Embed Size (px)
Citation preview

ANAEMIA FREE INIDIA

• Group photo
Our TeamPRESENTED At GYNAECON 10/10/2015
Our MISSION: SAY No TO ANAEMIA

DR. JYOTI BHASKAR
DR. SHARDA JAIN Dr.Jyoti Aggarwal
SOARING HIGH !! THROUGH
IRON LIBERATION

Embarrassing !!

Indian Scenario

MAGNITUDE
• 49.7% of Indian pregnant women suffer from anemia (WHO Global database, 2006)
20 % maternal deaths contributed by anemia
• Iron deficiency anemia (IDA) commonest cause of anemia in pregnancy
Most Common deficiency state in the worldPreventable and correctable cause of anemia.
Dr. Sharda Jain – An activist and protagonist of Anaemia Free India –
80% pregnant women are Anaemic

Every Parent Aspires That There Child will
Become anotherAPJ ABDUL KALAM

HARD FACT
HAEMOGLOBIN LEVELS AFFECTS
• INTELLIGENCE
• PERFORMACE• Diminished concentration• Disturbance in perception• Poor learning ability

Reduced Performance and Productivity
Decreased Work OutputDecreased Work Capacity

Anaemic Mother gives birth to an Anaemic Baby
• Irregular Heavy menstruation• Low pre-pregnancy iron stores• LBW babies and preterm delivery

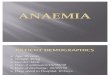
Hemorrhage30%
Anemia19%
Sepsis16%
Abortion9%
Obst. Lab10%
Toxemia8%
Others8%
CAUSES OF MATERNAL MORTALITY SRS-1998
- Direct cause of 20% of maternal deaths Indirect cause for another 20% of maternal deathsNothing is more expensive than a missed
opportunity!
UNCHANGED FOR 5 DECADES

Anaemia
Death
In India, over 300 maternal deaths EVERYDAY,
about 200 due to anemia: FOGSI Beyond numbers!
For every maternal death, there are 30 more who ‘almost died’.

Definition
WHO defines Anemia as
•Hb< 12 gm/dl in women •Hb< 13gm/dl in Men
•Anemia in pregnancy refer Hb < 11gm/dl.

MANAGEMENT

DIET --- IRON AND PROTEINS

WHO
• Anthelminthic medication in pregnant women with anaemia after 12 weeks of pregnancy
• Drug of choice is Mebendazole 100mg BD for 3 days OR Albendazole 400mg

FERROUS SULPHATE
FERROUS GLUCOMATE
FERROUS FUMARATE
Ferrous Succinate

PARENTERAL IRON THERAPY
INDICATIONS
• Non compliance with, or intolerance to, oral iron therapy
• Proven malabsorption
• No Hemoglobinopathy
• Advanced gestation/post partum with moderate to severe
anemia

FORMULATIONS
• Low molecular weight Iron Dextran
• Iron Sucrose
• Ferric Carboxymaltose

Problems With Existing Parenteral Iron Preparations
• The main disadvantage of Iron sucrose is the need for multiple infusions as the maximum weekly dose should not exceed 600 mg (200 mg IV, 1-3 times/week)
• Risk of anaphylaxis and allergic reactions
• Requirement of test dose administration
Cancado RD et al. Rev Bras Hematol Hemoter. 2011; 33(6): 461–469.

NEWER PREPARATIONS
Iron III carboxymaltose (ferric hydroxide carbohydrate complex)
• Controlled delivery of iron within cells of reticuloendothelial
system (primarily bone marrow) • Subsequent delivery to iron binding proteins ferritin and
transferrin.• Rapid incorporation into RBCS

Dosage
• Single intravenous dose of 1000 mg over 15 minutes (maximum 15 mg/kg by injection or 20 mg/kg by infusion)
• Dilution: • 500mg ferric carboxymaltose in 100mL sodium
chloride 0.9%. • 1000mg ferric carboxymaltose in 250mL sodium
chloride 0.9%

• Flush with 50mL sodium chloride 0.9% before and after iron infusion to minimise risk of extravasation.
• Maximum of 1000mg that can be given in one sitting.
• No test dose required

Indications
Were Parenteral iron is Indicated:
• Adolescents and All Women• Pregnant women in 2nd – 3rd trimester• Post-Partum Women• Before Surgeries

Take Home Message
• We Need to Build an Anaemia free India
• Be Obsessed – Detection and Treatment
• Switch Over Early – to Parenteral Iron
• FCM – is Safe, Patient Friendly and Effective

Iron strengthens!
Gold glittersSilver shines
But…

ISO 14001:2004 (EMS)
ISO 9001:2008
HELPLINE-9650588339/22414049
HELPLINE-9599044257
HELPLINE-9910081484ISO 9001:2008
HELPLINE9599044357
…..Caring hearts, healing hands