-
7/30/2019 Anaemia note
1/73
ANAEMIA
Dr R. Z. Azma
-
7/30/2019 Anaemia note
2/73
Anaemia
Defination:
Anaemia - haemoglobin (Hb)
- red blood cells (RBC)(reduction of more than 10% of the
normal
value of Hb or total number of RBC for age
and sex)
-
7/30/2019 Anaemia note
3/73
Reference ranges for Hbs at different ages
Age group Hb range (g/dl)
Newborn (< 1 week) 14 22
6 months old 11 14
Children (1 16 years) 11 15
Adults
Men
Women
13 16
12 - 14
-
7/30/2019 Anaemia note
4/73
Anaemia
Clinical grading (Adults)
Mild (Hb > 10 g/dl) Asymptomatic
Moderate (Hb 7 10
g/dl)
Pallor, lethargy
Dyspnoea, vertigo
headache
Severe (Hb < 7 g/dl) Tachycardia
hypotension
-
7/30/2019 Anaemia note
5/73
Mechanisms of anaemia
Production of RBCs depends on:
Haemopoietic stem cells (to function
satisfactorily)
Erythroid precursor cells (normal maturation and
released into circulation)
Hb synthesis (to function normally)
-
7/30/2019 Anaemia note
6/73
Mechanisms of anaemia
1. Decreased production
Ineffective erythropoiesis
Deficiency of B12/folate
Abnormal synthesis of haemoglobin (thalassaemia) Decreased
effective erythropoiesis
Aplastic anaemia/marrow failure
2. Increased blood loss
Gastrointestinal bleeding
3. Increased destruction
haemolysis
-
7/30/2019 Anaemia note
7/73
Classification of anaemia
1. Morphological
Based on red cell indices and blood film
Hypochromic microcytic anaemia (MCV , MCH)
Normochromic normocytic anaemia (MCV N, MCH N) Normochromic
macrocytic anaemia (MCV , MCH N)
2. Pathophysiological
Based on causes of anaemia
Iron deficiency anaemia Megaloblastic anaemia
Haemolytic anaemia
-
7/30/2019 Anaemia note
8/73
Classification of anaemia
MCV mean corpuscular volume (fl)
MCH mean corpuscular Hb (pg)
MCV (80 100 fl) Normocytic
MCV (< 80 fl) Microcytic
MCV (>100 fl) Macrocytic
MCH (27 - 32 pg) Normochromic
MCH (< 27 pg) Hypochromic
-
7/30/2019 Anaemia note
9/73
-
7/30/2019 Anaemia note
10/73
Physiological adaptations to anaemia
Reduced delivery of oxygen to tissues
Increased erythropoietin secretion by kidneys
More rapid delivery of blood
Heart rate and respiratory rate increased Cardiac output
increased
Increased in RBC 2,3 DPG shifts oxygendissociation curve to the
right.
-
7/30/2019 Anaemia note
11/73
Iron deficiency anaemiaA form characterized by low orabsent iron
store, low serum
iron conc, low transferrin
saturation, elevated transferrin,low Hb conc or hematocrit,
nhypochromic, microcytic rbc
-
7/30/2019 Anaemia note
12/73
Epidemiology
Iron deficiency anaemia (IDA) is the
commonest macronutrient deficiency in man
despite abundant iron content in the earth
crust.
30% of world population
50% of pregnant women 20% women
3% of men
-
7/30/2019 Anaemia note
13/73
Aetiology
IDA - reduction in iron supply to red cellprecursors.
Causes1. Dietary - defective intake of iron: poverty,
religious
tenets, vegetarian2. Increase physiological requirement infants,
children,
pregnancy
3. Blood loss - GIT (peptic ulcer,
haemorrhoids),menorrhagia.
4. Malabsorption partial gastrectomy, gluten
inducedenteropathy
-
7/30/2019 Anaemia note
14/73
Aetiology
IDA - reduction in iron supply to red cellprecursors.
Causes1. Dietary - defective intake of iron: poverty,
religious
tenets, vegetarian2. Increase physiological requirement infants,
children,
pregnancy
3. Blood loss - GIT (peptic ulcer,
haemorrhoids),menorrhagia.
4. Malabsorption partial gastrectomy, gluten
inducedenteropathy
-
7/30/2019 Anaemia note
15/73
Clinical features
Symptoms Signs
Anaemia
Lethargy
Dyspnoea
Headache
Poor concentration
Palpitation
IDA deficiency
Dysphagia
Anaemia
Pallor
Tachycardia
IDA deficiency
Painless glossitis
Angular stomatitis
Koilonychia
Skin atrophy
-
7/30/2019 Anaemia note
16/73
Clinical features
Koilonychia in severe iron
deficiency aneamia
Hiatus hernia can cause IDA
-
7/30/2019 Anaemia note
17/73
Laboratory investigations
Full blood count FBC
Hb
MCV
MCH.
Peripheral blood film
Serum iron and TIBC Serum ferritin
Bone marrow iron (rarely)
-
7/30/2019 Anaemia note
18/73
Laboratory investigations
Typical results seen in iron def. anaemia
Reduced Haemoglobin
Reduced MCV, MCH, MCHC
Peripheral blood film: hypochromic microcytic
anaemia
Reduced serum iron with raised TIBC
Reduced serum ferritin
Absent iron stores in bone marrow
-
7/30/2019 Anaemia note
19/73
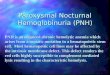
Full blood picture of iron deficiency anaemia
-
7/30/2019 Anaemia note
20/73
Treatments
To correct anaemia and replenish iron
stores:
Oral iron
Parenteral iron
Treat the underlying causes.
-
7/30/2019 Anaemia note
21/73
Megaloblastic Anaemia
Characterized by megaloblast
in bm, such s PA
-
7/30/2019 Anaemia note
22/73
Megaloblastic anaemia
Causes
Vitamin B12 deficiency
Folate deficiency
-
7/30/2019 Anaemia note
23/73
Megaloblastic anaemia
Impaired synthesis of DNA due to reducedsupply of the immediate
precursors of DNA
dA(adenine)TP and dG(guanine)TP (purines)
dT(thymine)TP and dC(cytosine)TP (pyrimidines)
Folate def: impairs in synthesis of dTTP folate is coenzyme for
thymidylate synthesis.
Vit B12 - cofactor to convert methyl THF
which enters the cell fr plasma to THF.
-
7/30/2019 Anaemia note
24/73
-
7/30/2019 Anaemia note
25/73
Megaloblastic anaemia
slow demethylation
of methyl THF
THF
purine
synthesisLack of B12
supply of precursors
needed for DNAsynthesis
incomplete
replication of
chromosomal DNA
Ineffective
haemopoiesis
In severe def
affect all
3 cell lines
(pancytopenia)
apoptosis ofNRBC in BM
-
7/30/2019 Anaemia note
26/73
Vit B12 def
CAUSES
Malabsorption Gastric causes
Pernicious anaemia
Congenital IF absence/abn fx
Total/partial gastrectomy
Intestinal causes Fish tapeworm
Intestinal stagnant loop syndrome
Ileal resection
Crohns ds
Inadequate dietary intake Vegetarian poverty
-
7/30/2019 Anaemia note
27/73
Pernicious anaemia
MA,affect older adults due 2 failure of gastric
mucosa 2 secrete adequate n potent IF
Severe lack of IF gastric atrophy.
Autoimmune in origin
May a/w myxoedeme, Hashimotos ds, Addisonsds, vitiligo,
hypoparathyroidism &hypogammaglobulinaemia.
Occur in families, F > M, 60 yr, blood gp A
incidence of Ca stomach. Thin stomach wall, plasma cell &
lymphoid infiltrate
of the lamina propria
-
7/30/2019 Anaemia note
28/73
-
7/30/2019 Anaemia note
29/73
Pernicious anaemia : (L) normal, (R) atrophy of all coats, loss
of gastric
glands & parietal cells & infiltration of the lamina
propria by lymphocytes &
plasma cells achlorhydria & sec. of IF is absent.
-
7/30/2019 Anaemia note
30/73
Pernicious anaemia :
showing premature
greying, blue eyes &
vitiligo
-
7/30/2019 Anaemia note
31/73
Marked vitiligo
P i i i
-
7/30/2019 Anaemia note
32/73
Pernicious anaemia
Antibodies :
- 90% ; parietal cell Ab in serum
- 50% ; type I or blocking Ab to IF ( inhibit IF bind to
B12 )
- 35% ; type II or precipitating Ab to IF, inhibits itsileal
binding site.
- 50% ; IF Ab, inhibit IF fx in gastric juice.
Congenital PA : presentation develop after age of 2
( Cong. Lack of IF )
F l t d f
-
7/30/2019 Anaemia note
33/73
Folate def
CAUSES
Nutritionalvegetarian, poverty, goats milkanaemia
Malabsorption tropical sprue, Coeliac ds, partial
gastrectomy, Crohns ds Excess utilization pregnancy,
haematological ds,inflammatory ds.
Excess urinary loss active liver ds, CHF
Drugs anticonvulsants, hyroxyurea Others alcoholism, intensive
care.
C li di
-
7/30/2019 Anaemia note
34/73
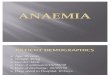
Coeliac disease
Coeliac disease (gluten-sensitive enteropathy orcoeliac sprue)
is disease of small intestine.
Gluten (substance found in wheat, barley and rye)
activates the immune system and causing damageto the delicate
lining of the small bowel -responsible for absorbing nutrients and
vitamins.
Histological section of jejunal bx villous atrophywith absence
of vili and hypertrophy of the mucosalcrypts
-
7/30/2019 Anaemia note
35/73
Figure 1: Healthy villi of
the small intestine (as
seen under the
microscope).
Figure 2: Damaged villi
of the small intestine.Figure 3: Villi
completely destroyedby the immune system.
Absence of vili and
hypertrophy of the
mucosal crypts
Cli i l f t
-
7/30/2019 Anaemia note
36/73
Clinical features
Symptoms and signs of
anaemia
Weakness
Tiredness
Shortness of breath
Pale
Angina
Heart failure
Symptoms and signs of
b12/folate deficiency
Glossitis
Angular cheilosis
Neurological symptoms
Cli i l f t
-
7/30/2019 Anaemia note
37/73
Clinical features
Lemon-yellow
appearance
combination anaemia& jaundice ( excessive
Hb breakdown in BM
due to ineffective
erythropoiesis )
-
7/30/2019 Anaemia note
38/73
Glossitis - the tongue is
beefy-red & painful
due to impaired DNA
synthesis in the mucosal
epithelium.
Angular cheilosis -
due to impaired
proliferation of
epithelial cells
Cli i l f t
-
7/30/2019 Anaemia note
39/73
Clinical features
Neurological symptoms :- numbness
- spastic ataxia : demyelination of the lateral &
posterior columns
- Brain involvement : optic atrophy
somnolence
dementia
frank psychosis
-
7/30/2019 Anaemia note
40/73
General tissue effects of cobalamin &
folate deficiency
Severe def. will affect rapidly growing ( DNA-synthesizing )
tissues :
Marrow : megaloblastic anaemia
Macrocytosis of epithelial cell surfaces ; mouth,stomach, small
intestine,respiratory, urinary &
female genital tracts.
Prematurity maternal c folate def.
Neural tube defects folate def in early
pregnancy
-
7/30/2019 Anaemia note
41/73
Cobalamine def may cause:
bilateral peripheral neuropathy / degeneration of the post.
& pyramidal tracts of the spinal cord
Rarely: optic atrophy and mental abnormalities Long term def in
infancy leads to poor brain
development & impaired intellectual development.
Cause : accumulation of S adenosyl
homocysteine ( excessive homocysteine entry, no
B12 to convert to methionine )
VITAMIN B12 NEUROPATHY( Subacute combined degeneration of the
cord )
-
7/30/2019 Anaemia note
42/73
Pernicious anaemia : cross section of spinal cord of a pt who
died c severe vit
B12 neuropathy ( subacute combined degeneration of the spinal
cord ). There
is demyelination of the lateral & posterior columns
Laboratory findings
-
7/30/2019 Anaemia note
43/73
Laboratory findings
FBC: Anaemia, in
severe def
pancytopenia, high
MCV, normal MCH.
PBF: Macrocytosis
with
anisopoikilocytosis
-
7/30/2019 Anaemia note
44/73
PBF: Hypersegmented neutrophils
-
7/30/2019 Anaemia note
45/73
BMA: Hypercellular - megaloblasts with dyserythropoiesis..
-
7/30/2019 Anaemia note
46/73
giant metamyelocytes
-
7/30/2019 Anaemia note
47/73
..hyperpolypoid megakaryocytes.
Other blood investigations
-
7/30/2019 Anaemia note
48/73
Other blood investigations
Serum folate low in folate deficiency
Serum B12 low in B12 deficiency
Management
Folate deficiency Tablet folic acid daily
B12 deficiency Intramuscular hydroxocobalamin,
every 3 months.
Those with Subacute combined degeneration of thecord if treat
with folate without B12, worsen the
condition.
-
7/30/2019 Anaemia note
49/73
HAEMOLYTIC ANAEMIA
Any of heterogenous grp of inherited anemias characterized
byshortened rbc survival, lack of spherocytosis, n normal
osmotic
fragility with erythrocyte membrane defects,
multipleintracellular enz def or other defect or unstable Hb
Haemolytic anaemia
-
7/30/2019 Anaemia note
50/73
Haemolytic anaemia
Normal RBC lifespan is 120 days after whichthey are removed by
RES (marrow, liver,
spleen).
Haemolytic anaemia anaemia due to
increased rate of red cell destruction.
Erythroid hyperplasia and anatomical
expansion of the marrow.
Haemolytic anaemia
-
7/30/2019 Anaemia note
51/73
Haemolytic anaemia
The normal adult marrow is capable ofproducing red cells 6 - 8x
more than normalrate, provided that there is adequate supplyof
iron, folate and B12.
HA is seen when the red cell survival is lessthan 30 days.
Mechanism:
Intravascular: haemolysis occur in circulation Extravascular:
removal of RBC in the RES
-
7/30/2019 Anaemia note
52/73
Clinical features
-
7/30/2019 Anaemia note
53/73
Pallor
Mild Jaundice
Splenomegaly
Some may have painful right abdomen
(chronic haemolysis pigment gallstone) Haematuria (intravascular
haemolysis)
Bossing of frontal and parietal bones
mongoloid appearance (marrow expansion inchronic haemolysis)
Clinical features
Laboratory findings
-
7/30/2019 Anaemia note
54/73
Anaemia with reticulocytosis.
PBF showed: spherocytes with
polychromatic cells (reticulocytes).
Laboratory findings
Spherocytes
Laboratory findings
-
7/30/2019 Anaemia note
55/73
serum bilirubin
urine and faecal urobilinogen serum haptoglobin Bone marrow:
erythroid hyperplasia
compensation mechanism
Ultrasound of abdomen gallstone
Laboratory findings
Laboratory findings
-
7/30/2019 Anaemia note
56/73
Features of intravascular haemolysis
(others similar with extravascular haemolysis) Fragmented red
cells (schizocytes) seen in
PBF.
Haemosiderinuria (iron storage protein,derived from the
breakdown of Hb in therenal tubular cells)
Haemoglobinaemia
Haemoglobinuria
Laboratory findings
S
-
7/30/2019 Anaemia note
57/73
Classification of HA
-
7/30/2019 Anaemia note
58/73
Classification of HA
Hereditary haemolytic anaemia
Acquired haemolytic anaemia
Classification of HA
-
7/30/2019 Anaemia note
59/73
Classification of HA
HEREDITARY HAEMOLYTIC ANAEMIA
Membrane
defects
Metabolic
defects
Haemoglobin
defectsHereditary
Spherocytosis
G6PD def Defective synthesis
(thalassaemia /)H. Elliptocytosis / H.
Pyropoikilocytosis
Pyruvate kinase def Abnormal variants
(eg. Hb S, Hb C,
unstable)
H. Stomatocytosis Pyrimidine 5-
nucleotidase def
South-east Asian
ovalocytosis
Glutathione
synthase def
-
7/30/2019 Anaemia note
60/73
ACQUIRED HAEMOLYTIC ANAEMIA
IMMUNE NON-IMMUNE
AUTOIMMUNE
Warm
autoimmune
HA
Cold
autoimmuneHA
Haemolytic
Transfusion
Reaction
INFECTIONS
FRAGMENTATION
SYND
CHEMICAL AND
PHYSICAL
AGENTS
DRUGS
ALLOIMMUNE
Haemolytic
Disease ofNewborn
G6PD deficiency
-
7/30/2019 Anaemia note
61/73
G6PD deficiency
G6PD catalyses the first step of pentose
phosphate pathway to produce NADPH.
Def of G6PD NADPH production lack ofreduced glutathione (GSH)
which protect themembrane Hb & other cell structure fr
oxidant
damage.
-
7/30/2019 Anaemia note
62/73
G6PD deficiency
-
7/30/2019 Anaemia note
63/73
G6PD deficiency
Mild G6PD deficiency is usually asymptomatic.
It is present in all cells but patient become
symptomatic in response to oxidant stress
(drugs, fava beans) or infections. In severe G6PD patient may
have chronic
haemolytic anaemia.
Clinical findings: anaemia, mild jaundice,haematuria
G6PD deficiency
-
7/30/2019 Anaemia note
64/73
G6PD deficiency
Lab findings;
FBP: red cells with
contracted Hb in ghostmembrane blister cells,bite cells,
NRBC
Haemoglobinuria
Haemosiderinuria Screening test:
Ultraviolet spot testnegative
G6PD assay(quantitative): low(The screening andquantitative
tests should notbe done during acute event)
Thalassaemia
-
7/30/2019 Anaemia note
65/73
Thalassaemia
Results from a reduced synthesis of or
chains. Autosomal recessive inheritance
Classifications:
Genetic If no globin chain is synthesized at all0 / 0-
thalassaemia
If some is still produced+ / +-thalassaemi
Clinical
Thalassaemia
-
7/30/2019 Anaemia note
66/73
Thalassaemia
Clinical classifications classified according to
degree of severity of symptoms:1.Major = severe anaemia and
transfusion dependent.
2. Intermedia = anaemia and splenomegaly
3.Minor = symptomless carrier only show changes in red
cell indices (hypochromic microcytic red cells).
Symptomatic for HA:
thal major,Hb Barts and HbH ds
Thalassaemia
-
7/30/2019 Anaemia note
67/73
Thalassaemia
thalassaemia syndromes majority of geneticlesions are point
mutations.
thalassaemia trait (o or+) - asymptomatic(clinically minor)
thalassaemia major (oo oro+)
symptomatic: Either no chain (o) or small amounts (+) are
synthesized.
Excess chains precipitate in erythroblasts and inmature red
cells causing ineffective erythropoiesis andhaemolysis.
Thalassaemia
-
7/30/2019 Anaemia note
68/73
Thalassaemia
Beta thal major inheritance
Thalassaemia
-
7/30/2019 Anaemia note
69/73
Thalassaemia
Clinical features
(major):
Severe anaemia
Hepatosplenomegaly
excessive red cell
destruction and
extramedullary
haemopoiesis.
Expansion of bones
marrow
hyperplasia
thalassaemic facies.
Thalassaemia
-
7/30/2019 Anaemia note
70/73
These are usually due to gene deletions
Asymptomatic in 1 or 2 gene deletions (/- ,
- /- or/--)
Symptomatic when 3 or 4 gene deletions (-/-- or --/--).
Hb H 3 gene deletions, small amount chain
available excess beta chain forming tetramers(4)and precipitate
in red cells (known as Hinclusions).
Thalassaemia
-
7/30/2019 Anaemia note
71/73
Patient survived till old age and some times require blood
transfusion (thalassaemia intermedia).
Hb H inher i tance
Thalassaemia
-
7/30/2019 Anaemia note
72/73
Hb Barts, no available
globin chain: failure foetal Hb
synthesis (eg. Hb F). Excess chain forming
tetramers (4 known asHb Barts).
death in utero or at birth
Hydrop fetal is inher i tance
-
7/30/2019 Anaemia note
73/73