Embed Size (px)
Citation preview

RCMCH
DR,MEDHAT EL-SAYEDCONSULTANT OF PEDIA-SURGERY
Chyptorchidism

Chyptorchidism Empty Scrotum.
One of the most commonpediatric surgical disorders.
Chyptorchidism occurs in approximately 10%mature newborns.
premature infants 20%.
There is little to be known aboutthe etiology.
Surgery is the corner stone of therapy

The testes originate in the mesonephric ridge on each sideof the fetal spine.
it is descend Drown downward Through the retroperitoneal Space. it is get Out through the abdominal
wall at (7th – 8th months) of gestation.
.
Testicular Embryology

Genes - Ovary/Testis Development

T. Klonisch et al. Developmental Biology 270 (2004) 1–18
(insulin-like peptide hormone 3)


Model for testicular migration• 1) migration of testis apparently involves twophases– Initial stage is transabdominal migration– Second stage is passage through the inguinal canal• 2) A number of hormones are involved in thisprocess– INSL3 (insulin-like peptide hormone 3)– Testosterone

5
Dartos musdein fascia of
theScrotum
Fascia of the triangleFemoral
ligcimentInguinalColl’s fascia in the Perineum
TuberclePubic
= 5 entopic site of the male descended testes + Transverse octopi (to the other scrotal site)
Ectopic testes :

Testosterone: masculinizing effects on the sensory
genito femoral nerve (GFN) nucleus
In males,
–L1 to L2 of the dorsal root ganglia
–Unilateral trans section of the GFN causes ipsilateral
cryptorchidism
•Sensory branch of the GFN acts via the neurotransmitter
–calcitonin gene-related peptide (CGRP)
–affects gubernacular migration during the inguinoscrotal
phase.
CGRP elicits rhythmic contractions of gubernacula
–stimulates growth and differentiation of neonatal
myogenic cells

Hormonal influences
maternal genadotropic hormone
+1st
+2nd
+3rd
Maternal Genadotropic hormone-
+
Stimulate the production of Androgenic hormones from the fetal testis.

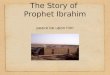
Figure 2. Spectrum of GnRH-induced LH secretion in men with GnRH deficiency. LH pulsations are indicated by asterisks. A, Normal adult male pattern of GnRH secretion with high amplitude regular LH pulsations and normal serum testosterone (T), testicular volume (TV) and sperm count; B, Disordered amplitude pattern of GnRH secretion in an IHH male, characterized by low amplitude LH pulsations, low serum T, and azoospermia; C, Sleep-entrained or developmental arrest pattern of LH secretion in an IHH male characterized by relatively low amplitude LH pulsations clustered during the night-time hours analogous to the pattern which normally occurs at puberty. Note that the TV is higher than in the subject with the apulsatile pattern; D, Apulsatile pattern of GnRH secretion in an IHH male with complete absence of endogenous LH pulsations, low serum T, prepubertal TV and azoospermia.


Hormone :
-Failure
Stimulate fetal testes to produce Hormone
Testicular receptor defect
Hormonal structure
defect
Male descended test
Insufficient Tesicular response to hCG in
36.5%

??? Why unilateral (75%)
Undescended is common
There is several other factors rather than hormonal or gubernaculums Cause.

Undescended testes
Empty scrotum
Retractile testes
is the testes which does not descend into the scrotum spontaneously, (with out cord traction or pain)
True surgical pathology
False surgical
pathology
Ectopic testes 3%-5%
Dysgenetic or atrophic testes
5%
Absent testes =intra
abdominal
True and undecided testes =palpable 89%

Retractile testes:
Empty stratum due to
Drop to Scrotumwhen children sleep or relaxed
Over action of cremasteric muscle
In adequate gubernaculums attachment of the testicle to the scrotum.
It is bilateral usually
It will be normal with adolescent

impalpable
•Hypo plastic or Absent test 8% empty Scrotum
- Hormonal
- Torsion - Intra uterine
- Extra uterine
• Testicular vessel obstruction
Exploration is necessary because total absence is uncommon.
Terato gensity is high.

True undescended testes Law :
• The higher the testis the more Dysgenetic, morphologic features gonad are likely to be.
• 75 % or more is unilateral.
• Spermatic artery shorter than normal is the commonest cause in unilateral.

Bilateral• hormonal (endocrinology) disturbance is common with Bilateral.
•Anatomic defect Limiting descent the test is:
- Ex trophy of the bladder.
- Gastorschisis.
- Pruns belly syndrne.
- hypospedias.
- Inter Sex anomalies.

Hormonal ttt :• The hormonal treatment is indicated for :
- Retractile test.
- Testes down to the scrotal neck.
- Bilateral undescended with proved hormonal disturbance.- Before surgery.
success rate•40%-50% For the 1st – 3th months after treatment.•10% -5% for the 6th months after ttt.

Side effect :
- Systemic effect.
- Testicular degeneration changes due to increase and decrease blood supply in short time.
failure of the medical treatment

Radiologic studies to localize the testis are currently of very little value.
---CT scan and ultrasonography are associated
with high false-negative rates in the evaluation of a non-palpable testis and are not recommended .
---Magnetic resonance angiography has been reported to have a nearly 100% sensitivity but requires sedation or anesthesia and is expensive and may be not cost-effective.
----clinical diagnosis and laparoscopic exploration are the up date diagnostic and therapeutic .
.

Surgery:•orchiopexy.
•Indications.
- to enhance fertility.
- incidence of torsion.
- to repair concomitant hernia.
- to prevent trauma and pain.
- provide easier examination for testicular tumor.- Psychological effect and cosmoses.

- Mobilization of the testicular artery vein, vas deference to lower down the testes in the scrotum directly rather than circuitous course.
Rational of Surgery:

Orchiopexy:

testes
gubernaculums
Released gubernaculums
Cord with the hernia sac Short cord
Hernial sac


Orchiopexy:

Inferior epigastric arteryFloor of the inguinal canal
Retroperitoneal space

Long looped vas
Ove-testes
testes



Thank you