Embed Size (px)
Citation preview

Implementation of a Venous Implementation of a Venous Thromboembolism (VTE) Prevention Thromboembolism (VTE) Prevention
Program Across VCHProgram Across VCH
Vancouver Coastal Health Quality and Patient Safety
Claire O’Quinn

Vancouver Coastal Health Authority
• Serves 25% of BC population• Over 1 million people with primary and
secondary care • 4 million people with tertiary and quaternary
care • One of 6 Health Authorities in BC• 58,560 km2 in Richmond, Vancouver, North
Shore, Sunshine Coast, Powell River and Sea to Sky communities
• 2 Denominational Affiliates

3
VCH AIM 2006Vancouver Coastal Health
Richmond Hospital
•Vancouver General Hospital•UBC Health Sciences Centre Hospital•St. Paul’s Hospital•Mount Saint Joseph Hospital
Lions Gate Hospital
Squamish General Hospital
St. Mary’s Hospital
Powell River General Hospital

• Venous thromboembolism (VTE) is …– Common: ~70% of VTE are related to hospitalization– Deadly: ~10% of all deaths in hospital – Associated with chronic, costly complications– Burdensome BC HA VTE is estimated @3000 annually
VCH = 770 a third of these patients will develop long term complication such as post-thrombic syndrome or chronic pulmonary hypertension
– Expensive: 1.5 billion in US and £640 million in UK– Preventable: most common preventable cause of death
in hospital
Why should we care?
1. Spencer Arch Intern Med 2007 4. Sadler J Royal Soc Med 1989
2. Spyropoulos Chest 2002 5. AHRQ 20013. British House of Commons 2005

Why should we care?• Thromboprophylaxis is the #1-ranked
patient safety strategy in hospitalized patients
• Venous Thromboembolism (VTE) Risk Assessment & Thromboprophylaxis are now Accreditation Canada Required Organizational Practice (ROP)
• Venous Thromboembolism (VTE) is also one of the BC MoH Key Results Area (KRP)
Agency for Healthcare and Research and Quality, Shojania 2001

The weight of evidence …• Strongly supports that prophylaxis reduces
VTE risk, including symptomatic VTE and deaths
• Demonstrates that sensible prophylaxis rarely causes clinically important bleeding or other adverse effects
• Shows that effective tools are available to implement local strategies to reduce VTE
• Indicates that prophylaxis is underutilized

Estimated VTE Burden in BC• Annual incidence of hospital-related VTE:
Population Total VTE Hosp VTE
Vancouver Coastal 1,092,358 1100 770
Fraser 1,541,479 1500 1050
Island 741,299 740 518
Interior 722,556 720 504
Northern 283,911 280 196
Total 4,381,603 4400 3080


Milestones• Project Team - April 2010• VCH-PHC Regional Policy - July 2010• VTE Regional Prevention Guidelines - Sept. 2010 • Regional PPO - Sept. 2010• Working Groups developed at each Community of
Care (Coastal, Richmond, Vancouver) - Oct. 2011• Toolkit developed - Nov. 2011

Goals VTE Program• Overall goal to improve patient safety
through compliance with evidence based guidelines on Thromboprophylaxis and to reduce the incidence of preventable hospital acquired VTE

Key Elements VTE Program• Have every patient evaluated for his/her risk
assessment of VTE on admission and transfer of service or area of care
• Prescribed thromboprophylaxis appropriate for his/her level of risk
• Document the rationale for any deviation from the recommended practice
• All patients will have Pre-printed orders (PPO) • Serves as a guideline for care providers to
provide evidence based practice

VTE Prevention is embedded in all admission pre-printed orders Thromboprophylaxis

VTE Prevention is embedded in all admission pre-printed orders Thromboprophylaxis

VTE Implementation/Spread• Timely & Effective Engagement
– Across the Organization– Across CoC and PHC– Across programs and services– Front line Staff, Physicians and Residents– Teamwork

Teamwork

Implementation Plan/Spread• Each CoC formed a VTE working group
• Pharmacists• Nursing Educator/Clinician• Physicians• Quality & Patient Safety • Unit Coordinators • Other

VTE Working GroupRoles & Responsibilities
• Identify all inpatient units requiring VTE prophylaxis • Review existing PPO than have reference VTE
prophylaxis• Decide to adopt the regional PPO or imbed the
required elements• Devise an implementation plan with timelines• Define the approach of your implementation• Identify workflow or processes that require change• Communicate the changes and new workflow• Educate Nurses, Pharmacists, Physicians etc.• Report Progress monthly to Project Group

Implementation/Spread• RH and VGH started their implementation
January 2011• VGH -Surgery chose a staggered
implementation • RH and VGH –The Medicine Program
implemented all medical units at the same time• LGH – chose a staggered approach• Coastal Rural is yet to be implemented

Implementation/Spread• Chart reviews were done post completion of
implementation and every 2 months• The results were analyzed and discussed with
the teams for process improvement• PDSA cycles were used to identify the required
system changes to ensure success.• Educational Toolkit for staff & patients
developed which could be customized for each site

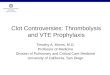
VTE Audit Results -VGH
0%
20%
40%
60%
80%
100%
Jan 11 Mar 11 May 11 July 11 Mar 12
VGH VTE Audits
% of Charts with VTE PPO# with Risk Assessement Completed% of Patients on Anticoagulants

Sustainability• Regional Chart Audits per month• 100 chart audits per facility over 100 beds• Report Audits results monthly to SLT• Report Audits results to clinical teams
monthly• Report Audits on Scoreboard• Ongoing education

Lessons Learned• Engagement is KEY
– It is continuous– All levels of the organization– It must be timely– Looks different at each level – Looks differently at each facility– Use of PSDA cycles assist with engagement

Lessons Learned• Process requiring review to facilitate
implementation– Streamline approval process for PPOs regionally &
locally– Decrease turnaround time for revisions and updates
to existing PPOs– Removal of outdated PPOs– Access to PPOs online– Determine who responsibility it is to manage on line
PPOs

Claire O’QuinnDirector, Vancouver Acute
Clinical Quality and Patient SafetyCP 381 – 855 West 12th Ave.
Vancouver, BC V5Z 1M9Tel: 604.875.4111 ext. 68450