Embed Size (px)
Citation preview

APPROACH TO
MULTIVALVULAR HEART DISEASE
Satyam Rajvanshi

HOW TO DEFINE MVHD

• Clinically significant MVHD?
• Pathological MVHD?
• VHD without organic valve ds?

• Clinically significant MVHD?
• Pathological MVHD?
• VHD without organic valve ds?
NO STANDARD DEFINITION

PRACTICAL DEFINITION

• Involvement of more than one heart valve
• Clinically significant – alters natural history, management
• Valve may or may not be pathological but must be grossly dysfunctional

WHY IS MVHD RELEVANT

• Presentation
• Natural history
• Management

• Presentation• Symptoms• Physical signs
• Natural history
• Management

• Presentation• Symptoms• Physical signs
• Natural history
• Management
Relative severity of separate lesions
Order of development of separate lesions

WHAT CAUSES MVHD

• Rheumatic Heart Disease• Infective endocarditis• Myocardial Dysfunction (Remodelled heart – MR, PR, TR)• Aging, Degenerative (calcific)• Disorders of other Organs – ESRD, Carcinoid• Myxomatous diseases – Marfan, EDS• CTDs – SLE, APLA, RA• Congenital diseases – Discrete Subaortic stenosis, HOCM,
Shone’s complex, Trisomy (13-15-18), Alkaptonuria• Endocardial Disorders• Thoracic/Mediastinal radiation therapy• Drugs – Ergotamine/Fen-Phen/Methysergide

• Significant stenosis at multiple valves are usually Rheumatic
• Significant regurgitation at multiple valves are likely Non Rheumatic
• Significant stenosis and regurgitation together are usually Rheumatic

• Quadrivalvular disease is most likely due to combination of causes – Rheumatic, infective, congenital, inflammatory or degenerative disease
• A unitary cause for quadrivalvular disease is either rheumatic or myxomatous degeneration

STATISTICS

ARF with carditis
MV 70-75%MV+AV 20-25%AV 5-8%TV 1-2%PV Rare
Ann Indian Acad Med Sci 1972;8:47-52

ARF with carditis
CLINICAL
MV 70-75%MV+AV 20-25%AV 5-8%TV 1-2%PV Rare
Ann Indian Acad Med Sci 1972;8:47-52

ARF with carditis
CLINICAL
MV 70-75%MV+AV 20-25%AV 5-8% HISTOPATHOLOGICAL
TV 1-2% 30-35%PV Rare 15-20%
Ann Indian Acad Med Sci 1972;8:47-52

ARF with carditis
MV 70-75% MC is MR
MV+AV 20-25% 90-95%
AV 5-8%TV 1-2%PV Rare
Ann Indian Acad Med Sci 1972;8:47-52

ARF with carditis
MV 70-75%MV+AV 20-25% 2nd MC is AR
AV 5-8% 20-40%
TV 1-2%PV Rare
Ann Indian Acad Med Sci 1972;8:47-52

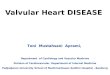
Frequency of RHD%
of p
atien
ts w
ith R
HD a
t 5-y
ears
Prognosis – Severity of carditis & Recurrences

RHD• 378 cases of juvenile RHD (<19 yr), Orrissa
MS 34.9%MR 14.8%AR 6.1%MS+MR 11.9%MS+AR 21.1%MS+MR+TS 4.8%MS+MR+TS+TR 6.4%
Indian Heart J 1999;51:653

RHD• 378 cases of juvenile RHD (<19 yr), Orrissa
MS 34.9%MR 14.8%AR 6.1%
MS+MR 11.9%MS+AR 21.1% >40% MVHDMS+MR+TS 4.8%MS+MR+TS+TR 6.4%
Indian Heart J 1999;51:653

RHD• >9000 RHD cases, Orrissa
MS 35%MR 10%AR or AS 3%MS+MR 15%MV+AV 25%MV+TV 12%
Indian Heart J 2003;55:152-157

RHD• >9000 RHD cases, Orrissa
MS 35%MR 10%AR or AS 3%
MS+MR 15%MV+AV 25% >50% MVHD
MV+TV 12%
Indian Heart J 2003;55:152-157

RHD• 518 RHD cases, JIPMER Pondicherry
MS+AS+TS 2.5%(Triple stenosis)
Indian Heart J 1999;51:667

RHD• NIMS, Hyderabad 2002
MS+MR 12.9%AS+AR 4.4%
MS+AR 13.9%MS+MR+AR 2.0%MS+MR+TR 8%MS+AR+TR 8%

RHD• 434 RHD AUTOPSY cases, Mumbai
MV 21%AV 2%
MV+AV 21%MV+AV+TV 27%MV+TV 5%MV+TV+PV 2%MV+AV+TV+PV 19%
Indian Heart J 2002;54:676-80

WHEN DO WE SUSPECT A MVHD

• Patient does not fit in single valve picture• By history/examination/ECG/CXR
• Presentation time frame different from usual natural history

• Know the classical markers of significant lesions

HISTORY-WISE

MS
• Exertional dyspnoea – 1st and MC symptom– PND– Orthopnea– 5-10 yrs from ARF to symptoms (15-20 yrs in
western population) – Progresses over 3-5 yrs from NYHA II to IV
(5-10 yrs in western population)• Hemoptysis• Systemic embolism• RVF – but after NYHA IV state

MR
• History– Long asymptomatic period – 10-20 yrs from ARF to
symptoms (a decade longer than MS)– Once severe MR – Symptomatic within 6-10 yrs– Symptoms herald LVSD or AF – Rapid decline in
survival• Chronic weakness/Fatigue/Exercise Intolerance
– MC • Dyspnoea – less common and late

AS
• History– Long asymptomatic period – 10-20 yrs from ARF to
symptoms (a decade longer than MS)– 10-15 yrs from Mild to Severe AS– Once severe AS – Symptomatic within 2 yrs– Symptoms – Rapid decline in survival
– 2 HF/3 Syncope/5 Angina• Exercise intolerance and dyspnoea – MC• Exertional Angina• Exertional Presyncope (> than Syncope)

AR
• Long (perhaps longest!) asymptomatic period – After ARF– After development of AR– Once symptomatic – course similar to AS
• Exercise intolerance and dyspnoea - MC• Palpitations – exertional and resting – even
painful! – may precede other symptoms by months-yrs
• Nocturnal (and exertional) angina

TS
• Never solitary• RVF – (Tender hepatomegaly, ascites,
anasarca) – without disabling dyspnoea• Fatigue/Exercise intolerance more prominent
than dyspnoea – d/t low CO

EXAMINATION-WISE

Severe MS
• Prolonged diastolic murmur• Thrill• A2 OS gap• Pulmonary hypertension• Cardiomegaly• Congestive Heart failure

A2-OS Gap
• Inversely proportional to severity• 40 – 120 msec• HR, LAP, LV EDP, LV compliance, mobility• Narrow always tight MS• Widened (falsely)– Bradycardia– AR– Low output (Sev PAH, TR, CHF)– Inc LV EDP (LV dysfunction)

Severe MR
• Cardiomegaly• LV S3/diastolic murmur• Wide split S2• ? Thrill• LV dysfunction• Pulmonary hypertension• Congestive Heart failure

Severe AS• Pulsus parvus et tardus• Peaking of systolic murmur• Paradoxical split S2• LV S4• Apico-carotid delay (often neglected)• Thrill• Cardiomegaly• LV dysfunction (S3)• Pulmonary hypertension• Congestive Heart failure

Severe AR
• Hill’s Sign• Duration of diastolic murmur• Austin Flint murmur• Thrill (rare)• Cardiomegaly• LV S3• LV dysfunction• Pulmonary hypertension• Congestive Heart failure

Things that Stand are
• AV disease– Pulse– Hill’s sign
• Murmur characteristic (except MR)• Diastolic thrill• S2– Paradoxical spilt – AS– Wide split – MR
• A2 OS gap - mostly

HOW TO APPROACH
MS/MR/AS/AR SEVERE?
MVHD SUSPECTED?
EXAMINEECG/ECHO/CATH
WHICH ONE IS DOMINANT?
MODIFYING / PRECIPITATING
FACTORS?
DIAGNOSISPROGNOSTICATE
MANAGEMENTGDM

Non valvular Factors
Modify/Precipitate presentation– Arrhythmias– Infective endocarditis– RF recurrence – valvulitis and myocarditis– Volume overload states – Anemia, worsening
Renal failure, Dietary non-compliance– Pressure overload states – Uncontrolled HTN– Ischemia – CAD/ACS, Respiratory illness, altitude– SIRS – Infection, MC Pneumonia

Non valvular Factors
Modify/Precipitate presentation– Arrhythmias– Infective endocarditis– RF recurrence – valvulitis and myocarditis– Volume overload states – Anemia, worsening
Renal failure, Dietary non-compliance– Pressure overload states – Uncontrolled HTN– Ischemia – CAD/ACS, Respiratory illness, altitude– SIRS – Systemic Infection, MC Pneumonia

Some Rules of Combined Valve Lesions
Severe lesions
dominate
Proximal lesions
dominate
Multivalvular disease – 1+1 may not be 2• Ability to
compensate

MS/MR

Severe MR – Is there MS?
• Thrill
• Prolonged MDM
• Opening Snap
• Loud S1
• Severe PAH

Pulmonary symptoms: Cough, Hemoptysis, Pulmonary Edema
S2 Variable Wide splitS1 Loud (mostly) VariablePAH Severe Variable
OS +

AS/AR

Severe AR - is there AS?
• Pulse
• Systolic decapitation
• Late peaking, harsher, louder murmur
• Heaving apical impulse
• Thrill

S2 Paradoxical Normal/NarrowS4 + -Apex Heaving, Not shifted Hyperkinetic, shifted
Hill’s Sign

MS/AR


MS Vs. Austin Flint
Characteristic MS Austin Flint
Diastolic Murmur Prolonged with thrill Soft/shorterApex RV
TappingLV
Hyperkinetic
Added sounds OS S3
PAH Severe mild
S1 Loud (mostly) -
AF Suggestive -
Hand grip

MS/AS

In severe AS – presence of loud S1, absence of S4 - indicates MS

MR/AR


• Exception to proximal distal rule – AR usually predominates in physical signs
• In Severe MR, mild-mod AR well tolerated• In Severe AR, even mild-mod MR worsens
symptoms as LV dilates further

MR/AS


+ TS

TS• Easily escapes detection• More fatigue, CHF/RVF - Less PND orthopnea• Distal lesions SYMPTOMS masked, signs may remain
prominent• JVP is the key
– Giant a waves– Slow Y descent
• Pulsatile liver• Murmur of TS
– Location– Pre systolic or mid diastolic– Inspiratory augmentation


TR
Characteristic High pressure Low pressure
Murmur PSM Early systolic with
variable duration
Pitch High low
Shape PSM Decrescendo
P2 Loud Normal
JVP CV waves Variable

INVESTIGATIONAL CAVEATS

• Doppler-echocardiographic methods have been validated in single valve disease but not in multivalve disease
• Interactions between different valve lesions.• Methods that depend less on loading
conditions are preferred, such as direct planimetry of the stenotic valves

Diagnostic caveats in MVHD

MANAGEMENT




• In the EuroHeart Survey, the operative risk ranged from 0.9% to 3.9% for single valve interventions and rose to 6.5% in cases of multiple valve disease
Ann Thorac Surg 1999;67:943-51
• In the Society of Thoracic Surgeons National Database, mortality was 4.3% and 6.4% for isolated aortic and mitral valve replacement, respectively, to 9.6% for multiple valve replacement (Doubles)
Eur Heart J 2003;24:1231-43

• TVR: overall operative mortality was 22 %
Ann Thorac Surg 2005;80:845-850
• Operative mortality was similar for TVR 13% vs. repair 18% p = 0.64.
• Higher mortality for higher NYHA class
Ann Thorac Surg 2009;87:83-89

CONCLUSION

MVHD
• Widely prevalent• Alters natural history and presentation• Requires careful evaluation• Management guidelines differ

La Clairvoyance, 1936 By Rene Magritte