 18 and 22 weeks of gestation.
• After 30 weeks gestation, the shadowing effects of the fetal ribs, ratio of fetal body mass-to-amniotic fluid increases so acquisition of images more difficult. • Early maternal transabdominal or trans-vaginal scan at 11 to 14
weeks of gestation, in pt with Increased nuchal translucency.• In the first trimester (11–14 weeks), cardiac details may not be
elicited well, but the presence of a pulsatile ductus venosus or tricuspid regurgitation can be a very strong marker for cardiac and chromosomal anomalies.
fetal echocardiography
Equipment &Technical aspects
• High frequency transducers probes for resolution and details
• Phased array transducers with fundamental frequencies between 4 and 12 MHz are generally used.
• Curvilinear probe with wider near-field of view.
• High frequency transducers with a narrower footprint
fetal echocardiography
• Low frequency transducers and harmonic imaging ---3rd trimester and
• axial resolution of 1 mm or less this is particularly important given the
small size of critical fetal cardiac structures. • Frames rates of 80 to 100 Hz are frequently
needed to view important events occurring at heart rates in excess of 140 beats per minute
fetal echocardiography
• Tissue Doppler imaging is useful in the assessment of fetal arrhythmia.
• decreased persistence, and increased compression. • The system should have the ability to zoom the
image without causing deterioration of image quality.
• A higher pulse repetition frequency (PRF) is required for colour Doppler in the fetus as compared to the settings used for routine obstetric colour Doppler.
fetal echocardiography
Determining the laterality of fetal body and image orientation
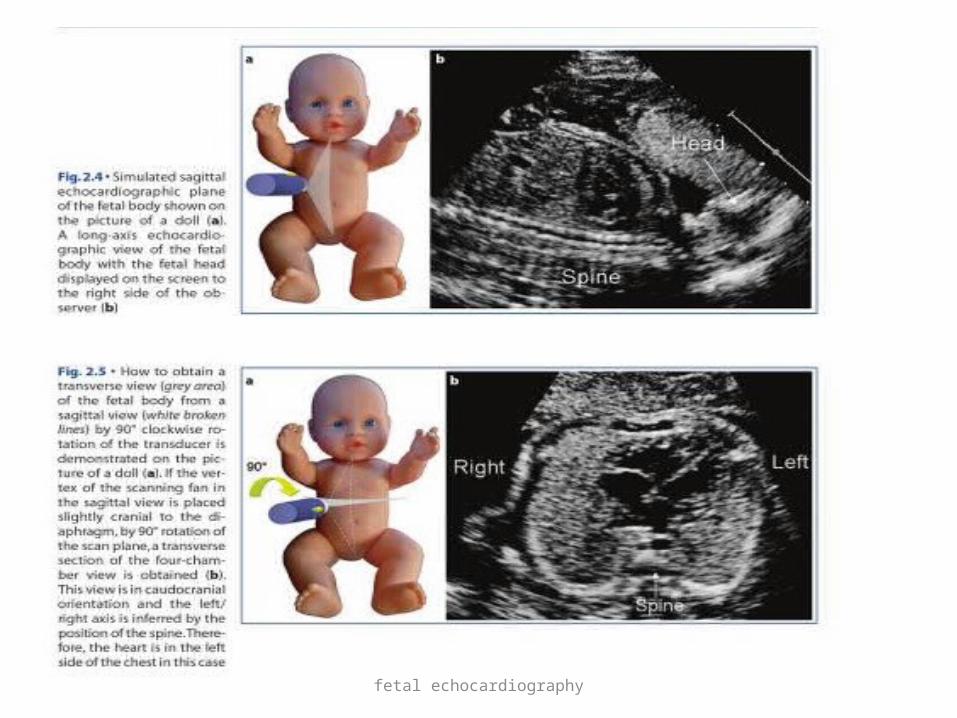
• Most common used method for assesing laterality is proposed by cordes et all.
• It is effective when fetus is in transverse positionProcedure:• Obtaining sagittal view of fetal body. Align transducer in long
axis of fetus (spine)• Orient the transducer so that fetal head is on the right side of
observer on the screen• Rotate the transducer 90* clockwise to obtain a transverse
view of fetal body • Tranverse section thus aquired is caudocranial axis
fetal echocardiography
fetal echocardiography

fetal echocardiography

fetal echocardiography
fetal echocardiography
Image orientation
• Craniocaudal• Caudocranial (standard view)• anatomical

fetal echocardiography
orientation
fetal echocardiography
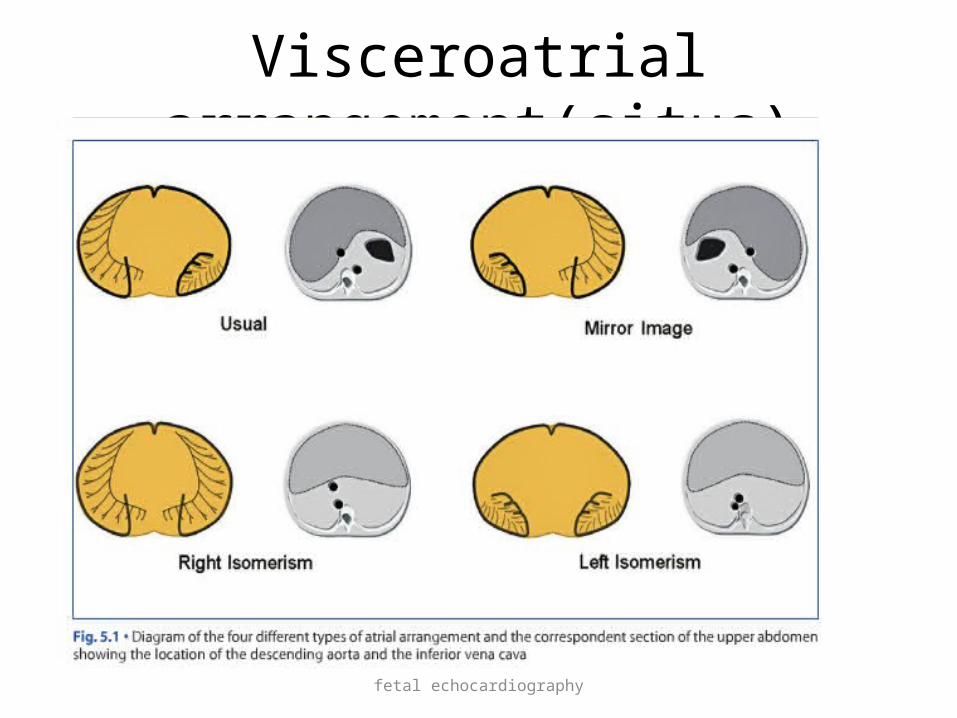
Visceroatrial arrangement(situs)
• To assess morphological arrangement of atria• Appendages are most constant component of
atria• LA appendage is tubular and hook shaped
with narrow junction with venous portion of atrium
• Vestibular aspect of LA is smooth• Pectinate muscle is restricted to appendage
fetal echocardiography
• RA appendage is triangular with broad junction with venous portion of the atrium
• Vestibular aspect of RA contain pectinate muscle
• There is close relationship between arrangement of atria and position of descending aorta and great veins at level of diaphagm

fetal echocardiography
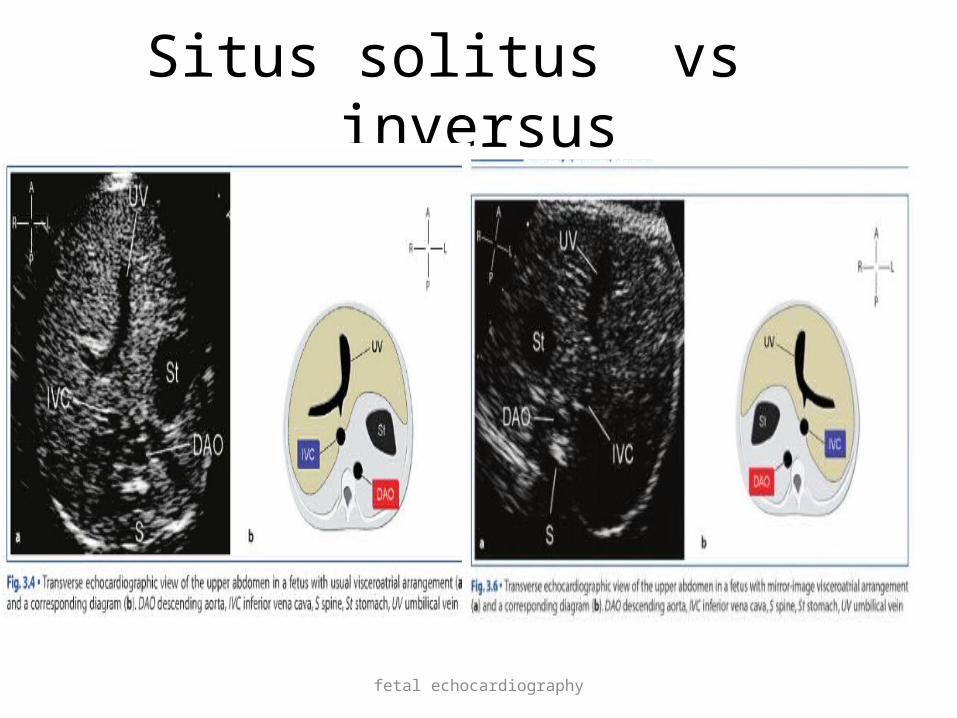
• Situs solitus descending aorta is left to midnline IVC to the right of midline stomach to the left portal sinus curves to the right predominant liver lobe to the right
fetal echocardiography
Situs solitus vs inversus

fetal echocardiography
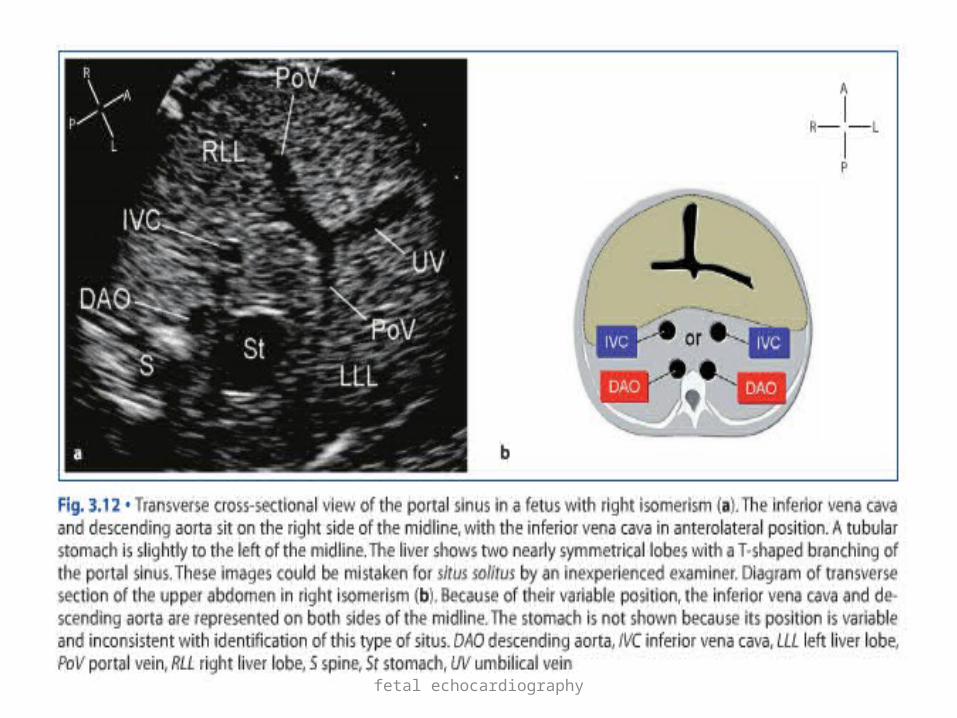
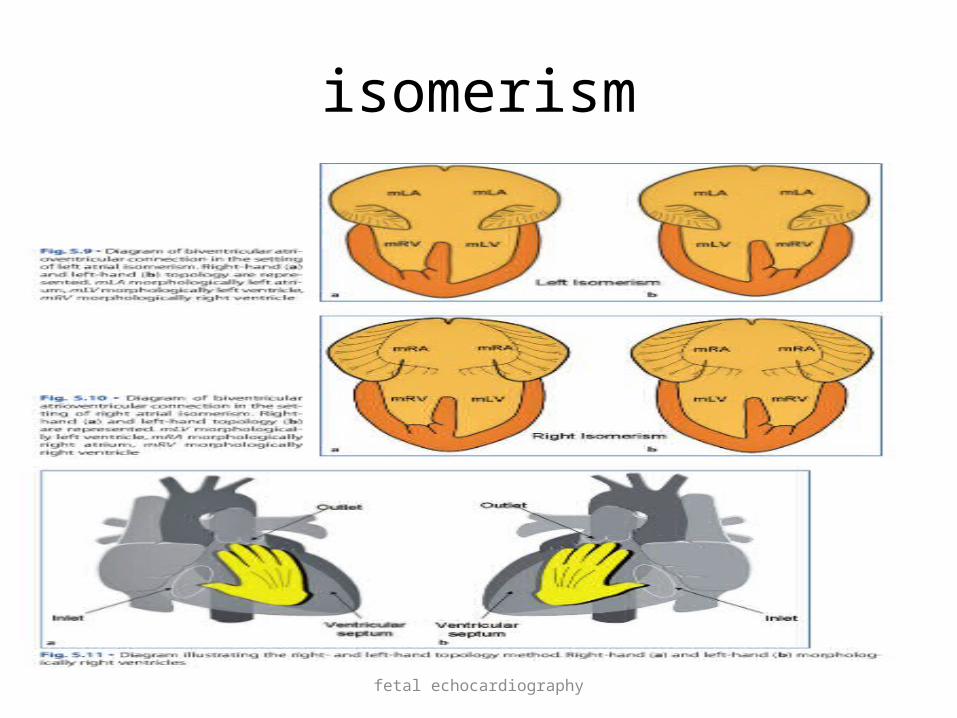
Right vs left isomerism
fetal echocardiography
fetal echocardiography
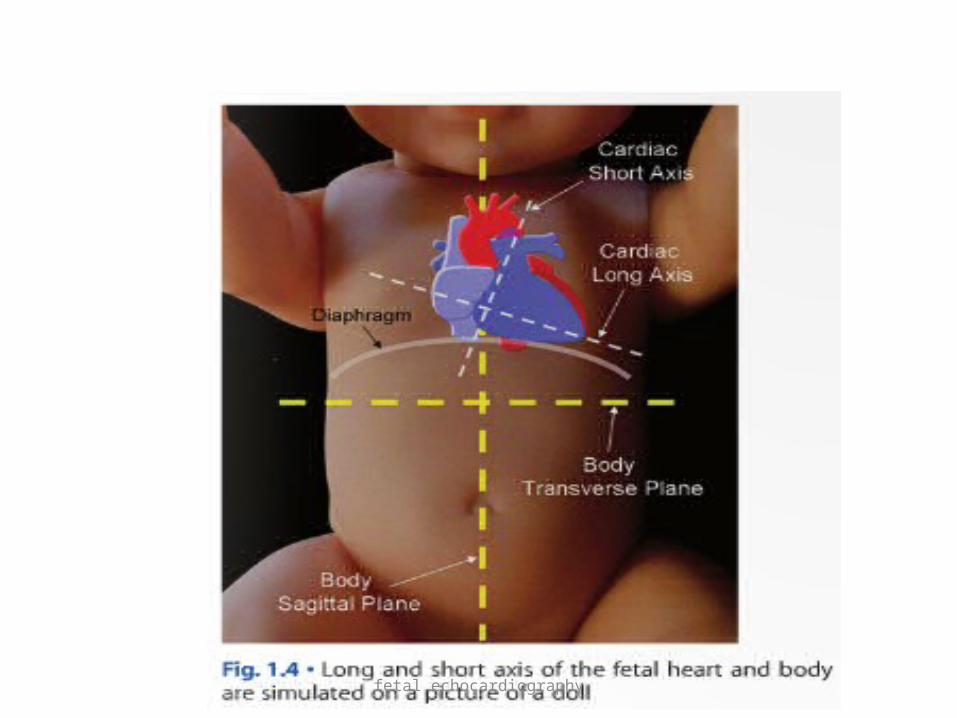
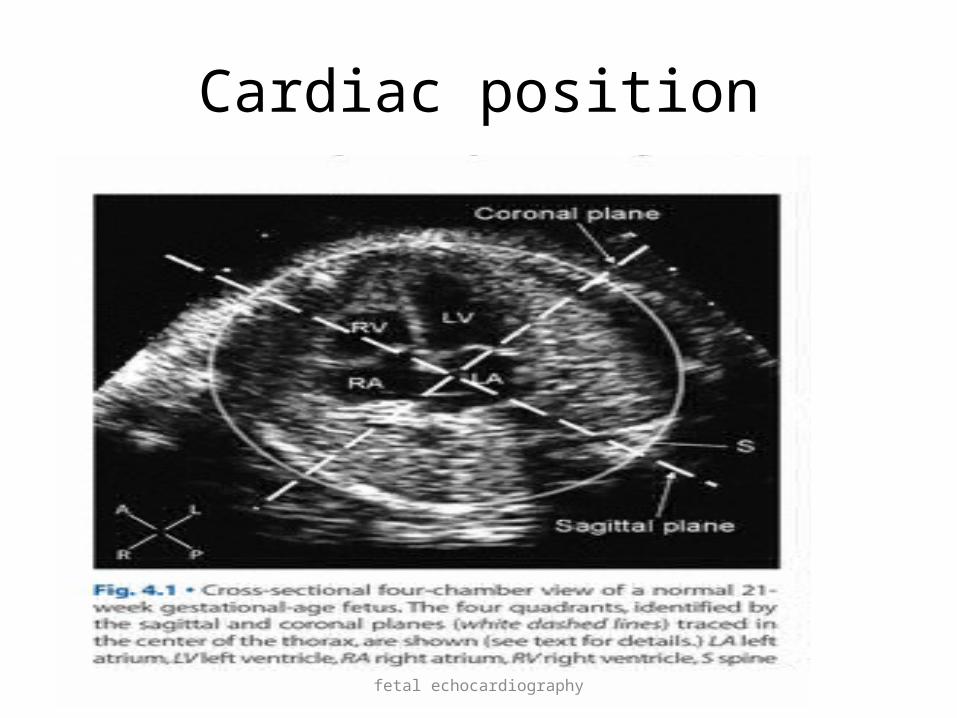
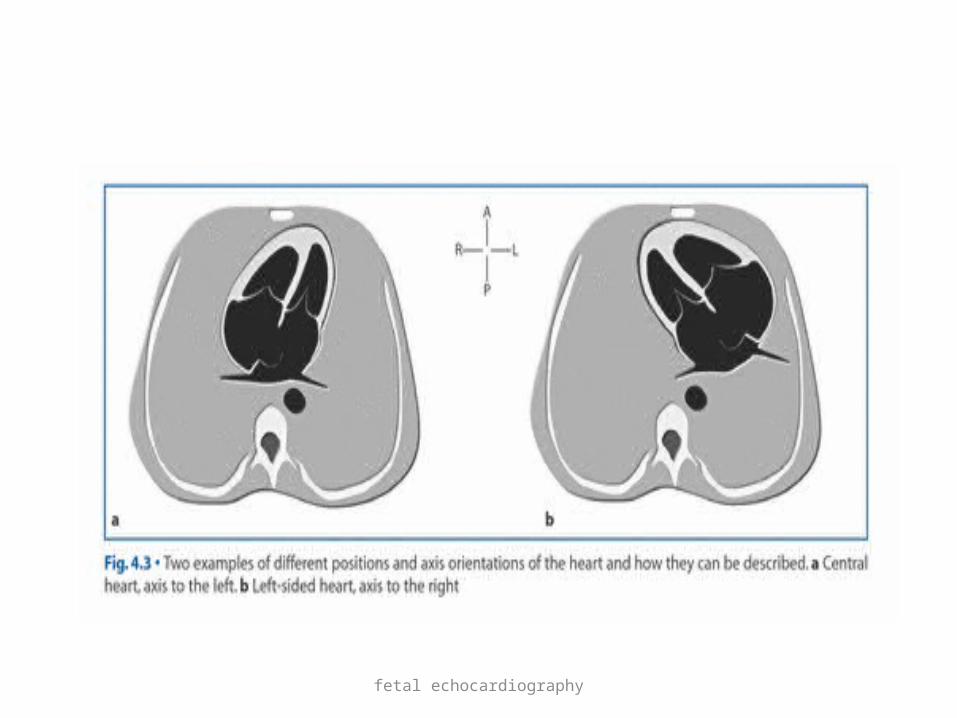
Cardiac position and Axis orientation
• Cardiac position and axis can be assessed in four chamber view
• In this view by tracing sagital and coronal planes through centre of thorax four quadrants are identified
• Lv and most of RV and anterior part of LA lie in left anterior quadrant
fetal echocardiography
fetal echocardiography
Cardiac position
fetal echocardiography
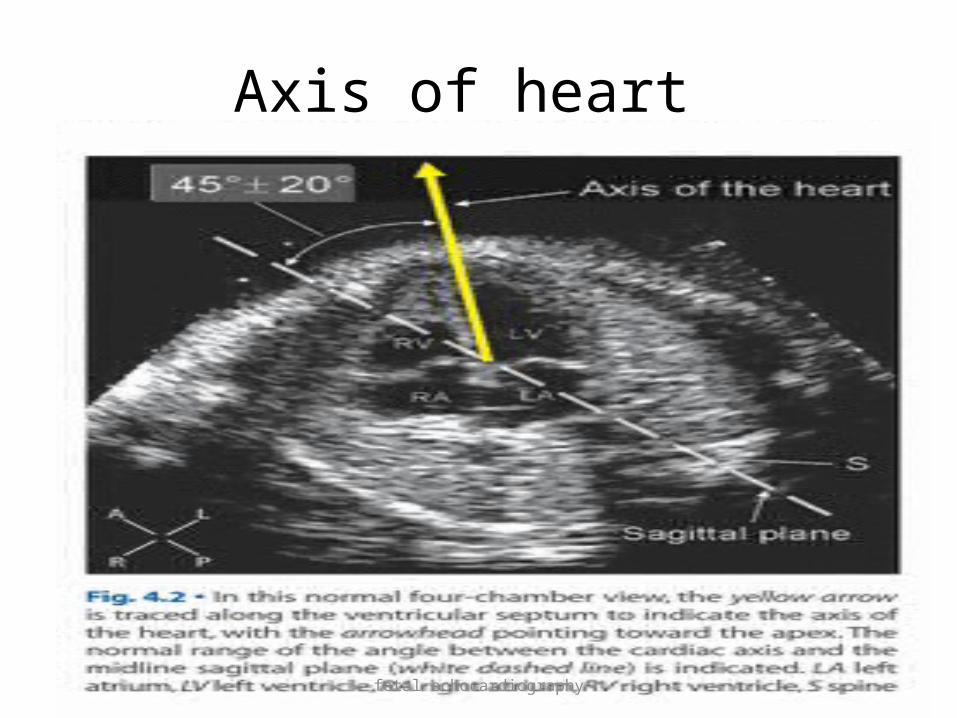
Axis orientation
• Axis of heart refer to its long axis• Axis orientation is expressed as the angle between a line
aalong the ventricular septum ,directed towards the cardiac apex and midline sagittal plane of thorax
• The normal cardiac axis is 45± 15°• . Altered axis is often associated with outflow tract
anomalies• Types levocardia Mesocardia dextrocardia
fetal echocardiography
Axis of heart
fetal echocardiography

fetal echocardiography
Segmental analysis
• Segments– atria ventricles arterial trunks systemic and pulmonary veins• Connections-atrioventricular ventriculoarterial venoatrial
fetal echocardiography
• Atria• LA appendage is tubular • Vestibular aspect of LA is smooth• RA appendage is triangular • Vestibular aspect of RA contain pectinate
muscle
fetal echocardiography
Visceroatrial arrangement(situs)
fetal echocardiography
fetal echocardiography
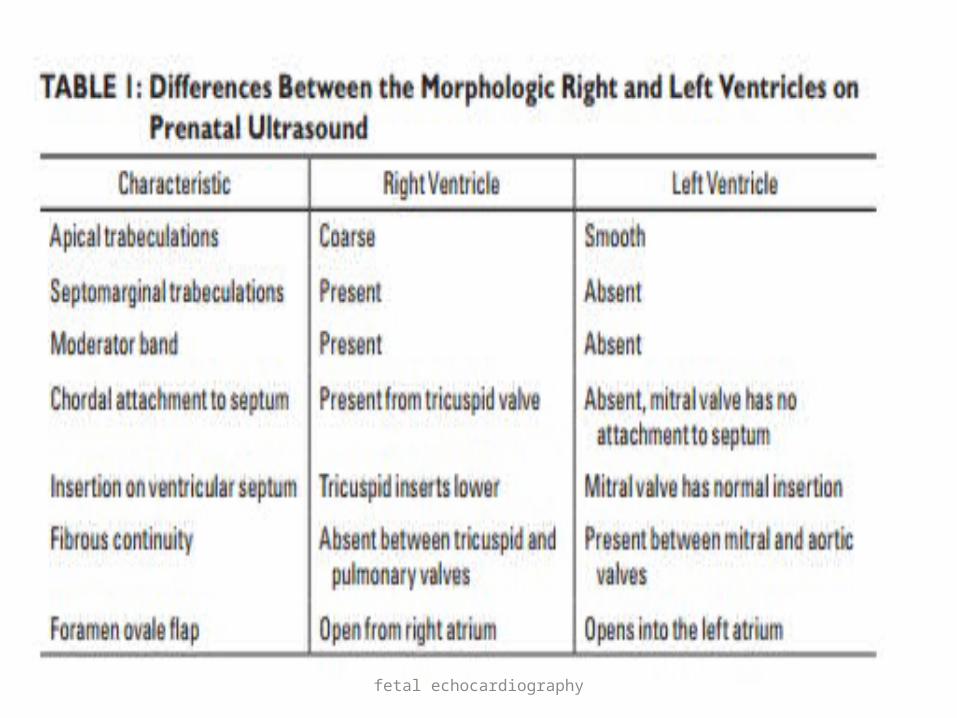
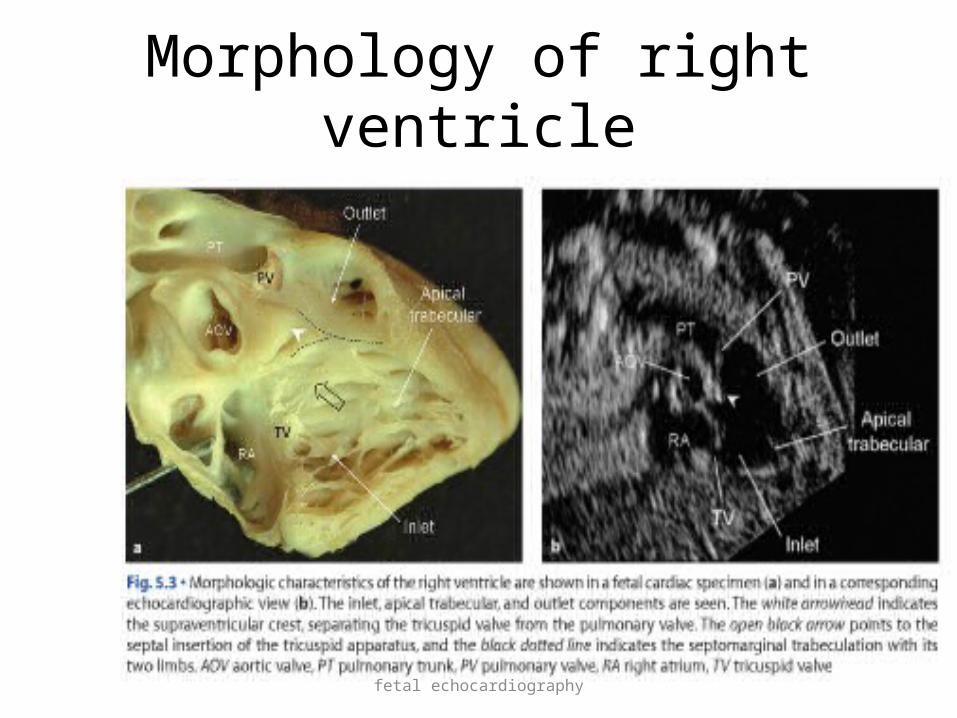
Morphology of right ventricle

fetal echocardiography
Morphological left ventricle

fetal echocardiography
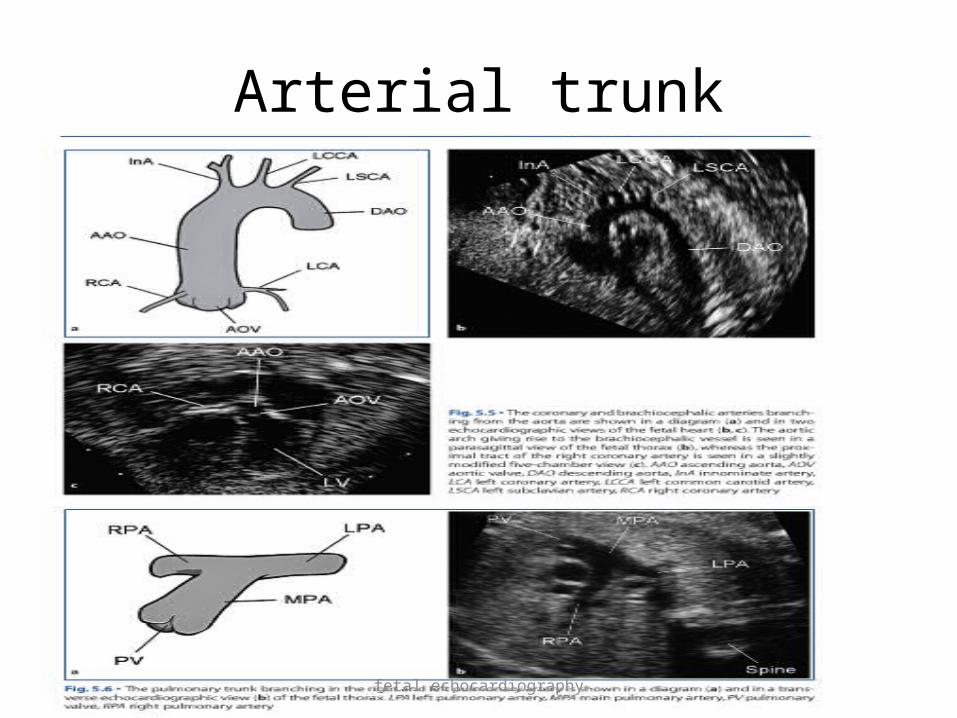
• Arterial trunk• Differentiated by branching pattern• Aorta – coronaries arise from sinuses run superiorly to form aortic arch and gives origin to
brachiocephalic vessels,CIA• Pulmonary artery runs anteroposteriorly and bifurcates
in right & left PA• Main PA connects to descending aorta via ductus
arteriosus
fetal echocardiography
Arterial trunk
fetal echocardiography
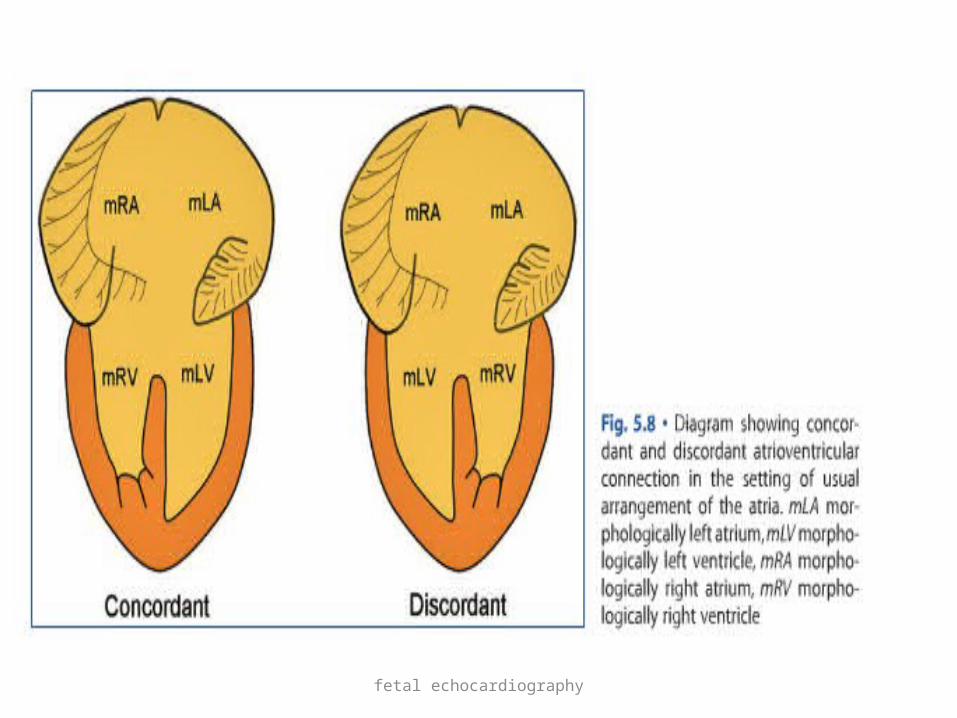
• Atrioventricular connection• Concordant: atrial chamber connected with
appropriate ventricle• Discordant: atrium is connected with
morphologically inappropriate ventricle• In isomerism morphologic RV is determined by
right and left hand topology(palm on septal surface and thumb in inlet and fingers in outlet of ventricle)
fetal echocardiography
fetal echocardiography
isomerism

fetal echocardiography
• Ventriculoarterial connection• Concordant vs discordant• double outlet RV/LV

fetal echocardiography

fetal echocardiography
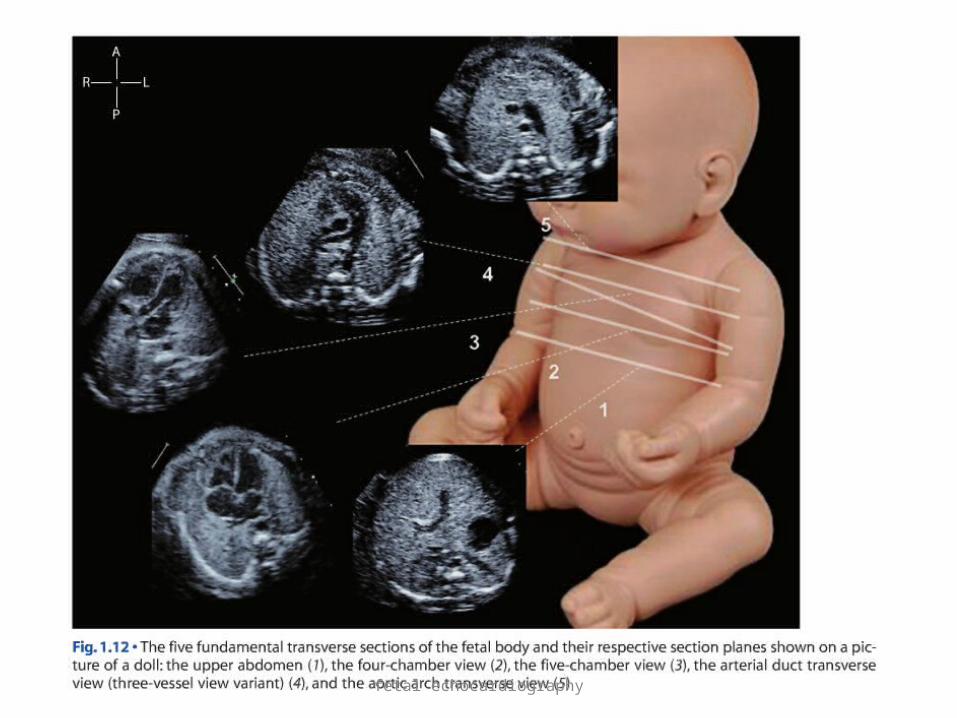
Echocardiographic projections
• Transverse views of fetal heart• Four chamber view• Five chamber view• Three vessel view• Arterial ductal transverse view• Aortic arch transverse view
fetal echocardiography

fetal echocardiography
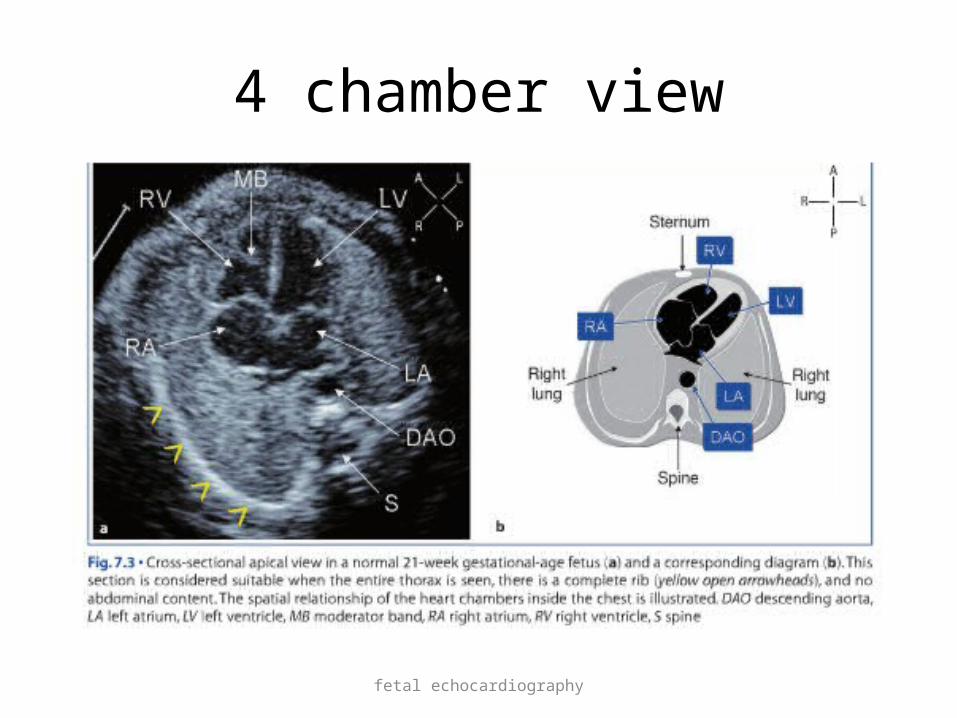
Four chamber view
• Obtained from transverse plane of upper abdo men by tracing IVC to RA and then cranial angulation give 4 chamber view
• RV is more anterior with blunted apex• LV is posterior with ellipsoidal shape• LA most posterior and close to spine and
descending aorta
fetal echocardiography
• Four chamber view:Symmetry of chambers Atrial Septum and PFO Ventricular Septum Atrioventricular Valves Ventricular functionRhythm abnormalities
fetal echocardiography
4 chamber view

fetal echocardiography

fetal echocardiography
• Abnormalities of four-chamber anatomy may characterize certain forms of congenital heart disease
• In many cases, the primary structural abnormality of the heart may be apparent in the view of the central fibrous body. Such defects may include Complete atrioventricular septal (canal) defect, Hypoplastic left heart syndrome, Hypoplastic right heart syndrome, Ebstein malformation of the tricuspid valve, and Various forms of single ventricle

fetal echocardiography
4chamber
fetal echocardiography
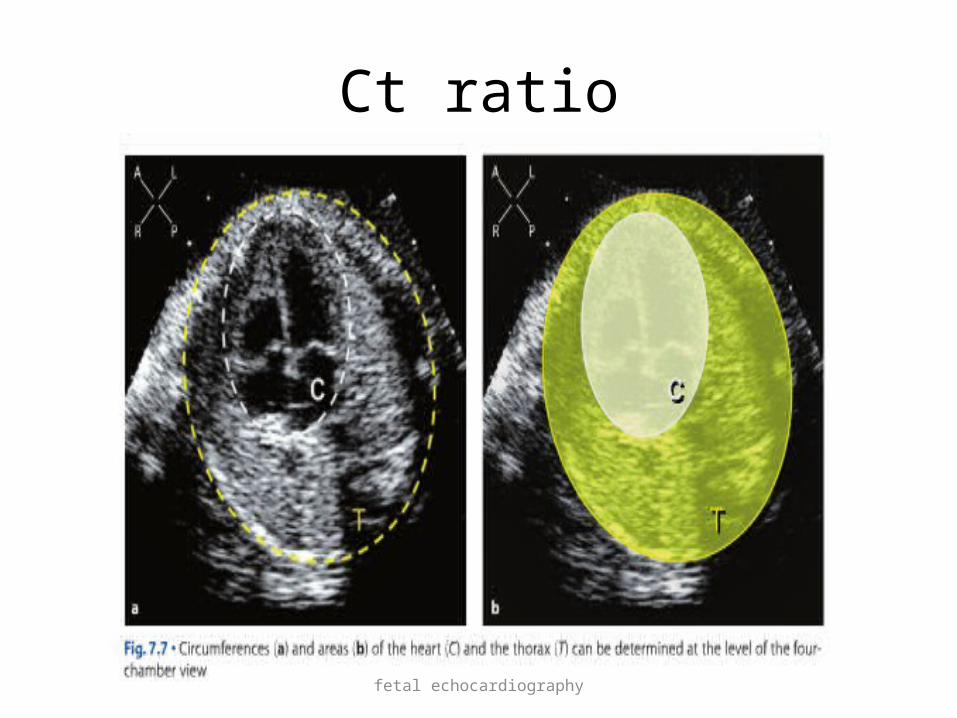
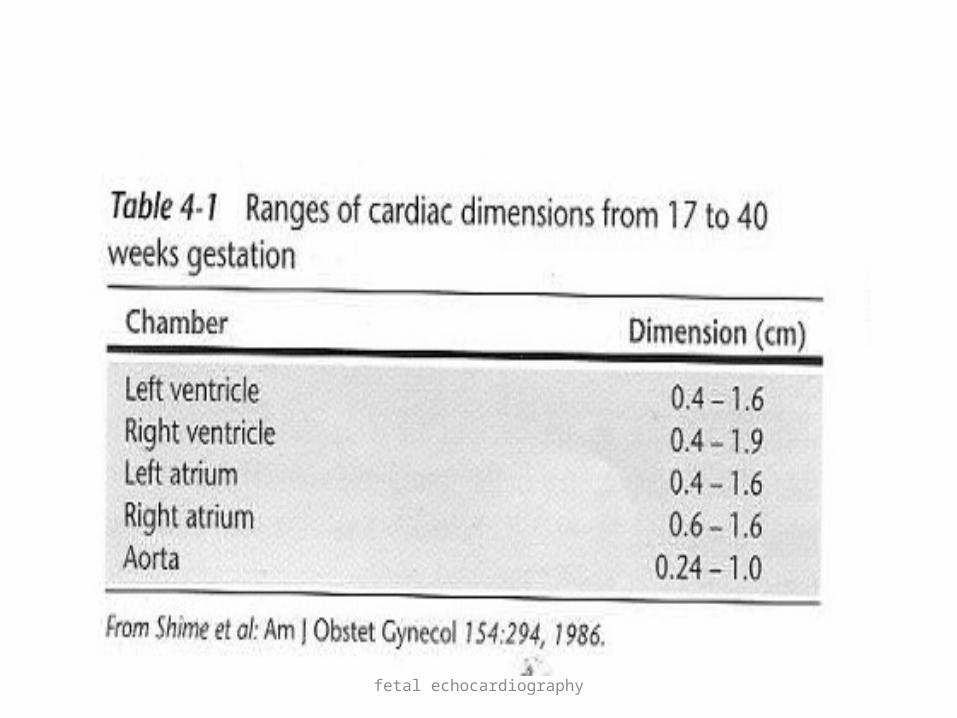
• Dimensions of heart• CT circumference ratio normal– mean value of 0.45at 17 weeks and
0.50 at term• CT area ratio normal 0.25-0.35 throughout pregnancy
fetal echocardiography
Ct ratio
fetal echocardiography
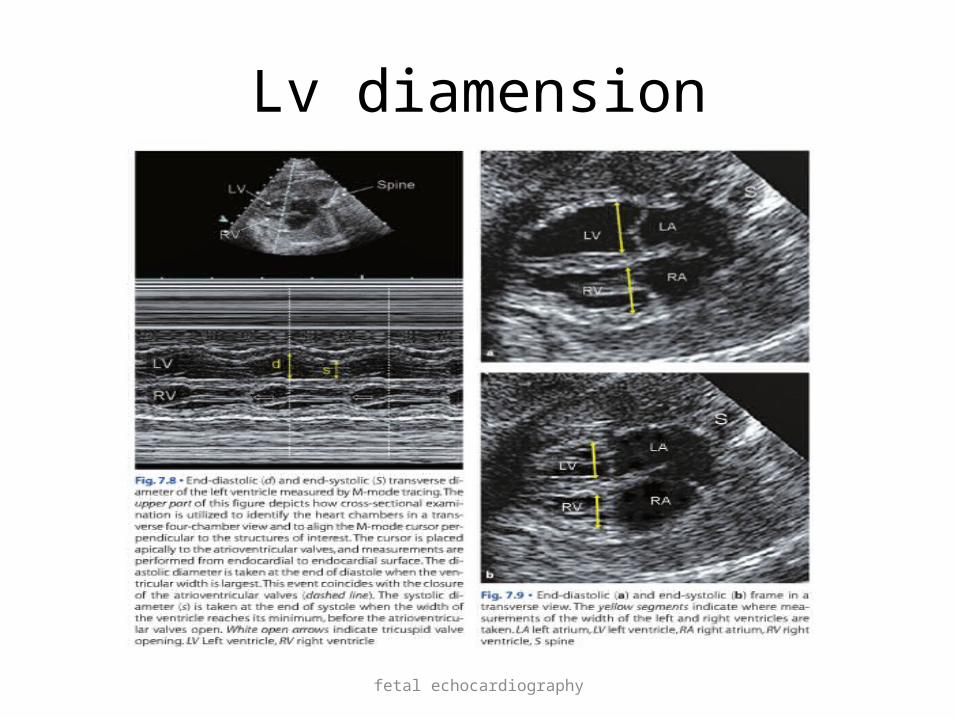
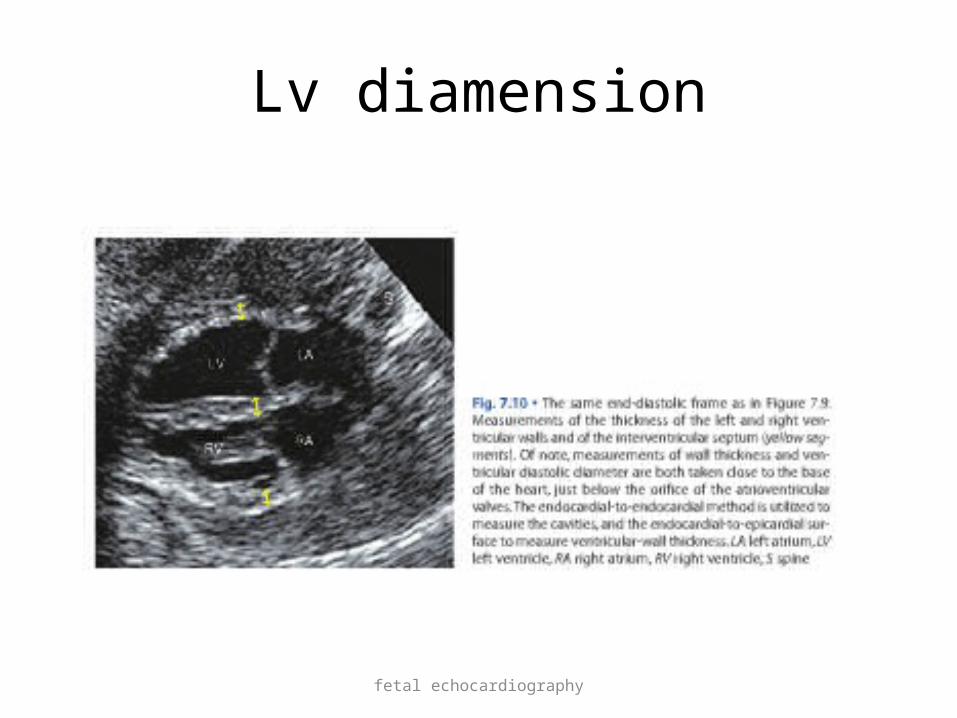
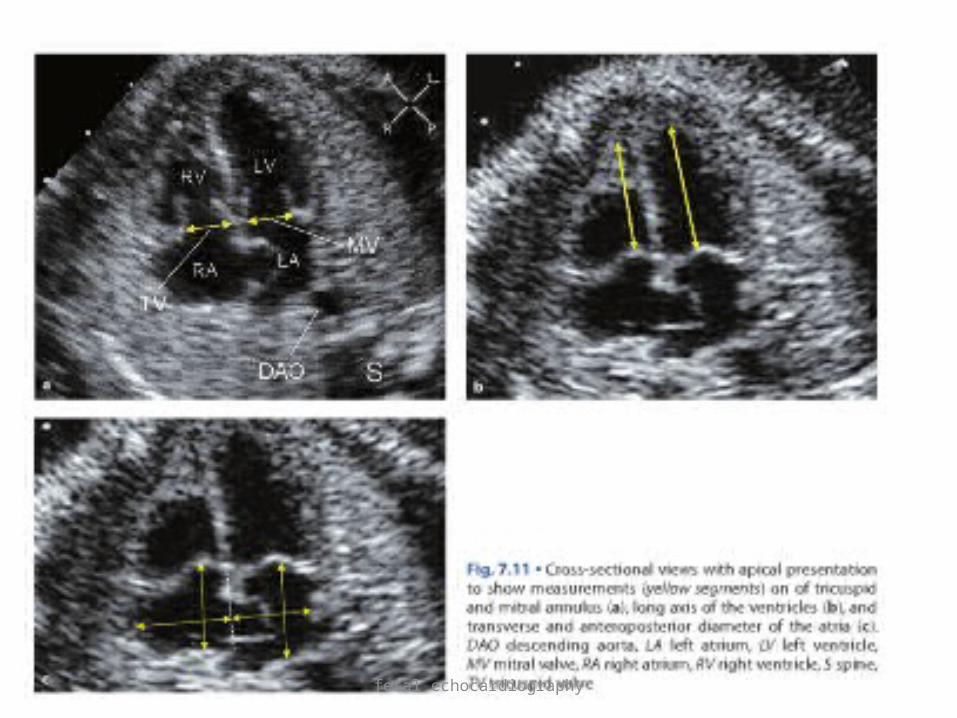
• Measurement• Fractionalshortening= (EDD-ESD)/EDD Normal value 34%• End systolic and diastolic transverse diameters
of ventricles• Thickness of IVS,LV,RV• LA volume• Mitral & tricuspid annulus diameter
fetal echocardiography
Lv diamension
fetal echocardiography
Lv diamension
fetal echocardiography
fetal echocardiography
fetal echocardiography
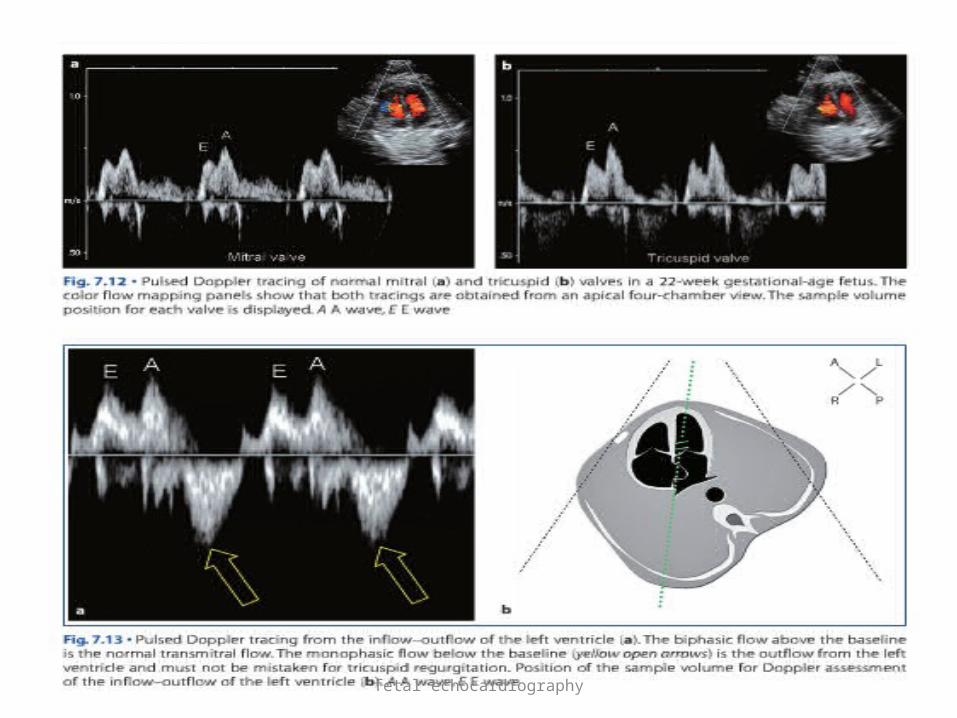
• Normal Doppler flow profile of tricuspid and mitral valve :
• Similar • Diastolic pattern with 2 peaks E and A• 2 peaks merge with each other when heart
rate > 160-170 beats/min• No backflow into atria during systole

fetal echocardiography
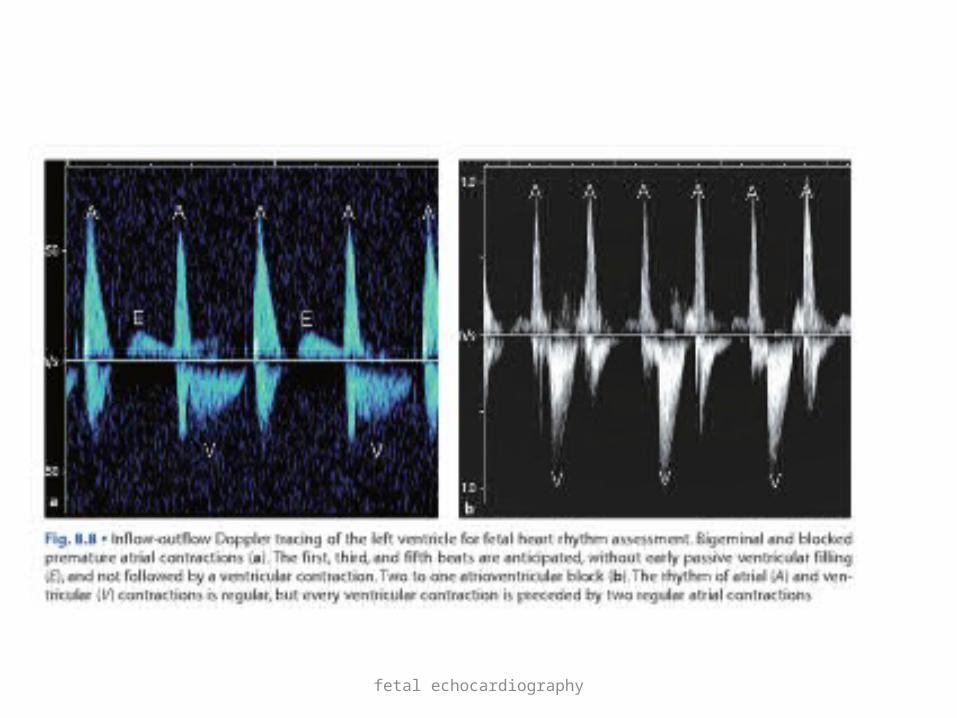
• E wave is smaller than A wave due to reduced fetal ventricular compliance so ventricular filling depend on regular atrial contraction( loss of sinus rhythm lead to fetal cardiac compromise)
• E wave increases throughout gestation with valu of 25cm/s at 16wks to 45cm/s at term for mitral valve and 30cm/s and 50cm/s for tricuspid valve
• A is relatively constant during gestation with 45cm/s for mitral and 50cm/s for tricuspid
• E/A ratio 0.5 at 16wks and 1 near term
fetal echocardiography
fetal echocardiography
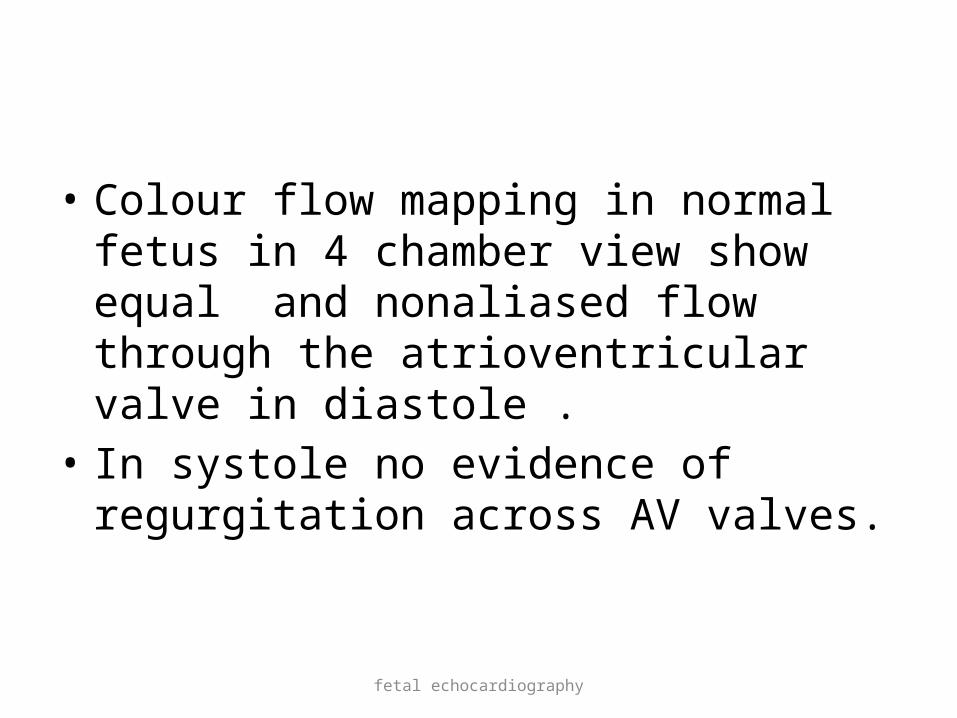
• Colour flow mapping in normal fetus in 4 chamber view show equal and nonaliased flow through the atrioventricular valve in diastole .
• In systole no evidence of regurgitation across AV valves.
fetal echocardiography
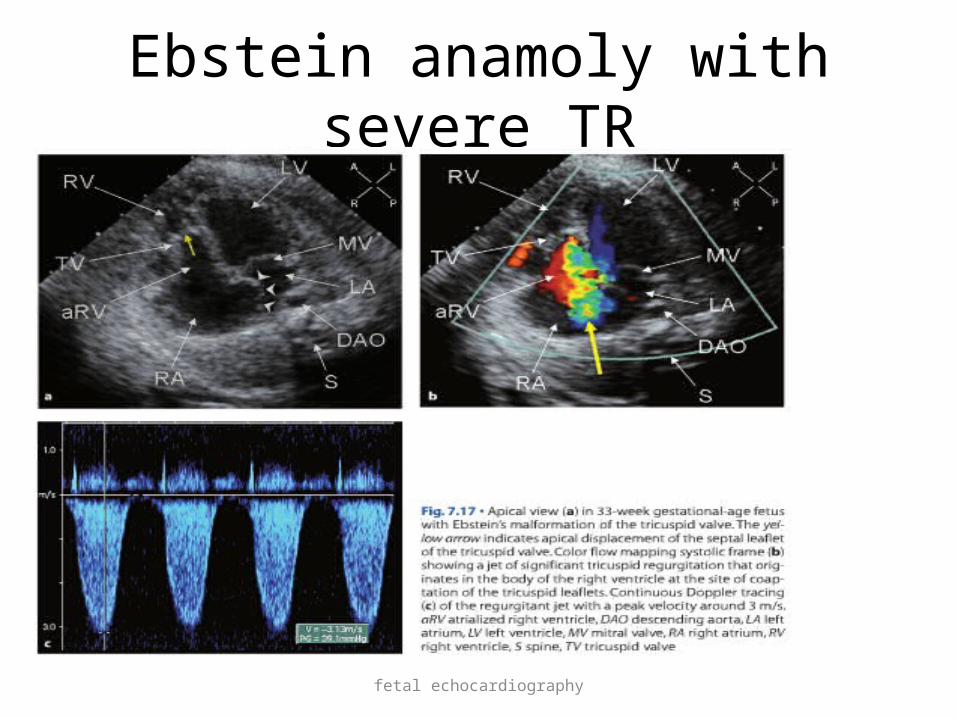
Ebstein anamoly with severe TR

fetal echocardiography
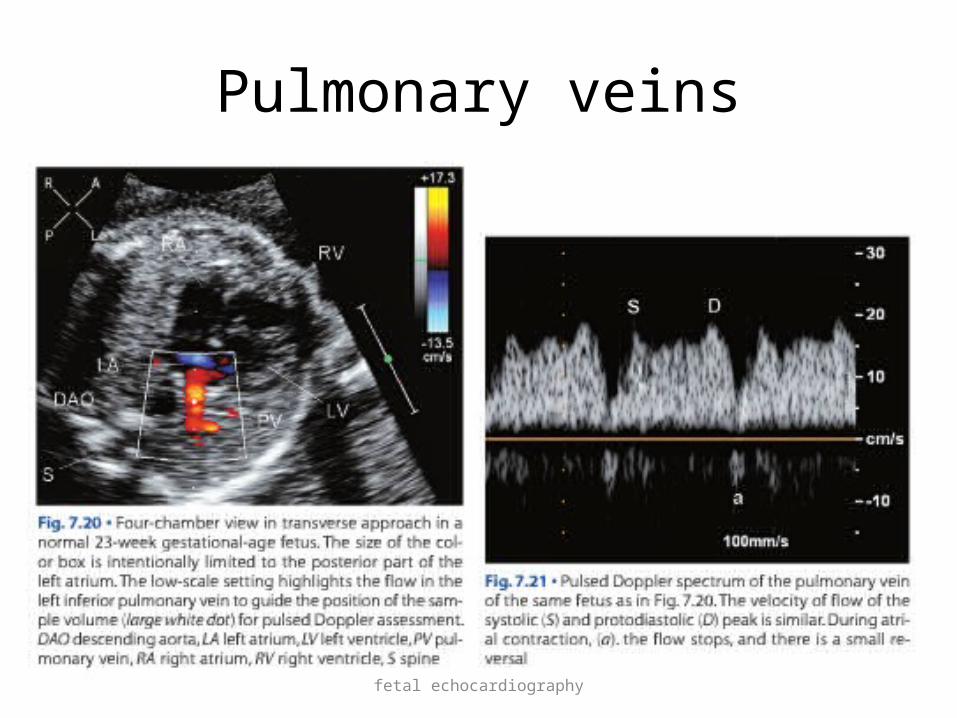
• Colour flow mapping of pulmonary veins reflects variation in pressure in LA
• Systolic peak slightly higher than diastolic peak with small atrial reversal
fetal echocardiography
Pulmonary veins

fetal echocardiography
• Cardiac rhythm• By M-mode and pulse wave doppler• M-mode method: atrial and ventricular wall
moventment is recorded at same time in sinus rhythm atrial contraction preced
ventricular contractionBy PW doppler: by inflow and outflow pulse
doppler of LV

fetal echocardiography
Cardiac rhythm
fetal echocardiography

fetal echocardiography
5 chamber view
• With cranial angulation from 4 chamber view give 5 chamber view
Structures seen are• Aortic valve and its root• Inflow ,trabecular and outflow of LV• LA and RA• Trabecular part of RV• Two pulmonary veins • SVC

fetal echocardiography
5 chamber view
fetal echocardiography
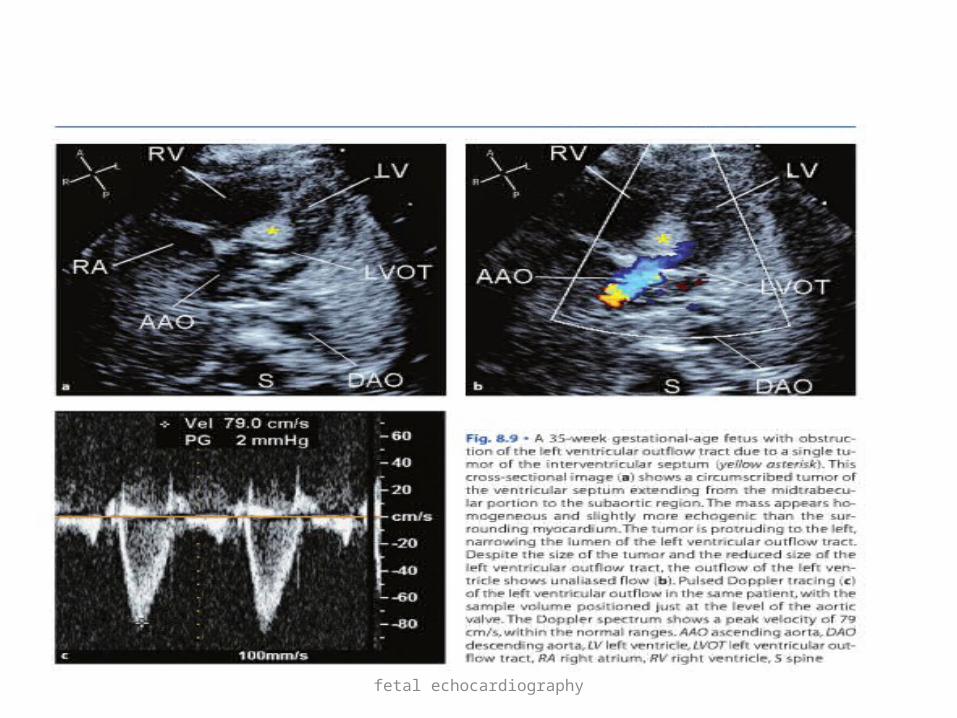
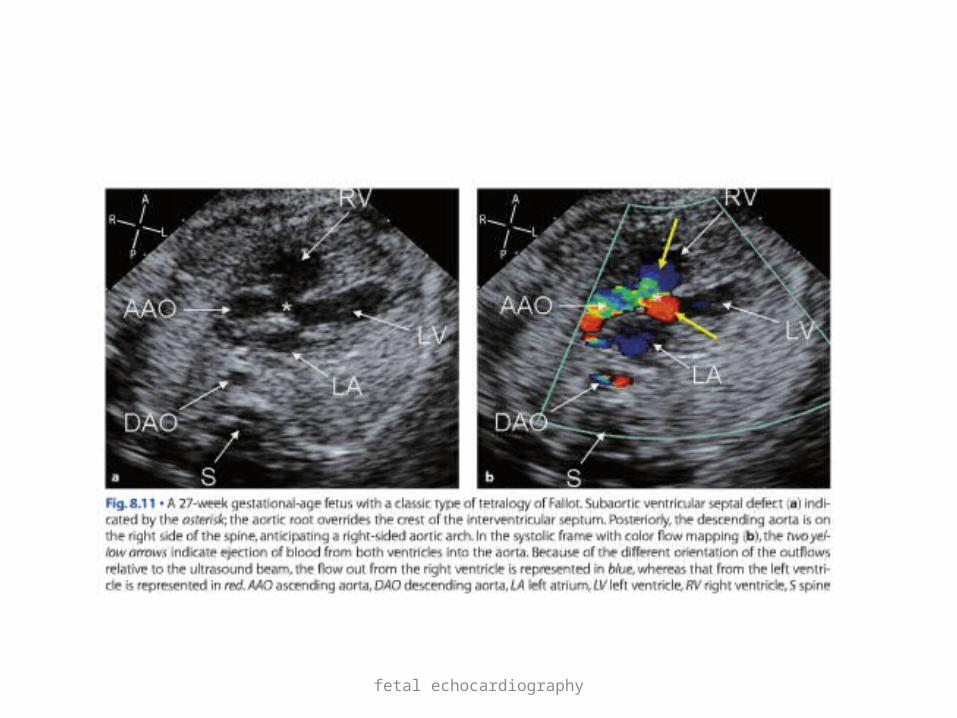
Useful to assess• Heart rhythm• LV outflow tract obstructions• Subaortic VSD
fetal echocardiography
fetal echocardiography

fetal echocardiography
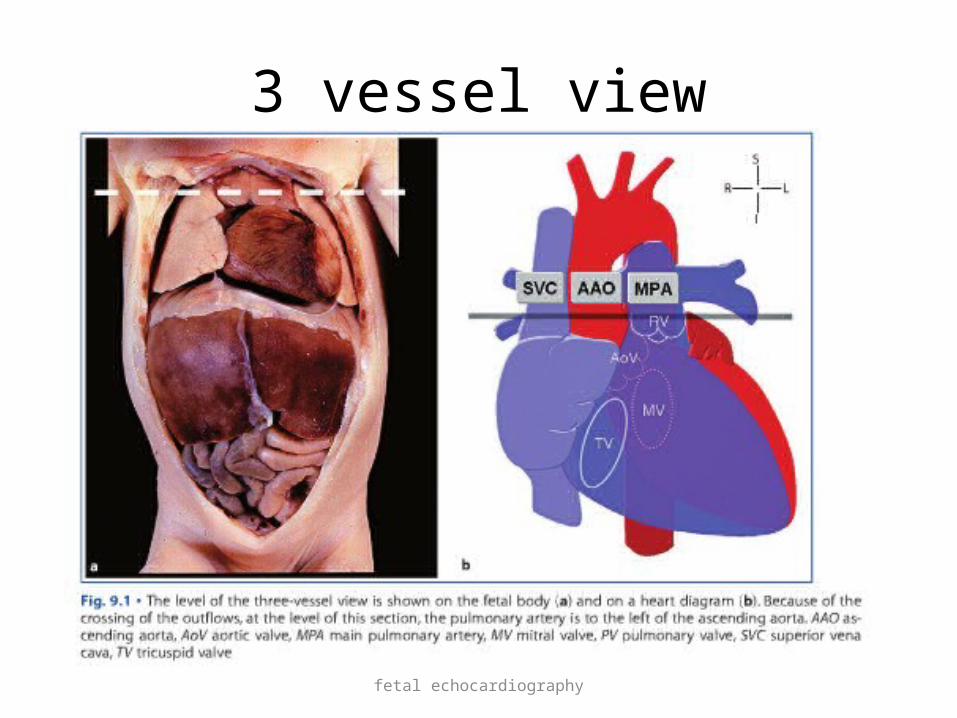
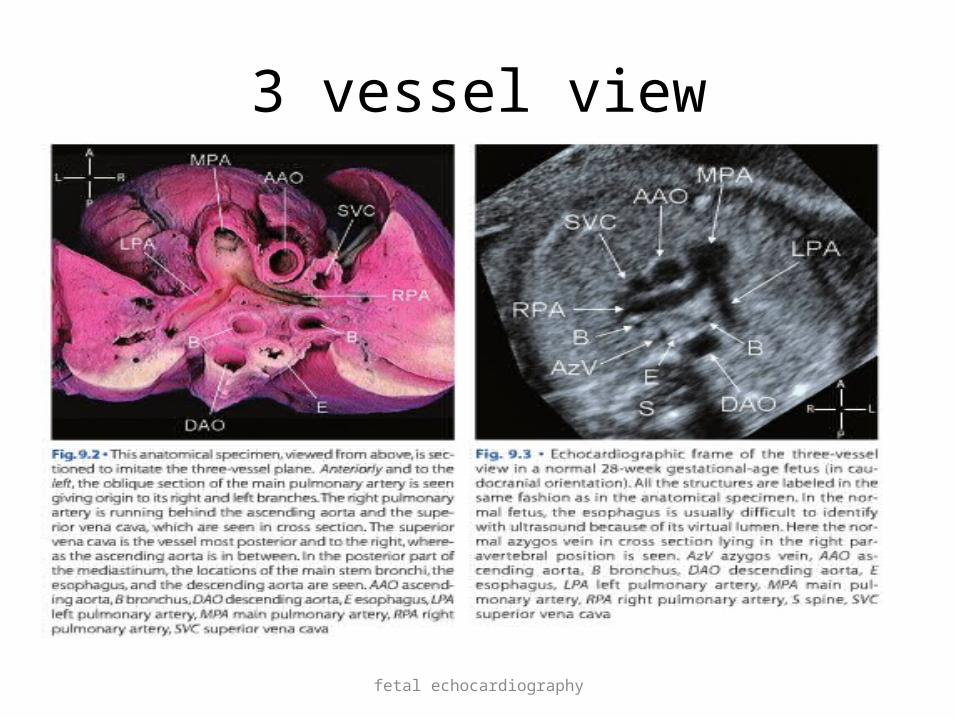
3 vessel view
• Obtained by sliding the scanning plane cephalad from four chamber view towards fetal upper mediastinum
• Significant lesions in ventricular outflow tracts show abnormal 3 vessel view
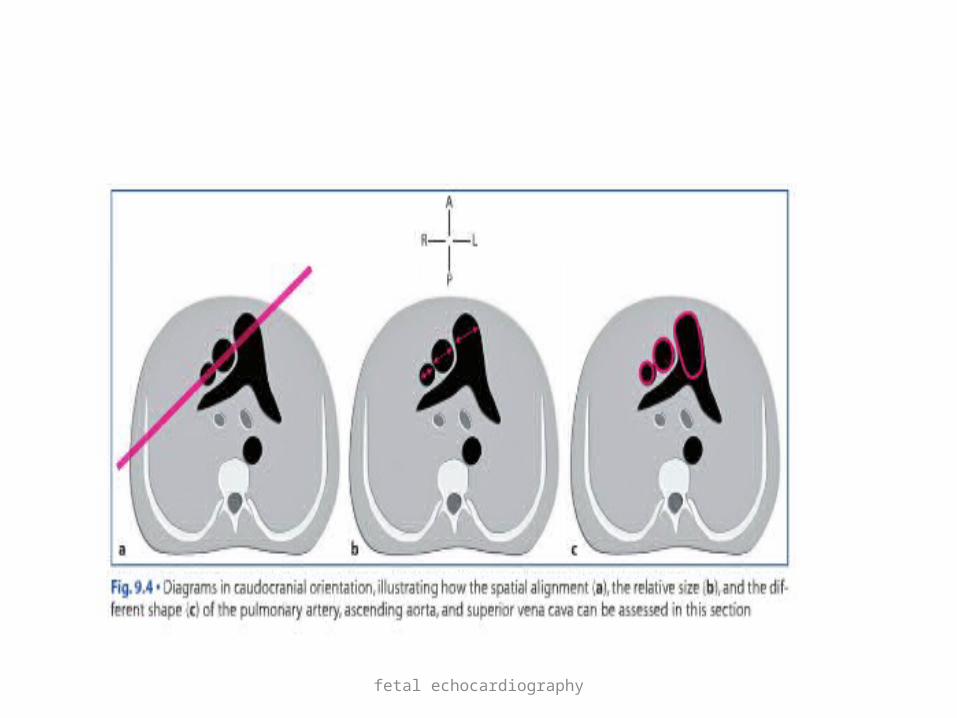
• Normally:• Pulmonary trunk is largest and anterior and left• SVC is smallest and posterior and right• Aorta is in between two• Show oblique axis of PA and short axis of aorta and
SVC
fetal echocardiography
3 vessel view
fetal echocardiography
3 vessel view
fetal echocardiography
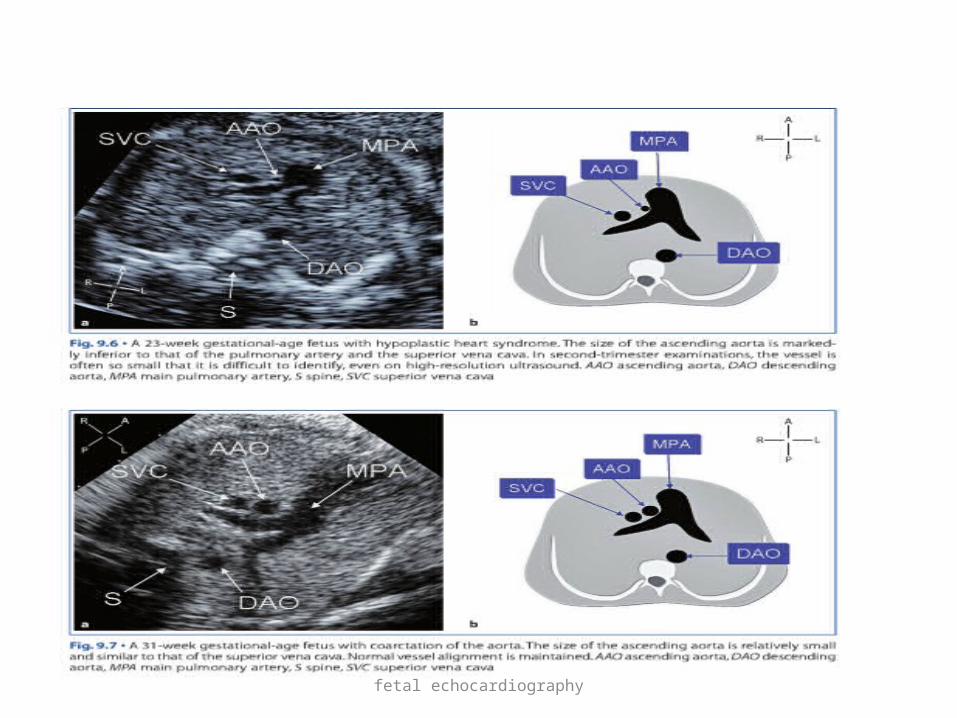
• Ascending aorta is defined as small if its diameter is equal or smaller than SVC diameter
• Pulmonary artery is defined as small if its diameter is equal or smaller than aorta diameter
fetal echocardiography
fetal echocardiography
• 3 vessel view abnormalities :• Abnormal vessel size(HLHS)• Abnormal vessel alignment(subrterial VSD)• Abnormal arrangment(TGA)
fetal echocardiography
fetal echocardiography
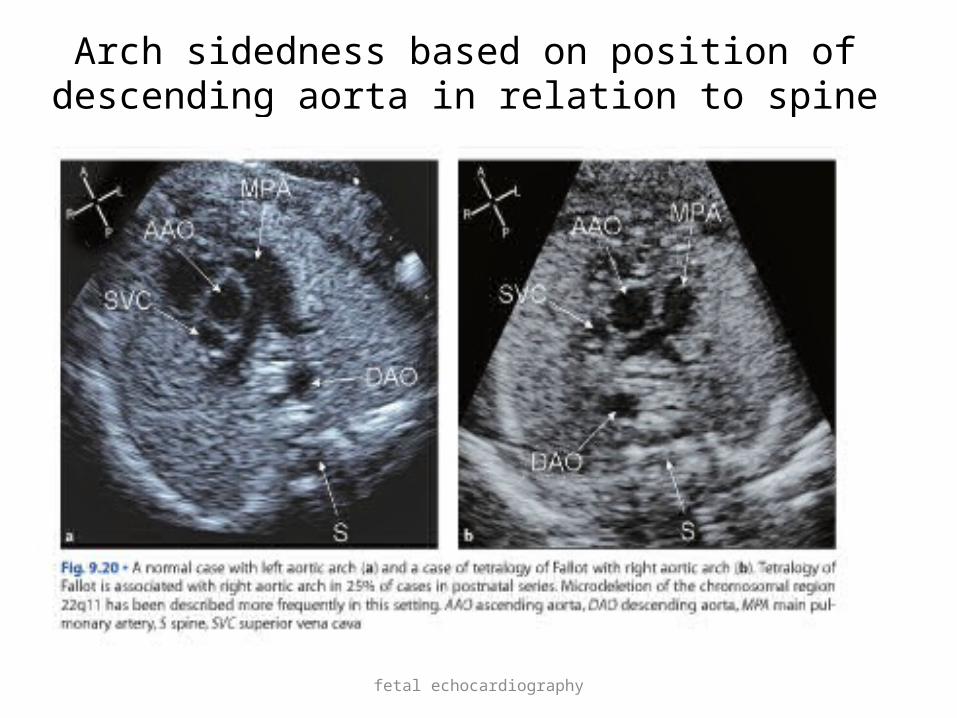
Arch sidedness based on position of descending aorta in relation to spine

fetal echocardiography
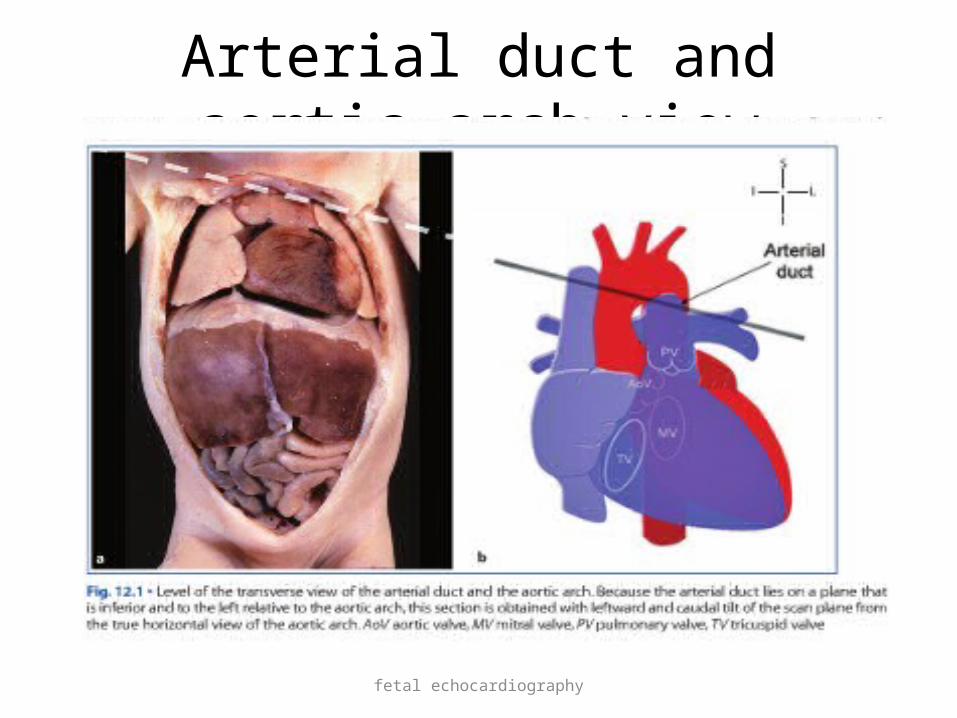
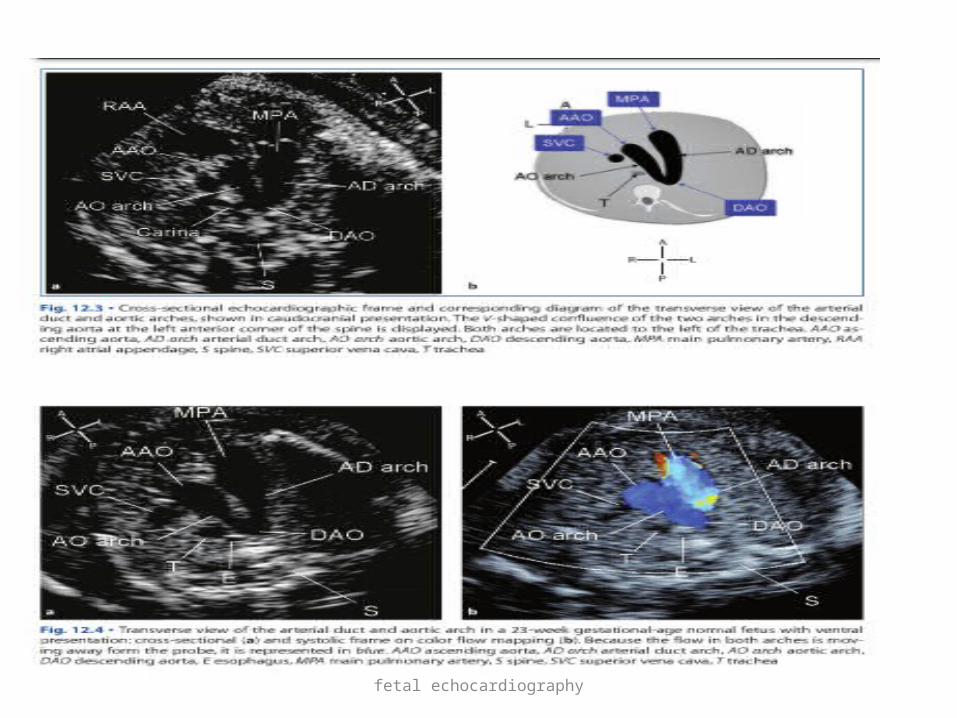
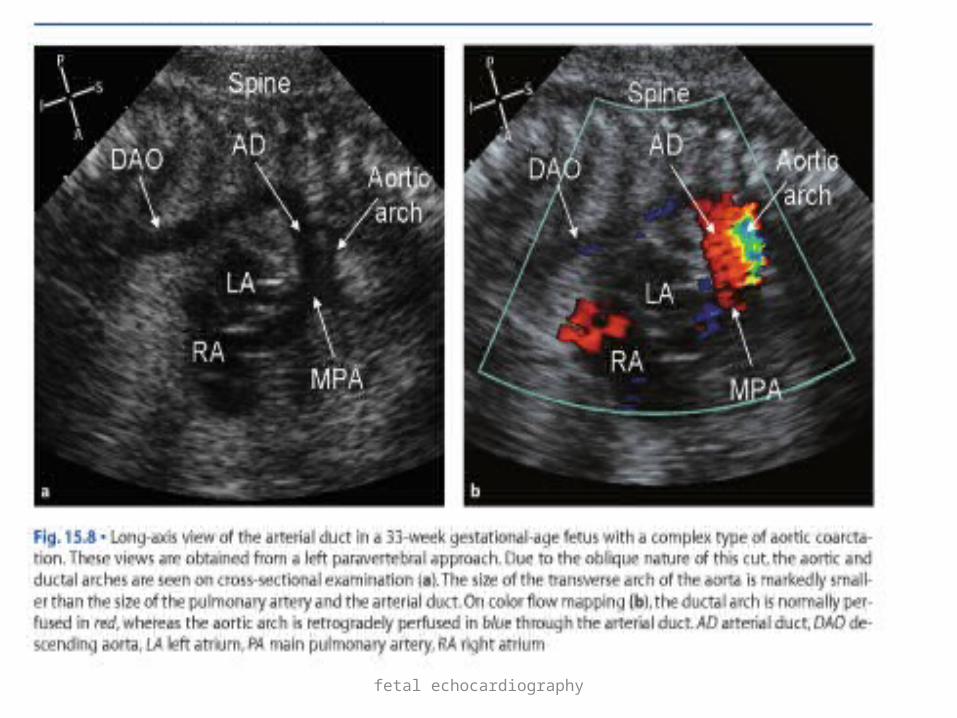
Arterial duct and aortic arch transverse view
• From transverse view of aortic arch slight caudal angulation to the left ,visualise arterial duct and aortic arch
Normal morphology• Aortic and ductal arches merges together into
descending aorta • Ductal arch larger than aortic isthmus and
both lie on left side
fetal echocardiography
Arterial duct and aortic arch view
fetal echocardiography
fetal echocardiography
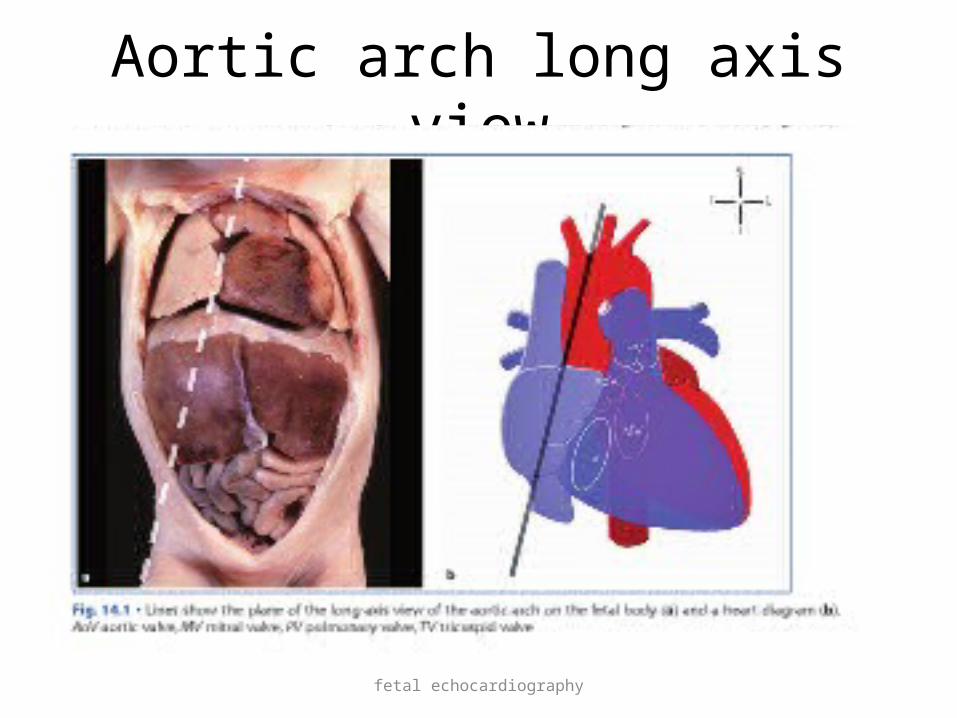
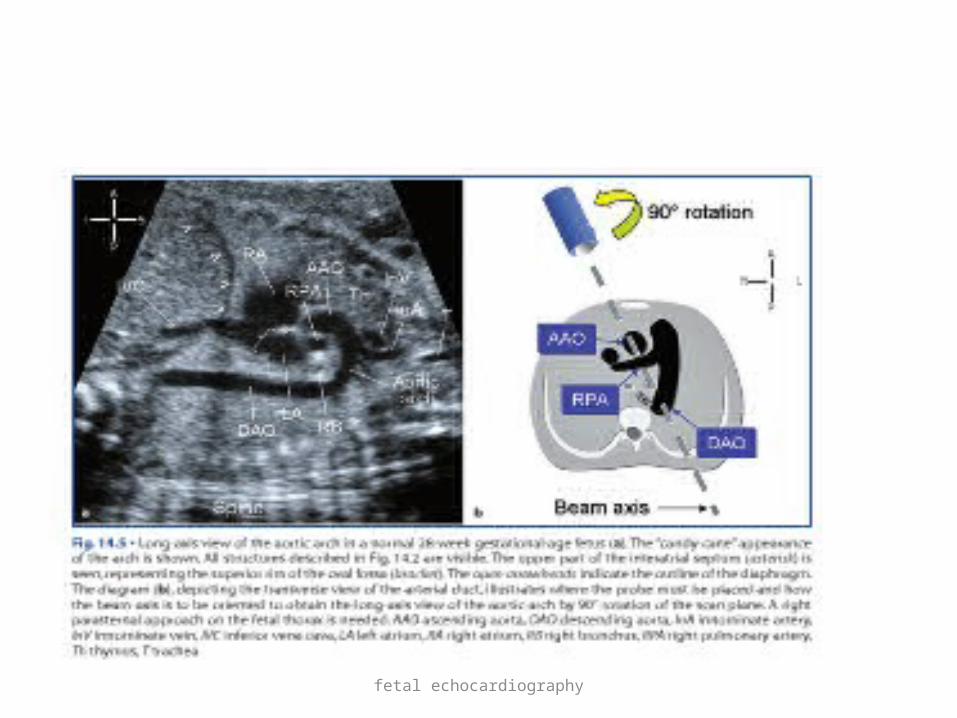
Aortic arch long axis view
• This view is obtained by parasagital plane with angulation from right of sternum to left shoulder
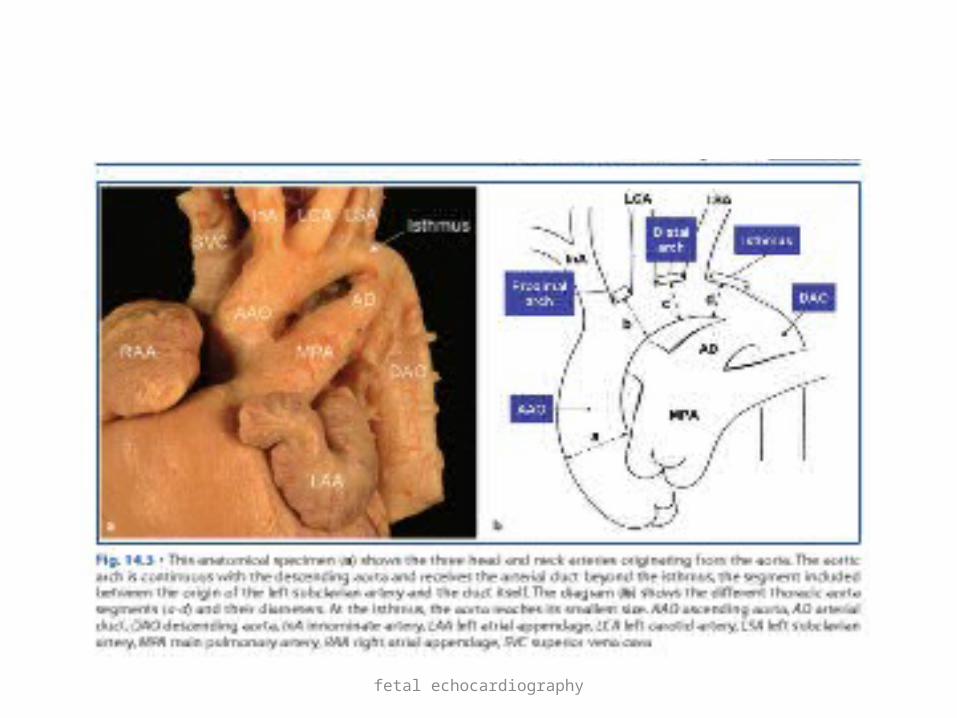
Normal morphology• Aortic arch in long axis(candy cane appearence)• Cross section of RPA • Isthmus is aortic segment between left
subclavian and aortic end of arterial duct
fetal echocardiography
Aortic arch long axis view
fetal echocardiography
fetal echocardiography

fetal echocardiography
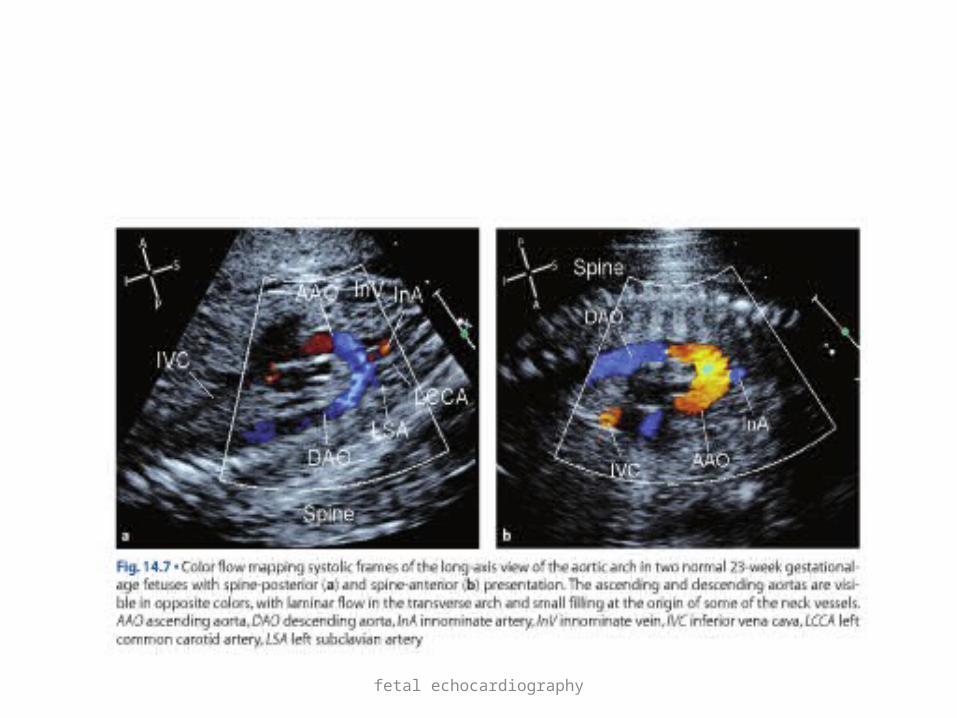
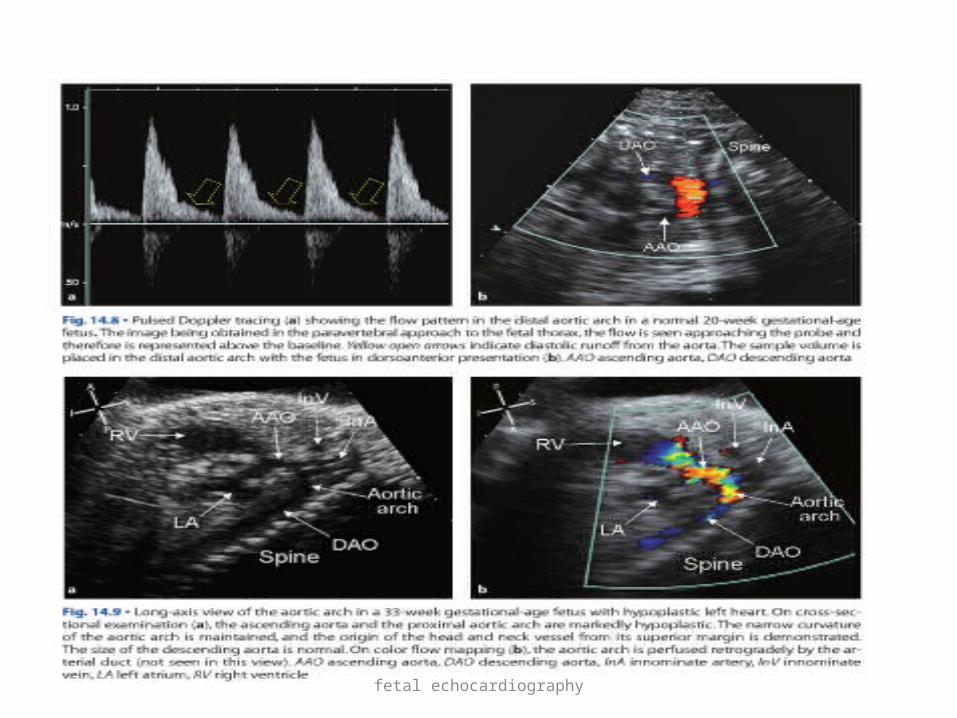
colour flow mapping across aortic archFlow in aortic arch changes direction by 180* so
different segments of aorta are represented in opposite colours
Doppler spectrum is monophasic wave but with a diastolic forward flow due to diastolic recoil of aortic ach and low placental resistance
fetal echocardiography
fetal echocardiography
fetal echocardiography
Arterial duct long axis view
• This view is obtained by parasagital plane with angulation from left of sternum to left shoulder
Normal morphology• The section show superiorly the main PA
which split into inferior branch (left PA) and superior branch(arterial duct)

fetal echocardiography
Ductal view
fetal echocardiography
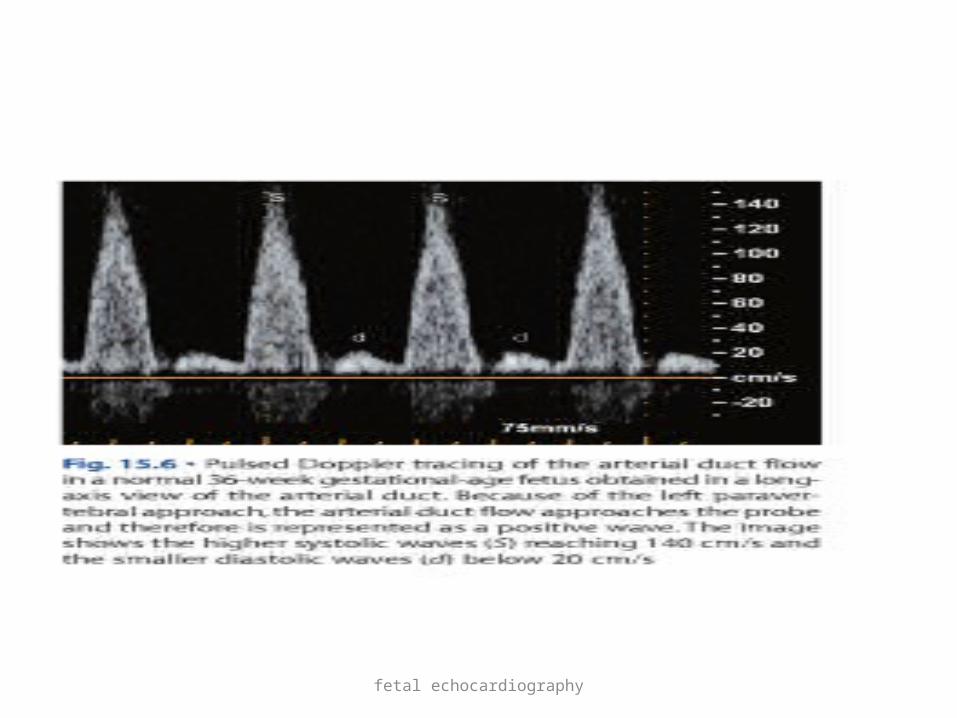
• Arterial ductal flow assessment by pulse wave doppler
• Systolic anterograde flow < 50cm/s at 6 wks to 130-160cm/s at end of pregnancy
• Diastolic peak velocity 0 at early pregnancy to 30-40cm/s near term
• Diastolic wave is due to rebound of energy potentially stored by walls of main PA which produces further flow from PA to aorta
fetal echocardiography
fetal echocardiography
fetal echocardiography
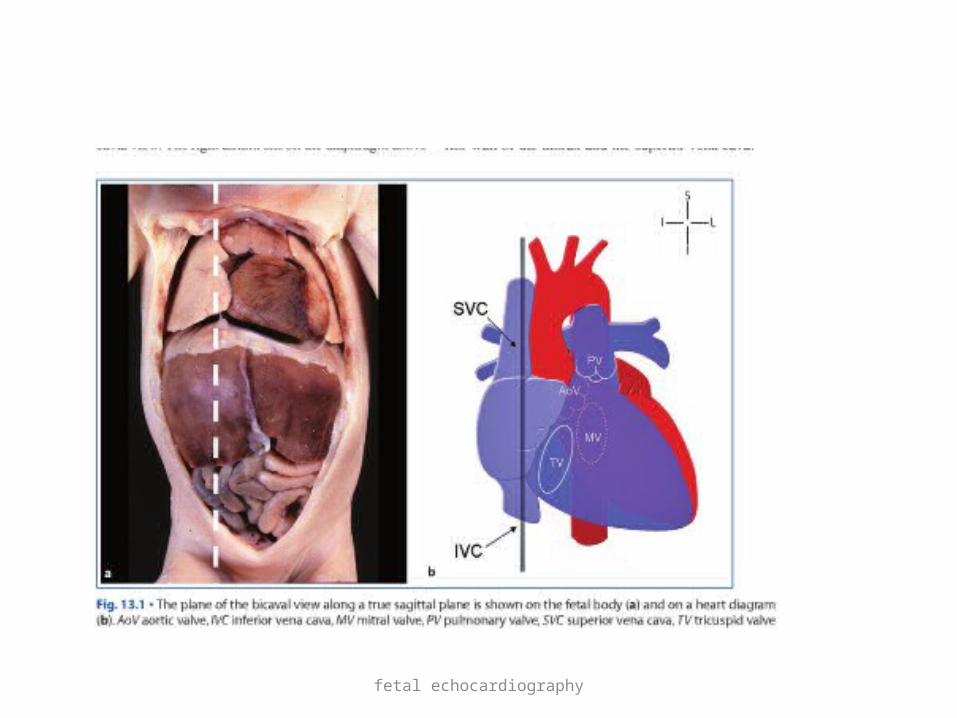
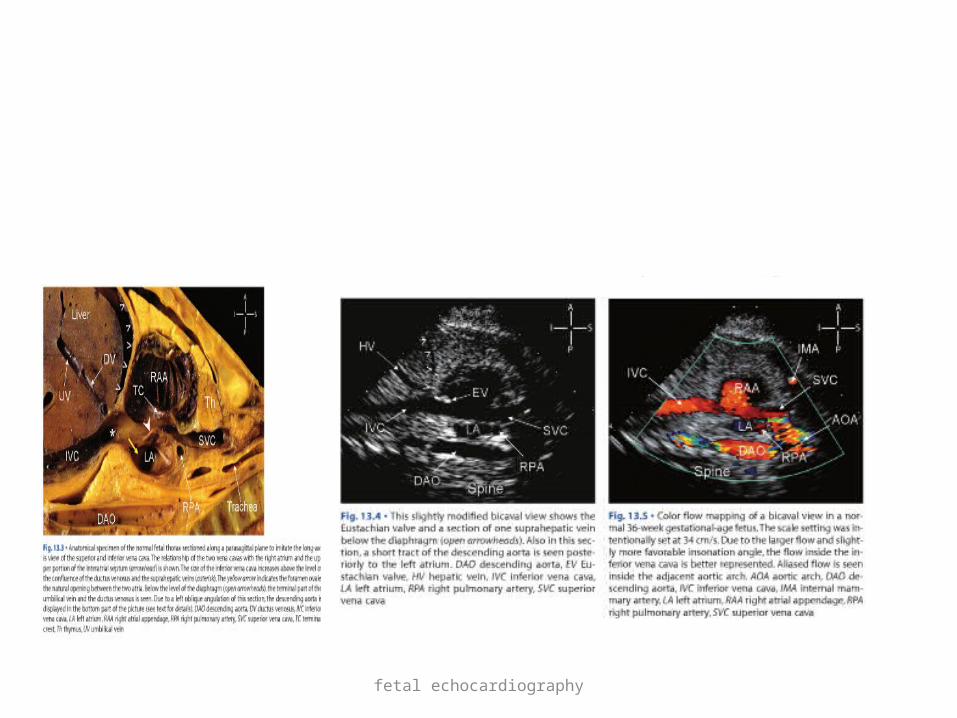
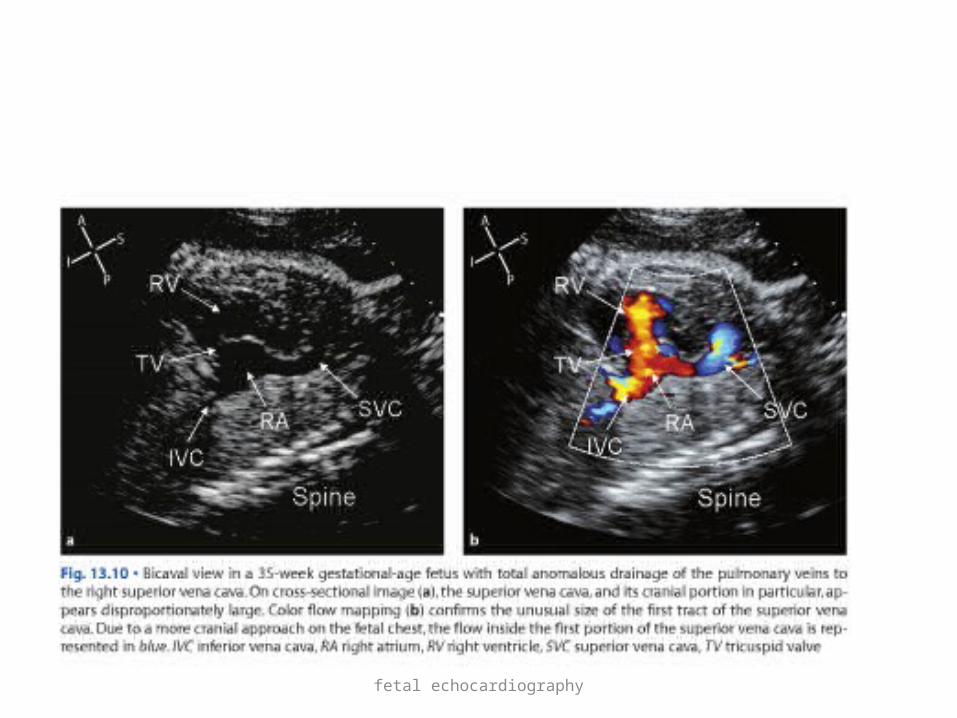
Bicaval view
• Obtained by orienting the scan plane along the true sagittal plane of fetal body immediately to right of midline
Normal morphology• Longitudinal section of SVC and IVC• RA and RAA• Cross section of RPA
fetal echocardiography
fetal echocardiography
fetal echocardiography
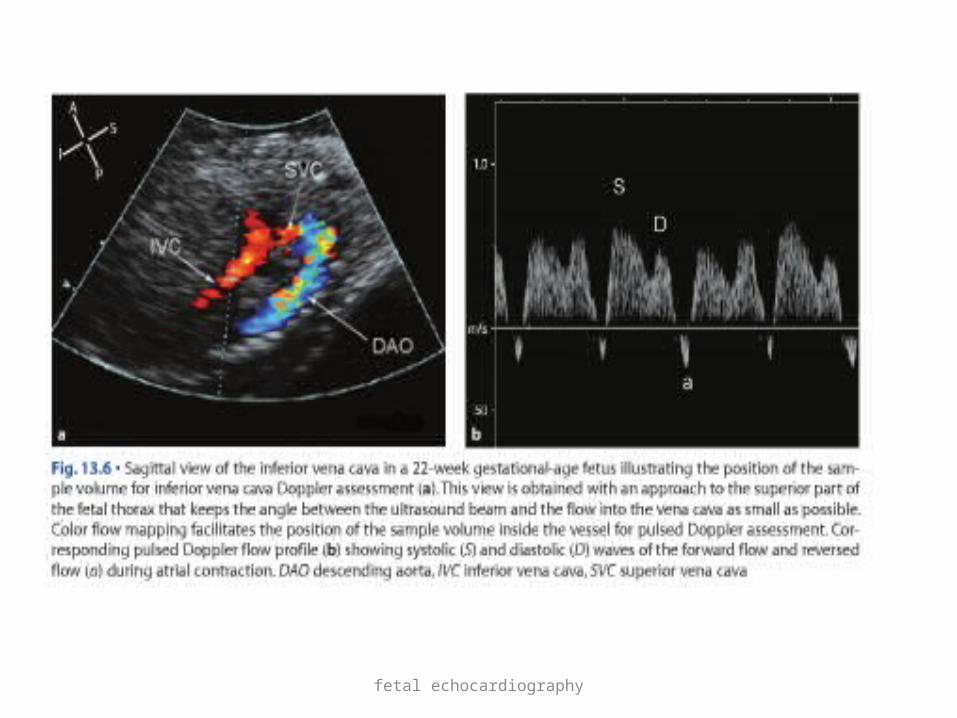
• Caval flow • S wave –due to atrial suction produced by movement
of tricuspid valve plane in an base to apex direction during ventricular systole
• D wave—in early diastole ,correspond to reduction in atrial pressure due to AV valve opening
• A wave –retrograde wave in late diastole due to atrial contraction
• ratio between peak s and peak d wave is constant with value of 1.8 + 0.2 through out gestation
fetal echocardiography
fetal echocardiography
fetal echocardiography
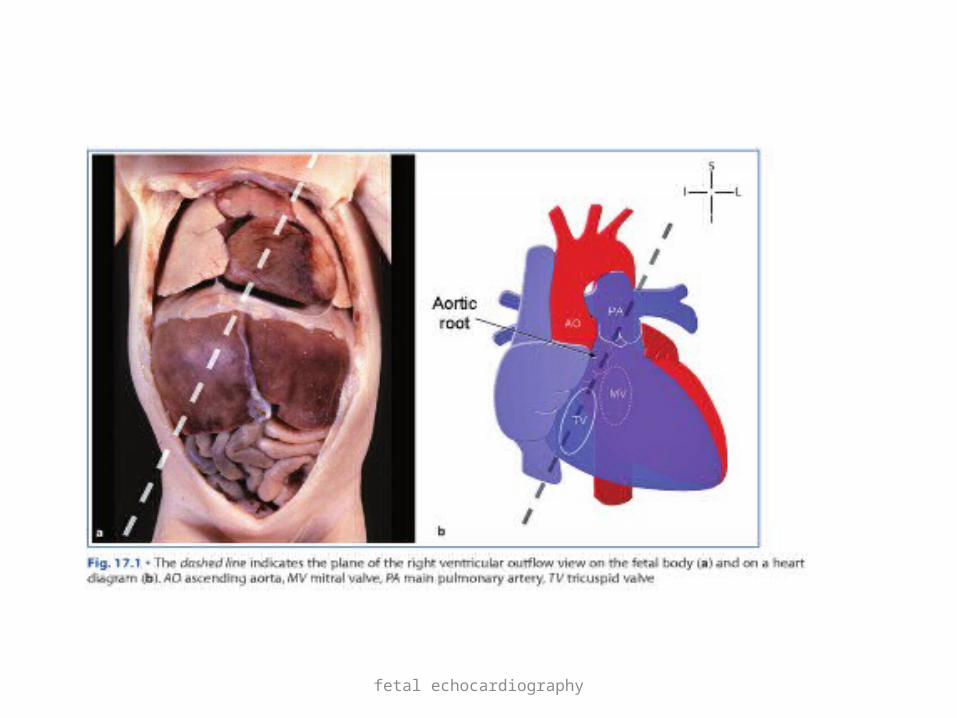
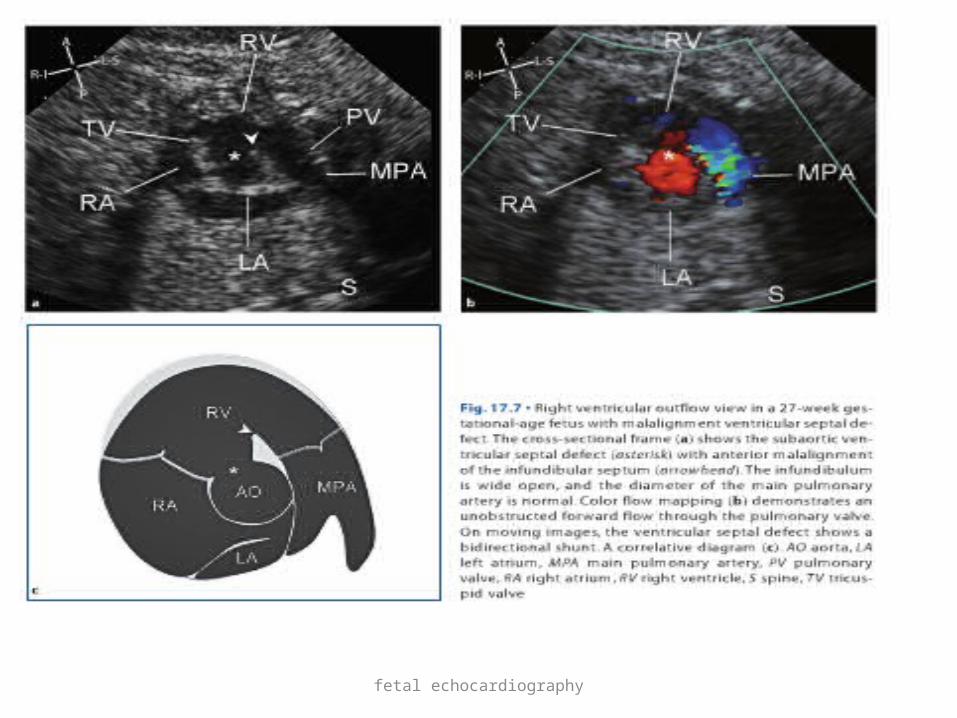
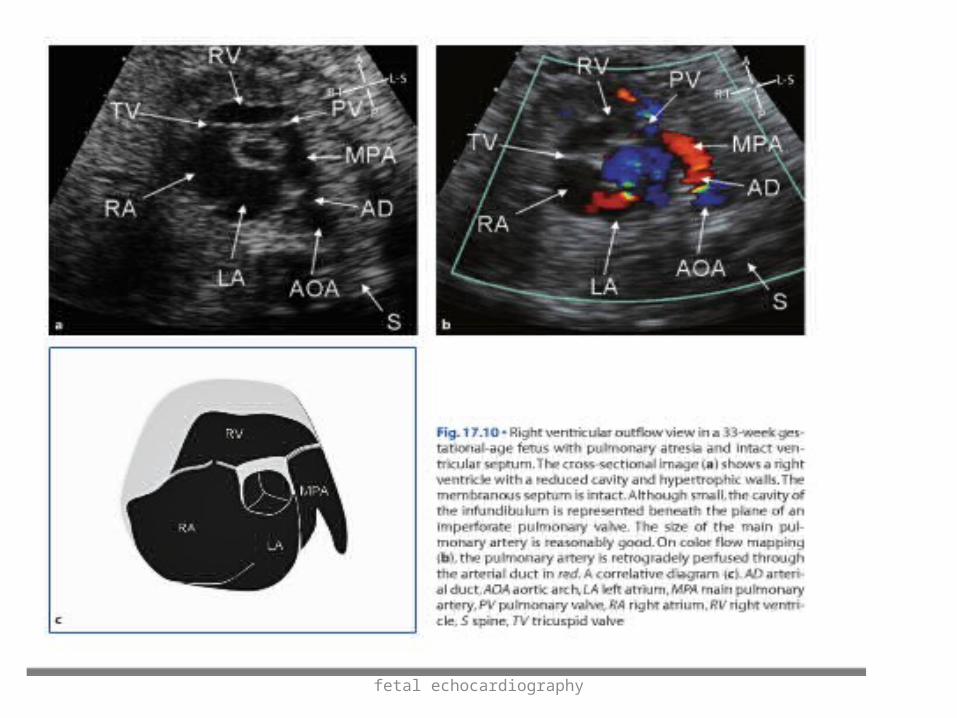
RV outflow view
• Slight left side rotation from sagittal plane (from right hypochondrium to left shoulder)
Normal morphology• Structures of right heart and crossection of
aortic root
fetal echocardiography

fetal echocardiography
fetal echocardiography
fetal echocardiography
fetal echocardiography
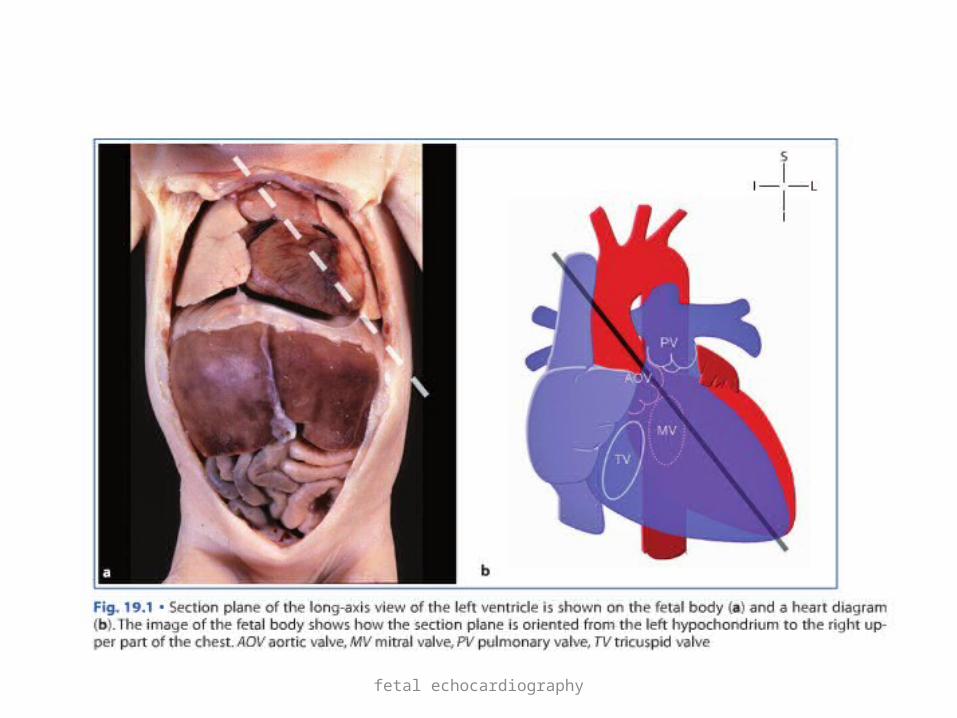
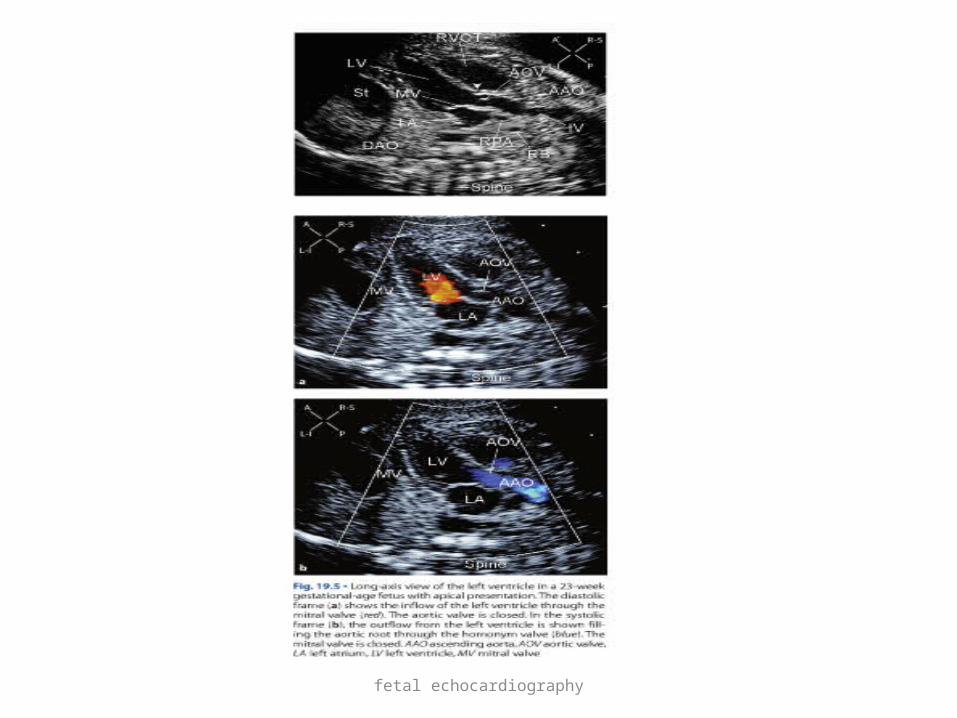
LV long axis view
• Plane that runs from left hypochondrium to right shoulder
• Obtained by rotating transducer 90* from apical 4 chamber view and tilting towards right shoulder
• Useful in assessing inlet and outlet portions of LV• Subarterial and anterior muscular VSD can be
seen• Aortic override can be assessed in subortic vsd
fetal echocardiography
fetal echocardiography

fetal echocardiography

fetal echocardiography
Pitfalls
• Some lesions such as minor VSDs may be missed.• Progressive defects, such as a bicuspid aortic
valve, may not be diagnosed at 18–20 weeks of gestation.
• Outflow tract anomalies may be missed.• Maternal habitus and fetal lie may be limitations.• Visualization of details may not be possible
before 18 weeks.
fetal echocardiography
Conclusion
• It may be difficult or time consuming to perform a dedicated fetal echocardiogram on all patients.
• Four-chamber view, the outflow tracts, and the three-vessel view would be sufficient to diagnose 80–85% of cardiac anomalies.

fetal echocardiography
Thank u