Embed Size (px)
Citation preview

1
Valvular Heart DiseaseB K Singh, MD, FACC
Disclosures: None

2
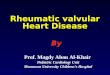
S1S4S3
S2 S2=A2P2
S1=M1T1
CARDIAC CYCLE

3
JVPCarotid
S1Slitting of S2
S3S4
Ejection clickOpening snap
Dynamic Auscultation
What is the most important part of the stethoscope?

4
Pre Test – True or False?
Loud S1 is consistent with severe MRParadoxical splitting of S2 rules out severe ASDelayed carotid upstroke suggests severe ASMurmur of valvular aortic stenosis increases with ValsalvaMurmur of HCM and MVP increases on standingNormal peak velocity of blood flow across aortic valve is 5m/sec (Doppler Echo)Development of pressure gradient across the valve indicates stensis. Asymptomatic but severe aortic stenosis needs urgent surgery.Send patient with CP and new onset diastolic murmur to ER
Pre Test- True or False?
Asymptomatic but severe MR with LVEF 0.45, needs MV surgery.All symptomatic valvular disease needs intervention.Mild MR and Mild AS need echocardiogram every year.Cardiac catheterization is needed in all patients to confirm the severity of valvular stenosis or regurgitation. Endocarditis prophylaxis is needed in patient with MVP and moderate MR.Percutaneous Trans Catheter Aortic Valve Replacement (TAVR) is indicated in a patient who refuses to have surgical AVR.EF = Stroke Volume/End diastolic volume. 0.60 normal

5
Valvular Heart Disease
• Etiology, Severity• Pathophysiology• Clinical Presentation• Testing: Echo/Doppler/Color Flow/Heart
Cath/EKG/X-ray• Natural History• Treatment
LVRV
LV
RA LA
LA
RA
Aortic Valve
Echocardiography

6
LA
LVLV
LA
LV
LA
AO
Echocardiography
AO
LA
LV
LA
LV
AO
PW Doppler
CW Doppler
Echocardiography

7
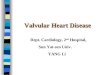
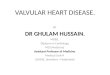
Critical Aortic StenosisCritical Aortic Stenosis
BernoulliEquationBernoulliEquation
PG = 4 V2PG = 4 V2
Catheterization vs DopplerCatheterization vs Doppler
max57
p-p 28
(55 mmHg)
Aortic StenosisAortic Stenosis

8
Valvular Aortic Stenosis
• Age- related etiology
• <30: Congenital (Unicuspid, Bicuspid)
• 40-60: Calcified bicuspid
• 40-60: Rheumatic
• >70: Senile degenerative/ Calcific
• Most common cause
• Senile degenerative
Classification of Disease Severity
ACC/AHA Guidelines
SevereModerateMild
< 0.6Valve Areacm2/m2
< 1.01.0 – 1.5> 1.5Valve Areacm2
> 4025 – 40< 25Mean Gradientmm Hg
> 4.03.0 – 4.0< 3.0Jet Velocitym/sec

9
Valvular Aortic Stenosis in Adults Average Course (Post Mortem Data)
Ross, Bruanwald: Circulation 1968: 38 (Supp V)
SymptomsSymptoms
MeanGradient
Clinical examination
AorticValveArea= =
Correlating Symptoms & Severity
Correlating Symptoms & Severity

10
Indications for AVR in Aortic Stenosis
• Symptomatic: Severe AS: irrespective of LVEF• Asymptomatic: Severe AS:• LVEF < 50• Abnormal Treadmill• Critical Aortic Stenosis• Moderate Aortic Stenosis: concomitant open heart surgery
like CABG, Aortic Aneurysm, Mitral Valve surgery• Low flow/low gradient/low aortic valve area: Dobutamine Echo• True critical AS with poor LVEF• Low LVEF with inability to open valve• SAVR vs TAVR
Bicuspid Aortic Valve
Screen first degree
relatives
Screen first degree
relatives
CoarctationDissectionAneurysm
Ascending AO 5 camsAscending AO 4.5 cms
Need surgery
CoarctationDissectionAneurysm
Ascending AO 5 camsAscending AO 4.5 cms
Need surgery
Scan entire aorta
(MRA or CTA)

11
Aortic Regurgitation
• Acute vs Chronic : Recognize the difference in Murmur intensity and symptoms and signs
• Acute AR: Endocarditis/ Aortic Dissection
• Chronic AR: Valvular: Degenerative/ Bicuspid/RHD
• Aortic root Disease: Aneurysm/ Marfan
• Indications of AVR: Symptomatic & Severe AR
Asymptomatic & Severe
LVEF <50 %
LVESD>50 mm
Suboptimal Treadmill test
Severe ARWide pulse pressureColor DopplerRV 60mlRF 55%ERO 0.3 cm2Descending aorta flow reversal
Mitral Regurgitation
• Acute vs Chronic
• Acute MR: Ruptured Papillary Muscle, Chordal Rupture, Endocarditis, ischemic
• Chronic MR: MVP, ischemic, Rheumatic,Endocarditis, LV dilation
• Severe MR: ERO 0.4 cm2,
• Regurgitant He (>60ml)
• Regurgitant (>55%)
• Vena contracta, color jet area.
• Assess. LV size and contractility (EF 60%) and LVESD (40mm), pulmonary hypertension, Afib

12
Valvular RegurgitationIndications for Operation
Presence of severe regurgitation
Presence of severe regurgitation
Any SymptomsAny Symptoms
Drop in EF(<60%MR, < 50%AR)
Drop in EF(<60%MR, < 50%AR)
LV Dilation. LVESD(>40mm MR, > 50 mm AR)
LV Dilation. LVESD(>40mm MR, > 50 mm AR)
OperateOperate
+

13
Mitral Stenosis
• Etiology: Rheumatic, Calcific
• Signs & Symptoms• Echocardiogram: Gold Standard to assess
severity and valve and sub valvular pathology, MR• 220/Pressure half time, (Doppler)• Severe MS: Mean gradient > 10 mmHg, MV. Area
less than 1 cm2
• Balloon Mitral Valvotomy• MVR• Atrial Fib could be very detrimental
Prosthetic Valve Complications
• Structural failure• Endocarditis• Thromboembolism• Thrombosis• Perivalvular leak• Hemolysis• Prosthesis – patient mismatch

14
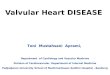
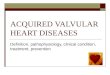
Mechanical Valve
bileaflet Tilting disk
RossHomograft
Mechanical StentlessTissue
Gold Standard Treatment for ValvularDiseases had been Prosthetic Valves
Edwards SAPIEN

15
60 Year-old Male St. Jude AVR
• No Hx thromboembolism, EF 60%• A) INR 2.5-3.5• B) INR 2.0-3.0• C) INR 2.5-3.5 + ASA 81mg• D) INR 2.0-3.0 + ASA 325mg• E) INR 2.0-3.0 + ASA 81mg
Mechanical Valves Target INR
INR 2.5 INR 3
AORTIC Other AVR ( Mechanical)
Bileaflet St jude Risk Factors
Medtronic - Hall ALL MITRAL
No risk factors
ASA is needed for all mechanical & biological valvesOn -X valve: INR 1.5-2

16
• INR 2-3 INR 2.5-3.5
• INR 2.5-3.5 INR 3.5-4.5
• No ASA Add ASA
Prosthetic ValvesEmbolic Events at Target INR
Pre/Post ProcedureMechanical Valves
Bridging Anticoagulation
• No Heparin Heparin
• Bileaflet AVR (ST JUDE) Bjork Shiley Valve
• No Risk factors Any MVR or TVR
AVR - 1 risk factor
• Previous event off Warfarin
• Recent thromboembolism (1yr)
AFHx ThromboembolismHyper coagulableLV < 30
AFHx ThromboembolismHyper coagulableLV < 30

17
Prosthetic Heart ValvesManagement of Anticoagulation
• Mechanical valves – all require warfarin• DO NOT USE DOACS (dabigatran etexilate,
apixaban, Xarelto, etc.• Bioprosthesis – warfarin for 3-6 months, then D/C
unless risk factors**
• AVR, no risk factors, first 3 months. Class iib – ASA only
AFHx ThromboembolismHyper coagulateLV < 30
AFHx ThromboembolismHyper coagulateLV < 30
Anticoagulation for Atrial Fibrillation in Patients with VHD (New Section)
Recommendations COR LOE
New: Anticoagulation with a VKA is indicated for patients with rheumatic mitral stenosis and AF I B-NR
New: Anticoagulation is indicated in patients with AF and a CHA2DS2-VASc score of 2 or greater with native aortic valve disease, tricuspid valve disease, or MR
I C-LD
New: It is reasonable to use a DOAC as an alternative to a VKA in patients with AF and native aortic valve disease, tricuspid valve disease, or MR and a CHA2DS2-VASc score of 2 or greater
IIa C-LD

18
Infective Endocarditis Prophylaxis
Recommendations COR LOE
Secondary prevention of rheumatic fever is indicated in patients with rheumatic heart disease, specifically mitral stenosis
I C
Modified: Prophylaxis against IE is reasonable before dental procedures that involve manipulation of gingival tissue, manipulation of the periapical region of teeth, or perforation of the oral mucosa in patients with the following:1. Prosthetic cardiac valves, including transcatheter-implanted prostheses and homografts. 2. Prosthetic material used for cardiac valve repair, such as annuloplasty rings and chords.(con’t)
IIa C-LD
Infective Endocarditis Prophylaxis
Recommendations COR LOE
(con’t)3. Previous IE.4. Unrepaired cyanotic congenital heart disease or
repaired congenital heart disease, with residual shunts or valvular regurgitation at the site of or adjacent to the site of a prosthetic patch or prosthetic device.
5. Cardiac transplant with valve regurgitation due to a structurally abnormal valve
IIa C-LD
Prophylaxis against IE is not recommended in patients with VHD at risk of IE for nondental procedures (e.g., TEE, esophagogastroduodenoscopy, colonoscopy, or cystoscopy) in the absence of active infection
III: No Benefit
B

19
2017 AHA/ACC Guideline for the Management of Patients With Valvular Heart
Disease(2014 guideline with 2017 focused update incorporated)
Developed in Collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, Society for Cardiovascular Angiography and Interventions,
Society of Cardiovascular Anesthesiologists, and Society of Thoracic Surgeons
© American College of Cardiology Foundation and American Heart Association
Thank You