Embed Size (px)
Citation preview

7/14/20117/14/2011
11
Advances in Fetal Advances in Fetal EchocardiographyEchocardiographyLuísLuís F. F. GonçalvesGonçalves, M.D., M.D.Oakland University William Beaumont School of Medicine, Rochester MIOakland University William Beaumont School of Medicine, Rochester MI
Division of Fetal Imaging, William Beaumont Hospital, Royal Oak, MIDivision of Fetal Imaging, William Beaumont Hospital, Royal Oak, MI
Fetal Echocardiography for Prenatal DiagnosisFetal Echocardiography for Prenatal Diagnosis
Authored by Drs. XinAuthored by Drs. Xin--Fang WANG and JiFang WANG and Ji--Peng XiauPeng Xiau
Wuhan Medical College, now Tongji Medical College, Wuhan Medical College, now Tongji Medical College, Huazhong University of Science & Technology, Wuhan, Huazhong University of Science & Technology, Wuhan, Central ChinaCentral China
140 women / 147 fetuses examined w/ M140 women / 147 fetuses examined w/ M--Mode Mode
Study describes a technique for diagnosis of early Study describes a technique for diagnosis of early pregnancy, observation of fetal heart and estimation of pregnancy, observation of fetal heart and estimation of fetal cardiac sizefetal cardiac size
Kleinman CS et al. Pediatrics 1980;65: 1059Kleinman CS et al. Pediatrics 1980;65: 1059--10681068

7/14/20117/14/2011
22
Sahn DJ et al. Circulation 1980;62:588Sahn DJ et al. Circulation 1980;62:588--597597 Sahn DJ et al. Circulation 1980;62:588Sahn DJ et al. Circulation 1980;62:588--597597
Sahn DJ et al. Circulation 1980;62:588Sahn DJ et al. Circulation 1980;62:588--597597
Yonouszai Ak et al. J Am Soci Echo 2008;21:470Yonouszai Ak et al. J Am Soci Echo 2008;21:470--88
velocityvelocity
Yonouszai Ak et al. J Am Soci Echo 2008;21:470Yonouszai Ak et al. J Am Soci Echo 2008;21:470--88
strainstrain
strain ratestrain rate

7/14/20117/14/2011
33
3D and 4D Evaluation of the 3D and 4D Evaluation of the Fetal HeartFetal Heart
Adult Aortic Valve Adult Aortic Valve –– 3D3D
Image from the Tomtech Website Image from the Tomtech Website -- GermanyGermany
PP
QRSQRS
TT PP
QRSQRS
TT
GatingGating
11 22 33 4 …4 … …n…n 11 22 33 44 Image Image numbernumber
Trigger Trigger pulsepulse
TimeTime
3D Heart Acquisition 3D Heart Acquisition No GatingNo Gating
Temporal Fourier Analysis of Temporal Fourier Analysis of the Periodic Cardiac Motionthe Periodic Cardiac Motion
ROIROIMagnitudeMagnitude
displaydisplay
Nelson et al. Med Phys 1995;22:973; JUM 1996;15:1Nelson et al. Med Phys 1995;22:973; JUM 1996;15:1
AmplitudeAmplitudeSummedSummedValues ofValues of
Fourier TransformFourier Transform
Heart motionHeart motionplusplus
FourierFourier--basedbasedCardiac cycleCardiac cycle
synchronizationsynchronization
Fundamental FHRFundamental FHR
Mechanical 4DUS Probes

7/14/20117/14/2011
44
STICSTICSSpatiopatioTTemporal emporal IImage mage CCorrelationorrelation
Retrospective gating algorithm Retrospective gating algorithm
Synchronizes volumetric imaging data to the Synchronizes volumetric imaging data to the phase of the fetal cardiac cycle at the time of phase of the fetal cardiac cycle at the time of acquisitionacquisition
Temporal information (motion) is incorporated Temporal information (motion) is incorporated into the final volume datasetinto the final volume dataset
Volume 1Volume 1 Volume 2Volume 2 Volume 3Volume 3 Volume 4Volume 4 Volume 5Volume 5 Volume 6Volume 6
Volume AcquisitionVolume Acquisition
4D Fetal Echocardiography4D Fetal EchocardiographyWhat Does The Technology Allow?What Does The Technology Allow?
Examination of the fetal heart in a systematic Examination of the fetal heart in a systematic manner, offline, after volume dataset acquisition, manner, offline, after volume dataset acquisition, in the absence of fetal movementin the absence of fetal movementin the absence of fetal movementin the absence of fetal movement
Correlation between image planes that are Correlation between image planes that are perpendicular to the main acquisition planeperpendicular to the main acquisition plane
Volume data can viewed by experts at a remote Volume data can viewed by experts at a remote sitesite
Tips for Volume AcquisitionTips for Volume AcquisitionTips for Volume AcquisitionTips for Volume Acquisition
Region of Interest (ROI)Region of Interest (ROI)
DecreasesDecreasesIncreasesIncreases
XX
YYDecreasesDecreasesframe rateframe rateIncreasesIncreasesframe rateframe rate

7/14/20117/14/2011
55
Acquisition AngleAcquisition Angle
XX
Acquisition angle determines Z (or depth)Acquisition angle determines Z (or depth)
YYZZ =15 to 40=15 to 40°°
Acquisition Angle SelectionAcquisition Angle Selection
Smaller angles for youngerSmaller angles for youngerSmaller angles for younger Smaller angles for younger fetusesfetuses
Larger angles for older fetusesLarger angles for older fetuses
Acquisition TimeAcquisition Time
Determines the duration of the 3D sweepDetermines the duration of the 3D sweep
Slower acquisition = better spatial resolutionSlower acquisition = better spatial resolution
Caveat: fetal movement Caveat: fetal movement
General rule:General rule:
Slow sweep for fetuses that are still Slow sweep for fetuses that are still
Fast sweep for those that are moving or breathingFast sweep for those that are moving or breathing

7/14/20117/14/2011
66
X6-1 Matrix Transducer
• 9,212 elements• self-contained beam former• frequency range 1-6 MHz• active aperture 36 x 17 mm
Working With Volume DataWorking With Volume DataWorking With Volume DataWorking With Volume Data
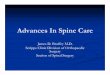
MultiplanarMultiplanar Display and NavigationDisplay and Navigation
transverse sagittal
A B
coronal
C
Gonçalves et al. Am J Obstet Gynecol 2003;189:1792Gonçalves et al. Am J Obstet Gynecol 2003;189:1792--18021802

7/14/20117/14/2011
77
Scroll in the original plane of acquisitionScroll in the original plane of acquisition 33--Step Technique to Systematically Step Technique to Systematically Visualize the Outflow TractsVisualize the Outflow Tracts
Gonçalves et al. Am J Obstet Gynecol 2003;189:1792Gonçalves et al. Am J Obstet Gynecol 2003;189:1792--18021802
Transposition of the great arteriesTransposition of the great arteries
Gonçalves et al. J Ultrasound Med 2004;23:1225Gonçalves et al. J Ultrasound Med 2004;23:1225--3131
LowLow--RiskRiskn = 112n = 112
Tetralogy of Fallot (n=5)Tetralogy of Fallot (n=5)Interrupted Ao arch (n=1)Interrupted Ao arch (n=1)
Complete TGA (n=3)Complete TGA (n=3)Corrected TGA (n=1)Corrected TGA (n=1)
Offline AnalysisOffline AnalysisBlinded examinersBlinded examiners
Outflow tract anomaliesOutflow tract anomaliesn = 10n = 10
1 case of hypoplastic 1 case of hypoplastic left heart correctly left heart correctly
diagnoseddiagnosed
ThreeThree--step techniquestep technique
Rizzo et al. Fetal Diagn Ther 2008;24:126Rizzo et al. Fetal Diagn Ther 2008;24:126--131131

7/14/20117/14/2011
88
Spin Technique For Spin Technique For Evaluation Of The LVOTEvaluation Of The LVOT
DeVore et al. Ultrasound Obstet Gynecol 2004;24:72DeVore et al. Ultrasound Obstet Gynecol 2004;24:72--8282
Spin Technique for Spin Technique for Evaluation of the RVOTEvaluation of the RVOT
DeVore et al. Ultrasound Obstet Gynecol 2004;24:72DeVore et al. Ultrasound Obstet Gynecol 2004;24:72--8282
Spin Technique for Spin Technique for Evaluation of the Aortic Evaluation of the Aortic ArchArch
DeVore et al. Ultrasound Obstet Gynecol 2004;24:72DeVore et al. Ultrasound Obstet Gynecol 2004;24:72--8282 Espinoza et al. JUM 2007;26:1181Espinoza et al. JUM 2007;26:1181--11881188
Espinoza et al. JUM 2007;26:1181Espinoza et al. JUM 2007;26:1181--11881188
Tetralogy of FallotTetralogy of Fallot
Espinoza et al. JUM 2007;26:1181Espinoza et al. JUM 2007;26:1181--11881188

7/14/20117/14/2011
99
Transposition of the Great ArteriesTransposition of the Great Arteries
Espinoza et al. JUM 2007;26:1181Espinoza et al. JUM 2007;26:1181--11881188
Truncus ArteriosusTruncus Arteriosus
Espinoza et al. JUM 2007;26:1181Espinoza et al. JUM 2007;26:1181--11881188
Pulmonary AtresiaPulmonary Atresia
Espinoza et al. JUM 2007;26:1181Espinoza et al. JUM 2007;26:1181--11881188
178 volume datasets 178 volume datasets Transverse acquisitionTransverse acquisition
Normal Normal heartheart
Conotruncal Conotruncal anomaliesanomalies
Other Other anomaliesanomalies
Visualization rates for the ductal archVisualization rates for the ductal arch
Espinoza et al. JUM 2007;26:1181Espinoza et al. JUM 2007;26:1181--11881188
n=116n=116 n=18n=18 n=34n=34
5.6%5.6%(1/18)(1/18)
93.1% 93.1% (108/116)(108/116)
79.4%79.4%(27/34)(27/34)
chichi--square, p<0.01square, p<0.01 chichi--square, p<0.01square, p<0.01
““The lack of visualization of the The lack of visualization of the sagittal view of the ductal arch sagittal view of the ductal arch should raise the index ofshould raise the index of
Espinoza et al. JUM 2007;26:1181Espinoza et al. JUM 2007;26:1181--11881188
should raise the index of should raise the index of suspicion for conotruncal suspicion for conotruncal anomalies.anomalies.””
Rendered ViewsRendered Views
DeVore et al. Ultrasound Obstet Gynecol 2003;22:380DeVore et al. Ultrasound Obstet Gynecol 2003;22:380--387387

7/14/20117/14/2011
1010
Rendered ViewsRendered Views Rendered Views Rendered Views –– AV ValvesAV Valves
Gonçalves et al. Am J Obstet Gynecol 2003;189:1792Gonçalves et al. Am J Obstet Gynecol 2003;189:1792--18021802
Normal AV ValvesNormal AV Valves
AV CanalAV CanalAV CanalAV Canal
Tricuspid StenosisTricuspid Stenosis
Gonçalves et al. Am J Obstet Gynecol 2003;189:1792Gonçalves et al. Am J Obstet Gynecol 2003;189:1792--18021802
Overriding Aorta Overriding Aorta -- RenderedRendered
Perinatology Research Branch, NICHD/NIH/DHHSPerinatology Research Branch, NICHD/NIH/DHHS
Stenotic Pulmonary Valve Stenotic Pulmonary Valve AnnulusAnnulus
Perinatology Research Branch, NICHD/NIH/DHHSPerinatology Research Branch, NICHD/NIH/DHHS
Absent Pulmonary Valve Absent Pulmonary Valve SyndromeSyndrome
Perinatology Research Branch, NICHD/NIH/DHHSPerinatology Research Branch, NICHD/NIH/DHHS

7/14/20117/14/2011
1111
Static, R. Chaoui, 2001Static, R. Chaoui, 2001 Dynamic, Deng, 2002Dynamic, Deng, 2002
Color STIC Color STIC -- RenderingRendering
Gonçalves et al. JUM 2004;23:473Gonçalves et al. JUM 2004;23:473--481481
Inversion ModeInversion ModeVisualization of Hollow Structures Without DopplerVisualization of Hollow Structures Without Doppler
Nelson et al. UMB 1998;24:1254
How is Invert Mode Rendering Generated?How is Invert Mode Rendering Generated?
Transverse Sagittal
Coronal
Inversion Mode ExampleInversion Mode Example
Perinatology Research Branch, NICHD/NIH/DHHS

7/14/20117/14/2011
1212
4D Rendering with Inversion 4D Rendering with Inversion
NORMALNORMAL TRANSPOSITIONTRANSPOSITION
Gonçalves et al. J Ultrasound Med 2005;24:415Gonçalves et al. J Ultrasound Med 2005;24:415--424424
AortaAorta AzygosAzygosveinvein
Interrupted IVCInterrupted IVCw/ azygous continuationw/ azygous continuation
Espinoza et al. Ultrasound Obstet Gynecol 2005;25:428Espinoza et al. Ultrasound Obstet Gynecol 2005;25:428--34 34
RightRight LeftLeftRightRight LeftLeft
BB--Flow ImagingFlow Imaging
Technology that digitally enhances signals from weak Technology that digitally enhances signals from weak blood reflectors from vessels and, at the same time, blood reflectors from vessels and, at the same time, , ,, ,suppresses strong signals from surrounding tissuessuppresses strong signals from surrounding tissues
Does not rely on Doppler methods to display blood flow, Does not rely on Doppler methods to display blood flow, is angle independent and interferes less with the frame is angle independent and interferes less with the frame raterate
BB--Flow Rendering of the Flow Rendering of the Aortic and Ductal ArchesAortic and Ductal Arches
Perinatology Research Branch, NICHD/NIH/DHHSPerinatology Research Branch, NICHD/NIH/DHHS

7/14/20117/14/2011
1313
Comparison Between Different Algorithms for Comparison Between Different Algorithms for 3D Rendering of the Aortic and 3D Rendering of the Aortic and DuctalDuctal ArchesArches
24 weeks24 weeks
BB--FlowFlow Power DopplerPower Doppler Color DopplerColor Doppler
Espinoza et al. JUM 2009;28:1375Espinoza et al. JUM 2009;28:1375--13781378
200 consecutive patients (13 200 consecutive patients (13 –– 40 weeks)40 weeks)
DeVore & Polanko. JUM 2005;24:1685DeVore & Polanko. JUM 2005;24:1685
Transverse acquisitionsTransverse acquisitions
44--chamber view as the initial point of image acquisitionchamber view as the initial point of image acquisition
4CH, 5CH, 3VV, 3VTV4CH, 5CH, 3VV, 3VTV
Adjustments in image distance allowed until desired Adjustments in image distance allowed until desired views were identified views were identified
Tomographic Ultrasound ImagingTomographic Ultrasound Imaging
Gonçalves et al. J Perinat Med 2006;34:39Gonçalves et al. J Perinat Med 2006;34:39--5555

7/14/20117/14/2011
1414
TomographicTomographic Ultrasound ImagingUltrasound Imaging
Gonçalves et al. J Perinat Med 2006;34:39Gonçalves et al. J Perinat Med 2006;34:39--5555
Hypoplastic Right VentricleHypoplastic Right VentriclePulmonary AtresiaPulmonary Atresia
Gonçalves et al. J Perinat Med 2006;34:39Gonçalves et al. J Perinat Med 2006;34:39--5555
Coarctation of the AortaCoarctation of the Aorta
Gonçalves et al. J Perinat Med 2006;34:39Gonçalves et al. J Perinat Med 2006;34:39--5555
Hypoplastic Left Heart SyndromeHypoplastic Left Heart Syndrome
Gonçalves et al. J Perinat Med 2006;34:39Gonçalves et al. J Perinat Med 2006;34:39--5555
AutomationAutomationAutomationAutomation

7/14/20117/14/2011
1515
Diagnosis of complete TGA in 10 confirmed casesDiagnosis of complete TGA in 10 confirmed cases
N l Ab l
Rizzo et al. J Ultrasound Med 2008;27:771-6
ViewNormal Abnormal
N % N %
4CH 10 100% 0 -
LVOT (cardiac plane 1) 1 10% 9 90%
RVOT (cardiac plane 2) 3 30% 7 70%
In all cases an abnormal ventriculoarterial connection was In all cases an abnormal ventriculoarterial connection was shown after activation of either cardiac plane 1 or 2shown after activation of either cardiac plane 1 or 2
Clinical QuestionsClinical QuestionsClinical QuestionsClinical Questions
How Often Are Volumes of How Often Are Volumes of Diagnostic Quality Acquired?Diagnostic Quality Acquired?
Feasibility of STIC in Feasibility of STIC in Clinical PracticeClinical Practice
STIC incorporated in clinical practice over a 2 month STIC incorporated in clinical practice over a 2 month period period pp
High risk fetuses / no suspected CHDHigh risk fetuses / no suspected CHD
2 experienced sonographers2 experienced sonographers
No more than 4 attempts per examNo more than 4 attempts per exam
Uittenbogaard et al. Ultrasound Obstet Gynecol 2008;31:625Uittenbogaard et al. Ultrasound Obstet Gynecol 2008;31:625--632632
Study populationStudy populationn = 165n = 165
Successful Successful acquisitionacquisition
STIC not attemptedSTIC not attemptedn = 17 (10%)n = 17 (10%)
STIC datasetsSTIC datasetsn =148n =148
Storage Storage errorserrors
7 (6%)7 (6%) n = 112 (76%)n = 112 (76%)
AnalysisAnalysisn=105 (64%)n=105 (64%)
n = 7 (6%)n = 7 (6%)
Uittenbogaard et al. Ultrasound Obstet Gynecol 2008;31:625Uittenbogaard et al. Ultrasound Obstet Gynecol 2008;31:625--632632
High qualityHigh qualityn=26 (25%)n=26 (25%)
Sufficient qualitySufficient qualityn=42 (40%)n=42 (40%)
Insufficient qualityInsufficient qualityn=37 (35%)n=37 (35%)
Factors associated with Factors associated with high quality volume high quality volume datasetsdatasets
BMI:BMI:
23 8 kg/m223 8 kg/m2 x 26 5 kg/m2 p =x 26 5 kg/m2 p =23.8 kg/m223.8 kg/m2 x 26.5 kg/m2, p x 26.5 kg/m2, p 0.040.04
Posterior placenta:Posterior placenta:
56.0% x 30.3%, p = 0.0556.0% x 30.3%, p = 0.05
Uittenbogaard et al. Ultrasound Obstet Gynecol 2008;31:625Uittenbogaard et al. Ultrasound Obstet Gynecol 2008;31:625--632632

7/14/20117/14/2011
1616
Objective:Objective:
T d t i h f tl STIC l d t tT d t i h f tl STIC l d t t
Cohen et al. JUM 2009;28:1645Cohen et al. JUM 2009;28:1645--16501650
To determine how frequently a STIC volume dataset To determine how frequently a STIC volume dataset could be obtained in nonobese patients at 18could be obtained in nonobese patients at 18--22 22 weeks of gestationweeks of gestation
Frequency of satisfactory images for screeningFrequency of satisfactory images for screening
45 minutes maximum time allowed for volume 45 minutes maximum time allowed for volume acquisitionacquisition
Cohen et al. JUM 2009;28:1645Cohen et al. JUM 2009;28:1645--16501650
Cohen et al. JUM 2009;28:1645Cohen et al. JUM 2009;28:1645--16501650 Cohen et al. JUM 2009;28:1645Cohen et al. JUM 2009;28:1645--16501650
TelemedicineTelemedicineTelemedicineTelemedicine100 fetuses between 18 and 37 weeks100 fetuses between 18 and 37 weeks
Volume acquisition by a general obstetrician with no Volume acquisition by a general obstetrician with no expertise in fetal echocardiographyexpertise in fetal echocardiography
Acquisition time = 7.5 sAcquisition time = 7.5 s
Acquisition angle = 30Acquisition angle = 30°°
Volumes stored for later review by an expert:Volumes stored for later review by an expert:
Scrolling in the original plane of acquisitionScrolling in the original plane of acquisition
Multiplanar displayMultiplanar display

7/14/20117/14/2011
1717
Visualization rates slightly Visualization rates slightly better, but not significantly better, but not significantly different between scrolling different between scrolling
in the original plane vs. in the original plane vs. multiplanar displaymultiplanar display
Viñals et al. Ultrasound Obstet Gynecol 2003;22:388Viñals et al. Ultrasound Obstet Gynecol 2003;22:388--394394
Visualization rates lower Visualization rates lower for apex/stomach for apex/stomach
continuity and threecontinuity and three--vessel vessel and trachea viewand trachea view
2 examiners instructed on how on perform a STIC 2 examiners instructed on how on perform a STIC volume acquisition by emailvolume acquisition by emailvolume acquisition by emailvolume acquisition by email
Acquisition time = 7.5 sAcquisition time = 7.5 s
Acquisition angle = 30 sAcquisition angle = 30 s
Specific instructions on how to avoid common Specific instructions on how to avoid common artifactsartifacts
Volumes uploaded to a web serverVolumes uploaded to a web server
Review by a sonologist with experience in fetal Review by a sonologist with experience in fetal echocardiographyechocardiography
50 fetuses (77 volumes)50 fetuses (77 volumes)20 20 –– 36 weeks of gestation36 weeks of gestation
20 to 40 min for 2520 to 40 min for 25--30 Mb volume upload30 Mb volume uploadInternet speed 128 to 300 kb/sInternet speed 128 to 300 kb/s
ExtraExtra cardiaccardiac
NormalNormaln = 47n = 47
NormalNormaln = 47n = 47
ExtraExtra--cardiac cardiac anomaliesanomalies
n = 2n = 2 AbnormalAbnormaln = 3n = 3
AbnormalAbnormaln = 3n = 3
Suspected Suspected echogenic focusechogenic focus
n = 1n = 1
VSDVSDAV canalAV canal
TGATGASTIC reviewSTIC review
OutcomeOutcome
Viñals et al. Ultrasound Obstet Gynecol 2005;25:25Viñals et al. Ultrasound Obstet Gynecol 2005;25:25--3131
Visualization rates slightly Visualization rates slightly better for Operator 2better for Operator 2
Viñals et al. Ultrasound Obstet Gynecol 2005;25:25Viñals et al. Ultrasound Obstet Gynecol 2005;25:25--3131
Visualization rates lower Visualization rates lower for apex/stomach for apex/stomach
continuity and threecontinuity and three--vessel vessel and trachea viewand trachea view
First TrimesterFirst TrimesterFirst TrimesterFirst Trimester
12 week pregnancy12 week pregnancySTIC w/ tomographic imagingSTIC w/ tomographic imaging

7/14/20117/14/2011
1818
Assessed whether early pregnancy heart volumes could Assessed whether early pregnancy heart volumes could be obtained by nonbe obtained by non--experts with remote interpretation by experts with remote interpretation by
Viñals et al. Ultrasound Obstet Gynecol 2008;31:633Viñals et al. Ultrasound Obstet Gynecol 2008;31:633--638638
yy p p yp p yexperts via telemedicine linkexperts via telemedicine link
49 singleton pregnancies between 11 and 13+6 weeks49 singleton pregnancies between 11 and 13+6 weeks
Acquisition parameters: 7.5 s / 15 degree angle / gray Acquisition parameters: 7.5 s / 15 degree angle / gray and color Dopplerand color Doppler
Successful acquisition = 39/45 cases (71%)Successful acquisition = 39/45 cases (71%)
Viñals et al. Ultrasound Obstet Gynecol 2008;31:633Viñals et al. Ultrasound Obstet Gynecol 2008;31:633--638638
Viñals et al. Ultrasound Obstet Gynecol 2008;31:633Viñals et al. Ultrasound Obstet Gynecol 2008;31:633--638638 Viñals et al. Ultrasound Obstet Gynecol 2008;31:633Viñals et al. Ultrasound Obstet Gynecol 2008;31:633--638638
107 consecutive singleton pregnancies107 consecutive singleton pregnancies107 consecutive singleton pregnancies 107 consecutive singleton pregnancies at 11 to 13+6 weeksat 11 to 13+6 weeks
Color STIC acquisitions Color STIC acquisitions –– 10 seconds / 20 degrees10 seconds / 20 degrees
Transabdominal onlyTransabdominal only92%92%
Additional transvaginalAdditional transvaginal8%8%
Turan et al. Ultrasound Obstet Gynecol 2009;33;652Turan et al. Ultrasound Obstet Gynecol 2009;33;652--5656

7/14/20117/14/2011
1919
First 3 volume datasets of high quality in 80%First 3 volume datasets of high quality in 80%
20% required up to 9 volume acquisitions until a 20% required up to 9 volume acquisitions until a satisfactory quality was achievedsatisfactory quality was achieved
12 anatomic landmarks including:12 anatomic landmarks including:12 anatomic landmarks, including:12 anatomic landmarks, including:
4 chamber view seen 100% of patients4 chamber view seen 100% of patients
two great arteries of equal size and crossing in 93% two great arteries of equal size and crossing in 93% of patientsof patients
Turan et al. Ultrasound Obstet Gynecol 2009;33;652Turan et al. Ultrasound Obstet Gynecol 2009;33;652--5656
AccuracyAccuracyAccuracyAccuracy
Singleton pregnancies at 21Singleton pregnancies at 21--36 weeks (n=1,163)36 weeks (n=1,163)g p gg p g ( )( )
Volumes acquired with gray scale + color Doppler imagingVolumes acquired with gray scale + color Doppler imaging
For suspected CHD, volumes were acquired until a good For suspected CHD, volumes were acquired until a good quality volume dataset was achieved with no time limitquality volume dataset was achieved with no time limit
Autopsy or postnatal followAutopsy or postnatal follow--up in all casesup in all cases
Average volume acquisition time:Average volume acquisition time:
Normal cases: 6.42 minutes, 70% success rateNormal cases: 6.42 minutes, 70% success rate
VSD cases: 53.26 minutes to obtain a good quality volumeVSD cases: 53.26 minutes to obtain a good quality volume
DanDan--dan et al. Arch Gynecol Obstet 2010 (online publication 5/6/2010)dan et al. Arch Gynecol Obstet 2010 (online publication 5/6/2010)
1,163 singletons1,163 singletons2121--36 weeks36 weeks
CHD w/o VSDCHD w/o VSDn=43n=43
CHD w/ VSDCHD w/ VSDn=58n=58
DanDan--dan et al. Arch Gynecol Obstet 2010 (online publication 5/6/2010)dan et al. Arch Gynecol Obstet 2010 (online publication 5/6/2010)
Simple VSDSimple VSDn=21 (36%)n=21 (36%)
Complex CHDComplex CHDn=37 (64%)n=37 (64%)
VSD size = 2 VSD size = 2 -- 10 mm10 mm1 false1 false--positive diagnosis by 2Dpositive diagnosis by 2D
2 VSDs missed by both 2D and STIC2 VSDs missed by both 2D and STIC
Compared STIC vs. 2D accuracy in a highCompared STIC vs. 2D accuracy in a high--risk risk populationpopulationpopulationpopulation
STIC performed after fetal echo by fetal medicine STIC performed after fetal echo by fetal medicine specialists wellspecialists well--trained in routine screening but trained in routine screening but inexperienced in fetal echocardiographyinexperienced in fetal echocardiography
Standard acquisition: 4Standard acquisition: 4--chamber view, preferably apicalchamber view, preferably apical
Volume review by specialists 1 year after acquisitionVolume review by specialists 1 year after acquisition
Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458--464464
342 w/ suspected CHD342 w/ suspected CHD1414--40 weeks40 weeks
NormalNormaln=167 (48.8%)n=167 (48.8%)
CHDCHDn=175 (51.2%)n=175 (51.2%)
Successful acquisition 98%Successful acquisition 98%Overall accuracy 91.% for STIC and 94.2% for 2DOverall accuracy 91.% for STIC and 94.2% for 2D
Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458--464464
STICSTICFalse negatives (n=9)False negatives (n=9)
VSD (n=8)VSD (n=8)
Aortic arch interruption Aortic arch interruption type B (n=1)type B (n=1)

7/14/20117/14/2011
2020
342 w/ suspected CHD342 w/ suspected CHD1414--40 weeks40 weeks
NormalNormaln=167 (48.8%)n=167 (48.8%)
CHDCHDn=175 (51.2%)n=175 (51.2%)
Successful acquisition 98%Successful acquisition 98%Overall accuracy 91.% for STIC and 94.2% for 2DOverall accuracy 91.% for STIC and 94.2% for 2D
Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458--464464
2D2DFalse negatives (n=3)False negatives (n=3)
VSD (n=2)VSD (n=2)
Persistent left SVCPersistent left SVC(n=1)(n=1)
342 w/ suspected CHD342 w/ suspected CHD1414--40 weeks40 weeks
NormalNormaln=167 (48.8%)n=167 (48.8%)
CHDCHDn=175 (51.2%)n=175 (51.2%)
Successful acquisition 98%Successful acquisition 98%Overall accuracy 91.% for STIC and 94.2% for 2DOverall accuracy 91.% for STIC and 94.2% for 2D
Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458--464464
STICSTICFalse positives (n=19)False positives (n=19)
VSD (n=10)VSD (n=10)
Coarctation of Ao (n=4)Coarctation of Ao (n=4)
Persistent LSVC (n=2)Persistent LSVC (n=2)
Pulmonary stenosis (n=1)Pulmonary stenosis (n=1)
Tricuspid dysplasia (n=1)Tricuspid dysplasia (n=1)
Rhabdomyoma (n=1)Rhabdomyoma (n=1)
342 w/ suspected CHD342 w/ suspected CHD1414--40 weeks40 weeks
NormalNormaln=167 (48.8%)n=167 (48.8%)
CHDCHDn=175 (51.2%)n=175 (51.2%)
Successful acquisition 98%Successful acquisition 98%Overall accuracy 91.% for STIC and 94.2% for 2DOverall accuracy 91.% for STIC and 94.2% for 2D
Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458--464464
2D2DFalse positives (n=17)False positives (n=17)
VSD (n=11)VSD (n=11)
Coarctation of Ao (n=4)Coarctation of Ao (n=4)
Tricuspid dysplasia (n=1)Tricuspid dysplasia (n=1)
Ostium primum ASD (n=1)Ostium primum ASD (n=1)
Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458--464464
ConclusionConclusion
•• ““...we present a large series of CHDs evaluated with ...we present a large series of CHDs evaluated with
STIC technology and conclude that, STIC technology and conclude that, in a highin a high--risk risk
populationpopulation 4D4D STIC echocardiography could beSTIC echocardiography could bepopulationpopulation, 4D, 4D--STIC echocardiography could be STIC echocardiography could be
incorporated into a clinical setting, with a high incorporated into a clinical setting, with a high
accuracy for offline reassurance of normality and accuracy for offline reassurance of normality and
diagnosis of any anomaly in the whole spectrum of diagnosis of any anomaly in the whole spectrum of
CHDCHD””
Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458Bennasar et al. Ultrasound Obstet Gynecol 2010;36:458--464464 Espinoza et al. JUM 2010;29:1573Espinoza et al. JUM 2010;29:1573--15801580
Objectives:Objectives:
To determine the accuracy of 4DUS for the diagnosis To determine the accuracy of 4DUS for the diagnosis of congenital heart defectsof congenital heart defects
To determine agreement of diagnostic impressions To determine agreement of diagnostic impressions among participting centersamong participting centers

7/14/20117/14/2011
2121
7 International Centers with Expertise 7 International Centers with Expertise in 4DUS Echocardiographyin 4DUS Echocardiography
Each center uploaded 20 volume datasets of fetuses with and without CHDEach center uploaded 20 volume datasets of fetuses with and without CHD
1818--26 weeks, B26 weeks, B--mode or Color, 1 volume/case, 90 randomly selected for analysismode or Color, 1 volume/case, 90 randomly selected for analysis
Sensitivity 93% (77Sensitivity 93% (77--100%)100%)
Specificity 96% (84Specificity 96% (84--100%)100%)
PPV 96% (83PPV 96% (83--100%)100%)
Espinoza et al. JUM 2010;29:1573Espinoza et al. JUM 2010;29:1573--15801580
PPV 96% (83PPV 96% (83 100%)100%)
NPV 93% (79NPV 93% (79--100%)100%)
Intercenter agreement kappa = 0.97Intercenter agreement kappa = 0.97
Median time to upload/download Median time to upload/download each dataset = 2 min (1each dataset = 2 min (1--3 min)3 min)
Median time to analyze each volume Median time to analyze each volume = 6 min (2= 6 min (2--15 min)15 min)
Datasets w/ limited quality = 10%Datasets w/ limited quality = 10%
Espinoza et al. JUM 2010;29:1573Espinoza et al. JUM 2010;29:1573--15801580