-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
1/22
Peripheral vascular intervention
DR. MIR JAMAL UDDINAssociate Professor of CardiologyNational
Institute of Cardiovascular Diseases
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
2/22
Peripheral vascular intervention
Vascular Access:
1. Common femoral arterial approach
a) Retrograde common femoral artery access
b) Antegrade common femoral artery access
c) Contralateral ileofemoral artery access or cross over
approach
d) Biletaral access
2. Popliteal approach
3. Brachial arterial approach
4. Radial arterial approach
5. Direct percuteneous carotid access or short cut down
technique in
the neck
6. Axillary approach
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
3/22
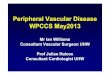
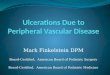
1A. Retrograde common femoral artery access. The most
frequently used vascular access.
Tips of CFA puncture
CFA well below the inguinal ligament is the optimum target
for
puncture.
Can identify the head of the femur by fluroscopy.
Can make a nick at the level of the lower border of the femoral
head.
Puncture should be 1-2cm below the level of inguinal
ligament.
At the level of the middle of head of femur.
Puncture needle with single wall technique is ideal.
Puncture needle should be placed at 450 angle.
Seldinger (double wall) puncture-not suitable
Avoid hydrophilic wire with puncture needle because these wires
can
be cut by needle.
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
4/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
5/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
6/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
7/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
8/22
Drawback of higher puncture:
Inadequate hemostasis
Bleeding
Retroperitoneal hematoma
Shock
Drawback of low puncture
Ineffective hemostasis
A-V fistula
Pseudoaneurysm
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
9/22
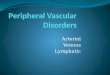
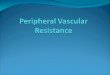
1B. Antegarade common femoral artery access
It is slightly more technically demanding than retrograde
access
& carry higher complication rate.
Tips to do antegrade common femoral artery
(CFA) access.
It is a essential to identify the femoral head under
fluoroscopy.
Skin nicks is made cranial to the centre of the femoral head.
After feeling the pulse of CFA at the level of the centre of
femoral head puncture needle is introduced through the skin
nick directed obliqued & caudally towards the centre of
the
femoral head.
Once CFA has entered guide wire is advanced under fluroscopy
toward SFA which runs medial to the profunada femoris.
AS in the origin of SFA & PFA there is over lapping in AP
view
so if]psilateral 20-400 oblique view should be taken.
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
10/22
Drawback of too cranial puncture:
Insufficient hemostatasis
Retroperitoneal hematoma
Shock
Drawback of too caudal puncture (>3cm below
the inguinal ligament) to the CFA:
Hematoma
Pseudoaneunysm
A-V fistula
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
11/22
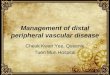
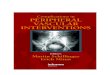
1C. Centralateral ileafemoral artery access or
crossover approach.
Used for intervention of centralateral ileac, CFA Profunda
femoris, SFAparticularly when the lesion is located in the ostium
or very proximal
portion of SFA, internal ileac, very distal lesion of external
iliac arteries.
Technique:-
Arterial sheath in situ in CFA.
Contralateral ileofemoral system is reached by placing a
small
dia 5-6F diagnostic catheter with an acute angle (preferably
IMA
catheter or JR cobra, Hook, Shepard- Hook) at the aortic,
bifurcation.
Catheter manipulated so that the tip of the catheter engages
ostium of contralateral common iliac artery.
J tipped 035// soft hydrophilic guide wire is then advanced to
the
CFA & diagnostic catheter is positioned to FA.
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
12/22
Guide wire is then exchanged with stiff exchange wire.
Diagnostic catheter & chordis sheath removed.
Then cross over sheath 6-8 F is advanced over the stiff quide
wire &placed in contralateral CFA.
Drawback:
In addition to conventional complication of retrogade CFA
puncture:-
1) Dissection of distal abdominal aorta.
2) Dissection of ostium of common iliac artery.
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
13/22
1D. Bilateral approach
Both RT & Lt CF A approach.
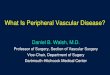
2. Popliteal approach-
20-30% cases standard technique including cross over &
antegrade
approach fail to cross total occlusion of SFA.
Indication-
Long SFA occlusion without visible proximal patent stump.
Prerequisite- Only patent proximal popliteal & distal
femoral artery &
sufficient peripheral run off.
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
14/22
Technique-
4F catheter placed in Ext iliac artery
Patient turned to prone position Popliteal puncture performed
with the assistance of roadmap
fluoroscopy after injection of contrast through 4F catheter.
6f sheath introduced into PA.
Disadvantage:
Frequency of puncture site related complication is
potentially
higher than with conventional technique.
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
15/22
Brachial arterial approach
Almost not used now a days.
If severe iliac obstruction of distal abdominal aorta 100%
occlusion then it can be used.
May be used as an alternative approach for intervention of
renal arteries.
Technique- Puncture of the brachial artery should be performed
in
its distal part above the antecubital fossa.
sheath usually not exceeding 6f
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
16/22
Drawback:
Ischemia to the hand
Spasm of the vessel
Hematoma.
Axillary approach:
Abandmd now a days
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
17/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
18/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
19/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
20/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
21/22
-
7/27/2019 Peripheral Vascular Intervention, lecture, nicvd
22/22