Embed Size (px)
Citation preview
Electronic Health Record and Quality:
The Current Evidence
Abha Agrawal, MD, FACP
COO / CMONorwegian American Hospital
Chicago, IL
IHT2 | Nov 7 2013

Agenda
• Current state of EHR adoption• EHR and quality benefits• EHR and quality risks• Socio-technical model for EHRs
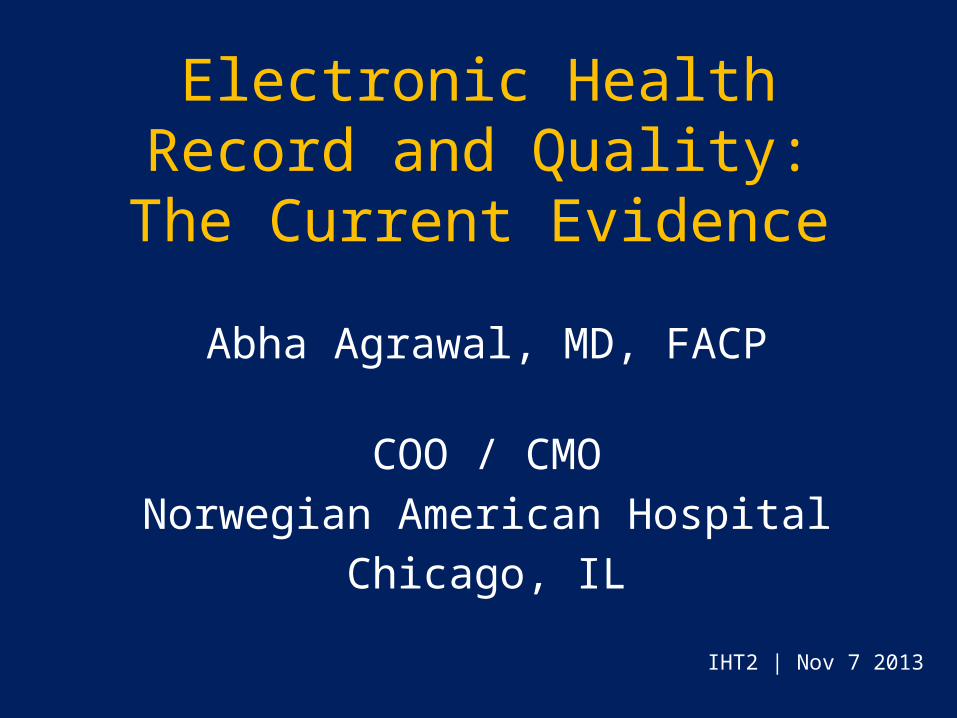
High global EHR adoption

US hospitals EHR Adoption has more than tripled since 2009
http://www.healthit.gov/sites/default/files/oncdatabrief9final.pdf

EHR adoption to date - ONC
• Registered Users– Ambulatory - 419,542– Hospitals – 4,569
• Payments – $6 billion to ambulatory– $ 10 billion to hospitals
http://www.healthit.gov/sites/default/files/oncdatabrief9final.pdf

Irrefutable Benefits of EHR versus Paper
• Access to information – any place, any time, multiple people
• Legibility / availability of information• Security / privacy• Communication / coordination• Decision-support at the point-of-care

Evidence: EHR and Quality

Computerized Physician Order Entry (CPOE): Medication Safety
Serious medication errors Preventable ADEs
10.7
4.694.86
3.99
55% decrease
5% decrease
Bates et al. JAMA. 1998; 280; 1311-16
Eve
nts
/ 10
0 pa
tient
day
s, m
ean
Paper Stand-alone E-Rx0
5
10
15
20
25
30
35
40
45
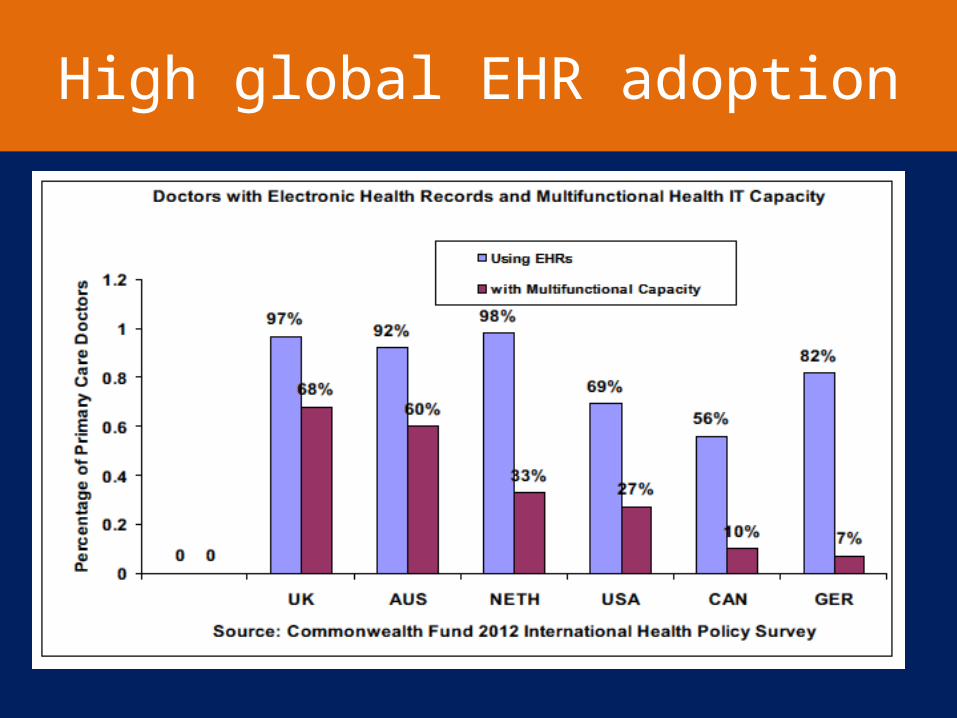
42.5
6.6
E-prescribing Reduces Medical Errors
85% decrease
Kaushal et al. JGIM. 2010
% o
f P
resc
riptio
n w
ith E
rror
(s)

Non-timing errors Potential ADEs0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
11.50%
3.10%
6.80%
1.60%
Bar-coding reduces potential ADEs
41% decrease
Poon et al. NEJM. 2010
51% decrease

EHR and Quality Benefits (Contd.)
• Laboratory safety1
– Critical results notification: time to resolution 29% shorter
• Smart monitoring2
– Remote monitoring in a 10-bed ICU decreased mortality by 46-68%
• Hand-offs3
– Computerized sign-outs reduced adverse events risk 5-fold
1. Kuperman et al. JAMIA 2010 | 2. Rosenfeld et al. Crit Care Med 2000 | 3. Petersen et al Jt Comm Journal 1998

Pre-EMR Post-EMR0
0.2
0.4
0.6
0.8
1
1.2
1
0.7
Computerized Physician Order Entry (CPOE): Inpatient Pediatric Mortality
20 % decrease
Longhurst et al. Pediatrics. 2010; 126; 14-21
Mea
n M
orta
lity
Rat
e
EHR’s Impact on Inpatient Outcomes
• Cross-sectional study of urban hospitals in Texas• 41 / 72 hospitals • Level of automation measured using a
questionnaire-based tool• Higher automation scores associated with fewer
complications, lower mortality rates, lower costs• 10% increase in automation score = 15% decrease
in adjusted odds of hospital deaths
Amarasingham et al. Arch Int Med. 2009:169:108-114

DM—eye visit
DM—HgbA1c t
esting*
DM—LD
L testi
ng
DM—nephro
pathy screening
Breast CA*
Chlamydia
Colorectal C
A
Peds pharyngitis
Peds URI
30
40
50
60
70
80
90
100
35.1
84.2 85.1
64.8
74.2
5348
74.2
93
32.7
90.187.6
78.6
65.8
51.3 52.9
90
PaperEHR
3-13% increase
EHR and Ambulatory Care Quality
* p <0.001 Kern et al. JGIM. 2013
2006 Systematic Review: Impact of HIT
• Impact on Quality– Increased adherence to guideline-based care– Enhanced disease surveillance– Decreased medication errors
• Impact on Efficiency– Decreased utilization e.g. redundant tests ordering– Mixed results on physician time
• Cost– Inconclusive data
Chaudhry et al. Ann Int Med. 2006: 144;742-752

2006 Systematic Review (Contd.)
• Most data from 4 benchmark institutions– Home-grown systems; highly customized– Decades of iterating, improving EHR systems– Local control, rapid improvement cycles– Strong informatics departments– Strong culture / expectation of EHR quality
improvement• Raises concerns about generalizability of results• Possibly, EHR impact is institution-dependent
Chaudhry et al. Ann Int Med. 2006: 144;742-752

Commercial / Vendor Systems
• Length of improvement cycles• Little or no local control• Relative immunity from consequences / “hold
harmless” clause• No reliable / centralized way of reporting
users’ concerns / safety events.

Impact of EHR on Quality: Academic vs. Non-academic hospitals
• Impact of EHR on six process measures• Two had statistically significant improvements. • Improvements were substantially greater in
academic hospitals vs. non-academic– More sophisticated IT– Different culture / leadership / priorities– Different physician hospital relationship– Different training model
• Possibly, EHR impact is context-dependentMcCullough et al. Health Affairs. 2010:29;647-654

2012 Systematic Review
• Clinical decision support systems improved process measures.
• Evidence for outcomes (clinical, economic, workload) sparse.
• Positive results across diverse settings and diverse systems!
Bright et al. Ann Int Med 2012:157;29-43
Value of IT investments: The VA Experience
• Cumulative cost: $4 billion• Benefits: $7.16 billion
– 65% or $4.6 billion – reducing unnecessary care– 27% or $1.9 billion – eliminating redundancies– Rest
• Reduced work• Reduced operating expenses
• Estimated net benefit >3 billion
Byrne et al. Health Affairs 2010:29;629-638

EHR and Quality: The VA Experience
Byrne et al. Health Affairs 2010:29;629-638

Buntin et al. Health Affairs. 2011:30;464-471
92% of the Articles on HIT Show Positive Results


EHR: Emerging Safety Concerns

Unintended Consequences of HIT
“No innovation comes without strings attached. The more technologically advanced an innovation,
the more likely its introduction will produce many consequences, both
anticipated and latent.”
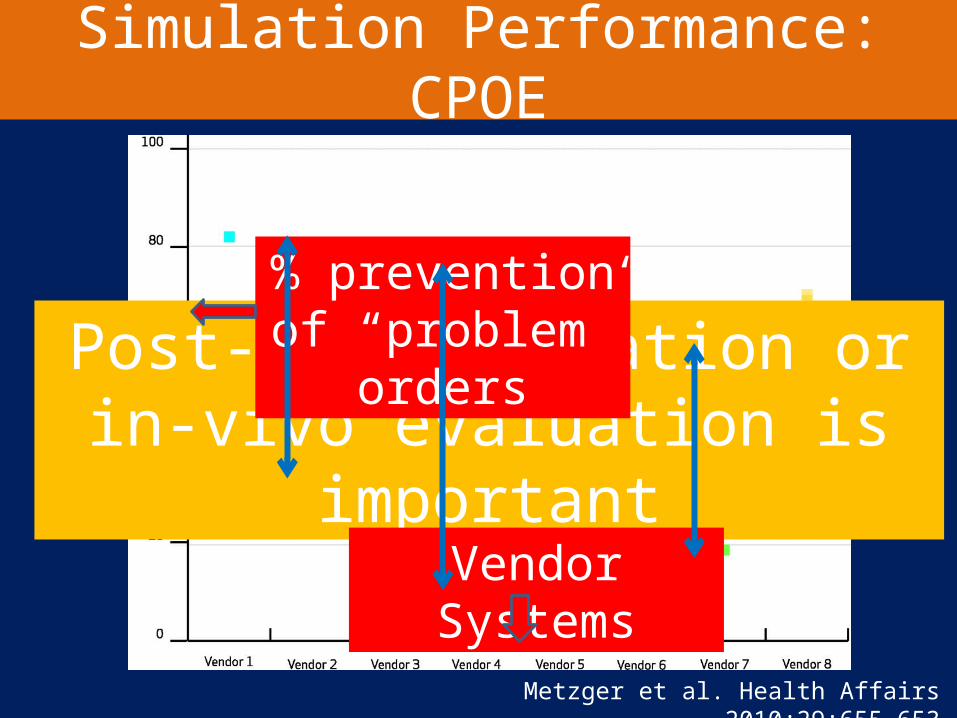
Simulation Performance: CPOE
Metzger et al. Health Affairs 2010;29:655-653
Post-implementation or in-vivo evaluation is important
Vendor Systems
% prevention of “problem” orders
CPOE Facilitating Medication Errors
• Tertiary care teaching hospital in Pennsylvania• Qualitative research: focus groups / interviews
of house officers• 22 types of NEW errors
A. Information errors due to fragmentation of dataB. Human-machine interface flaws
Koppel et al. JAMA. 2005;293:1197-1203

Pre-CPOE (13 months) Post-CPOE (5 months)0
1
2
3
4
5
6
7
2.8
6.57
Increased Neonatal Mortality After CPOE Implementation
Han et al. Pediatrics. 2005;116:1506-1512
Mea
n M
orta
lity
Rat
e
Increased Neonatal Mortality….(Contd.)
• “Lost time” in care of critically ill children and delays in time-sensitive therapies– Order entry not allowed before patient physically arrived
and fully registered• Reduced physician-nurse communication• No visible order flagging• Delays in medication dispensing and administration
– everything is computer-dependent• Too long to place orders
Han et al. Pediatrics. 2005;116:1506-1512

Alert Override / Fatigue
• Ambulatory care, 3000 prescribers1 – 90% of DDI alerts, 77 % of drug-allergy alerts
• 5 Ambulatory care practices2
– 90% of DDI and drug-allergy alerts• Review article3
– 49% to 96% - override of drug alerts
1. Isac et al . Arch Int Med. 2009 | 2.Weingart et al. Arch Int Med. 2003 | 3. van der sijs et al. JAMIA. 2006

EHR: Safety ConcernACP Ethics Case Studies

Physician Satisfaction with EHRs
• Physician dissatisfaction with current EHRs– Poor usability – Time-consuming data
entry– Less fulfilling work content– Interference with face-
face care

People
Technology (Hardware /
Software)
ProcessesOrganization
External Environment
Socio-technical Model of HIT
Health IT and Patient Safety. Institute of Medicine. 2010

Technology meets humanity: “Bloody Crossroads”

EHR User Experience

EHR’s Impact on Thinking
“Our writing equipment takes part in the forming of our thoughts.”- Frederick Nietzsche

EHR’s Impact on Thinking
• EHR as “cognitive partner”–Impacts our thinking patterns. –Influences our decision making–“Effects of” and “effects with”
technology
Horsky and Patel. J of Biomed Inf. 2005:38;264-266
EHR: Moving forward
• EHR user experience / usability must be evaluated / addressed.
• Technology alone is not sufficient: workflow / culture /environment are critical.
• Good implementation after thorough analysis• User engagement• Training• Constant evaluation• Understand and mitigate HIT-induced safety risks.
Mandl et al. NEJM. 2012:366;2240-2242

EHRs are essential for modern medicine.