Embed Size (px)
Citation preview
CLINICAL EXAMINATION OF PERIPHERAL
VASCULAR DISEASES
What is PVD?
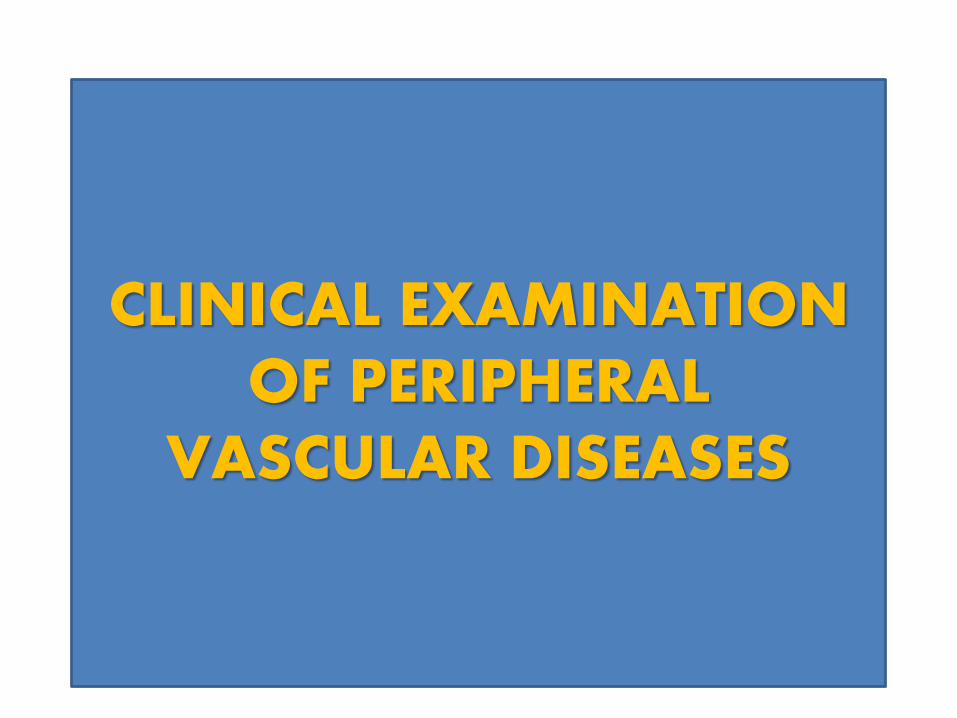
Definition:
• Also known as PAD or
PAOD.
• Occlusive disease of the
arteries of the extremity.
charac. by a reduction in
blood flow and hence 02
through the peripheral
vessels
when the need of the
tissues for 02
exceeds the
supply, areas of ischemia
and necrosis will develop
Pathophysiology:
• Arterial narrowing Decreased blood
flow = Pain
• Pain results from an imbalance between
supply and demand of blood flow that
fails to satisfy ongoing metabolic
requirements.
Factors that can contribute to the development
of peripheral vascular disorders :
atherosclerotic changes
thrombus formation
embolization
coagulability of blood
hypertension
inflammatory process/infection
CAUSES OF ISCHEAMIA
LARGE ARTERY OCCLUSION
-Atherosclerosis
-Embolism.
SMALL ARTERY OCCLUSION
-Buerger`s disease
-Raynaud`s disease
-embolism
-scleroderma
-physical agents –Trauma,radiation,electric
burns,pressure necrosis
ATHEROSCLEROSIS
AGE- above 50yrs
Vessels involved– medium sized & large vessels
aorta,femoral,carotids.
Nature of vessel- Thickned
Pathology – Deposition of atheromatous plaque in
the intima.
Risk factors – smoking, diabetes,hypertensive,
obesity,hypercholesterolaemia.
TAO (BUERGER`S DISEASE)
Age -20-40 yrs
Sex – Exclusively males
Vessel involved –Small & medium sized arteries.
Nature of vessel –Not thickned.
Pathology – Diffusion inflammatory reaction
involving all coats of vessels results
obliterans.
Risk factors – Smoking, hypercoagulable,
autonomic hyperactivity,
low socioeconomic.
RAYNAUD`S DISEASE
(PRIMARY RAYNAUD`S PHENOMENON)
-Occur in young females.
-Upper limbs more involved than lower limbs.
- Its episodic digital ischeamia on exposure to
cold
- Peripheral pulses are normal.
- Recurrent attacks.
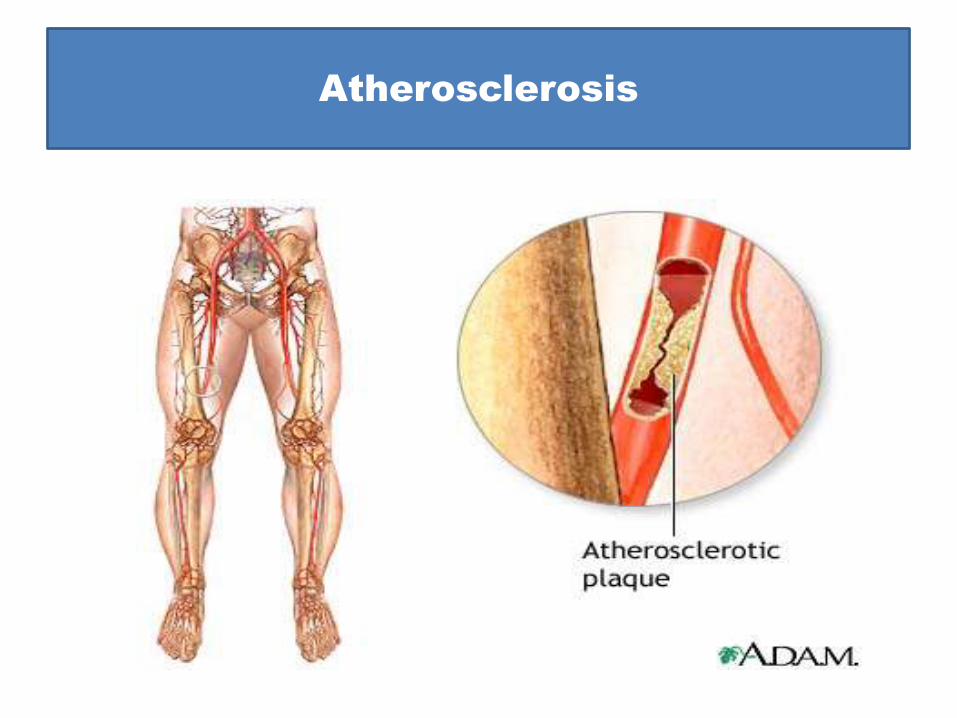
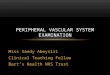
Atherosclerosis
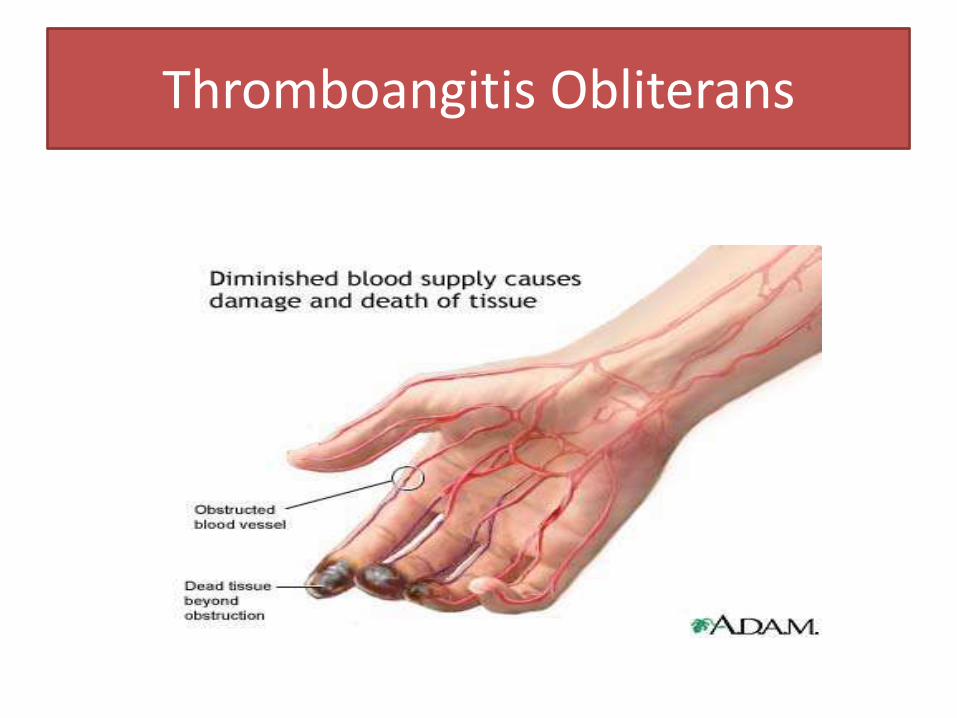
Thromboangitis Obliterans
CLINICAL EXAMINATION
HISTORY
1. AGE & SEX
Atherosclerosis – Older AGE M~ F
BURGER`S Disease - Mostly men age 20-40yrs
RAYNAUD`S DISEASE – Young women
Diabetic arteriopathy - middle age
2. LIMBS AFFECTED
Lower limbs –Buergers`s disease
- Atherosclerotic
-gangrene
Upper limbs- Raynaud`s disease
Superficial gangrene of fingers
-Raynauds disease
- cervical rib
-scalenus anticus syndrome
3.BILATERAL & UNILATERAL
BILATERAL –BURGER`S
-Raynaud`s disease.
Atherosclerotic – intially UL later B/L.
UNILATRAL – Embolus.
Diabetic gangrenous – U/L or B/L.
4.MODE OF ONSET
Spontaneously & gradually
-Atherosclerosis gangrene
- Raynaud`s disease
-Buerger`s disease
Suddenly
- embolic gangrene
Traumatic & infection
- Diabetic
5.PAIN
-site
-charcter
-radiation
TYPES
-Intermittent claudication.
claudication distance
Grades I,II,II (boyd`s classification)
- Rest pain
5.EFFECTS OF HEAT & COLD
Raynaud`s phenomenon
Raynaud`s disease
-local syncope
- local asphyxia
- local recovery ----- local gangrene
6. PARAESTHESIA
- Numbness.
- pins and needles sensation.
7.HISTORY OF SUPERFICAIL PHLEBITIS:
8.INVOLVMENT OF OTHER ARTERIES
-Transient attack, fainting .(stroke)
- chest pain (coronary arteries)
- abdominal pain (mesentric arteries)
- blurred vision (retinal areteries)
HISTORY IMPOTENCE
B/L internal iliac artey occlusion.
PAST HISTORY
cardiac attacks, embolic, frost bite.
PERSONAL HISTORY\: Smoking.
FAMILY HISTORY:
PHYSICAL EXAMINATION
LOCAL EXAMINATION
1.INSPECTION
Change in colour
Pallor
– sudden occlusion of arteries
- spasm of arteries in raynaud`s.
Congestion& cyanosed
-severe ischemia & pre gangrenous stage
2.SIGNS OF ISCHEMIA
1.Thinning of skin
2.Diminished growth of hair,
3.Loss of subcutaneous fat,
4.Trophic changes in nails
5.Muscle wasting
6.Minor ulceration over pressure area
3.BUERGER`S POSTURAL TEST:
Bauerger angle (vascular angle)
-normal indiviual legs will be pink raised
above 90degree
-severe ischemia buerger angle less than 30
degree
4.CAPILLARY FILLING TIME
-severe ischaemic it take 20-30 sec.
5.VENOUS FILLING TIME
-Noramal 5 sec.
-In ischaemic limb veins collapsed.

IN GANGRENE
- Extent & color of gangrene.
-TYPE
dry (mummified) .
wet (putrefying).
-LINE OF DEMARCATION.
- SKIP LESIONS
PALPATION
1. Skin temperature.
2.capillary filling time.
3.venous filling time.
4.crossed leg test (fuchsig test):
oscillatory movements obsent popliteal block.
5.Cold and warm water test.
TEST FOR UPPER LIMBS:
-Elevated arm test.
-Allen`s test.
-Costoclavicular compressive manoeurve.
-Hyperabduction manoeurve
-GANGREANGENOUS AREA.
-CREPITUS.
-LIMB ABOVE GANGRENOUS AREA.
PALPATION OF BLOOD VESSELS.
LOWE LIMBS
-Dorsalis pedis
-posterior tibial
-anterior tibial
-popliteal
-femoral
UPPER LIMB
-radial & ulnar
-brachial
subclavian
common carotid.
Superficaial temporal.
Examination of arterial wall
-PIulse
-condition of wall
- thrombosis of vessel.
CERVICAL RIB
-Adson`s test.
NEUROLOGICAL EXAMINATION:
AUSCULTATION
systolic bruit. In occlusion
-Blood pressure of both arms.
-Ankle brachial pressure index.
-Heart for murmur etc.
Differential diagnosis of limb pain
– Arteritis
– Ischemic intermittent claudication
– Nerve root pain, sciatica, neurogenic
– pseudoclaudication (spinal stenosis)
– Peripheral nerve pain (eg, diabetic neuropathy)
– Phlebitic syndrome after deep venous
thrombosis
– Thromboangiitis obliterans (Buerger disease)
– Venous claudication
INVESTIGATION:
complte blood picture.
blood sugar.
blood lipid profile.
-Doppler ultrasound blood flow detector.
-Duplex scan.
-Plethysmography.
- Angiography
1.Modification factors
a)Smoking Cessation
b)Rigorous BSL con
c)BP reduction
d)Lipid Lowering Therapy
• 2EXERCISE:
a)Claudication exercise rehabilitation program
b)45-60mins 3x weekly for 12 weeks
c)6 months later +6.5mins walking time (before
pain)
3.MEDICAL MANAGEMENT:
a)Antiplatelet therapy e.g.
Aspirin/Clopidogrel
b)Phosphodiesterase Inhibitor e.g. Cilostazol
c)Foot Care
PCI / SURGERY
Indications/Considerations:• Poor response to exercise rehabilitation + pharmacologic
therapy.• Significantly disabled by claudication, poor QOL• The patient is able to benefit from an improvement in
claudication• The individual’s anticipated natural hx and prognosis• Morphology of the lesion (low risk + high probabilty of
operation success)
• PCI:• Angioplasty and Stenting• Should be offered first to patients with significant
comorbidities who are not expected to live more than 1-2 years
• Bypass Surgery:
• Reverse the saphenous vein for femoro-popliteal bypass
• Synthetic prosthesis for aorto-iliac or ilio-femoral bypass
• Others = iliac endarterectomy & thrombolysis
• Current Cochrane review = not enough evidence for Bypass>PCI
• Amputation: Last Resort
ACUTE ARTERIAL DISEASE
sudden occlusion of major peripheral artery.
due to:
-Arterial embolus
-Trauma
-Acute arterial thrombosis
FEATURES OF ACUTE LIMB
ISCHEAMIA
1.PAIN
2.PALLOR
3.PULSELESNESS
4.PERISHING COLD
(POIKILOTHERMIA)
5.PARASTHESIAS
6.PARALYSIS
INVESTIGATION
-Angiography
TREATMENT
- THRMOBOLYSIS
SURGICAL
-embolectomy
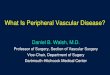
GANGRENE
• Gangrene implies death of macroscopic
portions of tissue; the term necrosis
may be used synonymously.
• It often affects the distal part of a limb
because of arterial obstruction (from
thrombosis, embolus or arteritis).
TYPES
- Dry gangrene
- Wet gangrene.
Signs of gangrene.
1.change of colour
pale,bluish purple and finally black.
2. loss of temperture.
3.loss of sensation.
4.loss of pulsation.
5.loss of function.
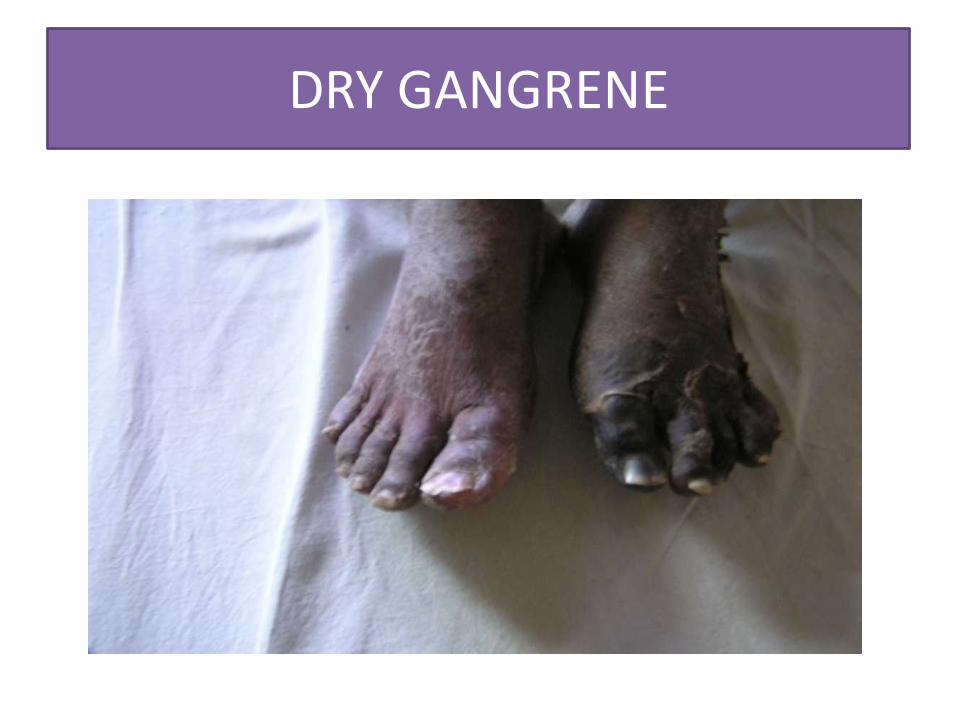
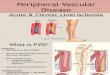
DRY GANGRENE

Wet gangrene
Causes of ischaemia
-Large vessel occlusion.
- Small vessel occlusion.
CAUSES OF GANGRENE.
cardiovascular
-traumatic .
-Infective.
-Diabetic
-Nervous diseases
-Physical gangrene . Frost bite
TREATMENT
- amputation.
THANK YOU