Embed Size (px)
DESCRIPTION
ophthalology
Citation preview

ACUTE INTRA OCULAR PRESSURE RISE
BYDR/MOHAMED ABDEL-AZIZD
SUPERVISOR
PROF.DR/KHALED HANAFY

Increased eye pressure can lead to optic nerve damage and vision loss.
this can happen immediately or gradually depending on the level of eye pressure.

Causes of acute IOP rise
_Causes of acute IOP increase, but with an open angle:
•Glaucomat-ocyclitic crisis (Posner Schlossman syndrome)
•Inflammatory open-angle glaucoma (Moderate to severe anterior chamber reaction)
•Retrobulbar hemorrhage or inflammation (Proptosis and restriction of ocular motility).
•Traumatic (hemolytic) glaucoma
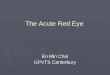
•Pigmentary glaucoma

pigmentary glaucoma. A – gonioscopy revealing pigment accumulation in the trabecular meshwork B – UBM showing iris concavity; C – Iris transillumination defects; D – Krukenberg's spindle

Retrobulbar hemorrhage due to trauma

_causes of acute IOP rise, with closed angle:
.Primary angle-closure glaucoma.
_causes of acute IOP rise, with closed angle: Secondary angle-closure glaucomas.
•Neovascular or inflammatory membrane pulling the angle closed (Neovascular Glaucoma)
•Mechanical closure of the angle secondary to anterior displacement of the lens iris diaphragm:
.Lens-induced [Pupillary block as a result of a large lens (phacomorphic) or small lens (nanophthalmos), or zonular loss/weakness (e.g., traumatic)

.Choroidal detachment (serous or hemorrhagic)
.Medication-induced [Usually bilateral with possible serous choroidal detachment (e.g: A history of topical carbonic anhydrase inhibitors).
.Choroidal swelling after extensive retinal laser surgery or after placement of a tight encircling band in retinal detachment surgery.
.Posterior segment tumor (e.g., choroidal or ciliary body melanoma, Malignant Melanoma of the Choroid)
.Aqueous misdirection syndrome (e.g., Malignant Glaucoma).

Advanced anterior segment neovascularization with ectropion uveae
Neovascular Glaucoma choroidal detachment
B-scan

ciliary body melanoma : (A) EOE is noted superonasally, with an associated sentinel vessel. (B)coloured photograph shows the ciliary body melanoma superonasally. (C) UBM demonstrating the ciliary body mass with a small area of scleral thickening corresponding to the EOE. (D) B-scan ultrasound with a dome-shaped mass corresponding to the melanoma.

Features of this syndrome:
_Recurrent episodes of mild cyclitis
_Uniocular involvement
_ Duration of attack varying from a few hours to several weeks
_Corneal edema with a few keratic precipitates .
_Normal IOP between episodes
_ IOP usually is elevated (40-60 mm Hg)
_IOP is related to the duration of uveitis but NOT to the degree of uveitis
Glaucomato cyclitic crisis

PSS:Fine kps,white eye and increase IOP

Treatment recommendations include the following:
_Topical steroids
_Topical anti-glaucoma drops
_Systemic carbonic anhydrase inhibitors
_Topical NSAIDs
_Carefully observe patients periodically for recurrences and for development of POAG
N:B.,antiglaucoma agents do not prevent recurrences of glaucomato cyclitic crisis.

_The acute rise in intraocular pressure (IOP) is related to red blood cells and their byproducts clogging the trabecular meshwork.
_Glaucoma is more likely to develop
with total hyphema or after rebleeding
Red cell glaucoma
hyphema from blunt trauma

Medical Care
IOP reduction if it is > 24 mm Hg in patients with sickle cell or > 30 mm Hg in other patients.
Avoid oral carbonic anhydrase inhibitors, especially acetazolamide in patients with sickle cell trait or disease. These drugs tend to increase sickling of erythrocytes
Surgical Care
Indications for anterior chamber wash-out are as follows:
_IOP >50 mmhg for 2 days or >35mmhg for 7 days

-Secondary angle-closure glaucoma due to lens intumescence.
•-Patients generally have decreased vision before the acute episode
Phacomorphic glaucoma
Phacomorphic glaucoma
-Phacomorphic glaucoma is more common in smaller hyperopic eyes
with a larger lens and a shallower AC
-Zonular weakness secondary to exfoliation, trauma, or age can play a part in causing phacomorphic glaucoma

Signs of phacomorphic glaucoma include the following:
_ High intraocular pressure (IOP) - Greater than 35 mm Hg
_Mid-dilated, sluggish, irregular pupil
_Corneal edema
_Injection of conjunctival and episcleral vessels
_Shallow central anterior chamber (AC)
_Lens enlargement and forward displacement
_Unequal cataract formation between the 2 eyes

Medical Care
_Medical treatment of phacomorphic glaucoma is aimed at rapidly reducing the IOP to prevent further damage to the optic nerve, to clear the cornea, and to prevent synechiae formation.
_Initial management should address the acute nature of the angle closure and include beta-blockers, alpha 2-adrenergic agonists, and carbonic anhydrase inhibitors.
_Miotics can worsen the secondary angle closure attack by increasing irido-lenticular contact.

_Laser iridectomy sometimes relieves the acute angle-closure attack, but the AC remains shallow.
_ These eyes are susceptible to repeated attacks of angle closure; therefore, cataract extraction should be performed if the AC does not deepen after laser iridectomy.
Secondary management
_begins with laser iridotomy to relieve the pupillary block.

N:B. On initial puncture of the capsule on an intumescent lens, an increased risk of a tear extending to the equator exists.
One method for dealing with this possibility is using a needle on a syringe to aspirate the liquefied cortex as the capsule is punctured.
N:B. Because of the increased risk of complications during cataract extraction, deepening of the AC with pars plana vitreous tap has been suggested (Dada et al.,2007).

Acute angle closure
is defined as at least 2 of the following symptoms: ocular pain, nausea/vomiting, and a history of intermittent blurring of vision with halos; and at least 3 of the following signs: IOP greater than 21 mm Hg, conjunctival injection, corneal epithelial edema, mid-dilated non reactive pupil, and shallower chamber in the presence of occlusion.
predispose individuals to AACG. These include shallower anterior chambers, thinner ciliary bodies, a thinner iris, anteriorly situated thicker lens and a shorter axial eye length.
A narrow angle has the most devastating consequences.

Abnormal forward bowing Iris characteristic of acute angle closure glaucoma
Acute Angle Closure Glaucoma: External Appearance

Emergency Care
_The treatment of acute angle-closure glaucoma (AACG) consists of IOP reduction, suppression of inflammation, and the reversal of angle closure.
_ Once diagnosed, the initial intervention includes acetazolamide, a topical beta-blocker, and a topical steroid.

_Topical steroids decrease the inflammatory reaction and reduce optic nerve damage.
_Addressing the extraocular manifestations of the disease is critical. This includes analgesics for pain and anti-emetics for nausea and vomiting.
_ Placing the patient in the supine position may aid in comfort and reduce IOP. It is also believed that, while supine, the lens falls away from the iris decreasing pupillary block.

After the initial intervention, the patient should be reassessed.
Reassessment includes evaluating IOP, evaluating adjunct drops, and considering the need for further intervention, such as osmotic agents and immediate iridotomy.
Approximately 1 hour after beginning treatment, pilocarpine, a miotic that leads to opening of the angle, should be administered every 15 minutes for 2 doses.

No standard rate of reduction for IOP exists; however, Choong et el identified a satisfactory reduction as IOP less than 35 mm Hg or a reduction greater than 25% of presenting IOP.
If the IOP is not reduced 30 minutes after the second dose of pilocarpine, an osmotic agent must be considered.
An oral agent like glycerol can be administered in non diabetics. In diabetics, oral isosorbide is used to avoid the risk of hyperglycemia associated with glycerol.

Patients who are unable to tolerate oral intake or do not experience a decrease in IOP despite oral therapy are candidates for IV mannitol.
_When medical therapy proves to be ineffective, corneal indentation (CI) can be used. any smooth instrument can be used to perform this procedure.
_Laser peripheral iridotomy (LPI), performed 24-48 hours after IOP is controlled, is considered the definitive treatment for AACG.

Thank you!