Embed Size (px)
Citation preview
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna
Fetal Echocardiography and Magnetocardiography
Last Review: 02/24/2021
Effective: 05/08/1996
Next Review: 01/27/2022
Number: 0106
Page 1 of 37
*Please see amendment for Pennsylvania Medicaid
at the end of this CPB.
I. Aetna considers fetal echocardiograms, Doppler and color flow
mapping medically necessary after 12 weeks gestation for any of
the following conditions:
A. A mother with type 1 diabetes or pregestational type 2 diabetes on
insulin during the first trimester; or
B. A mother with systemic lupus erythematosus; or
C. As a screening study in families with a first-degree relative of a fetus with congenital heart disease; or
D. Fetal nuchal translucency measurement of 3.5 mm or greater
in the first trimester; or
E. Following an abnormal or incomplete cardiac evaluation on an
anatomic scan, 4-chamber study
(Note: When the 4-chambered view is adequate and there are
no other indications of a cardiac abnormality, a fetal
echocardiogram is not considered medically necessary); or
F. For ductus arteriosus dependent lesions and/or with other known complex congenital heart disease; or
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 2 of 37
G. For pregnancies conceived by in vitro fertilization (IVF) or intra- cytoplasmic sperm injection (ICSI); or
H. In cases of persistent right umbilical vein; or
I. In cases of single umbilical artery; or
J. In cases of suspected or known fetal chromosomal abnormalities;
or
K. In suspected or documented fetal arrhythmia: to define the rhythm
and its significance, to identify structural heart disease and cardiac
function; or
L. In members with autoimmune antibodies associated with
congenital cardiac anomalies [anti-Ro (SSA)/anti-La (SSB)]; or
M. In members with familial inherited disorders associated with
congenital cardiac abnormalities (e.g., Marfan syndrome); or
N. In cases with monochorionic twins; or
O. In cases of multiple gestation and suspicion of twin-twin
transfusion syndrome; or
P. In members with seizure disorders, even if they are not
presently taking anti-seizure medication; or
Q. In cases with non-immune fetal hydrops or unexplained severe polyhydramnios; or
R. When members' fetuses have been exposed to drugs known to
increase the risk of congenital cardiac abnormalities including
but no t limited to:
Anti-seizure medications; or
Excessive alcohol intake; or
Lithium; or
Paroxetine (Paxil); or
Retinoids; or
S. When other structural abnormalities are found on ultrasound;
or
II. Aetna considers repeat studies of fetal echocardiograms medically
necessary for any of the following:
A. When the initial screening study indicates any of the following:
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 3 of 37
1. A ductus arteriosus dependent lesion; or
2. Structural heart disease with a suggestion of hemodynamic
compromise; or
3. Tachycardia other than sinus tachycardia or heart block; or
B. Fetal surveillance (e.g., congenital heart block) in mother with
documented diagnosis of Sjögren’s syndrome. Frequency of
testing: Doppler fetal echocardiography may be repeated every
1 to 2 weeks starting at 16 weeks gestation continuing through
28 weeks gestation, then every other week until 32 weeks
gestation to detect fetal (congenital) heartblock.
III. Aetna considers fetal echocardiograms experimental and
investigational for all other indications including the following (not
an all-inclusive list) because their effectiveness for these
indications has not been established.
As a screening test in advanced maternal age; or
Gestational diabetes even if requiring insulin after the first
trimester; or
Pregnantwomenreceivingselective serotoninreuptake
inhibitors (except paroxetine); or
Suspected cystic fibrosis.
IV. Aetna considers fetal magnetocardiography experimental and
investigational because its effectiveness has not been established.
Definition of fetal cardiac structures is currently possible at 12 weeks of
gestation with the use of vaginal probes with high-resolution transducers.
With current technologies, accurate segmental analysis of cardiac
structures and blood flow across valves, shunts, and the ductus
arteriosus is possible with a conventional transabdominal approach by 16
to 18 weeks of gestation.

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 4 of 37
According to the American Institute for Ultrasound in Medicine (AIUM),
fetal echocardiography is commonly performed between 18 and 22
weeks’ gestational age. Some forms of congenital heart disease may
even be recognized during earlier stages of pregnancy (AIUM, 2013).
Newer technology including endovaginal transducers can obtain images
of the heart as early as 12 weeks gestation (AHA, 2018).
Hutchinson et al. (2017) states that early fetal echocardiography (FE),
performed at 12 to 16 weeks' gestational age (GA), can be used to
screen for fetal heart disease similar to that routinely performed in the
second trimester; however, the efficacy of FE at earlier GAs has not been
as well explored, particularly with recent advances in ultrasound
technology. Pregnant women were prospectively recruited for first-
trimester FE. All underwent two-dimensional (2D) cardiac imaging
combined with color Doppler (CD) assessment, and all were offered
second-trimester fetal echocardiographic evaluations. Fetal cardiac
anatomy was assessed both in real time during FE and additionally offline
by two separate reviewers. Very early FE was performed in 202
pregnancies including a total of 261 fetuses, with 92% (n = 241) being
reassessed at greater than or equal to 18 weeks' GA. Transabdominal
scanning was used in all cases, and transvaginal scanning was used
additionally in most at less than 11 weeks' GA (n = 103 of 117 [88%]).
There was stepwise improvement in image resolution of the fetal heart in
those pregnancies that presented at later gestation for assessment.CD
assisted with definition of cardiac anatomy at all GAs. A four-chambered
heart could be identified in 52% of patients in the eighth week (n = 12 of
23), improving to 80% (n = 36 of 45) in the 10th week and 98% (n = 57 of
58) by the 11th week. The inferior vena cava was visualized by 2D
imaging in only 4% (n = 1 of 23) in the eighth week, increasing to 13% (n
= 6 of 45) by the 10th week and 80% (n = 25 of 31) by the 13th week. CD
improved visualization of the inferior vena cava at earlier GAs to greater
than 80% (n = 37 of 45) from 10 weeks. Pulmonary veins were not
visualized by either 2D imaging or CD until after the 11th week. Both
cardiac outflow tracts could be visualized by 2D imaging in the minority
from 8+0 to 10+6 weeks (n = 18 of 109 [16%]) but were imaged in most
from 11+0 to 13+6 weeks (n = 114 of 144 [79%]). CD imaging improved
visualization of both outflow tracts to 64% (n = 29 of 45) in the 10th week.
On 2D imaging alone, both the aortic and ductal arches were seen in only
29% of patients in the 10th week (n = 13 of 45), increasing to 58% when
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 5 of 37
CD was used (58% [n = 26 of 45]) and to greater than 80% (n = 47 of 58)
using CD in the 11th week. The authors concluded that very early FE,
from as early as 8 weeks, can be used to assess cardiac structures;
however, the ability to image fetal heart structures between 6 and 8
weeks is currently nondiagnostic. The use of CD significantly increases
the detection of cardiac structures on early FE. The ideal timing of
complete early FE, excluding pulmonary vein assessment, appears to be
after 11 weeks' GA.
Ventriglia et al. (2016) state that there is a growing body of evidence that
most of the major cardiac abnormalities can be diagnosed from 12-16
weeks of gestation (compared with the usual 18-22 weeks). Furthermore,
the reason for performing early fetal echocardiography (EFEC) is that "the
combined EFEC-NT (nuchal translucency) approach (11th-13th week)
gives a 60-70% increase in detection rate for CHD. Combined EFE-NT
analysis is also justified by the high CHD frequency in genetic syndromes
and the similarity of anatomic relations between cardiac structures at 11
13 wks GA and those of the second trimester." "The technical limits of
EFEC are CRL < 50 mm, an increase of maternal Body mass index
(BMI), unfavorable fetal position and a possible progression of cardiac
disease especially in outflow obstructions. This means that the pregnant
women should be informed about the limits of early screening and also
recommended to have a further scan as from 18 weeks for a more
complete diagnosis."
Patients are referred for fetal echocardiography because of an
abnormality of structure or rhythm noted on ultrasound examination or
because the patient is in a high-risk group for fetal heart disease.
Treatment of the patient is facilitated by the early recognition of the exact
nature of the cardiac problem in the fetus. The correct diagnosis may be
difficult because of fetal physiology, the effect on flow across defects and
valves, inability to see the fetus for orientation reference, and inability to
examine the fetus for clinical findings. For these reasons, fetal
echocardiography should be performed only by trained fetal
echocardiographers.
The umbilical cord normally contains two arteries and one vein embedded
in Wharton's jelly. The umbilical cord "achieves its final form by the 12th
week of gestation". Initially during umbilical cord development, there

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 6 of 37
are two umbilical arteries and two umbilical veins, in which the two veins
(left and right) converge into one. Obliteration of the right umbilical vein by
the end of the 6th week of gestation results in a single persisting left
umbilical vein (Spurway et al, 2012). However, persistence of the right
umbilical vein in the fetus is a variant of the intra-abdominal umbilical
venous connection. The estimated prevalence of an intrahepatic
persistent right umbilical vein is 1 per 786 births; which may be
an underestimated calculation in populations that do not undergo targeted
sonographic examinations. In addition, the variation in anatomy can be
subtle (Lide et al, 2016).
Lide et al (2016) provided a comprehensive review of the current data
surrounding an intra-hepatic persistent right umbilical vein in the fetus,
including associated anomalies and outcomes, to aid practitioners in
counseling and management of affected pregnancies. These
investigators performed a Medline, Embase, Cochrane Central Register
of Controlled Trials, and Northern Light database search for articles
reporting outcomes on prenatally diagnosed cases of a persistent right
umbilical vein. Each article was independently reviewed for eligibility by
the investigators. Thereafter, the data were extracted and validated
independently by 3 investigators. A total of 322 articles were retrieved,
and 16 were included in this systematic review. The overall prevalence of
an intra-hepatic persistent right umbilical vein was found to be 212 per
166,548 (0.13 %). Of the 240 cases of an intra-hepatic persistent right
umbilical vein identified, 183 (76.3 %) were isolated. The remaining
cases had a co-existing abnormality, including 19 (7.9 %) cardiac, 9 (3.8
%) central nervous system, 15 (6.3 %) genito-urinary, 3 (1.3 %) genetic,
and 17 (7 %) placental/cord (predominantly a single umbilical artery).
The authors concluded that a persistent right umbilical vein is commonly
an isolated finding but may be associated with a co-existing cardiac
defect in 8 % of cases. Therefore, consideration should be given to fetal
echocardiography in cases of a persistent right umbilical vein.
Canavan et al (2016) stated that a fetal persistent intrahepatic right
umbilical vein has been linked to anomalies and genetic disorders but can
be a normal variant. These researchers conducted a retrospective review
to determine other sonographic findings that can stratify fetuses for
further evaluation. A total of 313 fetuses had a persistent intra-hepatic
right umbilical vein identified on 17- to 24-week sonography. The

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 7 of 37
outcome was any major congenital anomaly or an adverse neonatal
outcome, which was defined as aneuploidy, fetal demise, or neonatal
death. A total of 217 patients (69.3 %) had a normal neonatal outcome;
69 patients (22.0 %) were lost to follow-up; 5 fetuses (2.1 %) had
aneuploidy; 4 of the 5 had additional sonographic findings, and 1 had an
isolated persistent intra-hepatic right umbilical vein; 24 fetuses had a
major anomaly in association with the persistent right umbilical vein; 26
additional fetuses had soft sonographic markers associated with
karyotypic abnormalities but were chromosomally normal. Of those with
adverse neonatal outcomes, 12 had a congenital heart defect (57 %). An
additional sonographic finding with a persistent intra-hepatic right
umbilical vein was predictive of a congenital anomaly or an adverse
neonatal outcome (p < 0.001), with a positive predictive value of 44.0 %
(95 % confidence interval[ CI]: 30.0 % to 58.7 %). An isolated persistent
intra-hepatic right umbilical vein had a 0.4 % risk for a congenital anomaly
or an adverse neonatal outcome. The authors concluded that a
persistent intra-hepatic right umbilical vein should prompt an extended
anatomic survey and a fetal cardiac evaluation. If the survey and cardiac
anatomy are reassuring, no further follow-up is needed. If additional
findings are identified, genetic counseling and invasive testing should be
considered.
Kumar et al (2016) appraised the incidence and significance of persistent
right umbilical vein (PRUV), the most common fetal venous aberration.
Based on a South Indian antenatal cohort, these researchers identified 23
cases of PRUV amongst 20,452 fetuses of consecutive pregnancies, from
2009 to 2014, yielding an incidence of 1 in 889 total births (0.11 %). The
median maternal age was 24 (inter-quartile range [IQR], 22 to 26) years,
and median gestational age at diagnosis was 23 (IQR, 22 to 24) weeks.
Intra-hepatic drainage of PRUV was seen in 91.3 % cases. In 3 cases
(13 %), ductus venosus was absent. In 52.2 % of the cases, additional
major abnormalities were observed - predominantly cardiovascular (39.1
%). The common minor marker was single umbilical artery (SUA; 13 %).
The karyotype was found to be normal in 6 cases (26 %) that underwent
invasive testing. When associated anomalies were inconsequential or
absent, the post-natal outcome was good, which reflected in 60.9 % of
these cases. Fetal echocardiography was one of the keywords listed in
this study.

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 8 of 37
In a prospective, observational study, Hill et al (1994) reviewed their
experience with antenatal detection and subsequent neonatal outcome of
fetuses with a persistent right umbilical vein. A total of 33 cases of
persistent right umbilical vein were detected during 15,237 obstetric
ultrasound examinations performed after 15 weeks' gestation. Persistent
right umbilical vein was detected at a rate of 1 per 476 obstetric
ultrasound examinations; 6 of 33 (18.2 %) fetuses with a persistent right
umbilical vein had additional important congenital malformations. The
authors concluded that careful 2nd- and 3rd-trimester ultrasound
examinations can detect a persistent right umbilical vein. When this
particular anomaly is detected, a thorough fetal anatomic survey,
including echocardiography, should be performed to rule out more serious
congenital malformations.
Wolman et al (2002) conducted a prospective evaluation of the incidence
and neonatal outcome of fetuses with persistent right umbilical vein. This
condition had traditionally been considered to be extremely rare and to be
associated with a very poor neonatal prognosis, but later evidence has
raised some doubts about the veracity of these contentions. Between
August 1995 and November 1998, a total of 8,950 low-risk patients were
prospectively evaluated at 2 medical centers. The sonographic diagnosis
of a persistent right umbilical vein was made in a transverse section of the
fetal abdomen when the portal vein was curved toward the stomach, and
the fetal gall bladder was located medially to the umbilical vein.
Persistent right umbilical vein was detected in 17 fetuses during the
study; 4 of them had additional malformations, of which 3 had been
detected antenatally. The authors established that the incidence of
persistent right umbilical vein in a low-risk population was 1:526. They
believed that the sonographic finding of this anomaly was an indication for
conducting targeted fetal sonography and echocardiography. When the
persistent right umbilical vein was connected to the portal system and
other anomalies were ruled out, the prognosis can generally be expected
to be favorable.
Martínez et al (2012) described the ultrasound findings, maternal and
perinatal variables in cases with a prenatal diagnosis of persistence of
right umbilical vein. This was a descriptive analysis of cases with prenatal
diagnosis of persistence of right umbilical vein in the Fetal Medicine Unit,
Department of Obstetrics and Gynecology, Hospital Universitario Severo
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 9 of 37
Ochoa. These investigators described ultrasound findings, maternal and
perinatal variables. They examined 9,198 fetuses and 6 cases (0.06 %)
were diagnosis prenatally of persistent right umbilical vein, between 20
and 29 weeks of gestation. The male/female ratio was 1/1. Ductus
venosus was presented in all cases; 2 fetuses (33 %) were proved to
have other structural anomalies and their parents opted for termination of
the pregnancy. All cases had no chromosomal anomaly associated and
after birth, neonatal developments were favorable. The authors
concluded that based on these findings and a literature review, after
prenatal diagnosis of persistent right umbilical vein, an exhaustive
morphological study, which included a fetal echocardiography, is
mandatory in order to rule out other structural malformations. Indication
for fetal karyotype study has to be individualized considering persistence
right umbilical vein type and other ultrasoundfindings.
A single umbilical artery (SUA) is present in 0.2 % to 0.6 % of livebirths,
occurring more frequently in twins and in small for gestational age and
premature infants. In infants with SUA, there is an increased rate of
chromosomal and other congenital anomalies. Studies have shown that
20 % to 30 % of neonates with SUA had major structural anomalies,
frequently involving multiple organs (Palazzi and Brandt, 2009; Thummala
et al, 1998). The most commonly affected organ is the heart. Single
umbilical artery is an isolated finding in the remaining 70 % to 80 % of
infants.
Conception by in vitro fertilization (IVF) or intra-cytoplasmic sperm
injection (ICSI) has been associated with an increased incidence of fetal
heart defects. A meta-analyses on the prevalence of birth defects in
infants conceived following IVF and/or ICSI compared with spontaneously
conceived infants reported a 30 % to 40 % increased risk of birth defects
associated with IVF and/or ICSI (Hansen et al, 2005). Researchers have
reported that infants conceived with the use of IVF and/or ICSI have a 2
to-4-fold increase of heart malformations compared with naturally
conceived infants.
Kurinczuk and Bower (1997) examined the prevalence of birth defects on
420 liveborn infants who were conceived after ICSI in Belgium compared
with 100,454 liveborn infants in Western Australia delivered during the
same period. Infants born after ICSI were twice as likely asWestern

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 10 of 37
Australian infants to have a major birth defect [odds ratio (OR) 2.03, 95 %
confidence interval (CI): 1.40 to 2.93); p = 0.0002] and nearly 50 % more
likely to have a minor defect (OR 1.49 (0.48 to 4.66); p = 0.49).
Secondary data-led analyses found an excess of major cardiovascular
defects (OR 3.99).
Koivurova et al (2002) evaluated the neonatal outcome and the
prevalence of congenital malformations in children born after IVF in
northern Finland in a population-based study with matched controls.
Children born after IVF (n = 304) in 1990 to1995 were compared with
controls (n = 569), representing the general population in proportion of
multiple births, randomly chosen from the Finnish Medical Birth Register
(FMBR) and matched for sex, year of birth, area of residence, parity,
maternal age and social class. Plurality matched controls were randomly
chosen from the FMBR and analyzed separately. Additionally, IVF
singletons were compared with singleton controls. The prevalence of
heart malformations was four-fold in the IVF population than in the
controls representing the general population (OR 4.0, 95 % CI: 1.4 to
11.7).
Reefhuis et al (2009) analyzed data from the National Birth Defects
Prevention Study, a population-based, multi-center, case-control study of
birth defects. Included were mothers of fetuses or live-born infants with a
major birth defect (case infants) and mothers who had live-born infants
who did not have a major birth defect (control infants), delivered during
the period October 1997 to December 2003. Mothers who reported IVF
or ICSI use were compared with those who had unassisted conceptions.
Among singleton births, IVF or ICSI use was associated with septal heart
defects (adjusted odds ratio [aOR] = 2.1, 95 % CI: 1.1 to 4.0).
As fetal heart disease is typically associated with structural abnormalities
and consequent aberrant blood flow through the heart, it is necessary to
perform Doppler studies and color flow mapping when such abnormalities
are detected with 2D fetal echocardiography.
The American College of Obstetricians and Gynecologists' Committee
Opinion on the treatment with selective serotonin reuptake inhibitors
during pregnancy (ACOG, 2006) noted that paroxetine use among

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 11 of 37
pregnant women and women planning pregnancy should be avoided, if
possible. Fetal echocardiography should be considered for womenwho
were exposed to paroxetine in early pregnancy.
In a practice bulletin on screening for fetal chromosomal anomalies,
ACOG (2007) has stated that patients who have a fetal nuchal
translucency measurement of 3.5 mm or greater in the first trimester,
despite a negative result on an aneuploidy screen, normal fetal
chromosomes, or both, should be offered a targeted ultrasound
examination, fetal echocardiogram, or both, because such fetuses are at
a significant risk for non-chromosomal anomalies, including congenital
heart defects, abdominal wall defects, diaphragmatic hernias, and genetic
syndromes.
Twin-twin transfusion syndrome (TTTS) is a severe complication of
monochorionic (1 placenta) twin pregnancies, characterized by the
development of unbalanced chronic blood transfer from one twin, defined
as donor twin, to the other, defined as recipient, through placental
anastomoses. If left untreated, TTTS is associated with very high peri
natal mortality and morbidity rates; and fetuses who survive are at risk of
severe cardiac, neurological, and developmentaldisorders.
The American Society of Echocardiography's guidelines and standards
for performance of the fetal echocardiogram (Rychik et al, 2004) stated
that multiple gestation and suspicion of TTTS is an indication of fetal
echocardiography.
Bahtiyar et al (2007) noted that congenital heart defects (CHDs) affect
approximately 0.5 % of all neonates. Recent literature points to a
possible increase in the CHD prevalence among
monochorionic/diamniotic (MC/DA) twin gestations. These researchers
hypothesized that MC/DA twin pregnancy is a risk factor for CHD. A
systematic review of all published English literature was conducted on
MEDLINE (Ovid and PubMed) from January 2000 through April 2007
using the medical subject heading terms "congenital heart defect" and
"monozygotic twins". Four observational studies were included in the
final analysis. Published historical data were used for the population
background risk of CHD. Relative risk (RR) estimates with 95 %
confidence intervals (CIs) were calculated by fixed and random effect
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 12 of 37
models. These investigators included a total of 40 fetuses with CHDs
among 830 fetuses from MC/DA twin gestations. Compared with the
population, CHDs were significantly more prevalent in MC/DA twins
regardless of the presence of TTTS (RR, 9.18; 95 % CI: 5.51 to 15.29; p
< 0.001). Monochorionic/diamniotic twin gestations affected by TTTS
were more likely to be complicated by CHDs than those that did not have
TTTS (RR, 2.78; 95 % CI: 1.03 to 7.52; p = 0.04). Ventricular septal
defects were the most frequent heart defects. Pulmonary stenosis and
atrial septal defects were significantly more prevalent in pregnancies
complicated with TTTS. The authors concluded that MC/DA twin
gestation appears to be a risk factor for CHDs. Conditions that lead to
abnormal placentation may also contribute to abnormal heart
development, especially in MC/DA twin pregnancies complicated with
TTTS. Fetal echocardiography may be considered for all MC/DA twin
gestations because ventricular septal defects and pulmonary stenosis are
the most common defects.
The Royal College of Obstetricians and Gynaecologists' clinical practice
guidelines on "Management of monochorionic twin pregnancy" (RCOG,
2008) stated that a fetal echocardiographic assessment should be
considered in the assessment of severe TTTS.
Pregnant Women Receiving Selective Serotonin Reuptake Inhibitors
Reefhuis and colleagues (2015) followed up on previously reported
associations between peri-conceptional use of selective serotonin
reuptake inhibitors (SSRIs) and specific birth defects using an expanded
dataset from the National Birth Defects Prevention Study. These
researchers performed a Bayesian analysis combining results from
independent published analyses with data from a multi-center population
based case-control study of birth defects. A total of 17,952 mothers of
infants with birth defects and 9,857 mothers of infants without birth
defects, identified through birth certificates or birth hospitals, with
estimated dates of delivery between 1997 and 2009 were included in this
analysis; exposures were citalopram, escitalopram, fluoxetine, paroxetine,
or sertraline use in the month before through the 3rd month of
pregnancy. Posterior OR estimates were adjusted to account for
maternal race/ethnicity, education, smoking, and pre-pregnancy obesity.
Main outcome measure was 14 birth defects categories that had

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 13 of 37
associations with SSRIs reported in the literature. Sertraline was the
most commonly reported SSRI, but none of the 5 previously reported birth
defects associations with sertraline was confirmed. For 9 previously
reported associations between maternal SSRI use and birth defect in
infants, findings were consistent with no association. High posterior ORs
excluding the null value were observed for 5 birth defects with paroxetine
(anencephaly 3.2, 95 % CI: 1.6 to 6.2; atrial septal defects 1.8, 95 % CI:
1.1 to 3.0; right ventricular outflow tract obstruction defects 2.4, 95 % CI:
1.4 to 3.9; gastroschisis 2.5, 95 % CI: 1.2 to 4.8; and omphalocele 3.5,95
% CI: 1.3 to 8.0) and for 2 defects with fluoxetine (right ventricular outflow
tract obstruction defects 2.0, 95 % CI: 1.4 to 3.1 and craniosynostosis 1.9,
95 % CI: 1.1 to 3.0). The authors concluded that these data provided
reassuring evidence for some SSRIs; but suggested that some birth
defects occurred 2 to 3.5 times more frequently among the infants of
women treated with paroxetine or fluoxetine early in pregnancy.
A 2015 study by the Centers for Disease Control and Prevention (CDC)
used new data to examine previous reported links between use of specific
SSRIs medications just before or during early pregnancy and the
occurrence of certain birth defects. Researchers looked at links with 5
different SSRI medications: citalopram, escitalopram, fluoxetine,
paroxetine, and sertraline. Although the new data confirmed the risks
seen with paroxetine, it did not appear to suggest that the risk is across
the board with all SSRIs. Therefore, fetal echocardiography is still
recommended for women exposed to paroxetine, but there doesn’t seem
to be enough evidence to recommend coverage of fetal echocardiograms
for all pregnant members receiving any SSRI. The study concluded that
despite the increased risks for certain birth defects from some SSRIs
found in this study, the actual risk for a birth defect among babies born to
women taking one of these medications is still very low. Because these
specific types of birth defects are rare, even doubling the risk still results
in a low absolute risk. For example, the risks for heart defects with
obstruction of the right ventricular outflow tract could increase from 10 per
10,000 births to about 24 per 10,000 births among babies of women who
are treated with paroxetine early in pregnancy.
Fetal Magnetocardiography
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 14 of 37
Fetal magnetocardiography (fMCG) is a new, non-invasive technique
used to monitor the spontaneous electrophysiological activity of the fetal
heart. Hrtankova and associates (2015) reviewed the evidence on the
clinical value of fMCG. These investigators performed an analysis of the
literature using database search engines PubMed, and SCOPE in field of
fMCG. Compared to cardiotocography and fetal electrocardiography,
fMCG is a more effective method with a higher resolution. The signal
obtained from the fetal heart is sufficiently precise and the quality allows
an assessment of PQRST complex alterations, and to detect fetal
arrhythmia. Thanks to early diagnosis of fetal arrhythmia, there is the
possibility for appropriate therapeutic intervention and the reduction of
unexplained fetal death in late gestation. These investigators also noted
that fMCG with high temporal resolution also increased the level of clinical
trials that recorded fetal heart rate (FHR) variability. According to the
latest theories, FHR variability is a possible indicator of fetal status and
enabled the study of the fetal autonomic nervous system indirectly. The
authors concluded that fMCG is an experimental method that requires
expensive equipment; it has yet to be shown in the future if this method
will get any application in clinical practice.
Eswaran and colleagues (2017) stated that fMCG provides the requisite
precision for diagnostic measurement of electrophysiological events in the
fetal heart. Despite its significant benefits, this technique with current
cryogenic based sensors has been limited to few centers, due to high
cost of maintenance. In this study, these researchers demonstrated that
a less expensive non-cryogenic alternative, optically pumped
magnetometers, can provide similar electrophysiological and quantitative
characteristics when subjected to direct comparison with the current
technology. They concluded that further research can potentially increase
its clinical use for fMCG.
Furthermore, an UpToDate review on "Overview of the general approach
to diagnosis and treatment of fetal arrhythmias" (Levine and Alexander,
2017) states that "Magnetocardiography shifts the electrical signals into
an evoked magnetic signal that can be processed to create a beat-to-beat
magnetocardiogram that looks much like a traditional electrocardiogram
(ECG). Continuous recordings can be performed for relatively sustained
periods and have permitted elegant demonstration of arrhythmia
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 15 of 37
onset/offset and more direct observation of mechanisms. The equipment
is not widely available, requires careful shielding and requires skilled
technical support, so the technology remainsinvestigational".
Fetal Surveillance in Sjögren’s Syndrome
Gupta and Gupta (2017) state that studies show a high incidence of poor
fetal outcomes for women with Sjögren’s syndrome; however pregnancy
outcomes in these women have not been extensively studied. The
authors conducted a literature review to evaluate Sjögren’s syndrome and
pregnancy. Gupta and Gupta found that well-known fetal outcomes in
Sjögren syndrome-complicated pregnancies include neonatal lupus and
congenital heart block (CHB), of which CHB is the most severe fetal
complication. CHB is thought to occur because of damage to the
atrioventricular node by anti-SS-A or anti-SS-B antibodies, or both. The
reported prevalence of CHB in the offspring of an anti-SS-A-positive
woman is 1% to 2%. The recurrence rate in a patient with antibodies, who
has a previous child affected, is approximately 10 times higher. Based on
Gupta’s review, frequent surveillance by serial echocardiograms and
obstetric sonograms between 16 to 20 weeks of gestation and thereafter
is required for at-risk pregnancies, with the goal of early diagnosis and
early treatment of incomplete CHB, thus improving the outcome for the
fetus.
Although there are no formal guidelines for type or frequency of testing to
detect fetal heart block, it is recommended that pregnant women with
Sjögren’s syndrome receive weekly pulsed Doppler fetal
echocardiography from the 18th through the 26th week of pregnancy and
then every other week until 32 weeks. "The most vulnerable period for the
fetus is during the period from 18 to 24 weeks gestation. Normal sinus
rhythm can progress to complete block in seven days during this high-risk
period. New onset of heart block is less likely during the 26th through the
30th week, and it rarely develops after 30 weeks of pregnancy" (eviCore,
2018).
A scientific statement from the American Heart Association by Donofrio et
al. (2014) states that maternal factors of Sjögren’s syndrome are
associated with the absolute risk of 1 to 5 percent of live births that will
have congenital heart block (CHB), risk increases to 11 to 19 percent for

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 16 of 37
prior affected child with CHB or neonatal lupus. It is recommended that
fetal echocardiography be performed at 16 weeks, then weekly or every
other week to 28 weeks. The authors state that studies have suggested
that high SSA values (≥50 U/mL) correlate with increased fetal risk, and
that concern for late myocardial involvement may justify additional
assessments in the third trimester. In addition to abnormalities in the
conduction system, up to 10% to 15% of SSA-exposed fetuses with
conduction system disease may also develop myocardial inflammation,
endocardial fibroelastosis, or atrioventricular (AV) valve apparatus
dysfunction. "Although the value of serial assessment for the detection of
the progression of myocardial inflammation or conduction system disease
from first-degree block (PR prolongation) to CHB has not been proved,
serial assessment at 1- to 2-week intervals starting at 16 weeks and
continuing through 28 weeks of gestation is reasonable to perform
because the potential benefits outweigh the risks. For women who have
had a previously affected child, more frequent serial assessment, at least
weekly, is recommended."
Fetal Echocardiography for Prediction of Fetal Demise After Laser Coagulation for Twin-Twin Transfusion Syndrome
In a systematic review and meta-analysis, Gijtenbeek and colleagues
(2019) examined the value of echocardiography and Doppler before
fetoscopic laser coagulation for TTTS in the prediction of intra-uterine
fetal demise (IUFD). These investigators compared pre-operative
parameters between fetuses with and without demise following laser
surgery. A total of 18 studies were included. Recipient twins have an
increased risk of demise in case of pre-operative absent/reversed flow
(A/REDF) in the umbilical artery (OR 2.76, 95 % CI: 1.78 to 4.28), absent
or reversed a-wave in the ductus venosus (OR 2.32, 95 % CI: 1.70 to
3.16), or a middle cerebral artery peak systolic velocity of greater than 1.5
multiples of the median (MoM) (OR 7.59, 95 % CI: 2.56 to 22.46). In
donors, only A/REDF in the umbilical artery (OR 3.40, 95 % CI: 2.68 to
4.32) and absent or reversed a-wave in the ductus venosus (OR 1.66, 95
% CI: 1.12 to 2.47) were associated with IUFD. No association was
found between donor-IUFD and pre-operative myocardial performance
index (MPI). Two studies found an association between abnormal MPI
and recipient demise. With this study, these researchers identified a set
of pre-operative Doppler parameters predictive of fetal demise following

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 17 of 37
laser surgery. The authors concluded that the utility of pre-operative
parameters that reflect cardiac function such as the MPI in predicting
IUFD remains unclear; more research is needed to examine the utility of
pre-operative echocardiographic parameters such as the MPI in
predicting IUFD.
The authors stated that this was the first review and meta‐analysis of pre
operative echocardiography and Doppler in the prediction of IUFD
following fetoscopic laser surgery. To maximize the sample size, these
researchers included all studies that examined fetal demise beforebirth,
not only early‐IUFD (less than 7 days). Other causes of demise such as
placental insufficiency or IUGR could therefore have influenced these
findings, even though the majority of IUFD following laser occurred in the
1st week after laser surgery. Other drawbacks of this study included the
following: Most studies were single-center reports, 50 % of the reports
were retrospective studies. In all but 1 study, selective coagulation was
used for all or for a proportion of cases. It is known that incomplete laser
coagulation is a risk factor for recurrent TTTS or post‐laser twin anemia
polycythemia sequence (TAPS) and therewith for possible subsequent
fetal demise. Finally, these investigators did not include fetal growth
discordance, selective fetal growth restriction (sFGR), or TAPS prior to
laser surgery in this study. They noted that future large‐scale prospective
studies could allow for multi-variate analysis into the interference of sFGR
and TAPS on fetal echocardiography and Doppler parameters for IUFD.
Incorporating signs of sFGR or TAPS, and factors such as Quintero
stage, hydrops, and gestational age at TTTS diagnosis, into aprediction
model together with the before‐mentioned Doppler parameters could be
useful in daily clinical care in cases where the risk of fetal demise turns
out to be high, to spend additional counseling time on cord occlusion as a
back‐up plan if laser surgery appears technically challenging. A
prediction model could also be useful in future clinical trials investigating
innovations in treatment of TTTS.
Documentation Requirements for Fetal Echocardiography
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 18 of 37
According to guidelines from the American Institute for Ultrasound in
Medicine (AIUM), fetal echocardiography should include the following
cardiac images:
Aortic arch;
Ductalarch;
Four-chamber view;
Inferior vena cava;
Left ventricular outflow tract;
Right ventricular outflow tract;
Short-axis views ("low" for ventricles and "high" for outflow tracts);
Superior vena cava; and
Three-vessel and trachea view.
According to the 2013 AIUM's practice parameter for the "Performance of
Fetal Echocardiography", indications for fetal echocardiography are often
based on a variety of parental and fetal risk factors for congenital heart
disease. However, most cases are not associated with known risk
factors. Common indications for a detailed scan of the fetal heart include
but are not limited to:
Maternal Indications Associated with Congenital Heart Disease
Autoimmune antibodies [anti-Ro (SSA)/anti-La (SSB)]
Familial inherited disorders (e.g., 22q11.2 deletion syndrome)
In-vitro fertilization
Metabolicdisease (e.g., diabetesmellitusandphenylketonuria)
Teratogen exposure (e.g., lithium andretinoids)
Fetal Indications
Abnormal cardiac screening examination
Abnormal heart rate or rhythm
Fetal chromosomal anomaly
Extra-cardiac anomaly
First-degree relative of a fetus with congenital heart disease
Hydrops
Increased nuchal translucency
Monochorionic twins
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 19 of 37
This AIUM (2013) practice parameter was published in conjunction with
the American College of Obstetricians and Gynecologists (ACOG), and
the Society for Maternal-Fetal Medicine (SMFM), and the American
Society of Echocardiography (ASE). Furthermore, this practice
parameter was endorsed by the American College of Radiology (ACR).
Source: AIUM Practice Parameter – Fetal Echocardiography (2013).
Code Code Description
76825 Echocardiography, fetal, cardiovascular system, real
time with image documentation (2D), with or without
M-mode recording;
76826 follow-up or repeat study
76827 Dopplerechocardiography, fetal, cardiovascularsystem,
pulsed wave and/or continuous wave with spectral
display; complete
76828 follow-up or repeat study
+93325 Doppler echocardiography color flow velocity mapping
(List separately in addition to codes for
echocardiography)
0475T Recording of fetal magnetic cardiac signal using at least
3 channels; patient recording and storage, data
scanning with signal extraction, technical analysis and
result, as well as supervision, review, and interpretation
of report by a physician or other qualified health care
professional
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 20 of 37
Code Code Description
0476T patient recording, data scanning, with raw electronic
signal transfer of data and storage
0477T signal extraction, technical analysis, and result
0478T review, interpretation, report by physician or other
qualified health care professional
0541T
0542T
Myocardial imaging by magnetocardiography (MCG) for
detection of cardiac ischemia, by signal acquisition using
minimum 36 channel grid, generation of magnetic-field
time-series images, quantitative analysis of magnetic
dipoles, machine learning–derived clinical scoring, and
automated report generation
Q9950 Injection, sulfur hexafluoride lipid microspheres, per ml
B97.10,
B97.89
Unspecified viral infection
D68.61 Antiphospholipid syndrome
E10.10
E13.9
Diabetes mellitus [do not report for gestational diabetes]
F10.20
F10.29
Alcohol dependence
G40.001
G40.919
Epilepsy and recurrent seizures
I34.0 - I37.9 Mitral valve disorders, aortic valve disorders, tricuspid
valve disorders and pulmonary valve disorders, specified
as nonrheumatic,
I42.3 Endomyocardial (eosinophilic) disease
I42.4 Endocardial fibroelastosis
I42.6 Alcoholic cardiomyopathy
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 21 of 37
Code Code Description
I50.1 - I50.9 Heart failure
I51.7 Cardiomegaly
I78.0 Hereditary hemorrhagic telangectasia
L93.0
L93.2
Lupus erythematosus
M05.40
M06.9
Rheumatoid arthritis
M32.0
M32.9
Systemic lupus erythematosus
M34.0
M34.9
Systemic sclerosis [scleroderma]
M35.00 -
M35.09
Sicca syndrome [Sjögren]
M35.9,
M36.8
Unspecified diffuse connective tissue disease
O24.011 -
O24.019,
O24.111 -
O24.119
O24.311 -
O24.319,
O24.811 -
O24.819
O24.911 -
O24.919
Diabetes mellitus in pregnancy [pre-existing, excludes
gestational diabetes]
O30.001
O30.93
Multiple gestation
O36.8310 -
O36.8399
Maternal care for abnormalities of the fetal heart rate or
rhythm
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 22 of 37
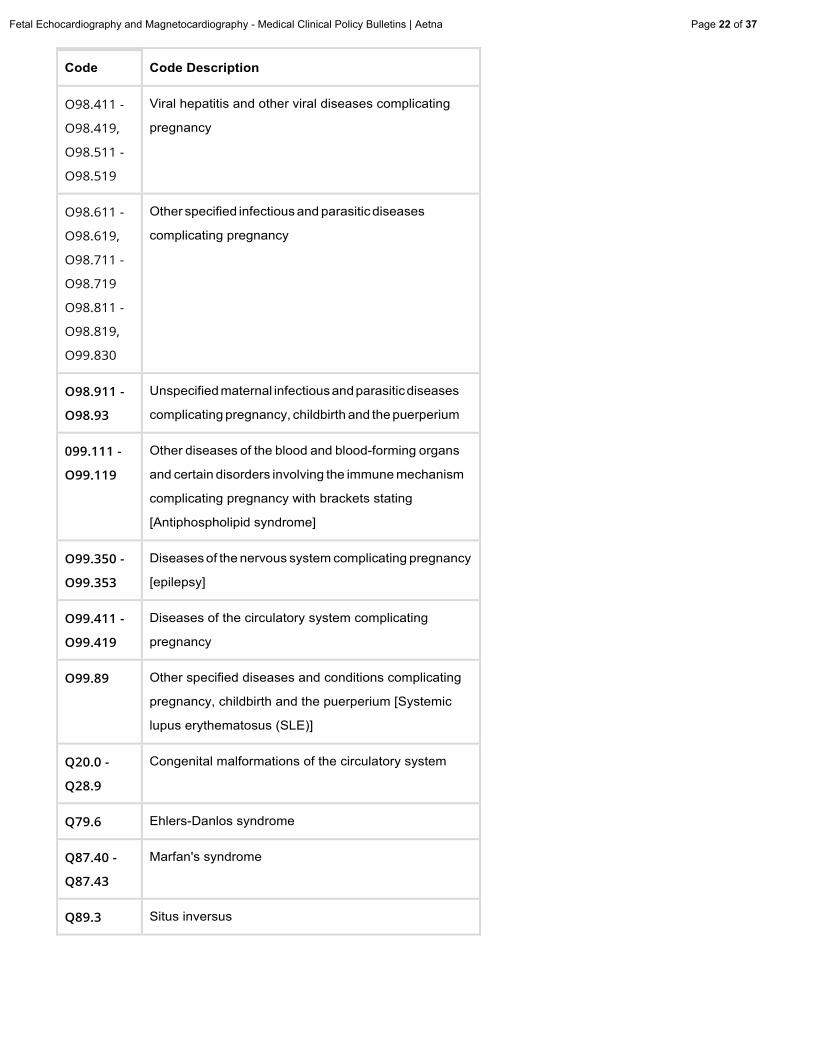
Code Code Description
O98.411 -
O98.419,
O98.511 -
O98.519
Viral hepatitis and other viral diseases complicating
pregnancy
O98.611 -
O98.619,
O98.711 -
O98.719
O98.811 -
O98.819,
O99.830
Other specified infectious and parasitic diseases
complicating pregnancy
O98.911
O98.93
Unspecified maternal infectious and parasitic diseases
complicating pregnancy, childbirth and the puerperium
099.111
O99.119
Other diseases of the blood and blood-forming organs
and certain disorders involving the immune mechanism
complicating pregnancy with brackets stating
[Antiphospholipid syndrome]
O99.350
O99.353
Diseases of the nervous system complicating pregnancy
[epilepsy]
O99.411
O99.419
Diseases of the circulatory system complicating
pregnancy
O99.89 Other specified diseases and conditions complicating
pregnancy, childbirth and the puerperium [Systemic
lupus erythematosus (SLE)]
Q20.0
Q28.9
Congenital malformations of the circulatory system
Q79.6 Ehlers-Danlos syndrome
Q87.40
Q87.43
Marfan's syndrome
Q89.3 Situs inversus
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 23 of 37
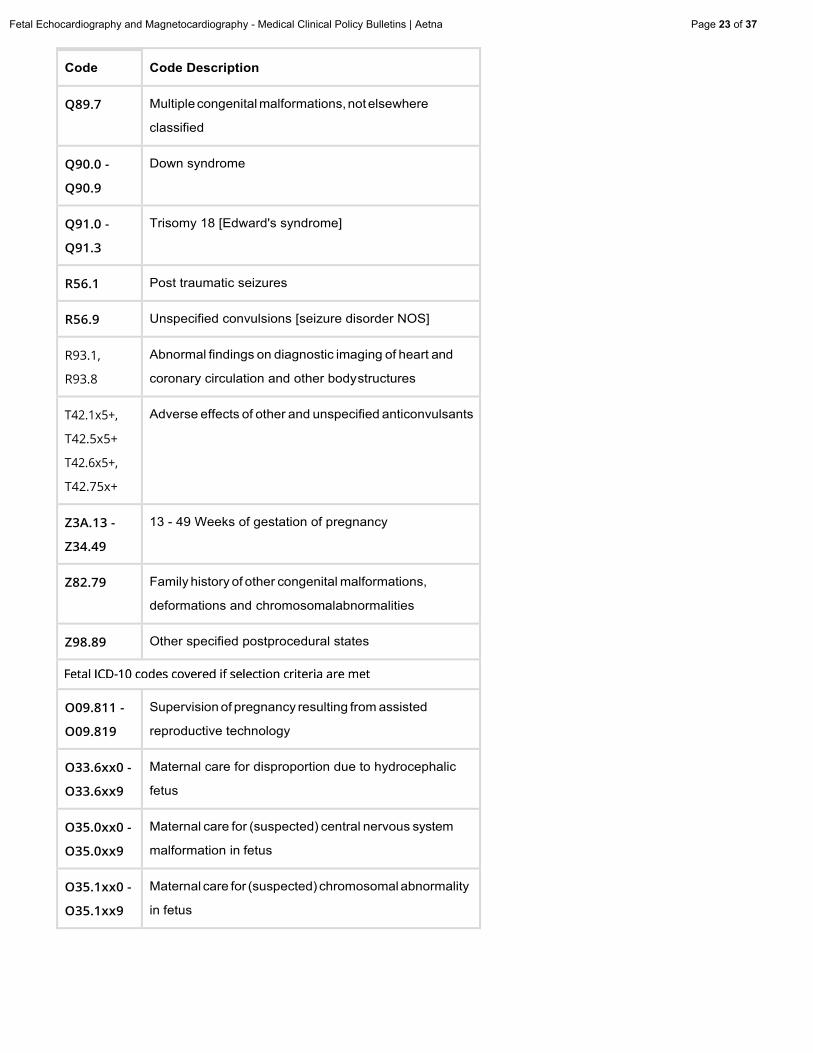
Code Code Description
Q89.7 Multiple congenital malformations, not elsewhere
classified
Q90.0
Q90.9
Down syndrome
Q91.0
Q91.3
Trisomy 18 [Edward's syndrome]
R56.1 Post traumatic seizures
R56.9 Unspecified convulsions [seizure disorder NOS]
R93.1,
R93.8
Abnormal findings on diagnostic imaging of heart and
coronary circulation and other body structures
T42.1x5+,
T42.5x5+
T42.6x5+,
T42.75x+
Adverse effects of other and unspecified anticonvulsants
Z3A.13
Z34.49
13 - 49 Weeks of gestation of pregnancy
Z82.79 Family history of other congenital malformations,
deformations and chromosomalabnormalities
Z98.89 Other specified postprocedural states
O09.811
O09.819
Supervision of pregnancy resulting from assisted
reproductive technology
O33.6xx0
O33.6xx9
Maternal care for disproportion due to hydrocephalic
fetus
O35.0xx0
O35.0xx9
Maternal care for (suspected) central nervous system
malformation in fetus
O35.1xx0
O35.1xx9
Maternal care for (suspected) chromosomal abnormality
in fetus
Code Code Description
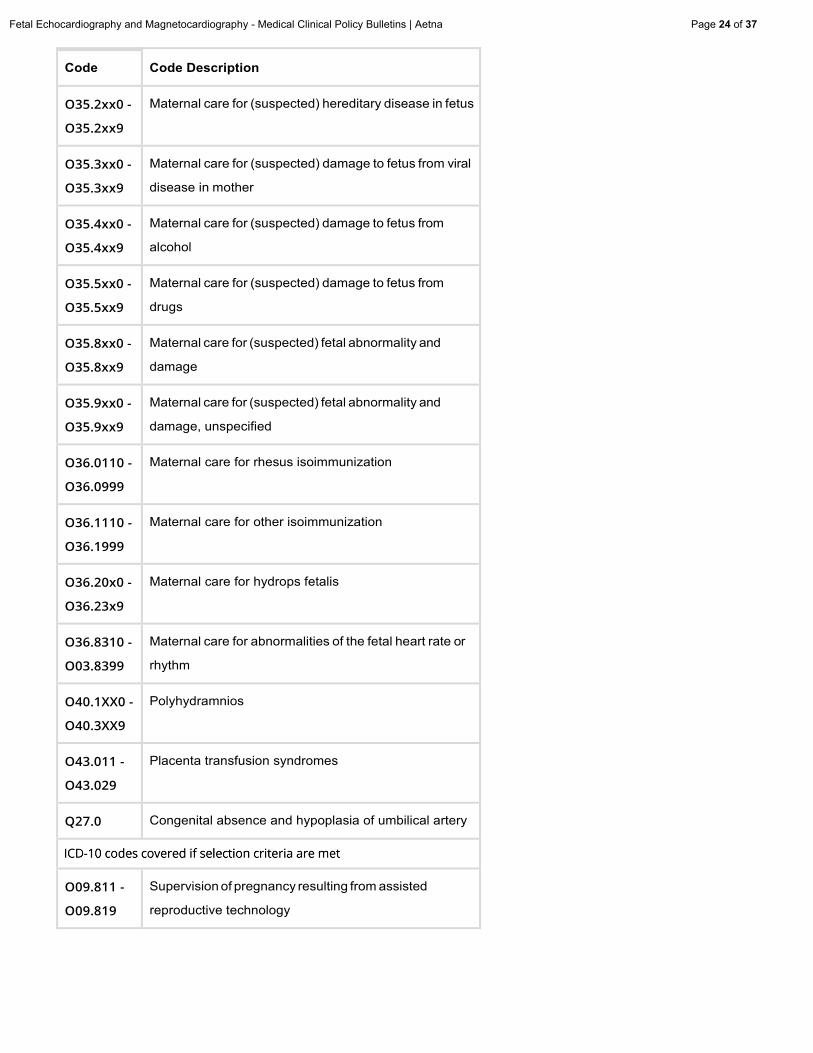
O35.2xx0
O35.2xx9
Maternal care for (suspected) hereditary disease in fetus
O35.3xx0
O35.3xx9
Maternal care for (suspected) damage to fetus from viral
disease in mother
O35.4xx0
O35.4xx9
Maternal care for (suspected) damage to fetus from
alcohol
O35.5xx0
O35.5xx9
Maternal care for (suspected) damage to fetus from
drugs
O35.8xx0
O35.8xx9
Maternal care for (suspected) fetal abnormality and
damage
O35.9xx0
O35.9xx9
Maternal care for (suspected) fetal abnormality and
damage, unspecified
O36.0110
O36.0999
Maternal care for rhesus isoimmunization
O36.1110
O36.1999
Maternal care for other isoimmunization
O36.20x0
O36.23x9
Maternal care for hydrops fetalis
O36.8310
O03.8399
Maternal care for abnormalities of the fetal heart rate or
rhythm
O40.1XX0
O40.3XX9
Polyhydramnios
O43.011
O43.029
Placenta transfusion syndromes
Q27.0 Congenital absence and hypoplasia of umbilical artery
O09.811
O09.819
Supervision of pregnancy resulting from assisted
reproductive technology
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 24 of 37
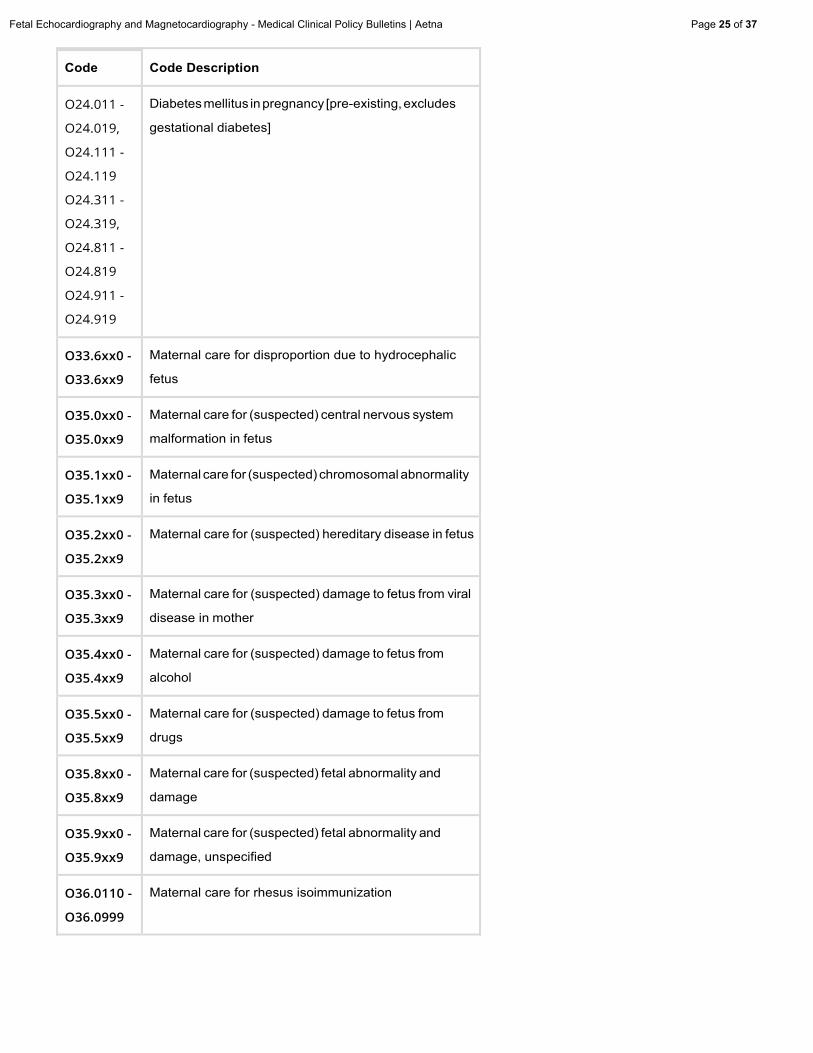
Code Code Description
O24.011 -
O24.019,
O24.111 -
O24.119
O24.311 -
O24.319,
O24.811 -
O24.819
O24.911 -
O24.919
Diabetes mellitus in pregnancy [pre-existing, excludes
gestational diabetes]
O33.6xx0
O33.6xx9
Maternal care for disproportion due to hydrocephalic
fetus
O35.0xx0
O35.0xx9
Maternal care for (suspected) central nervous system
malformation in fetus
O35.1xx0
O35.1xx9
Maternal care for (suspected) chromosomal abnormality
in fetus
O35.2xx0
O35.2xx9
Maternal care for (suspected) hereditary disease in fetus
O35.3xx0
O35.3xx9
Maternal care for (suspected) damage to fetus from viral
disease in mother
O35.4xx0
O35.4xx9
Maternal care for (suspected) damage to fetus from
alcohol
O35.5xx0
O35.5xx9
Maternal care for (suspected) damage to fetus from
drugs
O35.8xx0
O35.8xx9
Maternal care for (suspected) fetal abnormality and
damage
O35.9xx0
O35.9xx9
Maternal care for (suspected) fetal abnormality and
damage, unspecified
O36.0110
O36.0999
Maternal care for rhesus isoimmunization
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 25 of 37
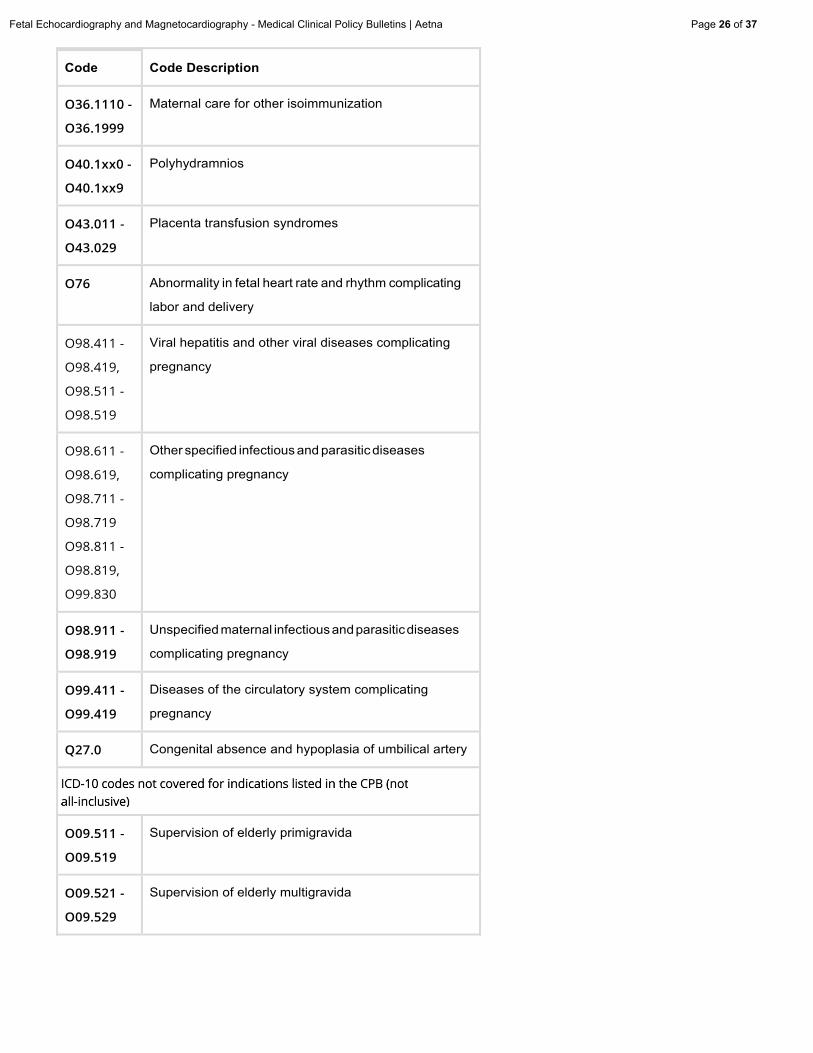
Code Code Description
O36.1110
O36.1999
Maternal care for other isoimmunization
O40.1xx0 -
O40.1xx9
Polyhydramnios
O43.011
O43.029
Placenta transfusion syndromes
O76 Abnormality in fetal heart rate and rhythm complicating
labor and delivery
O98.411 -
O98.419,
O98.511 -
O98.519
Viral hepatitis and other viral diseases complicating
pregnancy
O98.611 -
O98.619,
O98.711 -
O98.719
O98.811 -
O98.819,
O99.830
Other specified infectious and parasitic diseases
complicating pregnancy
O98.911
O98.919
Unspecified maternal infectiousandparasiticdiseases
complicating pregnancy
O99.411
O99.419
Diseases of the circulatory system complicating
pregnancy
Q27.0 Congenital absence and hypoplasia of umbilical artery
O09.511
O09.519
Supervision of elderly primigravida
O09.521
O09.529
Supervision of elderly multigravida
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 26 of 37
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 27 of 37
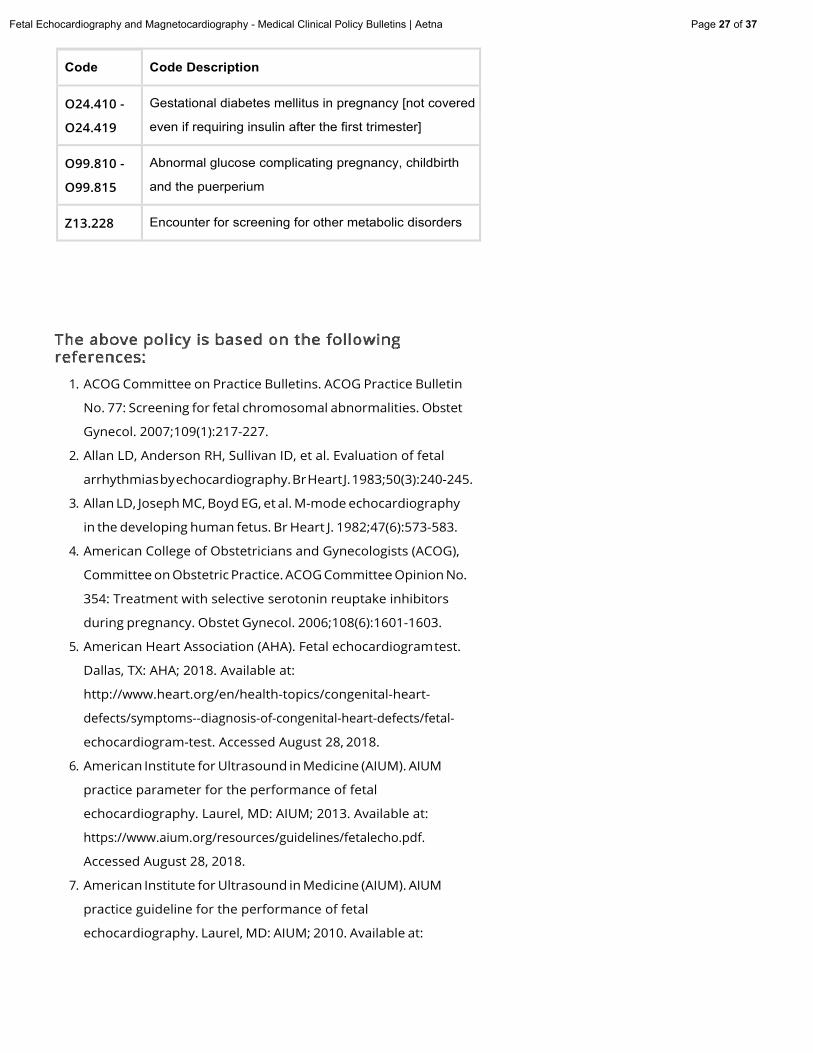
Code Code Description
O24.410
O24.419
Gestational diabetes mellitus in pregnancy [not covered
even if requiring insulin after the first trimester]
O99.810
O99.815
Abnormal glucose complicating pregnancy, childbirth
and the puerperium
Z13.228 Encounter for screening for other metabolic disorders
1. ACOG Committee on Practice Bulletins. ACOG Practice Bulletin
No. 77: Screening for fetal chromosomal abnormalities. Obstet
Gynecol. 2007;109(1):217-227.
2. Allan LD, Anderson RH, Sullivan ID, et al. Evaluation of fetal
arrhythmiasbyechocardiography.BrHeartJ.1983;50(3):240-245.
3. Allan LD, Joseph MC, Boyd EG, et al. M-mode echocardiography
in the developing human fetus. Br Heart J. 1982;47(6):573-583.
4. American College of Obstetricians and Gynecologists (ACOG),
Committee on Obstetric Practice. ACOG Committee Opinion No.
354: Treatment with selective serotonin reuptake inhibitors
during pregnancy. Obstet Gynecol. 2006;108(6):1601-1603.
5. American Heart Association (AHA). Fetal echocardiogramtest.
Dallas, TX: AHA; 2018. Available at:
http://www.heart.org/en/health-topics/congenital-heart
defects/symptoms--diagnosis-of-congenital-heart-defects/fetal
echocardiogram-test. Accessed August 28, 2018.
6. American Institute for Ultrasound in Medicine (AIUM). AIUM
practice parameter for the performance of fetal
echocardiography. Laurel, MD: AIUM; 2013. Available at:
https://www.aium.org/resources/guidelines/fetalecho.pdf.
Accessed August 28, 2018.
7. American Institute for Ultrasound in Medicine (AIUM). AIUM
practice guideline for the performance of fetal
echocardiography. Laurel, MD: AIUM; 2010. Available at:
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 28 of 37
https://www.smfm.org/attachedfiles/fetalEchoaiumsmfm.pdf.
Accessed October 25, 2010.
8. Azancot A, Caudell TP, Allen HD, et al. Analysis of ventricular
shape by echocardiography in normal fetuses, newborns, and
infants. Circulation. 1983;68:1201-1211.
9. Bahtiyar MO, Dulay AT, Weeks BP, et al. Prevalence of congenital
heart defects in monochorionic/diamniotic twin gestations: A
systematic literaturereview. J Ultrasound Med. 2007;26(11):1491
1498.
10. Berghella V, Pagotto L, Kaufman M, et al. Accuracy of prenatal
diagnosis of congenital heart defects. Fetal Diagn Ther.
2001;16(6):407-412.
11. Budorick NE, Kelly TF, Dunn JA, Scioscia AL. The single umbilical
artery in a high-risk patient population: What should be offered? J
Ultrasound Med. 2001;20(6):619-627.
12. Canavan TP, Hill LM. Neonatal outcomes in fetuses with a
persistent intrahepatic right umbilical vein. J Ultrasound Med.
2016;35(10):2237-2241.
13. Cheitlin MD, Alpert JS, Armstrong WF, et al. ACC/AHA Guidelines
for the clinical application of echocardiography: Executive
summary. A report of the American College of
Cardiology/American Heart Association Task Force on practice
guidelines (Committee on Clinical Application of
Echocardiography). Developed in collaboration with the
American Society of Echocardiography. J Am Coll Cardiol.
1997;29(4):862-879.
14. Cheitlin MD, Armstrong WF, Aurigemma GP, et al. ACC/AHA/ASE
2003 guideline update for the clinical application of
echocardiography--summary article: A report of the American
College of Cardiology/American Heart Association Task Force on
Practice Guidelines (ACC/AHA/ASE Committee to Update the
1997 Guidelines for the Clinical Application of Echocardiography).
J Am Coll Cardiol. 2003;42(5):954-970.
15. Chen HY, Lu CC, Cheng YT, et al. Antenatal measurement of fetal
umbilical venous flow by pulsed Doppler and B-mode
ultrasonography. J Ultrasound Med. 1986;5:319-321.
16. Copel J. Fetal cardiac abnormalities: Screening, evaluation, and
pregnancy management. UpToDate [online serial]. Waltham, MA:
UpToDate; reviewed December 2015.
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 29 of 37
17. Copel JA, Pilu G, Kiemman CS. Congenital heart disease and
extracardiac anomalies: Associations and indications for fetal
echocardiography.AmJ ObstetGynecol.1986;541:1121-1132.
18. Cristina MP, Ana G, Inés T, et al. Perinatal results following the
prenatal ultrasound diagnosis of single umbilical artery. Acta
Obstet Gynecol Scand. 2005;84(11):1068-1074.
19. Cyr DR, Guntheroth WO, Mack LA, et al. A systematic approach to
fetal echocardiography using real-time/A two-dimensional
sonography. J Ultrasound Med. 1986;5(6):343-350.
20. Desilets V, Audibert F; Society of Obstetrician and Gynaecologists
of Canada. Investigation and management of non-immune fetal
hydrops. J Obstet Gynaecol Can.2013;35(10):923-938.
21. DeVore OR, Donnerstein RL, Kiemman CS, et al. Fetal
echocardiography. I. Normal anatomy as determined by real
time-directed M-mode ultrasound. Am J Obstet Gynecol.
1982;144:249-260.
22. DeVore OR, Donnerstein RL, Klemman CS, et al. Fetal
echocardiography. II. The diagnosis and significance of a
pericardial effusion in the fetus using real-time-directed M-mode
ultrasound. Am J Obstet Gynecol.1982;144:693-700.
23. DeVore OR, Platt LD. The random measurement of the
transverse diameter of the fetal heart: A potential source of
error. J Ultrasound Med. 1985;4:335-341.
24. DeVore OR, Siassi B, Platt LD. Fetal echocardiography. IV. M-
mode assessment of ventricular size and contractility during the
second and third trimesters of pregnancy in the normal fetus.
Am J Obstet Gynecol. 1984;150:981-988.
25. DeVore OR, Siassi B, Platt LD. Fetal echocardiography. V. M-mode
measurements of the aortic root and aortic valve in second and
third trimester normal human fetuses. Am J Obstet Gynecol.
1985;152:543-550.
26. Donofrio MT, Moon-Grady AJ, Hornberger LK et al. Diagnosis and
treatment of fetal cardiac disease: A scientific statement from the
AmericanHeart Association. Circulation. 2014;129(21):2183-242.
27. Driggers RW, Spevak PJ, Crino JP, et al. Fetal anatomic and
functional echocardiography: A 5-year review. J Ultrasound Med.
2003;22(1):45-51.
28. Eswaran H, Escalona-Vargas D, Bolin EH, et al. Fetal
magnetocardiographyusingopticallypumpedmagnetometers:A
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 30 of 37
more adaptable and less expensive alternative? Prenat Diagn.
2017;37(2):193-196.
29. eviCore Healthcare. OB ultrasound imaging policy. Clinical
Guidelines, Version 20.0.2018. Bluffton, SC: eviCore; May 17,
2018.
30. Forbus GA, Atz AM, Shirali GS. Implications and limitations of an
abnormal fetal echocardiogram. Am J Cardiol. 2004;94(5):688
689.
31. Friedberg MK, Silverman NH. Changing indications for fetal
echocardiography in a University Center population. Prenat
Diagn. 2004;24(10):781-786.
32. Friedman AH, Copel JA, Kleinman CS. Fetal echocardiography and
fetal cardiology: Indications, diagnosis and management. Semin
Perinatol. 1993;17(2):76-88.
33. Frommelt MA, Frommelt PC. Advances in echocardiographic
diagnostic modalities for the pediatrician. Pediatr Clin North Am.
1999;46(2):427-439, xi.
34. Geipel A, Germer U, Welp T, et al. Prenatal diagnosis of single
umbilical artery: Determination of the absent side, associated
anomalies,Doppler findingsandperinataloutcome.Ultrasound
Obstet Gynecol. 2000;15(2):114-117.
35. Gijtenbeek M, Eschbach SJ, Middeldorp JM, et al. The value of
echocardiography and Doppler in the prediction of fetal demise
after laser coagulation for TTTS: A systematic review and meta-
analysis. Prenat Diagn. 2019;39(10):838-847.
36. Gomez O, Soveral I, Bennasar M, et al. Accuracy of fetal
echocardiography in the differential diagnosis between truncus
arteriosus and pulmonary atresia with ventricular septal defect.
Fetal Diagn Ther. 2016;39(2):90-99.
37. Gossett DR, Lantz ME, Chisholm CA. Antenatal diagnosis of single
umbilical artery: Is fetal echocardiography warranted? Obstet
Gynecol. 2002;100(5 Pt 1):903-908.
38. Granese R, Coco C, Jeanty P. The value of single umbilicalartery
in the prediction of fetal aneuploidy: Findings in 12,672 pregnant
women. Ultrasound Q. 2007;23(2):117-121.
39. Gupta S, Gupta N. Sjögren syndrome and pregnancy: A literature
review. Perm J. 2017;21:16-047.
40. Hansen M, Bower C, Milne E, et al. Assisted reproductive
technologies and the risk of birth defects -- a systematic review.
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 31 of 37
Hum Reprod. 2005;20(2):328-338.
41. Hansen M, Kurinczuk JJ, Bower C, Webb S. The risk of major birth
defects after intracytoplasmic sperm injection and in vitro
fertilization. N Engl J Med. 2002;346(10):725-730.
42. Hill LM, Mills A, Peterson C, Boyles D. Persistent right umbilical
vein: Sonographic detection and subsequent neonatal outcome.
Obstet Gynecol. 1994;84(6):923-925.
43. Hirata T, Osuga Y, Fujimoto A, et al. Conjoined twins in a triplet
pregnancyafter intracytoplasmic sperminjection and blastocyst
transfer: Case report and review of the literature. Fertil Steril.
2009;91(3):933.e9-e12.
44. Hrtankova M, Biringer K, Sivakova J, et al. Fetal
magnetocardiography: A promising way to diagnose fetal
arrhytmia and to study fetal heart rate variability?. Ceska
Gynekol. 2015;80(1):58-63.
45. Huggon IC, Ghi T, Cook AC, et al. Fetal cardiac abnormalities
identified prior to 14 weeks' gestation. Ultrasound Obstet
Gynecol. 2002;20(1):22-29.
46. Huhta JC, Strasburger JF, Carpenter RJ, et al. Pulsed Doppler fetal
echocardiography. J Clin Ultrasound.1985;13:247-254.
47. Hutchinson D, McBrien A, Howley L, et al. First-trimester fetal
echocardiography: Identification of cardiac structures for
screening from 6 to 13 Weeks' Gestational Age. J Am Soc
Echocardiogr. 2017;30(8):763-772.
48. Johnson B, Simpson LL. Screening for congenital heart disease: A
move toward earlier echocardiography. Am J Perinatol.
2007;24(8):449-456.
49. Keinman CS, Hobbins JC, Jaffe CC, et al. Echocardiographic
studies of the human fetus: Prenatal diagnosis of congenital
heart disease and cardiac dysrhythmias. Pediatrics.
1980;65:1059-1067.
50. Kiemman CS, Copel JA, Weinstein EM, et al. Treatment of fetal
supraventricular tachyarrhythmias. J Clin Ultrasound.
1985;13:265-273.
51. Kiemman CS, Donnerstein RY, DeVore OR. Fetal
echocardiography for evaluation of in utero congestive cardiac
failure: A technique for study of non-immune hydrops. N Engl J
Med. 1982;306:568-575.
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 32 of 37
52. Koivurova S, Hartikainen AL, Gissler M, et al. Neonatal outcome
and congenital malformations in children born after in-vitro
fertilization. Hum Reprod. 2002;17(5):1391-1398.
53. Kumar SV, Chandra V, Balakrishnan B, et al. A retrospective
single centre review of the incidence and prognostic significance
of persistent foetal right umbilical vein. J Obstet Gynaecol.
2016;36(8):1050-1055.
54. Kurinczuk JJ, Bower C. Birth defects in infants conceived by
intracytoplasmicsperminjection:Analternative interpretation.
BMJ. 1997;315(7118):1260-1265.
55. Levine JC, Alexander ME. Overview of the general approach to
diagnosis and treatment of fetal arrhythmias. UpToDate [online
serial]. Waltham, MA: UpToDate; reviewed May2017.
56. Li M, Wang W, Yang X, et al. Evaluation of referral indications for
fetal echocardiography in Beijing. J Ultrasound Med.
2008;27(9):1291-1296.
57. Lide B, Lindsley W, Foster MJ, et al. Intrahepatic persistent right
umbilical vein and associated outcomes: A systematic review of
the literature. J Ultrasound Med. 2016;35(1):1-5.
58. Lubusky M, Dhaifalah I, Prochazka M, et al. Single umbilical artery
and its siding in the second trimester of pregnancy: Relation to
chromosomal defects. Prenat Diagn.2007;27(4):327-331.
59. Mapp T. Fetal echocardiography and congenital heart disease.
Prof Care Mother Child. 2000;10(1):9-11.
60. Marques Carvalho SR, Mendes MC, Poli Neto OB, Berezowski AT.
First trimester fetal echocardiography. Gynecol Obstet Invest.
2008;65(3):162-168.
61. Martínez R, Gamez F, de Leon-Luis J, et al. Perinatal outcomes
after prenatal ultrasound diagnosis of persistence of right
umbilical vein. Ginecol Obstet Mex.2012;80(2):73-78.
62. Maulik D, Nanda NC, Saini VD. Fetal Doppler echocardiography:
Methods and characterization of normal and abnormal
hemodynamics. Am J Cardiol. 1984;53:572-578.
63. McAuliffe FM, Trines J, Nield LE, et al. Early fetal
echocardiography--a reliable prenatal diagnosis tool. Am J Obstet
Gynecol. 2005;193(3 Pt 2):1253-1259.
64. McCue CM, Mantakas ME, Tinglestad JB, et al. Congenital heart
block in newborns of mothers with connective tissue disease.
Circulation. 1977;56:82-89.
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 33 of 37
65. Nora JJ, Nora AH. The evolution of specific genetic and
environmental counseling in congenital heart diseases.
Circulation. 1978;57:205-213.
66. Palazzi DL, Brandt ML. Care of the umbilicus and management of
umbilical disorders. UpToDate [online serial]. Waltham, MA:
UpToDate; 2009.
67. Pierce BT, Dance VD, Wagner RK, et al. Perinatal outcome
following fetal single umbilical artery diagnosis. J Matern Fetal
Med. 2001;10(1):59-63.
68. Prucka S, Clemens M, Craven C, McPherson E. Single umbilical
artery: What does it mean for the fetus? A case-control analysis
ofpathologicallyascertained cases.GenetMed. 2004;6(1):54-57.
69. Randall P, Brealey S, Hahn S, et al. Accuracy of fetal
echocardiography in the routine detection of congenital heart
disease among unselected and low risk populations: A systematic
review. BJOG. 2005;112(1):24-30.
70. Reed KL, Sahn DJ, Scagnelli S, et al. Doppler echocardiographic
studies of diastolic function in the human fetal heart: Changes
during gestation. J Am Coll Cardiol.1986;8:391-395.
71. Reefhuis J, Devine O, Friedman JM, etal; and the National Birth
Defects Prevention Study. Specific SSRIs and birth defects:
Bayesian analysis to interpret new data in the context of
previous reports. BMJ. 2015;351:h3190.
72. Reefhuis J, Honein MA, Schieve LA, et al; National Birth Defects
Prevention Study. Assisted reproductive technology and major
structural birth defects in the United States. Hum Reprod.
2009;24(2):360-366.
73. Rinehart BK, Terrone DA, Taylor CW, et al. Single umbilical artery
is associated with an increased incidence of structural and
chromosomal anomalies and growth restriction. Am J Perinatol.
2000;17(5):229-232.
74. Royal College of Obstetricians and Gynaecologists (RCOG).
Management of monochorionic twin pregnancy. London, UK:
Royal College of Obstetricians and Gynaecologists (RCOG);
December 2008.
75. Rychik J, Ayres N, Cuneo B, et al. American Society of
Echocardiography guidelines and standards for performance of
the fetal echocardiogram. J Am Soc Echocardiogr. 2004;17(7):803-
810.
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 34 of 37
76. Sahn DJ. Resolution and display requirements for
ultrasound/Doppler evaluation of the heart in children, infants
and unborn human fetus. J Am Coll Cardiol. 1985;5(Suppl 1):12S
19S.
77. Schulman H, Fleischer A, Stern W, et al. Umbilical velocity wave
ratios in human pregnancy. Am J Obstet Gynecol. 1984;148:985-
990.
78. Shime J, Gresser CD, Rakowski H. Quantitative two-dimensional
echocardiographic assessment of fetal growth. Am J Obstet
Gynecol. 1986;154:290-300.
79. Silverman NH, Enderlein MA, Stanger P, et al. Recognition of fetal
arrhythmias by echocardiography. J Clin Ultrasound.
1985;13:255-263.
80. Silverman NH, Golbus MS. Echocardiographic techniques for
assessing normal and abnormal fetal cardiac anatomy. J Am Coll
Cardiol. 1985;5(Suppl 1):20S-29S.
81. Simpson LL. Indications for fetal echocardiography from a
tertiary-care obstetricsonographypractice. J Clin Ultrasound.
2004;32(3):123-128.
82. Smith V, Nair A, Warty R, et al. A systematic review on the utility
of non-invasive electrophysiological assessment in evaluating
for intra uterine growth restriction. BMC Pregnancy Childbirth.
2019;19(1):230.
83. Society for Maternal-Fetal Medicine (SMFM), Norton ME,
Chauhan SP, Dashe JS. Society for maternal-fetal medicine
(SMFM) clinical guideline #7: Nonimmune hydrops fetalis. Am J
Obstet Gynecol. 2015;212(2):127-139.
84. Spurway J, Logan P, Pak S. The development, structure and blood
flow within the umbilical cord with particular reference to the
venous system. Australasian Journal of Ultrasound in Medicine.
2012;15(3):97-102.
85. Srinivasan S. Fetal echocardiography. Indian J Pediatr.
2000;67(7):515-521.
86. St. John Sutton MG, Oewitz MH, Shah B, et al. Quantitative
assessment of growth and function of the cardiac chambers in
the normal human fetus: A prospective longitudinal
echocardiographic study. Circulation.1984;69(4):645-654.
87. Thummala MR, Raju TN, Langenberg P. Isolated single umbilical
artery anomaly and the risk for congenital malformations: A
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 35 of 37
meta-analysis. J Pediatr Surg. 1998;33(4):580-585.
88. Tometzki AJ, Suda K, Kohl T, et al. Accuracy of prenatal
echocardiographic diagnosis and prognosis of fetuses with
conotruncalanomalies. J AmColl Cardiol.1999;33(6):1696-1701.
89. Ventriglia F, Caiaro A, Giancotti A. et al. Reliability of early fetal
echocardiography for congenital heart disease detection: A
preliminary experience and outcome analysis of 102 fetuses to
demonstrate the value of a clinical flow-chart designed for at-risk
pregnancy management. Pediatrics & Therapeutics. 2016; 6:270.
90. Wilson KL, Czerwinski JL, Hoskovec JM, et al. NSGC practice
guideline: Prenatal screening and diagnostic testing options for
chromosome aneuploidy. J Genet Couns. 2013;22(1):4-15.
91. Winsberg F. Echocardiography of the fetal and newborn heart.
Invest Radiol. 1972;3:152-158.
92. Wolman I, Gull I, Fait G, et al. Persistent right umbilical vein:
Incidence and significance. Ultrasound Obstet Gynecol.
2002;19(6):562-564.
93. Yacobi S, Ornoy A. Is lithium a real teratogen? What can we
conclude from the prospective versus retrospective studies? A
review. Isr J Psychiatry Relat Sci.2008;45(2):95-106.
94. Yu D, Sui L, Zhang N. Performance of first-trimester fetal
echocardiography in diagnosing fetal heart defects: Meta-
analysis and systematic review. J Ultrasound Med.
2020;39(3):471-480.
95. Zhang YF, Zeng XL, Zhao EF, Lu HW. Diagnostic value of fetal
echocardiographyfor congenital heart disease: A systematic
review and meta-analysis. Medicine (Baltimore).
2015;94(42):e1759.

Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 36 of 37
Copyright Aetna Inc. All rights reserved. Clinical Policy Bulletins are developed by Aetna to assist in administering plan benefits and
constitute neither offers of coverage nor medical advice. This Clinical Policy Bulletin contains only a partial, general description of plan or
program benefits and does not constitute a contract. Aetna does not provide health care services and, therefore, cannot guarantee any
results or outcomes. Participating providers are independent contractors in private practice and are neither employees nor agents of Aetna
or its affiliates. Treating providers are solely responsible for medical advice and treatment of members. This Clinical Policy Bulletin may be
updated and therefore is subject to change.
Copyright © 2001-2021 Aetna Inc.
Fetal Echocardiography and Magnetocardiography - Medical Clinical Policy Bulletins | Aetna Page 37 of 37
AETNA BETTER HEALTH® OF PENNSYLVANIA
Amendment to Aetna Clinical Policy Bulletin Number: 0106 Fetal
Echocardiography and Magnetocardiography
There are no amendments for Medicaid.
revised 02/24/2021





























