Embed Size (px)
Citation preview


Complications in Peripheral VascularInterventions
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page i

CPVI_Prelims.qxp 4/5/2007 5:09 PM Page ii

Complications in Peripheral Vascular Interventions
Edited by
MARTIN SCHILLINGER MD
ProfessorDepartment of Internal Medicine IIDivision of AngiologyUniversity of Vienna Medical SchoolViennaAustria
ERICH MINAR MD
ProfessorDepartment of Internal Medicine IIDivision of AngiologyUniversity of Vienna Medical SchoolViennaAustria
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page iii

© 2007 Informa UK Ltd
First published in the United Kingdom in 2007 by Informa Healthcare, Telephone House,69–77 Paul Street, London EC2A 4LQ. Informa Healthcare is a trading division of Informa UKLtd. Registered Office, 37/41 Mortimer Street, London W1T 3JH. Registered in England andWales number 1072954.
Tel: +44 (0)20 7017 5000Fax: +44 (0)20 7017 6336Website: www.informahealthcare.com
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying,recording, or otherwise, without the prior permission of the publisher or in accordance withthe provisions of the Copyright, Designs and Patents Act 1988 or under the terms of anylicence permitting limited copying issued by the Copyright Licensing Agency, 90 TottenhamCourt Road, London W1P 0LP.
Although every effort has been made to ensure that all owners of copyright material have beenacknowledged in this publication, we would be glad to acknowledge in subsequent reprints oreditions any omissions brought to our attention.
Although every effort has been made to ensure that drug doses and other information are presented accurately in this publication, the ultimate responsibility rests with the prescribingphysician. Neither the publishers nor the authors can be held responsible for errors or for anyconsequences arising from the use of information contained herein. For detailed prescribinginformation or instructions on the use of any product or procedure discussed herein, pleaseconsult the prescribing information or instructional material issued by the manufacturer.
A CIP record for this book is available from the British Library.Library of Congress Cataloging-in-Publication Data
Data available on application
ISBN-10: 1 84184 628 7ISBN-13: 978 1 84184 628 6
Distributed in North and South America byTaylor & Francis6000 Broken Sound Parkway, NW, (Suite 300)Boca Raton, FL 33487, USA
Within Continental USATel: 1 (800) 272 7737; Fax: 1 (800) 374 3401Outside Continental USATel: (561) 994 0555; Fax: (561) 361 6018Email: [email protected]
Distributed in the rest of the world byThomson Publishing ServicesCheriton HouseNorth WayAndover, Hampshire SP10 5BE, UKTel: +44 (0)1264 332424Email: [email protected]
Composition by Exeter Premedia Services Private Ltd, Chennai, India
Printed and bound in India by Replika Press Pvt Ltd.
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page iv

Contents
List of contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Foreword Michael R Jaff . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . x
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xi
Part I: Complications – general considerations
1. Introduction to complications in peripheral vascular interventions – frequency of complications and worst scenarios Martin Schillinger . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2. Identifying (high) risk patients for endovascular treatment – unfavorable medical comorbidities Erich Minar . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3. Being prepared – standards for patient care and adequate bail-out equipmentMartin Schillinger . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
4. a. Contrast media associated complications Rainer Oberbauer . . . . . . . . . . . . . . . . . . . . . . . . 27
b. General complications of angiography and peripheral interventions – radiotoxicityEberhard Kuon and Michael Wucherer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Part II: Specific complications by vessel area or specific scenarios
5. Arterial and venous access site complications Martin Schillinger . . . . . . . . . . . . . . . . . . . . . . . 51
6. a. Complications of pharmacologic interventions: antiplatelet, antithrombotic, and anticoagulant agents Hong H Keo and Iris Baumgartner . . . . . . . . . . . . . . . . . . . . . . . . . 71
b. Complications of thrombolytic therapy in peripheral vascular interventions Jose A Silva and Christopher J White . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
7. Carotid stenting complications from the femoral artery to the intracranial circulation Robert D Ecker, Horst Sievert, and L Nelson Hopkins . . . . . . . . . . . . . . . . . . . . . . . . . . 97
8. Complications in percutaneous subclavian and vertebral artery interventions Julio A Rodriguez, Francisco Guerrero-Baena, Dawn M Olsen, and Edward B Diethrich . . . . . . . . 117
9. Aortic aneurysmal disease Joe T Huang, Takao Ohki, and Frank J Veith . . . . . . . . . . . . . . . . . . 139
10. Complications in renal and mesenteric vascular interventions Martin Schillinger and Thomas Zeller . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 159
11. Complications of aorto-iliac intervention Deepa Gopalan and Peter Gaines . . . . . . . . . . . . . . . 177
12. Femoropopliteal segment Richard R Heuser . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 187
13. Complications of tibioperoneal interventions Erich Minar and Lanfroi Graziani . . . . . . . . . . 201
14. Complications in the percutaneous management of failing hemodialysis fistulas and grafts Dierk Vorwerk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
15. Venous interventions C Binkert . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 219
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page v

CPVI_Prelims.qxp 4/5/2007 5:09 PM Page vi

Iris Baumgartner MD
Professor and Head of AngiologyDivision of AngiologySwiss Cardiovascular CenterUniversity HospitalBernSwitzerland
Christoph Binkert MD
Associate Professor of RadiologyAssociate Director of Interventional RadiologyBrigham and Women’s HospitalHarvard Medical School Boston, MAUSA
Edward B Diethrich MD
Medical Director Arizona Heart Institute and Arizona Heart Hospital Phoenix, AZUSA
Robert D Ecker MD
Departments of Neurosurgery University at Buffalo and Toshiba StrokeResearch CenterSchool of Medicine andBiomedical SciencesUniversity at BuffaloState University of New YorkandMillard Fillmore Gates HospitalKaleida Health, BuffaloNew York, NYUSA
Peter Gaines MB ChB, FRCP, FRCR
Professor, Sheffield Vascular InstituteNorthern General HospitalSheffieldUK
Deepa Gopalan MB BS, MSc, MRCP, FRCR
Fellow, Sheffield Vascular InstituteNorthern General HospitalSheffieldUK
Lanfroi Graziani MD
Servizio di EmodinamicaInstituto Clinico ‘Citta di Brescia’BresciaItaly
Francisco Guerrero-Baena MD
Vascular Surgery FellowArizona Herat Institute/HospitalPhoenix, AZUSA
Richard Heuser MD
Director of CardiologySt Luke’s Medical CenterPhoenix, AZandMedical DirectorPhoenix Heart CenterPhoenix, AZandClinical Professor of MedicineUniversity of Arizona College of MedicineTucson, AZUSA
Contributors
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page vii

L Nelson Hopkins MD
Department of Radiology University at Buffalo and Toshiba StrokeResearch CenterSchool of Medicine and Biomedical SciencesUniversity at BuffaloState University of New YorkandMillard Fillmore Gates HospitalKaleida HealthBuffaloNew York, NYUSA
Joe T Huang MD
Division of Vascular SurgeryDepartment of SurgeryAlbert Einstein College of MedicineMontefiore Medical CenterNew York, NYUSA
Hong H Keo MD
Division of AngiologySwiss Cardiovascular CenterUniversity HospitalBernSwitzerland
Eberhard Kuon MD
Department of CardiologyKlinik Fraenkische SchweizEbermannstadtGermany
Erich Minar MD
ProfessorDepartment of Internal Medicine IIDivision of AngiologyUniversity of Vienna Medical SchoolViennaAustria
Rainer Oberbauer MD
ProfessorDepartment of Internal Medicine IIIDivision of Nephrology and DialysisViennaAustria
Takao Ohki MD, PhD
Professor and ChiefDepartment of Vascular SurgeryJikei University School of MedicineTokyoJapanandProfessor of SurgeryNorth Shore LIJ Health SystemAlbert Einstein College of MedicineLake SuccessNew York, NYUSA
Dawn M Olsen PAC
Vascular Surgery Physician AssistantArizona Heart Institute/HospitalPhoenix, AZUSA
Julio A Rodriguez MD
Director of Vascular Surgery DepartmentMedical Director of Wound Healing CenterArizona Heart Institute/HospitalPhoenix, AZUSA
Martin Schillinger MD
ProfessorDepartment of Internal Medicine IIDivision of AngiologyUniversity of Vienna Medical SchoolViennaAustria
Horst Sievert MD
ProfessorCardiovascular CenterBethanienFrankfurtGermany
Jose A Silva MD
Department of Cardiology Ochsner Clinic FoundationNew Orleans, LAUSA
viii LIST OF CONTRIBUTORS
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page viii

LIST OF CONTRIBUTORS ix
Frank J Veith MD
Division of Vascular SurgeryDepartment of SurgeryAlbert Einstein College of MedicineMontefiore Medical CenterNew York, NYUSA
D Vorwerk MD
Professor of RadiologyChairmanDepartment of Diagnostic and Interventional RadiologyKlinikum IngolstadtIngolstadtGermany
Christopher J White MD
Chairman Department of Cardiology Ochsner Clinic FoundationNew Orleans, LAUSA
Michael Wucherer PhD
Institute of Medical PhysicsKlinikum NürnbergNürnbergGermany
Thomas Zeller MD
ChairmanDepartment of AngiologyHerzzentrum Bad KrozingenBad KrozingenGermany
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page ix

With the aging population in industrializedcountries, increased body weight among manyWestern countries, resulting in a pandemic of dia-betes mellitus, and continued tobacco abuse, it isof no surprise that peripheral arterial disease isoccurring with increased frequency. Primarilydue to atherosclerosis, arterial occlusive diseaseof the lower extremity, renal, mesenteric, brachio-cephalic, and carotid arteries presents significantchallenges to practicing physicians. In addition,aneurysmal disease of the thoracic and abdominalaorta represents significant risk to life.
Due to the advances in techniques and tech-nology, endovascular approaches now representthe initial strategy for management of these com-plex patients. As devices become more flexible,lower profile, and more precise, percutaneoustransluminal angioplasty, stents, covered stents,atherectomy, laser, cryotherapy, and other modal-ities will continue to be used in difficult anatomicsituations.
Undoubtedly, due to the challenging natureof atherosclerotic vascular disease, complications
will become part and parcel of the interventionists’practice. The key, of course, will be early recogni-tion with prompt and appropriate management.
This textbook is a welcome addition to thelibrary of any physician involved in the diagnosisand management of vascular disease. Recognizedexperts in the field, representing multiple special-ties, cover the broad spectrum of vascular com-plications. Each author methodically evaluatesthe specific complications of each vascular bed,discussing important tips to manage the com-plications, as well as methods to avoid them initially.
Congratulations to Professors Schillinger and Minar who provide key insights into thediagnosis and management of iatrogenic vas-cular complications, along with managementstrategies.
Michael R Jaff, DOAssistant Professor of MedicineMassachusetts General Hospital
Boston, MA, USA
Foreword
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page x

Minimal invasive endovascular treatment ofperipheral arteries is one of the most rapidlyevolving techniques in interventional therapies.Advanced technologies enable treatment of morecomplex lesions in severely diseased patients.Increasing evidence suggests that, particularlyin high-risk patients, endovascular solutionsoffer substantial advantages compared to vascu-lar surgical procedures. Nevertheless, growingnumbers of procedures are associated with anincreased incidence of complications. Knowledgeof specific complications in different vessel areaswill support the interventionist in preventing suchadverse events and, if necessary, provide consid-erable reassurance if such complications need tobe resolved. The present book aims to systemat-ically cover specific complications in peripheralvascular interventions. Typical and atypical com-plications are described for major peripheralvessel areas and methods to handle these eventsare outlined.
The book is divided in two parts: Part I reviewsgeneral aspects on complications in peripheralinterventions, Part II covers the specific vesselareas. Each chapter on the specific vessel areasincludes
• Introduction to the frequency and type ofcomplications in this vessel area
• Factors identifying patients at high-risk forcomplications
• Complications of specific interventional stepsand tools
• Methods to detect potential complications –which diagnostic steps are needed routinelyto rule out or identify complications
• Endovascular, surgical, and medical tech-niques to resolve complications
• Methods to avoid complications• Summary• Check list for emergency equipment for
interventions in this specific vessel area.
We intended to focus on practical tips for theinterventionist in the cath lab, to review compli-cated cases and outline different strategies inreal-life cases, and thus to share the experienceof high-volume interventionists with the reader.We hope that this book is a practical guide forquality improvement which will help to improvethe safety of our patients undergoing peripheralvascular interventions.
Martin SchillingerErich Minar
Preface
CPVI_Prelims.qxp 4/5/2007 5:09 PM Page xi

CPVI_Prelims.qxp 4/5/2007 5:09 PM Page xii

Part I
Complications – general considerations
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 1

CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 2

INTRODUCTION
Endovascular therapy emerged as one of themost rapidly evolving fields in medicine duringthe last decade. In 1964 Dotter and Judkinsreported the first angioplasties performed in thefemoropopliteal vessel area using coaxial cathetersystems up to 12 French gauge in diameter. It soon became apparent that the concept of vessel-sized dilators was not suitable, howeverit took another 10 years until Grüntzig and Hopffdescribed a coaxial balloon catheter that inflatedto a fixed diameter and thus initiated the era ofballoon angioplasty. The equipment was contin-uously miniaturized and thus could be used invirtually any vessel segment. Currently, endovas-cular therapy has replaced vascular surgery formany indications. The use of stents has improvedthe durability of the results, and advanced tech-nologies now enable the treatment of complexlesions in patients who otherwise could nothave been revascularized.
Despite major advances during recent years,complications in peripheral vascular interven-tions remain a major issue. Because angioplastyfor most entities of peripheral vascular diseasedoes not generally have a more durable resultthan surgical reconstruction, its use is justified
mainly by its reduced risk combined with a rea-sonable likelihood for success. The latter can beachieved in the vast majority of cases; technicalsuccess rates usually range between 95 and almost100%. In contrast, complications increase mor-bidity and mortality, prolong the hospital stay,and increase the costs for healthcare providers.Strategies for prevention and management of com-plications therefore are a major goal in educationand training of interventionists. The present bookgives an overview about complications in periph-eral vascular interventions, describes how torecognize risk factors for pitfalls, and reportsstrategies to prevent and handle critical situations.
FREQUENCY AND IMPACT OF COMPLICATIONS
The frequency of complications mainly dependson the clinical setting in which the interventionsare performed. Emergency interventions for rup-tured aortic aneurysm still carry a high mortalityrisk of between 15 and 50%. In contrast, electiveperipheral angioplasties can be done with com-plication rates below 1%. Table 1.1 gives anoverview on the frequency of complications afterelective angioplasty procedures.1
1
Introduction to complications in peripheralvascular interventions – frequency ofcomplications and worst scenariosMartin Schillinger
Introduction • Frequency and impact of complications • Classification of complications •Worst scenarios
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 3

The frequency and characteristics of compli-cations differ for specific vessel areas; details aregiven in the relevant chapters. The major princi-ples of complications, however, unequivocallyapply to all vascular segments. Table 1.2 givesan overview on reported frequencies of compli-cations for interventions in different vesselsareas.2–23 Quantitatively, the frequencies of com-plications in different vessel areas seem compa-rable; the impact of complications, however,differs widely for the specific vessel areas. Forexample, embolization is usually a relatively
benign complication in peripheral arteries, butremains a major concern during carotid stent-ing. Principles of complications are briefly dis-cussed below.
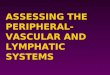
The most frequent complications involve thevascular access site.24,25 On the one hand, the ratesof access site complications can be substantiallyreduced due to decreasing diameters of sheaths,low-traumatic puncture techniques, adequatepreinterventional imaging modalities, and mod-ern closure devices. On the other hand, aggres-sive anticoagulant therapies in high-risk patientsincrease the likelihood for puncture site compli-cations. Therefore, a frequency of 2 to 4% forpuncture-related complications remains the mostfrequent clinical problem after endovascular pro-cedures (Figures 1.1 and 1.2).
Complications at the site of angioplasty usuallyare rare and most of these complications can beresolved by endovascular techniques.
• The formation of clots during the interventionat the site of angioplasty hardly ever occurs inpatients under adequate antiplatelet therapy
4 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 1.1 Complications of electiveangioplasty
Complication Incidence (%)
Puncture site (total) 4.0Bleeding 3.4False aneurysm 0.5Arteriovenous fistula 0.1
Angioplasty site (total) 3.5Thrombus 3.2Rupture 0.3
Distal vessel (total) 2.7Dissection 0.4Embolization 2.3
Systemic (total) 0.4Renal failure 0.2Myocardial infarction (fatal) 0.2Cerebrovascular accident (fatal) 0.6
ConsequencesSurgical repair 2.0Limb loss 0.2Mortality 0.2
Table 1.2 Frequencies of complications forelective angioplasty and stenting proceduresin different vessel areas
Intervention Incidence (%)
Carotid arteries 6–10Subclavian and vertebral arteries 6–10Aortic stent graft implantation 8–12Renal and mesenteric arteries 4–10Iliac arteries 4–8Femoral arteries 4–6Below the knee arteries 4–8Venous interventions 2–6 Figure 1.1 Large hematoma after inguinal arterial
puncture.
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 4

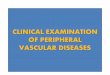
and when heparin or bivalirudin is used withadequate dosage and monitoring during theintervention. The incidence of early stentthrombosis in peripheral interventions couldbe dramatically reduced by the introductionof dual antiplatelet therapy combining aspirinand thienopyridines and is encountered inless than 2% of the cases (Figure 1.3).22
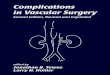
• Dissection is a common problem after balloonangioplasty (Figure 1.4). Its frequency varieswith the anatomy of the target vessel siteand the length of the treated segment, and isstrongly correlated with the balloon-to-arteryratio.
• Similarly, arterio-venous (AV) fistulas arecommon after revascularization of long seg-ment occlusion, especially in the case of subin-timal angioplasty (Figure 1.5). Nevertheless,the use of stents has virtually eliminated theproblems associated with dissection or AVfistulas at the treated segment, as long as awire can be successfully passed to the truevessel lumen.
• Bleeding and rupture are rare but sometimesdramatic clinical problems. Perforation mayoccur due to improper manipulation withthe wire (Figure 1.6), particularly when stiff
INTRODUCTION TO CPVI – FREQUENCY OF COMPLICATIONS 5
Figure 1.2 Pseudoaneurysm in the right groin 24 hoursafter removal of a 7 French sheath.
Figure 1.3 Acute stent thrombosis 24 hours after long segment stenting of the superficial femoral artery in a patientunder aspirin monotherapy.
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 5

hydrophilic guidewires are used. Rupturemay occur during balloon angioplasty of rigidobstructions (Figure 1.7), or due to vastoversizing of balloons. Typical settings forruptures are the origin of calcified visceralarteries, heavily calcified lesions in the aorta,and the external iliac artery.
Complications at vessel segments distal tothe target site
• Distal dissections can be mostly avoided bycautious handling of the guidewire. Keepingan eye on the tip of the guidewire alwayshas to be considered, especially when longover-the-wire (OTW) guidewires are used, e.g.for over-the-bifurcation procedures. Duringchanging maneuvers of catheter material with
long OTW guidewires the tip of the wirealways should be visualized by fluoroscopy.
• Peripheral embolization is a problem mainlyin fresh thrombotic lesions. Nevertheless, par-ticularly in case of long chronic total occlusions,the risk for peripheral macroembolization
6 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 1.4 Long segment flow-limiting dissection afterballoon angioplasty of a superficial femoral artery.
Figure 1.5 AV fistula of the left popliteal artery.
Figure 1.6 Perforation with the tip of the guidewire in thesubsegmental renal arteries during renal artery stenting.
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 6

always has to be considered and the outflowhas to be checked routinely (Figure 1.8).Besides the risk of embolizing large particles,all interventions carry a risk for micro-embolic showers. The clinical sequelae ofthese microemboli can be clinically silent orfatal, depending on the affected vessel area.
Much attention has been paid to avoid cerebralmicroembolization during carotid stenting,2–8
and embolization during renal angioplastyleading to renal failure has also become anissue during recent years.12 Most frequently,however, clinical signs of embolization can beobserved at the foot (Figure 1.9). These emboliare usually extremely painful for the patientand it may take weeks to months until thepain completely resolves. Heparin, anti-inflammatory drugs, and corticosteroids areused to treat these patients. In this context, theentity of cholesterol emboli has to be men-tioned, a rare clinical complication with signsof peripheral embolization, systemic inflam-mation, and progressive renal failure.
Systemic complications
Systemic complications include renal failure due to contrast nephropathy,26 infection withsepticemia, myocardial infarction, and stroke.Fortunately, the latter ones very infrequently areobserved in territories other than coronary orcarotid interventions. Renal failure remains a clin-ically relevant problem, particularly in diabeticpatients, patients with pre-existent renal dysfunc-tion, and patients with congestive heart failure.
INTRODUCTION TO CPVI – FREQUENCY OF COMPLICATIONS 7
Figure 1.7 Large extravasation due to rupture of the leftexternal iliac artery during balloon angioplasty.
Figure 1.8 Distal embolization after stenting of the proximal superficial femoral artery: the tibioperoneal trifurcation isoccluded by embolic material.
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 7

Device-related complications
Device-related complications during interventionsare rather infrequent events, although brokenwires, malfunctioning stents, and embolizationof catheter shaft material has been reported inalmost all vessel areas.
• Infection of implants also occurs very infre-quently. Predominantly with historical cov-ered stent grafts, larger numbers of infectedimplants were reported.
• In contrast to these anecdotal complications,chronic device failure due to stent fractureseems to occur in a considerable proportion ofpatients, particularly in the femoropoplitealvessel area, and has become a matter of con-cern (Figures 1.10 and 1.11).
Finally and most importantly, the clinicalimpact and consequences of complications of periph-eral vascular interventions mainly depend onthe skills of the interventionists. Almost all ofthe above mentioned complications can be pre-vented by careful patient selection, planning of the
8 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 1.9 Microemboli to the foot after renal angioplastywith left retrograde arterial access. Figure 1.10 Stent fractures in the superficial femoral artery.
Figure 1.11 Stentgraft fracture and endoleak formationleading to recurrence of a popliteal aneurysm 14 monthsafter initially successful stentgraft implantation.
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 8

procedure, and selection of adequate materials.If complications occur, it will be the skill andexperience of the interventionist who has toresolve the problem in the cath lab that deter-mine whether it will just be a challenging casewith a good clinical outcome or a complicatedcase which results in a clinical catastrophe.
CLASSIFICATION OF COMPLICATIONS
According to the Society of InterventionalRadiology guidelines, complications are classifiedas minor or major.Minor complications:
• no therapy, no consequence, or• nominal therapy, no consequence; includes
overnight admission for observation only.
Major complications:
• require therapy, minor hospitalization (lessthan 48 hours)
• require major therapy, unplanned increasein level of care, prolonged hospitalization(greater than 48 hours)
• have permanent adverse sequelae, or• result in death.
WORST SCENARIOS
The ‘hit list’ of worst scenarios is certainly a very individual ranking of personal nightmares.Nevertheless, statistics seem to hold true formost interventionists as some major complica-tions occur sooner or later during an interven-tional career.
Vessel rupture and massive bleeding is one of thefew acutely life-threatening complications whichthe interventionist always has to be prepared todeal with. Immediate recognition of the problemand rapid sealing of the site of rupture may savethe patient’s life. The premise for successful seal-ing of rupture sites is an adequate armentariumof the cath lab: this mainly includes large balloonsfor immediate balloon occlusion, covered stentswith different diameters and lengths, and vascularcoils in different sizes. Figure 1.12 shows anexample of a ruptured renal artery during angio-plasty of a left-sided ostial renal artery stenosis.The patient developed massive abdominal pain
INTRODUCTION TO CPVI – FREQUENCY OF COMPLICATIONS 9
Figure 1.12 Rupture of the renal artery during balloon angioplasty of a left-sided ostial renal artery stenosis and successful sealing of the rupture site using a large compliant balloon. (Courtesy of Dr P Waldenberger, Innsbruck,Austria.)
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 9

during balloon inflation and became hemody-namically unstable immediately thereafter. Therupture site was acutely sealed by a large, com-pliant balloon in the abdominal aorta, coveringthe origin of the left renal artery. The patient wastaken urgently to the operating theatre andunderwent an emergency operation. The vascularsurgeon found the renal artery completely rup-tured from the aorta and was able to resolve theproblem by bypass surgery. The patient survivedwith a prolonged stay in the intensive care unit.
Acute vessel occlusion where perfusion is crucial.Acute ischemia during endovascular treatmentcan be relatively benign or potentially life-threatening, mainly depending on the ischemiatolerance of the affected organ system. Thehuman brain is without doubt the least tolerantto ischemia. Acute occlusion of the arteries ofthe brain therefore is a true nightmare of carotidinterventionists. Figure 1.13 shows an exampleof an acute occlusion of the carotid artery duringstent implantation. Fortunately, this was due toa severe spasm of the internal carotid arterywhich could be resolved by intra-arterial appli-cation of 0.1 mg nitroglycerin and removal ofthe filter wire without any clinical complications.
Perforation and compartment syndrome maycomplicate a procedure hours after the patienthas left the cath lab, when subacute bleedingremains initially unrecognized or left untreated.Compartment syndromes more frequently occurin the popliteal fossa and below the knee, wheresmaller amounts of blood cause relevant com-pression and increase in compartment pressures.Figure 1.14 shows an angiogram with massivebleeding to the popliteal fossa after failed recanal-ization of a P1 occlusion. The complication couldbe managed by prolonged balloon inflation andexternal compression. Nevertheless, the patienthad to undergo fasciotomy the day after the inter-vention and had a markedly prolonged hospitalstay.
Finally, contrast-induced renal failure leading topermanent renal replacement therapy certainlybelongs to the absolute worst scenarios afterelective endovascular procedures.26 Renal fail-ure after endovascular procedures substantiallyincreases patients’ morbidity and mortality andreduces quality of life. Fortunately, this compli-cation is rare, mostly predictable, and can beavoided by adequate patient selection, patientpreparation, and careful use of contrast media.
10 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 1.13 Acute occlusion of the carotid artery during filter-protected carotid stenting. Complete restoration of flow wasachieved after application of 0.1 mg nitroglycerin, which resolved the severe spasm of the artery.
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 10

In conclusion, the hit list of worst complica-tions will permanently change during the life ofthe interventionist. Certainly, we don’t have to make all mistakes ourselves to learn how toavoid them. We hope that this book will help toclarify risk factors and mechanisms for compli-cations and provide strategies to handle andavoid adverse outcomes.
REFERENCES
1. Pentecost MJ, Criqui MH, Dorros G et al. Guidelines forperipheral percutaneous transluminal angioplasty ofthe abdominal aorta and lower extremity vessels.Circulation 1994; 89: 511–31.
2. Sherif C, Dick P, Sabeti S et al. Neurological outcomeafter carotid artery stenting compared to medical ther-apy in patients with asymptomatic high grade carotidartery stenosis. J Endovasc Ther 2005; 12: 145–55.
3. Boltuch J, Sabeti S, Amighi J et al. Procedure-relatedcomplications and neurological adverse events afterprotected vs. unprotected carotid stenting. J EndovascTher 2005; 12: 538–47.
4. Ahmadi R, Willfort A, Lang W et al. Carotid arterystenting: effect of learning and intermediate term mor-phological outcome. J Endovasc Ther 2001; 8: 539–49.
5. Ahmadi R, Schillinger M, Sabeti S et al. Renal arteryPTA and stent implantation: immediate and late clinicaland morphological outcome. Wien Klin Wochenschr2002; 114: 21–7.
6. Mlekusch W, Schillinger M, Sabeti S et al. Frequencyand risk factors for hemodynamic instability due tohypotension and bradycardia after elective carotidstenting. J Endovasc Ther 2003; 10: 851–9.
7. Sabeti S, Schillinger M, Mlekusch W et al. Contralateralhigh grade carotid artery stenosis or occlusion is notassociated with an increased risk for poor neurologicaloutcome after carotid stenting. Radiology 2004; 230:70–6.
8. Schillinger M, Dick P, Wiest G et al. Covered vs. bare selfexpanding stents for endovascular treatment of carotidartery stenosis. J Endovasc Ther 2006; 13: 508–14.
9. Schillinger M, Haumer M, Schillinger S et al. Risk strati-fication after subclavian artery PTA: increased rate of restenosis after stent implantation. J Endovasc Ther2001; 8: 550–7.
10. Schillinger M, Haumer M, Schillinger S et al. Outcomeof conservative vs. interventional treatment of subcla-vian artery stenosis. J Endovasc Ther 2002; 9: 139–46.
11. Sabeti S, Schillinger M, Mlekusch W et al. Contrastinduced acute renal failure in patients undergoing renalartery angiography vs. renal artery PTA. Eur J VascEndovasc Surg 2002; 24: 156–60.
12. Amighi J, Sabeti S, Dick P et al. Impact of rapidexchange vs. over-the-wire technique on procedure com-plications of renal artery angioplasty. J Endovasc Ther2005; 12: 233–9.
13. Schillinger M, Exner M, Mlekusch W et al. Fibrinogenand restenosis after endovascular treatment of the iliacarteries: a marker of inflammation or coagulation?Thromb Haemost 2002; 87: 959–65.
14. Ahmadi R, Ugurluoglu A, Schillinger M et al. Duplex-ultrasound guided femoropopliteal PTA: initial and 12 months results – a case control study. J EndovascTher 2002; 9: 873–81.
15. Dick P, Mlekusch W, Sabeti S et al. Outcome afterendovascular treatment of deep femoral artery stenosis:results in a consecutive patient series and systematicreview of the literature. J Endovasc Ther 2006; 13: 221–8.
16. Sabeti S, Schillinger M, Amighi J et al. Patency of nitinolvs. wallstents in the superficial femoral artery – a propensityscore adjusted analysis. Radiology 2004; 232: 516–21.
17. Schillinger M, Haumer M, Schlerka G et al. Restenosisafter percutaneous transluminal angioplasty in patientswith peripheral artery disease: the role of inflamma-tion. J Endovasc Ther 2001; 8: 477–83.
18. Amighi J, Sabeti S, Schlager O et al. Outcome of conser-vative vs. interventional treatment of patients with
INTRODUCTION TO CPVI – FREQUENCY OF COMPLICATIONS 11
Figure 1.14 Perforation and bleeding to the popliteal fossaafter failed recanalization of a P1 occlusion. The patienthad to undergo fasciotomy the day after the procedure.
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 11

intermittent claudication. Eur J Vasc Endovasc Surg2004; 27: 254–8.
19. Sabeti S, Amighi J, Ahmadi R et al. Outcome of long-segment femoropopliteal stent implantation using self-expanding nitinol stents. J Endovasc Ther 2005; 12: 6–12.
20. Schlager O, Dick P, Sabeti S et al. Stenting of the super-ficial femoral artery – the dark sides: restenosis, clinicaldeterioration and fractures. J Endovasc Ther 2005; 12:676–84.
21. Schillinger M, Mlekusch W, Haumer M et al. One yearfollow up after percutaneous transluminal angioplastyand elective stent implantation in de-novo versus recur-rent femoropopliteal lesions. J Endovasc Ther 2003; 10:288–97.
22. Schillinger M, Sabeti S, Loewe C et al. Balloon angio-plasty versus implantation of nitinol stents in thesuperficial femoral artery. N Engl J Med 2006; 354:1879–88.
23. Schillinger M, Exner M, Mlekusch W et al. Endovascularrevascularization below the knee: 6-months results andpredictive value of C-reactive protein level. Radiology2003; 227: 419–25.
24. Mlekusch W, Dick P, Sabeti S et al. CloSur PAD vs.manual compression for puncture site management afterpercutaneous procedures. J Endovasc Ther 2006; 13: 23–31.
25. Mlekusch W, Haumer M, Mlekusch I et al. Predictionof iatrogenic pseudoaneurysm after percutaneousendovascular procedures. Radiology 2006; 240: 597–602.
26. Schillinger M, Haumer M, Mlekusch W et al. Predictingrenal failure after peripheral percutaneous transluminalangioplasty in high-risk patients. J Endovasc Ther 2001;8: 609–14.
27. Standards of Practice Committee of the Society ofCardiovascular and Interventional Radiology. Standardsfor interventional radiology. J Vasc Interv Radiol 1991;2: 59–65.
12 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter01.qxp 4/5/2007 2:37 PM Page 12

IMPORTANCE OF ACCURATE IDENTIFICATIONOF HIGH RISK PATIENTS
Risk identification should allow the clinician todevelop the optimal treatment strategy for thepatient and to provide better informed consent.From a scientific point, evaluation of comorbid-ity is important in healthcare outcomes researchbecause variation in baseline patient characteris-tics may significantly contribute to differences inoutcome.1,2 Clinical reports that evaluate revas-cularization procedures, particularly those thatcompare different treatment methods, may bedifficult to interpret when differences in factorsthat can affect complication rate and outcomeare not identified and characterized. The com-pleteness and reliability of data concerningcomorbidity and therefore the risk of any inter-vention affect the validity of risk adjustment mod-els and the accuracy of comparisons betweendifferent patient cohorts. However, it shouldalso be stressed that risk factors that affect peri-interventional morbidity and mortality rates arenot identical with those that relate to patency.
Concerning the group of patients undergoingendovascular procedures, the type of comor-bidity can be classified as vascular or non-vascular. Due to lack of data in the literature, therecommendations given in this chapter with
regard to pre-interventional evaluation to iden-tify (high) risk patients for endovascular treat-ment are mainly based on personal experienceand on data from surgical literature.
VASCULAR COMORBIDITY
Atherosclerosis as systemic disease
Most of the patients treated by endovascularprocedures suffer from atherosclerotic disease.Other causes for occlusive or aneurysmatic disease – such as inflammatory diseases – arerare. Atherosclerosis is a systemic disease notlimited to a single vessel region. This explainsthe often found coincidence of either sympto-matic or asymptomatic vascular disease in thedifferent areas.
Prevalence of cardiovascular comorbidity
The reported prevalence of coronary heart dis-ease (CHD) in patients with peripheral arterialocclusive disease (PAOD) ranges from 14 to90%, depending on the sensitivity of the diag-nostic test.3 In a landmark study by Hertzer et al,4 coronary angiography was performed in 1000 patients (mean age 64 years) underconsideration for elective peripheral vascular
2
Identifying (high) risk patients forendovascular treatment – unfavorablemedical comorbiditiesErich Minar
Importance of accurate identification of risk patients • Vascular comorbidity • Non-vascularcomorbidity • Is risk reduction possible by drug application? • Summary
CPVI_Chapter02.qxp 4/5/2007 2:38 PM Page 13

reconstruction. The primary vascular diagnosiswas abdominal aortic aneurysm (AAA) in 263patients, cerebrovascular disease (CVD) in 295,and PAOD in 381. Severe correctable CHD wasidentified in 25% of the entire series (AAA, 31%;CVD, 26%; and PAOD, 21%). The prevalence ofrenal artery stenosis in patients with PAOD isreported up to 40%.
This high comorbidity is responsible for thepoor long-term prognosis in many of these patientgroups. The annual mortality rate derived fromepidemiologic studies, e.g. of patients withlower extremity PAOD, is 4 to 6%, and is highestin those with the most severe disease. The 1-yearmortality rate in patients with critical limb ische-mia is approximately 25% and may be as high as45% in those who have undergone amputation.
Data in the literature concerning cardiovascular risk evaluation
As a consequence of the coexistence of athero-sclerosis in many vessel regions, there is anincreased risk of myocardial infarction, stroke,and cardiovascular death in these patients. Inde-pendent of this long-term risk for cardiovascularevents, patients undergoing an intervention fortheir vascular disease have an acutely increasedperi-interventional risk. This is well established forpatients undergoing vascular surgery. Althoughthe overall perioperative event rate has declinedover the past decades, the 30-day cardiovascularmortality still remains as high as 2–5%.5 Myocar-dial infarction accounts for up to 40% of postop-erative fatalities and can therefore be consideredas the major determinant of perioperative mor-tality associated with vascular surgery.
A number of scoring systems have beendeveloped over the years that aim to quantifythe risk of perioperative morbidity and mortality.The majority of studies tried to validate an indexfor risk of cardiac complications. The identifica-tion of risk factors associated with increased riskof mortality should help in decision-makingabout the need for additional preoperative cardiac testing. It may also influence the deci-sion about the type and timing of intervention.The ACC (American College of Cardiology)/AHA (American Heart Association) have pub-lished guidelines to provide a standardized
method of evaluating the cardiac risk before non-cardiac surgery and selecting patients at risk formore extensive testing.6 Otherwise, debate con-tinues regarding the extent and type of cardiacevaluation necessary before major vascular sur-gery procedures. It has been reported that coro-nary revascularization before elective vascularsurgery did not significantly alter the incidenceof perioperative myocardial infarction amongpatients with stable CHD.7 Furthermore, inten-sive non-invasive testing often triggers a clinicalcascade, exposing the patient to progressivelyriskier testing and intervention, and results inincreased costs and unnecessary delays. There-fore, screening of high-risk patients for cardiacischemia seems not essential for revasculari-zation, but rather to optimize the perioperativepatient management concerning optimal med-ical therapy.
Compared to the surgical literature concern-ing perioperative risk evaluation, correspondingstudies concerning the peri-interventional riskidentification in patients undergoing endovascu-lar procedures are rare.8–10 This is probably dueto the fact that until recently most endovascularinterventions were low-risk procedures. This hasonly changed during the last years by rapidlyincreasing use of endovascular treatment ofcarotid stenosis and aortic aneurysms.
In a recently published study by Hofmann et al,9
the authors did multivariable analysis to create arisk score identifying high-risk patients for carotidartery stenting. The primary endpoint reflectingperiprocedural complications encompassed minorand major stroke, non-fatal myocardial infarc-tion, and all-cause mortality within 30 days. Theiranalysis in 606 consecutive patients revealeddiabetes mellitus with inadequate glycemic con-trol (HbA1c > 7%), age � 80 years, ulceration ofthe carotid artery stenosis, and a contralateralstenosis > 50% as independent risk factors. Arisk score formed with these variables showed asuperior predictive value compared with singlerisk factors. The presence of two or more of theserisk factors identified patients with a risk of 11%for a periprocedural complication compared with2% in patients with a score of 0 or 1.
There is uniform consent that cardiovascularcomplications are more often encountered inpatients of older age. Furthermore, an increased
14 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter02.qxp 4/5/2007 2:38 PM Page 14

risk of hemorrhagic complications has beenreported in women.11
There are only few data considering the majormedical morbidity – not only cardiovascularevents – after endovascular interventions, e.g. inpatients with PAOD treated by angioplasty.Axisa et al12 reported the outcome after periph-eral angioplasty in 988 patients after 1377 inter-ventions between 1995 and 1998. Major medicalmorbidity (including bronchopneumonia, renalfailure, stroke, and myocardial infarction) com-plicated 33/1377 procedures (2.4%).
Recommendations concerning cardiovascular risk evaluation
It is generally assumed that endovascular treat-ment is associated with reduced risk of cardiovas-cular complications compared to open surgery.Furthermore, for most interventions there seemsto be a significant mortality advantage for endo-vascular as compared with traditional surgery.Therefore proponents of endovascular treatmentalways stress these most important advantages –especially from the patient’s point of view – oflow procedural morbidity and mortality. Thisreduced peri-interventional cardiovascular mor-bidity and mortality is also the main reason for thedramatic shift in revascularization managementover the last few years.
The extent of preinterventional risk evaluationis mostly guided by the severity of the interven-tion, e.g. patients with planned endovasculartreatment of aortic aneurysm should be evaluatedand managed with the same intensity as surgicalcandidates due to the potential necessity of con-version to open surgery. Otherwise, consideringthe potential risk – despite being (very) low formost endovascular procedures – of severe com-plications with the necessity of surgery, eachpatient with planned endovascular interventionshould undergo some basic evaluation.
Identification of potentially serious cardiac disorders
History, physical examination, and electrocar-diogram should focus on the identification ofpotentially serious cardiac disorders such as CHD(prior myocardial infarction and angina pectoris),
heart failure, and severe arrhythmias. Diabeticsshould be evaluated with special care due to theincreased prevalence of CHD and the possiblepresence of silent ischemia. Chest radiographyand echocardiography are helpful procedures inpatients with dyspnea on exertion and clinical sus-picion of heart failure or valvular disease. Non-invasive stress testing, myocardial scintigraphy,and coronary (CT) angiography are only recom-mended in patients with clinically severe CHD.
Identification of potentially serious cerebrovascular disorders
History and duplex sonography are sufficient fordiagnosis of (a)symptomatic carotid artery steno-sis. This information is not necessary for mostendovascular procedures except cerebrovascu-lar treatment itself. However, in patients sched-uled for aortic stent grafting, knowledge about thepresence of high-degree carotid stenosis is helpfulto avoid severe or prolonged hypotension duringthe intervention. Furthermore, such basic investi-gation of the carotid arteries is useful to help in thedecision for carotid stenting in case of eventualfurther rapid progression in the degree of stenosis.
NON-VASCULAR COMORBIDITY
Identification of the patient with pulmonary disease
History and clinical examination are sufficient to identify potential problems concerning thepatient’s pulmonary status. History should includethe following questions: smoking, asthma, dysp-nea and severity of breathlessness, and cough.Especially chronic severe cough may cause prob-lems during the intervention. Chest radiographyand a lung function test are recommended beforeendovascular stent grafting of aortic aneurysm andin all patients with severe pulmonary disorders.
Identification of the patient with renal disease
Chronic kidney disease is in general a major andserious risk factor for cardiovascular disease, andendstage renal disease is the major contributorto the high morbidity and mortality observed inthis population.
VASCULAR AND NON-VASCULAR COMORBIDITIES 15
CPVI_Chapter02.qxp 4/5/2007 2:38 PM Page 15

Determination of creatinine is sufficient forroutine preinterventional evaluation. However,although creatinine is a specific marker for renalfunction, it may be insensitive to mild and mod-erate degrees of renal impairment. As a result,patients with subclinical renal disease may remainundiagnosed because of a normal serum creati-nine value. Estimates of glomerular filtration rate(GFR) are the best overall indices of the level ofrenal function. The Cockroft–Gault equation isthe most commonly used equation to estimateGFR. It is important to reduce the amount ofcontrast agent as much as possible in patientswith impaired renal function. Furthermore,these patients may most benefit from the use ofalternative contrast agents and periproceduralrenal protection techniques.
Sufficient hydration – which is advised for allpatients undergoing endovascular procedures –is absolutely necessary in patients with risk fac-tors for chronic renal insufficiency to preventcontrast induced nephropathy.
Identification of further risk patients
Patients with diabetes
Correction of inadequate glycemic control inpatients with diabetes mellitus before electiveendovascular intervention is recommended.9
Besides the well-known risk of diabetes for severeatherosclerotic disease and renal impairment, thepatient with diabetes has to be carefully managedperi-interventionally with regard to the antidia-betic medication. Concomitant use of metforminmay lead to lactic acidosis due to metformin accu-mulation. Thus, metformin should be discontin-ued prior to use of contrast media. Blood glucoseshould be controlled in short intervals in insulin-dependent diabetics to avoid hyper- and hypo-glycemic episodes.
Patients with hypertension
The elevation of both systolic blood pressure (SBP)and diastolic blood pressure (DBP) is known to becontributory to cardiovascular mortality. Severalpopulation-based studies in hypertensive patientsand also in the general population have alsodemonstrated pulse pressure (PP = SBP – DBP)
as an independent risk predictor.13 Central arterystiffness seems the main explanation for this rela-tionship between a wide PP and cardiovascularevents.
Patients with hypertension should be regu-larly monitored during and after the interventionto avoid hypertensive episodes with increasedbleeding risk, especially at the puncture site. It isstrongly recommended to continue antihyperten-sive treatment also on the day of intervention. (Thespecial problems in patients with carotid stent-ing are discussed in the corresponding chapter.)
Patients with urologic disorders
Male patients with prostatic hypertrophy maydevelop urinary retention – favored by bed restand compression bandage – with the necessityof urinary catheterization, and further urinarytract infection requiring antibiotics. Successfuluse of closure devices can reduce this risk.
Patients with thyroid disease
Application of conventional contrast media mayrarely cause iodine-induced thyrotoxicosis. Thisrisk is very low in euthyroid patients, however itis increased in patients with latent hyperthy-roidism. In these patients, consultation with anendocrinologist is recommended to initiate thenecessary premedication with perchlorate and athyrostatic drug.
Patients with coagulation disorders
A history of spontaneous hemorrhagic compli-cations and antithrombotic therapy as well aslaboratory tests are necessary to identify patientswith potential bleeding complications. Since anti-platelet agents are routinely used in all endovas-cular procedures, a platelet count is obligatory.Furthermore, global coagulation tests as pro-thrombin time and activated partial thrombo-plastin time should be done routinely. In patientswith abnormal test results, consultation with ahematologist/hemostaseologist is recommended.
Since the common peri-interventional use of acombination of antiplatelet and anticoagulant(heparin) therapy significantly increases thebleeding risk, patients with potential bleeding
16 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter02.qxp 4/5/2007 2:38 PM Page 16

sources such as a gastric/duodenal ulcer shouldbe identified at least by history.
Heparin-induced thrombocytopenia is a life-threatening disorder that rarely followsexposure to unfractionated or (less commonly)low-molecular-weight heparin. Patients classi-cally present with a low platelet count or a rela-tive decrease of 50% or more from baseline.Severe thrombotic complications may developin the arterial and venous system. Patients witha history of heparin-induced thrombocytopeniashould not be treated with low-molecular-weightheparins, since these have high cross-reactivitywith circulating PF4–heparin antibodies. Threedirect thrombin inhibitors are currently avail-able for such patients: lepirudin, argatroban,and bivalirudin. Other therapies for heparin-induced thrombocytopenia are danaparoid andfondaparinux.
Patients with anemia
Anemia is a well-recognized factor that exacer-bates myocardial ischemia in the presence ofrestricted coronary reserve. Data regarding theprognostic importance of anemia in patientswho undergo peripheral interventions are lack-ing.14 After percutaneous coronary interventions,patients with anemia had significantly highermortality rates during hospitalization comparedwith those who did not.
Since anemia might be an indicator for a hithertounrecognized bleeding source with the risk ofaggravation by any antithrombotic treatment, thisparameter is important for identification of highrisk patients. The cause of anemia should be clar-ified and corrected before planned intervention.
Patients with allergy
History regarding a disposition to allergy,atopy, or drug hypersensitivity, and especially a known allergy to contrast agents, is very impor-tant. Iodinated contrast media can cause aller-gic reactions (itching, urticaria, angio-edema,and bronchospasm or arterial hypotension and shock) within minutes after administration. Life-threatening anaphylactic reactions due to iodi-nated contrast media are very rare. Despite thefact that the increased use of non-ionic iodinated
contrast media has been associated with a decreasein the incidenceof mild to moderate, and possiblysevere, reactions, prophylacticdrug regimens thataim to decrease the incidence of reactions (pre-medication) are still widely used in clinical prac-tice despite a lack of data supporting the use ofsuch premedication – steroids, antihistamines –in patients with a history of allergic reactions.Recently, Tramèr et al15 published a systematicreview of trials testing the efficacy of antihista-mines and corticosteroids. The authors concludethat its usefulness is doubtful because of thelarge numbers of patients who would have to betreated to prevent one reaction.
IS RISK REDUCTION POSSIBLE BY DRUG APPLICATION?
The observation that manipulating and targetingcertain parameters in selected patients can influ-ence the general cardiovascular risk has beenreported in numerous studies. Recently it waspostulated that there is a need for a shift inemphasis from risk stratification by non-invasivetesting to risk modification by the application ofmedical interventions which prevent periopera-tive ischemia.16 Concerning the vascular patient,the use of statins and �-blockers in particularmay reduce severe complications. �-Blockers canrestore the supply/demand mismatch, by thereduction of myocardial oxygen use by decreas-ing sympathetic tone and myocardial contractil-ity. There is some evidence suggesting that�-adrenergic receptor antagonists reduce car-diovascular morbidity and mortality in high-risk patients undergoing non-cardiac surgery.17
The evidence to date is consistent and suggeststhat �-blockers reduce perioperative cardiacevents in high-risk patients. There is no evidencethat �-blockers are also helpful in low to moder-ate risk patients. As clinicians we need to bemindful of �-blocker withdrawal, and makeevery effort to prevent it.
The prehospital or preprocedural use of statinshas been found to be associated with reductionsin the incidence of in-hospital death in patientswith acute coronary syndromes, of periproce-dural myocardial infarction after percutaneouscoronary intervention, and of perioperative mor-tality in patients undergoing major non-cardiac
VASCULAR AND NON-VASCULAR COMORBIDITIES 17
CPVI_Chapter02.qxp 4/5/2007 2:38 PM Page 17

vascular surgery.18 However, there is a completelack of studies and knowledge concerning peri-interventional application of such drugs inpatients undergoing peripheral endovascularprocedures. Statins may prevent plaque insta-bility and thrombosis due to their pleiotropiceffects, such as improvement of endothelial func-tion, reduction of inflammation, and stabilizationof atherosclerotic plaques. �-Blockers can restorethe supply/demand mismatch by the reductionof myocardial oxygen use by decreasing sympa-thetic tone and myocardial contractility.
Peri-interventional pain control is helpful toavoid problems with restlessness of the patient.Furthermore, several studies suggest that effec-tive pain management leads to a reduction in cat-echolamine increase and in hypercoagulability.
SUMMARY
Patients at increased risk for peri-interventionalevents mostly can be identified on the basis ofsimple clinical and laboratory markers. It has tobe stressed that a good history and physicalexam-ination by an experienced physician are the basicmeasures to identify any risk patient. This enableseffective risk evaluation despite keeping it simpleand cheap.
Table 2.1 summarizes the recommended mini-mal program before any endovascular interven-tion. Further tests depend on the results of theseexaminations and on the risk of the interventionitself.
REFERENCES
1. de Groot V, Beckerman H, Lankhorst G et al. How tomeasure comorbidity: a critical review of availablemethods. J Clin Epidemiol 2003; 56: 221–9.
2. Humphries KH, Rankin JM, Carere RG et al. Co-morbidity data in outcomes research. Are clinical data derived from administrative databases a reliable alternative to chart review? J Clin Epidemiol 2000; 53: 343–9.
3. Golomb BA, Dang TT, Criqui MH. Peripheral arterialdisease: morbidity and mortality implications. Circula-tion 2006; 114: 688–99.
4. Hertzer NR, Beven EG, Young JR et al. Coronary arterydisease in peripheral vascular patients: a classificationof 1000 coronary angiograms and results of surgicalmanagement. Ann Surg 1984; 199: 223–33.
5. Nowygrod R, Egorova N, Greco G et al. Trends, com-plications, and mortality in peripheral vascular surgery.J Vasc Surg 2006; 43: 205–16.
6. Eagle KA, Berger PB, Calkins H et al. ACC/AHAguideline update for perioperative cardiovascular eval-uation for noncardiac surgery – executive summary. J Am Coll Cardiol 2002; 39: 542–53.
7. McFalls EO, Ward HB, Moritz TE et al. Coronary-arteryrevascularization before elective major vascular sur-gery. N Engl J Med 2004; 351: 2795–804.
8. Danetz JS, McLafferty RB, Schmittling ZC et al.Predictors of complications after a prospective evalua-tion of diagnostic and therapeutic endovascular proce-dures. J Vasc Surg 2004; 40: 1142–8.
9. Hofmann R, Niessner A, Kypta A et al. Risk score for peri-interventional complications of carotid arterystenting. Stroke 2006; 37: 2557–61.
10. Groschel K, Ernemann U, Riecker A et al. Incidence andrisk factors for medical complications after carotidartery stenting. J Vasc Surg 2005; 42: 1101–6.
11. Kawamura A, Piemonte TC, Nesto RW et al. Impact ofgender on in-hospital outcomes following contemporarypercutaneous intervention for peripheral arterial disease. J Invas Cardiol 2005; 17(8): 433–6.
12. Axisa B, Fishwick G, Bolia A et al. Complications fol-lowing peripheral angioplasty. Ann R Coll Surg Engl2002; 84: 39–42.
13. Aboyans V, Criqui MH. Can we improve cardiovascularrisk prediction beyond risk equations in the physician’soffice? J Clin Epidemiol 2006; 59: 547–58.
18 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 2.1 Minimal program for risk evaluationbefore any endovascular intervention
History and clinical examination:• cardiac disorders: MI, angina, arrhythmia, heart
failure• cerebrovascular disorders: TIA, stroke• pulmonary disorders: smoking, asthma,
dyspnea, cough• further history/(clinical examination) concerning
– diabetes, hypertension, hemorrhagic andthrombotic complications, gastroduodenalulcer, allergy
– medication: antiplatelet, anticoagulant,antihypertensive, antidiabetic
Laboratory tests:• blood glucose, hemoglobin, platelets, prothrombin
time, creatinine, sodium, potassium, C-reactiveprotein, TSH (thyroide-stimulating hormone)
Electrocardiogram
CPVI_Chapter02.qxp 4/5/2007 2:38 PM Page 18

14. Nikolsky E, Mehran R, Aymong E, et al. Impact of ane-mia on outcomes of patients undergoing percutaneouscoronary interventions. Am J Cardiol 2004; 94: 1023–27.
15. Tramèr MR, von Elm E, Loubeyre P et al. Pharma-cological prevention of serious anaphylactic reactionsdue to iodinated contrast media: systematic review.BMJ 2006; 333: 675.
16. Karthikeyan G, Bhargava B. Managing patients under-going non-cardiac surgery: need to shift emphasis fromrisk stratification to risk modification. Heart 2006; 92:17–20.
17. Fleisher LA, Beckman JA, Brown KA et al. ACC/AHA2006 Guideline Update on Perioperative CardiovascularEvaluation for Noncardiac Surgery: Focused Update onPerioperative Beta-Blocker Therapy. J Am Coll Cardiol2006; 47: 2343–55.
18. Paraskevas KI, Liapis CD, Hamilton G et al. Can statinsreduce perioperative morbidity and mortality inpatients undergoing non-cardiac vascular surgery? EurJ Vasc Endovasc Surg 2006; 32: 286–93.
VASCULAR AND NON-VASCULAR COMORBIDITIES 19
CPVI_Chapter02.qxp 4/5/2007 2:38 PM Page 19

CPVI_Chapter02.qxp 4/5/2007 2:38 PM Page 20

INTRODUCTION
The frequency and impact of complicationsdepend on various factors including the patient’smorbidity and risk profile, access site morphol-ogy, and characteristics of the access route andtarget vessel segment. These factors define low-risk, intermediate-risk, and high-risk patients/interventions, respectively, and define patientswho are not suitable for an endovascularapproach. The first step to safely perform an inter-vention therefore is to perform a thorough prein-tervention non-invasive work-up to classify thepatient’s risk and to develop an interventionalstrategy. Besides patient-associated factors, theperformance of the interventionist is the secondmajor determinant to influence the risk for com-plications. The third important factor is imagingduring and after the intervention to recognizepotential problems early. Finally, standardizedpostintervention care and surveillance help toimprove patients’ safety.
PRE-, PERI-, AND POSTINTERVENTION CARE
Before discussing bail-out material whichshould be available in the cath lab, some basicprinciples for planning of the intervention arelisted; these are in accordance with recommen-dations international societies.1–12
Preprocedure
• A written medical history should be availableincluding current symptoms, major comor-bidities and risk factors, list of medication,history of allergic reactions, and details of pre-vious vascular interventions and operations.
• Results of physical examination have to beavailable including heart and lung examina-tions and pulse status.
• Laboratory results including complete bloodcount, coagulation, serum creatinine, elec-trolytes, and thyroid hormone level have tobe done before the intervention.
• Evaluation of the access site has to be doneprior to bringing the patient to the cath lab.In patients with a regular pulse at the punc-ture site and without vascular bruits usuallyno further imaging is mandatory. Duplexsonography of the puncture site should bedone in any patient with suspected pathologyand is also helpful to precisely locate theartery in special indications (e.g. before punc-turing the popliteal artery to avoid formationof an arterio-venous fistula (AV) fistula).
• Complete imaging of the target vessel segmentand the run-off is required, although nowadaysnon-invasive methods like computed tomog-raphy (CT) angiography or magnetic reso-nance (MR) angiography seem adequate to
3
Being prepared – standards for patientcare and adequate bail-out equipmentMartin Schillinger
Introduction • Pre-, peri-, and postintervention care • Bail-out equipment
CPVI_Chapter03.qxp 4/5/2007 2:38 PM Page 21

plan the procedure. Diagnostic conventionalangiography can be omitted if these alterna-tive imaging methods are available withexcellent quality.
• Based on the findings of non-invasive imag-ing, the interventionist should define a treat-ment strategy before starting the intervention.This includes preparation of adequate mate-rial to access the target vessel segment and aselection of materials which likely will be nec-essary to treat the lesion. The preparation ofthese materials helps to keep the time of theintervention as short as possible.
• The interventionist has to be aware of thepotential complications – knowing about whatmay happen helps to avoid it.
Periprocedure
• Interventions should be completely documented.• All patients should have continuous cardiac
monitoring and intermittent blood pressure mon-itoring; for some elective and all emergencyinterventions continuous invasive blood pres-sure measurements should be considered.
• All patients need an intravenous access foradministration of fluids or medication. Thisaccess should be checked immediately beforebeginning the procedure.
• If the patient is sedated, pulse oximetry isrequired to monitor oxygen saturation.
• After completion of the intervention completefinal angiograms of the target vessel segment andrun-off vessels have to be done to identifypotential complications early. Particularly incases of new or increasing patients’ com-plaints, interventionists have to search forproblems.
• The interventionist has to know the availablebail-out equipment and should be trained inusing it.
• Finally, some complications cannot beresolved by endovascular solutions, there-fore there is a definite need for cooperationwith vascular surgery and availability foremergency operations.
Postprocedure
• All patients should be observed at bed rest inthe initial postprocedure period. The time for
bed rest depends on the size and locationof the puncture hole. Before ambulation, thepuncture hole has to be checked by a trainednurse or physician.
• The first ambulation should be done undersurveillance.
• Surveillance at an intensive or coronary careunit is necessary only after emergency inter-ventions in critical locations or in patients aftersevere complications.
• After the intervention trained professionalsshould regularly examine the patient for signsof malperfusion of the treated organ system. Theintensity of this examination will depend onthe treated vessel segment: e.g. pulse palpationshould be done after intervention of arteriesof the extremities, and neurologic evaluationhas to be done after carotid stenting.
• Renal function should be checked at least once24 hours after the procedure. In patients withrisk factors for renal dysfunction, prolongedmonitoring of serum creatinine is necessaryto identify patients with late renal failure.
• Finally, the interventionist who has per-formed the procedure should be available inthe early postintervention phase and shouldexamine the patient before discharge.
BAIL-OUT EQUIPMENT
The following section gives an overview andcomments on bail-out equipment used in thespecific chapters of the book.
Emergency drugs
Interventionists and nurses have to be familiarwith the following emergency medications. Thesedrugs should be available in every cath lab, irre-spective of which vascular interventions are per-formed at the facility.
Vasopressors like epinephrine, vasopressin, ordopamine are needed in hemodynamically unsta-ble patients. This may be due to various causeslike severe bleeding and hemorrhagic shock,allergic shock in response to contrast media,malign arrhythmias, or myocardial infarction, orin a worst case scenario during cardiopulmo-nary resuscitation. Epinephrine, of course, hasto be available in the emergency crash cart.
22 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter03.qxp 4/5/2007 2:38 PM Page 22

The usual dosage of epinephrine is a bolusdosage of 1 mg during resuscitation or perfusiondosages of 0.1 to 1.0 �g/kg/min for treatment ofhemodynamic shock. Vasopressin is given duringcardiopulmonary resuscitation as a single dose by40 IU in patients with asystole. Dopamine is usu-ally administered in dosages of 3 to 12 �g/kg/minin patients with hemodyamic deterioration.
Anti-arrhythmic drugs which should be avail-able mainly include atropine, particularly whencarotid stenting is performed in the cath lab facil-ity. Atropine increases heart rate, but per se doesnot increase blood pressure. The usual dosagesof atropine are in steps of 0.5 mg; completevagolysis is achieved by 3 mg, more than 3 mgatropine therefore should not be administered.Other anti-arrhythmic drugs such as amiodaroneshould be available in the emergency crash cart.Availability of fluids for intravenous volumeexpansion is mandatory. These include crystalloidfluids like physiologic sodium chloride, 5% glucose, and 20% or 33% glucose infusions, aswell as colloid fluids for extra-volume expansion.Fluids are needed to handle most forms ofhypotension and shock; glucose is needed totreat hypoglycemia. Specific medications to treatallergic reactions include cortisone and antihista-minic dugs, besides the above-mentioned epi-nephrine for treatment of allergic shock.
Anti-coagulant medication includes heparin,bivalirudin, glycoprotein (Gp) IIbIIIa antago-nists, and lytics. Usual dosages of heparin arebetween 2000 and 10 000 IU; in complex inter-ventions and high-risk patients heparin shouldbe monitored by activated clotting time (ACT)measurements (keeping the ACT around 250seconds). Bivalirudin is a relatively novel directthrombin inhibitor which is administered in afixed dose and infusion by kg body weight.Similarly, Gp IIbIIIa inhibitors are given adjustedto the patient’s body weight. The dosage of lyt-ics depends on the substance and indication.The usual dosage for acute lysis with recom-bined tissue plasminogen activator (rtPA) is abolus of 6 mg and further steps of 2 mg until theclot has dissolved.
Procoagulant substances include protamine,which antagonizes heparin in a more or less 1:1ratio, and prothrombin complex concentrate,which substitutes all factors of the prothombin
complex in patients with acute bleeding compli-cations and severe coagulation disorders (eitherdue to medications like warfarin or due to bleed-ing diasthesis).
Vasodilators like nitroglycerin, papaverin, ilo-medin, or calcium channel blockers are useful tohandle or prevent vessel spasms. In particular,for radial or brachial access or during carotidstenting vasodilators can be essential. The usualdosage for nitroglycerin is in steps of 0.1 mg.Anti-epileptic agents should be available, particu-larly when cerebrovascular interventions areperformed in the cath lab facility.
In summary, the list of medications includes:
• vasopressors: epinephrine, vasopressin,dopamine
• anti-arrhythmics: atropine• fluids: crystalloid and colloid infusions,
including glucose infusions• anti-allergic drugs: cortisone and antihista-
minic drugs• anticoagulant medication: heparin, Gp
IIbIIIa inhibitors (abciximab), lytics• procoagulant substances: protamine, pro-
thrombin complex concentrate• vasodilators: nitroglycerin, calcium channel
blockers, ilomedin• anti-epileptic agents: lorazepam, phospheny-
toin.
Various emergency tools
A tracheostomy set should be available for carotidstenting procedures. In rare cases with perfora-tions of external carotid arteries, severe bleedingmay cause compression of the larynx and cancause asphyxia.
A standard emergency crash cart including defib-rillator, intubation set, and drugs for cardiopul-monary resuscitation has to be readily available.
Tourniquets are helpful to handle peripheralbleeding complications. Large blood pressurecuffs can be used for the extremities. These areparticularly effective in combination with balloonblockage inside the vessel at the site of rupture.Many bleedings can be stopped by this combi-nation of internal and external compression, par-ticularly when the use of coils or (covered) stentsneeds to be avoided.
BEING PREPARED 23
CPVI_Chapter03.qxp 4/5/2007 2:38 PM Page 23

In summary, the list of various emergencytools includes:
• tracheostomy set• emergency crash cart• tourniquets, large blood pressure cuffs.
Wires and catheter material
The choice of wires will depend on operatorpreference. Wires in 0.014, 0.018, and 0.035 inchshort (180 cm) and long length (260 to 300 cm) should be available. Extra stiff wires likeAmplatzTM extra stiff, LunderquistTM extra stiff,or Supra-coreTM wires should be available for emer-gency purposes to guarantee sufficient back-upin critical situations. In particular, stent grafts areusually better deployed via an extra stiff wire.
Similarly, there is a wide variety of cathetersand, for most situations, the skill of the interven-tionist will be more important than the curve ofthe catheter. Standard catheter forms include pig-tail, multi-purpose, cobra, side-winder, straight,head-hunter, Sos-omni, IM, or Judkins right (JR)coronary. Some specific catheters suggested by theauthors of this book are the Quick-Cross® Catheter(The Spectranetics Corp, Colorado Springs, CO),the Soft-Vu® Berenstein (AngioDynamics, Queens-bury, NY), or the Impulse® IM AngiographicCatheter (Boston Scientific Corp, Natick, MA).Furthermore, for emergency intracranial interven-tions during carotid stenting 0.014- to 0.021-inchmicrocatheters and wires should be available whena skilled interventionist is adequately trained toperform intracranial bail-out interventions.
Summary of wires and catheters:
• 0.035-inch glide wire• 0.035-inch extra back-up wire• 0.018-inch wire (e.g. Boston Scientific V18
Control Wire)• 0.014-inch wires including floppy intracra-
nial wires• standard diagnostic curves 4 to 6 French:
pigtail, MP, side-winder, IM, JR, cobra, etc.• 0.014- and 0.021-inch microcatheters.
Sheaths
The choice of sheath available will widely dependon the kind of procedures which are planned in
the cath lab facility. As long as aortic interven-tions are not performed, sheath sizes of up to 12French in short and long length will be sufficient.These include stable and long cross-over sheathswhich are available from various distributors.Importantly, the size of the available sheaths hasto be coordinated with the brand of coveredstents which are on the shelf. Most of these stentgrafts will need large sheath diameters. If aorticinterventions are performed, even larger sheathsare needed to accommodate the devices. Theauthors of the book recommend 16–24 FrenchCheck-Flo introducers (Cook, Bloomington, IN).
Summary of sheaths:
• 4 to 12 French when aortic interventions arenot performed; maximum size has to be coor-dinated with stent grafts for bail-out situa-tions. Length of the sheath: 6, 7, and 8 Frenchshould be available in up to 90 cm for access tothe supraaortic vessels or transbrachial accessto the lower limbs; larger sheaths should beavailable in up to 45 cm to enable cross-overaccess.
• 16 to 24 French when aortic interventionsare planned.
Thrombolysis catheters
A variety of thrombolysis catheters is available andnone has been proved to be superior. In this bookthe Uni*fuse® Infusion Catheter (Angiodynamics),and EKOS LysUS® Infusion System (EKOS Corp,Bothell, WA) for ultrasound-enhanced thrombolysisare described. The authors also have good expe-rience with Mewissen thrombolysis cathetersand McNamara thrombolysis catheters. Impor-tantly, the length of the thrombolysis catheterhas to be sufficient to enable cross-over access.Various length in perfusion lumen can be helpful.
Summary of thrombolysis catheters:
• thrombolysis catheters in up to 8 Frenchwith a working length of 90 to 100 cm.
Rheolythic thrombectomy catheters
Rheolytic thrombectomy catheters are not a manda-tory tool for the cath lab, but can be helpful insome situations. In this book the AngioJet®
Thrombectomy System (Possis Medical, Inc,Minneapolis, MN) is described.
24 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter03.qxp 4/5/2007 2:38 PM Page 24

Summary of rheolythic thrombolysis catheters:
• none mandatory.
Aspiration thrombectomy catheters
In contrast to the above mentioned rheolythicthrombolysis catheters, 0.014 inch aspirationcatheters are mandatory. For small arteries theDiver CETM Clot Extraction Catheter (ev3, Inc,Plymouth, MN) or the Pronto aspiration catheteris useful. For peripheral applications, flexible guid-ing catheters with atraumatic tips like the Cordisbright-tip 6 to 9 French guide catheters withremovable hemostatic valves are very effective.
Summary of aspiration catheters:
• 0.014 aspiration catheter for small vesselapplication
• 6 to 9 French guiding catheter with flexibletip and 90 to 100 cm working length withremovable hemostatic valve for large vesselapplications.
Embolization material
Embolization material can be crucial to handleperforations or pseudoaneurysms. There is avariety of coils available, either detachable coilsor mechanistically more easily pushable coils.Besides coils, liquid embolic agents like NBCA orOnyx can be helpful in certain situations. In theauthor’s opinion pushable coils will be sufficientfor almost all peripheral applications, except formicrocoil in supra-aortic indications.
Summary of embolization material:
• coils: detachable, pushable, microcoils• liquid embolization material.
Retrieval devices
These devices are essential to retrieve particles,thrombi, or catheter material. Usually snares indifferent sizes should be on the shelf. Addition-ally, special retrieval devices like the Merci® retrieverare described in this book.
Summary of retrieval devices:
• snares in different sizes like: EN Snare®
Intravascular Retrieval Devices (InterV,Gainesville, FL), 15 mm and 25 mm AmplatzGoose Neck Snare® (ev3), 12–20 mm and
18–30 mm EN snare® (interv Medical DeviceTechnologies, Inc)
• Expro® Elite (CoMed Medical Specialties,Littleton, CO)
• Merci® retriever.
Balloons
Besides the usual angioplasty balloons, whichcan also be used for vessel sealing, large diameterangioplasty balloons have to be available to blockthe aorta, such as the 12–26 mm AtlasTM PTADilation catheter (Bard Peripheral, Tempe, AZ).Furthermore, special occlusion balloons like the20–40 mm Equalizer® (Boston Scientific) are avail-able, which are less traumatic to the vascular walland should not induce vessel injury and resteno-sis. Another useful tool is the cutting balloon.Although this device will hardly ever be used toresolve a complication, it can help to avoid com-plications by adequate plaque preparation andtreatment of resistant lesions.
Summary of balloons:
• regular angioplasty balloons sized from2 mm with low-profile OTW design to 10 mm
• large diameter balloon for blockage of theaorta: 10 to 26 mm
• optional cutting balloon and atraumaticocclusion balloons.
Stents
Stents became an important tool for the treatmentof peripheral artery disease and the use of stentshas resolved many frequent minor complicationslike vessel dissections or AV fistulas. Stents, how-ever, also play an essential role in the handlingof complications. Covered stents and non-coveredstents can be used to seal rupture sites, pseudo-aneurysms, and AV fistulas. Balloon-expandingand self-expanding formats in sizes of 2 to 12 mmare needed. Covered stents should be availablefrom 6 to 14 mm. In the book the following cov-ered stents are discussed: iCastTM Covered Stent(Atrium Medical Corp, Hudson, NH), VIABAHN®
Endoprosthesis Stent-Graft (WL Gore & Associ-ates, Inc, Flagstaff, AZ), Wallgraft® (Boston Scien-tific), and Fluency® (CR Bard, Inc, Murray Hill,NJ). Stents appropriately sized for the intracranialcirculation like Neuroform or MiniVision should
BEING PREPARED 25
CPVI_Chapter03.qxp 4/5/2007 2:38 PM Page 25

be considered as bail-out material for supra-aorticinterventions. Special stents exist for crossing thevertebral artery or left internal marmarianartery (LIMA) like the Bridge® Assurant Stent(Medtronic, Inc, Minneapolis, MN), a modulardesign less likely to jail these vessels. Finally, aor-tic stent graft extensions are needed when aortic dis-ease is treated, like the 23, 26, 28.5 mm aorticextender (Excluder, WL Gore & Associates, Inc)or the 22–32 mm main body extension (Zenith,Cook, Bloomington, IN).
Summary of stents:
• self-expanding bare stents 4 to 12 mm• balloon-expanding bare stents 2 to 12 mm• self-expanding or balloon-expanding cov-
ered stents 6 to 14 mm• intracranial stents, stents to cover the verte-
bral artery or LIMA• aortic stent graft extensions.
Protection devices
Protection devices are most frequently used incarotid stenting, mainly to avoid complicationsrather than for actual treatment of complica-tions. Besides a wide variety of filter devices anddistal balloon occlusion systems, proximal balloonocclusion systems like the PAES® Parodi Anti-Embolic System (WL Gore & Associates, Inc) orthe MoMa® anti-embolic device (Invatec, Italy)should be available in the cath lab to manage raresituations of thrombotic or embolic occlusion ofthe carotid arteries. Besides their role in carotidstenting, filter systems are also used duringrenal stenting or high-risk peripheral interven-tions. Current devices, however, are not ideallydesigned for these applications. Furthermore, ret-rievable filters for protection during thrombolysis invenous applications exist like the Recovery G2TM
(Bard Peripheral, Tempe, AZ), the Gunther TulipTM
(Cook), or Optease® (Cordis, Miami Lakes, FL).Summary of protection devices:
• filter systems• proximal balloon occlusion systems• venous filters.
REFERENCES
1. Spies JB, Bakal CW, Burke DR et al. Angioplasty standard of practice. J Vasc Interv Radiol 2003; 14:S219–21.
2. Standards of Practice Committee of the Society ofCardiovascular and Interventional Radiology. Guidelinefor percutaneous transluminal angioplasty. Radiology1990; 177: 619–30.
3. Singh H, Cardella JF, Cole PE et al. Quality improve-ment guideline for diagnostic arteriography. J VascInterv Radiol 2003; 14: S283–8.
4. Standards of Practice Committee of the Society ofCardiovascular and Interventional Radiology. Standardsfor interventional radiology. J Vasc Interv Radiol 1991; 2:59–65.
5. American College of Cardiology/American HeartAssociation Ad Hoc Task Force in Cardiac Catheteriza-tion. ACC/AHA guidelines for cardiac catheterizationand cardiac catheterization laboratories. Circulation 1991;84: 2213–47.
6. Rutherford RB. Standards for evaluating results ofinterventional therapy for peripheral artery disease.Circulation 1991; 83: 6–11.
7. Pentecost MJ, Criqui MH, Dorros G et al. Guidelines forperipheral percutaneous transluminal angioplasty ofthe abdominal aorta and lower extremity vessels. J VascInterv Radiol 2003; 14: S495–515.
8. Martin LG, Rundback JH, Sacks D et al. Qualityimprovement guidelines for angiography, angioplasty,and stent placement in the diagnosis and treatment ofrenal artery stenosis in adults. J Vasc Interv Radiol2003; 14: S297–310.
9. Kajan DK, Patel NH, Valji K et al. Quality improve-ment guideline for percutaneous management ofacute limb ischemia. J Vasc Interv Radiol 2005; 16:585–95.
10. Connors JJ, Sacks D, Becker GJ et al. Carotid arteryangioplasty and stent placement: quality improvementguidelines to ensure stroke risk reduction. J Vasc IntervRadiol 2003; 14: S317–19.
11. Society of Interventional Radiology Standards ofPractice Committee. Guideline for percutaneous trans-luminal angioplasty. J Vasc Interv Radiol 2003; 14:S209–17.
12. Hirsch AT, Haskal ZJ, Hertzer NR et al. ACC/AHAguidelines for the management of patients with periph-eral arterial disease (lower extremity, renal, mesenteric,and abdominal aorta). J Vasc Interv Radiol 2006; 17:1383–98.
26 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter03.qxp 4/5/2007 2:38 PM Page 26

This chapter focuses on radiocontrast mediainduced acute renal failure (CM-ARF) and onlybriefly discusses other complications such asallergies and hyperthyroidism at the end.
DEFINITION OF CONTRAST MEDIA INDUCED ARF
Comparability of epidemiologic data as well aspreventive and therapeutic strategies amongstudies depends on the uniform definition of theoutcome parameter. In the case of CM-ARF how-ever, this basal requirement is not met. The defi-nition of CM-ARF is not uniform and at least fourdifferent classifications exist that are commonlyused. Some authors refer to ARF as doubling ofbaseline creatinine, others as increase of baselinevalue by more than 25% or 50%, or as absoluteincrease of creatinine by more than 0.5 mg/dl ormore than 1 mg/dl (25%,1 50%,2 >0.53). Definitionof ARF as the clinically important hard outcomeof dialysis dependency is very rare.
CLINICAL IMPORTANCE OF CONTRASTMEDIA INDUCED ARF
The clinical impact of CM-ARF again dependson its definition and the indication for the con-trast media application (comorbidities). It isintuitive that mild reversible elevations of aninitial normal serum creatinine are of no majorconcern. However, more severe impairments of
renal function are associated with profoundchanges in the risk of developing other compli-cations and death.3 Marenzi and colleagues foundthat an increase in serum creatinine within thefirst 3 days after percutaneous intervention by0.5 mg/dl or more in patients with acute myocar-dial infarction was associated with prolongedhospitalization and a significantly higher mor-tality. Mortality is even exaggerated if patientswith underlying chronic kidney disease developCM-ARF after percutaneous coronary interven-tion.4 Dangas and coworkers used a similar studysetting and definition of CM-ARF as Marenziand showed that the effect of CM-ARF on overallmortality in patients without chronic renal fail-ure (CRF) is roughly the same as the mortality ofpatients with CRF who did not develop CM-ARF. In both groups, CRF without CM-ARF andCM-ARF without prior CRF, between 5 and 10%of patients died within one year. The develop-ment of CM-ARF in patients with CRF, how-ever, was associated with a 1-year mortality ofalmost 25% (Figure 4a.1).
Now this high mortality is clearly explainableby the underlying comorbidity of CRF andtightly associated problems such as cardiovas-cular disease and frequent infection. To addressthe issues of the impact of comorbidities on the high mortality in patients with CM-ARF,Levy and coworkers performed a retrospectivecohort study of 16 248 patients.1 One hundred
4a
Contrast media associated complicationsRainer Oberbauer
Definition of contrast media induced ARF • Clinical importance of contrast media induced ARF •Frequency of contrast media induced ARF • Risk factors of contrast media nephropathy – identifying high-risk patients • Prevention of contrast media induced ARF • Other causes of ARF after contrastapplication • Treatment of contrast media induced ARF • Complications of contrast media other thanARF • Summary • Acknowledgments
CPVI_Chapter04a.qxp 4/5/2007 2:38 PM Page 27

and eighty-three subjects developed CM-ARFdefined as an increase in baseline serum creati-nine of at least 25% and above 2 mg/dl. Evenafter adjustment for the more comorbidities in the CM-ARF group, the OR of dying was 5 times higher in these subjects (Figure 4a.2). Asin other similar studies investigating the associ-ation of postoperative ARF and mortality, deathfrom renal causes was rare.5 The conclusion ofthese studies is that renal failure appears to modifythe propensity for other non-renal complicationswhich cannot be treated by hemofilatration ordialysis. Examples of these conditions are systemicinflammation, catabolism, hemorrhagic diathesis,gastrointestinal ulcerations, hypercirculation,cardiomyopathy, and pulmonary edema.
FREQUENCY OF CONTRAST MEDIA INDUCED ARF
The true rate of CM-ARF in clinical routine isprobably underestimated given the fact that manycontrast media utilizing procedures are per-formed on an outpatient basis without sequential
creatinine measurement. Furthermore, elderlypatients in particular may exhibit normal serumcreatinine values despite having reduced glomeru-lar filtration rates. On the other hand, misclassi-fication of CM-ARF may occur in cases whereother factors such as cholesterol emboli, infections,
28 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Number at riskTime in months
CKD/CIN
CKD/CIN
p < 0.0001
CKD/No CIN
CKD/No CIN
No CKD/CIN
No CKD/CIN
No CKD/No CIN
No CKD/No CIN
384
1641637
4906
313
1599608
4858
305
1560595
4805
289
1539591
4788
251
1378542
4375
25
20
15
10
Cum
ulat
ive
perc
enta
ge o
f dea
th
5
0
0 3 6 9 12
Figure 4a.1 One-year survival after percutaneous coronary intervention in patients with or without chronic kidney disease(CKD) and with or without contrast induced nephropathy (CIN). Reprinted with permission from Dangas et al 2005.4
0
10
20
30
40
50
60
70
2 6 10 14
ICU score
Mor
talit
y (%
)
No ARF
ARF
FFiigguurree 44aa..22 Acute renal failure is an independent predictorof mortality. Figure modified with permission from Levy et al 1996.1
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 28

altered hemodynamics, or nephrotoxic comedica-tion are actually responsible for ARF.
In clinical studies the incidence rate variesconsiderably depending on patient selection, thecontrast medium used, and the definition of CM-ARF. Patients without major comorbiditiesdevelop CM-ARF defined as a rise in baselinecreatinine of more than 50% in the low singledigit percentage range.2 Even patients withpre-existing CRF and diabetes mellitus exhibitCM-ARF in only 9% of cases.
If less stringent criteria of CM-ARF areapplied in high-risk patients, the incidence ofCM-ARF ranges from less than 5% in iodixanoltrials to 50% and above in trials of iopentol andioxilan (Figure 4a.3).6 Even trials where the samecontrast medium was used show considerable het-erogeneity of incidence. Five trials using iohexol,for example, reported CM-ARF rates between10 and 40%. These wide ranges show impres-sively that, as mentioned above, the frequency
of CM-ARF is highly dependent on the definitionof variables.
RISK FACTORS OF CONTRAST MEDIANEPHROPATHY – IDENTIFYING HIGH-RISK PATIENTS
Similiar to the ARF developing in ICU patients,CM-ARF is rarely caused by the single insult of contrast media use alone. In the majority ofpatients experiencing CM-ARF, chronic condi-tions of the cardiovascular system as well asother risk factors such as diabetes mellitus, mul-tiple myeloma, CRF, infections, or nephrotoxiccomedications are present.
The main single risk factor for CM-ARF is prob-ably dehydration, although this statement is onlyindirectly supported by published data. Severalstudies have shown that intravenous volumeexpansion prior to the application of contrastmedium reduces the rate of CM-ARF. This has
CONTRAST NEPHROPATHY 29
250
27 79 48 65 64 54 39 106
155
98 61 47 39 29 45 91 50 56
40
p < 0.001
p < 0.001
Iohexol844 mOsm/kg
Iodixanol290 mOsm/kg
Iopamidol796 mOsm/kg
NS
Ioxilan
Iopromide
Iomeprol
Iopentol
Inci
denc
e of
CIN
(%
)
35
30
25
20
15
10
5
0
Figure 4a.3 Incidence of contrast media induced nephropathy (CIN) in patients with chronic renal insufficiency receivingnon-ionic contrast agents in various prospective studies. Numbers in bars refer to the references in the paper bySolomon.6 Reprinted with permission.
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 29

been shown for normal vs half normal saline, andsodium bicarbonate vs normal saline.7–9 However,these studies are limited due to a huge type twoerror.
Besides dehydration the amount rather thanthe type of contrast medium is predictive for thedevelopment of CM-ARF, because nowadaysonly low- or iso-osmolar non-ionic contrast mediaare used. A recent systematic review by Solomonconcluded that factors other than contrast mediumosmolarity such as patient’s age and the appliedvolume are more important risk factors for CM-ARF.6 This study as well as others showed, how-ever, that iopamidol and iodixanol are probablyassociated with less risk for CM-ARF thaniohexol.10 Alternatively, if patients exhibit a contraindication to iodinated contrast media,gadolinium chelates may be used instead to per-form angiography.11
It is generally well accepted that patients with diabetes mellitus have a higher risk for the development of CM-ARF. However, as withmany other risk factors, diabetes is not a dichoto-mous state but rather represents a continuum of a disease ranging from asymptomatic abnormalregulation of blood glucose to the most severeend organ damage including macro- and microan-giopathy. This may explain why some authorsidentified diabetes mellitus as a major risk factorfor the development of CM-ARF whereas othersdid not find a significant association with CM-ARF in multivariate analyses.6,12 In the multivari-ate logistic regression model designed by Mehranet al to predict the development of CM-ARF afterpercutaneous coronary intervention, congestive
heart failure, arterial hypotension, CRF, diabetes,and anemia were significantly associated withCM-ARF (Table 4a.1). The same group of authorsshowed more recently that there is no linear rela-tionship between hematocrit and CM-ARF. Theodds of developing CM-ARF were only increasedif the hematocrit dropped below 36%, whichwas the lowest quintile in their analysis.13 Thiscohort study, however, does not address whethercorrection of anemia before intervention willresult in decreased rates of CM-ARF.
Further potential risk factors for CM-ARF are nephrotoxic comedications such as the fre-quently used NSAIDs, but also aminoglyco-sides, amphotericin B, cisplatin, or calcineurininhibitors. Although there is no hard evidencethat these drugs may further increase the rate orduration of CM-ARF, it can be assumed basedon their pharmacodynamics.
PREVENTION OF CONTRAST MEDIA INDUCED ARF
The best preventive measure for CM-ARF is tothink about it in advance. As is true for so manyother situations in life, prevention is much moreefficient than dealing with the adverse conse-quences of a situation. This consideration shouldinclude an estimation of the risk to benefit ratioof the planned diagnostic or therapeutic inter-vention and potential alternative strategies with-out contrast medium in patients at high risk forCM-ARF.
The single best preventive measure of CM-ARF is intravenous hydration, if possible up to
30 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 4a.1 Multivariate predictors of CM-ARF after percutaneous coronary intervention. Modifiedand reprinted with permission from Mehran et al 200412
Variable OR 95% CI p value
Hypotension 2.537 1.973–3.262 <0.0001Intra-aortic balloon pump use 2.438 1.677–3.544 <0.0001Congestive heart failure 2.250 1.682–3.011 <0.0001Serum creatinine >1.5 mg/dl 2.053 1.586–2.658 <0.0001Age >75 years 1.847 1.509–2.260 <0.0001Anemia 1.601 1.328–1.930 <0.0001Diabetes mellitus 1.508 1.260–1.806 <0.0001Contrast volume (per 100 ml) 1.290 1.210–1.375 <0.0001
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 30

8 hours prior to CM application. The type andvolume of choice is not entirely clear but 20 ml/kgof a full electrolyte solution or 154 mEq/l at a rateof 3 ml/kg bolus followed by a continuous infu-sion of 1 ml/kg of a sodium bicarbonate solutionhas been shown to be efficient.8,9 Addition ofmannitol and furosemide to half normal salinein patients with underlying CRF or to normalsaline in patients without CRF does not seem tobe additionally effective.14,15
In addition to volume expansion, several drugshave been investigated for the prevention of CM-ARF. Among the most recently and widely stud-ied medications is acetylcysteine (ACC). Amongthe first randomized controlled trials in patientswith CRF and thus at higher risk, Tepel andcoworkers showed that two doses of 600 mgACC given on the day before and after the appli-cation of a non-ionic low-osmolar contrast agentfor a CT scan could reduce the incidence of CM-ARF.16 All patients were also hydrated withsaline in this trial. In this paper 10 subjects expe-rienced a rise in serum creatinine by more than0.5 mg/dl at 2 days after radiocontrast applica-tion, one in the ACC and nine in the controlgroup. Furthermore, mean serum creatinine evendecreased in the ACC group after CM applica-tion but rose in the control group. To account forpotential interference of ACC with creatininemeasurement, the authors spiked the controlgroup samples with ACC at 2.5 mM but did notderive different values for serum creatinine withand without the ACC supplementation.
In a more recent study, however, Hoffmannand coworkers showed that ACC reduced serumcreatinine in 50 healthy volunteers in the absenceof contrast media but did not affect cystatine cserum concentrations, which is another indicatorof the glomerular filtration rate.17 Based on thesedata it may be speculated that tubular secretionbut not glomerular filtration of creatinine isenhanced by ACC. It is well appreciated thattubular secretion of serum creatinine increaseswith decreasing GFR. Patients in the Tepel studyexhibited a mean serum creatinine of about 2.5 mg/dl. An alternative explanation may bethe fact that ACC alters creatinine metabolismin vivo by activation (suppression of inhibitors)of the creatinine kinase as described by Genetet al.18
From the many studies published after theTepel paper in 2000, no clear conclusion can bedrawn in terms of ACC efficiency to preventCM-ARF. Some of the earlier and small studiesshowed benefits, others did not find any advan-tage over placebo control19–23 (Figure 4a.4). Thisis also reflected by the inhomogeneous findingsof the 10 meta-analyses covering ACC and CM-ARF to date.24–33 This heterogeneity is even moreastonishing since there are only a few random-ized controlled trials of ACC on CM-ARF of bet-ter quality and these systematic reviews includedthe same original studies.
In conclusion, since ACC may be beneficialand is rather cheap and well tolerated it may beused for prophylaxis of CM-ARF, at least inpatients who cannot tolerate vigorous hydration.However, adequately hydrated patients with alow risk of CM-ARF will probably derive nomeasurable benefit from an ACC pretreatment.
Adenosine antagonists have long been evalu-ated for their diuretic and natriuretic propertiesin several circumstances of renal impairment.34
Among the most widely studied adenosine antag-onists is theophylline, which has been shown inclinical trials of low statistical power to maintainGFR after contrast medium application.35–38 Fewpublished studies, however, do not support thesefindings, which may also be seen as publicationbias towards positive outcomes.39 The situation israther similar to the ACC trials, where, dependingon the covariables, different results were found.
Other medical interventions that have beenevaluated for their protective efficacy againstcontrast induced ARF are ascorbic acid, prosta-glandin E1, dopamine, fenoldopam (a selectivedopamine receptor agonist), and statins.40–45 Mostof these published studies showed a beneficial effectof the respective intervention with the exception offenoldopam, which has been proven ineffective inthe largest randomized trial in patients under-going percutaneous coronary interventions.46,47
However, the relative paucity of reproduced dataand the likely publication bias of these small trialspreclude a firm conclusion.
In the clinical routine a frequently asked ques-tion of the thoughtful interventionist is whetherCM-ARF can be prevented by a postinterven-tional hemodialysis or hemofiltration. Since con-trast medium is eliminated mainly by glomerular
CONTRAST NEPHROPATHY 31
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 31

filtration, 70% of the injected dose is clearedwithin a few minutes from the circulation. Thus inpatients without major renal impairment the renalplasma flow of more than 1000 ml/min guaranteesrapid contrast elimination. Now should prophy-lactic hemodialysis or hemofiltration be per-formed in patients with severely impaired renalfunction? Sterner and colleagues showed thatimmediate hemodialysis after contrast expositioncould lower the contrast plasma levels by 80%, butthe authors did not observe a difference in thepostinterventional GFR between the control andthe dialysis group.48 It is of note that both groupsreceived adequate preinterventional hydration.Berger and colleagues came to a similar conclusionalthough their sample size was small.49 Theseauthors noticed, however, that in some patientshemodialysis even seemed to have a negativeeffect on CM-ARF. This was also concluded by a
much larger study published in the same year byVogt and colleagues from Bern.50 The authors ran-domized 113 patients with mild to moderate renalimpairment to postinterventional hemodialysisor no extracorporeal therapy. Patients withhemodialysis showed a significantly higher rise inserum creatinine after intervention compared tothe non-dialyzed subjects (Figure 4a.5). Unex-pectedly, in a more recent study, Marenzi andcolleagues used a similar study setting althoughwith larger contrast volumes and identical sam-ple size but derived the opposite results usinghemofiltration rather than hemodialysis to removethe contrast dye from the patients’ circulation.51
The hemofiltration sessions were started beforethe intervention and continued in an ICU settingfor 18 to 24 hours. Thereported effect of this inter-vention was a reduction in the risk for CM-ARFby 90% which is larger than that observed for all
32 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
–0.6
Agrawal (unpub) (3)
Loutrianakis (2003) (4)
Kay (2003) (43)
Goldenberg (2003) (16)
Boccalandro (2003) (25)
Vallero (2002) (4)
Shyu (2002) (18)
Oldemeyer (2002) (23)
Kahlon (2002) (4)
Durham (2002) (7)
Diaz-Sandoval (2002) (6)
Briguori (2002) (36)
Allaqaband (2002) (10)
Adamian (2002) (6)
Tepel (2000) (14)
Nogareda (2003) (100)
–0.4 –0.2 0
Risk difference (95% Cl)
0.2 0.4 0.6
Figure 4a.4 Forest plot of weighted risk difference of all 16 controlled clinical trials. Relative weight is reported inparentheses after year of publication. Reprinted with permission from Kshirsagar et al 2004.30
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 32

other therapeutic interventions so far. It is ofnote that 25% of all control subjects in this trialrequired at least one hemodialysis treatment forclinical indications.
Based on the findings from these different trialsit is generally accepted nowadays that postinter-ventional hemodialysis is not to be performedeven in patients with moderately impaired base-line renal function. Whether longer term pro-phylactic hemofiltration should be consideredin patients with moderately impaired baselinerenal function who are expected to receive alarge amount (>250 ml) of contrast agent remains
to be determined. In the study by Marenzi andcolleagues, the benefits of randomization couldhave been attenuated by confounding by indica-tion.51 Patients in the hemofiltration group alsoreceived anticoagulant therapyand intensive careobservation/treatment. Therefore the effective-ness of pre- and postinterventional hemofiltrationafter percutaneous coronary intervention needs tobe validated by other investigators and a modi-fied study design before prophylactic hemofil-tration can be unequivocally recommended. Untilthen the attending physician may decide on thebasis of the patient’s background characteristicsand availability of resources.
OTHER CAUSES OF ARF AFTER CONTRAST APPLICATION
Not every ARF occurring after percutaneousinterventions is causally related to the contrastmedia application. As mentioned above, CM-ARFoccurs predominately in patients with many otherrisk factors for ARF such as cardiovascular dis-ease, infections, diabetes, pre-existing CRF, etc. Inclinical praxis an increase in serum creatinine isalmost always classified as contrast nephropathy,whereas other factors such as cholesterol crystalembolism after percutaneous interventions mayoccur. A popular rule of thumb is that a risingserum creatinine in the first day(s) after inter-vention occurs predominately as a consequenceof contrast application, whereas a later rise ofcreatinine and LDH is more predictive of choles-terol emboli. The validity of this rule howeverremains to be investigated.
The reported incidence of cholesterol emboliin the kidneys is below 1%.52 This low numberreported in clinical studies is derived by usingthe incidence of peripheral signs of cholesterolemboli such as black toes as proxy for the inci-dence of cholesterol emboli in the kidneys.However, the renal plasma flow is usually con-siderably higher than the perfusion of the ather-osclerotic legs of resting patients. Since renalbiopsies and serial sectioning of the biopsy coreare virtually never performed in patients experi-encing ARF after intervention the true incidencewill remain unknown. Nevertheless, autopsystudies reported an incidence of cholesterolmicroembolization of between 0.8 and 12%.53
CONTRAST NEPHROPATHY 33
0
200
250
300
350
400
1 2 3Day
4 5 6
200
250
300
350
400
Ser
um c
reat
inin
e (µ
m/l)
All patients
Patients given >150 ml ofradiocontrast media
Figure 4a.5 Mean (± SE) serum creatinine concentrationsbefore and after the administration of radiocontrast mediain patients with chronic renal insufficiency. Only data frompatients who did not require subsequent hemodialysis areincluded. Reprinted with permission from Vogt et al 2001.50
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 33

TREATMENT OF CONTRAST MEDIA INDUCED ARF
As in most cases of multifactorial ARF developingin the ICU, no established causal therapy of CM-ARF exists. Among the key issues in the treatmentof CM-ARF is the avoidance of additional renalinsults after CM-ARF has occurred. This includesaverting or discontinuation of medications thatalter renal hemodynamics such as NSAIDs, cal-cineurin inhibitors, maybe angiotensin convertingenzyme inhibitors, or angiotensin II receptor block-ers. Furthermore, tubulotoxic medication such asamphotericin B or aminoglycoside antibioticsshould not be used, nor re-exposure to radiocon-trast medium if not vitally necessary.
In general, we are aiming for improvement inthe systemic hemodynamic situation by provid-ing sufficient hydration and by fighting systemicinflammation if possible. If all efforts are ineffec-tive and the patient needs renal replacement ther-apy, hemodialysis or hemofiltration is started.Which of the two extracorporeal therapies is better suited depends on the clinical situation;however, in hemodynamically instable patientscontinuous hemofiltration will be the clear treat-ment of choice. The recovery of native renal func-tion is generally good unless other severe riskfactors for ARF such as congestive heart failure orpre-existing chronic renal failure exist.
COMPLICATIONS OF CONTRAST MEDIAOTHER THAN ARF
Hypersensitivity/anaphylaxis
Hypersensitivity reactions have been reportedfor all groups of contrast media including high-osmolar and low-osmolar ionic dimmers, aswell as non-ionic monomers and iso-osmolarcontrast media. However, the non-ionic mediasuch as iohexol, iopamidol or iopromide (low-osmolar monomers) and iodixanol or iotrolan(iso-osmolar dimers) tend to induce less allergicreaction compared to high-osmolar ionic con-trast media. The incidence of delayed type reac-tions (>1 hour after contrast application) wasreported to be in the low single digit percentrange.54 The clinical presentation of the hyper-sensitivity ranges from urticaria and skin rash to more severe phenotypes such as laryngeal
edema, bronchospasm, true anaphylactic shock,and, exceptionally rarely, sudden death. Sincethe exact pathophysiology behind these eventsremains unclear, many different terminologiessuch as anaphylaxis, anaphylactoid, allergic,pseudo-allergic, or idiosyncratic are in use todescribe the reactions following contrast mediaapplications.
Unfortunately there is no pre-exposure testthat may be used to predict the individual’s riskfor such adverse effects. The cutaneous iodinepath test is not predictive at all and the intra/sub-cutaneous iodine injection carries the same risk oftrue hypersensitivity as the intravenous contrastmedia investigation itself. Interestingly, the intra-arterial administration of contrast media is asso-ciated with less hypersensitivity. About everyother subject known to be allergic against contrastmedia exhibits a hypersensitivity reaction againafter rechallenge. The non-ionic media have a muchlower rate of complications, and for all groups,intravenous injection carries a much higher riskthan intra-arterial injection. The only disadvantageof non-ionic media is their cost.
Thyrotoxicosis
All contrast media contain about 30% iodine.Assuming an average volume of 100 ml perangiography, roughly 30 g of iodine are applied.This is about 200 000 times more than the 150 �gdaily amount required for thyroid hormone syn-thesis. Although the thyroid maintains normalfunction in the vast majority of subjects investi-gated with contrast media, a few people (espe-cially those with euthyroid goiter) may develophyperthyroidism. There is, however, no validprediction rule for the individual patient at risk.Furthermore, there seems to be no cross-reactivitybetween contrast hypersensitivity, developmentof hyperthyroidism, and other types of true IgEmediated allergy (Gell and Coombs’s type Ireaction) such as asthma (for review see refer-ence 55). Thus an effective preventive measurefor this scenario is not known.
SUMMARY
It is critical to consider potential adverse effects ofcontrast media before application. Patients with
34 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 34

documented allergies against contrast media whoneed to have re-exposure may benefit from pre-treatment with corticosteroids and antihistamines.
The most effective preventive measure for ARFis adequate hydration; full electrolyte solutionsare probably ideal for that purpose. Acetylcys-teine may be used since it is really cheap and hasalmost no side-effects; its efficacy, however, isunclear to date and there is good evidence thatonly tubular handling of creatinine is altered byacetylcysteine (Table 4a.2).
ACKNOWLEDGMENTS
This work was supported by a European UnionMarie Curie grant (No. 513868) and the AustrianScience Fund VzFnF (Grant P-18325) awarded toDr Oberbauer, Austria.
REFERENCES
1. Levy EM, Viscoli CM, Horwitz RI. The effect of acuterenal failure on mortality. A cohort analysis. JAMA1996; 275(19): 1489–94.
2. Parfrey PS, Griffiths SM, Barrett BJ et al. Contrast material-induced renal failure in patients with diabetesmellitus, renal insufficiency, or both. A prospectivecontrolled study. N Engl J Med 1989; 320(3): 143–9.
3. Marenzi G, Lauri G, Assanelli E et al. Contrast-inducednephropathy in patients undergoing primary angio-plasty for acute myocardial infarction. J Am CollCardiol 2004; 44(9): 1780–5.
4. Dangas G, Iakovou I, Nikolsky E et al. Contrast-induced nephropathy after percutaneous coronaryinterventions in relation to chronic kidney disease andhemodynamic variables. Am J Cardiol 2005; 95(1): 13–19.
5. Chertow GM, Levy EM, Hammermeister KE et al.Independent association between acute renal failureand mortality following cardiac surgery. Am J Med1998; 104(4): 343–8.
6. Solomon R. The role of osmolality in the incidence ofcontrast-induced nephropathy: a systematic review ofangiographic contrast media in high risk patients.Kidney Int 2005; 68(5): 2256–63.
7. Bader BD, Berger ED, Heede MB et al. What is the besthydration regimen to prevent contrast media-inducednephrotoxicity? Clin Nephrol 2004; 62(1): 1–7.
8. Mueller C, Buerkle G, Buettner HJ et al. Prevention ofcontrast media-associated nephropathy: randomizedcomparison of 2 hydration regimens in 1620 patientsundergoing coronary angioplasty. Arch Intern Med2002; 162(3): 329–36.
9. Merten GJ, Burgess WP, Gray LV et al. Prevention ofcontrast-induced nephropathy with sodium bicarbonate:a randomized controlled trial. JAMA 2004; 291(19):2328–34.
10. Aspelin P, Aubry P, Fransson SG et al. Nephrotoxiceffects in high-risk patients undergoing angiography.N Engl J Med 2003; 348(6): 491–9.
11. Wagner HJ, Kalinowski M, Klose KJ et al. The use ofgadolinium chelates for X-ray digital subtractionangiography. Invest Radiol 2001; 36(5): 257–65.
12. Mehran R, Aymong ED, Nikolsky E et al. A simple riskscore for prediction of contrast-induced nephropathyafter percutaneous coronary intervention: developmentand initial validation. J Am Coll Cardiol 2004; 44(7):1393–9.
13. Nikolsky E, Mehran R, Lasic Z et al. Low hematocrit pre-dicts contrast-induced nephropathy after percutaneouscoronary interventions. Kidney Int 2005; 67(2): 706–13.
14. Solomon R, Werner C, Mann D et al. Effects of saline,mannitol, and furosemide to prevent acute decreases inrenal function induced by radiocontrast agents. N EnglJ Med 1994; 331(21): 1416–20.
15. Stevens MA, McCullough PA, Tobin KJ et al. A prospec-tive randomized trial of prevention measures in patientsat high risk for contrast nephropathy: results of theP.R.I.N.C.E. Study. Prevention of Radiocontrast InducedNephropathy Clinical Evaluation. J Am Coll Cardiol1999; 33(2): 403–11.
16. Tepel M, van der Giet M, Schwarzfeld C et al. Preven-tion of radiographic-contrast-agent-induced reductionsin renal function by acetylcysteine. N Engl J Med 2000;343(3): 180–4.
17. Hoffmann U, Fischereder M, Kruger B et al. The valueof N-acetylcysteine in the prevention of radiocontrast
CONTRAST NEPHROPATHY 35
Table 4a.2 Prophylactic strategy for theprevention of contrast media induced acuterenal failure
1 Evaluate hydration status and cardiac functionof the patient; avoid concomitant nephrotoxicsubstances such as NSAIR, aminoglycosides,or vasopressors
2 Intravenous hydration of the patient with fullelectrolyte solutions (isotonic saline) at roughly100 ml/h for 6 to 12 h. Alternatively isotonicsodium bicarbonate solution may be used atthe same rates
3 Acetylcysteine at 600 mg bid before and onthe day of the intervention
4 Use low volume of low- or iso-osmolal contrastmedium in patients at higher risk for CM-ARF
5 No prophylactic use of hemodialysis or hemofiltration
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 35

agent-induced nephropathy seems questionable. J AmSoc Nephrol 2004; 15(2): 407–10.
18. Genet S, Kale RK, Baquer NZ. Effects of free radicals oncytosolic creatine kinase activities and protection byantioxidant enzymes and sulfhydryl compounds. MolCell Biochem 2000; 210(1–2): 23–8.
19. Diaz-Sandoval LJ, Kosowsky BD, Losordo DW. Acetyl-cysteine to prevent angiography-related renal tissueinjury (the APART trial). Am J Cardiol 2002; 89(3): 356–8.
20. Kay J, Chow WH, Chan TM et al. Acetylcysteine for pre-vention of acute deterioration of renal function follow-ing elective coronary angiography and intervention: arandomized controlled trial. JAMA 2003; 289(5): 553–8.
21. Fung JW, Szeto CC, Chan WW et al. Effect of N-acetyl-cysteine for prevention of contrast nephropathy inpatients with moderate to severe renal insufficiency: arandomized trial. Am J Kidney Dis 2004; 43(5): 801–8.
22. Webb JG, Pate GE, Humphries KH et al. A randomizedcontrolled trial of intravenous N-acetylcysteine for theprevention of contrast-induced nephropathy after car-diac catheterization: lack of effect. Am Heart J 2004;148(3): 422–9.
23. Burns KE, Chu MW, Novick RJ et al. Perioperative N-acetylcysteine to prevent renal dysfunction in high-risk patients undergoing CABG surgery: a randomizedcontrolled trial. JAMA 2005; 294(3): 342–50.
24. Duong MH, MacKenzie TA, Malenka DJ. N-Acetyl-cysteine prophylaxis significantly reduces the risk ofradiocontrast-induced nephropathy: comprehensivemeta-analysis. Catheter Cardiovasc Interv 2005; 64(4):471–9.
25. Nallamothu BK, Shojania KG, Saint S et al. Is acetylcys-teine effective in preventing contrast-related nephropa-thy? A meta-analysis. Am J Med 2004; 117(12): 938–47.
26. Misra D, Leibowitz K, Gowda RM et al. Role of N-acetylcysteine in prevention of contrast-inducednephropathy after cardiovascular procedures: a meta-analysis. Clin Cardiol 2004; 27(11): 607–10.
27. Bagshaw SM, Ghali WA. Acetylcysteine for preventionof contrast-induced nephropathy after intravascularangiography: a systematic review and meta-analysis.BMC Med 2004; 2: 38.
28. Pannu N, Manns B, Lee H et al. Systematic review ofthe impact of N-acetylcysteine on contrast nephropathy.Kidney Int 2004; 65(4): 1366–74.
29. Ma IW, Hladunewich M. Does the prophylactic use of N-acetylcysteine prevent contrast nephropathy in patientswith renal insufficiency? CMAJ 2004; 170(8): 1231.
30. Kshirsagar AV, Poole C, Mottl A et al. N-Acetylcysteinefor the prevention of radiocontrast induced nephropa-thy: a meta-analysis of prospective controlled trials. J Am Soc Nephrol 2004; 15(3): 761–9.
31. Alonso A, Lau J, Jaber BL et al. Prevention of radiocon-trast nephropathy with N-acetylcysteine in patients
with chronic kidney disease: a meta-analysis of random-ized, controlled trials. Am J Kidney Dis 2004; 43(1): 1–9.
32. Isenbarger DW, Kent SM, O’Malley PG. Meta-analysisof randomized clinical trials on the usefulness of acetyl-cysteine for prevention of contrast nephropathy. Am JCardiol 2003; 92(12): 1454–8.
33. Birck R, Krzossok S, Markowetz F et al. Acetylcysteinefor prevention of contrast nephropathy: meta-analysis.Lancet 2003; 362(9384): 598–603.
34. Oberbauer R, Schreiner GF, Meyer TW. Natriureticeffect of adenosine A1-receptor blockade in rats.Nephrol Dial Transplant 1998; 13(4): 900–3.
35. Erley CM, Duda SH, Schlepckow S et al. Adenosineantagonist theophylline prevents the reduction ofglomerular filtration rate after contrast media applica-tion. Kidney Int 1994; 45(5): 1425–31.
36. Kolonko A, Wiecek A, Kokot F. The nonselectiveadenosine antagonist theophylline does prevent renaldysfunction induced by radiographic contrast agents. J Nephrol 1998; 11(3): 151–6.
37. Kapoor A, Kumar S, Gulati S et al. The role of theo-phylline in contrast-induced nephropathy: a case-controlstudy. Nephrol Dial Transplant 2002; 17(11): 1936–41.
38. Huber W, Schipek C, Ilgmann K et al. Effectiveness oftheophylline prophylaxis of renal impairment aftercoronary angiography in patients with chronic renalinsufficiency. Am J Cardiol 2003; 91(10): 1157–62.
39. Kramer BK, Preuner J, Ebenburger A et al. Lack of reno-protective effect of theophylline during aortocoronarybypass surgery. Nephrol Dial Transplant 2002; 17(5):910–15.
40. Spargias K, Alexopoulos E, Kyrzopoulos S et al.Ascorbic acid prevents contrast-mediated nephropathyin patients with renal dysfunction undergoing coro-nary angiography or intervention. Circulation 2004;110(18): 2837–42.
41. Sketch MH, Jr, Whelton A, Schollmayer E et al.Prevention of contrast media-induced renal dysfunctionwith prostaglandin E1: a randomized, double-blind,placebo-controlled study. Am J Ther 2001; 8(3): 155–62.
42. Koch JA, Plum J, Grabensee B et al. Prostaglandin E1: anew agent for the prevention of renal dysfunction in highrisk patients caused by radiocontrast media? PGE1 StudyGroup. Nephrol Dial Transplant 2000; 15(1): 43–9.
43. Hans SS, Hans BA, Dhillon R et al. Effect of dopamine onrenal function after arteriography in patients with pre-existing renal insufficiency. Am Surg 1998; 64(5): 432–6.
44. Tumlin JA, Wang A, Murray PT et al. Fenoldopammesylate blocks reductions in renal plasma flow afterradiocontrast dye infusion: a pilot trial in the preventionof contrast nephropathy. Am Heart J 2002; 143(5):894–903.
45. Khanal S, Attallah N, Smith DE et al. Statin therapyreduces contrast-induced nephropathy: an analysis of
36 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 36

contemporary percutaneous interventions. Am J Med2005; 118(8): 843–9.
46. Stone GW, McCullough PA, Tumlin JA et al.Fenoldopam mesylate for the prevention of contrast-induced nephropathy: a randomized controlled trial.JAMA 2003; 290(17): 2284–91.
47. Briguori C, Colombo A, Airoldi F et al. N-Acetylcysteine versus fenoldopam mesylate to preventcontrast agent-associated nephrotoxicity. J Am CollCardiol 2004; 44(4): 762–5.
48. Sterner G, Frennby B, Kurkus J et al. Does post-angiographic hemodialysis reduce the risk of contrast-medium nephropathy? Scand J Urol Nephrol 2000;34(5): 323–6.
49. Berger ED, Bader BD, Bosker J et al. [Contrast media-induced kidney failure cannot be prevented by hemodial-ysis.] Dtsch Med Wochenschr 2001; 126(7): 162–6.
50. Vogt B, Ferrari P, Schonholzer C et al. Prophylactichemodialysis after radiocontrast media in patients with
renal insufficiency is potentially harmful. Am J Med2001; 111(9): 692–8.
51. Marenzi G, Marana I, Lauri G et al. The prevention ofradiocontrast-agent-induced nephropathy by hemofil-tration. N Engl J Med 2003; 349(14): 1333–40.
52. Alamartine E, Phayphet M, Thibaudin D et al. Contrastmedium-induced acute renal failure and cholesterolembolism after radiological procedures: incidence, riskfactors, and compliance with recommendations. Eur JIntern Med 2003; 14(7): 426–31.
53. Zuccala A, Zucchelli P. A renal disease frequentlyfound at postmortem, but rarely diagnosed in vivo.Nephrol Dial Transplant 1997; 12(8): 1762–7.
54. Yasuda R, Munechika H. Delayed adverse reactions tononionic monomeric contrast-enhanced media. InvestRadiol 1998; 33(1): 1–5.
55. Idee JM, Pines E, Prigent P et al. Allergy-like reactionsto iodinated contrast agents. A critical analysis. FundamClin Pharmacol 2005; 19(3): 263–81.
CONTRAST NEPHROPATHY 37
CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 37

CPVI_Chapter04a.qxp 4/5/2007 2:39 PM Page 38

The first angiography was performed in 1896(Figure 4b.1). In the course of time, however, itbecame evident that even low doses cannot beconsidered safe or harmless with respect to car-cinogenesis.1 Currently mean patient radiationexposure due to percutaneous interventions isrelatively high and varies greatly between dif-ferent centers and interventionists2 (Figure 4b.2):for percutaneous cardiac interventions (PCIs),typical mean published dose area product val-ues (DAPs), range from 73 up to 190 Gy × cm2.4
For special interventional procedures determin-istic radiation effects like chronic radiodermati-tis or even deep musculocutaneous injury mayresult,1,5 and represent a matter of serious con-cern (Figure 4b.3). For this reason, directives ofthe International Commission on RadiologicProtection (ICRP) and the EURATOM Council 6,7
stipulate that ‘All medical exposure for radiodi-agnostic purposes . . . shall be kept as low asreasonably achievable’ (ALARA), even belowaccepted reference values recently proposed8 inconsideration of both state of the art and indi-vidual circumstances. The ICRP indeed pointsout that, unfortunately, ‘many interventionistsare not aware of the potential for injury from
procedures, their occurrence, or simple methodsfor decreasing their incidence utilising dose con-trol strategies’1 and recommends credentialingradiation protection training programs for inter-ventionists over and above that required bygeneral radiologists.9,10 Up to today, however,there exists worldwide no validated educationalcourse in radiation reducing techniques whichhas proven of significant benefit in reducingpatient radiation exposure in daily routine.
FREQUENCY AND IDENTIFICATION OFRADIOTOXICITY DUE TO INTERVENTIONALANGIOGRAPHY
Definitions
The former radiation units Roentgen (R), rad,and rem have been replaced by the SI units Gray(Gy; 1 Gy = 100 rad) for air kerma (kinetic energyreleased in matter) and absorbed dose, as well asby the Sievert (Sv; 1 Sv = 100 rem), now appliedfor dose equivalent. For X-rays the radiationweighting factor is 1 for conversion from absorbeddose to dose equivalent (1 Sv = 1 Gy). Entranceskin air kerma (ESAK) prescribes the dose in the
4b
General complications of angiography andperipheral interventions – radiotoxicityEberhard Kuon and Michael Wucherer
Frequency and identification of radiotoxicity due to interventional angiography • Risk factors for radiotoxicity • Prevention of radiotoxic effects • Diagnosis and therapy of radiotoxic effects •Conclusion
The one waits for times to change, another tackles challenging timesDante Alighieri
CPVI_Chapter04b.qxp 4/5/2007 2:40 PM Page 39

entrance plane of the patient without backscatterradiation. Entrance skin dose includes backscatterand represents the most appropriate quantity forcharacterization of deterministic risks, especiallyradiation induced skin lesions.
DAP is the product of the air kerma in theentrance plane of the patient and the area of theirradiating beam, and can be easily measured nearthe X-ray tube. It is independent of the distancefrom the X-ray source; it is best suited to estimateradiation exposures of fluoroscopy guided inter-ventions with varying angulations.
The effective dose (ED) is the sum of all riskweighted organ dose equivalents and was pri-marily defined by the ICRP to stipulate limits foroccupational radiation exposures. The stochasticrisk is proportional to the effective dose. DAPto ED conversion factors for special conditions(undercouch tube position, 80 to 110 kV and 2to 5 mm aluminium filtration, adult standardpatient) have been calculated to range between0.13 and 0.26 mSv/Gy × cm2 for thoracic, 0.18and 0.33 mSv/Gy × cm2 for abdominal, and 0.15and 0.33 mSv/Gy × cm2 for hip examinations.11
Therefore two types of radiotoxic effects –deterministic as well as stochastic – are of majorrelevance and both should be taken into accountin clinical routine.
Deterministic effects
Table 4b.1 summarizes skin reactions and theirthreshold doses. There exist no reliable data aboutthe incidence of various types of deterministicskin lesions. These effects are likely to occur afterprolonged exposure to the same skin area. In clin-ical routine faint erythema due to local exposure
40 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 4b.1 The first angiography: postmortem depictionof a hand (von Haschek and Lindenthal, Vienna, January1896; German museum of X-ray technology); contrastmedium was a mixture of lime, mercury, and paraffin oil.
0
50
100
150
200
1998 2000 2002 2004 2006
DAP(Gy × cm2)
Coronary angioplasty
Coronary angioplasty
Combined intervention (PCI)
Figure 4b.2 Patient dose area products (DAPs) fromcoronary angiography (filled triangles), percutaneous transluminal coronary angioplasty (gray circles), andcombined coronary interventions (open squares), published from 1998 to 2004, vary greatly in extent.
Figure 4b.3 Chronic radiodermatitis of the left shoulder.
CPVI_Chapter04b.qxp 4/5/2007 2:40 PM Page 40

of 2 to 3 Gy, eliciting an activation of histaminelike substances, typically goes unnoticed becauseof its brief presence. Main erythema followingthreshold values of 2 to 8 Gy is caused by aninflammation subsequent to the destruction ofbasal cells in the epidermis. With a prevalence of50% at about 21 Gy necrosis as a result of vascu-lar damage in the dermis will develop 10–16weeks after exposure.12,13
For the 17 cm and the 13 cm image intensifierfield (and a focus image intensifier/focus skinmagnification ratio of approximately 2) patiententrance skin areas of approximately 60 cm2
and 40 cm2 will result.14 According mean fluoro-scopic DAP rates at levels of approximately 40 ±12 mGy × cm2/s generated in clinical routine(Table 4b.1)12,15 reported threshold doses for thechest region will be achieved by the fluoroscopytimes and DAP values under conditions of dif-ferent image intensifier sizes respective entranceskin areas.
Stochastic effects
Although there are clear benefits from the use ofdiagnostic X-rays and in especially for interven-tional procedures, it is generally acknowledged
that their use involves some risk of cancer. In 14developed countries, estimates of the risk attrib-utable to diagnostic X-rays ranged from 0.6 in theUnited Kingdom up to 4.4% in Japan, corre-sponding to an estimated annual X-ray exposurefrequency of 0.49 up to 1.57 per individual,respectively.16 Indeed a survey of UK practice17
has suggested that the comparatively low fre-quency of diagnostic X-ray use is due in part tothe detailed guidance for doctors on the indica-tors for X-ray examinations issued by the RoyalCollege of Radiologists.18 The additional individ-ual stochastic lifetime cancer mortality risk of aneffective dose of 1 Sv over the course of 40 yearshas been calculated as 7–11% for high-level and5–10% for low-level (<0.1 Sv/h) radiation inten-sity,19,20 and the stochastic lifetime cancer mortal-ity risk of a cardiac intervention generating aneffective dose of 10 mSv is calculated to amountto approximately 0.4‰.14,21–23 For patients with amean age of around 60 years undergoing cardiacinterventions, approximately 0.2‰ of them willdie from stochastic hazards of the related radiationexposure. In the UK the prospective incidenceof cancer due to cerebral and coronary angiogra-phy has been calculated to amount to 0.18‰ and0.28‰, respectively, and therefore again to be
RADIOTOXICITY 41
Table 4b.1 Threshold doses, calculated fluoroscopy time and DAPs, respectively, for various skineffects as well as onset time toward skin reaction (chest region)
Threshold values for Single dose Fluoroscopy time 1 DAP2 DAP3 Onset(Gy) (min) (Gy × cm2) (Gy × cm2) (weeks)
Early transient erythema 2 50 120 80 hoursTemporary epilation 3 75 180 120 3Main erythema 6 150 360 240 1.5Permanent epilation 7 175 420 280 3Dry desquamation 10 250 600 400 4Invasive fibrosis 10 250 600 400Dermal atrophy 11 275 660 440 14Teleangiectasis 12 300 720 480 52Moist desquamation 15 375 900 600 4Late erythema 15 375 900 600 6–10Dermal necrosis 18 450 1080 720 10Secondary ulceration 20 500 1200 800 6
1Mean fluoroscopic DAP rate 40 ± 16 mGy × cm2/s for the 17 cm image intensifier field (110 interventionists – performing 10 coronaryangiographies each – at 20 cardiac centers): equivalent to a skin dose (irradiated skin area approx 60 cm2) of 0.04 Gy/min.2For one angulation and an irradiated skin area of 60 cm2.3For one angulation and an irradiated skin area of 40 cm2.
CPVI_Chapter04b.qxp 4/5/2007 2:40 PM Page 41

lower than in other developed countries.16 Indeed,a recently performed European benchmarkingproject revealed slightly lower DAPs for coronaryinterventions in Ireland and the UK.8
Statistical models indicate a fatal cancer riskincrement range of 0.4 to 1.2‰, the latter figurecharacterizing the upper 90% confidence limit.Conclusively the risk of mortality from a malig-nancy induced during a typical cardiologicintervention with a DAP of 200 Gy × cm2 wasconsidered in the actual ACC/AHA ClinicalCompetence Statement to be less than 1%.10
Optimized interventional techniques in clini-cal routine, however, have facilitated meanDAPs of 4.2 ± 1.6 Gy × cm2 for elective coronaryangiography and 7.8 ± 6.1 Gy × cm2 for coronaryangioplasty.3,24
RISK FACTORS FOR RADIOTOXICITY
The deterministic as well as stochastic risk ofpatients undergoing interventional proceduresincreases with obesity, procedure complexity,high-resolution magnification or image intensi-fier entrance dose level, and operator fatigue.Furthermore, that risk will depend on equipmentperformance and the interventionist’s experiencein radiation reducing techniques – as reportedbelow – for example, correct beam collimation.Keeping the image intensifier as close to the patientas possible minimizes the source to image distance(SID), which results in less blurring of the image,and also allows the image intensifier to serve asa barrier between the patient and the operator.24
PREVENTION OF RADIOTOXIC EFFECTS
Efficient interventional techniques towardsreduction of patient exposure include measuresas follows:
• Restriction to essential radiographic frames andruns essential for diagnostic purposes. Inter-ventionists should be aware of (comparedwith fluoroscopy) the typically 12- to 25-foldhigher intensity of radiography, which creates60–70% of total DAP. A new rotary switch,triggering each coronary run towards one totwo heart cycle lengths, has enabled a reduc-tion of patients’ effective dose from coronaryangiography to 0.8 mSv.25
• Collimation to the region of interest (‘buttonhole’technique) The senior cardiologist shouldshow the interventional cardiologic begin-ners how to collimate during fluoroscopy byshort taps on the foot switch, with advan-tage taken of the ‘last image hold’ function.Beginning from partly closed lateral tubeattached lead blinds, fluoroscopy guided col-limation to the region of interest will occa-sion far less DAP than collimation from awide open image intensifer entrance field.14,26
Collimation to the region of interest moreoverimproves image quality and will efficientlyreduce backscatter and in consequence theoperator dose while, for example, aspiratingan occluding thrombus (Figure 4b.4).
• Adequate instead of best possible image quality.The widely accepted ALARA principleobliges interventionists to achieve adequateinstead of best possible image quality for bothradiography and fluoroscopy, which occa-sions slightly higher contrast and produces
42 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 4b.4 Collimate even during emergency interventions such as absorption of occluding thombus(left panel) and for documentation of the final result.
CPVI_Chapter04b.qxp 4/5/2007 2:41 PM Page 42

insignificantly more background mottling.27
In addition, a low-level fluoroscopy modeshould be used as often as possible. If theinterventional communities accept a radi-ographic frame rate of 12.5/s for an ade-quate documentation of the coronary arteriesin motion, an identical fluoroscopic pulserate of 12.5/s, supported by the commonlyavailable technical advancement of ‘gap fill-ing’, should consequently be judged sufficientto guarantee diagnostic and interventionalsafety and accuracy.14,15 The coronary modeinstead of the digital subtraction techniquefacilitates DAPs below 15 Gy × cm2, even for complex interventions such as excimerlaser angioplasty (ELCA) of renal in-stentrestenoses (Figure 4b.5).
• Lowest justifiable magnification. Use of the low-est degree of image magnification requiredfor accurate interpretation substantiallyreduces skin dose. Dose increments due tomagnification are generally higher for con-ventional image intensifier systems than forflat panel detector systems.10,27
• Full inspiration during radiography for chestregions of interest reduces superimpositionof the diaphragm and in consequence radia-tion intensity.
• Preference for tube angulations that rotate outskeletal structures out of the radiation beam.
• Geometric considerations – heed the inverse-square law. The distance between the X-raytube and the patient should be practicablymaximized. Keeping the image intensifier asclose to the patient as possible minimizes the
source to image distance, which decreasesblurring of the image and allows the imageintensifier to serve as a barrier between thepatient and operator.10 The operator’s occu-pational dose, moreover, depends on his orher case load, adequate use and acceptanceof lead protection devices, and distancefrom the isocenter.28–30 Interventionists, how-ever, should remember to step back from thepatient’s isocenter diagonal to the couch, andnot simply backwards, in order not to leavethe ceiling-attached lead glass protection.29
• Well-experienced and well-rested operators.Radiation exposure to patients resulting fromPCIs is influenced by fatigue and signifi-cantly rose by 28%, due to more and longerradiographic runs, after the cardiologists’workload amounted to more than 6 h.31
• Keep DAP in sight and mind in order to pro-mote self-surveillance of the personnel.32
• Radiation-reducing planning of diagnostic cathe-terization requires profound knowledge aboutless irradiating angulations.24 In invasivecardiology six standard runs are used – onefor the left ventricle, three for the left coronaryartery (LCA), and two for the right coronaryartery (RCA) – depending on anatomy anddiagnostic details supplemented by 1 to 4well-collimated variable projections.2 At ananthropomorphic Rando–Alderson phantom,for the chest region and during fluoroscopy,the mean patient DAP rate and the respec-tive operator dose were lowest in the postero-anterior (PA) angulation and rosesignificantly by 3.7 and 10.6 times the PA 0°
RADIOTOXICITY 43
Figure 4b.5 Adequate instead of best possible image quality: test angiographic mode instead of digital subtractiontechnique in the abdominal and pelvis region. Excimer laser angioplasty (ELCA) of a recurrent renal in-stent restenosis.
CPVI_Chapter04b.qxp 4/5/2007 2:41 PM Page 43

baseline values toward left anterior oblique(LAO) 100°, and 3.7 and 2.4 times towardright anterior oblique (RAO) 100°, respec-tively. Patient and operator values for allPA projections, angulated to the right andleft, increased approximately 2.5 times toward
30° craniocaudal angulations24,33 (Figures 4b.6and 4b.7).
• Rotational angiography, rotating the gantry at40°/s throughout an angle of 120° aroundthe region of interest, facilitates a three-dimensional impression under conditions
44 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
200 cm
180 cm
160 cm
140 cm
120 cm
100 cm
80 cm
60 cm
40 cm
20 cm
0 cm40°
30°20°
10°0°
10°20°
400
300200
150
100
50
200 300400
50030°
40°
500
600
700
800
900
1000
Cranial
PA
Caudal
Height
PA 0°
Figure 4b.6 Isodose lines in a three-dimensional graph of the operator’s personal dose per time (�Sv/h), as a function oftube angulation and height above ground for craniocaudal postero-anterior (PA) angulations.33 Reproduced from Kuon et al.Fortschr Röntgenstr 2004; 176: 739–45 with permission from Georg Thieme Publishers.
30°
20°
10°
0°
10°
20°
30°
100° 90° 80° 70° 60° 50° 40° 30° 20°10° 0° 10° 20° 30°40°50°60°70°80°90°100°
0
200
400
600
800
1000
1200
1400
1600
1800
2000
2200
2400
2600
LAO
RAO
PA
Caudal
Cranial
Operator exposure[µSv/h]
Figure 4b.7 Calculated isodose lines in a three-dimensional graph of the operator’s mean personal dose per time (�Sv/h), as a function of tube angulation. LAO = left anterior oblique, PA = postero-anterior, RAO = right anterior oblique.24
CPVI_Chapter04b.qxp 4/5/2007 2:41 PM Page 44

of adequate image quality and represents,even in invasive cardiology, a new, safe, anduseful method for the special indication ofadvanced renal insufficiency: the volume ofcontrast medium, the overall DAP, and thenumber of radiographic frames are signifi-cantly below typical published values in thestandard mode.34
Conclusively a patient’s anatomic state, e.g.weight, as well as the complexity of interventionis a relevant, influencing factors of patient dose.For routine clinical cardiac procedures, consistentcollimation could be proved to be the most effi-cient influencing factor. For diagnostic purposes,again collimation and restrictions to the essentialnumber of radiographic frames and to adequateinstead of best possible image quality were moreefficient than optimization of fluoroscopy time.26
Operator’s radiation exposure
In addition to the above mentioned recommen-dations, the operator’s occupational exposurealso depends on an adequate use and acceptanceof lead protection devices, case load, and dis-tance from the isocenter. Halving the source tooperator distance will quadruple the originaloccupational scatter radiation.
Use of 1.0-mm overcouch and undercouchshielding facilitated a reduction of stray radiationin the operator’s position during fluoroscopytowards an anthropomorphic Rando–Aldersonphantom from a mean of 4.7 �Sv/Gy × cm2 to6% of baseline. The closure of radiation leakagebetween the table-attached over- and undercouchprotection devices by a 1.0-mm lead equivalentundercouch top and overcouch flap adjacent to thetable reduced mean stray radiation in the opera-tor’s position to approximately 1%. The addi-tional use of a 0.5 mm lead apron, collar, glasses,foot-switch shield, and 1.0 mm lead coveraround the patient’s thighs was efficient downto mean levels below 10 nSv/Gy × cm2 and inconsequence to mean levels of 0.2% of baseline29
(Figure 4b.8).
DIAGNOSIS AND THERAPY OF RADIOTOXIC EFFECTS
Deterministic radiotoxic effects typically willand should be treated by dermatologic special-ists familiar with and experienced in therapeu-tic challenges of radiogenic skin injuries. If aninterventional procedure carries a significant riskof such injury, in addition to risks of embolism,stroke, and contrast medium allergy patients
RADIOTOXICITY 45
Figure 4b.8 Optimized table-attached radiation protection with closure of radiation leakage between overcouch andundercouch lead protection devices and a lead cover around the patient’s thighs.
CPVI_Chapter04b.qxp 4/5/2007 2:41 PM Page 45

should be counselled on the future possibility oferythema or more serious skin injury. Moreover,all patients with estimated skin doses of � 2 Gyshould be counselled after the procedure andfollowed for up to 2 weeks after exposure.1
CONCLUSION
Adequate radiation reducing techniques andconsistent use of table-attached and individualprotection devices in clinical routine will indeedprevent observable deterministic injuries andwill avoid a significant increase in cancer risk. Anew practical 90 minute minicourse in radiationreducing techniques enabled cardiologic inter-ventionists to optimize mean patient DAP valuesof coronary angiography by 47%.15 Conclusively,this validated pilot initiative of the Encourage to Less Irradiating Cardiologic InterventionalTechniques (ELICIT) study group is promisingand resolves discussions about adequate train-ing and supervision in those techniques.1,9,10,35
In efforts to validate efficient training programsin invasive cardiology and angiology, regulardocumentation of fluoroscopic and radiographicDAP fractions, and number of radiographicframes – i.e. time-adjusted dose parametersDAPR/frame and DAPF/time – in addition tofluoroscopy time and total DAP, has beenproved to be a reliable instrument for self-surveillance and supervisory control of eachoperator’s individual long-term efforts towardsless radiation exposure.15,28
REFERENCES
1. Valentin J. Avoidance of radiation injuries from medicalinterventional procedures, ICRP Publication 85. AnnICRP 2000; 30: 7–67.
2. Kuon E, Dahm JB, Robinson DM et al. Radiation-reducingplanning of cardiac catheterisation. Z Kardiol 2005; 94:663–73.
3. Kuon E, Empen K, Rohde D et al. Radiation exposure topatients undergoing percutaneous coronary interven-tions – are current reference values too high? Herz2004; 29: 208–17.
4. Larrazet F, Dibie A, Philippe F et al. Factors influencingfluoroscopy time and dose–area product values duringad hoc one-vessel percutaneous coronary procedures.Br J Radiol 2003; 76: 473–7.
5. Monaco JL, Bowen K, Tadros PN et al. Iatrogenic deepmusculocutaneous injury after percutaneous coronaryintervention. J Invas Cardiol 2003; 15: 451–6.
6. Recommendations of the International Commission onRadiological Protection, ICRP Publication 60, PergamonPress. Ann ICRP 1991; 21: 26,153,172.
7. European Commission Council Directive (97/43/EURATOM) on health protection of individuals againstthe dangers of ionizing radiation in relation to medicalexposure. Official J Eur Commun 1997; L180: 22–7.
8. Neofotistou V, Vanó E, Padovani R et al. Preliminaryreference levels in interventional cardiology. EurRadiol 2003; 13: 2259–63.
9. MARTIR – Multimedia and Audiovisual RadiationProtection Training in Interventional Radiology. CD-ROM. Radiation Protection 119. Publication Departmentof the European Commission, Office for Official Publi-cations of the European Communities, Luxembourg 2002:[email protected].
10. Hirshfeld JW, Balter S, Brinker JA et al. ACCF/AHA/HRS/SCAI Clinical Competence Statement on PhysicianKnowledge to Optimize Patient Safety and Image Qual-ity in Fluoroscopically Guided Invasive Cardiovascu-lar Procedures. A Report of the American College ofCardiology Foundation/American Heart Association/American College of Physicians Task Force on ClinicalCompetence and Training. Circulation 2005; 111: 511–32.
11. Hart D, Jones DG, Wall BF. Estimation of effective dosein diagnostic radiology from entrance surface dose anddose area measurements, National Radiological Protec-tion Board (NRPB-R 262). London: HMSO PublicationsCentre, 1994: 1–57.
12. Wagner LK, Eifel PJ, Geise RA. Potential biologicaleffects following high X-ray dose interventional proce-dures. J Vasc Interv Radiol 1994; 5: 71–84.
13. Wagner LK. Biologic effects of high X-ray doses. RSNAPublication 26 November 1995: 167–70.
14. Kuon E, Glaser C, Dahm JB. Effective techniques toreduce radiation dosage to patients undergoing inva-sive cardiac procedures. Br J Radiol 2003; 76: 406–13.
15. Kuon E, Empen K, Robinson DM et al. Efficiency of amini-course in radiation-reducing techniques – an‘Encourage to Less Irradiating Cardiologic InterventionalTechniques (ELICIT®)’ pilot-initiative. Scientific letter.Heart 2005; 91: 1221–2.
16. Berrington de González A, Darby S. Risk of cancer fromdiagnostic X-rays: estimates for the UK and 14 othercountries. Lancet 2004; 363: 245–351.
17. Tanner RJ, Wall BF, Shrimpton PC et al. Frequency ofmedical and dental examinations in the UK: 1997/98.Chilton: National Radiological Protection Board, 2000.
18. Royal College of Radiologists. Making the Best Use of aDepartment of Clinical Radiology: Guidelines for doctors,5th edn. London: Royal College of Radiologists, 2003.
46 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter04b.qxp 4/5/2007 2:41 PM Page 46

19. United Nations Scientific Committee on the Effect ofAtomic Radiation. Sources, effects and risks of ionizingradiation. Annex F. Radiation carcinogenesis in man.UNSCEAR report to the UN general assembly. New York:United Nations, 1988: E.88.IX.7.
20. Committee on the Biological Effects of Ionizing Radiation.Health effects of exposure to low levels of ionizing radia-tion. BEIR V National Academy of Sciences/NationalResearch Council. Washington, DC: National AcademyPress, 1990.
21. Johns PC, Renaud L. Radiation risk associated withPTCA. Primary Cardiol 1994; 20: 27–31.
22. Karppinen J, Parviainen T, Servomaa et al. Radiationrisk and exposure of radiologists and patients duringcoronary angiography and percutaneous transluminalcoronary angioplasty (PTCA). Radiat Prot Dosim 1995;57: 481–5.
23. Harrison D, Ricciardello M, Collins L. Evaluation ofradiation dose and risk to the patient from coronaryangioplasty (PTCA). Aust NZ J Med 1998; 28: 57–63.
24. Kuon E, Dahm JB, Empen K et al. Identification of less-irradiating angulations in invasive cardiology. J Am CollCardiol 2004; 44: 1420–8.
25. Kuon E, Schmitt M, Dorn C et al. Predialing the numberof cinegraphic frames enables an effective patient dosedue to coronary angiography of 0.8 mSv. FortschrRöntgenstr 2003; 175: 1706–10.
26. Kuon E, Robinson DM, Empen K et al. Fluoroscopytime – an overestimated factor for patient radiationexposure in invasive cardiology. Fortschr Röntgenstr2005; 177: 812–17.
27. Kuon E, Dorn C, Schmitt M et al. Radiation dose reduc-tion in invasive cardiology by restriction to adequate
instead of optimized picture quality. Health Phys 2003;84: 626–31.
28. Kuon E, Günther M, Gefeller O et al. Standardization ofoccupational dose to patient’s DAP enables reliableassessment of radiation-protection devices in invasivecardiology. Fortschr Röntgenstr 2003; 175: 1545–50.
29. Kuon E, Schmitt M, Dahm JB. Significant reduction ofradiation exposure to operator and staff during cardiacinterventions by analysis of radiation leakage andimproved lead shielding. Am J Cardiol 2002; 89: 44–9.
30. Vanó E, Gonzalez L, Guibelalde E et al. Radiation exposure to medical staff in interventional and cardiacradiology. Br J Radiol 1998; 71: 954–60.
31. Kuon E, Dahm JB, Schmitt M et al. Time of day influ-ences patient’s radiation exposure due to percutaneouscardiac interventions. Br J Radiol 2003; 76: 189–91.
32. Wyart P, Dumant D, Gourdier M et al. Contribution ofself-surveillance of the personnel by electronic radiationdosemeters in invasive cardiology. Arch Mal CoeurVaiss 1997; 90(2): 233–8.
33. Kuon E, Empen K, Reuter G et al. Personal operator dosein invasive cardiology as a function of body height andtube angulation. Fortschr Röntgenstr 2004; 176: 739–45.
34. Kuon E, Niederst PN, Dahm JB. Usefulness of rota-tional spin for coronary angiography in patients withadvanced renal insufficiency. Am J Cardiol 2002; 90(4):369–73.
35. European Commission. Guidelines on education andtraining in radiation protection for medical exposures.Radiation protection 116. European Commission. Luxem-bourg: Directorate General Environment, Nuclear Safetyand Civil Protection, 2000. URL: http://europe.eu.int/comm/environment/radprot.
RADIOTOXICITY 47
CPVI_Chapter04b.qxp 4/5/2007 2:41 PM Page 47

CPVI_Chapter04b.qxp 4/5/2007 2:41 PM Page 48

Part II
Specific complications by vessel area orspecific scenarios
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 49

CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 50

INTRODUCTION TO THE FREQUENCY ANDKIND OF ACCESS SITE COMPLICATIONS
Percutaneous transluminal procedures are associ-ated with a considerable risk of access site compli-cations.1,2 Although life-threatening complicationsrarely occur after routine percutaneous vascularapproaches, a 1 to 6% incidence of hematoma,pseudoaneurysms, or arteriovenous (AV) fistulasis reported after coronary and peripheral proce-dures,2–4 and 20 to 40% of these patients requiresurgical repair.5,6 In particular, the widespread useof aggressive platelet inhibition tends to increasethe frequency of complications at the vascularaccess site,7–9 and lead to considerable morbidityand costs due to prolongation of the hospitalstay.10 Optimization of access site managementafter percutaneous transluminal procedures isthus recognized as a matter of immediate clini-cal importance.11
Access sites
Technically feasible arterial access routes includeroutinely transfemoral, transradial, and trans-brachial punctures. Transpopliteal, transaxillar,pedal, or carotid approaches are less frequently
performed due to an increased risk of complica-tions. For venous access, transfemoral and trans-jugular approaches are most frequently used.Arterial and venous access site complicationsinclude hematoma, bleeding, pseudoaneurysmformation, AV fistula, infection, nerve injury,vessel dissection, and vessel occlusion.
Incidence of complications
Reported frequencies of access site complica-tions depend on whether diagnostic or thera-peutic procedures are considered. After purelydiagnostic procedures severe hematoma (requir-ing transfusion or surgery, or causing delayeddischarge) are reported in 0 to 0.68%, dissectionor occlusion are reported in 0 to 0.76%, and for-mation of pseudoaneurysms or AV fistulas in0.04 to 0.2% of cases.12 In interventional proce-dures, these frequencies rise due to larger sheathsizes, more aggressive anticoagulation, andlonger duration of the procedures. Bleeding isreported in 3.4%, pseudoaneurysms or AV fistu-las in 0.6%, and dissections or occlusions in upto 1%.13 Retroperitoneal hematoma is an infre-quent (0.15%) but morbid complication.
5
Arterial and venous access site complicationsMartin Schillinger
Introduction to the frequency and kind of access site complications • Factors identifying high-riskpatients for complications • Complications of specific interventional steps and tools • Methods to detect potential complications – which diagnostic steps are needed routinely to rule out or identifycomplications? • Endovascular, surgical, and medical techniques to resolve complications • Methods toavoid complications • Summary • Check list for emergency equipment
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 51

Blood loss
Bleeding and hematoma (Figure 5.1) may occureither acutely during the intervention due tofailed puncture of the artery or vein, duringremoval of the sheath, or subacutely hours afterthe intervention. Risk factors for bleeding includefemale gender, advanced age, low body weight,obesity, hypertension, renal insufficiency, coagu-lation disorders, aggressive anticoagulation, anddiseased access sites. Furthermore, aortic insuf-ficiency was reported to associate with poor vascular closure. Puncture technique and sheathsize are procedural factors which influence thelikelihood for bleeding. Bleeding most frequentlyoccurs after popliteal and antegrade femoralaccess. Axillary puncture also is associated with a higher risk for bleeding. Radial punctureis safest with respect to bleeding; retrogradefemoral access also is considered quite safe inthis context.
Persistent bleeding can lead to hemorrhagicshock, and development of large hematomas.Secondary problems of hematomas are infec-tion, hemorrhagic shock, and compression/compartment syndromes. Persistent bleeding isa particular problem at access sites where externalcompression cannot be performed adequately,e.g. after transaxillary access (Figure 5.2), and ataccess sites where compartment syndromes eas-ily occur, e.g. after brachial or popliteal access.Treatment of bleeding consists of compression,either manually or by external compression
devices such as FemostopTM (RADI MedicalSystems, Uppsala, Sweden). Patients with persis-tent bleeding have to be monitored with respectto heart rate, blood pressure, and blood count.Alternative treatments include prolonged ballooninflation, coiling of the leakage, implantation ofcovered stents, and vascular surgery.
Bleeding to deep subcutaneous tissue or retro-peritoneal bleeding may initially not cause anyapparent clinical signs and thus can be easilyoverlooked with catastrophic clinical consequen-ces. There are two potential manifestations ofretroperitoneal bleeding: first, an ilipsoashematoma when blood enters and is confinedwithin the fascia of the iliopsoas muscle. Thiscomplication is associated with the risk of com-pression neuropathy as the lumbar plexus maybe affected due to compartment syndrome by thehematoma. Second, retroperitoneal bleeding canoccur to the space between the peritoneum andretroperitoneal structures, which is vast, can con-tain huge quantities of blood and can be difficult todetect clinically until hemodynamic deteriorationoccurs. Infection usually is a problem of largehematomas, or in patients after repair of pseudo-aneurysms. Other complications like permanentnerve injury very rarely occur.
Hematoma can be a rather harmless complica-tion leading to ecchymosis. In contrast, largehematomas can cause compression or compartmentsyndromes, and may be complicated by infection.
Compression of adjacent structures by hema-tomas can occur. For example, compression of afemoral or iliac vein can lead to lower extremitydeep venous thrombosis with its complications.
52 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 5.1 Large hematoma after 8 French transfemoralaccess. The complication could be managed by prolongedmanual compression.
Figure 5.2 Hematoma after transaxillary access. Thisapproach has been abandoned at our institution.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 52

This is an especially worrisome complication asdeep vein thrombosis should be treated by anti-coagulation; recent bleeding and large hema-tomas usually prohibit an immediate start withfull-dose anticoagulation and these patientstherefore are at a considerable risk for pulmo-nary infarction. Compression of nerves maylead to irreversible injury, and neurologic deficitdue to nerve compression is a clear indicationfor surgical decompression. Finally, large hema-tomas with massive swelling may also causeconsiderable tension on the skin and can induceskin necrosis.
Depending on the size of the compartment,relatively large amounts of blood are required tocause compartment syndromes at the thigh, whereassmaller amounts of blood can cause popliteal or brachial compartment syndrome. Swelling,massive pain, paresthesia, and later on motordysfunction are signs of compartment syndromewhich must be urgently treated by fasciotomy,otherwise the extremity and the life of thepatient are endangered. Various techniques existto measure compartment pressures, in most casesclinical judgment will prompt the decision forsurgery.
Infection
The rate of infection at the access site is verysmall (below 0.1%) in the absence of hematomaand secondary procedures to resolve access sitecomplications. This incidence increases whenlarge hematomas, surgical procedures, or throm-bin injection complicate vascular access. There-fore, antibiotic prophylaxis seems indicated inpatients with very large hematomas, particu-larly when ultrasound indicates a large volumefor the hematoma, and also in patients with sec-ondary surgical interventions at the access site.
Pseudoaneurysms
These are the most frequent arterial access sitecomplications (Figure 5.3) and mostly are due toprimarily insufficient access site management,e.g. inadequate manual compression or failedclosure devices. Pseudoaneurysms bear the riskof late rupture, and therefore have to be treatedeven when the diameter of the pseudoaneurysmis small. Besides the risk of rupture, infection ofthe pseudoaneurysm can complicate the furthercourse of the patient. Embolization from a pseu-doaneurysm is a very rare event.
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 53
Figure 5.3 Ultrasound image of a partially thrombosed inguinal pseudoaneurysm after transfemoral access with a 6 French sheath.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 53

Arteriovenous fistulas
These are the result of a failed puncture when theartery and the vein are punctured (Figure 5.4).Depending on the shunt volume, an AV fistulamay remain asymptomatic and can be treatedconservatively when the shunt is small, but mayalso cause signs of leg ischemia or heart failurein cases with large shunt volumes. There arealso cases with a combination of an AV fistulaand a pseudoaneurysm (Figure 5.5). The highestrisk for development of AV fistulas is reportedafter popliteal puncture, and prepuncture ultra-sound is definitively recommended to localizethe artery and vein before accessing the vessel.
Access vessel dissection, occlusion
Dissection or occlusion of the access vessel rarelyoccurs in healthy vascular segments. In patientswith heavy disease at the access site – e.g. com-mon femoral artery stenosis – puncturing theplaque and advancing the wire may cause plaquedisruption, vessel dissection, and occlusion.Hydrophilic guidewires usually have a higherrisk for dissection. The risk for dissection is also
increased when the vessel segment proximal tothe access site is severely stenosed or occluded –in these patients pulsatile flow can be absent evenin the true lumen and differentiating betweentrue and false lumen can be difficult.
54 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 5.4 Ultrasound image of an inguinal arteriovenous fistula and a partially thrombosed pseudoaneurysm aftertransfemoral access with a 6 French sheath.
Figure 5.5 Angiographic image of an arteriovenous fistulaand a pseudoaneurysm after transfemoral arterial access.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 54

FACTORS IDENTIFYING HIGH-RISK PATIENTSFOR COMPLICATIONS
Several risk factors identifying high-risk patientsfor access site complications have been described,unfortunately some of these risk factors likeobesity or severe aortic insufficiency cannot bemodified. Nevertheless, adequate puncture tech-nique and puncture site management allow safeaccess even in these high-risk patients.
Morphology of the access site
Mechanical constriction of the arterial wall atthe puncture hole after removal of the sheath incombination with platelet aggregation is the keyfeature of local hemostasis at the arterial accesssite. The morphology of the access site thereforeplays a major role. Increased patient’s age, femalesex, obesity, uncontrolled arterial hypertension,and previous procedures via the same access routeare well known risk factors in this context.Plaques, severe calcification, or even pre-existentstenosis at the site of puncture increase the riskfor bleeding, dissection, and acute or subacuteocclusion. Furthermore, the puncture at atypicalsites and the puncture of prosthetic or vein graftsare associated with higher rates of adverse events.For the most frequent arterial access, the trans-femoral approach, puncture of the commonfemoral artery is recommended and puncture ofthe superficial femoral artery (distal puncture)as well as puncture of the external iliac artery(proximal puncture) are associated with higherfrequencies of pseudoaneurysms (for the super-ficial femoral artery puncture) and bleeding (forthe iliac puncture).
Systemic coagulation disorders
Low platelet counts are known to predict bleedingcomplications after vascular surgery. In thiscontext, a strong association between low prein-tervention platelet counts and occurrence of pseu-doaneurysms after arterial puncture recentlyhas also been acknowledged as a risk factor forpseudoaneurysm formation after percutaneousinterventions in patients with a platelet countbelow 200.000/L.14
Considering the importance of platelet aggre-gation for local hemostasis, an association between
antiplatelet medications and subacute puncture sitecomplications is not unexpected.14 Combinedplatelet inhibition by acetylsalicylic acid andclopidogrel has been recognized previously as arisk factor for local hemorrhagic complications.15,16
The additional administration of abciximab syn-ergistically attenuates platelet aggregation17 andthus increases the risk for bleeding and pseudo-aneurysms. Patients with combined and aggressiveantiplatelet medications thus have to be consid-ered as high risk for access site complications.
Artificial coagulation disorders, like oral antico-agulation or therapy with low molecular weightheparin, have to be considered important risk fac-tors for access site complications. In these patients,optimization of coagulation prior to punctureshould be anticipated whenever possible. Lowmolecular heparin should be stopped on the dayof the procedure whenever possible.
Sheath size
The size of the arterial or venous sheath is amajor determinant for complications. The largerand the stiffer the sheath, the higher the risk forlocal injury. Routine sheath sizes for trans-femoral arterial access range from 4 to 8 Frenchand have a relatively low risk for arterial injury.Particularly when larger sheaths are used forimplantation of stent grafts, access vessel anat-omy has to be assessed in advance to ensure thatthese large sheaths will pass through the pelvicarteries without troubles.
Location of the puncture site
Retrograde transfemoral access is consideredthe safest approach to endovascular therapies.The antegrade femoral approach has a higherrisk for bleeding and pseudoaneurysm forma-tion. Transradial access is considered the safestapproach with respect to bleeding, however itbears a higher risk for vessel thrombosis. Brachialor axillary puncture has a higher risk of neuro-praxia involving the median nerve or otherbranches of the brachial plexus. With decreas-ing diameter of the punctured vessel, the riskfor dissection and thrombosis increases and has
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 55
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 55

been reported to be as high as 15% for trans-radial access with sheath sizes above 6 French.
Puncture technique
Finally, another most important determinant foraccess site complications is puncture technique.This will be described later in this chapter.
COMPLICATIONS OF SPECIFIC INTERVENTIONAL STEPS AND TOOLS
The most common technique and probably stillthe gold standard for achieving local hemostasisat the arterial puncture site is conventional man-ual compression. Thereafter, prolonged bed restis recommended. Recommendations rangefrom 4 hours after removal of a 4 Frenchsheath, to 6 hours after 5 French sheaths, toovernight bed rest after removal of 6 French orlarger sheaths after interventional procedures.Although safe,18,19 this technique is time con-suming, sometimes painful for the patient,potentially induces vasovagal reflexes with adrop in blood pressure and heart rate, requiresprolonged immobilization and an overnighthospital stay, and thus may have cost implica-tions. Nevertheless, if adequate compressiontimes are ensured,20 the rate of complicationscan be reduced to below 2%. In this context,compression times of at least 15 to 20 and 5minutes after bleeding has stopped have beenrecommended. During manual compression avasovagal reflex may cause bradycardia andhypotension. Blood pressure and heart ratemonitoring is therefore recommended duringremoval of the sheath; fluids and atropine (insteps of 0.5 mg iv) are useful to handle theseadverse events and can be used as a prophylac-tic measure in patients with low blood pressureand/or low heart rate. It has to be acknowl-edged that atropine per se increases only theheart rate but not the blood pressure, thereforehypotension without bradycardia is not ade-quately treated by atropine.
The development of specific closure devicespromised faster time to ambulation, and anincrease in safety and patients’ comfort. Severalstudies addressed the efficacy and safety ofsuture-mediated closure devices compared with
conventional compression;21–27 however, a clinicalbenefit has not as yet been demonstratedunequivocally, 22,28,29 as no large randomized trialreported a reduction of complications. Mostclosure devices have been approved only forretrograde femoral access. Furthermore, closuredevices may introduce complications rather thanavoiding them. Complications associated withclosure devices are acute vessel occlusion, dis-section, and bleeding.
The following case illustrates a complicationinduced by the closure device AngiosealTM (StJude Medical), which was used to close a 10French transfemoral access site after carotidangioplasty with a MoMaTM (Invatec) proximalballoon occlusion system. After the intervention,the patient developed progressive rest pain inthe right foot and lower limb. DuplexTM sonogra-phy of the access site in the right groin revealedan acute occlusion of the superficial femoralartery where the AngiosealTM device was implan-ted and the patient was therefore returned to thecath lab. An angiogram from cross-over revealeda flush occlusion of the superficial femoral artery(Figure 5.6). The occlusion was recanalized andrepeatedly dilated, but the intravascular anchorof the closure device reoccluded the artery imme-diately. Therefore, a 7/20 self-expanding nitinolstent (Smart ControlTM, CordisTM) was implantedat the origin of the SFA (Figure 5.6) and patencywas restored.
METHODS TO DETECT POTENTIAL COMPLICATIONS – WHICH DIAGNOSTICSTEPS ARE NEEDED ROUTINELY TO RULEOUT OR IDENTIFY COMPLICATIONS?
Clinical examination of the vascular access siteafter percutaneous procedures before patientdischarge and identification of subacute compli-cations is becoming increasingly recognized as amatter of the utmost importance.30 For clinicalroutine, duplex sonography is suggested to be the gold standard in the assessment of the vascular access site after arterial puncture.30–33
In this context, color coded duplex ultrasound isvery helpful in visualizing complications likepseudoaneurysms (Figure 5.3) or arteriovenousfistulas (Figure 5.4). Ultrasound can further pre-cisely document the success of complication
56 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 56

management, e.g. by manual or ultrasoundguided compression (Figure 5.7).
The question whether all patients have toundergo duplex sonography, or whether physi-cal examination is reliable to exclude access sitecomplications remains a debated issue. How-ever, recent research14 has indicated that physicalexamination indeed is very reliable in excludingiatrogenic pseudoaneurysms. The presence ofpulsatile groin masses was 100% predictive ofpseudoaneurysms in duplex sonography with-out false positive findings.14 Vascular bruits aresensitive indicators for arteriovenous fistulas.For routine purposes it seems acceptable to relyon physical examination for the postinterventionevaluation of the puncture site and to performconfirmatory ultrasound evaluation only inpatients with pulsatile groin masses, rather thanmandatory duplex ultrasound after all percuta-neous transluminal interventions.
In patients with unexplained back or ab-dominal pain, or hemodynamic deterioration
postintervention, acute bleeding has to be con-sidered as a most important differential diag-nosis. As long as these patients can be initiallystabilized, computed tomography will be the diag-nostic method of choice to assess the site ofbleeding and, in particular, to assess whetheroccult retroperitoneal bleeding is ongoing. Inintractable unstable patients, exploratory surgeryhas to be considered as a primary measure.
Angiography will be the diagnostic method ofchoice when a repeat intervention is planned toresolve an access site complication, e.g. coilingor stent graft implantation. Otherwise, angiog-raphy can be replaced by non-invasive evalua-tion in almost all cases.
ENDOVASCULAR, SURGICAL, AND MEDICALTECHNIQUES TO RESOLVE COMPLICATIONS
The choice of technique to resolve an access sitecomplication mainly depends on the kind andacuity of the complication. The following section
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 57
Acute occlusion of the SFAafter Angioseal closure
After recanalizationand stenting of the SFA origin
Figure 5.6 Acute occlusion of the superficial femoral artery (SFA) after access site closure using the AngiosealTM (St JudeMedical) closure device (left image). The occlusion was recanalized by cross-over balloon angioplasty and implantation ofa 7.0/20 self-expanding nitinol stent (SMART ControlTM, CordisTM) at the origin of the SFA (right image).
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 57

will outline various treatment options for accesssite complications.
Compression
The method of first choice in stable patients withaccess site complications, particularly pseudo-aneurysms, is prolonged manual or ultrasound com-pression. Manual compression over a time periodof 25 to 30 minutes followed by a pressure ban-dage and overnight bed rest has a success rate ofapproximately 60%. This can be improved to80–90% by ultrasound guidance.34–38 In this case,the neck pseudoaneurysm is compressed directlywith the ultrasound transducer over a timeperiod of 25 to 30 minutes, leading to stasis in the sack of the aneurysms and subsequentthrombosis. The procedure is followed by anovernight pressure bandage. Alternatively, acompression device like the FemostopTM device(RADI Medical Systems, Uppsala, Sweden) canbe placed under ultrasound guidance on thepseudoaneurysm; the expected success rate alsoranges around 80%. Although quite effective,ultrasound guided compression is frequentlyextremely painful for the patient, and very timeconsuming for the physician; alternatives aretherefore needed. Complications of ultrasound
guided compression are extremely rare. Casereports describe the rupture of pseudoaneu-rysms during ultrasound guided compressionwhich had to be resolved by surgery. Compre-ssion therapy can also be effective in patientswith arteriovenous fistulas, although the successrate is usually below 50%, mainly dependingon concomitant antiplatelet and anticoagulanttherapy.
Compression therapy is also the treatment ofchoice for persistent bleeding at the access site.Additionally, these patients have to be monitoredwith respect to heart rate and blood pressure.
Vascular surgery
Vascular surgery is traditionally the treatmentof choice when compression has failed, as wellas in all patients with ruptured pseudoaneu-rysms or acute bleeding from the access sitewhich cannot be handled by endovascular pro-cedures.39–42 Furthermore, patients with hemo-dynamically relevant arteriovenous fistulaswhich do not respond to compression therapyfrequently have to undergo surgery. The successrate of surgical procedures approaches 100%,and frequently the operation can be done underlocal anesthesia. In patients with a largehematoma, these clots can be removed, althoughthis approach usually requires general anesthe-sia. Unfortunately, infection, nerve injury, lymphfistulas, and formation of seromas frequentlycomplicate the postoperative course and prolonghospitalization in 15 to 25% of the patients.Surgery is also the treatment of choice for patientswith compartment syndromes, large hematomas,and ongoing (retroperitoneal) bleeding.
Thrombin injection
During the late 1990s, reports described the suc-cessful closure of iatrogenic pseudoaneurysmsby instillation of fibrin and fibrin derivates, andlater on bovine, recombinant, and human throm-bin.43–49 Today, thrombin injection has replacedmost other substances. Technically, the injectionis performed under ultrasound guidance. Ideally,the neck of the pseudoaneurysm is compressedby the ultrasound transducer during injection ofthe procoagulant substance. The success rate of
58 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 5.7 Thrombosed pseudoaneurysm after successfulultrasound guided compression for 20 minutes.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 58

thrombin injection is 95 to 98%. The most seriouscomplication is peripheral embolization of theprocoagulant material in up to 2%. Fortunately,most peripheral emboli are resolved sponta-neously and critical limb ischemia necessitatingthrombolysis or surgery hardly ever develops.43
Both human and bovine thrombin can be usedfor injection in the pseudoaneurysm. The poten-tial disadvantages of bovine thrombin are aller-gic reactions and cross-reactions with factor V ofthe coagulation cascade.50–54 Direct comparisonof human vs bovine thrombin, however, showedno significantly lower complication rate withhuman thrombin, but a significantly higher suc-cess rate with bovine thrombin, suggesting thatthis substance may be preferred.45
We routinely use bovine thrombin in incre-ments of 5000 IU under ultrasound guidance.The following case report demonstrates the util-ity of thrombin infection in a 42-year-old femalepatient. The patient was submitted 12 weeksafter a neuroradiologic intervention due toincreasing swelling of the right groin. Duplexsonography revealed a 50 × 30 × 30 mm pseudo-aneurysm with a short and large caliber neck (3 mm diameter). Systolic peak velocity in theneck was above 4 m/s, suggesting a very highflow within the aneurysm – not an ideal candi-date for thrombin injection (Figure 5.8). Thepatient refused surgical therapy and opted forthrombin injection, despite the higher risk forperipheral emblization in patients with widenecks of the pseudoaneurysm. After disinfectionof the skin, an 18 G needle was advanced undersonographic control and manual compression ofthe common femoral artery until the tip of theneedle was visualized centrally within thepseudoaneurysm. Thereafter, 5000 IU thrombin(D-Stat flowable haemostat™, Vascular Solu-tions, Mn, MI) was slowly injected under sono-graphic control; complete occlusion was achievedafter injection of another 5000 IU of the sub-stance (Figure 5.9). Immediately after thrombininjection, the right lower leg was pale and cold,and the pulse of the arteria dorsalis pedis wasnot palpable, suggesting peripheral emboliza-tion. Since the patient remained asymptomatic,a pressure bandage was applied on the rightgroin and the patient was observed overnight.Two hours after thrombin injection, clinical
signs of ischemia had disappeared and 24 hoursafter the injection ultrasound revealed a regularperfusion of the ipsilateral arteria dorsalis pedis(Figure 5.9), suggesting spontaneous lysis of theembolic material. Ten days after the interven-tion the pseudoaneurysm remained completelyoccluded and the patient was free of symptoms(Figure 5.10).
Alternatively, in patients with wide necks, acombined procedure can help to resolve the prob-lem: by an endovascular cross-over approachthe access site can be sealed by an occlusionballoon (Figure 5.11), under balloon protectionthrombin usually can be safely injected.
Stent implantation
In case of dissection or vessel occlusion at theaccess site, balloon dilation and stent implanta-tion with self-expanding stents can usuallyresolve the problem, as shown in Figure 5.6. Foringuinal complications, either a cross-over accessor a transbrachial access is technically possible;long sheaths are mandatory in these cases.Entering the true lumen sometimes can be chal-lenging, the choice of an adequate wire is mosthelpful in these cases. We prefer a BostonScientificTM 0.018 control wire with flexible tip forthese cases.
Stent graft implantation
This is a relatively novel and still debated optionto treat access site complications. Most accesssites are located in vessel areas with highmechanical stress, like the groin for arterialaccess or the neck for venous interventions. Theformerly available stent grafts were very rigid,and frequently balloon expandable, whichseems not an adequate option for these vesselareas. Today more flexible and self-expandingstent grafts are available, which can be used incertain indications to manage access site com-plications. The initial success rate approaches100%. However, some permanent limitations ofthe use of stent grafts have to be considered:most importantly, the access site cannot be usedfor later interventions after implantation of astent graft. Secondly, stent graft fractures have
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 59
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 59

been reported and may cause late problems.Thirdly, stent graft restenosis occurs in up to50% of the patients, depending on the vesselarea. Therefore, stent grafts should not be con-sidered the treatment of first choice for accesssite complications. The following two cases
briefly describe stent graft implantations formanagement of arterial and venous access sitecomplications.
A 59-year-old male patient was submitted toour cardiology department suffering an acutecoronary syndrome. The patient received aspirin,
60 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 5.8 Duplex sonography of an iatrogenic pseudoaneurysm in the common femoral artery with a central jet (upperimage) and a wide neck (lower image).
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 60

clopidogrel 300 mg loading dose, full dose lowmolecular heparin and abciximab, and under-went urgent coronary angiography. Due to dif-fuse coronary three-vessel disease, endovascular
revascularization was not attempted; the patientcould be stabilized and was scheduled for elec-tive bypass surgery. Two days postintervention,an increasing swelling and enlarging hematoma
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 61
Figure 5.9 Ultrasound B-image immediately after thrombin injection and complete thrombosis of the pseudoaneurysms;the hyperechogenic reflex indicates the site of the thrombin depot (red arrows, upper image). The lower image shows theultrasound Doppler signal of the ipsilateral arteria dorsalis pedis.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 61

in the right groin was detected and ultrasoundconfirmed a large hematoma and diffuse pseu-doaneurysm without a detectable neck. The pa-tient was therefore not considered a candidatefor thrombin injection and the vascular surgeonrefused to operate on the bleeding due to theaggressive anticoagulation regimen. The patientwas therefore brought back to the cath lab andan angiogram was obtained via the contralat-eral approach (Figure 5.12). Thereafter, a 45 cm 9French sheath was placed over the bifurcationvia a stiff 0.035-inch AmplatzTM wire. The samewire was used to guide a self-expanding 6.0/60Fluency StentgraftTM (CR Bard, Inc) to the bleed-ing site and seal the bleeding site (Figure 5.13).The postintervention course was uneventfuland the patient later underwent aortocoronarybypass surgery.
The second case describes the course of a 38-year-old patient who suffered an arteriovenousfistula and subacute bleeding following a venousaccess to the right jugular vein (Figure 5.14). Thepatient was not suitable for surgery due tosevere comorbidities, therefore stent graft repairwas considered. After diagnostic angiographyand confirmation of the bleeding, a long 9 French
62 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 5.10 Duplex sonography 10 days after thrombin injection demonstrates complete occlusion of the pseudoaneurysmand regular patency of the common femoral artery.
Figure 5.11 Balloon occlusion for a femoral iatrogenicpseudoaneurysm – under balloon protection, thrombininjection can be performed even in cases with very wideaneurysm necks to minimize the risk of embolization.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 62

sheath was placed in the common carotid arteryvia a stiff wire (Figure 5.15). Then a FluencyStengraftTM 8.0/30 (CR Bard, Inc) was implantedand the bleeding site and arteriovenous fistulawas sealed successfully (Figure 5.16).
Coil embolization
The reported experience with coil embolizationof access site complications is very limited. Thisoption may be considered, when the neck of thepseudoaneurysm is long enough to safely posi-tion a catheter and place the coils. Nevertheless,there is a substantial risk for dislocation of thecoils, if the neck of the bleeding site is too short
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 63
Figure 5.12 Angiography of a bleeding and diffusepseudoaneurysm of the right groin.
Figure 5.13 Implantation of a 6.0/60 Fluency StentgraftTM
(CR Bard, Inc) to seal an inguinal bleeding site andpseudoaneurysm.
(a)
(b)
Figure 5.14 Duplex ultrasound revealing an arteriovenousfistula between the internal jugular vein and the commoncarotid artery after venous access. a) Sagittal view b) Transverse view.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 63

64 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
45° LAO 45° RAO
Figure 5.15 Angiographic images of the arteriovenous fistula and bleeding of the common carotid artery – a large sheathand guidewire for subsequent stent graft implantation are already in place.
45° LAO 45° RAO
Figure 5.16 Implantation of a covered stent graft (FluencyTM 8.0/40, CR Bard, Inc) to cover the bleeding site in thecommon carotid artery.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 64

and, usually, percutaneous liquid embolizationby thrombin is the method of choice.
METHODS TO AVOID COMPLICATIONS
Preprocedure assessment
In patients without a history of peripheral ar-tery disease, without previous punctures at theplanned access site, and with a regularly palpa-ble pulse no additional preprocedure imagingseems necessary. If there is any doubt on diseaseat the access site, preprocedure ultrasound exami-nation helps to estimate the feasibility and riskfor a puncture. Particularly, when the puncturesite is heavily diseased, the interventionist whowill perform the puncture should perform theultrasound examination to get an idea of poten-tial problems. If ultrasound is not available – e.g.the patient is already in the cath lab – plain fluo-roscopy of the puncture site may visualizeheavy calcifications and identify pre-existentstents nearby the puncture site. Fluoroscopy ofthe puncture site should always be done if pre-vious stent implantation in this area is suspectedor documented. Ultrasound guided puncturescan be used when access is extremely difficult.
Choice of access site
Using the transfemoral puncture, the femoral headshould be located by fluoroscopy before puncture,as the common femoral artery is usually locatedexactly at the level of the femoral head. Externalanatomic structures are relatively unreliable withrespect to locating the common femoral artery.
For access sites other than transfemoral cer-tain premises always have to be considered. Asstated above, the popliteal access is associatedwith a higher rate of arteriovenous fistulas; ultra-sound guided puncture is extremely helpful inthese cases. In patients with planned accessthrough the arteries of the upper extremities twooptions can be considered: transbrachial or tran-sradial access. Transbrachial access has a lower rateof vessel thrombosis (1 to 2%), but in cases whenthrombosis occurs, the clinical consequencescan be deleterious and frequently necessitatesurgery. Transbrachial puncture should be done2 cm proximally to the elbow joint to avoid theradial bifurcation. Transradial access is associated
with a higher rate of vessel thrombosis (5 to 10%),but in patients with patent palmar arc, clinicalconsequences of radial artery thrombosis usuallyremain negligible. If long segment radial arterythrombosis occurs without adequate collateralflow, severe consequences may arise (Figures 5.17and 5.18). Before the radial approach, testing for collateral flow – e.g. by the Allen test – is recommended.
Patient selection and preparation
Bleeding disorders should be corrected before theintervention in all patients undergoing electivetreatment. This includes stopping low molecularweight heparin on the day of the interventionwhenever possible, monitoring the amount ofheparin administered during the procedure byACT measurements, and checking the ACT oractivated partial thromboplastin time (aPTT)before removing the sheath.
Puncture technique and choice of needle
Whenever possible ‘anterior wall puncture’should be performed to avoid bleeding andminimize the extent of vessel injury. One-partneedles (open needles) support anterior wallpuncture, whereas the classical two-part Seldin-ger needle frequently causes puncture throughthe artery and entry to the lumen during back-ward movement of the puncture device. TheSeldinger technique is considered outdated by
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 65
Figure 5.17 Severe skin necrosis after radial access andradial artery thrombosis.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 65

many interventionists and should be avoided inall patients under aggressive anticoagulation orin patients undergoing thrombolysis. Introduc-tion of the wire has to be done cautiously, andhas to be avoided when pulsatile flow is absentor attenuated (particularly if no proximal lesionis suspected). Hydrophilic (glide) wires bear thepotential danger of easily dissecting the vesselrather than entering in the true lumen. We stillfrequently use hydrophilic wires for arterialpunctures, but the interventionist has to beaware of this risk. In case the appropriateness ofthe puncture is in doubt, a small amount ofcontrast should be administered to perform a‘needle angiography’ and assess the puncture siteby angiography. The wire then can be advancedunder fluoroscopic view. Special attention shouldbe brought to the tip of the wire – the tip shouldbe freely moving, otherwise vessel dissectionhas to be considered. A useful test to reassuretrue lumen entry with the wire is to advance thewire to the first bifurcation: if the wire followsthe expected course of the bifurcating vesseltrue lumen access is almost guaranteed; in caseswith subintimal entry, the wire will get stuckat the first bifurcation. It seems essential to reas-sure true lumen entry with the wire before thesheath is inserted.
During the intervention
Regularly aspirating and flushing the sheathand adequate anticoagulation help to reduce therisk for thrombosis. For aspiration maneuversonly sheaths with removable hemostatic valvesshould be used as clots frequently get stuck inthe sheath at the level of the hemostatic valve. Ifin doubt, when aspiration through the sheath isnot possible, the sheath should be exchangedrather than flushed to avoid embolization.
Removing the sheath and access site closure
If closure devices with anchor (AngiosealTM, St Jude MedicalTM), clip (StarcloseTM, AbbottVascularTM), or needle (Perclose) systems areplanned, a final angiogram of the access siteshould be obtained to assess whether collaterals(e.g. deep femoral artery) are involved in theaccess route and to assess the diameter of thepunctured artery. Most currently available clo-sure devices are approved only for retrogradefemoral access and are not recommended for avessel diameter below 4.5 mm. Personally, weavoid the use of closure devices in locationsother than the common femoral artery, as weexperienced serious adverse events with differ-ent closure devices in the superficial femoral
66 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 5.18 Doppler flow profiles in a patient with occluded radial artery after radial access.
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 66

artery and the brachial artery. Furthermore, ifthe access site shows heavy calcification, closuredevices frequently do not work properly. Inthese cases manual compression or compressionwith external devices like the Femostop com-pression device is recommended. Timing forremoving the sheath for manual compressiondepends on the size of the sheath and theamount and kind of anticoagulation. Withsheath sizes up to 6 French, immediate removalseems safe with any kind of anticoagulation. Iflarger sheaths are in place, the effect of anticoag-ulation (heparin, bivalirudin) should be mini-mized until the sheath is removed – for heparinthis can be checked by the ACT or aPTT.
Control of blood pressure
Before removing the sheath, blood pressureshould be checked – and lowered if elevated.Personally, we prefer systolic blood pressuresat maximum 140 mm when the sheath isremoved.
Pressure bandage and bed rest
There are no uniform recommendations for bedrest and pressure bandages and no scientific evi-dence for their use. We routinely apply pro-longed pressure bandages in all patients aftermanual compression of the access site, and evenin patients who received a closure device, a short-term pressure bandage (4 hours) seems useful.After manual compression we recommend 4hours of bed rest for a 4 French sheath, 6 hours for5 French, and overnight bed rest for 6 French orlarger. All patients with closure devices have abed rest of 4 hours at our institution.
Postintervention care
The access site should be checked regularly dur-ing the first few hours postintervention by atrained nurse or physician, particularly beforefirst ambulation. First ambulation should bedone under surveillance. Before discharge theaccess site again has to be checked by a trainedphysician – we recommend that the interven-tionist personally checks the access site beforeambulation.
SUMMARY
Access site complications are the most frequentcomplications encountered after percutaneousprocedures. Occurrence of these complicationscan be a severe burden for the patient and thehealthcare system and can extinguish the advan-tage of a minimally invasive endovascularapproach. Several risk factors for access sitecomplications are known and high-risk patientscan be identified preprocedure. Adequate punc-ture technique and thorough postprocedureaccess site management can minimize the fre-quency of these complications. Several methodsto handle access site complications are availableand the interventionist has to be familiar withthese techniques.
CHECK LIST FOR EMERGENCY EQUIPMENT
• thrombin, e.g. (D-Stat flowable haemostatTM,Vascular Solutions, Mn, MI)
• occlusion balloons 4 to 10 mm depending onthe size of the access vessel
• self-expanding bare metal nitinol stents fortreatment of dissections and occlusions
• self-expanding stent graft, e.g. Fluency stentgraft (CR Bard), Wallgraft (Boston Scientific),or Viabahn (Gore) in adequate sizes to fit theaccess vessel
• pushable coils• ultrasound machine with duplex mode• CT facility for emergency imaging of retro-
peritoneal bleeding.
REFERENCES
1. Dangas G, Mehran R, Kokolis S et al. Vascular compli-cations after percutaneous coronary interventions fol-lowing hemostasis with manual compression versusarteriotomy closure devices. J Am Coll Cardiol 2001; 38:638–41.
2. Muller DW, Shamir KJ, Ellis SG et al. Peripheral vascularcomplications after conventional and complex percuta-neous coronary interventional procedures. Am J Cardiol1992; 69: 63–8.
3. Wyman RM, Safian RD, Portway V et al. Current com-plications of diagnostic and therapeutic cardiac cathe-terization. J Am Coll Cardiol 1988; 12: 1400–6.
4. Popma JJ, Satler LF, Pichard AD et al. Vascular compli-cations after balloon and new device angioplasty.Circulation 1993; 88: 1569–78.
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 67
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 67

5. Waksman R, King SB 3rd, Douglas JS et al. Predictorsof groin complications after balloon and new-devicecoronary intervention. Am J Cardiol 1995; 75: 886–9.
6. Omoigui NA, Califf RM, Pieper K et al. Peripheral vas-cular complications in the Coronary AngioplastyVersus Excisional Atherectomy Trial (CAVEAT-I). J AmColl Cardiol 1995; 26: 922–30.
7. Tcheng JE. Clinical challenges of platelet glycoproteinIIb/IIIa receptor inhibitor therapy: bleeding, reversal,thrombocytopenia and retreatment. Am Heart J 2000;139: S38–45.
8. Wasson JH, Sox HC, Neff RK et al. Clinical predictionrules. Applications and methological standards. N EnglJ Med 1985; 313: 793–9.
9. Popma JJ, Satler LF, Pichard AD et al. Vascular compli-cations after balloon and new device angioplasty.Circulation 1993; 88: 1569–78.
10. Davis C, Vanriper S, Longstreet J et al. Vascular compli-cations of coronary interventions. Heart Lung 1997; 26:118–27.
11. Hirano Y, Ikuta S, Uehara H et al. Diagnosis of vascularcomplications at the puncture site after cardiac cathe-terization. J Cardiol 2004; 43: 259–65.
12. Singh H, Cardella JF, Cole PE et al. Quality improve-ment guidelines for diagnostic arteriography. J VascInterv Radiol 2003; 14: S283–8.
13. Pentecost MJ, Criqui MH, Dorros G et al. Guidelines forperipheral percutaneous transluminal angioplasty ofthe abdominal aorta and lower extremity vessels. J VascInterv Radiol 2003; 14: S495–515.
14. Mlekusch W, Haumer M, Mlekusch I et al. Predictionof iatrogenic pseudoaneurysm after percutaneousendovascular procedures. Radiology 2006; 240:597–602.
15. Chu MWA, Wilson SR, Novick RJ et al. Does clopido-grel increase blood loss following coronary arterybypass surgery. Ann Thorac Surg 2004; 78: 1536–41.
16. Brener SJ, Moliterno DJ, Lincoff M et al. Relationshipbetween activated clotting time and ischemic or hemor-rhagic complications. Circulation 2004; 110: 994–8.
17. Scazziota A, Altman R, Rouvier J et al. Abciximabtreatment in vitro after aspirin treatment in vivo hasadditive effects on platelet aggregation, ATP releaseand P-selectin expression. Thromb Res 2000; 100:479–88.
18. Thore V, Berder V, Huplon P et al. Role of manual com-pression time and bed rest duration on the occurrenceof femoral bleeding complications after sheath retrievalfollowing 4Fr left-sided cardiac catheterization. J IntervCardiol 2001; 14: 7–10.
19. Simon A, Bumgarner B, Clark K et al. Manual versusmechanical compression for femoral artery hemostasisafter cardiac catheterization. Am J Crit Care 1998; 7:308–13.
20. Katzenschlager R, Uguruoglu A, Ahmadi A et al.Incidence of pseudoaneurysm after diagnostic and thera-peutic angiography. Radiology 1995; 195: 463–6.
21. Chevalier B, Lancelin B, Koning R et al. Effect of a clo-sure device on complication rates in high-local-riskpatients: results of a randomized multicenter trial. CathCardiovasc Interv 2003; 58: 285–91.
22. Rickli H, Unterweger M, Sutsch G et al. Comparison ofcosts and safety of a suture-mediated closure devicewith conventional manual compression after coronaryartery interventions. Cath Cardiovasc Interv 2002; 57:297–302.
23. Wetter DR, Rickli H, von Smekal A et al. Early sheathremoval after coronary artery interventions with use ofa suture-mediated closure device: clinical outcome andresults of Doppler US evaluation. J Vasc Interv Radiol2000; 11: 1033–7.
24. Kornowski R, Brandes S, Teplitsky I et al. Safety andefficacy of a 6 French Perclose arterial suturing devicefollowing percutaneous coronary interventions: a pilotevaluation. J Invas Cardiol 2002; 14: 741–5.
25. Meyerson SL, Feldman T, Desai TR et al. Angiographicaccess site complications in the era of arterial closuredevices. Vasc Endovasc Surg 2002; 36: 137–44.
26. Lewis-Carey MB, Kee ST. Complications of arterial clo-sure devices. Tech Vasc Interv Radiol 2003; 6: 103–6.
27. Wagner SC, Gonsalves CF, Eschelman DJ et al.Complications of a percutaneous suture-mediated clo-sure device versus manual compression for arteri-otomy closure: a case controlled study. J Vasc IntervRadiol 2003; 14: 735–41.
28. Carey D, Martin JR, Moore CA et al. Complications offemoral artery closure devices. Cath Cardiovasc Interv2001; 52: 3–8.
29. Kussmaul WG, Buchbinder M, Whitlow PL et al. Rapidarterial hemostasis and decreased access site complica-tions after cardiac catheterization and angioplasty:results of a randomized trial of a novel hemostaticdevice. J Am Coll Cardiol 1995; 25: 1685–92.
30. Hirano Y, Ikuta S, Uehara H et al. Diagnosis of vascularcomplications at the puncture site after cardiac cathe-terization. J Cardiol 2004; 43: 259–65.
31. Helvie MA, Rubin JM, Silver TM et al. The distinctionbetween femoral pseudoaneurysms and other causes ofgroin masses: value of duplex Doppler sonography.Am J Roentgenol 1988; 150: 1177–80.
32. Sheik KG, Adams DB, McCann R et al. Utility ofDoppler color flow imaging for identification of femoralarterial complications of cardiac catheterisation. AmHeart J 1989; 117: 623–8.
33. Paulson EK, Kliewer MA, Hertzberg BS et al. ColorDoppler sonography of groin complications followingfemoral artery catheterization. Am J Roentgenol 1995;165: 439–44.
68 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 68

34. Cox GS, Young JR, Gray BR et al. Ultrasound-guidedcompression repair of postcatheterization pseudo-aneurysms: result of treatment in one hundred cases. J Vasc Surg 1994; 19: 683–6.
35. Mooney MJ, Tollefson DF, Andersen CA et al. Duplex-guided compression of iatrogenic pseudoaneurysms. J Am Coll Surg 1995; 181: 155–9.
36. Khoury M, Batras S, Berg R et al. Duplex-guided com-pression of iatrogenic femoral artery pseudoaneurysms.Am J Surg 1994; 60: 234–7.
37. Dorfman GS, Cronan JJ. Postcatheterization femoralartery injuries: is there a role for nonsurgical treatment.Radiology 1991; 178: 629–30.
38. Ugurluoglu A, Katzenschlager R, Ahmadi R et al.Ultrasound guided compression therapy in 134 patientswith iatrogenic pseudo-aneurysms: advantage of routineduplex ultrasound control of the puncture site follow-ing transfemoral catheterization. VASA 1997; 26: 110–16.
39. Lumsden AB, Miller JM, Kosinski AS et al. A prospec-tive evaluation surgically treated groin complicationsfollowing percutaneous cardiac procedures. Am Surg1994; 60: 132–7.
40. Perler BA. Surgical treatment of femoral pseudo-aneurysm following cardiac catheterization. Cardio-vasc Surg 1993; 1: 118–21.
41. Messina LM, Brothers TE, Wakefield TW et al. Clinicalcharacteristics and surgical mangement of vascularcomplications in patients undergoing cardiac catheter-ization: interventional versus diagnostic procedures. J Vasc Surg 1991; 13: 593–600.
42. Lin PH, Dodson TF, Bush RL et al. Surgical interventionfor complications caused by femoral artery catheteriza-tion in pediatric patients. J Vasc Surg 2001; 34: 1071–8.
43. Paulson EK, Nelson RC, Mayes CE et al. Sonogra-phically guided thrombin injection of iatrogenicfemoral pseudoaneurysms: further experience of asingle institution. Am J Roentgenol 2001; 177: 309–16.
44. Paulson EK, Sheafor DH, Kliewer MA et al. Treatmentof iatrogenic femoral arterial pseudoaneurysms:
comparison of US-guided thrombin injection withcompression repair. Radiology 2000; 215: 403–8.
45. Vazquez V, Reus M, Pinero A et al. Human thrombinfor treatment of pseudoaneurysms: comparison ofbovine and human thrombin sonogram-guided injec-tion. Am J Roentgenol 2005; 184: 1665–71.
46. Kang SS, Labropoulos N, Mansour MA et al. Expandedindications for ultrasound-guided thrombin injectionof pseudoaneurysms. J Vasc Surg 2000; 31: 289–98.
47. Kang SS, Labropoulos N, Mansour MA et al. Percu-taneous ultrasound guided thrombin injection: a newmethod for treating postcatheterization femoral pseudo-aneurysms. J Vasc Surg 1998; 27: 1032–8.
48. Brophy DP, Sheiman RG, Amatulle P et al. Iatrogenicfemoral pseudoaneurysm: thrombin injection afterfailed US-guided compression. Radiology 2000; 214:278–82.
49. La Perna L, Olin JW, Goines D et al. Ultrasound-guided thrombin injection for the treatment of post-catheterization pseudoaneurysms. Circulation 2000;102: 2391–5.
50. Grewe PH, Muegge A, Germing A et al. Occlusion ofpseudoaneurysms using hunan or bovine thrombinusing contrast-enhanced ultrasound guidance. Am J Cardiol 2004; 93: 1540–2.
51. Krueger K, Zaehringer M, Strohe D et al. Post-catheterization pseudoaneurysm: result of US-guidedpercutaneous thrombin injection in 240 patients.Radiology 2005; 236: 1104–10.
52. Pope M, Johnston KW. Anaphylaxis after thrombininjection of a femoral pseudoaneurysm: recommenda-tions for prevention. J Vasc Surg 2000; 32: 190–1.
53. Spotnitz WD. Fibrin sealant in the United States: clini-cal use at the University of Virginia. Thromb Haemost1995; 74: 482–5.
54. Sheldon PJ, Oglivie SB, Kaplan LA. Prolonged general-ized urticarial reaction after percutaneous thrombininjection for treatment of a femoral artery pseudo-aneurysm. J Vasc Interv Radiol 2000; 11: 759–61.
ARTERIAL AND VENOUS ACCESS SITE COMPLICATIONS 69
CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 69

CPVI_Chapter05.qxp 4/5/2007 2:42 PM Page 70

INTRODUCTION TO FREQUENCY AND TYPEOF COMPLICATION WITH ANTIPLATELET,ANTITHROMBOTIC, AND ANTICOAGULANTAGENTS
In recent years a dramatic increase in the num-ber of percutaneous transluminal interventionshas occurred. As a result of technologic advancesand the increasing number of training centers,catheter-based interventions are performed inmore extensively diseased arterial segmentsthan has been carried out in the past. As vesselwall injury is the unavoidable consequence ofendovascular treatment, more complex inter-ventions go along with an increased thromboticrisk.1 Today, it is the supplementary aggressivemedical therapy (Table 6a.1) that provides goodclinical patency even in complex peripheralinterventions, but at the cost of bleeding events. The following review gives the reader an overview on current guidelines, opinions,and possible complications due to antiplatelet,antithrombotic, and anticoagulant agents andtheir management.
Antiplatelet and antithrombotic agents
Acetylsalicylic acid (aspirin) exerts its majorantithrombotic effect by irreversibly acetylatingplatelet cyclo-oxygenase-1, thereby inhibitingprostanoid biosynthesis.2 Peak plasma levelsoccur 30 to 40 minutes after aspirin ingestionand the virtually complete inhibition of plateletfunction is evident by 1 hour. As 10% of the cir-culating platelets are replaced each day, 5 to 6days following aspirin ingestion will be neededfor approximately 50% normal platelet function.
The role of aspirin to prevent cardiovascularevents has been shown in numerous large-scaletrials.3,4 In addition, aspirin reduces the risk ofvascular graft or arterial occlusion by about40%.5,6 The dose of aspirin has been the subject ofsome debate, with 75–325 mg once a day shownto be efficient.3,7 Larger doses have no apparentadditional benefit, but increase the relative riskof upper gastrointestinal bleeding by 5.6% forplain aspirin, and 7% for buffered aspirin.8 Otheradverse effects such as gastrointestinal discom-fort (1.22%), rash (0.10%), diarrhea (0.11%), or
6a
Complications of pharmacologic interventions: antiplatelet, antithrombotic,and anticoagulant agentsHong H Keo and Iris Baumgartner
Introduction to frequency and type of complication with antiplatelet, antithrombotic, and anticoagulantagents • Factors identifying patients at risk for bleeding complications • Bleeding complications ofspecific interventional steps and tools • Methods to detect potential complications – which diagnosticsteps are needed routinely to rule out or identify complications • Endovascular, surgical, or medicaltechniques to resolve complications • Methods to avoid complications • Summary • Check list foremergency equipment
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 71

intracranial hemorrhage (0.47%) are rather rare.4
Aspirin resistance has been reported to vary from5 to 57% based on a large variety of measurementtechniques.9,10 Until further data are forthcoming,we do not recommend laboratory testing forpatients with aspirin resistance nor do we recom-mend the use of alternative agents. Similar con-clusions have been reached by the WorkingGroup on Aspirin Resistance.11
A minority of patients are unable to tolerateaspirin because of allergic reactions and hyper-sensitivity, which can be clinically manifest asrespiratory tract disease (rhinitis and asthma, 10%)or urticaria/angioedema (0.07 to 0.2%).12 We dorecommend the use of alternative agents such asclopidogrel if appropriate.
Clopidogrel is an effective antithrombotic agentthat blocks the activation of platelets by irre-versible binding to the adenosine diphosphate(ADP) receptors. This, in turn, prevents ADP-dependent activation of the glycoprotein IIb/IIIa(GP IIb/IIIa) complex, the primary platelet recep-tor for fibrinogen, and von Willebrand factor,the final common pathway in platelet aggrega-tion.13 Clopidogrel given 75 mg daily inhibitsplatelet aggregation by 25 to 30% on the secondday of ingestion, and reaches steady state (50 to60% inhibition) after 4 to 7 days. A loading dose
of 300 to 600 mg accelerates its activity and isrecommended if an urgent endovascular inter-vention is planned and the patient was not onaspirin or clopidogrel before. In the CAPRIE trial,13
the efficacy of 75 mg of clopidogrel daily wascompared to aspirin 325 mg for secondary pre-vention of atherothrombotic events. Clopidogrelwas marginally more effective than aspirin andresulted in a moderately lower rate of gastroin-testinal bleeding (0.5% vs 0.7%). Due to highcosts its prescription is still limited to patientsintolerant to aspirin, or after coronary stenting,acute coronary syndrome, and cerebrovascularinsult with additional risk factors.4,14,15 To date,no data exist to support the routine use of clopi-dogrel or aspirin plus clopidogrel in patients withperipheral arterial disease (PAD) undergoingperipheral endovascular interventions, althoughthe majority of interventionalists advocate clopi-dogrel on top of aspirin for at least for 28 days.14,16
Life-threatening bleeding was shown to beincreased when comparing single (aspirin orclopidogrel) antiplatelet with dual (aspirin plusclopidogrel) antiplatelet therapy given forlonger terms (CURE14 1.8% vs 2.2%, MATCH15
1.3% vs 2.6%); whether this is clinically relevantfor short-term therapy after peripheral endovas-cular interventions is uncertain (it probably is not).
72 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 6a.1 Antiplatelet, antithrombotic, and anticoagulant agents commonly used
Generic name Trade name™
Switzerland USA Germany Austria
Acetylsalicylic acid Aspirin Aspirin Aspirin Aspirin Tiatral ASS-ISIS Thrombo ASThrombace Herz ASSAspegic
Clopidogrel Plavix Plavix Plavix PlavixIscover Iscover
Abxicimab Reopro Reopro Reopro ReoproTirofiban Aggrastat Aggrastat Aggrastat AggrastatEptifibatid Integrilin Integrelin Integrilin IntegrilinUnfractionated heparin Liquemin Heparin Liquemin HeparinWarfarin Coumadin CoumadinPhenprocoumon Marcoumar Marcoumar MarcoumarAcenocoumarol Sintrom Sintrom Lepirudin Refludan Refludan Refludan RefludanBivalirudin Not available Angiomax Angiox AngioxArgatroban Not available Acova Not available Argatra
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 72

A history of gastrointestinal bleeding is associ-ated with the highest risk of recurrent bleed-ing. In a recent study 320 patients with a historyof gastrointestinal bleeding were randomizedto receive 75 mg clopidogrel daily or 80 mg ofaspirin plus esomeprazole at a dose of 20 mgdaily. The bleeding rate was 8.6% (96% CI, 4.1 to13.1%) versus 0.7% (95% CI, 0 to 2.0%, p = 0.001),underlining the need to combine aspirin aswell as clopidogrel therapy with proton pumpinhibitors to avoid serious bleeding complica-tions.17 Clopidogrel non-responders have beenreported to vary between 25 and 30%, of whichthe clinical relevance has not been adequatelyestablished.
Intravenous platelet GP IIb/IIIa receptor inhibitorshave shown convincing clinical efficacy in per-cutaneous coronary interventions (PCIs), unsta-ble angina/non-Q-wave myocardial infarction,and in combination with thrombolytics inmyocardial infarction. Indication for ‘off-label’ usein peripheral interventions is more restricted,because its application has to be balanced againstbleeding complications and high costs. At pre-sent, its adjunctive use during peripheral endo-vascular interventions is justified in patientsbeing at risk of early re-occlusion, i.e. subacuteor long-segment arterial occlusions, poor run-off,residual intraluminal thrombus, or profounddistal embolization.18
Abciximab, a monoclonal antibody that inhibitsthe binding of fibrinogen to platelet GP IIb/IIIareceptors, is the most widely studied of the GPIIb/IIIa inhibitors. A bolus of 0.25 mg/kg wasfound to result in approximately 80% receptorblockade, needed to be clinically efficient. Gradualrecovery of platelet function occurs over time,with bleeding times returning to near-normal val-ues by 12 hours. A large-sized randomized clinicaltrial (RIO trial) to test the safety and efficacy ofthe adjunctive use of abciximab (0.25 mg/kgbolus, followed by infusion of 0.125 �g/kg/minfor 12 hours) during endovascular revasculariza-tion of long-segment femoro-popliteal occlusionsis underway. Bleeding and thrombocytopeniarepresent the most frequent serious adverseeffects of abciximab treatment. In a randomizedstudy performed at our center, all bleeding com-plications associated with abciximab were limitedto the access site (abciximab vs placebo; OR 2.9,
95% CI 1.04 to 8.2, p = 0.04). None of thepatients had to be treated by red blood cell sub-stitution or surgery, nor needed intensive care.There was a non-significant trend for more localbleedings in patients with additional heparininfusion after the procedure (OR 1.51, 95% CI0.44 to 5.24), and more bleeding with higher age,female sex, increased creatinine, and larger sizeof sheath.18
A significant increase in major bleeding inpatients treated with abciximab and concomi-tant heparin was also described in the EPIC trial.19
A reduction in concomitant heparin dosage (70 U/kg with the introduction of an arterialsheath; followed by infusion up to a maximumof 7 U/kg/hour), and more rapid sheath removalgreatly reduces bleeding owing to abciximab.Thrombocytopenia with a platelet count <50 000cells/�L is reported to vary between 1 and 2% ofcases treated.20 In almost all cases, thrombocy-topenia can be resolved by withdrawing theoffending drug and, if necessary, by platelettransfusion. Spontaneous recovery occurs within5 to 7 days.19,21
Results of a randomized clinical pilot trial(PROMPT) on intra-arterial pulse-spray infu-sion thrombolysis using urokinase in combina-tion with abciximab or placebo were presentedby Duda, Tepe, and colleagues.22,23 There were 70patients with acute or sub-acute non-limb–threat-ening ischemia enrolled in the study. Resultsshowed a 9% amputation rate in patients treatedin combination with abciximab vs 22% in patientstreated with placebo, whereas non-invasive arte-rial measurements (i.e. ankle–brachial index)were comparable in both groups. The dose ofurokinase and time required for vessel reopeningwere lower in patients treated in combinationwith abciximab. However, the non-fatal majorbleeding rate was 8% in the urokinase plusabciximab arm.22
Anticoagulant agents
Unfractionated heparin (UFH) is traditionallyadministered during endovascular interventionsto prevent expansion of thrombi, embolization,and new thrombus formation. Heparin com-plexes with endogenous antithrombin III andinactivates coagulation factors IIa, IXa, Xa, XIa,
PHARMACOLOGICAL INTERVENTION 73
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 73

and XIIa, but it does not resolve already existingthrombus, thus limiting its efficiency. The half-lifeof heparin is approximately 60 minutes dependingon the dose administered, and is prolonged inpatients with renal or hepatic dysfunction. Despitewidespread use, there are no solid recommenda-tions regarding dosing of heparin, as no random-ized study has established the beneficial role ofany antithrombotic agent during peripheral endo-vascular interventions. With this uncertainty inmind, heparin is commonly administered as abolus of 50 to 100 IU/kg following vascular access,supplemented by 25 to 50 IU/kg every 60 to 90 minutes or adjusted based on ACT measure-ments until the procedure is finished.24 Heparinin combination with GP IIb/IIIa inhibitorsincreases the risk of major bleeding up to 14%and minor bleeding up to 7.4%, respectively.19,25
In addition to its well-known bleeding com-plications, heparin may induce immune-mediatedplatelet activation leading to heparin-inducedthrombocytopenia with more than 5 days oftreatment, a condition that is rare but potentiallyfatal if not recognized in the early state.
Low molecular weight heparins (LMWH) arederived from UFH by chemical and enzy-matic depolymerization and, like heparin, exerttheir major anticoagulant effects by activatingantithrombin. LMWH has reduced antifactor IIaactivity relative to antifactor Xa activity. It has amore favorable benefit/risk ratio and superiorpharmacokinetic properties compared to UFH.There are no firm clinical data reporting a significant effect on overall mortality or cardio-vascular events for LMWH in patients withintermittent claudication and no convincing dataexist for their routine use in peripheral endovas-cular interventions. We prefer the use of UFHduring peripheral interventions. Advantages ofUFH over LMWH are two-fold: firstly the possi-bility to adapt the dose in severe renal insuffi-ciency, and secondly the possibility to neutralizethe antithrombin activity by protamine in caseof severe bleeding complications.
Oral anticoagulation: there are no firm clinicaldata reporting a significant effect on overallmortality or cardiovascular events of vitamin Kantagonists in patients with intermittent claudi-cation. Therefore, there is no firm indication fororal anticoagulation in PAD as the complexity of
management and bleeding risks seem to far out-weigh the benefits, unless the patient has otherconcomitant diseases needing anticoagulationsuch as atrial fibrillation.
Direct thrombin inhibitors: in contrast to heparin,which blocks thrombin generation indirectly,thrombin inhibitors directly bind to thrombinand block the interaction with its substrate fib-rinogen. Direct thrombin inhibitors are increas-ingly used with encouraging success rates.
• Hirudin inhibits thrombin by irreversiblebinding to two sites of the thrombin molecule;no specific antidote exists. Hirudin is clearedby the kidney and should not be used inpatients with renal failure. The TIMI 9B trial26
in the coronary settings compared hirudin(0.1 mg/kg bolus, followed by infusion of0.1 mg/kg per hour) to heparin as an adjunctto thrombolytic therapy and reported hirudinto be at least as effective as heparin. Majorhemorrhage was similar in the heparin (5.3%)and hirudin (4.6%) groups; intracranial hem-orrhage occurred in 0.9% of heparin and 0.4%of hirudin treated patients, respectively.
• Lepirudin, a recombinant derivative of hirudin,is the prototype of a direct thrombin inhibitor.The dose for patients with normal renal func-tion is a bolus of 0.4 mg/kg followed by infu-sion at 0.15 mg/kg per hour. The effect ismonitored by measurement of the activatedpartial thromboplastin time (aPTT). Lepirudinis safe and effective for patients withheparin-associated antiplatelet antibodies.27
• Bivalirudin is a synthetic polypeptide, ananalog of hirudin, which binds to the activesite of thrombin. Its plasma half-life is 25minutes after intravenous injection and onlya fraction is excreted via the kidneys. Potentialbenefits of bivalirudin over heparin includereduced periprocedural thrombosis, morereliable anticoagulation with a reduced needfor activated clotting time measurements, andfewer bleeding complications.28 It was demon-strated to be superior to heparin in reducingischemic events in the REPLACE-2 trial.29
Except for observational results reported bysingle centers, no evidence exists for the useof bivalirudin in peripheral endovascularinterventions.
74 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 74

• Argatroban is a synthetic direct thrombininhibitor with activity against free and clot-bound thrombin. Standard dosing for heparin-induced thrombocytopenia is 2 �g/kg perminute intravenously titrated to achieve anaPTT 1.5 to 3 times control.30 In the settings ofheparin-induced thrombocytopenia patientsundergoing PCI, argatroban has been usedat a dose of 25 mg/kg per minute followinga 350 mg/kg bolus. The maintenance dose istitrated to achieve an activated clotting timeof 250–300 seconds, with results comparableto historic heparin controls.31 Despite multi-ple studies reporting the usefulness ofdirect thrombin inhibitors in the coronarycirculation, its use in peripheral vascularinterventions has not been well established.Extrapolation of data from PCI to the peri-pheral interventional field is difficult. Moretrials specifically looking at interventions inthe periphery are clearly warranted.
FACTORS IDENTIFYING PATIENTS AT RISKFOR BLEEDING COMPLICATIONS
Contraindication for pharmacologic therapy isbased on medical conditions thought to increasethe risk of local and systemic bleeding. General
attention must be paid to patient-related risk fac-tors, which identify them for increased bleedingcomplications, such as higher age, female sex,increased creatinine, larger size of sheaths, and ahigher dose or a combination of antiplateletsand anticoagulants. A history of gastrointestinalbleeding is associated with the highest risk ofrecurrent bleeding. Absolute and relative con-traindications of intravenous thrombolysis asdefined by the National Institute of Health32
were also adopted for off-label use of platelet GPIIb/IIIa receptor inhibitors (Table 6a.2).33 Accordingto clinical experience and recommended caveats,the list of relative contraindications should becompleted by severe renal failure (serum crea-tinine > 2.5 mg/dl), genitourinary bleeding ofclinical significance within the previous 6 weeks,a history of bleeding diathesis a platelet count < 100 000/mm3, arteriovenous malformations oraneurysms, vasculitis, and contraindications orknown allergic reactions to GP IIb/IIIa inhibitors.
BLEEDING COMPLICATIONS OF SPECIFICINTERVENTIONAL STEPS AND TOOLS
Major differences in pharmacotherapy-associatedcomplications in different vessel areas have beenobserved. Pharmacotherapy-associated bleeding
PHARMACOLOGICAL INTERVENTION 75
Table 6a.2 Contraindication for thrombolysis and GP IIb/IIIa inhibitors
AAbbssoolluuttee ccoonnttrraaiinnddiiccaattiioonnssActive clinically significant bleedingIntracranial hemorrhagePresence or development of compartment syndrome
RReellaattiivvee ccoonnttrraaiinnddiiccaattiioonnssCardiopulmonary resuscitation within the past 10 daysMajor non-vascular surgery or trauma within the past 10 daysUncontrolled hypertension (systolic >180 mmHg or diastolic >100 mmHg)Puncture of non-compressible vesselIntracranial tumorRecent eye surgeryNeurosurgery (intracranial, spinal) within the past 3 monthsIntracranial trauma within 3 monthsRecent gastrointestinal bleeding within the past 10 daysEstablished cerebrovascular event (including transient ischemic attacks) within the past 2 monthsRecent internal or non-compressible hemorrhageHepatic failureBacterial endocarditisPregnancy and immediate postpartum statusDiabetic hemorrhagic retinopathyLife expectancy <1 year
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 75

in abdomino-pelvic arteries may be life-threat-ening and warrants urgent diagnostic work-upwith angiography or computer tomography.Bleeding in peripheral arteries of the limb can bediagnosed by ultrasound, or by angiographyfor confirming the diagnosis and concomitanttherapeutic intervention.
METHODS TO DETECT POTENTIAL COMPLICATIONS – WHICH DIAGNOSTICSTEPS ARE NEEDED ROUTINELY TO RULE OUT OR IDENTIFY COMPLICATIONS
Crucial in reducing the risk of bleeding is to rec-ognize risk factors and to reconsider indicationsbefore administration of antiplatelets, anticoag-ulants, or their combination. Most risk factorscan be noted from the patient history. Baselinelaboratory assessment emphasizing the plasmacoagulation system, hematologic parameters, andrenal function is clearly needed prior to each intra-arterial intervention. In cases with a suspicion ofhepatic dysfunction, liver enzymes should beassessed. Ultrasound and Doppler analysis mayprovide additional information about the targetlesion and the access site. In cases where ultra-sound cannot be performed (e.g. adipositas, mul-tilevel arterial disease) diagnostic angiographyor MR angiography should be performed firstin order to plan the definitive intervention, thusminimizing periprocedural complications.
When abciximab is administered, plateletsneed to be followed at 4 and 12 to 24 hours afterthe intervention in order to recognize throm-bocytopenia during maintenance infusion of the drug.
To minimize bleeding complications withtherapeutic doses of heparin the aPTT is moni-tored. The aPTT should be measured approxi-mately 6 hours after the bolus dose of heparin,and the start of maintenance infusion, whichshould be adjusted according to the result.
ENDOVASCULAR, SURGICAL, OR MEDICALTECHNIQUES TO RESOLVE COMPLICATIONS
When clinically relevant bleeding of the vesselarea is suspected, diagnostic work-up should beperformed, according to the urgency of the situ-ation, to identify the bleeding site and potential
appropriate ways to treat the underlying cause.Contrast-enhanced computer tomography orangiography is the diagnostic tool of choice.Discontinuation of antiplatelet agents and anti-coagulation drugs has to be assessed accordingto the condition of the patient and the severity ofbleeding.
Duplex ultrasound has a high sensitivity andspecificity in detecting a false aneurysm (pseudo-aneurysm) at the access site,34 and specific treatment,
76 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 6a.1 Clinical finding of a huge pseudoaneurysm in a patient after left-sided access for endovascularintervention (oral anticoagulation, INR 3).
Figure 6a.2 Angiographic documentation of the pseudoaneurysm emerging from the deep femoral artery.
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 76

Table 6a.3 Recommended dose of commonly used antiplatelet, antithrombotic, and anticoagulantagents
Generic name Dosage Plasma half-life
Acetylsalicylic acid 75 to 325 mg daily; we recommend 100 mg daily for 2 to 3 hoursPAD – higher doses do not provide more benefit, but are associated with higher bleeding complications14
Clopidogrel Loading dose 300 mg; maintenance dose 75 mg daily 8 hours
Abciximab 0.25 mg/kg bolus, followed by maintenance infusion of 10 to 30 min0.125 �g/kg/min for 12 hours
Unfractionated heparin 50 to 100 IU/kg bolus with vascular access, followed Dose-dependentby 25 to 50 IU/kg every 60 to 90 min or adjusted 1 hour (100 IU/kg)according to ACT until the procedure is finished 2.5 hours (400 IU/kg)
i.e. ultrasound-guided compression or, in carefullyselected patients, ultrasound guided thrombininjection, can be initiated.35 Ultrasound-guidedthrombin injection is particularly useful inpatients on anticoagulants or on GP IIb/IIIainhibitor therapy and with a low probability of successful closure by ultrasound-guidedcompression alone. Endovascular coil emboliza-tion or covered stent deployment are options toseal frank bleeding related to vessel laceration orrupture, but can also be used to seal the neck of alarge pseudoaneurysm in cases where surgery
bears a substantial risk and the other options havefailed (Figures 6a.1–6a.3). Surgery always remainsan option if other less invasive measures fail.
In cases of bleeding complications due toaggressive anticoagulation with heparin, 1 mgof protamine as a bolus rapidly neutralizesapproximately 100 U of heparin. The effect ofGP IIb/IIIa inhibitors can be reversed by trans-fusion of platelets. No direct antidotes exist tocounteract the effect of aspirin, clopidogrel,LMWH, and direct thrombin inhibitors. Serious,acute bleeding complications need replacementof fluid (saline 0.9%, colloidal fluids), transfu-sion of erythrocytes, and rarely administrationof platelets, fresh frozen plasma, or prothrombincomplex concentrate.
METHODS TO AVOID COMPLICATIONS
The best approach to avoid local bleeding com-plications at the access site is to use the smallestintroducer sheaths possible, and to remove themrapidly at the end of the procedure. The indica-tion for an aggressive dual antiplatelet therapyor anticoagulation should always be balancedagainst the risk/benefit ratio for the patienttreated. A reduction in the dosage of concomi-tant heparin and rapid sheath removal reducebleeding complications due to abciximab.36 Com-orbidities and laboratory parameters should beavailable before each intervention, and addi-tional diagnostic work-up should be performedif necessary.
PHARMACOLOGICAL INTERVENTION 77
Figure 6a.3 Exclusion of the pseudoaneurysm after coilembolization.
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 77

SUMMARY
Endovascular therapy for PAD is rapidly expand-ing. Therefore, there is clearly a need for moreevidence on periprocedural antiplatelet andanticoagulant treatment during and after theseinterventions. To date, an intra-arterial UFH bolusduring, and dual antiplatelet therapy using aspirin
and clopidogrel for 28 days after endovasculartherapy represent the most commonly used stan-dard. Access site and gastrointestinal bleedingare the most commonly seen complications, usu-ally managed by local repair, proton-pump inhib-itors, and, if needed, fluid replacement and rarelyblood transfusion, protamine, or fresh frozenplasma.
CHECK LIST FOR EMERGENCY EQUIPMENT
Be familiar with commonly used drugs, theirindication, dosage, and application (Table 6a.3).Be aware of the possibility of reversing theeffects of antiplatelet, antithrombotic, and anti-coagulant agents (Table 6a.4). Be aware of con-traindications for thrombolysis and treatmentwith GP IIb/IIIa inhibitors. The decision to useabciximab must clearly outweigh the risk ofbleeding. Be aware of peri- and postproceduralbleeding complications and recommend closemonitoring (vital signs, local puncture site) andproton-pump inhibitors in patients at high-riskfor bleeding.
REFERENCES
1. Jorgensen B, Meisner S, Holstein P et al. Early rethrom-bosis in femoropopliteal occlusions treated with percu-taneous transluminal angioplasty. Eur J Vasc Surg 1990;4: 149–52.
2. Eikelboom JW, Hirsh J, Weitz JI et al. Aspirin-resistantthromboxane biosynthesis and the risk of myocardialinfarction, stroke, or cardiovascular death in patients athigh risk for cardiovascular events. Circulation 2002;105(14): 1650–5.
3. Antithrombotic Trialists’ Collaboration. Collaborativemeta-analysis of randomised trials of antiplatelet ther-apy for prevention of death, myocardial infarction, andstroke in high risk patients. BMJ 2002; 324: 71–86.
4. CAPRIE Steering Committee. A randomised, blinded,trial of clopidogrel versus aspirin in patients at risk ofischaemic events (CAPRIE). Lancet 1996; 348: 1329–39.
5. Dormandy JA, Rutherford RB. Management of periph-eral arterial disease (PAD). TASC Working Group. Trans-Atlantic Inter-Society Concensus (TASC). J Vasc Surg2000; 31: S1–296.
6. Antiplatelet Trialists’ Collaboration. Collaborativeoverview of randomised trials of antiplatelet therapy.Prevention of death, myocardial infarction, and strokeby prolonged antiplatelet therapy in various categoriesof patients. BMJ 1994; 308: 81–106.
78 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 6a.4 Reversing the effects ofantiplatelet, antithrombotic, and anticoagulant agents
Generic name Antidote
Acetylsalicylic acid No direct antidoteavailable; reverse theeffect by transfusionof platelets ifappropriate
Clopidogrel No direct antidoteavailable; reverse theeffect by transfusionof platelets ifappropriate
Glycoprotein IIb/IIIa No direct antidoteavailable; reverse theeffect by transfusionof platelets ifappropriate
Unfractionated heparin 1 mg of protaminerapidly neutralizesapproximately 100 Uof unfractionatedheparin, fresh frozenplasma
Low molecular weight No direct antidote heparin available; reverse the
effect by transfusionof fresh frozenplasma if appropriate
Vitamin K antagonist Vitamin K (2 to 10 mg)orally or intravenouslydepending on theurgency of thesituation, fresh frozenplasma, prothrombincomplex concentrate,or recombinant factorVIIa if appropriate
Thrombin inhibitors No direct antidoteavailable; reverse theeffect by transfusionof platelets ifappropriate
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 78

7. Awtry EH, Loscalzo J. Aspirin. Circulation 2000; 101:1206–18.
8. Kelly JP, Kaufman DW, Jurgelon JM et al. Risk ofaspirin-associated major upper-gastrointestinal bleedingwith enteric-coated or buffered product. Lancet 1996;348: 1413–16.
9. Sane DC, McKee SA, Malinin AI et al. Frequency ofaspirin resistance in patients with congestive heart fail-ure treated with antecedent aspirin. Am J Cardiol 2002;90(8): 893–5.
10. Gum PA, Kottke-Marchant K, Welsh PA et al. A pro-spective, blinded determination of the natural historyof aspirin resistance among stable patients with cardio-vascular disease. J Am Coll Cardiol 2003; 41(6): 961–5.
11. Michelson AD, Cattaneo M, Eikelboom JW et al; WorkingGroup on Aspirin Resistance. Aspirin resistance: posi-tion paper of the Working Group on AspirinResistance. J Thromb Haemost 2005; 3(6): 1309–11.
12. Jenkins C, Costello J, Hodge L. Systematic review ofprevalence of aspirin induced asthma and its implica-tions for clinical practice. BMJ 2004; 328(7437): 434.
13. Steinhubl SR, Berger PB, Mann JT 3rd et al; CREDOInvestigators. Clopidogrel for the Reduction of EventsDuring Observation. Early and sustained dual oralantiplatelet therapy following percutaneous coronaryintervention: a randomized controlled trial. JAMA 2002;288(19): 2411–20.
14. Peters RJ, Mehta SR, Fox KA et al. Effects of aspirindose when used alone or in combination with clopido-grel in patients with acute coronary syndromes: obser-vations from the Clopidogrel in Unstable angina toprevent Recurrent Events (CURE) study. Circulation2003; 108: 1682–7.
15. Diener HC, Bogousslavsky J, Brass LM et al; MATCHinvestigators. Aspirin and clopidogrel compared withclopidogrel alone after recent ischaemic stroke or tran-sient ischaemic attack in high-risk patients (MATCH):randomised, double-blind, placebo-controlled trial. Lancet2004; 364: 331–7.
16. ACC/AHA 2005 Guidelines for the Management ofPatients With Peripheral Arterial Disease (LowerExtremity, Renal, Mesenteric, and Abdominal Aortic)Circulation 2006: 113; 463–654.
17. Doggrell SA. Aspirin and esomeprazole are superior toclopidogrel in preventing recurrent ulcer bleeding.Expert Opin Pharmacother 2005; 6: 1253–6.
18. Dorffler-Melly J, Mahler F, Do DD et al. Adjunctiveabciximab improves patency and functional outcome inendovascular treatment of femoropopliteal occlusions:initial experience. Radiology 2005; 237: 1103–9.
19. Use of a monoclonal antibody directed against the plateletglycoprotein IIb/IIIa receptor in high-risk coronaryangioplasty. The EPIC Investigation. N Engl J Med 1994;330: 956–61.
20. Patrono C, Coller B, FitzGerald GA et al. Platelet-activedrugs: the relationships among dose, effectiveness, andside effects. The Seventh ACCP Conference on Antithrom-botic and Thrombolytic Therapy. Chest 2004; 126:234S–64.
21. Randomised placebo-controlled and balloon-angioplasty-controlled trial to assess safety of coronary stentingwith use of platelet glycoprotein-IIb/IIIa blockade. TheEPISTENT Investigators. Evaluation of Platelet IIb/IIIaInhibitor for Stenting. Lancet 1998; 352: 87–92.
22. Duda SH, Tepe G, Luz O et al. Peripheral arteryocclusion: treatment with abciximab plus urokinaseversus with urokinase alone – a randomized pilot trial (the PROMPT Study). Radiology 2001; 221:689–96.
23. Tepe G, Schott U, Erley CM et al. Platelet glycoproteinIIb/IIIa receptor antagonist used in conjunction withthrombolysis for peripheral arterial thrombosis. Am JRoentgenol 1998; 172: 1343–6.
24. Becker GJ, Katzen BT, Dake MD. Noncoronary angio-plasty. Radiology 1989; 170: 921–40.
25. Platelet glycoprotein IIb/IIIa receptor blockade andlow-dose heparin during percutaneous coronary revas-cularization. The EPILOG Investigators. N Engl J Med1997; 336: 1689–96.
26. Antman EM. Hirudin in acute myocardial infarc-tion. Thrombolysis and Thrombin Inhibition in Myo-cardial Infarction (TIMI) 9B trial. Circulation 1996; 94:911–21.
27. Mudaliar JH, Liem TK, Nichols WK et al. Lepirudin is a safe and effective anticoagulant for patients withheparin-associated antiplatelet antibodies. J Vasc Surg2001; 34: 17–20.
28. Lincoff AM, Bittl JA, Harrington RA et al; REPLACE-2Investigators. Bivalirudin and provisional glycoproteinIIb/IIIa blockade compared with heparin and plannedglycoprotein IIb/IIIa blockade during percutaneouscoronary intervention: REPLACE-2 randomized trial.JAMA 2003; 289: 853–63.
29. Lincoff AM, Kleiman NS, Kereiakes DJ et al; REPLACE-2Investigators. Long-term efficacy of bivalirudin andprovisional glycoprotein IIb/IIIa blockade vs heparinand planned glycoprotein IIb/IIIa blockade duringpercutaneous coronary revascularization: REPLACE-2randomized trial. JAMA 2004; 292: 696–703.
30. Lewis BE, Wallis DE, Berkowitz SD et al. Argatrobananticoagulant therapy in patients with heparin-inducedthrombocytopenia. Circulation 2001; 103: 1838–43.
31. Lewis BE, Matthai WH Jr, Cohen M et al. Argatrobananticoagulation during percutaneous coronary interven-tion in patients with heparin-induced thrombocytopenia.Cathet Cardiovasc Interv 2002; 57: 177–84.
32. Thrombolytic therapy in threatment: summary of anNIH Consensus Conference. BMJ 1980; 280: 1585–7.
PHARMACOLOGICAL INTERVENTION 79
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 79

33. Thrombolysis in the Management of Lower LimbPeripheral Arterial Occlusion – a Consensus Document.Working Party on Thrombolysis in the Management ofLimb Ischemia. Am J Cardiol 1998; 81: 207–18.
34. Coughlin BF, Paushter DM. Peripheral pseudoaneu-rysms: evaluation with duplex US. Radiology 1988; 168:339–42.
35. Tisi P, Callam M. Surgery versus non-surgical treatmentfor femoral pseudoaneurysms. Cochrane Database SystRev 2006; 25(1): CD004981.
36. Zehnder T, Birrer M, Do DD et al. Percutaneous catheterthrombus aspiration for acute or subacute arterial occlu-sion of the legs: how much thrombolysis is needed? Eur J Vasc Endovasc Surg 2000; 20: 41–6.
80 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter06a.qxp 4/5/2007 2:43 PM Page 80

INTRODUCTION TO THE FREQUENCY ANDTYPE OF COMPLICATIONS WITH THROMBOLYSIS
The vascular system is vulnerable to thrombusformation, which may lead to partial or completeinterruption of blood flow and may cause tissuehypoxia and result in tissue loss. Therapies aimedat thrombus dissolution are of paramount impor-tance in vascular and endovascular medicine.Fibrinolytic agents have historically been con-sidered the archetype of the thrombus dissolv-ing agents, and have been shown to be of greatclinical utility in almost every vascular territory.
The most frequent complications of fibrinolytictherapy are bleeding complications, which varyin severity depending upon the agent use, whethertherapy is given systemically or locally, the doseand length of infusion, the clinical circumstances,and the vessel(s) treated. In general terms, thereported incidence of major bleeding complica-tions (defined as intracranial bleeding, or anybleeding requiring transfusion or discontinua-tion of therapy) ranges from 7 to 45% (see below).Other complications include mild allergic reac-tions, which are not uncommon and are usu-ally associated with the use of streptokinase;however, serious allergic/anaphylactic reactionsare rare and occur in less than 1% of the cases(see below).
FACTORS IDENTIFYING HIGH-RISK PATIENTSFOR COMPLICATIONS
There are well-recognized patient and clinicalcharacteristics which increase the likelihood ofcomplications associated with fibrinolytic therapyand therefore may preclude its use in an absoluteor relative degree (Table 6b.1). As a general rule,intravenous thrombolysis is precluded in patientswith absolute contraindications, and must beavoided in patients with relative contraindica-tions. The use of intra-arterial thrombolysis inthose circumstances requires individual judgment.The choice to proceed with this form of therapymay be considered if the anticipated benefits sig-nificantly outweigh potential complications.
Other factors that affect the incidence of com-plications are related to the specific agent usedor those related to the clinical condition for whichthe thrombolytic agent was used.
Fibrinolytic agent-related complications
It is beyond of the scope of the present discussionto review the pathophysiology of the fibri-nolytic system or to address the specific mecha-nisms of action of each of the current fibrinolyticagents. However, the reader should rememberthat under physiologic as well as non-physiologicconditions, plasmin is ultimately responsible for
6b
Complications of thrombolytic therapy inperipheral vascular interventionsJose A Silva and Christopher J White
Introduction to the frequency and type of complications with thrombolysis • Factors identifying high-riskpatients for complications • Methods to detect potential complications • Summary
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 81

fibrin degradation. It is also important to keep inmind that in conditions of health, fibrin forma-tion and degradation occur in a continuousfashion through the activation of the intrinsic orextrinsic coagulation cascade and intrinsic tissueplasminogen activator. The balance betweenfibrin production, i.e. clot formation, and fibrindegradation, i.e. thrombolysis or clot degrada-tion, is complex and regulated by multipleintermediaries that will promote or inhibit theformation of plasmin.1–3
The ultimate goal of fibrinolytic agents is topromote clot lysis by stimulating the conversionof the proenzyme plasminogen to the activeenzyme plasmin (the final step of the fibrinolyticsystem). However, plasmin is a relatively non-specific protease, capable of hydrolyzing manyproteins in addition to fibrin, such as fibrinogen,factors V and VIII, von Willebrand factor, kinino-gen, and prekallikrein, among others.1 Conse-quently, the formation of plasmin may lead tohydrolysis, i.e. degradation, of multiple coagu-lation factors, potentially enhancing the risk forbleeding complications.
During the process of thrombosis, a large num-ber of plasminogen molecules are incorporatedinto the clot. This is known as thrombus-bound(or fibrin-bound) plasminogen, to distinguish itfrom the circulating plasminogen in plasma. Itis this fibrin-bound plasminogen which, afteractivation, leads to thrombus dissolution. Fibrin-specific agents such as tissue plasminogen activator(t-PA), and tenecteplase (TNK) preferentially acti-vate the fibrin-bound plasminogen, whereasnon-fibrin-specific agents such as streptokinase(STK), urokinase (UK), and reteplase (r-PA) donot discriminate between bound and circulatingplasminogen, and may also cause degradation ofcirculating fibrinogen and other clotting factors,such as factors V and VIII (Table 6b.2).
Streptokinase
The discovery of streptokinase in 1933 broughtabout marked interest in the development offibrinolytic agents that has spanned the pastseven decades.4 Streptokinase is a single-chainnon-enzymatic protein produced by �-hemolyticstreptococcus. Early clinical experience with thisagent was complicated by frequent pyogenic andallergic reactions. Despite technical improvementin its production, streptokinase remains highlyantigenic and has the potential for causing aller-gic reactions.5 In 1999, the US Food and DrugAdministration (FDA) warned of increasing life-threatening events associated with the use ofstreptokinase. Furthermore, patients with a recentexposure to streptococci and patients recentlytreated with streptokinase develop high levelsof circulating antistreptococcal antibodies capableof neutralizing streptokinase. These individualsare resistant to standard doses of this fibrinolyticagent, requiring higher doses of the drug to exceedthe saturation point of existing antibodies.6
Streptokinase needs to bind to a molecule ofplasminogen before being able to become a plas-minogen activator (i.e. requires plasminogenas a cofactor and as a substrate); consequently,fewer plasminogen molecules remain availableto turn into plasmin and produce the desiredfibrinolytic action, potentially shifting hydroly-sis in the direction of other molecules such asfibrinogen and factors V and VIII, among others.These complex interactions of streptokinase make
82 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 6b.1 Contraindications for intra-arterial fibrinolytic therapy
AAbbssoolluuttee ccoonnttrraaiinnddiiccaattiioonnssProfound, intolerable limb ischemiaActive internal bleedingCerebrovascular accident within 3 monthsIntracranial pathologic condition
RReellaattiivvee ccoonnttrraaiinnddiiccaattiioonnssRecent major surgery or traumaMinor gastrointestinal bleedingSevere hypertensionValvular heart diseaseAtrial fibrillationEndocarditisCoagulation disorderPregnancyMinor surgerySevere liver diseaseExtra-anatomic axillofemoral bypass graft or knittedDacron graft
SSttrreeppttookkiinnaasseeKnown allergyRecent streptococcal infectionPrevious therapy within 6 months
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 82

COMPLICATIONS OF THROMBOLYTIC THERAPY 83
Tabl
e 6b.
2 C
hara
cter
isti
cs o
f th
e m
ost
com
mon
ly u
sed
fibrino
lyti
cs i
n pe
riph
eral
int
erve
ntio
ns
Str
epto
kina
seU
roki
nase
t-PA
Ret
epla
seTe
nect
epla
se
Sou
rce
�-H
emol
ytic
Fe
tal
rena
l ce
ll R
ecom
bina
nt D
NA
Plas
min
ogen
R
ecom
bina
nt
stre
ptoc
occu
scu
lture
ste
chno
logy
activ
ator
DN
A te
chno
logy
Met
abol
ism
Live
rLi
ver
Live
rLi
ver
Live
rH
alf-l
ife23 m
in16 m
in4–5
min
14 m
in20–2
4 m
inFi
brin
spe
cific
ity+
++
+++
++
++++
Adva
ntag
esLo
w c
ost
Dire
ct a
ctiv
ator
Fibr
in s
elec
tive;
Fi
brin
sel
ectiv
e;
Fibr
in s
elec
tive;
di
rect
act
ivat
ordi
rect
act
ivat
ordi
rect
act
ivat
orD
isad
vant
ages
Alle
rgic
rea
ctio
ns.
Expe
nsiv
eEx
pens
ive
Expe
nsiv
eEx
pens
ive
Com
plex
int
erac
tions
Reg
iona
l in
fusi
on d
oses
5000–1
0000 U
/h*
2000–4
000 U
/min
0.0
5–0
.1 U
/kg/
h0.5
(0.2
5–1
.0)
U/h
0.2
5–1
.0m
g/h
30
000–6
0000 U
/h**
for
1–2
hou
rs;
then
1000–2
000 U
/min
Appr
oved
ind
icat
ions
AMI,
PE,
DVT
, ar
teria
l PE
, ve
nous
cat
hete
rAM
I, st
roke
, PE
, ve
nous
AMI
AMI
thro
mbo
sis/
embo
lism
occl
usio
nca
thet
er o
cclu
sion
AMI,
acut
e m
yoca
rdia
l in
farc
tion;
DVT
, de
ep v
enou
s th
rom
bosi
s; P
E, p
ulm
onar
y em
bolis
m;
t-PA,
tis
sue
plas
min
ogen
act
ivat
or.
*Lo
w d
ose;
**hi
gh d
ose.
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 83

the kinetics, half-life, and bioavailability highlyvariable and unpredictable.6,7
Despite the problem of antigenicity and unpre-dictable pharmacokinetics, many studies haveshown clinical benefits of this agent for the treat-ment of acute myocardial infarction (MI),5 orwhen catheter delivered for the treatment of acutearterial occlusions or deep venous thrombosis(DVT); however, bleeding complications occurredmore frequently than with the use of urokinase(see below).8–10
A complex of streptokinase and anisoylatedplasminogen-streptokinase activator complex(APSAC) or anistreplase was developed in anattempt to solve some of these problems, yet,clinical trials did not demonstrate any improve-ment in efficacy or decrease in antigenicity withthis compound.6
Urokinase
This fibrinolytic agent is a serine protease that isnormally present in urine as a product of renaltubular cells. Urokinase, in contrast to streptoki-nase, is a direct activator of plasminogen and isnon-antigenic. The lack of circulating antibodiesand its direct mechanism of action allow for apredictable dose–response relationship.6,11
During the 1990s, urokinase became the pre-ferred fibrinolytic agent in the non-coronary cir-culation and a great deal of experience wasgained with this drug. However, in 1999 Abbottlaboratories discontinued its production due toFDA concerns regarding the potential for viralcontamination. The safety issues were addressedand the drug was reintroduced in 2002.12
In phase I of the thrombolysis or peripheralarterial surgery (TOPAS) trial, three differentdoses of urokinase (2000, 4000, or 6000 IU/minfor 4 hours, followed by 2000 IU/min for a max-imum of 48 hours) were compared with surgeryfor the treatment of acute lower extremityischemia. The patients who received the inter-mediate dose achieved comparable rates of com-plete thrombolysis compared to the low-doseand high-dose regimens (71% versus 67% and60%, respectively; p = NS). However, the rateof hemorrhagic complications was signifi-cantly lower in the intermediate (2%), comparedto the low (13%) and high-dose (16%) regimens
(p < 0.05). In addition, the one-year mortality(14% versus 16%) and amputation-free survival(75% versus 65%) rates were similar in the inter-mediate dose and surgical patients.13
The incidence of major bleeding complicationsin patients treated for peripheral athero-occlusivedisease ranges from 0 to 16%.14,15 The Prourokinaseversus Urokinase for Recanalization of PeripheralOcclusions: Safety and Efficacy (PURPOSE) trial,found a high (16.7%) incidence of major (nointracranial bleeding) and minor bleeding com-plications in the urokinase group using a maxi-mum loading dose of 250 000 IU, followed by240 000 IU/h for 4 hours, 120 000 IU/h for thenext 4 hours, and 60 000 IU/h thereafter.15 Theincidence of intracranial bleeding with urokinaseis in the range of 0 to 2.1%.16–20
Tissue plasminogen activator (t-PA)
A great deal of the clinical experience obtainedwith t-PA has been gained in the last few years, inthe period when urokinase was withdrawn fromthe market.12 Similar to urokinase, studies usingt-PA for thrombolysis differ in dose, infusionlength, infusion technique, weight-adjustment,and clinical condition, therefore relatively widecomplication ranges have been reported. Onestudy21 reported an incidence of major bleedingcomplications and intracranial bleeding of 2.2%and 0%, respectively, compared to rates of 46%and 4% obtained for the same complications in adifferent report.22 In addition, doses of t-PA haveranged from 0.25 mg/h to as high as 10 mg/h(40-fold increase). A report summarizing 12 pub-lished studies of 1291 patients receiving 13 dif-ferent dose regimens found a mean incidence ofmajor bleeding complications of 5.1% (range 0 to17%), and a 0.54% incidence (range 0 to 2.2%) ofintracranial bleeding.23 The complication ratesof this last study contrast with a British registryof 697 patients where an 11.9% incidence of majorbleedings was observed.24 When the catheter-directed infusion of t-PA was weight adjusted,in a small prospective study of 35 patients withacute occlusion of native and bypass grafts, noapparent decrease in bleeding complications wasobserved when compared with historical controlsusing urokinase; however, patients who receivedlow-dose infusion (0.02 mg/kg/h) had a lower
84 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 84

incidence of major bleedings compared to thosewho received a combined low-dose/high-dose(0.02–0.04 mg/kg/h) regimen (15% versus 46%;p = 0.06).25
In a consecutive series of 653 patients treatedwith arterial or venous thrombolysis, Ouriel et al18
compared the complication rates between t-PAand urokinase. The complication rates were higherin the patients receiving t-PA (Figure 6b.1), butthe mortality rate, although also higher in thisgroup, was statistically not different (2.7% versus6.2%; p = 0.22).
Reteplase (r-PA)
Before removal of urokinase from the US marketin 1999, there were no data available on the use ofr-PA for thrombolysis in the non-coronary circula-tion. Its introduction for catheter delivery use, inthe non-coronary circulation, was supported bytrials of acute myocardial infarction showing thatthis fibrinolytic agent had a similar safety profile tothat of t-PA.26 In a prospective study of 87 patientswith three different doses of r-PA, complete lysisrates were similar in the three regimens (84 to87%); however, bleeding complications weredirectly proportional to the dose (Figure 6b.2).27
In a small registry of 37 patients with acutearterial occlusion (n = 26) or DVT (n = 11), there
were no occurrences of intracranial hemorrhage;however, a similar direct relationship between r-PA dose and bleeding complications was ob-served in the arterial occlusion group (Figure6b.3). In the DVT group, procedural bleedingoccurred in three (27%) patients. The use ofunfractionated heparin in subtherapeutic (n = 18)or therapeutic (n = 8) doses appeared not toaffect the bleeding complications.28 Reteplase hasalso been tested for the treatment of deep venousthrombosis with favorable results and a lowbleeding complication rate (see below).29
COMPLICATIONS OF THROMBOLYTIC THERAPY 85
0.6%
12%
22%
4.9%2.8% 1.5%
22%
44%
0
10
20
30
40
50
Hemat
oma(
p<0.00
01)
Bleedin
g*(p
=0.00
4)
ICH (p
=0.03
1)
Cardio
pulm
onar
y**(p
=0.01
5)
%
Urokinase
t-PA
(*) Requiring transfusion
(**) Requiring transfer to the intensive care unit
ICH, intracranial hemorrhage
Figure 6b.1 Complication rates of urokinase versus t-PA.18
5.4
13.3
2.9
0 10Bleeding complications (%)
20
0.125
0.25
0.5
r-P
A d
ose
(U/h
)
Figure 6b.2 Bleeding complications with three differentinfusion doses of r-PA in 87 patients with acute arterialocclusion.27
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 85

Tenecteplase (TNK)
Tenecteplase appears to have an improved safetyprofile compared to t-PA, in studies of acutemyocardial infarction.30 Compared to other fibri-nolytics in the non-coronary circulation, there isstill limited experience. In a study of 60 limbswith acute arterial occlusion (n = 24) or DVT (n = 36) using two different doses of TNK (0.25or 0.50 mg/h) thrombolysis rates were similarfor the arterial (83%) and venous groups (87%),and major bleeding complications occurred in onlyone case (1.8%).31 In another small pilot study, 18patients with arterial (n = 13) or venous (n = 5)occlusive disease were treated with infusions of0.25 mg/h. Technical success was obtained in100% and clinical success in 85% and 80% of thearterial and venous groups, respectively. Majorbleeding complications occurred in only onepatient (5.5%).32
Tenecteplase has also been used in conjunc-tion with platelet IIb/IIIa inhibitors. In a pilotstudy in 16 patients with acute arterial (n = 11)or venous (n = 5) thrombo-occlusive disease,TNK was catheter delivered as a 5 mg bolus, fol-lowed by 0.25 mg/h in infusion of intravenouseptifibatide (180 �g/kg double bolus, followedby 1 �g/kg/min infusion). Clinical success wasobtained in 82% of the arterial and 80% of thevenous cases, and major bleeding occurred in onlyone case (6.3%).33 In a larger study, 48 patientswith acute limb ischemia were treated withTNK at doses of 0.5 mg/h (n = 22) or 0.25 mg/h(n = 26), in conjunction with periprocedural
unfractionated heparin (500 U/h) and peripro-cedural and postprocedural tirofiban for 6 to 12 hours. Complete thrombolysis was obtainedin 73% (mean infusion time of 7.5 hours andmean TNK dose of 4.8 mg). Major bleeding com-plications occurred in 10.4% without intracranialhemorrhage or deaths.34
Although the results of these small reports arepromising, larger studies testing catheter deliveredTNK are necessary to determine its clinical effec-tiveness compared to other fibrinolytic agents.Whether the addition of a platelet IIb/IIIa inhibitorwill enhance the thrombolytic success of TNK orother fibrinolytic agents without increasing bleed-ing complications remains to be seen.
Complications related to specific clinicalapplications of thrombolysis
Acute arterial occlusion, limb ischemia
The use of fibrinolytic therapy for acute limbischemia has emerged as the preferred treatmentmodality in selected patients. Candidates forthrombolysis must be able to tolerate ischemiafor the duration of the infusion, which is one ofthe main limitations of this revascularizationstrategy.
The largest experience of intra-arterial fibri-nolysis for the treatment of limb ischemia hasbeen with urokinase and t-PA. Studies compar-ing the effectiveness of these two drugs havediffered in the doses used and the sample sizes(Table 6b.3).18,21,22,35–39 All but one study demon-strated that t-PA is slightly more effective thanurokinase in achieving complete thrombolysis(Figure 6b.4), while t-PA carries a higher incidenceof bleeding complications (Figure 6b.5).Theseresults have been confirmed by a literature reviewof 48 studies comparing complications of 2226urokinase-treated patients and 1927 t-PA-treatedpatients for peripheral arterial occlusions.40 Inthis report the major amputation rate was similarin both groups (7.9% versus 7.2%; p = NS); how-ever, the bleeding complications and mortalityrates were significantly higher in the t-PA-treatedpatients (Figure 6b.6).
Despite evidence showing the efficacy ofthrombolytic therapy in the treatment of acutearterial occlusion, it was not until lysis was
86 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
50
18.2
11.1
0 10 20 30 40 50 60
< 1.0
1.0–1.5
> 1.5
r-P
A d
ose
(U/h
)
Bleeding complications (%)p = 0.27
Figure 6b.3 Bleeding complications with three differentinfusion doses of r-PA in 26 patients with acute arterialocclusions.28
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 86

compared to surgery, and showed comparableclinical benefits, that thrombolysis was acceptedas a viable alternative treatment to surgery. Inthe Rochester trial, a non-randomized study, 114patients with acute peripheral thrombotic arterialischemia were treated with surgery or urokinase.The 12-month amputation rate was 18% for bothgroups, but the mortality rate in the thrombolysisgroup was only a third of the mortality rate obser-ved with surgery (16% versus 42%; p = 0.01).41
Subsequently two prospective randomized trialscompared thrombolysis versus surgical revascu-larization for thrombotic occlusion causing limbischemia.16,36 Both studies showed similar ampu-tation and mortality rates in the thrombolysisand the surgical groups. However, major bleed-ing complications were higher in the throm-bolytic group, in both the STILE trial (5.6% versus0.7%; p = 0.014), and the TOPAS trial (13% versus6%; p = 0.005).
Deep venous thrombosis
Anticoagulation with heparin (unfractionated orlow-molecular-weight heparin) has been thestandard treatment for deep venous thrombosis(DVT). This therapy is effective in preventingpulmonary embolism, but has limitations in pre-venting chronic postphlebitis in as many as 90%of the patients following DVT.42 Studies usingsystemic fibrinolysis have shown that the use ofthese agents is as effective as heparin in prevent-ing pulmonary embolism and mortality, but supe-rior to heparin and warfarin in achieving earlythrombus dissolution (~ 45%) and in decreasingpostphlebitic syndrome.43,44 In a study that pooledresults from eight prospective randomized trials,comparing systemic streptokinase with heparin,it was found that patients treated with fibrinolysisachieved a rate of thrombus dissolution almostthree times more frequently than those treatedwith heparin; however, the incidence of majorbleeding complications was also nearly four timeshigher in the streptokinase-treated patients.44
The magnitude of early thrombus dissolu-tion has been shown to be increased when thefibrinolytic agent is locally infused comparedto when it is given systemically. In addition,catheter-directed therapy has a positive impacton patients’ quality of life by preserving valve
COMPLICATIONS OF THROMBOLYTIC THERAPY 87
Tabl
e 6b.
3 D
oses
use
d in
eig
ht s
tudi
es c
ompa
ring
uro
kina
se a
nd t
-PA
Stu
dy (
refe
renc
e)Ty
pe o
f oc
clus
ion
# o
f pa
tient
sU
roki
nase
dos
e (IU
)t-P
A do
se
Mey
erov
iz e
t al
35
Leg
occl
usio
n32
60 K
bol
us;
240 K
/h×
2 h
,10
mg
bolu
s, t
hen
5m
g/h
120 K
/h×
2 h
, th
en 6
0 K
/hup
to
20 h
STI
LE t
rial3
6Le
g oc
clus
ion
249
250 K
bol
us;
240 K
/h×
4 h
,0.0
5–0
.1m
g/kg
/h120 K
/hS
chw
eize
r et
al3
7Le
g oc
clus
ion
120
60 K
/h5
mg
bolu
s, t
hen
5m
g/h
Cin
a et
al2
2Le
g oc
clus
ion
58
150 K
bol
us t
hen
50 K
/h5
mg
bolu
s, t
hen
1m
g/h
Our
iel
et a
l18
Leg
occl
usio
n/D
VT653
4 K
/min
0.0
5–0
.1m
g/kg
/hM
ahle
r et
al3
8Le
g oc
clus
ion
234
100 K
/h*,
or 2
0 K
/cm
2.5
mg/
h*,
or 0
.5m
g/cm
of t
hrom
bus/
h**
of t
hrom
bus/
h**
Sho
rtel
l et
al3
9Le
g oc
clus
ion/
DVT
73
240 K
×4 h
, th
en 1
20 K
/h2
mg/
hS
ugim
oto
et a
l21
Leg
occl
usio
n/D
VT70
90 K
/h–1
20 K
/h0.5
–1.0
mg/
h
*H
ess
tech
niqu
e; *
*S
chne
ider
tec
hniq
ue.
DVT
, de
ep v
enou
s th
rom
bosi
s; h
, ho
ur;
K,
1000 I
U.
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 87

function and decreasing the development of post-phlebitic syndrome.45 In one multicenter registryof 473 patients treated with catheter-deliveredurokinase, complete thrombolysis was obtainedin 31% and substantial thrombolysis (50 to 99%thrombus resolution) in 83%. Complete thrombol-ysis was significantly higher in acute (�10 days)than in chronic (>10 days) DVT (34% versus 19%;p < 0.01). Major bleeding complications occurred
in 11% (the majority at the puncture site), andmortality was less than 1%.46
The experience with catheter-delivered t-PAor r-PA for the treatment of DVT is limited. In anearly small study of 24 patients treated with t-PA(at 3 mg/h), the success rate was 75% but majorbleeding complications occurred in 25%.47 In astudy comparing t-PA and urokinase for arterialocclusion (n = 39) and DVT (n = 54) in 93 limbs,
88 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
63
38
7379
50
918982
50
85
75
62
0
10
20
30
40
50
60
70
80
90
100
Mey
erov
iz35
Schweiz
er e
t al37
Cina e
t al22
Mah
ler e
t al38
Shorte
ll et a
l39
Sugim
oto
et a
l21
% o
f suc
cess
Urokinase
t-PA
Figure 6b.4 Thrombolysis effectiveness: urokinase versus t-PA.21,22,35–39
37.3
19
0
912
2.223
9.6
31
46
22
0
10
20
30
40
50
Mey
erov
iz35
Schweiz
er e
t al37
Cina e
t al22
Ouriel
et a
l18
Mah
ler e
t al38
Shorte
ll et a
l39
Sugim
oto
et a
l21
%
Urokinase
t-PA
0
Figure 6b.5 Major bleeding complications: urokinase versus t-PA.21,22,35–39
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 88

the efficacy (84% vs 88%; p = 0.69) and bleedingcomplication rates (4.4% vs 4.2%) were similarin the urokinase and t-PA groups.21
A pilot study tested catheter-delivered r-PAin 25 patients with DVT.29 In this study 20 (80%)patients received 0.5 U/h, and five (20%) patientsreceived 1.0 U/h of r-PA, in addition to subther-apeutic unfractionated heparin doses of 300–400U/h. Thrombolytic success was obtained in 23(92%) patients, and there was only one (4%) majorbleeding complication. There were two patientsin whom the nadir of fibrinogen was below 90 mg/dL, requiring transfusion of fresh frozenplasma. A retrospective analysis of 74 patientsand 82 limbs with DVT compared catheter-delivered urokinase, t-PA, and r-PA.48 Complete(71%, 66%, 50%; p = 0.63) and complete pluspartial (97%, 97%, 100%, p = 0.83) resolution ofthrombus, as well as major complication rates(5.3%, 3.1%, 8.3%, p = 0.88), were similar in theurokinase, t-PA, and r-PA groups respectively.
Pulmonary embolism
In the US pulmonary embolism (PE) is responsi-ble for over 50 000 deaths annually, with a casefatality rate of 15% at 3 months.49,50 However, themortality rate more than doubles in patientswho develop hemodynamic instability or rightventricular dysfunction.51 The standard treatment
for this condition has been anticoagulation withheparin followed by a 3 to 6 month course ofwarfarin anticoagulation.52 Several randomized,controlled trials comparing thrombolytic therapywith heparin in patients with an acute PE havedemonstrated more rapid clot resolution in thosetreated with fibrinolysis. 53–59 However, a benefi-cial effect of thrombolytic therapy on clinicaloutcomes, including the recurrence of PE andmortality, has been difficult to demonstrate. Inaddition, some investigators have suggested thattreatment with fibrinolytic agents increases majorbleeding complications and they therefore recom-mend a more conservative approach.60
A meta-analysis61 involving 11 prospectiverandomized trials and 748 patients comparedpatients treated with fibrinolytic therapy versusheparin for the endpoints of mortality, recurrentPE, and bleeding complications. Compared withheparin, thrombolytic therapy was associatedwith a non-significant reduction in recurrentPE or death (6.7% versus 9.6%; OR 0.67, 95% CI0.40 to 1.12), a non-significant increase in majorbleeding (9.1% versus 6.1%; OR 1.42, 95% CI 0.81to 2.46), and a significant increase in bleedingcomplications (22.7% versus 10.0%; OR 2.63, 95%CI 1.53 to 4.54) (Figure 6b.7). Thrombolytic therapycompared to heparin was associated with a sig-nificant reduction in recurrent PE or death in trialsthat enrolled patients with hemodynamically
COMPLICATIONS OF THROMBOLYTIC THERAPY 89
11
0.4
3
8.4
6.2
16
1.1
5.6
0
10
20
Majorhemorrhage(p < 0.007)
Transfusions(p = 0.002)
ICH (p = 0.02) Mortality(p < 0.001)
%
Urokinase
t-PA
ICH: intracranial hematoma
Figure 6b.6 Major bleeding complications and mortality: urokinase (n = 2226) versus t-PA (n = 1927).40
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 89

unstable PE (9.4% vs 19.0%; OR 0.45, 95% CI 0.22to 0.92) but not in trials that excluded thesepatients (5.3% vs 4.8%; OR 1.07, 95% CI 0.50 to2.30). An earlier meta-analysis comparing fibri-nolytic therapy versus heparin also showed a sig-nificant increase in major bleeding complicationsin the thrombolysis-treated patients (Figure 6b.8).62
Acute ischemic stroke
In 1996, the FDA approved t-PA for the treat-ment of acute ischemic stroke based on its safetyand effectiveness when given within 3 hours ofsymptom onset.63 Its approval was based on theresults of the National Institute of NeurologicalDisorders and Stroke (NINDS) RecombinantTissue Plasminogen Activator Stroke Study, inwhich 624 patients with ischemic stroke weretreated with 0.9 mg/kg of t-PA within 3 hours ofthe onset of symptoms.64 In the t-PA group, 31 to50% had complete or near complete recovery atthe 3-month follow-up, whereas in the placebogroup this was achieved in only 38% (p < 0.05),and these differences persisted one year after theevent. However, the mortality rate was similarin both groups, and the incidence of sympto-matic brain hemorrhage was much higher in the
t-PA treated group (6.1% vs 0.6%; p < 0.05).Interestingly, the benefits of intravenous throm-bolysis for acute stroke were not duplicated inthree other trials.65–67 However, only 14% of thepatients received thrombolysis within 3 hours ofsymptom onset, whereas in the NINDS, 99.7%did (48% within 90 minutes).
The use of intra-arterial thrombolysis in acuteischemic stroke with angiographically documen-ted occlusion in the middle cerebral artery or afirst-order branch was shown to yield even higherreperfusion rates. Using pro-urokinase, partialor complete reperfusion was achieved in 67%compared to 18% in the heparin alone group (p < 0.001), when therapy was given with 2 hoursof symptom onset in the PROACT II study.68 Theprimary outcome measure analyzed was the abil-ity to live independently 3 months following thestroke and was much higher in the pro-urokinasegroup than in the heparin alone group (p < 0.05).However, this better clinical outcome in the pro-urokinase group was also achieved at the expenseof a higher intracranial bleeding rate (10% ver-sus 2%; p < 0.06). A higher NIHSS score, longertime to recanalization, lower platelet count, andhyperglycemia, have been found to be indepen-dent predictors for hemorrhagic transformation
90 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
0.01
Odds ratio (log scale)
Favors thrombolysis
Study
UPET, 1973 10/82 14/78 0.63 0.26 – 1.53
0.41 0.02– 10.83
0.35 0.03 – 4.42
0.31 0.03 – 3.36
0.51 0.01 – 27.68
1.59 0.05 – 47.52
2.35 0.09 – 60.24
2.65 0.25 – 28.24
0.12 0.01 – 2.35
0.01 0.00 – 0.77
1.36 0.48 – 3.87
0/13 1/17
1/14 2/11
1/15 3/16
0/20 0/10
1/9 0/4
1/33 0/25
3/20 1/16
0/46 4/55
0/4 4/4
8/118 7/138
25/374 36/374 0.67 0.40 – 1.12
Tibbutt et al, 1974
Ly et al, 1978
Dotter et al, 1979
Marini et al, 1988
PIOPED, 1990
Levine et al, 1990
Dalla-Volta et al, 1992
Goldhaber et al, 1993
Jerjes-Sanchez et al, 1995
Konstantinides et al, 2002
Total
Thrombolysis Heparin OR 95% CI
Favors heparin
0.1 1 10 100
Figure 6b.7 Recurrent PE or death in trials comparing thrombolysis with heparin for initial treatment of acute pulmonaryembolism.61 Reproduced with permission from Wan et al. Circulation 2004; 110: 744–9.
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 90

in patients receiving intra-arterial thrombolytictherapy.69 There are no randomized data compar-ing intra-arterial versus intravenous thrombolytictherapy for the treatment of acute ischemic stroke.
Stent thrombosis
Percutaneous transluminal angioplasty with adju-vant stent placement has emerged as one of thebest and most frequently used revascularizationstrategies in many vascular territories. However,stent thrombosis, although a relatively infrequentcomplication, may occur and frequently carriesdire consequences. Stent thrombosis has beenreported in essentially every vascular territory,with an incidence as high as 20% after femoro-popliteal arterial revascularization in early series.70
Although the true incidence of this complicationis difficult to estimate, it appears to be significantlylower in more recent studies of femoro-popliteal,iliac, renal, mesenteric, or carotid circulationwith a reported incidence of less than 2% in mostseries,71–78 and it is often related to suboptimalstent expansion or vascular dissection adjacent tothe stent.79
Fibrinolytic therapy has been reported to besuccessful in treating this complication in smallcase series and case reports.70,76 However, thereare no data addressing the systematic use of theseagents for the treatment of stent thrombosis, con-sequently, the incidence of complications relatedto this form of therapy is unknown. It is reason-able to infer that bleeding complications willalso depend on the dose, length, and type of fib-rinolytic used.
METHODS TO DETECT POTENTIAL COMPLICATIONS
Bleeding is the most feared and most commoncomplication of fibrinolytic therapy and is theresult of the systemic effect of the thrombolyticagent. Although the use of local, catheter-directedthrombolysis may decrease systemic effects, majorbleeding complications still occur in 5 to 15%. Itis also important to mention that recent experi-ence indicates that the incidence of bleeding cor-relates more with the duration of therapy thanwith the total dose of the agent infused. Con-sequently, it may be preferable to use higher-dose
COMPLICATIONS OF THROMBOLYTIC THERAPY 91
0.01 0.1 1 10 100
Relative risk
Overall 1.76 (1.04, 2.98)
Jerjes-S (1995)
Levine (1990)
Marini (1988)
Goldhaber (1993)
PAIMS2 (1992)
PIOPED (1990)
Ly (1978)
Tibbutt (1974)
UPET (1973) 1.90 (0.99, 3.66)
1.31 (0.09, 19.00)
1.57 (0.35, 7.06)
1.50 (0.07, 30.59)
1.20 (0.23, 6.34)
2.39 (0.22, 25.54)
(Not estimable)
(Not estimable)
(Not estimable)
Relative risk (95% Cl)
Figure 6b.8 Graphic representation of the relative risk (95% confidence interval [CI]) of major hemorrhage in the thrombol-ysis versus heparin groups.62 Reproduced with permission from Thabut et al. J Am Coll Cardiol 2002; 40: 1660–7.
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 91

protocols for a shorter period of time.80,81 Althoughspecific parameters of coagulation do not appearto correlate with the risk of bleeding duringthrombolysis, a systemic lytic state increases thiscomplication. Consequently, documentation of adecrease in fibrinogen of more than 50%, or pro-longation of the thrombin time to more than twotimes normal, is important so that corrections aremade should bleeding occur.
When systemic thrombolysis has been usedand the development of a major bleeding com-plication such as gastrointestinal bleeding orintracranial hemorrhage is suspected, the infusionof the drug must be stopped immediately. If gas-trointestinal bleeding is being considered but isnot overt, serial measurements of the hematocritas well as assessment of blood in stool must becarried out immediately while fluids are infused.If gastrointestinal bleeding is obvious, blood mustbe kept on hold for transfusion, particularly ifthe patient develops hemodynamic compromise(see below). The development of any neurologicmanifestation such as confusion, stupor, seizures,or even mild changes in the mental statusshould be viewed as a possible intracranial hem-orrhage, therefore, a CT scan of the brain mustbe obtained to confirm or rule out this complica-tion. If bleeding is confirmed, neurosurgery con-sultation is indicated. The onset of eye pain orvisual loss should also alert one to the possibilityof intraocular bleeding.82 Prompt consultationwith an ophthalmologist must be obtained imme-diately to minimize ocular damage.
Endovascular, surgical, and medicaltechniques to resolve complications
In the case of catheter-delivered thrombolysis,the development of oozing around the catheterentry site without significant hematoma, duringadvanced or final stages of the treatment, can becontrolled with local measures such as pressuredressings (although this rarely produces completehemostasis) and close observation of the patientuntil the infusion is completed. On the other hand,the development of oozing in the early stages oftherapy, when a long (12 to 24 hours) infusionis anticipated, deserves a different approach.The operator may be able to stop the oozing byexchanging the access sheath for a larger sheath
(usually 1 French larger size); however, if thismeasure does not achieve hemostasis, and a hema-toma is developing, it is likely that the treatmentwill have to be discontinued. The developmentof a hematoma or bleeding at a remote site war-rants therapy cessation. Fibrinogen should bereplaced with fibrinogen-rich components suchas cryoprecipitate or fresh-frozen plasma, fol-lowed by blood transfusion if a significant dropin the hematocrit occurs.
Distal embolization probably occurs much morefrequently than is clinically appreciated, but rarelyrequires discontinuation of therapy. If distal embo-lization of thrombus is recognized, an increase inthe infusion rate is preferred to facilitate dissolu-tion of the embolic particles. If severe or worsen-ing of the ischemia occurs despite these measures,the infusion may be stopped to reassess the patencyof the vessel with angiography. If profoundischemia is developing, the operator may considerthe use of a mechanical thrombectomy device orsurgical embolectomy. Several cases of emboliza-tion to the ipsilateral extremity have been reportedduring intra-arterial lytic therapy for occlusion ofextra-anatomic (axillofemoral) grafts.80 For thisreason, several investigators consider lytic therapyunsuitable for the treatment of these bypassesdue to their length, and choose a more tradi-tional approach, such as surgical thrombectomy.
The treatment of bleeding complicationsdepends on the severity and the time when theyoccur. In the case of systemic thrombolysis, ifpatients develop any evidence of major bleedingsuch as gastrointestinal bleeding or intracranialhemorrhage, the infusion of the drug must bestopped immediately, as mentioned previously.If gastrointestinal bleeding occurs, fluid replace-ment and transfusions may be given if hemody-namic compromise and/or significant decrease inthe hematocrit are confirmed. The development ofany neurologic manifestation should be viewed asintracranial bleeding until proven otherwise, sothese patients must get a CT scan of the brain. Ifintracranial hemorrhage is confirmed, neurosur-gery consultation must be obtained emergently.The occurrence of visual loss or eye pain shouldalso alert one to the possibility of intraocularbleeding as mentioned before.82 Prompt diagno-sis and treatment is crucial to preserve functionin the affected eye.
92 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 92

Vascular access complications such as hema-toma, pseudoaneurysm, and arterio-venous fistulaformation at the site of vascular access, or retro-peritoneal bleeding (if the common femoral arte-rial access has been used), may occasionallyoccur. They are the most frequent site for bleed-ing complications following vascular access, witha reported incidence of 2 to 6%.83–85 Only rarelydo these complications require surgical repair andin the majority of the cases they may be man-aged conservatively or percutaneously.86 Theseparticular complications are addressed elsewherein this book, hence we will not discuss them inthis chapter.
Pulmonary embolism can occur during treat-ment for DVT, however its occurrence is lowand appears to be similar to that seen with con-ventional heparin therapy. In the absence of othercomplications, continuation of lytic therapy isthe treatment of choice. If recurrent emboli areobserved, discontinuation of the fibrinolytic,heparin administration, and placement of a cavalfilter may prevent further morbidity or mortality.The development of fatal PE has been describedduring intra-arterial fibrinolysis of lower limbischemia, as a result of venous stasis of the targetlimb, leading to DVT, partial thrombus lysis, andpulmonary embolization.87 This is a very rare occur-rence and treatment options include cessation oflytic therapy with heparinization or switching tointravenous fibrinolysis. If the latter option ischosen, the operator must remember to leave thearterial catheter/sheath in place to minimize riskof bleeding from the arterial puncture site.
Allergic reactions to streptokinase are not infre-quent, however, most are minor febrile episodesthat usually respond to aspirin or acetominophen.Serious allergic reactions are infrequent with thecurrent streptokinase, and even more rare witht-PA.88,89 They must be managed with intravenoussteroids and conventional therapy for anaphy-lactic reactions.
SUMMARY
Fibrinolytic therapy is an important treatmentmodality for patients with thombotic stenoses orocclusions in the peripheral arterial and venouscirculation. The first fibrinolytic agent avail-able for peripheral vascular interventions was
streptokinase, which at present is rarely useddue to its frequent immunologic reactions, unpre-dictable pharmacokinetics, and relatively frequentbleeding complications. Most clinical experiencehas been obtained with the non-fibrin-selectiveurokinase and the fibrin-selective t-PA, which,overall, are equally effective for this condition,although t-PA may act more rapidly. Major bleed-ing complications appear to be slightly morefrequent in t-PA treated patients. The experiencewith reteplase and tenecteplase is very limited,but potentially promising in terms of safety pro-file and effectiveness.
Recent randomized trials have shown thatcatheter-delivered fibrinolytic therapy is analternative to surgical embolectomy in selectedpatients without profound ischemia. Intra-arterialfibrinolysis has been shown to decrease the long-term incidence of the postphlebitic syndromeand to increase the quality of life compared toanticoagulation. Thrombolysis should be offeredto these patients, particularly those with exten-sive DVT affecting the iliofemoral venous system.Systemic fibrinolysis should be considered forpatients with massive pulmonary embolism caus-ing hypotension and right ventricular dysfunc-tion. Recent meta-analyses have shown that in thisgroup of patients, fibrinolysis decreases mortal-ity as well as recurrent pulmonary embolism.Patients with acute ischemic stroke, presentingwithin 3 hours of symptom onset, should also beconsidered for fibrinolytic therapy.
Major bleeding complications occur in 5 to 15%of the patients undergoing this form of therapy. Inpatients with suspected gastrointestinal or intra-cranial bleeding, fibrinolytic therapy must be dis-continued, and fibrinogen replaced. In patientswith bleeding around the catheter entry site, theneed to stop therapy must be individualizedaccording to the severity of bleeding, length ofinfusion, and symptoms.
REFERENCES
1. Henkin J, Marcotte P, Yang H. The plasminogen–plasminsystem. Prog Cardiovasc Dis 1991; 34: 135–64.
2. Segui R, Estelles A, Mira Y. PAI-1 promoter 4G/5Ggenotype as an additional risk factor for venous throm-bosis in subjects with genetic thrombophilic defects. BrJ Haematol 2000; 111: 122–8.
COMPLICATIONS OF THROMBOLYTIC THERAPY 93
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 93

3. Meissner MH, Zierler BK, Bergelin RO et al. Coagulation,fibrinolysis, and recanalization after acute deep venousthrombosis. J Vasc Surg 2002; 35: 278–85.
4. Tillet WS, Garner RL. The fibrinolytic activity ofhemolytic streptococci. J Exp Med 1933; 58: 485–8.
5. ISIS-3 (Third International Study of Infarct SurvivalCollaborative Group). ISIS-3: a randomized comparisonof streptokinase versus tissue plasminogen activatorversus anistreplase and aspirin and heparin versusheparin alone among 41,299 cases of suspected acutemyocardial infarction. Lancet 1992; 339: 1574–7.
6. Comerota AJ, Carman TL. Thrombolytic agents and theiractions. In Rutherford RB. Vascular Surgery, 6th edn,Vol 1. Philadelphia: Elseviers Saunders, 2005: 530–45.
7. Coller BS. Platelets and thrombolytic therapy. N Engl JMed 2000; 322: 33–42.
8. Van Breda A, Katsen BT, Deutsche AS. Urokinase versusstreptokinase in local thrombolysis. Radiology 1987;165: 109–11.
9. Graor RA, Young JR, Risius B et al. Comparison and costeffectiveness of streptokinase and urokinase in the treat-ment of deep vein thrombosis. Ann Vasc Surg 1987: 1:524–8.
10. Urokinase–Streptokinase Pulmonary Embolism Trial:phase II results: a cooperative study. JAMA 1974; 229:1606–13.
11. Razavi MK, Lee DS, Hoffmann LV. Catheter directedthrombolytic therapy for limb ischemia: current statusand controversies. J Vasc Interv Radiol 2004; 15: 13–23.
12. Gates J, Hartnell GG. When urokinase was gone:commentary on another year of thrombolysis withouturokinase. J Vasc Interv Radiol 2004; 15: 1–5.
13. Ouriel K, Veith FJ, Sasahara. Thrombolysis or PeripheralArterial Surgery: phase I results. TOPAS Investigators.J Vasc Surg 1996; 23: 64–73.
14. Bookstein JJ, Fellmeth B, Roberts A et al. Pulsed-spraypharmacomechanical thrombolysis: preliminary clinicalresults. Am J Roentgenol 1989; 152: 1097–100.
15. Ouriel K, Kandarpa K, Schuerr DM et al. Prourokinaseversus Urokinase for Recanalization of PeripheralOcclusions, safety and efficacy: the PURPOSE Trial. J Vasc Interv Radiol 1999; 10: 1083–91.
16. Ouriel K, Veith FJ, Sasahara AA. A comparison ofrecombinant urokinase with vascular surgery as initialtreatment for acute arterial occlusion of the legs.Thrombolysis or Peripheral Arterial Surgery (TOPAS)Investigators. N Engl J Med 1998; 1105–11.
17. Ouriel K, Shortell CK, DeWeese JA et al. A comparisonof thrombolytic therapy with operative revasculariza-tion in the initial treatment of acute peripheral arterialischemia. J Vasc Surg 1994; 19: 1021–30.
18. Ouriel K, Gray B, Clair DG et al. Complications associ-ated with the use of urokinase and recombinant tissueplasminogen activator for catheter-directed peripheral
arterial and venous thrombolysis. J Vasc Interv Radiol2000; 11: 295–8.
19. Wholey MH, Maynar MA, Wholey MH et al. Com-parison of thrombolytic therapy of lower extremityacute, subacute, and chronic arterial occlusion. CathetCardiovasc Diagn 1998; 44: 159–69.
20. Matas Docampo M, Gomez Palones F, FernandezValenzuela V et al. Intraarterial urokinase for acutenative arterial occlusion of the limbs. Ann Vasc Surg1997; 11: 565–72.
21. Sugimoto K, Hofman LV, Razavi MK et al. The safety,efficacy, and pharmacoeconomics of low-dose alteplasecompared with urokinase for catheter-directed throm-bolysis of arterial and venous occlusions. J Vasc Surg2003; 37: 512–17.
22. Cina CS, Goth RH, Chan J et al. Intraarterial catheter-directed thrombolysis: urokinase versus tissue plasmino-gen activator. Ann Vasc Surg 1999; 13: 571–5.
23. Semba CP, Murphy TP, Bakal CW et al. Thrombolytictherapy with the use of alteplase (rt-PA) in peripheralarterial occlusive disease: review of the clinical literature.The Advisory Pannel. J Vasc Interv Radiol 2000; 11:149–61.
24. Thomas SM, Gaines PA. Vascular surgical society ofGreat Britain and Ireland: avoiding complications ofthrombolysis (abstract). Br J Surg 1999; 86: 710.
25. Arepally A, Hofmann LV, Kim HS et al. Weight-basedrt-PA thrombolysis protocol for acute native arterial andbypass graft occlusions. J Vasc Interv Radiol 2002; 13:45–50.
26. The GUSTO III Investigators. A comparison of reteplasewith alteplase for acute myocardial infarction. N Engl JMed 1997; 337: 1118–23.
27. Castaneda F, Swischuk JL, Li R et al. Declining-dosestudy of reteplase treatment for lower extremity arterialocclusions. J Vasc Interv Radiol 2002; 13: 1093–8.
28. Ouriel K, Katzen B, Mewissen M et al. Reteplase inthe treatment of peripheral arterial and venous occlu-sions. A Pilot Study. J Vasc Interv Radiol 2000; 11:849–54.
29. Castaneda F, Li R, Young K et al. Catheter-directedthrombolysis in deep venous thrombosis with use ofreteplase: immediate results and complications from apilot study. J Vasc Interv Radiol 2002; 13: 577–80.
30. ASSENT-2 Investigators. Single bolus tenecteplase com-pared with front-loaded alteplase in acute myocardialinfarction: the ASSENT-2 double blind randomized trial.Lancet 1999; 354: 716–22.
31. Razabi MK, Wong H, Kee ST et al. Initial clinical resultsof tenecteplase (TNK) in catheter-directed throm-bolytic therapy. J Endovasc Ther 2002; 9: 593–8.
32. Burkart DJ, Borsa JJ, Anthony JP et al. Thrombolysis ofoccluded peripheral arteries and veins: a pilot study. J Vasc Interv Radiol 2002; 13: 1099–102.
94 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 94

33. Burkart DJ, Borsa JJ, Anthony JP et al. Thrombolysis ofacute peripheral arterial and venous occlusions withtenecteplase and eptifibatide: a pilot study. J Vasc IntervRadiol 2003; 14: 729–33.
34. Allie DE, Herbert CJ, Lirtzman MD et al. Continuoustenecteplase infusion combined with peri/postproce-dural platelet glycoprotein IIb/IIIa inhibition in periph-eral arterial thrombolysis: initial safety and feasibilityexperience. J Endovasc Ther 2004; 11: 427–35.
35. Meyerovitz MF, Goldhaber SZ, Reagan K et al.Recombinant tissue-type plasminogen activator versusurokinase in peripheral arterial and graft occlusions.Radiology 1990; 175: 75–8.
36. STILE Investigators. Results of a prospective random-ized trial evaluating surgery versus thrombolysis forischemia of the lower extremity. The STILE trial. AnnSurg 1994; 220: 251–66.
37. Schweizer J, Altmann E, Stosslein F et al. Comparisonof tissue plasminogen activator and urokinase in thelocal infiltration thrombolysis of peripheral arterialocclusions. Eur J Radiol 1996; 22: 129–32.
38. Mahler F, Schneider E, Hess H. Recombinant tissue plas-minogen activator versus urokinase for local thrombolysisof femoropopliteal occlusions: a prospective, random-ized multicenter trial. J Endovasc Ther 2001; 8: 638–47.
39. Shortell CK, Queiroz R, Johansson M et al. Safety andefficacy of limited-dose tissue plasminogen activator inacute vascular occlusions. J Vasc Surg 2001; 34: 854–9.
40. Ouriel K, Kandarpa K. Safety of thrombolytic therapywith urokinase or recombinant tissue plasminogen acti-vator for peripheral arterial occlusion: a comprehensivecompilation of published work. J Endovasc Ther 2004;11: 436–46.
41. Ouriel K, Shortell CK, DeWeese JA et al. A comparisonof thrombolytic therapy with operative revasculariza-tion in the initial treatment of acute peripheral arterialischemia. J Vasc Surg 1994; 19: 1021–30.
42. Akesson H, Brudin L, Dahlstron JA et al. Venous func-tion assessed during a 5-year period after ilio-femoralvenous thrombosis treated with anticoagulation. Eur JVasc Surg 1990; 4: 43–8.
43. Comerota AJ, Aldridge SA. Thrombolytic therapy foracute deep venous thrombosis. Semin Vasc Surg 1992;5: 76–84.
44. Goldhaber SZ, Buring JE, Lipnick RJ et al. Pooled analy-sis of randomized trials of streptokinase and heparin inphlebographically documented acute DVT. Am J Med1984; 76: 393–7.
45. Comerota AJ, Throm RC, Mathias SD et al. Catheter-directed thrombolysis for iliofemoral deep vein throm-bosis improves health-related quality of life. J VascSurg 2000; 32: 130–7.
46. Mewissen MW, Seabrook GR, Meissner MH et al.Catheter-directed thrombolysis for lower extremity
deep venous thrombosis: report of a national multicen-ter registry. Radiology 1999; 211: 39–49.
47. Verhnage R, Stockx L, Lacroix H et al. Catheter-directedlysis of iliofemoral vein thrombosis. Eur Radiol 1977; 7:996–1001.
48. Grunwald MR, Hoffmann LV. Comparison of urokinase,alteplase, and reteplase for catheter-directed thrombol-ysis of deep venous thrombosis. J Vasc Interv Radiol2004; 15: 347–52.
49. Goldhaber SZ. Pulmonary embolism. N Engl J Med1998; 339: 93–104.
50. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonaryembolism: clinical outcomes in the International Cooper-ative Pulmonary Embolism Registry (ICOPER). Lancet1999; 353: 1386–9.
51. Kaspar W, Konstantinides S, Geibel A et al. Managementstrategies and determinants of outcome in acute majorpulmonary embolism: results of a multicenter registry.J Am Coll Cardiol 1997; 30: 1165–71.
52. Quinlan DJ, McQuillan AM, Eikelboom JW. Low-molecular-weight heparin compared with intravenousunfractionated heparin for treatment of pulmonaryembolism: a meta-analysis of randomized, controlledtrials. Ann Intern Med 2004; 140: 175–83.
53. Ly B, Arnesen H, Eie H et al. A controlled clinical trial ofstreptokinase and heparin in the treatment of majorpulmonary embolism. Acta Med Scand 1978; 203: 465–70.
54. Levine M, Hirsh J, Weitz J et al. A randomized trial of asingle bolus dosage regimen of recombinant tissueplasminogen activator in patients with acute pulmonaryembolism. Chest 1990; 98: 1473–9.
55. Goldhaber SZ, Haire WD, Feldstein ML et al. Alteplaseversus heparin in acute pulmonary embolism: ran-domised trial assessing right-ventricular function andpulmonary perfusion. Lancet 1993; 341: 507–11.
56. Dalla-Volta S, Palla A, Santolicandro A et al. PAIMS 2:alteplase combined with heparin versus heparin in thetreatment of acute pulmonary embolism. PlasminogenActivator Italian Multicenter Study 2. J Am Coll Cardiol1992; 20: 520–6.
57. Tibbutt DA, Davies JA, Anderson JA et al. Comparisonby controlled clinical trial of streptokinase and heparinin treatment of life-threatening pulmonary embolism.Br Med J 1974; 1: 343–7.
58. The Urokinase Pulmonary Embolism Trial: a nationalcooperative study. Circulation 1973; 47 Suppl II: II1–108.
59. The PIOPED Investigators. Tissue plasminogen activatorfor the treatment of acute pulmonary embolism: a col-laborative study by the PIOPED Investigators. Chest1990; 97: 528–33.
60. Stein PD, Hull RD, Raskob G. Risks for major bleedingfrom thrombolytic therapy in patients with acute pul-monary embolism: consideration of noninvasive man-agement. Ann Intern Med 1994; 121: 313–17.
COMPLICATIONS OF THROMBOLYTIC THERAPY 95
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 95

61. Wan S, Quinlan DJ, Agnelli G et al. Thrombolysis com-pared with heparin for the initial treatment of pulmonaryembolism. A meta-analysis of the randomized controlledtrials. Circulation 2004; 110: 744–9.
62. Thabut G, Thabut D, Myers RP et al. Thrombolytic ther-apy of pulmonary embolism. A meta-analysis. J AmColl Cardiol 2002; 40: 1660–7.
63. Activase, alteplase recombinant for acute ischemic stroke:efficacy supplement. Paper presented at Peripheral andCentral Nervous System Drug Advisory CommitteeMeeting, 1996, Bethesda, MD.
64. National Institute of Neurological Disorders and Strokert-PA Stroke Study Group. Tissue plasminogen activatorfor acute ischemic stroke. N Engl J Med 1995; 333:1581–7.
65. Hacke W, Kaste M, Fieschi C et al. Intravenous throm-bolysis with recombinant tissue plasminogen activatorfor acute hemispheric stroke. JAMA 1995; 274: 1017–25.
66. Hacke W, Kaste M, Fieschi C et al. Randomized, dou-ble-blind placebo controlled trial of thrombolytic ther-apy with intravenous alteplase in acute ischemic stroke(ECASS II). Lancet 1998; 352: 1245–51.
67. NINDS t-PA Stroke Study Group. Intracerebral hemor-rhage after intravenous t-PA for ischemic stroke. Stroke1997; 28: 2109–18.
68. Furlan A, Higashida R, Wecshler L et al. Intraarterialprourokinase for acute ischemic stroke. The PROACT IIstudy: a randomized controlled trial. Prolyse in acutecerebral thromboembolism. JAMA 1999; 282: 2003–11.
69. Kidwell CS, Saver JL, Carneado J et al. Predictors ofhemorrhagic transformation in patients receiving intra-arterial thrombolysis. Stroke 2002; 33: 717–24.
70. Do-dai-Do, Triller J, Walpoth BH et al. A comparisonstudy of self-expandable stents versus balloon angio-plasty alone in femoro-popliteal artery occlusions.Cardiovasc Interv Radiol 1992; 15: 306–12.
71. Schillinger M, Sabeti S, Loewe C et al. Balloon angio-plasty versus implantation of nitinol stents in thesuperficial femoral artery. N Engl J Med 2006; 354:1879–88.
72. Bosch JL, Hunink MG. Meta-analysis of the results ofpercutaneous transluminal angioplasty and stent place-ment for aortoiliac occlusive disease. Radiology 1997;204: 87–96.
73. Ivanovic V, McKusick MA, Johnson CM et al. Renalartery stent placement: complications at a single tertiarycare center. J Vasc Interv Radiol 2003; 14: 217–25.
74. White CJ, Ramee SR, Collins TJ et al. Renal artery stentplacement: utility in lesions difficult to treat with balloonangioplasty. J Am Coll Cardiol 1997; 30: 1445–50.
75. Yadav JS, Wholey MH, Kuntz RE et al. Protectedcarotid-artery stenting versus endarterectomy in high-riskpatients. N Engl J Med 2004; 351: 1493–501.
76. Steine-Boker S, Cejna M, Nasel C et al. Successful revas-cularization of acute carotid stent thrombosis by facili-tated thrombolysis. Am J Neuroradiol 2004; 25: 1411–13.
77. Sharafuddin MJ, Olson CH, Sun S et al. Endovasculartreatment of celiac and mesenteric arteries stenoses:applications and results. J Vasc Surg 2003; 38: 692–8.
78. Silva JA, White CJ, Collins TJ et al. Endovascular therapyfor chronic mesenteric ischemia. J Am Coll Cardiol2006; 47: 944–50.
79. Kitchens C, Jordan W, Wirthlin D et al. Vascular com-plications arising from maldeployed stents. VascEndovasc Surg 2002; 36: 145–54.
80. Graor Ra, Risius B, Denny KM et al. Local thrombolysisin the treatment of thrombosed arteries, bypassed grafts,and arteriovenous fistulas. J Vasc Surg 1985; 2: 406–9.
81. McNamara TO, Fisher JR. Thrombolysis of peripheralarterial and graft occlusions: improved results using high-dose urokinase. Am J Roentgenol 1985; 144: 769–78.
82. Chorich LJ, Derick RJ, Chambers RB et al. Hemorrhagicocular complications associated with the use of systemicthrombolytic agents. Ophthalmology 1998; 105: 428–31.
83. Popma JJ, Satler LF, Pichard AD et al. Vascular compli-cations after balloon and new device complications.Circulation 1993; 88: 1568–78.
84. Johnson LW, Esente P, Giambartolomei A et al.Peripheral vascular complications of coronary angio-plasty by the femoral and brachial techniques. CathetCardiovasc Diagn 1994; 31: 165–72.
85. Waksman R, King SB III, Douglas JS et al. Predictors ofgroin complications after balloon and new-device coro-nary intervention. Am J Cardiol 1995; 75: 886–9.
86. Samal AK, White CJ. Percutaneous management of accesssite complications. Cathet Cardiovasc Interv 2002; 57:12–23.
87. Sicard GA, Schier JJ, Totty WG et al. Thrombolytic ther-apy for acute arterial occlusion. J Vasc Surg 1985; 2: 65–9.
88. NIH Consensus Development Conference: thrombolytictherapy in treatment. BMJ 1980; 1: 1585.
89. Cannas S, De Leo A, Marzari A. Anaphylactoid reactionduring administration of tissue plasminogen activator(t-PA). G Ital Cardiol 1997; 27: 278–80.
96 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter06b.qxp 4/5/2007 2:44 PM Page 96

INTRODUCTION
Atherosclerotic carotid artery disease
With the introduction of distal embolic protection(DEP) devices and stents designed for the carotidcirculation, several clinical studies have demon-strated the morbidity and mortality for carotidangioplasty and stenting (CAS) in high-riskpatients with atherosclerotic carotid artery diseaseto be on a par with or better than for carotid end-arterectomy (CEA).1–12 High-risk CAS registriesthat included the outcome of myocardial infarction(MI), unlike the North American SymptomaticCarotid Endarterectomy Trial (NASCET)13,14 andthe Asymptomatic Carotid Atherosclerosis Study(ACAS),15 have reported 30-day rates of MI,stroke, or death ranging from 3.9 to 8.2%.4,5,7,8,10,11,16
The Stenting and Angioplasty with Protection in Patients at High-Risk for Endarterectomy(SAPPHIRE) trial had 5.8% 30-day and 12% 1-yearevent rates, also including MI.12 A review of ourseries of patients at the University at Buffalo hasdemonstrated morbidity and mortality ratesparalleling those of NASCET and ACAS, even ina group of patients undergoing CAS of whom78% would not have qualified for enrolment in
these studies due to anatomic or physiologichigh-risk profiles.17 Low-risk CAS trials are ongo-ing. Nevertheless, from femoral artery punctureto DEP device retrieval and final angiography,potential exists for complications during CAS thatcan be threatening to life, limb, or brain. Manage-ment of these complications can take the effort ofa team that includes neuroradiologists, cardiolo-gists, neurosurgeons, and vascular surgeons,depending on the clinical and technical skill set ofthe individual interventionists. Although delayedneurologic, cardiac, and peripheral complicationscan occur, an acute neurologic event often requiresimmediate intervention or the hope for meaning-ful salvage declines precipitously. Unlike CEA,CAS is usually performed while the patient isawake, which allows continuous neurologic andangiographic assessment and prompt recognitionof potential problems.
Non-atherosclerotic carotid artery disease
Along with atherosclerotic disease, there areother arteriopathies that occur in the carotid ar-tery that, when symptomatic, can be addressed withsimilar tools and techniques as atherosclerotic
7
Carotid stenting complications from the femoral artery to the intracranial circulationRobert D Ecker, Horst Sievert, and L Nelson Hopkins
Introduction • Identifying patients at high risk for complications • Complications of specific interventionalsteps and complications for specific interventional tools • Methods for detecting complications •Treatment of complications • Methods to avoid complications • Summary • Check list for emergencyequipment for interventions in this specific vessel area
CPVI_Chapter07.qxp 4/5/2007 6:25 PM Page 97

carotid stenosis. These pathologies include dis-section, fibromuscular dysplasia (FMD), carotidpseudoaneurysm, and true aneurysm. Thesefour entities can also be faced in the context ofatherosclerotic disease, either as secondary pro-cesses or as complications.
Dissection
Carotid artery dissections can occur sponta-neously or after trauma, including seeminglyminor events or more significant forces, like chi-ropractic manipulation or motor vehicle acci-dents with fracture dislocations. In some patients,both sides can be affected with or without verte-bral artery involvement. The dissection flap canbe associated with significant decrease in flow, orthrombus and occlusion, or can lead to subtle sta-sis of contrast material with essentially normalhemodynamics. Traditionally, carotid dissectionhas been treated with heparin and warfarin ther-apies for two reasons: the majority of patients inlarge retrospective series have done well and,until the maturation of techniques for carotidstenting over the last 10 years, little else wasavailable.18 However, what to do about the patientwith a history of repetitive ischemic attacks orhigh National Institutes of Health Stroke Scale(NIHSS) score on presentation? In this subset ofdissection, primary stenting can be performedsafely.19
The most important aspect of treating a dis-section is identifying the extent of the flap. Doesit extend into the intracranial circulation? Is thedissection an extension of an aortic dissection?An aortic arch run with a 5 French (Fr) pigtailcatheter can usually identify the proximal extentof the dissection. A soft navigable 0.014-inchmicrowire and microcatheter are generally chosento attempt to gain initial access. The wire shouldeasily pass through the dissection into the truelumen. Resistance suggests that the wire or catheteris in the false lumen. When this occurs, the micro-catheter system should be brought well back intothe proximal normal artery and then access reat-tempted. Once access to the distal true lumen is obtained, the distal anatomic boundaries of the dissection can be identified. For dissectionsextending into the intracranial compartment, onlyballoon-mounted cardiac stents were available
until recently. Self-expanding nitinol stents (e.g., NeuroformTM, WingspanTM; Boston Scientific,Natick, MA) are now available that haveextended the application of stenting (albeit off-label) to the treatment of dissections within thetortuosities of the intracranial vasculature.
Acute aortic dissection with great vesselinvolvement carries a high mortality with med-ical and surgical management.20 There are casereports of successful stenting of the great vesselsto the level of the arch.21 We have had one expe-rience with this in an 84-year-old woman withan NIHSS score of 18 who presented with anacute right hemispheric stroke. Cranial com-puted tomographic (CT) perfusion imagingdemonstrated significant hemispheric hypop-erfusion (Figure 7.1a). Angiography demon-strated poor flow to the hemisphere, with initialfilling of the external carotid artery (ECA)branches (Figure 7.1b). After access to the truelumen had been gained, the placement ofoverlapping WallstentsTM (Boston Scientific/Schneider, Minneapolis, MN) resulted inmarked improvement in flow (Figure 7.1c). Atthe time of the 3-month follow-up evaluation,the patient was once again living independently.Suspicion for aortic dissection, based on the clinical history of chest pain prior to the onset of ischemic symptoms, led to the performance of a CT angiogram that demonstrated the dis-section, which was managed conservatively(Figure 7.1d).
Fibromuscular dysplasia
Fibromuscular dysplasia (FMD) is a non-atherosclerotic, non-inflammatory arteriopathyof small and medium size arteries that oftenaffects the renal and carotid arteries.22 Angiogra-phically, it is diagnosed by a distinct beading ofthe artery with alternating areas of dilatationand stenosis. Most often, this finding is of littleclinical significance. However, patients can devel-op secondary dissections and symptomatic steno-sis requiring treatment, often tracking high inthe cervical segment of the carotid artery wherefilters are not easily used, but flow reversal mightbe possible. Soft, trackable self-expanding stentslike the XpertTM (Abbott Vascular, Inc, RedwoodCity, CA; off-label for this indication) can produce
98 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter07.qxp 4/5/2007 6:25 PM Page 98

excellent results, and balloon angioplasty alonecan often be effective without stenting for pureFMD. Patients with Ehlers–Danlos syndrome,especially type IV, as the underlying conditionare a high-risk group for treatment-related mor-bidity and long-term failure, and the decision totreat such patients should be carefully weighedagainst the risks of further vessel dissection.One patient treated recently at the Universityat Buffalo had bilateral, chronic, symptomaticdissections of the carotid artery secondary to
FMD (Figure 7.2a, left). The left-sided lesion wastreated with an Xpert stent without DEP due tothe high location and low risk for embolic phe-nomena; the right side was similarly treatedwith an XpertTM stent (Figure 7.2a, middle). Proximalto the stented region, the artery developed sig-nificant pseudospasm overlying the pre-existingFMD (Figure 7.2a, right). Angioplasty of this regionwas performed with a fair result, and a follow-upangiogram performed the next day showed aremarkably normal artery (Figure 7.2b).
CAROTID STENTING COMPLICATIONS 99
(a) (b)
(c)
(d)
Figure 7.1 (a) CT perfusion image shows severe hypoperfusion of the right hemisphere. (b) Initial angiogram reveals fillingof the ECA before the ICA (left and right: lateral views, at higher magnification on the right). (c) Angiographic images (left,oblique projection; right, AP projection) show improved flow after deployment of overlapping WallstentsTM (BostonScientific/Schneider, Minneapolis, MN). (d) CT angiogram demonstrating an aortic dissection.
CPVI_Chapter07.qxp 4/5/2007 6:25 PM Page 99

Carotid pseudoaneurysm and aneurysm
Carotid pseudoaneurysms, or aneurysms that donot involve all three layers of the arterial wall,can be associated with dissection (acute andchronic) or FMD. Treatment is indicated insymptomatic patients and those with enlarginglesions. Low-porosity self-expanding stentsincluding the WallstentTM, Magic Wallstent® (BostonScientific), and Xact® (Abbott Vascular) can bedeployed across the lesion, and the placement ofone of these stents will often result in thrombo-sis of the lesion. Sometimes two stents are neces-sary. True aneurysms of the cervical portion ofthe carotid artery are uncommon, but can bedealt with similarly. The stent needs to bridgethe aneurysm neck from the distal to the proxi-mal segments of the non-diseased parent artery.As with pseudoaneurysms, two stents are some-times necessary (Figure 7.3a–c).
IDENTIFYING PATIENTS AT HIGH RISKFOR COMPLICATIONS
Patient selection is the most important factor in minimizing complications associated withCAS.23,24 Categories of major risk factors for CAS include medical, neurologic, anatomic, andgenetic arteriopathy. Age is often listed as a risk factor, but it is the anatomic challenges andmedical comorbidities that come with age thatincrease the risk for most patients.25–27 Medically,the major risk factor in patients with carotid
stenosis is MI. Patients with severe left main dis-ease and severe triple vessel disease are at majorrisk for MI. A sudden decline in blood pressureand the onset of severe bradycardia presentmajor risk for MI in patients with severe left maincoronary artery disease and/or severe triple-vessel disease. In this group, if CAS before coro-nary intervention is necessary, minimal or nodilation of the stent after deployment will gener-ally avoid major hemodynamic swings, and thepatient can be sent for cardiac surgery, with aplan made for follow-up and retreatment asnecessary. Neurologic risk increases with recentlarge infarction, crescendo transient ischemicattacks (TIAs), and stroke in evolution. Largeinfarctions present a significant risk for hemor-rhage.28,29 Traditionally, patients with large infarc-tion are allowed to ‘heal’ their stroke for 6 weeksprior to intervention. Patients with active TIAsor stroke in evolution need to be treated but arehigher risk for neurologic injury.
Patients with high-risk anatomy may includethose with calcified tortuous aortic arches, tortu-ous and severe iliofemoral disease, and proxi-mal or distal tortuosity of the common carotidartery (CCA) or internal carotid artery (ICA).Patients considered at high risk for CAS includethose with long, irregular or concentrically cal-cified stenosis, pseudo-occlusion, string sign,carotid artery kinking, and intraluminal throm-bus. Not all high-risk patients can be avoided.For example, treatment should likely be delayed
100 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b)
Figure 7.2 (a) Left, preoperative angiographic image shows right ICA with FMD and dissection. Middle, right ICA afterstent placement (Xpert, Abbott Vascular, Inc, Redwood City, CA). Right, severe proximal pseudospasm post-stenting. (b) 12 hours after stand-alone angioplasty (left, AP view; right, lateral view).
CPVI_Chapter07.qxp 4/5/2007 6:25 PM Page 100

for 6 weeks in a patient who has a large completedinfarction with territory still at risk. Conversely,treatment should promptly be undertaken in apatient in need of urgent coronary artery bypassgrafting (CABG) who presents with crescendoTIAs and an MI. Each case should be evalu-ated on an individual basis. For patients who are candidates for carotid intervention, it should beremembered that CEA remains a safe and effec-tive operation if CAS is thought to be too risky.In fact, CEA and CAS are amazingly comple-mentary procedures; in those situations for whichone is high risk, the other is usually feasible withacceptable risk. It is important to remember that
backing out of a CAS procedure is rarely a prob-lem for the patient, whereas persisting in the faceof technical challenges may result in an avoid-able stroke.
Creative endovascular solutions can be foundeven in high-risk patients when treatment isdeemed necessary. For patients with intraluminalthrombus and symptomatic carotid disease, thetraditional treatment has been heparin and war-farin therapy with re-evaluation in 6 weeks to 3 months. In four patients with multiple episodesof TIAs, we have used a trapping technique withproximal and distal balloon occlusion with goodsuccess (Figure 7.4a–e). Flow reversal devices,
CAROTID STENTING COMPLICATIONS 101
(a) (b)
(c)
Figure 7.3 (a) True carotid aneurysm (left, AP view; right, lateral view). (b) Three months after the placement of a singleWallstentTM with persistent filling (left, AP; right, lateral). (c) The placement of overlapping WallstentsTM resulted incomplete occlusion of the aneurysm (left, lateral; right, AP).
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 101

102 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b)
(c) (d)
(e)
Figure 7.4 Internal trapping and stenting of symptomatic carotid stenosis with intraluminal thrombus. (a) MR imageshowing small left frontal infarction. (b) MR angiogram showing critical left ICA stenosis. (c) Angiogram with critical stenosisand flame-shaped intraluminal thrombus. (d) Post-stenting cervical angiogram. (e) Post-stenting MR image showing no newareas of stroke.
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 102

CAROTID STENTING COMPLICATIONS 103
which are just becoming clinically available inthe United States, may prove useful in this set-ting and in the context of kinks that make land-ing of a DEP unfeasible.30 As reviewed earlier,patients with Ehlers–Danlos syndrome and FMDprovide a great challenge because of the poor tol-eration of their vessel walls to manipulation withwires and balloons. The decision to treat sucharteriopathies should be carefully considered.
Low-risk patients are those with either asymp-tomatic or single retinal or hemispheric TIAswith no previous cardiac history.31 Anatomically,type I aortic arches with both straight proximaland distal anatomy provide the easiest anatomicsubstrate for CAS. Many of these patients havenot been treated in the carotid stenting pool thathas been reserved for ‘high-risk’ patients.Ongoing low-risk trials like the AsymptomaticCarotid Stenosis, Stenting versus EndarterectomyTrial (ACT I) will determine how these patientsfare with CAS when compared with CEA.
COMPLICATIONS ASSOCIATED WITHINTERVENTIONAL STEPS AND TOOLS
Patient preparation for CAS
Many of the risks associated with CAS can bemitigated pre- and periprocedurally. Patientsshould receive a loading dose of aspirin and clopi-dogrel at least 72 hours before the procedure.Generally, the loading dose is 600 mg of clopido-grel and 650 mg of aspirin, with the daily dosesbeing 75 mg and 325 mg, respectively. The inter-ventional suite should have dedicated nurs-ing personnel familiar with all the equipment,devices, and pharmacologic agents, critical caremanagement, and the disease process treated.Guide catheters are flushed with normal saline(0.9% NaCl) with 5000 units of heparin in eachpressure bag. The air will have been activelyremoved from each flush bag. Alternatively, thecatheters should be flushed frequently. Lidocaine(1%) is percutaneously administered for localanesthesia, and midazolam (1 mg) and fentanyl(50 �g) may be intravenously administered forsedation. Femoral access is gained with a 19 gaugeneedle and a single-wall puncture technique and a 5 or 6 Fr groin sheath. A femoral artery
angiographic run is then obtained. Heparin (50–60units per kg body weight) is administered toobtain an activated coagulation time of >250 sec-onds. Alternatively, direct thrombin inhibitorssuch as bivalirudin may be used. Guide catheteraccess is gained directly with a 6 Fr guide catheter(for example: Envoy®, Cordis, Miami Lakes, FL)for lesions that can be treated in general with astent that is 8 mm or less in diameter (for exam-ple, a WallstentTM); for 8 to 10 mm lesions, a 6 Frguide sheath (Cook Shuttle select; Cook, Inc,Bloomington, IN) is brought into the CCA withan exchange maneuver or over slip catheter(Cook). Another option is to use an appropriatecoronary guide catheter.
Overview of basic technique from the femoralartery to the common carotid artery
Femoral artery access
The femoral artery approach is most commonlyused for CAS. As approximately 33% of patientshave both significant carotid artery disease andsevere symptomatic peripheral vascular dis-ease,32,33 the interventionist should also be famil-iar with radial and brachial approaches. Inaddition, femoral artery complications are likelymore common in this population as many havefemoral artery disease. Access site complicationsdo not make the surface of primary or secondaryendpoints in most of the major carotid stent tri-als, therefore the incidence is not clearly known.Other chapters of this book will focus onfemoral artery access complications and theirmanagement.
Aortic or brachiocephalic access
In the process of gaining access to the CCA witha guide catheter, injury to any of the major aor-tic branches and brachiocephalic vessels canoccur, resulting in dissection or thrombotic occlu-sion. Many patients with carotid stenosis havesevere atherosclerotic debris throughout theirarterial trees. Care should be taken when gainingaccess to the proximal carotid artery. Minor, non-flow-limiting dissections of the proximal bra-chiocephalic vessels can be observed, regardless
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 103

of whether the patient is receiving a heparininfusion. If concern exists, but the decision ismade not to stent a dissection flap, repeatedangiography within 24 hours may be indicated.In flow-limiting situations, the lesion should bestented. A microcatheter and soft wire can beused to locate the distal true lumen if wire accessis lost, with angiography performed via the micro-catheter to ensure that the distal wire is in the truelumen.
Stroke can occur at any point after femoralartery access. If a patient develops a sudden neu-rologic change, the diagnoses entertained shouldinclude hemorrhage and ischemia – most oftendue to embolism. Quick access should be gainedto the vessel suspected of harboring the prob-lem, based on the findings of the neurologicexamination. If the patient’s airway is compro-mised, intubation should be performed. If novessel cut-off or slow flow is appreciated, hemor-rhage must be ruled out, and the patient shouldundergo a cranial CT scan. The specifics of neu-rologic rescue will be discussed later.
Guide catheter placement: external carotidartery perforation and embolism
The ECA and its branches are often used tosupport a guidewire during the exchange of adiagnostic catheter for a guide sheath or catheter.This maneuver is felt to be safer than exchangingdevices within the CCA because it preventspremature crossing of the lesion and showeringof emboli. Additionally, it gives the purchaseessential in the setting of a difficult aortic arch thatmight not be otherwise accessible. In our experi-ence of more than 1500 stenting procedures, wehave had five ECA branch artery ruptures sec-ondary to wire perforations in four cases and amisdeployed PercuSurge embolic protectionballoon (Medtronic, Minneapolis, MN) in an addi-tional case.34 The four wire perforations were secondary to advancement of the stiff exchangewire through the facial artery (two cases) and thelingual branch and artery to the sternocleidomas-toid (one case each). A brief description of themanagement of these complications follows.
The first patient was electively intubated with-out endovascular intervention, and the hematoma
tamponaded the bleeding spontaneously. Thesecond patient required an emergent tracheos-tomy because of massive swelling of the tongue(Figure 7.5a). In the third patient, the artery to the sternocleidomastoid was accessed with a0.014-inch microcatheter, and the branch arterywas occluded with N-butyl-2-cyanoacrylate(NBCA). The fourth patient’s hematoma wasnoted only at the conclusion of the procedure andhand pressure on either side of the cheek stoppedthe progression of the hematoma. In the fifthpatient, a PercuSurge balloon was inadvertentlyplaced in the ascending pharyngeal artery,which was aligned with the ICA and originatedfrom the carotid bulb. Upon inflation, the arteryruptured and contrast extravasation could beseen (Figure 7.5b). A microcatheter was used toaccess this artery, and it was occluded with coils(Figure 7.5c).
Some lessons have been learned from thesecases. First, large branches of the ECA, preferablythe internal maxillary artery or occipital artery,should be used for exchange maneuvers. Second,carotid artery branch rupture can lead to life-threatening airway emergencies. A tracheostomyset should be available in the interventional suite.A physician who can intubate the patient or per-form an emergency tracheostomy to establish anairway should be readily accessible. Third, carotidinterventionists need to be comfortable withmicrocatheters and embolic agents like NBCA,coils, silk, gel foam, and even autologous clot, asa means to stop bleeding from perforations.Although a rare event, ECA branch artery perfo-ration can quickly lead to airway compromise ifnot recognized and treated promptly.
An equally rare event is ECA embolism tocarotid ophthalmic collaterals, which may leadto retinal embolism and blindness. Anatomi-cally, embolization can occur through middlemeningeal and superficial temporal collateralsto the ophthalmic artery and/or via direct ICAreconstitution associated with embolic phenom-ena or retrograde embolization through the ECAto ophthalmic and retinal branches. Wilentz et alstudied 188 consecutive patients undergoingCAS with the Theron-type DEP system (in whichdebris is flushed into the ECA) or the Percu-Surge system with careful funduscopy, fluores-cein angiography, and visual field testing.35
104 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 104

Overall, 6 of 118 patients had retinal emboli,which was symptomatic in 2 patients (1.7%).Looking at the two different systems, 13.2% (5 of38 patients) treated with the Theron system hademboli, versus 1.25% of the PercuSurge group.In fact, in the setting of ICA occlusion, amauro-sis fugax from the ECA collateral through theophthalmic artery retrograde to the retinal arterycan occur and responds well to carotid revascu-larization.36 The predominance of the literatureregarding ECA revascularization is from theCEA literature.36–38 Embolic protection should beused if possible during ECA angioplasty andstenting.
Once visual loss has occurred, angiographyshould be obtained to determine the location ofthe occlusion. Central retinal artery occlusionscan sometimes be opened with antiplatelet agentsinfused into the ophthalmic artery. If the oph-thalmic artery is patent, the agent can be directlyinfused. If a shower of emboli is suspected,
administration of eptifibatide as a bolus dose(180 �g/kg) and a 23-hour infusion (2 �g/kg forat least 12 hours) or other IIb/IIIa antiplateletagent is indicated.
Distal embolic protection: from device deployment to retrieval
The technique of DEP has lowered morbidityand mortality rates associated with CAS. Addi-tionally, DEP devices provide excellent plat-forms on which to perform CAS. However, eachstep of CAS from crossing the stenosis toretrieval of the DEP device has potential forcomplication. Transcranial Doppler (TCD) datahave documented hits indicative of embolism atall stages of CAS; however, most TCD-detectedemboli are clinically silent. On the basis of TCD data in which protected stenting with thePercuSurge device was compared to unprotectedstenting, the highest-risk maneuvers for embolic
CAROTID STENTING COMPLICATIONS 105
(a) (c)
(b)
Figure 7.5 (a) Extravasation from the lingual artery caused by exchange wire. (b) Perforation of ascending pharyngeal arteryfrom PercuSurge balloon (Medtronic, Minneapolis, MN). (c) Coils in ascending pharyngeal artery with no extravasation.
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 105

risk in unprotected stenting, in order from lowestto highest, were predilation angioplasty, stenting,and postdilation angioplasty.39 In the PercuSurge-protected stenting group, guide sheath place-ment, guidewire manipulation, and deflation ofthe device were high embolic periods.39 DEP sig-nificantly lowered the risk of hits documentedby TCD imaging. Stenting performed in conjunc-tion with filter devices for DEP (Filterwire EX®,Boston Scientific; Accunet®, Guidant, Santa Clara,CA) in a series of 10 patients was monitoredwith a multifrequency TCD imaging system.40
The system utilized was capable of distinguish-ing between gaseous and solid emboli. DuringDEP deployment, more than 8000 microemboliwere detected, with more than 40% being solid.During the stenting procedure, more than 7000microemboli were detected, again with over40% being solid. No patient developed clinicalsequelae. Microemboli occur even in the gentlesthands, but with good patient selection and tech-nique, the occurrence of symptomatic embolicphenomena can be kept low.
In the US market, five devices FDA approvedfor carotid use: the Fiterwire EX® and theFilterwire EZTM (with the NexStert® [BostonScientific]), the AccunetTM filter (with theAcculinkTM stent)(Guidant), the EmboShield®filter (with the Xact® stent) (Abbott Vascular),and the SpiderTM filter (ev3, Plymouth, MN).There are at least four other non-approved com-mercially made filters. Additional types of embolicprotection devices include balloon occlusioncatheters (PercuSurge; TriActive System, KenseyNash, Exton, PA), proximal occlusion devices(MOMA, Invatec, Brescia, Italy), and flow reversaldevices (Parodi Anti-Embolic System, WL Gore& Associates, Flagstaff, AZ).
The indication for proximal versus distal protection has not been determined. Logically,intraluminal thrombus, soft plaque, and poor dis-tal landing zone would be indications for proxi-mal protection. The results of the EuropeanImaging in Carotid Angioplasty and Risk ofStroke (ICAROS) study showed that gray-scalemedian (GSM) scores of 25 or less (representingechogenic plaque) are associated with higherembolic potential.41 The investigators created aprospective registry of 418 CAS cases from 11 cen-ters and recorded GSM scores preprocedurally.
Eleven of 155 (7.1%) patients with GSM of 25 orless had strokes versus 4 of 263 (1.5%) patientswith GSM greater than 25 (p value of 0.005).Taking this one step further, the authors vali-dated the use of DEP in patients with GSMgreater than 25 (p = 0.01), but not in those withGSM of 25 or less. For those patients, stentingwith proximal embolic protection devices orCEA may prove safer.
This portion of the chapter will focus on com-plications from filter DEP devices as they areused most often for embolic protection. In ourpractice, the PercuSurge device is the most oftenused alternative to filters, with the most com-mon indications being ICA less than 2.8 mm indiameter, intraluminal thrombus, and acuteocclusion (i.e., where clot burden is likely highand might potentially overwhelm a filter). Whencrossing a carotid lesion, plaque dissection andembolization can occur. In the case of dissection,the patient is already therapeutically heparinized,and if the true lumen can be entered with the DEP,it should be crossed and stented along with thestenosis. If the lesion cannot be crossed with theDEP, a microwire and catheter should be used tocross the lesion. The true lumen is identified witha microcatheter angiographic run, and the DEPis then brought into position. The EmboShield®and SpiderTM filters are ideal for such situations.The EmboShield® platform is a microwire-basedfree-floating filter with the filter brought intoplace after passage with the microwire; the SpiderTM
filter is delivered through a microcatheter afterpassage of a lesion with a microwire and micro-catheter. Embolic phenomena associated withcrossing the lesion require quick completion ofthe cervical carotid stenting portion of the proce-dure in order to gain access to the distal intracra-nial circulation. Inability to cross a lesion shouldlead to reconsideration of the procedure and con-sideration of the feasibility of endarterectomy.
Ideally, the filter should be deployed in astraight segment distal to the stenosis, wellopposed to the carotid wall. Predeployment ofthe filter can occur in the lesion inadvertently.Most often, this occurs secondary to the operatoradvancing the wire but not the housing sheath ofthe DEP. When unsheathing a filter, if the filterwire is not fixed as the sheath is retracted, theentire system can be dragged through the lesion.
106 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 106

In this case, the DEP should be recaptured andredeployed distally. With monorail deliverysystems, such maneuvers are not always possi-ble. Pushing the filter back into the ICA abovethe lesion is often a better choice than draggingthe entire system through a lesion. A secondarystrategy for retrieval is to exchange out the initialDEP sheath and to run a 4 Fr angled catheter upthe wire and recapture the misdeployed device.
Loss of the filter device is rare, but possible.With the EmboShield®, which is a free-floating fil-ter, the striped wire provided in the package mustbe used because it has a tapering segment that actsas a stop for the filter. Filter devices have beensheared off with recapturing. In these dire settings,the options include snare retrieval into the guidecatheter, stenting the filter against the vessellumen, or operative retrieval. If the DEP is in thebony segment of the skull base, operative retrievalmay be impossible. Before any maneuvers areundertaken to retrieve a lost filter or other detritus,consideration should be given to arresting flow tem-porarily to avoid distal intracranial embolization.
In arteries in which a kink in the CCA or ICAhas been moved cranially, with significant move-ment of the filter DEP device, and in some par-ticularly sensitive arteries, carotid vasospasm canoccur. Generally, this is not a clinically or anangiographically significant problem, but strokehas been described in conjunction with suddensevere spasm just after the deployment of anAngioGuardTM embolic protection device (Cordis).42
Three patients in one of the initial series using theEmboShield® developed spasm, which was flowlimiting in two patients.43 In non-flow-limitingspasm, the case should be completed and the fil-ter recaptured. Generally, the spasm clears afterthe passage of a few minutes. Contrast materialremaining within the arterial wall should causeconcern for dissection. In flow-limiting situationsor if significant time has passed and the spasmpersists, intra-arterial nitroglycerin (100–200 �g)is usually effective. Distal dissection at the level of the filter can occur, more commonly sowith the PercuSurge device than with the filterdevices. For cases of small, asymptomatic, andnon-flow-limiting dissections, clinical observationis recommended. Stenting is warranted if thedissection is symptomatic or flow limiting. Spasmalso occurs when a kink in the carotid artery is
moved cranially by the DEP and guide catheter.This can be ignored as it will resolve with deviceretrieval and often resolves after stenting andpostdilatation angioplasty.
Predilatation angioplasty, as mentioned earlier,is a low-risk portion of the procedure. Generally, a3.0 or 3.5 × 30-mm balloon is used. Attentionshould be paid to blood pressure reduction due tocarotid baroreceptor response. Patients who donot have pacemakers, are not undergoing CASpre-CABG, and have initial baseline heart rates ofless than 70 beats per minute may benefit from0.75 mg of atropine given at least 2 to 3 minutesbefore balloon inflation. Postdilatation angio-plasty is a high risk for both embolic phenomenaand severe baroreceptor response. Balloon size ischosen based on the measurement of the stent in the distal ICA; the balloon is undersized by 0.5 mm. Angioplasty balloons in vessels in patientsundergoing CAS pre-CABG are generally slightlyunderdilated to avoid a severe baroreceptorresponse. Dopamine or phenylephrine should beloaded at the start of the case for rapid adminis-tration if the patient’s blood pressure drops sig-nificantly. It is important to remember that atropinemay mitigate against severe bradycardia but willhave no effect on hypotension.
Immediate complications associated withstenting are unusual. With dual antiplatelettherapy for 4 weeks and with arteries larger than3 mm, acute and subacute thrombosis is uncom-mon. Subacute thrombosis has occurred twice atthe University at Buffalo Neurosurgery practicewhen cardiac surgeons stopped the patients’antiplatelet medications within the first 2 weeksbefore CABG. Aspirin use was discontinued beforeurologic surgery in another patient 3 monthsafter stenting of a carotid dissection with stentsextending from the proximal segment of the ICAto the petrous segment of the ICA, and the stentbecame occluded; some degree of abnormalendothelialization was likely present in this case,and a hypercoagulation state may have beenimplicated. A dual antiplatelet regimen 4 weekspostprocedure and aspirin use for lifetime appearsessential. Drawing on the cardiology literature,early stent thrombosis is likely due to a dissectionunrecognized at treatment or an undersized orexpanded stent; late thrombosis is likely due tostent mismatch to the artery, hypersensitivity,
CAROTID STENTING COMPLICATIONS 107
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 107

abnormal endothelialization, or poor compliancewith antiplatelet medications.44 The stent shouldbe sized to the CCA and the size of the postdi-latation balloon based on the measurement ofthe stent in the ICA.
If arterial occlusion occurs acutely during theprocedure, the diagnosis includes severe spasm,dissection, thrombosis from plaque and/orplatelet aggregation, and a filter that is filled with embolic material. As long as there is no dis-section, the spasm will resolve. Nitrates can begiven, as mentioned earlier. Treatment is requiredfor an occlusive dissection. A microcatheter andmicrowire need to be brought past the flap intothe true lumen to accomplish this. If the clot hasnot embolized to the intracranial circulation andthe patient is asymptomatic, consideration maybe given to heparinizing the patient overnight,checking the angiographic collateralization, andperforming stenting later. In the acutely symp-tomatic patient, stenting after the administrationof a lytic agent and IIb/IIIa inhibitor may be nec-essary. If the filter is filled with embolic debris, autility catheter can be used to perform a suctionthrombectomy and the filter should be carefullycaptured and brought through the stent so as tonot disturb the captured debris. Successful out-comes have been reported for a small series ofpatients undergoing operative rescue after acuteor subacute stent thrombosis.45 However, if theexperience with emergency CEA for treatmentof acute carotid occlusion is a guide, the associ-ated morbidity and mortality is greater than20%.46 The hope is that with CAS, where wehave the ability to visualize and access the entirecerebral vascular system, and with newly evolv-ing techniques for treatment of acute stroke, wewill have better salvage procedures and successwith endovascular techniques.
Recapturing the filter device is the final tech-nical step of CAS with DEP. When this step goessmoothly, it is effortless; however, when accessingthe filter with the recapturing sheath proves dif-ficult, dissections, stent movement, and shearingof the filter device can occur. The most commonsetting for difficulty in recapturing the filter iswith an open-celled stent on a significant curveor with the DEP parked in a tortuous distal vessel.A systematic approach to recapturing maneu-vers will generally lead to successful recapture:
1. Advancing the guide catheter into the stentwill bias the wire away from the stent wall,allowing the recaptured sheath to pass.
2. Having patients inhale deeply or turn theirheads opposite the direction of the vesselcurve can help straighten the curve or elon-gate the artery enough for passage of thesheath. More aggressively, pressing on thestent in the patient’s neck will also changethe bias of the wire.
3. If the sheath is impeded by a stent tine, redi-latation with a larger balloon or spinningthe sheath with forward pressure will helpflatten the tine or allow passage of thesheath.
4. If other maneuvers fail, a 4 or 5 Fr angledglide catheter can be passed over the DEPwire and used to capture the filter.
Intracranial complications
The intracranial complications of carotid stent-ing can be grouped into large vessel occlusion,shower of emboli, and hemorrhage. In any patientwith an acute or delayed neurologic change notexplained at the cervical level, all three sourcesshould be entertained. In the acute setting, acerebral angiogram should be performed to lookfor vessel cut-off or slow flow and emptying. If aclear large vessel cut-off can be seen, an immedi-ate attempt should be undertaken to recanalizethe occluded vessel. A microcatheter (0.014-inchlumen or larger) should be brought through thelesion to confirm patency of the distal vessel andconfirm the length of the occlusion. In cases ofacute stroke at the University at Buffalo, we havebeen using the 021-ID microcatheter for the Merci®device (Concentric Medical, Mountain View, CA)as the initial catheter to obviate the necessity for additional exchange maneuvers. One or two passes with the Merci® retriever should beattempted (Figure 7.6a,b). If this device is notavailable, thrombolytics can be used initially.There is some evidence that IIb/IIIa inhibitorsgive additive benefit.47 Other devices that can beused to open occlusions of large intracranial ves-sels (M1 segment of the middle cerebral artery,A1 segment of the anterior cerebral artery, P1segment of the posterior cerebral artery, basilarartery, carotid artery) include balloon angioplasty,
108 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 108

snares, large microcatheters, and stents48 (Figure7.7a–c).
In settings other than clear large vessel cut-off,if the DEP has already been deployed, the proce-dure should be completed and a cranial CT scanobtained. Intracranial hemorrhage (ICH) can
present as slow flow and, prior to expansion ofthe hematoma and development of significantmass effect, it may appear as a shower of emboli.If an angiogram documents slow flow and the CTis negative for hemorrhage, IIb/IIIa antiplateletagents are administered as a bolus dose followed
CAROTID STENTING COMPLICATIONS 109
(a) (b)
Figure 7.6 (a) M1/M2 embolus after endarterectomy. (b) Opening of middle cerebral artery with Merci® retriever (Concentric Medical, Mountain View, CA).
(a)
(b)
(c)
Figure 7.7 (a) Superior and inferior M2 occlusion. (b) Opening of M2 divisions with stents. (c) Wires in M3 branches andunsubtracted view demonstrating both stents.
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 109

by a 23-hour infusion. The patient’s blood pres-sure should be controlled tightly, with a systolicblood pressure of less than 160 mmHg. If a hem-orrhage is identified (Figure 7.8a–c), the systemicheparin anticoagulation should be reversed withprotamine, the blood pressure tightly controlled,and a repeat CT scan obtained in 6 to 12 hours.Life-threatening hematomas in neurologicallysalvageable patients can be evacuated. In the set-ting of hematoma expansion but no operativeindication, factor VII can be given to stop theprogression of the hemorrhage. According tothe trauma literature, most ICHs expand withinthe first 12 hours.49 Strong consideration shouldbe given to stopping the patient’s dual anti-platelet therapy. The source of reperfusion hem-orrhage remains debatable; some advocate ahyperperfusion origin, whereas others havesuggested hemorrhagic conversion of a showerof emboli. In different cases, both sources arelikely possible. However, once the hemorrhagehas occurred, the treatment is identical.
Occasionally, a patient will present with anintracranial aneurysm ipsilateral to a criticallysevere carotid stenosis. In a review of NASCETdata, 1 of 90 patients with aneurysms knownbefore the performance of CEA experiencedaneurysm rupture (at 6 days post CEA).50 On the basis of the findings of the InternationalStudy of Unruptured Intracranial Aneurysms(ISUIA),51 the following approach seems ratio-nal: for patients with unruptured, asymptomaticaneurysms smaller than 6 mm, CAS can beperformed prior to any aneurysm treatment;and for patients with unruptured, symptomaticaneurysms 6 mm or larger, the aneurysm shouldlikely be treated before CAS is performed.
Systemic complications
Systemic complications of endoluminal carotidintervention include seizures, MI, contrast mate-rial nephropathy, and contrast material allergy.If a patient has a seizure during angiography,
110 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a)
(b)
(c)
Figure 7.8 (a) High-grade symptomatic carotid restenosis. (b) Good revascularization with angioplasty and stenting. (c) Massive reperfusion hemorrhage.
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 110

attention should first be paid to basic life supportand pharmacologic seizure control consisting ofthe establishment of an airway and administra-tion of lorazepam (2 mg) and a phosphenytoinload (18–20 mg/kg body weight). The differentialdiagnoses include embolism (air, necrotic debris),ischemia from vessel occlusion or vasospasm,ICH, hyperperfusion, and contrast sensitivity(which is less common with lower osmolar loadagents). After the seizure has been aborted andcontrol of the airway established, angiographyshould be performed and a CT scan obtained andthe differential diagnosis worked through until asource is identified. An electroencephalogram isperformed if necessary.
The rate of MI in the SAPPHIRE trial was 2.5%at 1 year, which was statistically lower than therisk for MI during CEA.12 One of the major bene-fits for CAS in the major studies completed isthe lower incidence of intraprocedural and post-procedural MI. However, MI still occurs in theCAS population. Standard measures that includenitrate infusion, beta blockade, and heparinadministration should be initiated if MI is diag-nosed by obtaining cardiac enzymes and electro-cardiogram. A cardiologist should be consultedearly, because those patients with Q-wave infarc-tion seen on the electrocardiogram usually willrequire acute coronary revascularization.
Acute allergy to contrast material is anothersetting in which airway safety is ensured. The patient should be intubated if necessary.Methylprednisolone (120 mg given parenterally)and epinephrine (1 mg) are administered as nec-essary. Patients with known contrast mediaallergies are treated with 30 mg of prednisone at12 hours and then 1 hour before the procedure,along with 50 mg of benadryl.
The exact incidence of contrast nephropathyis not clear. In one study of patients with creati-nine levels less than 1.5 mg per deciliter, only8% of patients had an increase in their level of0.5 mg per deciliter, and none had rises greaterthan 1.0 mg per deciliter with angiography. Otherdata suggest that contrast nephropathy is thethird most common cause of renal failure in hospitalized patients.52 Certainly, the state of apatient’s renal function prior to angiography isthe greatest determinant of post-treatmentrenal failure. A recent exhaustive review of
contrast nephropathy52 gives a few practicalguidelines for renal prophylaxis in patientswith pre-existing elevated creatinine levels.Hydration with normal saline (0.9% NaCl) for2 to 12 hours at a level of 1 ml/kg/h before con-trast administration is recommended. Low dosesof low osmolar contrast agents like iodixanolshould be given. Doses greater than 5 ml/kg ofbody weight divided by serum creatinine levelare associated with higher risk.
METHODS FOR DETECTING COMPLICATIONS
As reviewed in the previous section, the physio-logic and neurologic examination of the patientwhile on the angiography table is the first steptaken to detect a complication. Comparison ofthe initial control cervical and intracranial angio-graphic images with the final angiographicimages obtained, with the patient still on thetable, is the second step. Angiographically, ves-sel cut-off and slow intracranial flow during thecapillary phase can suggest a shower of embolior focal embolic occlusion. When there has beenneurologic change and no clear vessel cut-off,CT scanning is required to rule out intracranialhemorrhage. All patients should undergo repeatcarotid duplex imaging within 24 hours post-procedure as a baseline measurement; however,this has rarely, if ever, been the means for identi-fying a complication. If CT scanning is negativefor hemorrhage, any patient experiencing TIA orstroke systems during the periprocedural periodis brought to the angiogram suite for a repeatstudy. For systemic complications, these shouldbe identified and the usual pathways followed asdescribed above, i.e., electrocardiogram, enzymesfor suspicion of MI, CT scan, anti-epilepticagents, and electroencephalogram for seizureactivity.
TREATMENT OF COMPLICATIONS
The site- and equipment-specific complications havebeen reviewed earlier. However, some generalcomments can be made regarding managementof complications by frequency. A recent review ofthe data for more than 300 patients who under-went CAS at the University at Buffalo Depart-ment of Neurosurgery has shown morbidity
CAROTID STENTING COMPLICATIONS 111
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 111

and mortality in line with the NASCET andACAS standards of <6% major morbidity andmortality for symptomatic lesions and <3% forasymptomatic lesions.17 Among those complica-tions that occurred most commonly, shower ofemboli, reperfusion hemorrhage, and MI wereresponsible for the major morbidity and mortal-ity. One patient had femoral artery shut downcaused by the placement of a closure device thatrequired open vascular repair.
Embolic showering is generally detected by achange in the patient’s neurologic examinationon the angiography table including, but not lim-ited to, hemiplegia, neglect, or speech difficulty.Angiographically, there will be slowing in thecapillary phase. If CT scanning demonstrates nohemorrhage, these patients are brought back tothe angiogram suite and a bolus dose of eptifi-batide or another IIb/IIIa inhibitor is infusedinto the appropriate hemisphere, and a drip ishung for a 23-hour infusion. Most patients willimprove. Frank vessel drop-out has not oftenoccurred, but would require microcatheteraccess of the lesion and either thrombolysis, Merci®retrieval, or stenting, as mentioned.
The diagnosis of intracranial hemorrhagerequires heparin reversal and is often a fatalevent. Severe hypoperfusion and hemorrhagicallyconverted stroke are the most common causes.Hemorrhage may necessitate intracranial pres-sure monitoring, drainage of CSF, or operativeremoval. One interesting case at the Universityat Buffalo occurred in a 45-year-old man with asymptomatic left carotid artery dissection andno significant infarction on preoperative imaging. After loading doses of aspirin and clopi-dogrel had been administered, the patient wasbrought to the angiography suite (Figure 7.9a).After femoral artery access was obtained, suffi-cient heparin was administered to produce anactivated coagulation time of >250 seconds. A 6 Fr Cook shuttle was then brought into the left ICA. The lesion was crossed with a PVS wire(Boston Scientific/Precision Vascular Systems,West Valley City, UT) and s110 catheter (BostonScientific) and then an AllstarTM 14-inch wire(Guidant) was brought into the petrous segmentof the carotid artery. Overlapping XpertTM stentswere placed across the dissection flap with excel-lent angiographic results (Figure 7.9b). The patient
did well until 8 hours postprocedure when hecomplained of sudden worsening of his pretreat-ment headache and quickly progressed to clinicalherniation. After CT scanning revealed non-confluent temporal, paracentral, and basal gan-glia hemorrhages (Figure 7.9c), the patient wasbrought to the operating room and underwent acraniotomy with removal of temporal clot. Hemade a fair recovery after several weeks of reha-bilitation therapy. Because of his mild preopera-tive symptoms, repeat magnetic resonance (MR)imaging was not obtained before the procedure,which may have demonstrated larger areas ofischemic injury with petechial hemorrhage thanclinically suspected.
METHODS TO AVOID COMPLICATIONS
The best way to avoid complications of CAS is topredict in the preoperative setting who is not agood candidate. Patients with asymptomaticdisease who have concurrent severe medicalcomorbidities (i.e., ejection fraction <30%, activecardiac ischemia, severe chronic obstructive pul-monary disease, or severe peripheral vasculardisease) are best left alone. Although there aremany techniques to gain access to type III arches,e.g., Simmons 2 or 3 guide catheters (TerumoMedical, Somerset NJ), wire obturator combina-tions like a Vitek (Cordis) or slip catheter (Cook)with a guide catheter, and balloon purchasefollowed by guide catheter placement, if theoperator is inexperienced or there is no clearindication for CAS, these patients are generallybetter with medical management or CEA. Severecalcific stenoses with proximal and distal kinksare well treated with CEA and can provide agreat challenge for CAS.
After the decision has been made to treat withCAS, appropriate guide catheter choice is criti-cal. In a challenging proximal arch, a 6 Fr angledEnvoy® catheter can be a good choice, so long asa stent longer than 8 mm is not needed for ade-quate coverage of the lesion. For short CCAs ortight stenoses with kinks, a stiffer guide catheterlike a Cook shuttle is an excellent choice. Appro-priate dosing of heparin and loading of antiplateletmedications is essential. Use of platelet aggre-gometers, although these devices are relativelynew, may well help to lower the embolic risks of
112 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 112

stenting by identifying those patients who willnot benefit from standard antiplatelet regimens.Technical problems with filters and stents can bebest avoided by understanding the mechanics ofall the devices before performing stenting proce-dures. Most often, technical problems relate toguide catheter access, and the inability to cross alesion with a stent or to recapture a filter devicecan often be solved by simply bringing the guidecatheter higher. The details of bailout techniqueshave been reviewed earlier in this chapter.
SUMMARY
Carotid artery angioplasty and stenting can beperformed with low morbidity and mortality.However, complications can occur that canquickly take a patient from normal health tosevere neurologic impairment or death. UnlikeCEA in which a few simple tools are used, a
detailed understanding of the complexities of theCAS systems is necessary. Furthermore, as manyof the patients have blood vessel disorders andmultisystem disease, systemic complications likeMI and renal failure are possible. Good mentor-ing by an experienced operator, careful patientselection, an understanding of the limitationsand benefits of each device, and meticulous carebefore, during, and after the procedure will max-imize the potential for excellent clinical results.
CHECK LIST FOR EMERGENCY EQUIPMENTFOR INTERVENTIONS IN THIS SPECIFICVESSEL AREA
The following is a list of emergency supplies forCAS complications in our interventional suite:
• protamine; reteplase, eptifibatide• epinephrine (for allergic reactions)
CAROTID STENTING COMPLICATIONS 113
(a)
(c)
(b)
Figure 7.9 (a) Angiogram demonstrating the extent of the flow-limiting dissection. Left, lower cervical (AP view); right, highercervical (lateral view). (b) Immediately after the deployment of overlapping XpertTM stents (Abbott Vascular, Inc, Redwood City,CA). Left, AP view; right, lateral view. (c) CT images demonstrating non-synchronous, non-confluent ICHs. Left, left temporal ICHand subarachnoid hemorrhage; middle, left temporal and left basal ganglia hemorrhages; right, left parietal ICH.
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 113

114 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
• nitroglycerin (for catheter-induced spasm,angina)
• atropine (for treatment of bradycardia orasystole)
• lorazepam and phosphenytoin (anti-epilepticagents)
• tracheostomy set• emergency crash cart• 0.014- to 0.021-inch microcatheters and
wires• detachable or pushable coils• liquid embolic agents: NBCA, Onyx®• MERCI® retriever• stents appropriately sized for the intracra-
nial circulation: e.g., NeuroformTM, MiniVision(Guidant).
REFERENCES
1. CaRESS Steering Committee. Carotid revascularizationusing endarterectomy or stenting systems (CARESS):phase I clinical trial. J Endovasc Ther 2003; 10(6): 1021–30.
2. CaRESS Steering Committee. Carotid RevascularizationUsing Endarterectomy or Stenting Systems (CaRESS)phase I clinical trial: 1-year results. J Vasc Surg 2005;42(2): 213–19.
3. Bosiers M, Peeters P, Deloose K et al. Does carotidartery stenting work on the long run: 5-year results inhigh-volume centers (ELOCAS Registry). J CardiovascSurg (Torino) 2005; 46(3): 241–7.
4. Das S, Bendok BR, Getch CC et al. Update on currentregistries and trials of carotid artery angioplasty andstent placement. Neurosurg Focus 2005; 18(1): e2.
5. Gray WA, Hopkins LN, Yadav S et al. Protected carotidstenting in high-surgical-risk patients: The ARCHeRresults. J Vasc Surg 2006; 44(2): 258–68.
6. Gray WA for the CREST Investigators. CREST Update:January 2005 (oral presentation). International Sympo-sium on Endovascular Therapy (ISET) 2005, MiamiBeach, FL, 17 January 2005.
7. Hopkins LN for the CABERNET investigators. Resultsof carotid artery revascularization using the BostonScientific FilterWire EX/EX and the EndoTex NexStent.Results from the CABERNET clinical trial. 26 May 2005.EuroPCR Conference (Paris, France) 2005.
8. Ramee S for the Evaluation of the Medtronic AVESelf-expanding Carotid Stent System with Distal Protec-tion in the Treatment of Carotid Stenosis (MAVEriC)Investigators: Preliminary data from the MAVEriC I & IIcarotid stenting clinical trials (presentation). Presented at Transcatheter Cardiovascular Therapeutics (TCT)Meeting, Washington DC, 29 September 2004.
9. Safian R. The 30-day results of the Carotid Revascu-larization with ev3 Arterial Technology Evolution(CREATE) pivotal trial. Presented at the Society ofInterventional Radiology Meeting, New Orleans LA, 31 March–5 April 2005.
10. White CJ, Iyer SS, Hopkins LN et al. Carotid stentingwith distal protection in high surgical risk patients: theBEACH trial 30 day results. Cathet Cardiovasc Interv2006; 67(4): 503–12.
11. Whitlow P. Registry Study to Evaluate the NeuroshieldBare Wire Cerebral Protection System and X-Act Stentin Patients at High-Risk for Carotid Endarterectomy(SECuRITY): Carotid artery stenting with a distal-protection device safe in high-risk patients. Presented atTranscatheter Cardiovascular Therapeutics Meeting,Washington DC, 17 September 2003. Heart Wire 2003;http://www.clevelandclinic.org/heartcenter/pub/news/archive/2003/security9_17.asp (accessed December 21,2005).
12. Yadav JS, Wholey MH, Kuntz RE et al. Protectedcarotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med 2004; 351(15): 1493–501.
13. Barnett HJ, Taylor DW, Eliasziw M et al. Benefit ofcarotid endarterectomy in patients with symptomaticmoderate or severe stenosis. North American Sympto-matic Carotid Endarterectomy Trial Collaborators. N Engl J Med 1998; 339(20): 1415–25.
14. North American Symptomatic Carotid EndarterectomyTrial Collaborators. Beneficial effect of carotid endar-terectomy in symptomatic patients with high-grade caro-tid stenosis. N Engl J Med 1991; 325(7): 445–53.
15. Executive Committee for the Asymptomatic CarotidAtherosclerosis Study. Endarterectomy for asympto-matic carotid artery stenosis. JAMA 1995; 273(18): 1421–8.
16. Anonymous. CAS Clinical Trial Update. EndovascularToday 2004; September: 79.
17. Ecker RD, Lau T, Levy EI et al. Thirty-day morbidityand mortality rates for carotid artery intervention bysurgeons who perform both carotid endarterectomyand carotid angioplasty and steat placement. J Neurosurg2007; 106: 217–21.
18. Schievink WI, Mokri B, O’Fallon WM. Recurrent spon-taneous cervical-artery dissection. N Engl J Med 1994;330(6): 393–7.
19. Kadkhodayan Y, Jeck DT, Moran CJ et al. Angioplastyand stenting in carotid dissection with or without asso-ciated pseudoaneurysm. Am J Neuroradiol 2005; 26(9):2328–35.
20. Fann JI, Sarris GE, Miller DC et al. Surgical manage-ment of acute aortic dissection complicated by stroke.Circulation 1989; 80(3 Pt 1): I257–63.
21. Pavkov I, Horner S, Klein GE et al. Percutaneous transluminal angioplasty with stenting in extended supra-aortic artery dissection. Croat Med J 2004; 45(2): 217–19.
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 114

CAROTID STENTING COMPLICATIONS 115
22. Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl JMed 2004; 350(18): 1862–71.
23. Goldstein LB, McCrory DC, Landsman PB et al.Multicenter review of preoperative risk factors for carotidendarterectomy in patients with ipsilateral symptoms.Stroke 1994; 25(6): 1116–21.
24. Ouriel K, Hertzer NR, Beven EG et al. Preproceduralrisk stratification: identifying an appropriate popula-tion for carotid stenting. J Vasc Surg 2001; 33(4): 728–32.
25. Ballotta E, Renon L, Da Giau G et al. Octogenarianswith contralateral carotid artery occlusion: a cohort athigher risk for carotid endarterectomy? J Vasc Surg2004; 39(5): 1003–8.
26. Reed AB, Gaccione P, Belkin M et al. Preoperative riskfactors for carotid endarterectomy: defining the patient athigh risk. J Vasc Surg 2003; 37(6): 1191–9.
27. Villalobos HJ, Harrigan MR, Lau T et al. Advancementsin carotid stenting leading to reductions in periopera-tive morbidity among patients 80 years and older.Neurosurgery 2006; 58(2): 233–40.
28. Meyer FB, ed. Sundt’s Occlusive CerebrovascularDisease, 2nd edn. Philadelphia: WB Saunders, 2004.
29. Pritz MB. Timing of carotid endarterectomy afterstroke. Stroke 1997; 28(12): 2563–7.
30. Parodi JC, Ferreira LM, Sicard G et al. Cerebral protec-tion during carotid stenting using flow reversal. J VascSurg 2005; 41(3): 416–22.
31. Goldstein LB, Samsa GP, Matchar DB et al. Multicenterreview of preoperative risk factors for endarterectomyfor asymptomatic carotid artery stenosis. Stroke 1998;29(4): 750–3.
32. de Virgilio C, Toosie K, Arnell T et al. Asymptomaticcarotid artery stenosis screening in patients with lowerextremity atherosclerosis: a prospective study. AnnVasc Surg 1997; 11(4): 374–7.
33. House AK, Bell R, House J et al. Asymptomatic carotidartery stenosis associated with peripheral vascular disease: a prospective study. Cardiovasc Surg 1999;7(1): 44–9.
34. Ecker RD, Guidot CA, Hanel RA et al. Perforation of external carotid artery branch arteries during endo-luminal carotid revascularization procedures: conse-quences and management. J Invas Cardiol 2005; 17(6):292–5.
35. Wilentz JR, Chati Z, Krafft V et al. Retinal embolizationduring carotid angioplasty and stenting: mechanismsand role of cerebral protection systems. Cathet Cardio-vasc Interv 2002; 56(3): 320–7.
36. Walker PJ, May J, Harris JP et al. External carotidendarterectomy for amaurosis fugax in the presence ofinternal carotid artery occlusion. Aust NZ J Surg 1994;64(1): 48–52.
37. Ong TJ, Harper CA, O’Day J. Restoration of ocular cir-culation and some visual function following external
carotid endarterectomy. Clin Exp Ophthalmol 2000;28(4): 329–31.
38. Rush DS, Holloway WO, Fogartie JE Jr et al. The safety,efficacy, and durability of external carotid endarterec-tomy. J Vasc Surg 1992; 16(3): 407–13.
39. Al-Mubarak N, Roubin GS, Vitek JJ et al. Micro-embolization during carotid stenting with the distal-balloon antiemboli system. Int Angiol 2002; 21(4): 344–8.
40. Chen CI, Iguchi Y, Garami Z et al. Analysis of emboliduring carotid stenting with distal protection device.Cerebrovasc Dis 2006; 21(4): 223–8.
41. Biasi GM, Froio A, Diethrich EB et al. Carotid plaqueecholucency increases the risk of stroke in carotid stent-ing: the Imaging in Carotid Angioplasty and Risk ofStroke (ICAROS) study. Circulation 2004; 110(6):756–62.
42. Cardaioli P, Giordan M, Panfili M et al. Complicationwith an embolic protection device during carotid angio-plasty. Cathet Cardiovasc Interv 2004; 62(2): 234–6.
43. Macdonald S, Venables GS, Cleveland TJ et al. Protectedcarotid stenting: safety and efficacy of the MedNovaNeuroShield filter. J Vasc Surg 2002; 35(5): 966–72.
44. Serruys PW, Kutryk MJ, Ong AT. Coronary-arterystents. N Engl J Med 2006; 354(5): 483–95.
45. Setacci C, de Donato G, Setacci F et al. Surgical manage-ment of acute carotid thrombosis after carotid stenting:a report of three cases. J Vasc Surg 2005; 42(5): 993–6.
46. Meyer FB, Sundt TM Jr, Piepgras DG et al. Emergencycarotid endarterectomy for patients with acute carotidocclusion and profound neurological deficits. Ann Surg1986; 203(1): 82–9.
47. Deshmukh VR, Fiorella DJ, Albuquerque FC et al.Intra-arterial thrombolysis for acute ischemic stroke:preliminary experience with platelet glycoproteinIIb/IIIa inhibitors as adjunctive therapy. Neurosurgery2005; 56(1): 46–55.
48. Levy EI, Ecker RD, Horowitz MB et al. Stent-assistedintracranial recanalization for acute stroke: earlyresults. Neurosurgery 2006; 58: 458–63.
49. Kazui S, Naritomi H, Yamamoto H et al. Enlargementof spontaneous intracerebral hemorrhage. Incidenceand time course. Stroke 1996; 27(10): 1783–7.
50. Kappelle LJ, Eliasziw M, Fox AJ et al. Small, unrup-tured intracranial aneurysms and management ofsymptomatic carotid artery stenosis. North AmericanSymptomatic Carotid Endarterectomy Trial Group.Neurology 2000; 55(2): 307–9.
51. Wiebers DO, Whisnant JP, Huston J 3rd et al.Unruptured intracranial aneurysms: natural history,clinical outcome, and risks of surgical and endovascu-lar treatment. Lancet 2003; 362(9378): 103–10.
52. Barrett BJ, Parfrey PS. Clinical practice. Preventingnephropathy induced by contrast medium. N Engl JMed 2006; 354(4): 379–86.
CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 115

CPVI_Chapter07.qxp 4/5/2007 6:26 PM Page 116

INTRODUCTION TO THE FREQUENCY ANDTYPE OF COMPLICATIONS
More and more, clinicians rely on angioplasty andstenting to correct flow abnormalities. Subclavianartery stenosis and occlusions have traditionallybeen managed with classic, open surgical repairvia a transthoracic or cervical approach. Thisinvolved carotid–subclavian bypass or subclavianartery transposition. Introduction of extra-anatomic surgical techniques allowed for satisfac-tory long-term patency and decreased incidenceof serious complications related to aortic inflow.1–4
Unfortunately, though the minimally invasiveapproach reduced mortality, there was anincrease in local complications.5,6 Percutaneousrevascularization has become popular in the man-agement of upper extremity claudication andsubclavian steal syndrome,7,8 coronary steal syn-drome,9,10 and treatment of pathologic atheroscle-rotic lesions of the subclavian artery (SCA)including Takayasu’s arteritis,11–13 Behcet’s dis-ease,14 fibromuscular dysplasia,15 radiation-induced stenosis,16 true aneurysms,17 mycoticaneurysms,18 post-traumatic pseudoaneurysms,arteriovenous fistulae, bleeding,19–21 and sponta-neous22 or iatrogenic dissections23 (Table 8.1).
Management of extracranial vertebral diseasehas been a controversial issue because, althoughoperative and follow-up results reported werepromising, reported experience in this field rep-resented only a few centers,24–26 and most verte-bral occlusive disease has been managed withmedical treatment. Once thought to be benign,posterior cerebral disease was shown in theNew England Medical Center Posterior CirculationRegistry to increase the risk of stroke, causingmajor disability in 18% and death in 3.6%.27
A growing literature of case series suggestsendovascular intervention with percutaneoustransluminal angioplasty (PTA) and stenting is asafe and effective treatment for extracranial ver-tebral artery atherosclerotic stenosis of >50% atthe vertebral artery origin28–33 and promotes afavorable hemodynamic response after angio-plasty.34 Some early reports of angioplasty alonefor vertebral artery origin stenosis cited a markedincidence of restenosis.33 Primary deployment ofstents to stenotic lesions in the extracranial ver-tebral arteries, however, has shown high levelsof technical success (98–100%),28–33 making pri-mary stenting at the origin of the vertebralartery the therapy of choice.
8
Complications in percutaneous subclavianand vertebral artery interventionsJulio A Rodriguez, Francisco Guerrero-Baena, Dawn M Olsen, and Edward B Diethrich
Introduction to the frequency and type of complications • Factors identifying high-risk patients forcomplications • Complications of specific interventional steps and complications of specific interventional tools • Methods to detect potential complications – which diagnostic steps are neededroutinely to rule out or identify complications • Endovascular, surgical, and/or medical techniques toresolve complications • Methods to avoid complications • Summary • Check list for emergencyequipment for interventions in this specific vessel area
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 117

Although randomized trials to assess endovas-cular management of posterior cerebral cir-culation atherosclerotic occlusive disease arelacking,35 there are many case reports docu-menting satisfactory results. However, given thesmall numbers and variations in type of proce-dures, it is difficult to determine the true inci-dence of complications and long-term patency.The complications cited in our review have beenexperienced by most of the readers dedicated to
endovascular therapy. Endoluminal proceduresare less commonly performed in the subclavianand vertebral arteries as compared to lower-limb revascularization, and there are no reportedstandards for treatment and management ofpotential complications. Potential complicationsare shown in Table 8.2, and key points to con-sider in preventing them are listed in Table 8.3.Tables 8.4 and 8.5 provide information from theliterature about common complications of sub-clavian and vertebral interventions, respectively.Our experience with these types of interventionhas led to the following comments about techni-cal management of the procedures and theircomplications.
FACTORS IDENTIFYING HIGH-RISK PATIENTS FOR COMPLICATIONS
Disease in the subclavian is most commonlyfound at the arch origins, and there oftenremains a 1–2 cm stump of subclavian arteryfrom the aortic lumen, allowing adequate accessfor angioplasty and stenting. Normally, subcla-vian and innominate artery lesions are concen-tric, although the proximal aortic stump maypresent some asymmetry secondary to flow dis-turbances caused by plaque formation, partic-ularly at the 90° origin of the left subclavianartery. In general, lesions are not associated withloose debris, but ulcerated plaques may be seenin the vertebral artery and are sometimes associ-ated with upper limb embolization. Althoughsubclavian lesions are quite often calcific innature, most are easily crossed, ballooned, andstented. Lesions in the second part of the subcla-vian artery, however, should be evaluated verycarefully to ensure that stent placement will notinterfere with patency of the vertebral artery orthe internal mammary artery. Subclavian lesionsfrequently affect the left side more often than theright because of the intrathoracic segment, andare generally limited to the proximal segment.Overall, endovascular manipulation of the sub-clavian is relatively safe.
In the innominate artery, elongation mayoccur with age. Access by a retrograde femoralapproach may be difficult, and there may be anincrease of risk of right carotid events secondaryto manipulation. Other anatomic considerations
118 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 8.1 Clinical indications for endovascularinterventions
Clinical indications for endovascular procedures
1. Chronic upper limb ischemiaa. distal embolizationb. limb claudication with no response to
conservative management2. Neurologic symptoms
a. subclavian steal syndrome withvertebrobasilar symptoms
b. contralateral vertebral and/or multivesselsupraortic disease
c. unstable plaque/dissection withembolization or high risk
3. Acute upper limb ischemia4. Acute vertebral occlusion (dissection and/or
thrombosis)5. Myocardial risk
a. subclavian – coronary steal syndrome –IMA (symptomatic or asymptomatic)
b. prior to CABG in subclavian arterystenosis
c. subclavian artery patency protection incoronary disease patient who may needcoronary revascularization in future
6. Failing or rescue of an acute occlusion of anextra-anatomic bypass graft
7. Failing dialysis AV fistula8. Arterial access for another procedure (heart
catheterization)9. True aneurysms
10. Traumatic arterial injurya. pseudoaneurysmsb. AV fistulac. bleeding
11. Spontaneous rupturea. aneurysmsb. other non-traumatic entities – cerebral
fibromuscular dysplasia
IMA, internal mammary artery; CABG, coronary arterybypass graft; AV, arteriovenous.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 118

that increase embolic risk with a femoralapproach are a bovine arch (10%), type II or IIIarch, right-sided lesions, an arch origin of the leftvertebral artery (5%), or an ostial lesion that
must be crossed during arch navigation. Lesionsof the aortic arch and brachiocephalic artery maybe associated with extensive atherosclerosis.36–38
Accurate diagnostic assessment that includescareful imaging with angiographic studies (con-ventional angiography, CTA, and MRA) andhemodynamic explorations via cervical duplexultrasound are important in reducing the risk ofprocedure-related emboli39 and global ischemia.Indeed, ischemic neurologic symptoms may be aconsequence of aortic arch navigation with hemi-spheric embolization or innominate artery andright common carotid manipulation.40–42 Jaegeret al43 reported that 94% of asymptomatic lesionsdetected in 8 patients who underwent angio-plasty or angioplasty plus stenting of brachio-cephalic arteries by diffusion-weighted MRIwere located in territories irrigated by the targetvessel. Although MRI is not a routine study inthe preoperative work-up of the brachiocephalicvessels, it is useful for identifying thrombus andplaque characteristics that may increase the riskof embolization.44 Calcific atherosclerotic plaquesaffecting either the subclavian or vertebral arter-ies are also prone to dissection (Figure 8.1), whichis probably the most common complication rela-ted to angioplasty, and a potential cause of exten-sive damage and procedural failure.
The left vertebral artery is dominant in 50% ofindividuals, whereas right dominance occurs in25%. Dominance may be clinically significant inocclusive disease and related to the trend towardleft-sided lesions in the subclavian territory.Anatomically, the vertebral artery measures 3–5 mm and can be divided into four differentsegments – three extracranial and one intracra-nial portion (Figure 8.2). The first portion corre-sponds to the origin of the vessel to the levelwhere it enters the transverse foramen of the cer-vical vertebral body. The extracranial portion ofthe vertebral artery can be affected by numerousetiologic factors, athererosclerotic disease beingthe most common. Other conditions includefibromuscular dysplasia, dissection, vasculitis,or extrinsic compression – this is particularlytrue in the intervertebral segment and is mostlydue to trauma or an osteophyte. The most com-mon extracranial location is ostial, where thelesions may have fibrous characteristics that makethem less prone to ulceration.45 Symptoms related
SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 119
Table 8.2 Subclavian and vertebral arterycomplications
Complications
1. Related to the puncture sitea. thrombosisb. bleedingc. pseudoaneurysmd. AV fistulae. arterial injuryf. peripheral nerve injury
2. Related to aorto-iliac navigationa. peripheral atheroembolism: to limbs,
visceral, cerebralb. arterial injury
3. Related to the use of contrasta. allergiesb. renal failurec. metabolic problems
4. Related to target vessel manipulationa. spasmb. peripheral embolism (microembolic,
atheroembolism) to upper limb, cerebral, IMA
c. wire tip injuryi. subintimal dissectionii. perforation
d. postballooning injuryi. dissectionii. plaque rupture
e. damage to arteries in close proximity:vertebral, right common carotid, IMA
f. ‘in situ’ vessel ruptureg. ‘in situ’ thrombosish. aortic dissection
5. Related to hemodynamic response to theangioplastya. cerebral hyperperfusion syndromeb. upper limb hyperperfusion syndrome
(hyperemia, swelling)c. compartment syndrome
6. Delayed complicationsa. dissectionb. pseudoaneurysmc. mycotic aneurysm
7. Failurea. in-stent restenosisb. occlusionc. persistence of symptoms
IMA, internal mammary artery; AV, arteriovenous.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 119

to vertebral artery stenosis are part of the verte-brobasilar insufficiency constellation, includingbrief TIAs, dizziness, difficulty with visual focus,and loss of balance. These symptoms are relatedto ischemia of the vestibulocerebellar structures
in the medulla and cerebellum.46 Associated intra-cranial and bilateral disease may increase cere-bral ischemia.47
The natural tortuosity of the vertebral arteryat V1 and V3 segments makes this vessel prone
120 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 8.3 Key points to consider to minimize endovascular complications
Minimizing complications in subclavian and extracranial territories
1. Indicationa. accurate case selection
2. Characterize disease at the target vessela. approach: aorta, arch anatomyb. for subclavian artery
i. stenosis vs occlusionii. proximal subclavian stumpiii. vertebral artery and LIMAiv. vertebral retrograde flowv. extension towards axillary artery
c. for vertebral arteryi. stenosis, dissectionii. location proximal/distal (segment involved V1–V4)iii. single/tandem
3. Anticoagulate the patienta. antiplatelets prior to procedureb. heparinization during the procedure; maintain ACT above 250c. ESR normalized in arteritis, steroid therapy if needed
4. Choose access sitea. associate complementary techniques if needed (aorto-iliac procedure, brachial cutdown)b. antegrade access requires a subclavian stump on aortic sidec. retrograde access requires careful ‘crossing technique’ of the lesion
5. Obtain an optimal view of the extension of the artery to treata. unfold the subclavian artery to see branch ostium over the aortab. same for ostial vertebral artery over subclavian artery
6. Protective techniques to avoid embolization and neighboring vessel injury if neededa. vertebral and internal mammary artery (wire catheterization, kissing balloon technique)b. right common carotid artery protection in right subclavian – innominate artery procedures
7. Rule out technical defects after procedurea. visible defects on angiographic imaging
i. flow defects (dissection, occlusion, residual stenosis)ii. extravasation (perforation, rupture)
b. invisible defects on operative angiographic imagingi. hemodynamic evaluation of flow (pressure gradient across the lesion)ii. IVUS (stent apposition to arterial wall, dissection, residual stenosis)
8. If selective stenting is preferreda. innominate and subclavian artery stenting is recommended after suboptimal angioplasty and occlusionb. ostial vertebral artery stenting is recommendedc. antiplatelet therapy
9. Follow-upa. in-stent restenosis has a silent evolution; close follow-up is mandatoryb. in patients with mammary–coronary bypass grafting, subclavian patency follow-up becomes important.
LIMA, left internal mammary artery; ACT, accelerated clotting time; ESR, erythrocyte sedimentation rate; IVUS, intravascularultrasound.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 120

SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 121
Tabl
e 8.4
Com
plic
atio
ns i
n su
bcla
vian
art
ery
inte
rven
tion
s
Auth
orTo
tal
(#)
PTA/
sten
tS
ucce
ss i
n C
ompl
icat
ions
Dea
thoc
clus
ions
(%
)
Hen
ry e
t al
132
113
57/4
69/1
9 (
47)
3 (
2.7
%)
acce
ss c
ompl
icat
ions
, 1 (
3.1
%)
0br
achi
al t
hrom
bosi
s, 4
(3.6
%)
diss
ectio
n,
1 (
0.9
%)
vess
el o
cclu
sion
, 1 (
0.9
%)
TIA,
1 (
0.9
%)
stro
keS
chill
inge
r et
al1
30
115
89/2
613/2
7 (
48)
7 (
6.1
%)
min
or c
ompl
icat
ions
, 3 (
2.6
%)
0vi
scer
al e
mbo
lizat
ion,
1 (
0.9
%)
TIA
deVr
ies
et a
l42
110
43/5
913/2
0 (
65)
3 (
2.7
%)
diss
ectio
ns,
2 (
1.8
%)
TIA,
1 (
1.8
%)
2 (
1.8
%)
stro
keM
artin
ez e
t al
56
17
0/1
617/1
7 (
100)
1 (
6%
) st
ent
mig
ratio
n, 1
(6%
) th
rom
bosi
s 0
(res
idua
l st
enos
is)
Hut
tl et
al4
189
89/0
Not
spe
cifie
d2 (
2.3
%)
groi
n he
mat
oma,
2 (
2.2
%)
resi
dual
0
sten
osis
, 4 (
4.5
%)
TIA,
1 (
1.1
%)
stro
keB
roun
tzos
et
al84
49
0/4
9N
ot s
peci
fied
2 (
5%
) gr
oin
hem
atom
a, 1
(2%
) br
achi
al-a
xilla
ry
0th
rom
boem
bolis
m,
2 (
4.1
%)
resi
dual
ste
nosi
s,
1 (
2%
) ve
ssel
thr
ombo
sis,
1 (
2%
) TI
AB
ates
et
al131
94
0/9
113/1
5 (
87)
8 (
8.5
%); 2
(2.1
%)
acce
ss h
emat
oma,
0
2 (
2.1
%)
embo
lism
, 1 (
1.1
%)
perip
hera
l ar
teria
l th
rom
bosi
s, 1
(1.1
%)
sten
t m
igra
tion
(spa
sm), 1
(1.1
%)
hear
t fa
ilure
epi
sode
Sul
livan
et
al58
73
0/6
96/1
0 (
60)
1 (
1.4
%)
brac
hial
em
boliz
atio
n, 3
(9.7
%)
0br
achi
al h
emat
oma,
1 (
3.2
%)
brac
hial
AV
fistu
la,
1 (
3.2
%)
brac
hial
pse
udoa
neur
ysm
, 1 (
2%
) fe
mor
al p
seud
oane
urys
m,
2 (
2.9
%)
VA o
rigin
co
vera
ge,
1 (
1.4
%)
LIM
A em
boliz
atio
nAm
or e
t al
40
89
0/8
37/1
3 (
54)
5 (
5.6
%)
min
or a
cces
s co
mpl
icat
ions
, 1 (
1.1
%)
2 (
2.2
%)
limb
embo
lizat
ion,
1 (
1.1
%)
LIM
A em
boliz
atio
n, 1
(1.1
%)
TIA,
1 (
1.1
%)
stro
ke
Al-M
ubar
ak e
t al
134
38
0/3
51/4
(25)
no c
ompl
icat
ions
0Ty
agi
et a
l53
61 (
32 T
.A.)
59/0
3/5
(60)
2 (
3.3
%)
diss
ectio
n, 1
(1.6
%)
thro
mbo
sis,
0
1 (
1.6
%)
resi
dual
ste
nosi
sR
odrig
uez
et a
l10
110
5/1
05
25/3
0 (
83)
4 a
cces
s th
rom
bosi
s, 5
(4.5
%)
diss
ectio
n,
04 (
3.6
%)
resi
dual
ste
nosi
s, 3
(2.7
%)
thro
mbo
sis,
1 s
tent
mig
ratio
n (0
.9%
), 1
(0.9
%)
TIA
Sad
ato
et a
l135
70/7
7/7
(100)
1 (
20%
) br
achi
al t
hrom
bosi
s, 1
(14.3
%)
1 (
14.3
%)
resi
dual
ste
nosi
s an
d th
rom
bosi
s (1
4.3
%), 1
str
oke
cont
inue
d
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 121

122 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Tabl
e 8.4
Com
plic
atio
ns i
n su
bcla
vian
art
ery
inte
rven
tion
s –
cont
inue
d
Auth
orTo
tal
(#)
PTA/
sten
tS
ucce
ss i
n C
ompl
icat
ions
Dea
thoc
clus
ions
(%
)
Erbs
tein
et
al75
24
24/0
2/2
(100)
5 (
20.8
%)
diss
ectio
n, 5
(20.8
%)
resi
dual
0
sten
osis
, 1 (
4.2
%)
TIA
Insa
ll et
al1
33
37
33/0
2/2
(100)
1 (
2.7
%)
groi
n he
mat
oma
1 (
2.7
%)
perip
hera
l 1 (
2.7
%)
arte
ry t
hrom
bosi
s, 3
(8.1
%)
resi
dual
ste
nosi
s,1 (
2.7
%)
stro
keW
ilms
et a
l136
23
21/0
—1 (
4.3
%)
perip
hera
l em
bolis
m 1
(4.3
%)
0pe
riphe
ral
arte
ry t
hrom
bosi
sM
otar
jem
e36
93
84/2
6/1
3 (
46)
1 (
1.1
%)
perip
hera
l em
bolis
m0
Ath,
ath
eros
cler
otic
; C
CA,
com
mon
car
otid
art
ery;
LIM
A, l
eft
inte
rnal
mam
mar
y ar
tery
; PT
A, p
ercu
tane
ous
tran
slum
inal
ang
iopl
asty
; TA
, Ta
kaya
su a
rter
itis;
TIA
, tr
ansi
ent
isch
emic
atta
ck;
VA,
vert
ebra
l ar
tery
.
to injury during endoluminal intervention.48
Dissection or perforation is a risk, particularlywith interventions at distal territories of the ver-tebral artery, V3 and V4 (Figure 8.3). These seg-ments are subject to wire tip injury duringnavigation that may result in life-threateningintracranial bleeding and can be difficult to con-trol.49 Postoperatively, patency has been relatedto reference vessel diameter.50
Some differences in the distribution of athero-sclerotic posterior circulation occlusive diseasemay be related to gender and race. Caucasianstend to have lesions at the origin of the left verte-bral artery and high-grade lesions of the extracra-nial vertebral arteries. African-American patientstend to have lesions of the distal basilar artery,high-grade lesions of intracranial branch vessels,and symptomatic intracranial branch disease.51,52
Other etiologies such as fibromuscular dysplasiaor Takayasu’s arteritis affect younger patients,particularly women. In treating Takayasu’s arteri-tis, high rates of dissection and suboptimal dilata-tion and restenosis are often seen in long lesions.53
When acute inflammation is suspected, preopera-tive steroid treatment that normalizes the ESRmay improve outcome.12,54,55
COMPLICATIONS OF SPECIFIC INTERVENTIONAL STEPS AND TOOLS
Oral antiplatelet therapy is used in stenting pro-cedures in the subclavian and vertebral arteriesand may be given preoperatively, or once thevessel is accessed. Local anesthesia with mildsedation allows the assessment of neurologicepisodes, but there are disadvantages to usinglocal anesthesia, as patient movement during theprocedure can be problematic when ‘roadmap-ping’ is being used to guide balloon angioplastyor stent deployment.
Endovascular management of subclavian arteryocclusions was initially associated with failurerates as high as 54%.36 However, in other series,mid-term patency rates of up to 84% werereported.56,57 The best way to access the targetlesion is still controversial, and the risks and ben-efits of different approaches (femoral, brachial)have to be assessed on a case-by-case basis. Our preference, especially in a tight lesion, is the
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 122

SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 123
Tabl
e 8.5
Com
plic
atio
ns i
n ve
rteb
ral
arte
ry i
nter
vent
ions
Auth
orTo
tal
(#)
PTA/
sten
tS
ucce
ssC
ompl
icat
ions
Dea
th
Albu
quer
que
et a
l61
33 (
prox
imal
VA)
33/0
32 (
97%
)1 (
3%
) di
ssec
tion,
1 (
3%
) st
ent
mal
depl
oym
ent
1 (
3%
) C
hast
ain
et a
l48
55 (
prox
imal
VA)
0/5
554 (
98%
)1 (
1.8
%)
diss
ectio
n2 (
3.6
%)
non-
rela
ted
Clo
ud e
t al
101
14 (
prox
imal
VA)
4/1
014 (
100%
)1 (
7.1
%)
resi
dual
ste
nosi
s, 1
(7.1
%)
72 h
0
post
oper
ativ
e TI
A, 1
(7.1
%)
brac
hial
hem
atom
aH
auth
et
al49
16 (
11 p
roxi
mal
,9/3
14 (
87%
)1 (
6.2
5%
) di
ssec
tion
with
ves
sel
occl
usio
n0
1 c
ervi
cal,
4 d
ista
l V4
)H
igas
hida
et
al28
41 (
34 p
roxi
mal
,41/0
—1 (
2.4
%)
vess
el r
uptu
re,
2 (
4.9
%)
spas
m,
05 d
ista
l VA
, 3 B
A)2 (
4.9
%)
TIA,
2 (
4.9
%)
stro
keJa
nsse
ns e
t al
137
19 (
prox
imal
VA)
19/0
17 (
89%
)4 (
21%
) re
sidu
al s
teno
sis,
4 (
21%
) di
ssec
tions
,0
1 (
5.2
%)
groi
n he
mat
oma,
1 (
5.2
%)
acce
ss
diss
ectio
n (b
ilate
ral
iliac
art
ery)
Jenk
ins
et a
l29
38 (
34 p
roxi
mal
,0/3
838 (
100%
)1 (
2.6
%)
TIA
04 c
ervi
cal
VA)
Mal
ek e
t al
31
13 (
10 p
roxi
mal
,0/1
313 (
100%
)5 (
38%
) di
ssec
tions
, 1 (
7.7
%)
TIA
03 c
ervi
cal
VA)
Mot
arje
me3
639 (
35 p
roxi
mal
,0/3
636 (
92%
)1 (
2.6
%)
bila
tera
l bl
indn
ess,
(bi
late
ral
seve
re
01 c
ervi
cal
and
VA s
teno
sis
PTA)
2 d
ista
l VA
)Pi
otin
et
al100
7 (
prox
imal
VA)
7/0
7 (
100%
)no
com
plic
atio
ns0
Web
er e
t al
70
38 (
prox
imal
VA)
0/3
838 (
100%
)2 (
5.3
%)
diss
ectio
ns,
1 (
2.6
%)
TIA
0
CA,
car
otid
art
ery;
PTA
, pe
rcut
aneo
us t
rans
lum
inal
ang
iopl
asty
; TI
A, t
rans
ient
isc
hem
ic a
ttac
k; V
A, v
erte
bral
art
ery.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 123

percutaneous brachial approach through a 5–6Fr sheath because proximity to the site of thelesion allows better ‘pushability’ of the device.In general, the closer the puncture site is to thearea of therapy, the easier it is to maneuver andaccess the area of interest. Accurate lesion can-nulation is required to prevent plaque ruptureand retrograde dissection to the thoracic aorta.Such complications have the potential for severe consequences.58,59
Femoral puncture sites are a considerable dis-tance from lesions of the upper extremity andmay be problematic when the arch configurationis tortuous or the great vessel origins are anom-alous in their take-offs. A coaxial techniqueincorporating a diagnostic catheter may increasethe strength of the guiding catheter, and place-ment of a long 7–8 Fr sheath in the vicinity of the target can also be helpful, providing betterangiographic views closer to the lesion and offer-ing better support for guiding a stent through atight channel. A long sheath allows more place-ment options if navigation complications neces-sitate implantation of a stent in other territories(such as the iliac artery).60
Wire selection may be dictated by therapistexperience and the target vessel and its charac-teristics. In our experience, an angled 0.035-inchhydrophilic guidewire and a straight 5 Fr angio-graphic catheter are adequate for most proce-dural approaches. In occlusions, if the initialmaneuver is unsuccessful, a straight 0.035-inchstiff wire through a 45° angled catheter can enablecannulation of the core of the plaque (Figure 8.4).Predilatation with a 4 mm balloon can accom-modate a stent device. From our point of view,lower profile wires (0.014 to 0.018-inch) can beconsidered in extraordinary cases for subclavianand innominate lesions, mainly when predila-tation with a low-profile balloon is necessary.Different views (left/right oblique with cranialangulation) are recommended to obtain optimalvisualization of the origin of the vessel to treat.
124 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
white arrow – prevertebral dissection
Figure 8.1 Angiogram of a subclavian artery dissection.
Figure 8.2 Anatomical classication of vertebral arterysegments.
Vertebral Artery: V1 – extends from the arterialostium to the level where it enters at C6transverse foramen, V2 – “intraoseum” from C6to C2, V3 – extracranial but high in posteriorneck at level of C1, V4 – intracranial from C1 tobasilar artery
C2
C3
C4
C5
C6
V1
V2
V3
V4
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 124

The identification of the origin becomes para-mount at the time of stent deployment, since oneof the well-known causes of in-stent restenosiscan be the inadvertently missed arterial ostium.
Routinely, balloon-expandable stents are thedevice of choice in an ostial location because oftheir radial strength and ease of deployment.Selection of stent size is based on the adjacent nor-mal vessel and the length of the lesion. In general,the diameter of the balloon is 1 mm smaller thanthe balloon the stent is mounted on. In subclavianterritories, self-expanding stents are useful intortuous settings or in treating lesions at pointsof flexion. In these cases, the diameter of the stentmay be 1–2 mm larger than the native vessel. Thesmall diameter of vertebral arteries makes the useof short, low-profile balloon-expandable coronarystents ideal here.61 This is an area in which stiffdevices (wires, balloons, stents) can cause tech-nical difficulties that have the potential to leadto major complications. Although we do notfavor the use of stents in V2 and V3 segmentsdue to the bony encasement of the vessel, othershave placed stents here successfully.62–64 If stenting
is necessary in these segments, a flexible stent isadvisable.
Local complications can occur with attemptedpercutaneous recanalization of the subclavianand vertebral arteries, including dissection, perfo-ration, disruption, thrombosis, and embolization.In addition, complications such as the dissectionof the arch aorta or vertebral artery may occur.Subintimal wire penetration or a catheter crossingagainst a rigid plaque can create a dissectionplane, and this is a common complication in sub-clavian artery interventions. Though enteringunder a plaque in high-grade lesions and re-entering into the true lumen may be a successfulstrategy, it is not always possible, especially inan occluded subclavian artery. While it is tempt-ing to proceed in a subintimal plane, balloonangioplasty and stenting here may result in perforation of the vessel.
Plaque fracture related to angioplasty or stentmaldeployment can create a flap (Figure 8.5).Dissections of brachiocephalic vessels may extendinto adjacent territories including the aorta58
(Figure 8.6) or vertebral arteries (Figure 8.7),
SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 125
Aortic dissection complicating a subclavian occlusion angioplasty attempt. (a) dye staining both the ascending anddescending aortic wall. (b) Two weeks later patient returns with chest pain. A pseudoaneurysm of the aorta is noted(white arrow). (c) schematic demonstrating the extension of the problem, (d) thoracic endograft placement to excludethe SCA and the pseudoaneurysm, (e) post-endograft angiogram demonstrating adequate seal. (f) chest CT-scan 1month after the onset, free of endoleak.
(a) (b) (c) (d) (e) (f)
Figure 8.3 Subclavian artery dissection that involves the descending thoracic aorta. New pseudoaneurysm develops and is treated with an endograft.
(a) (b) (c) (d) (e)
(a,b) Crossing technique in a subclavian artery total occlusion. (c,d) Use of an angulated catheter and a straightwire to stay within the core of the plaque. (e) “zig-zagging” of the wire usually leads to subintimal space, and ultimatelyto a dissection.
Figure 8.4 Crossing technique in subclavian artery occlusion.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 125

extending toward the upper limb and includingthe LIMA such that there is compromise ofmyocardial revascularization.65 Persistent dis-section beyond the stented area can result in pro-cedure failure due to flow disturbance and, insome cases, development of a pseudoaneurysm.66
Dissection at the ostium or prevertebral subcla-vian is likely to extend into the aortic arch,
descending thoracic aorta, or vertebral artery,with sequelae that may be quite severe andinclude pseudoaneurysm development, rupture,or vertebrobasilar symptoms. If a dissection occursand involves the descending thoracic aorta, itsextension needs to be evaluated to determinethe necessity of further treatment such as thoracicstenting or endoluminal grafting (Figure 8.3).
The subclavian artery is a thin-walled vesselcompared with the carotid. The subclavian issusceptible to close trauma and operative injuryeven during conventional procedures and, thoughrare, perforation due to direct wire injury hasbeen reported in endovascular intervention.67–69
Tortuousity in subclavian and vertebral arteriesmay contribute to the potential for wire injurywhen there is an attempt to maneuver the lesionor manipulation occurs inadvertently at thelevel of the branches.70 Iatrogenic arterial wall dis-ruption can also be caused by balloon angioplastyor stent deployment. Both procedures transmitincreased radial force from non-compliant devicesto the vessel wall, and may produce a tear in aweakened area or in an underlying calcific lesion.
Vessel rupture is rare in the subclavian, andvertebral artery manipulation is more often asso-ciated with wall injuries71,72 (see Table 8.5). Broad-bent et al presented two cases of supra-aorticvessel rupture (one carotid and one subclavian)in a heterogeneous series of 180 patients.72
Careful vessel diameter evaluation and deviceselection is of the utmost importance in avoidingoverdilatation and arterial injury.
Manifestations of wall injuries due to perfo-ration and rupture may present early or bedelayed. Early presentation can range from asimple operative finding that can be managed inthe same session, or one that results in a neckhematoma, pseudoaneurysm, or an active, life-threatening bleed in the thorax. Delayed presen-tation may be seen as a pulsatile mass secondaryto pseudoaneurysm formation73 (Figure 8.8).
The incidence of thrombosis is limited with theuse of systemic periprocedural anticoagulation.The majority of the time, acute thrombosis isassociated with the brachial artery access site. Itcan also occur due to an untreated iatrogenic dis-section from wire advancement or balloon angio-plasty. Subacute events may occur secondary topersistent stenosis. Incomplete dilatation was
126 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b)
(a) intimal flap (arrow) with subsequent thrombosis, afterbrachial approach, (b) subclavian artery intraluminalthrombus secondary to a suboptimal angioplasty
Figure 8.5 Angiogram demonstrating brachial artery flapand subclavian artery thrombus.
Aortic dissection secondary to attempt of subclavianstenosis. The white arrow indicates the area ofdissection on the proximal descending thoracicafter attempting crossing the stenosis.
Figure 8.6 Aortic dissection secondary to attempt ofsubclavian angioplasty.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 126

initially described as a potential source of throm-botic and embolic complications.74 Causal factorsmay include suboptimal high-grade lesion angio-plasty, a persistent dissection at the target lesionafter balloon angioplasty (or in areas that might
remain uncovered by the stent), unrecognized orineffectively treated disease, maldeployed stents,and diseased axillary or brachial arteries that affect‘run-off’.75 We experienced a case of dissection dis-tal to the deployed stent in our series10 (Table 8.4).
Embolization during endovascular manage-ment of subclavian and vertebral artery stenosesis also possible. There are two main sources ofemboli. Debris can be liberated from the intimalarterial surface as endovascular devices advanceto the target lesion. The other possibility isembolization from the target lesion itself. This isparticularly concerning in subclavian–vertebralprocedures due to the associated risk of stroke.Some series have shown a potential protectivemechanism of direct vs selective stenting inreducing the incidence of embolic events.40 Thereis, however, a well-known mechanism of physio-logic protection during the angioplasty of thesubclavian artery as described by Bachman, whoevaluated vertebral flow after subclavian arteryballoon angioplasty in patients with vertebralflow reversal secondary to subclavian steal syn-drome.76 Ultrasound monitoring of the homo-lateral vertebral flow patterns has also beendescribed by Ringelstein,77 who documentedantegrade flow in 10 successfully treated patientswith delay longer than 20 seconds after dilata-tion. This unexpected hemodynamic behaviorprovides physiologic protection that contributesto the low rate of neurologic events in patientstreated for subclavian steal syndrome. MRI ofischemic lesions before and after brachiocephalicangioplasty also suggests the safety of subclavian
SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 127
Post subclavian angioplasty a dissection develops that extends into the ostium of the vertebral artery. (black & white arrows)The origin of the VA has to be stented to correct the dissection and the compromised lumen. The subclavian artery wastreated following the VA intervention.
Figure 8.7 Dissection in the subclavian artery extended to the vertebral artery.
(a)
(b)
(a) Traumatic pseudoaneurysm arising from the ostium ofthe right subclavian artery, (b) Pseudoaneurysm excludedwith a Gore endograft from distal common carotid approach
Figure 8.8 Pseudoaneurysm of the innominate artery,treated with endoluminal graft.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 127

procedures.43 Supra-aortic occlusive disease isrelated to extensive atherosclerosis, and neuro-logic symptoms may be a consequence of aorticarch navigation. Atherosclerotic plaque can befragmented after balloon angioplasty and liber-ate debris to the circulation; the same plaqueoffers a thrombogenic surface to platelets. Poten-tial affected end organs are the upper limb andbrain (via the posterior circulation and the rightcarotid artery).
After completion of an endovascular proce-dure, patients should be transferred to theintensive care unit and monitored. The sheath iswithdrawn when the ACT is below 150 seconds.The patient is usually discharged the followingday. In our experience, implantation successnears 100% for stent placement in the subclavianand innominate arteries, and we have had goodsuccess in the vertebral artery as well.
METHODS TO DETECT POTENTIAL COMPLICATIONS – WHICH DIAGNOSTICSTEPS ARE NEEDED ROUTINELY TO RULE OUT OR IDENTIFY COMPLICATIONS
Preoperative assessment
Preoperative study is vital in determining theindication, approach, and technique for endovas-cular intervention in the subclavian and verte-bral arteries. Clinical findings (access pulses orbruits, upper limb pulses, asymmetry and pres-sure gradients, cervical bruits or palpable pul-satile masses or thrill) and global brachiocephalicimaging must be part of the routine preopera-tive work-up.
Although useful in determining subclavianflow changes, carotid disease, and most cases ofvertebral origin stenosis,78,79 duplex ultrasoundis less useful for morphologic study of lesionsbecause of the intrathoracic location of left subclavian artery origin. Nevetheless, it canreveal hemodynamic patterns of subclavian stealin its later stages.80,81 In vertebral stenosis, duplexultrasound is less specific than for other occlu-sive entities (i.e., hypoplasia, aplasia, dissection).It is useful in establishing the flow pattern invertebral artery for preoperative evaluation ofprocedural embolic risk. Coronary embolizationin patients with prior myocardial revasculariza-
tion has been well described with antegradeflow in the vertebral artery; retrograde internalmammary artery (IMA) flow may also be prob-lematic, but is relatively rare.80
Angiography is the gold standard for diagno-sis of cerebrovascular occlusive disease.82,83
However, newer techniques such as angioCT orMRI offer satisfactory non-invasive target lesionimaging and three-dimensional (3D) reconstruc-tion (Figure 8.9). Careful aortic arch study maydetect atherosclerotic sources of emboli and wall-attached vessel thrombus.44,84
Operative assessment
Angiography is the main imaging method dur-ing endoluminal procedures, and roadmappingallows satisfactory views of the target lesion andangioplasty and stenting sites. However, the ostial
128 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b)
(c) (d)
64 slice CT-scan with 3D reconstruction of the arch andcarotids. (A, B) right vertebral artery difficult to visualizeon the AP and right lateral view, its origin is easilyappreciated on the rotational left lateral view. (C ,D)A posterior view is required to fully evaluate the ostiumof the left vertebral artery.
Figure 8.9 64-slice VCT axial view of the vertebral artery.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 128

location of most of the subclavian or vertebralartery lesions may be difficult to visualize usingstandard arch views because of superimposedimages of the subclavian artery origin over theaorta and of the first segment of the vertebralartery over the subclavian artery. Additional obli-que views are of the utmost importance for accu-rate diagnosis. Angiographic information alsoremains very useful for visualizing active bleed-ing secondary to perforation or vessel disrup-tion, spasm, thrombosis, or embolic phenomena,but it is less helpful in determining cross-sectional plaque volume, the extent of the lesion,and the morphology of plaque composition,85
distribution or wall defects.86,87
Assessment of flow restoration may be obtainedby determining the pressure gradient between theupper limbs or on either side of the target lesionvessel in the vertebral artery.88 Such determina-tions allow accurate evaluation of underlyingremnant flow defects (residual stenosis, elasticrecoil, dissection) that can threaten early outcomeand impair long-term patency. Flow defects sec-ondary to suboptimal angioplasty stenting can bemissed using angiography alone. In 100 patientswith a residual intra-arterial mean pressure gra-dient higher than 10 mmHg, Tetteroo et al89 foundangiography sensitivity and specificity to be 45%and 63%, respectively, for postprocedural diagno-sis of residual stenosis following iliac angioplasty.
The 360° tomographic imaging provided byintravascular ultrasound (IVUS) is extremely use-ful in endovascular intervention in the subclavianand innominate arteries. Serial images are stackedby the computer during a single ‘pull-through’and reassembled into a 3D reconstruction thatallows the whole length of the artery to be dis-played at one time. Lesions may be examined fromany angle, slice, or rotation – an advance we havefound particularly helpful in peripheral interven-tions. In one series of thoracic outlet syndromecases, subclavian vein IVUS imaging results werecomparable to those obtained by venography.90
Postprocedural IVUS studies in coronary andfemoropopliteal arteries have been used to assessstent attachment, maldeployment, dissection, andluminal irregularities caused by plaque rupture.91
They may also determine the presence of calcifica-tion and residual stenosis <70%,86,87 which can bemissed by angiography,89 and increase the risk of
in-stent thrombosis and procedural failure.Although the IVUS literature for subclavian angio-plasty is lacking, experiences reported in equiva-lent diameter vessels such as the iliac arteriesindicated in vitro IVUS sensitivity was 74% for dis-section and 59% for media rupture.92 Clinical useof IVUS has revealed visible defects in 45% ofpatients undergoing endovascular intervention(including dissections, inadequate stent dilatation,migration, and thrombus entrapment) that werenot seen using uniplanar angiography.93
Transcranial Doppler ultrasound has been usedsuccessfully to detect procedure-related embolicsigns during and after vertebral angioplasty94 andto evaluate hemodynamic response to vertebralangioplasty. This non-invasive technique is use-ful for operative monitoring94,95 and postoperativeevaluation of posterior cerebral procedures,though standardized protocols are lacking.Diffusion-weighted MRI is another non-invasivemeans of diagnosing cerebral infarction.96
ENDOVASCULAR, SURGICAL, AND/ORMEDICAL TECHNIQUES TO RESOLVE COMPLICATIONS
Prevention of complications through the use ofthe appropriate technique is an important goal.Following stent deployment, an angiographiccontrol image should be taken, and the gradientrecorded. As described above, IVUS may besuperior to angiography in detecting inadequatestent deployment and, when the IVUS imagessuggest suboptimal deployment, a larger balloonshould be used to expand the stent.
Perforation occurs more commonly duringtreatment of total rather than partial occlusionsof the vessel and may be caused by creation ofa subintimal dissection (as above) or followingoverdilatation of the balloon before or after thestent has been deployed. Location of the perfo-ration is relevant when it comes to management.If it is a large perforation, the patient will exhibithypotension. Delayed identification of a perfora-tion usually results in hypotension, tachycardia,shortness of breath, or even chest pain. A postop-erative chest X-ray will demonstrate a hemothorax.
Management of a perforation may be difficultto resolve percutaneously. Simple balloon angio-plasty may tamponade the bleed, but more than
SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 129
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 129

one inflation may be necessary, and reversal ofthe anticoagulation may be helpful. If the deci-sion is made to reverse the heparin, an endograftshould be available in case balloon dilatationalone is unsuccessful. The location of the perfo-ration, however, can limit the use of an endo-graft.45,74,97 Angiography may be the most usefulmethod to determine if the lesion is amenable toendovascular repair.98 If the right subclavianartery ostium is involved, the endograft mayextend proximally and compromise the rightcommon carotid artery. If the pre- or postverte-bral artery is the site of perforation, then a shortendograft must be selected so as to avoid cover-age of the vertebral artery. If the perforation islocated at a region unsuitable for deployment ofa covered stent, then the decision to convert toopen repair should be made early on. A ballooncan remain inflated while exposure is obtained.
When intimal injury is caused by arterial cannulation, local thrombosis of the vessel andocclusion may be treated with thrombolytics.Acute thromboses or emboli presenting within 24 hours are most amenable, and thrombolysis isour preferred option to restore patency of graftsoccluded less than 14 days. Acute stent thrombo-sis in the vertebral artery has been reported tocause transient diplopia and ataxia99 spasm, dis-section, restenosis, and TIA.28,100,101 The use of astent at the origin and proximal segment of thevertebral artery will help to prevent the potentialcomplications of dissection and early restenosis.This is important because spasm and dissectionhave been linked to immediate occlusion andtransient or permanent neurologic complications.
In treating chronic occlusion, or in situationswhere severe acute ischemia is present, surgicalintervention is generally preferred over thrombol-ysis. Typically, thrombosis is most often associatedwith the access site. It can be related to the targetvessel as well, primarily due to the disruption ofa plaque and creation of a dissection. Diagnosismay be made intraoperatively with evidence ofslow flow through the brachial artery. It may alsobe recognized based on dampened waveformsin the arterial line of the involved upper extrem-ity. In addition, upper extremity pallor or cool-ness may be apparent perioperatively. Arterialduplex is helpful in documenting the extension
of the acute arterial occlusion. Management ofthrombosis includes prevention with adequateanticoagulation. Choose stents that can be deliv-ered via small caliber sheaths (5 or 6 Fr sheath),and use the methods previously described toavoid dissection. Usually, thrombosis occurs inthe early postoperative period, while the patientis being recovered. If the caliber of the brachialartery is a concern, early sheath removal should beconsidered in order to prevent early thrombosis.
Local thrombosis in the subclavian is best pre-vented by adequate anticoagulation. Percuta-neous treatment may include thrombolysis if thesheath remains in place; the newest lytic agentsoffer better management due their shorter half-life. However, in order to revascularize localthrombosis and avoid bleeding risks associatedwith fibrinolysis, the dose and duration of treat-ment may be reduced, and direct suction andthrombectomy102 or mechanical thrombectomyprocedures may be tried.103,104 Results of suchinterventions in other vascular territories,105,106
either as a single therapy or followed by fibrino-lysis, have been satisfactory. It should be notedthat experience and knowledge about preventionof vertebral or coronary embolization are lacking.Indeed, embolization is a complication that hasbeen related to rotational (Rotarex-Straub Medical,Switzerland)107 and hydrodynamic (AngioJet-PossisMedical Inc, Minneapolis) atherectomy devices.106
Embolization is usually identified postopera-tively. As a consequence of embolization, neuro-logic deficits ranging from mild to profound maybe evident. A CT scan or MRI of the head willdocument the territory involved and any evidenceof bleed. Thrombolytics can be considered whenthere is early recognition of symptoms. Upperextremity embolization can occur with discolor-ation or pain in the digits. If the embolus occludesthe distal circulation of the upper extremity andacute thrombosis occurs, the symptoms will likelybecome more severe, necessitating hepariniza-tion and embolectomy.
Conventional anti-aggregation methods andprocedural heparinization should be consideredstandard in cerebral procedures.28 Abciximab is a glycoprotein (GP) IIb/IIIa antagonist whichdiminishes platelet aggregation and thrombus for-mation and may have anticoagulant108 and throm-
130 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 130

bolytic effects.109 Periprocedural abciximab hasbeen shown to decrease ischemic complicationsand late clinical events after coronary angio-plasty,110 but these results have not been repro-duced in the carotids to prevent neuroembolicevents.28,111,112 However, satisfactory results withGP IIb/IIIa antagonists have been reported,whether used for pharmacologic thrombolysis,62,113
angioplasty, and stenting109,114–117 or other neurovas-cular endovascular procedures.118 Intravenousand/or intra-arterial abciximab has been usedalone or as an adjuvant thrombolytic therapy119–121
and may be a useful tool for managing throm-boembolic episodes without cerebral hemorrhage.
Mechanical reperfusion has been adapted tosmaller coronary and intracranial vessels to treatthromboembolic episodes of diverse origin inhigh-risk patients. Intra-arterial thrombectomydevices, snares for clot retrieval,122,123 and directsuction thrombectomy124,125 cause mechanicaldisruption that may increase the penetration offibrinolytic agents. Similarly, micro-guidewirepassage, laser photoacoustic emulsification, andprimary intracranial angioplasty or endovascu-lar ultrasound may potentiate fibrinolytics orGPIIb/IIIa antagonists.
Spasm and dissection have been linked toimmediate occlusion that leads to transient orpermanent neurologic complications. Arterialspasm is a common response to guidewire tip andcatheter manipulation in the brachiocephalicvessels. Although reversible, it may threatencerebral ischemic status. Intra-arterial vasodila-tors, papaverine, nitroglycerin, or calcium-channelblockers, can alleviate spasm. Nifedipine bymouth or sublingually may prevent and treatvertebral spasm.126
METHODS TO AVOID COMPLICATIONS
Avoiding complications requires good judgment.Do not be overly aggressive. Watch the behaviorof the wire – if the wire does not travel withoutresistance, or if it begins to ‘buck’ and follow a‘zig-zag’ pattern, it is likely in a subintimal plane.Pristine technique that includes gradually cross-ing the lesion is advocated. Avoid creating dis-sections. Avoid angioplasty in subintimal planeseven if the true lumen is re-entered. The force of
the inflation or overinflation may result in perfo-ration. Careful vessel diameter evaluation is ofthe utmost importance in order to avoid overdi-latation and arterial injury secondary to deviceselection.
The best management is prevention ofembolization. Gentle manipulation of the wires,catheters, and sheath is key. As cited above, directstenting is less likely to cause embolization, prob-ably because the procedure is simpler and targetlesion manipulation is reduced.40 Symptomaticcerebral embolization is more likely when treat-ing the right subclavian or innominate artery. Ifthe stenosis or occlusion involves either of thesevessels, then each movement (even simply cross-ing the lesion with a wire) risks embolization tothe common carotid artery, which is in closeproximity. If a lesion at either of these vesselsappears highly calcific or difficult to cross dueto high-grade occlusion, a temporary occlusionof the common carotid artery126 can be perfor-med using a dual brachio-femoral approach in a kissing-balloon fashion to access the targetvessel from the brachial artery (Figure 8.10). Inaddition, aspiration of any debris prior to defla-tion of the occluding balloon may be accom-plished using a long femoral sheath placed atthe ostium of the common carotid artery. Atpresent, sizes of the carotid protection devices,such as filters, limit their use in the subclavianand vertebral arteries; however, alternative pro-
SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 131
Double balloon technique for cerebral protection(arrow)when treating lesions at the ostium of the subclavian orthose that extend into the innominate artery.
Figure 8.10 Double balloon technique as protection forright carotid artery.
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 131

tection devices, like the Parodi system, havebeen successfully applied in this territory.127
Double-balloon techniques are also recommen-ded when there is concern of vertebral arterycompromise (via occlusion or dissection) sec-ondary to subclavian manipulation.40,128 This isespecially important when there are vertebralostial plaques, distal or long lesions in the sub-clavian, or antegrade vertebral flow. Myocardialprotection in patients with prior coronary revas-cularization can be performed by balloon occlu-sion of the LIMA.129
Follow-up
Although restenosis is not as common in the sub-clavian and vertebral arteries as in the vessels ofthe lower extremities, Przewlocki et al128 haveidentified three independent restenosis risk fac-tors in the subclavian and innominate arteries:
1. the implantation of more than one stent2. low stent diameter, and3. difference in systolic blood pressure between
the arms after the procedure.
Similarly, Schillinger et al reported three inde-pendent predictors of restenosis as follows:
1. lesion length more than 2 cm2. residual stenosis greater than 30%, and3. stent implantation.130
Female gender has been proposed as a risk factorfor restenosis as well.131 deVries et al42 compared102 cases of PTA alone in 43 patients vs selectivestent placement for suboptimal dilatation andprocedural dissection in 59 patients. Overall,there was a 5-year patency rate of 89% and, aftera mean follow-up of 34 months, there was nodifference in long-term outcome, even in casestreated for an arterial occlusion. All cases ofrestenosis were attributed to hyperplasia and wereseen during the first 26 months of follow-up,leading the authors to recommend limitedfollow-up. Conversely, Przewlocki et al128 notedrestenosis as late as 2–3 years after angioplasty inthese regions and suggested a longer follow-upperiod to assess the potential for complications.Lin et al performed angiographic evaluation of32 lesions at a mean 11.0 ± 9.6 months followingstenting and reported restenosis in 8 (25%) ves-sels; all patients were asymptomatic. Reference
vessel diameter was the only predictor ofrestenosis in vertebral artery ostial stents.50
SUMMARY
Angioplasty and stenting have been used success-fully in a number of vascular territories to correctflow abnormalities and restore patency, and mayreduce the incidence of serious complications as compared to open surgical intervention. Anexpanding literature suggests endovascular ther-apy is safe and effective and promotes a favorablehemodynamic response, though data from ran-domized trials are not yet available. The complica-tions associated with endovascular therapy areoften preventable. The use of appropriate tech-nique is one of the most important means of eliminating complications. Avoiding technicaldifficulties requires good judgment, and preoper-ative study is vital in determining the indicationand optimal approach for endovascular interven-tion in the subclavian and vertebral arteries. Clin-ical findings and global brachiocephalic imagingmust be part of the routine preoperative work-up.
Angiography remains the gold standard fordiagnosis of cerebrovascular occlusive disease,though newer techniques such as angioCT orMRI offer satisfactory non-invasive target lesionimaging. Three-dimensional reconstruction imag-ing via IVUS is extremely useful for determiningthe presence of calcification and residual stenosis,dissections, inadequate stent dilatation, migration,and thrombus entrapment not visualized withuniplanar angiography. Transcranial Dopplerultrasound is also helpful in operative moni-toring and postoperative follow-up. Carefulvessel diameter evaluation is of the utmostimportance in order to avoid overdilatation andarterial injury secondary to device manipula-tion. Gentle manipulation of the wires, catheters,and sheath is imperative as each movement(even simply crossing the lesion with a wire) risksembolization to the common carotid artery.Although restenosis is not as common in thesubclavian and vertebral arteries as in the vesselsof the lower extremities, it has been reported tooccur as late as 2–3 years after angioplasty; clini-cal follow-up and imaging remains extremelyimportant in patients who have undergoneendovascular intervention.
132 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 132

CHECK LIST FOR EMERGENCY EQUIPMENTFOR INTERVENTIONS IN THIS SPECIFICVESSEL AREA
Angiographic catheters
• Quick-Cross® Catheter (The SpectraneticsCorp, Colorado Springs, CO)
• Soft-Vu® Berenstein (AngioDynamics,Queensbury, NY)
• Impulse® IM Angiographic Catheter (BostonScientific Corp., Natick, MA)
Low-profile balloons
• Savvy® PTA Dilatation Catheter® (CordisCorp, Miami Lakes, FL)
• OPTATM PRO PTA Balloon DilatationCatheter (Cordis Corp, Miami Lakes, FL)
• SterlingTM Monorail® Balloon DilatationCatheter (Boston Scientific Corp, Natick, MA)
Cutting balloons
• FlextomeTM Cutting Balloon® Device (BostonScientific Corporation, Natick, MA)
• AngioSculptTM Scoring Balloon Catheter(AngioScore, Inc, Fremont, CA)
Guiding catheter and long sheath shuttle
(For selective angiographic imaging, increased strengthof distal access, and accurate delivery of balloonexpandable stent by sheath retrieval)
• VISTA BRITE TIP® Guiding Catheter(Cordis Corp., Miami Lakes, FL); shapes: IM,MPA1, Hockey Stick
• Flexor® Check-Flo® Introducers (Cook®
Vascular, Inc, Vandergrift, PA)
Covered stents(For subintimal wire dissection, post predilatationdissection or possible wall injury, perforation, ordisruption)
• iCastTM Covered Stent (Atrium MedicalCorp, Hudson, NH)
• VIABAHN® Endoprosthesis Stent-Graft (WL Gore & Associates, Inc, Flagstaff, AZ)
Snares(Many uses, including thrombectomy)
• Expro® Elite (CoMed Medical Specialties,Littleton, CO)
• EN Snare® Intravascular Retrieval Devices(InterV, Gainesville, FL)
Thrombolysis systems
• Uni*fuse® Infusion Catheter (Angiodynamics,Queensbury, NY)
• EKOS LysUS® Infusion System (EKOS Corp,Bothell, WA), for ultrasound-enhancedthrombolysis
Aspiration thrombectomy
• Diver CETM Clot Extraction Catheter (Ev3,Inc, Plymouth, MN)
Rheolytic thrombectomy
• AngioJet® Thrombectomy System (PossisMedical, Inc, Minneapolis, MN)
Stents for crossing vertebral artery or LIMA
• Bridge® Assurant Stent (Medtronic, Inc,Minneapolis, MN), a modular design lesslikely to jail these vessels
Protection devices
• PAES® Parodi Anti-Embolic System (WLGore & Associates, Inc, Flagstaff, AZ)
REFERENCES
1. Diethrich EB, Garrett HE, Ameriso J et al. Occlusivedisease of the common carotid and subclavian arteriestreated by carotid-subclavian bypass. Analysis of 125cases. Am J Surg 1967; 114: 800–8.
2. De Bakey ME, Crawford ES. Resection and homograftreplacement of innominate and carotid arteries withuse of shunt to maintain circulation. Surg GynecolObstet 1957; 105(2): 129–35.
3. DeBakey ME, Crawford ES, Cooley DA et al. Surgicalconsiderations of occlusive disease of innominate,carotid, subclavian, and vertebral arteries. Ann Surg1959; 149(5): 690–710.
4. Crawford ES, Stowe CL, Powers RW Jr. Occlusion ofthe innominate, common carotid, and subclavian arter-ies: long term results of surgical treatment. Surgery1983; 94: 781.
SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 133
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 133

5. Cinna CS, Safar HA, Lagana A et al. Subclaviancarotid transposition and bypass grafting: consecutivecohort study and systematic review. J Vasc Surg 2002;35: 422–9.
6. Kieffer E. Chirurgie des troncs supra-aortiques. In:Enciclopedie Medico – Chirurgical. Traite de Techniqueschirurgicales – Chirurgie Vasculaire. Paris: Elsevier,1987: 43–120.
7. Mathias K, Staiger J, Thron A et al. [Percutaneoustransluminal dilatation of the subclavian artery(author’s translation).] Dtsch Med Wochenschr 1980;105(1): 16–18.
8. Kerber CW, Cromwell LD, Loehden OL. Catheterdilatation of proximal carotid stenosis during distalbifurcation endarterectomy. Am J Neuroradiol 1980; 1:348–9.
9. Westerband A, Rodriguez JA, Ramaiah V et al.Endovascular therapy in prevention and managementof coronary–subclavian steal. J Vasc Surg 2003; 38(4):699–703; discussion 704.
10. Rodriguez JA, Werner A, Martinez R et al. Stenting foratherosclerosis occlusive disease of the subclavianartery. Ann Vasc Surg 1999; 13: 254–60.
11. Joseph G, Pati PK, Mathews P. Multivessel cutting bal-loon angioplasty in a patient with type III nonspecificaortoarteritis. Ind Heart J 2003; 55(2): 175–7.
12. Sharma BK, Jain S, Bali HK et al. A follow-up study ofballoon angioplasty and de-novo stenting in Takayasuarteritis. Int J Cardiol 2000; 75(Suppl 1): S147–52.
13. Bali HK, Jain S, Jain A et al. Stent supported angio-plasty in Takayasu arteritis. Int J Cardiol 1998; 66(Suppl 1): S213–17.
14. Park JH, Chung JW, Joh JH et al. Aortic and arterialaneurysms in Behcet disease: management with stent-grafts: initial experience. Radiology 2001; 220: 745–50.
15. Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl JMed 2004; 350: 1862–71.
16. Hassen-Khodja R, Kieffer E, and University Associationfor Research in Vascular Surgery. Radiotherapy-inducedsupra-aortic trunk disease: early and long-term resultsof surgical and endovascular reconstruction. J VascSurg 2004; 40(2): 254–61.
17. Chambers CM, Curci JA. Treatment of nonaorticaneurysms in the endograft era: aneurysms of theinnominate and subclavian arteries. Semin Vasc Surg2005; 18(4): 184–90.
18. Sanada J, Matsui O, Terayama N et al. Stent-graftrepair of a mycotic left subclavian artery pseudo-aneurysm. J Endovasc Ther 2003; 10(1): 66–70.
19. Patel AV, Marin ML, Veith FJ. Endovascular graft repairof penetrating subclavian artery injuries. J EndovascSurg 1996; 3(4): 382–8.
20. Marin ML, Veith FJ, Panetta TF. Transluminally placedendovascular stented graft repair for arterial trauma. J Vasc Surg 1994; 20(3): 466–72; discussion 472–3.
21. Castelli P, Caronno R, Piffaretti G. Endovascular repairof traumatic injuries of the subclavian and axillaryarteries. Injury 2005; 36(6): 778–82.
22. Joo JY, Ahn JY, Chung YS. Treatment of intra- andextracranial arterial dissections using stents andembolization. Cardiovasc Interv Radiol 2005; 28(5):595–602.
23. Galli M, Goldberg SL, Zerboni S. Balloon expandablestent implantation after iatrogenic arterial dissectionof the left subclavian artery. Cathet Cardiovasc Diagn1995; 35(4): 355–7.
24. Berguer R, Flynn LM, Kline RA et al. Surgical recon-struction of the extracranial vertebral artery: man-agement and outcome. J Vasc Surg 2000; 31(1 Pt 1):9–18.
25. Kieffer E, Praquin B, Chiche L et al. Distal vertebralartery reconstruction: long-term outcome. J Vasc Surg2002; 36(3): 549–54.
26. Imparato AM. Vertebral arterial reconstruction: anineteen-year experience. J Vasc Surg 1985; 2(4): 626–34.
27. Caplan LR, Wityk RJ, Glass TA et al. New EnglandMedical Center Posterior Circulation registry. AnnNeurol 2004; 56(3): 389–98.
28. Higashida RT, Tsai FY, Halbach VV et al. Transluminalangioplasty for atherosclerotic disease of the vertebraland basilar arteries. J Neurosurg 1993; 78: 192–8.
29. Jenkins JS, White CJ, Ramee SR et al. Vertebral arterystenting. Cathet Cardiovasc Interv 2001; 54: 1–5.
30. Kachel R, Endert G, Basche S et al. Percutaneous trans-luminal angioplasty (dilatation) of carotid, vertebral,and innominate artery stenoses. Cardiovasc IntervRadiol 1987; 10: 142–6.
31. Malek AM, Higashida RT, Reilly LM et al. Subclavianarteritis and pseudoaneurysm formation secondary tostent infection. Cardiovasc Interv Radiol 2000; 23(1):57–60.
32. Mukherjee D, Roffi M, Kapadia SR et al. Percutaneousintervention for symptomatic vertebral artery steno-sis using coronary stents. J Invas Cardiol 2001; 13:363–6.
33. Storey GS, Marks MP, Dake M et al. Vertebral arterystenting following percutaneous transluminal angio-plasty: technical note. J Neurosurg 1996; 84: 883–7.
34. Gahn G, Richter A, Bourquain H et al. Cerebrovascularreserve before and after vertebral artery angioplasty.Am J Neuroradiol 1999; 20(5): 785–6.
35. Cochrane Database System Review 2005 Apr 18; (2):CD000516. Update of: Cochrane Database SystemReview 2000; (2): CD000516.
36. Motarjeme A. Percutaneous transluminal angioplasty ofsupra-aortic vessels. J Endovasc Surg 1996; 3(2): 171–81.
37. Brountzos EN, Petersen B, Binkert C et al. Primarystenting of subclavian and innominate artery occlusivedisease: a single center’s experience. Cardiovasc IntervRadiol 2004; 27(6): 616–23.
134 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 134

38. Branchereau A, Magnan PE, Espinoza H et al. Subcla-vian artery stenosis: hemodynamic aspects and surgicaloutcome. J Cardiovasc Surg (Torino) 1991; 32(5): 604–12.
39. Tunick PA, Kronzon I. Protruding atheromas in thethoracic aorta: a newly recognized source of cerebraland systemic embolization. Echocardiography 1993;10(4): 419–28.
40. Amor M, Eid-Lidt G, Chati Z et al. Endovascular treat-ment of the subclavian artery: stent implantation withor without predilatation. Cathet Cardiovasc Interv2004; 63: 364–70.
41. Huttl K, Nemes B, Simonffy A et al. Angioplasty of theinnominate artery in 89 patients: experience over 19years. Cardiovasc Interv Radiol 2002; 25: 109–14.
42. deVries JP, Jager LC, van den Berg JC et al. Durabilityof percutaneous transluminal angioplasty for obstruc-tive lesions of proximal subclavian artery: long termresults. J Vasc Surg 2005; 41: 19–23.
43. Jaeger HJ, Mathias KD, Drescher R et al. Diffusion-weighted MR imaging after angioplasty or angioplastyplus stenting of arteries supplying the brain. Am JNeuroradiol 2001; 22(7): 1251–9.
44. Bitar R, Moody AR, Leung G et al. In vivo identificationof complicated upper thoracic aorta and arch vesselplaque by MR direct thrombus imaging in patientsinvestigated for cerebrovascular disease. Am JRoentgenol 2006; 187(1): 228–34.
45. Lord RSA. Atheroembolic mechanisms. In: Surgery ofOcclusive Cerebrovascular Disease. Saint Louis, IL:CV Mosby Company, 1986, 112–13.
46. Wityk RJ, Chang HM, Rosengart A. Proximal extracra-nial vertebral artery disease in the New EnglandMedical Center Posterior Circulation Registry. ArchNeurol 1998; 55: 470–8.
47. Shin HK, Yoo KM, Chang HM et al. Bilateral intracra-nial vertebral artery disease in the New EnglandMedical Center Posterion Circulation Registry. ArchNeurol 1999; 56: 1353–8.
48. Chastain HD, Campbell MS, Iyer S et al. Extracranialvertebral artery placement: in-hospital and follow-upresults. J Neurosurg 1999; 91: 547–52.
49. Hauth EA, Gissler HM, Drescher R et al. Angioplastyor stenting of extra- and intracranial vertebral arterystenoses. Cardiovasc Interv Radiol 2004; 27(1): 51–7.
50. Lin YH, Juang JM, Jeng JS et al. Symptomatic ostialvertebral artery stenosis treated with tubular coronarystents: clinical results and restenosis analysis. J EndovascTher 2004; 11(6): 719–26.
51. Savitz SI, Caplan LR. Vertebrobasilar disease. N Engl JMed 2005; 352: 2618–26.
52. Wityk RJ, Lehman D, Klag M et al. Race and sex dif-ferences in the distribution of cerebral atherosclerosis.Stroke 1996; 27: 1974–80.
53. Tyagi S, Verma PK, Gambhir DS et al. Early and long-term results of subclavian angioplasty in aortoarteritis
(Takayasu disease): comparison with atherosclerosis.Cardiovasc Interv Radiol 1998; 21(3): 219–24.
54. Lusic I, Maskovic J, Jankovic S et al. Endoluminalstenting for subclavian artery stenosis in Takayasu’sarteritis. Cerebrovasc Dis 2000; 10(1): 73–5.
55. Min PK, Park S, Jung JH et al. Endovascular therapycombined with immunosuppressive treatment for occlu-sive arterial disease in patients with Takayasu’s arteritis.J Endovasc Ther 2005; 12(1): 28–34.
56. Martinez R, Rodriguez JA, Torruella L et al. Stentingfor occlusion of the subclavian arteries: technicalaspects and follow-up results. Tex Heart Inst J 1997;24: 23–7.
57. Mathias KD, Luth I, Haarmann P. Percutaneous trans-luminal angioplasty of proximal subclavian arteryocclusions. Cardiovasc Interv Radiol 1993; 16(4):214–18.
58. Sullivan TM, Gray BH, Bacharach JM et al. Angioplastyand primary stenting of the subclavian, innominate,and common carotid arteries in 83 patients. J Vasc Surg1998; 28(6): 1059–65.
59. Diethrich EB, Ndiaye M, Reid DB. Stenting in thecarotid artery: initial experience in 110 patients. J Endovasc Surg 1996; 3(1): 42–62.
60. Kumar K, Dorros G, Bates MC et al. Primary stentdeployment in occlusive subclavian artery disease.Cathet Cardiovasc Diagn 1995; 34(4): 281–5.
61. Albuquerque FC, Fiorella D, Han P et al. A reappraisalof angioplasty and stenting for treatment of vertebralorigin stenosis. Neurosurgery 2003; 53: 607–16.
62. Abou-Chebl A, Yadav JS, Reginelli JP et al. Intracranialhemorrhage and hyperperfusion syndrome followingcarotid artery stenting: risk factors, prevention, andtreatment. J Am Coll Cardiol 2004; 43(9): 1596–601.
63. Jenkins JS, White CJ, Ramee SR et al. Vertebral arterystenting. Cathet Cardiovasc Interv 2001; 54: 1–5.
64. Malek AM, Higashida RT, Reilly LM et al. Subclavianarteritis and pseudoaneurysm formation secondary tostent infection. Cardiovasc Interv Radiol 2000; 23(1):57–60.
65. Schmitter SP, Marx M, Bernstein R et al. Angioplasty-induced subclavian artery dissection in a patient withinternal mammary artery graft: treatment with endovas-cular stent and stent-graft. Am J Roentgenol 1995;165(2): 449–51.
66. Kitchens C, Jordan W Jr, Wirthlin D et al. Vascularcomplications arising from maldeployed stents. VascEndovascular Surg 2002; 36(2): 145–54.
67. Morris CS, Bonnevie GJ, Najarian KE. Non surgicaltreatment of acute iatrogenic renal artery angioplastyand stenting. Am J Roentgenol 2001; 17(6): 1353–7.
68. Ecker RD, Guidot CA, Hanel RA et al. Perforation ofexternal carotid artery branch arteries during endolu-minal carotid revascularization procedures: consequencesand management. J Invas Cardiol 2005; 17(6): 292–5
SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 135
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 135

69. Gunning MG, Williams IL, Jewitt DE et al. Coronaryartery perforation during percutaneous intervention:incidence and outcome. Heart 2002; 88(5): 495–8.
70. Weber W, Mayer TE, Henkes H et al. Efficacy of stentangioplasty for symptomatic stenoses of the proximalvertebral artery. Eur J Radiol 2005; 56(2): 240–7.
71. Pernes JM, Marzelle J, Auguste M et al. Techniquesendoluminales de traitement des lesions des troncssupra-aortiques (a l’exception de la carotide interne).Encycl Med Chir Techniques Chirurgicales – ChirurgieVasculaire. Paris: Elsevier, 1999: 43–128.
72. Broadbent LP, Moran CJ, Cross DT 3rd et al. Manage-ment of ruptures complicating angioplasty and stent-ing of supraaortic arteries: report of two cases and areview of the literature. Am J Neuroradiol 2003;24(10): 2057–61.
73. Lin YH, Juang JM, Jeng JS et al. Symptomatic ostialvertebral artery stenosis treated with tubular coronarystents: clinical results and restenosis analysis. J Endo-vasc Ther 2004; 11(6): 719–26.
74. Vitek JJ. Subclavian artery angioplasty and the originof the vertebral artery. Radiology 1989; 170: 407–9.
75. Erbstein BA, Wholey MH, Smoot S. Subclavian arterysteal syndrome: treatment by percutaneous translumi-nal angioplasty. Am J Roentgenol 1988; 151: 291–4.
76. Bachman DM, Kim RM. Transluminal dilatation forsubclavian steal syndrome. Am J Roentgenol 1980; 135:995–6.
77. Ringelstein EB. Delayed reversal of vertebral artery bloodflow following percutaneous transluminal angioplastyfor subclavian steal syndrome. Neuroradiology 1984;26(3): 189–98.
78. de Bray JM, Pasco A, Tranquart F et al. Accuracy ofcolor-Doppler in the quantification of proximal vertebralartery stenoses. Cerebrovasc Dis 2001; 11(4): 335–40.
79. Visona A, Lusiani L, Castellani V et al. The echo-Doppler (duplex) system for the detection of vertebralartery occlusive disease: comparison with angiography.J Ultrasound Med 1986; 5: 247–50.
80. Buckenham TM, Wright IA. Ultrasound of the extracra-nial vertebral artery. Br J Radiol 2004; 77: 15–20.
81. Romero JM, Lev MH, Chan ST et al. Ultrasound ofneurovascular occlusive disease: interpretive pearlsand pitfalls. Radiographics 2002; 22: 1165–76.
82. Crawley F, Clifton A, Brown MM. Treatable lesionsdemonstrated on vertebral angiography for posteriorcirculation ischaemic events. Br J Radiol 1998; 71(852):1266–70.
83. Science Advisory Committee. Cerebral angiography:a report for health professionals by the executiveCommittee of the Stroke Council, American HeartAssociation. Circulation 1989; 79: 474.
84. Brountzos EN, Petersen B, Binkert C et al. Primarystenting of subclavian and innominate artery occlusive
disease: a single center’s experience. Cardiovasc IntervRadiol 2004; 27(6): 616–23.
85. Vince DG, Davies SC. Peripheral application of intravas-cular ultrasound virtual histology. Semin Vasc Surg2004; 17(2): 119–25.
86. Vogt KG, Schroeder TV. Intravascular ultrasound foriliac artery imaging. Clinical review. J CardiovascSurg (Torino) 2001; 42(1): 69–75.
87. Vogt KC, Just S, Rasmussen JG et al. Prediction of out-come after femoropopliteal balloon angioplasty byintravascular ultrasound. Eur J Vasc Endovasc Surg1997; 13(6): 563–8.
88. Liu CP, Ling YH, Kao HL. Use of a pressure-sensingwire to detect sequential pressure gradients for ipsilat-eral vertebral and subclavian artery stenoses. Am JNeuroradiol 2005; 26(7): 1810–12.
89. Tetteroo E, van Engelen AD, Spithoven JH et al. Stentplacement after iliac angioplasty: comparison ofhemodynamic and angiographic criteria. Dutch Iliac Stent Trial Study Group. Radiology 1996; 201:155–9.
90. Chengelis DL, Glover JL, Bendick P et al. The use ofintravascular ultrasound in the management of thoracicoutlet syndrome. Am Surg 1994; 60(8): 592–6.
91. Cheneau E, Mintz GS, Leborgne L et al. Intravascularultrasound predictors of subacute vessel closure afterballoon angioplasty or atherectomy. J Invas Cardiol2004; 16(10): 572–4.
92. van Lankeren W, Gussenhoven EJ, Qureshi A et al.Intravascular ultrasound and histology in in vitro assess-ment of iliac artery angioplasty. Cardiovasc IntervRadiol 1999; 22(1): 50–5.
93. Navarro F, Sullivan TM, Bacharach JM. Intravascularultrasound assessment of iliac stent procedures. J Endovasc Ther 2000; 7(4): 315–19.
94. Sawada M, Hashimoto N, Nishi S et al. Detection ofembolic signals during and after percutaneous trans-luminal angioplasty of subclavian and vertebral arteriesusing transcranial Doppler ultrasonography. Neuro-surgery 1997; 41(3): 535–40.
95. Mintz EP, Gruberg L, Kouperberg E et al. Vertebralartery stenting using distal emboli protection andtranscranial Doppler. Cathet Cardiovasc Interv 2004;61(1): 12–15.
96. Manzoor A, Masaryl T. Imaging of stroke. State of theart. Semin Vasc Surg 2004; 2: 181–205.
97. Staikov IN, Do DD, Remonda L et al. The site of atheromatosis in the subclavian artery and itsimplication for angioplasty. Neuroradiology 1999; 41:537–42.
98. Danetz JS, Cassano AD, Stoner MC et al. Feasibility ofendovascular repair in penetrating axillo-subclavianinjuries: a retrospective review. J Vasc Surg 2005;41(2): 246–54.
136 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 136

99. Kim DJ, Lee BH, Kim DI. Stent-assisted angioplasty ofsymptomatic intracranial vertebrobasilar artery steno-sis: feasibility and follow-up results. Am J Neuroradiol2005; 26: 1381–8.
100. Piotin M, Spelle L. Percutaneous transluminal angio-plasty and stenting of the proximal vertebral artery forsymptomatic stenosis. Am J Neuroradiol 2000; 21:727–31.
101. Cloud GC, Markus HS. Diagnosis and management ofvertebral artery stenosis. Q J Med 2003; 96: 27–34.
102. Purkayastha S, Jayadevan ER, Kapilamoorthy TR et al.Suction thrombectomy of thrombotic occlusion of thesubclavian artery in a case of Takayasu’s arteritis.Cardiovasc Interv Radiol 2006; 29(2): 289–93.
103. Zeller T, Frank U, Burgelin K et al. Acute thromboticsubclavian occlusion treated with a new rotationalthrombectomy device. J Endovasc Ther 2002; 9(6):917–21.
104. Bush RL, Bhama JK, Lin PH et al. Transient ischemicattack due to early carotid stent thrombosis: successfulrescue with rheolytic thrombectomy and systemicabciximab. J Endovasc Ther 2003; 10(5): 870–4.
105. Silva JA, Ramee SR. The emergence of mechanicalthrombectomy; a clot burden reduction approach.Semin Interv Cardiol 2000; 5(3): 137–47.
106. Kasirajan K, Gray B, Beavers FP et al. Rheolyticthrombectomy in the management of acute and suba-cute limb-threatening ischemia. J Vasc Interv Radiol2001; 12: 413–21.
107. Duc SR, Schoch E, Pfyffer M et al. Recanalization ofacute and subacute femoropopliteal artery occlusionswith the Rotarex catheter: one-year follow-up, single-center experience. Cardiovasc Interv Radiol 2005;28(5): 603–10.
108. Coller BS. Anti-GPIIb/IIIa drugs: current strategies andfuture directions. Thromb Haemost 2001; 86(1): 427–43.
109. Houdart E, Woimant F, Chapot R et al. Thrombolysisof extracranial and intracranial arteries after IV abcix-imab. Neurology 2001; 12;56(11): 1582–4.
110. Narins CR, Miller DP, Califf RM et al. The relationshipbetween periprocedural myocardial infarction and sub-sequent target vessel revascularization following per-cutaneous coronary revascularization: insights fromthe EPIC trial. Evaluation of IIb/IIIa platelet receptorantagonist 7E3 in Preventing Ischemic Complications.J Am Coll Cardiol 1999; 33(3): 647–53.
111. Qureshi AI, Suri MF, Khan J et al. Abciximab as anadjunct to high-risk carotid or vertebrobasilar angio-plasty: preliminary experience. Neurosurgery 2000;46(6): 1316–24; discussion 1324–5.
112. Hofmann R, Kerschner K, Steinwender C et al.Abciximab bolus injection does not reduce cerebralischemic complications of elective carotid artery stent-ing: a randomized study. Stroke 2002; 33(3): 725–7.
113. Heo JH, Lee KY, Kim SH et al. Immediate reocclusionfollowing a successful thrombolysis in acute stroke: apilot study. Neurology 2003; 60(10): 1684–7.
114. Ho DS, Wang Y, Chui M et al. Intracarotid abciximabinjection to abort impending ischemic stroke duringcarotid angioplasty. Cerebrovasc Dis 2001; 11(4):300–4.
115. Kittusamy PK, Koenigsberg RA, McCormick DJ.Abciximab for the treatment of acute distal emboliza-tion associated with internal carotid artery angioplasty.Cathet Cardiovasc Interv 2001; 54(2): 221–33.
116. Wallace RC, Furlan AJ, Moliterno DJ et al. Basilarartery rethrombosis: successful treatment with plate-let glycoprotein IIB/IIIA receptor inhibitor. Am JNeuroradiol 1997; 18(7): 1257–60.
117. Fiorella D, Albuquerque FC, Han P et al. Strategies forthe management of intraprocedural thromboemboliccomplications with abciximab (ReoPro). Neurosurgery2004; 54(5): 1089–97; discussion 1097–8.
118. Aviv RI, O’Neill R, Patel MC et al. Abciximab inpatients with ruptured intracranial aneurysms. Am JNeuroradiol 2005; 26(7): 1744–50.
119. Kwon OK, Lee KJ, Han MH et al. Intraarteriallyadministered abciximab as an adjuvant thrombolytictherapy: report of three cases. Am J Neuroradiol 2002;23(3): 447–51.
120. Eckert B, Koch C, Thomalla G et al. Aggressive therapywith intravenous abciximab and intra-arterial rtPA andadditional PTA/stenting improves clinical outcome inacute vertebrobasilar occlusion: combined local fibrinol-ysis and intravenous abciximab in acute vertebrobasilarstroke treatment (FAST): results of a multicenter study.Stroke 2005; 36(6): 1160–5.
121. Steiner-Boker S, Cejna M, Nasel C et al. Successfulrevascularization of acute carotid stent thrombosis by facilitated thrombolysis. Am J Neuroradiol 2004;25(8): 1411–13.
122. Chopko BW, Kerber C, Wong W et al. Transcathetersnare removal of acute middle cerebral artery throm-boembolism: technical case report. Neurosurgery 2000;46(6): 1529–31.
123. Fourie P, Duncan IC. Microsnare-assisted mechanicalremoval of intraprocedural distal middle cerebral arterialthromboembolism. Am J Neuroradiol 2003; 24(4): 630–2.
124. Vallee JN, Crozier S, Guillevin R et al. Acute basilarartery occlusion treated by thromboaspiration in acocaine and ecstasy abuser. Neurology 2003; 61(6):839–41.
125. Lutsep HL, Clark WM, Nesbit GM et al. Intraarterialsuction thrombectomy in acute stroke. Am J Neuroradiol2002; 23(5): 783–6.
126. Vitek JJ, Keller FS, Duvall ER et al. Brachiocephalicartery dilation by percutaneous transluminal angioplasty.Radiology 1986; 158(3): 779–95.
SUBCLAVIAN AND VERTEBRAL ARTERY INTERVENTIONS 137
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 137

127. Pieniazek P, Musialek P, Motyl R et al. Use of theParodi Anti-Emboli System and transient subclaviansteal for cerebral protection during emergent vertebralartery recanalization. J Endovasc Ther 2004; 11(4):511–16.
128. Przewlocki T, Kablak-Ziembicka A, Pieniazek P et al.Determinants of immediate and long-term results ofsubclavian and innominate artery angioplasty. CathetCardiovasc Interv 2006; 67(4): 519–26.
129. Jones RD, Uberoi R. Subclavian artery angioplasty forthe treatment of angina using a double balloon tech-nique to protect a left internal mammary artery graft.Eur Radiol 2002; 12: 908–10.
130. Schillinger M, Haumer M, Schillinger S. Risk stratifi-cation for subclavian artery angioplasty: is there anincreased rate of restenosis after stent implantation? J Endovasc Ther 2001; 8: 550–7.
131. Bates MC, Almehmi A. Fatal subclavian stent infectionremote from implantation. Cathet Cardiovasc Interv2005; 65(4): 535–9.
132. Henry M, Polydorou A, Henry I et al. Angioplasty andstenting of extracranial vertebral artery stenosis. IntAngiol 2005; 24(4): 311–24.
133. Insall RL, Lambert D, Chamberlain J et al. Percu-taneous transluminal angioplasty of the innominate,subclavian and axillary arteries. Eur J Vasc Surg 1990;4: 591–5.
134. Al-Mubarak N, Liu MW, Dean LS et al. Immediate andlate outcomes of subclavian artery stenting. CathetCardiovasc Interv 1999; 46(2): 169–72.
135. Sadato A, Satow T, Ishii A et al. Endovascular recanal-ization of subclavian artery occlusions. Neurol MedChir (Tokyo) 2004; 44(9): 447–53; discussion 454–5.
136. Wilms G, Baert A, Dewaele D et al. Percutaneous trans-luminal angioplasty of the subclavian artery: early andlate results. Cardiovasc Interv Radiol 1987; 10(3): 123–8.
137. Janssens E, Gautier C, Godefroy O et al. Percutaneoustransluminal angioplasty of proximal vertebral arterystenosis: long-term clinical follow-up of 16 consecu-tive patients. Neuroradiology 2004; 46(1): 81–4.
138 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter08.qxp 4/5/2007 2:45 PM Page 138

INTRODUCTION TO THE FREQUENCY AND TYPE OF COMPLICATIONS
The most devastating complication of aortic dis-ease is hemorrhage, resulting in death. Thoracicand abdominal aortic aneurysms have a naturalhistory of expansion and inevitable rupture, ifleft untreated. Aortic dissections and penetrat-ing aortic ulcers are other major aortic diseaseprocesses with serious consequences.
Abdominal aortic aneurysms (AAAs) areresponsible for 15 000 deaths in the United Statesannually.1 They represent the third leading causeof death in men over 60 years of age. Thoracicaneurysms occur less frequently than AAAs,with an incidence of 10.4 cases per 100 000 person-years.2 Acute aortic dissection is the most frequentcatastrophe of the aorta. It has an incidence of 5 to 30 cases per 1 million people per year.3–6
Untreated, the mortality of acute dissection is50% within the first 24 hours.7
Traditional open surgical repair of AAAs anddissections has consisted of transperitoneal orretroperitoneal incision, followed by aortic cross-clamping, and transposition of the diseased seg-ment with a tube graft. The 30-day mortality ofopen abdominal aortic aneurysm repair standsat 3.8 to 8.2%.8 The more common complica-tions of open repair include hemorrhage, cardiacischemia, hypotension from aortic declamping,sexual dysfunction, iatrogenic ureteral injury,
renal failure, distal embolization, visceral ischemia,and paraplegia. Late complications include aorto-enteric fistula (0.9%), pseudoaneurysm (1.3%),and graft infection (0.4%).9
Open repair of thoracic aortic aneurysmsand dissection is an invasive procedure thatincludes thoracotomy, aortic cross-clamping,left heart bypass, and transposition of the tho-racic aorta with a tube graft. Mortality rates forpatients undergoing open thoraco-abdominaland descending thoracic aortic aneurysm repairsrange from 4 to 21%.10–13
The first endovascular abdominal aortic aneu-rysm repair (EVAR) in a human was describedby Parodi in 1991.14 The first EVAR was com-pleted in the United States in 1995.15 Since then,advances in the endovascular treatment ofthoracic and abdominal aortic diseases haveaccelerated with breathtaking speed. It is nowreported that 45 to 80% of patients with AAAsare candidates for EVAR.16–18 This phenomenonis primarily due to increasing experience, newertechnology, and increasing referrals.
EVAR has the advantage of avoiding majorabdominal or retroperitoneal incisions and bowelmanipulation, as well as decreasing postopera-tive pain and fluid requirements.19 EVAR alsoobviates many of the cardiac, respiratory, and renalcomplications that frequently accompany openrepair, with reductions from 11 to 5% in cardiac
9
Aortic aneurysmal diseaseJoe T Huang, Takao Ohki, and Frank J Veith
Introduction to the frequency and type of complications • Complications after endovascular aorticaneurysm repair • Types of complications • Factors identifying high-risk patients for complications ofEVAR • Complications of thoracic endovascular grafting (EVG) • Methods to detect/avoid complications • Emergency endovascular aortic aneurysm repair • Summary
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 139

complications and 5 to 3% in pulmonary compli-cations.20 EVAR is thus associated with fasterrecovery times and shorter intensive care stays.
In patients with diseases of the descendingthoracic aorta, up to 57% of these patients arepotential candidates for endovascular grafting.21
Indications for endovascular therapy of thoracicaortic disease are constantly expanding. Diseasestreatable by endovascular techniques now includechronic dissections, pseudoaneurysms, degener-ative aneurysms, mycotic aneurysms, traumaticaortic dissections, type B aortic dissections, intra-mural hematomas, and penetrating aortic ulcers.22
Endovascular repair of thoracic aortic disease isparticularly appealing to patients who would nor-mally be considered poor surgical candidates. It isconsiderably less invasive than open surgicaloptions and avoids complications associated withopen thoracotomy, aortic cross-clamping, and leftheart bypass. Perioperative mortality rates of 3 to 12% have been reported for endovasculartreatment.23
COMPLICATIONS AFTER ENDOVASCULARAORTIC ANEURYSM REPAIR
While there are distinct advantages to endovascu-lar repair of thoracic and aortic diseases, thereare also disadvantages of endografting for thesediseases. By undergoing an endovascular aorticrepair, the patient is committing to lifelong imag-ing surveillance because of a host of complicationsspecific to endovascular therapy. Endovascularrepair is also potentially more costly than opensurgery, with the graft device comprising 52% oftotal costs.24
Initial experience with EVAR saw conversionsto open repair secondary to limited operatorexperience, patient selection, and early genera-tion devices. However, the rate of early conver-sion (defined as any open repair within 30 daysof initial EVAR) has fallen to 0.7%.25 In oneseries by Verzini et al, causes for early conversionto open repair included significant vessel calci-fications, aortic neck rupture, and inability tocatheterize the contralateral limb of the graft.26
Treatment included open repair with tube graftsor bifurcated grafts. Rates of late conversionrange widely, from 4 to 50%.14 The recently pub-lished EVAR 1 trial, with an average follow-up
of 3.3 years, reported a cumulative conversionrate of 2.6%.27
While actual rates of secondary interventionafter EVAR range from 10 to 20% per year, thereis a higher number of observed complications.28–30
According to the EVAR 1 trial results at 4 years,41% of patients experienced at least one compli-cation after EVAR, compared with 9% in the openrepair group. The most common complicationsin this study were type II endoleaks (42%), type Iendoleaks (14%), graft thrombosis (6.5%), andgraft migration (6.5%).27 Similarly, the DutchRandomized Endovascular Aneurysm Manage-ment (DREAM) trial had a rate of secondaryintervention for EVAR that was three times therate of open repair in the first 9 months.31
In the DREAM trial, the acute benefit ofEVAR translated into lower cumulative rates of aneurysm-related deaths. At 2 years, theaneurysm-related death rate was, 2.1% for EVARand 5.7% for open repair. There was, however, nodifference in cumulative survival between openrepair and endovascular repair at 2 years (89.6%vs 89.7%). Four-year results from the EVAR 1 trialalso demonstrated a small but a significant reduc-tion in aneurysm-related deaths with EVAR(4% versus 7%), with no difference in all-causemortality between the two groups of patientsrandomized to EVAR versus open repair.
In one series by Cao et al, 1119 patients treatedwith either open repair or EVAR were followedover a minimum of 7 years.32 The overall risk forsecondary procedures after EVAR was reportedat 49.4%, compared with 7.1% in the open repairgroup. Despite the higher rate of re-intervention,freedom from aneurysm-related death at 84months showed minor differences (97.5% in theEVAR group and 95.9% in the open repairgroup).32,33
TYPES OF COMPLICATIONS
Endoleaks
Endoleaks are complications unique to endovas-cular aneurysm repair. An endoleak is definedas persistent blood flow outside the graft andwithin the aneurysm sac.34 Positive predictors ofendoleak include large proximal aortic neck diam-eter, large aneurysm size, severe angulation of
140 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 140

the proximal infrarenal neck, patent inferiormesenteric artery (IMA), and lack of thrombus orsmall amounts of thrombus in the aneurysm sac.Twenty percent of patients will present withendoleak at some point during follow-up. Sevenpercent of these patients present one monthpostoperatively and the remaining 13% are foundlater.35–38 There are four major types of endoleaks,as listed in Table 9.1. Types I and III are termedgraft-related endoleaks, while type II is referredto as a collateral endoleak. Approximately 70%of early endoleaks disappear within 30 days,with the majority being type II endoleaks.39–41
Diagnosis of endoleaks is accomplished primar-ily through computed tomography (CT) scanningwith iv contrast. It is useful for detecting contrastflow in the sac and for measuring aortic diame-ters. The imaging protocol should include delayedphases in order to visualize any vessels thatmay be supplying type II endoleaks. Biphasic CTscanning improves rates of detection by 11%when compared to CT scanning with arterial phaseonly.42 CT angiography with three-dimensional(3D) reconstruction is also useful, but not aswidely available. Color duplex ultrasound isalso frequently used, with a sensitivity of 95%and specificity of 97% for detecting endoleaks.43
Duplex imaging is better at detecting limb outflowdisturbances than CT. Ultrasound also has theadvantage of being non-invasive, non-irradiating,and more repeatable. However, it is highly oper-ator dependent and artifacts such as bowel gasand body fat can obscure findings. Magneticresonance arteriography (MRA) and selective arte-riography are other diagnostic modalities. Angiog-raphy is an invasive procedure with inherentrisks, but offers the possibility of simultaneousendoleak treatment at the time of diagnosis. Plainabdominal films are also very helpful to evaluatefor stent fracture, stent migration, limb disasso-ciations, and graft kinks.
Type I endoleak
The incidence of type I endoleak is approxi-mately 10%.44 It is defined as an inadequate sealbetween the endograft and native aorta at theproximal or distal attachment sites, which resultsin continued blood flow and pressurization intothe aneurysm sac. Proximal type I endoleaksnecessitate intervention as they are likely to per-sist and can lead to aneurysm rupture.
Endovascular treatment modalities includeballoon angioplasty of the proximal and distal
AORTIC ANEURYSMAL DISEASE 141
Table 9.1 Endoleak classification system
Classification Alternative terms Forms
Type I Graft-related endoleak A Proximal graft attachment sitePeri-graft leak B Distal graft attachment siteAttachment endoleak C Iliac occluderPeri-graft channel
Type II Retrograde endoleak A Simple or to-and-fro (1 patent branch)Branch endoleak B Complex or flow-through (�2 patent branches)Collateral flow Patent branches lumbar, IMA, intercostals,
internal iliac, subclavian, etc.Type III Fabric tear A Junctional leak or modular disconnect
Modular disconnection B Fabric disruptionMinor (<2 mm; e.g. suture holes)Major (�2 mm)
Type IV Fabric porosity (<30 days Graft wall fabric porosity or suture holesafter graft placement)
Endotension Type V endoleak See Table 9.2EndopressurePseudo-endoleakPressure leak
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 141

ends, the placement of additional bare stents (usu-ally balloon-expandable stents), and the place-ment of additional aortic cuffs.45 If endovascularintervention cannot be carried out, early or lateconversion to open repair may be necessary.Options include banding of the proximal or distalattachment sites, suturing of the endoleak underdirect visualization, or open surgical repair with aconventional graft.19 The key to preventing type Iendoleaks is appropriate oversizing of the prox-imal and distal ends of the graft.46 However, oneshould note that excessive oversizing (>30%)will also lead to increased rates of migration(Figure 9.1a–c).
Type II endoleak
Type II endoleaks are defined as flow from patentside branches, e.g. inferior mesenteric arteries,lumbar arteries, visceral vessels, and hypogas-tric arteries. The incidence of this complicationranges from 10 to 25% and comprises the major-ity of endoleaks.44 Those identified via angiogra-phy upon completion of endograft deploymentare often managed conservatively, because mosttype II endoleaks are considered to be low flowand resolve spontaneously.
Vigilant monitoring of these endoleaks, aswell as measurement of the AAA diameter uti-lizing CT, has been advocated, with an increasein diameter of 5 mm representing a significantvalue.47 However, the association between type II
endoleaks and aneurysm sac enlargement isunclear. While some studies have shown a higherincidence of aneurysm growth in the presence oftype II endoleaks, others have not demonstrateda significant change in aneurysm size despite thepresence of type II endoleaks.38,48–50 It is impor-tant to note that type II endoleaks are not entirelybenign, as they have been associated with casesof aneurysm rupture, albeit anecdotal.51–54 Thereis continued debate about the significance of thistype of endoleak and the timing of intervention.Some groups advocate conservative managementfor all type II endoleaks while others intervenein all type II endoleaks. Others recommendtreatment if the aneurysm sac is observed to beexpanding.50,55–57 It is also important to exclude inthese patients the possibility of type I or type IIIendoleaks that should be fixed more promptly.
Treatment methods for type II endoleaks in-clude coil embolization of the responsible branch,either via a transarterial approach (femoral orbrachial) or direct translumbar puncture of theaneurysm sac. The inferior mesenteric artery canbe approached through the superior mesentericand meandering collaterals, while the lumbararteries can be accessed through hypogastric andthe ilio-lumbar artery. These treatment options,however, are technically challenging.58–62 Othermethods include laparoscopic clipping of sidebranches, injection of thrombin polymer, andthrombogenic sponge placement within the sac tofacilitate thrombosis of the excluded aneurysm.63
142 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b) (c)
Figure 9.1 (a) Type I endoleak. (b) Type I endoleak with proximal aortic cuff placement. (c) Type I endoleak; completionangiogram.
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 142

In one study by Baum et al, 92% of patients treatedwith translumbar embolization of the aneurysmsac were successfully treated, while 80% ofpatients who underwent transarterial emboliza-tion of the inferior mesenteric artery failed ther-apy.58 The study concluded that transarterialtechniques to embolize aneurysm sacs may notbe durable methods of treating type II endoleaks.
Various studies have also examined the prac-tice of preoperative embolization of patent sidebranches to prevent type II endoleaks. Resultsindicate that the presence of patent lumbar andinferior mesenteric vessels is a poor predictor ofthe formation of type II endoleaks. Therefore,such preventive measures should not be taken44
(Figures 9.2 and 9.3).
Type III endoleak
A type III endoleak is persistent blood flow froma tear in the graft fabric or from component sepa-ration. It is subcategorized as a minor disruptionwhen the fabric perforation is less than 2 mmand as a major disruption when the perforationis greater than 2 mm.63 Grouped with type Iendoleaks, type III endoleaks occur in approxi-mately 12% of patients undergoing EVAR.19
This type of complication increases the risk ofrupture nearly 9-fold.51 Therefore, discovery of atype III endoleak necessitates prompt therapy,
especially if it appears late during follow-up.Endovascular management of type III endoleaksconsists of deploying additional stent graftsover the graft defects. If the damage to the stentgraft is severe, then conventional open repair isnecessary (Figure 9.4).
Type IV endoleak
Type IV endoleaks are due to graft porosity andsuture holes that permit the leakage of bloodthrough the graft. Approximately 30% of graftswill allow contrast into the aneurysm sac in thefirst few days after EVAR. However, most resolve
AORTIC ANEURYSMAL DISEASE 143
Figure 9.2 Type II endoleak on CT scan.
(a)
(b)
Figure 9.3 (a) Translumbar angiogram of type II endoleak.(b) Translumbar catheterization with coil embolization oftype II endoleak.
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 143

spontaneously within one month.64 Earlier devices,which utilized thinner graft material, encounteredhigher rates of type IV endoleak than currentdevices. Type IV endoleaks are believed to belimited in their nature.
Endotension
Endotension, also referred to as type V endoleak,is defined as persistent or recurrent pressuriza-tion of the aneurysm sac after EVAR in the absenceof endoleak.22 An alternate definition is pressur-ization of the aneurysm sac, regardless of thepresence of a detectable endoleak. As describedby Gilling-Smith et al, this broader definitionstates that increased sac pressure is the causativefactor for aneurysm rupture, rather than bloodflow.65,66 Possible causes of endotension are listedin Table 9.2.
The presence of endotension is suspectedwhen there are observed increases in aneurysm
diameter on radiographic imaging. The next stepin diagnosis involves aneurysm sac pressuremeasurements, either through direct intra-arterialcatheterization or translumbar puncture of theaneurysm sac. These options are invasive bynature. As a result, there has been an impetus todevelop newer non-invasive methods for moni-toring direct sac pressures. Recently approvedfor commercial use is a wireless, battery-less,radiofrequency-activated pressure sensor that canbe implanted in the excluded aneurysm sac at thetime of EVAR. The advent of this device makesit possible to non-invasively detect endotensionand potential endoleaks67 (Figure 9.5).
Treatment for endotension includes open sur-gical repair, especially if the aneurysm becomesextremely large and causes a mass effect (Figure9.6). Symptoms may include abdominal or backpain and constipation. However, in a reportfrom the EUROSTAR registry on 2463 patients,endotension was identified in 97 patients (3.7%),
144 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b) (c)
Figure 9.4 (a) Type III endoleak due to component separation. (b) Type III endoleak on angiogram. (c) Type III endoleak;completion angiogram after additional cuff placement.
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 144

of whom only 3 (3.3%) underwent open repair.68
Other treatment options include conservativemanagement with an increased frequency of clin-ical and radiographic monitoring and secondaryendograft procedures.69 Our policy is to treatendotension conservatively until the patient com-plains of symptoms related to the presence of alarge aneurysm sac. Endotension may also betreated endovascularly by placing a second layerof endograft within the first one. This reliningmethod is effective in decreasing the porosity ofthe first endograft (Table 9.2).
Stent migration
Graft migration is defined as movement of thegraft more than 5 mm distally. Movement occurswhen the displacement forces on the graft exceedthe strength of the endograft at its proximal anddistal attachment sites. Displacement from theproximal site poses the greatest risk of danger.
Stent migration can lead to endoleak, graftkinking, rupture, and graft thrombosis.70 Ourielet al reported a migration rate of 3.6% at oneyear after EVAR.71 Reported migration ratesvary widely, with Conners et al reporting a 7%rate of migration at 1 year, 20% at 2 years, and42% at 3 years.72 In the AneuRx clinical trial,migration was reported in 94 of 1119 cases.73
Freedom from migration was 98.6% at 1 year,93.4% at 2 years, and 81.2% at 3 years by Kaplan–Meier analysis (Figure 9.7).
One risk factor for stent migration is dilation ofthe proximal aortic neck after EVAR and resultantdislodgement of the stent. The incidence of proxi-mal neck dilatation has a range of 10 to 36%.72–80
It is known that patients with larger aneurysmsare at higher risk for neck dilatation.72,75 Univariateand multivariate analysis of the study by Zarinset al revealed that renal artery to stent graft dis-tance and proximal fixation length are also signifi-cant predictors of migration, with each millimeterincrease in distance below the renal arteries in-creasing risk for subsequent migration by 5.8%and each millimeter increase in proximal fixationlength decreasing risk for migration by 2.5%.73
Mohan et al studied 2862 patients using amathematical regression model for blood flowto identify variables associated with stent graftmigration.81 Ninety-nine (3.5%) patients devel-oped stent graft migration, which was clinicallyrelevant in 85 (3.0%) patients. Hypertension,smoking, maximal aortic diameter, and distaltransverse aortic diameter correlated with migra-tion in their univariate analysis. Analysis of graftcharacteristics revealed that increasing proximalgraft size was associated with migration, witheach increase of 1.0 mm in graft diameter elevat-ing the risk of migration by 1.13. Patients with aproximal graft diameter greater than 30 mm werefound to have 2.5 times the risk of migrationcompared to patients with a graft diameter of lessthan 24 mm in multivariate analysis. Likewise,for patients with a distal transverse aortic diam-eter greater than 30 mm, the risk was 2.54 timesgreater compared to patients with a diameter ofless than 24 mm. The risk of stent graft migra-tion was also increased for longer aneurysms(longer than 12.6 cm) and for those with iliacartery diameters larger than 1.6 cm. On multi-variate analysis, current smoking, hypertension,
AORTIC ANEURYSMAL DISEASE 145
Table 9.2 Mechanisms of endotension
PPoossssiibbllee mmeecchhaanniissmmss ooff eennddootteennssiioonn113344
PPrreessssuurree ttrraannssmmiissssiioonn ttoo aanneeuurryyssmm ssaacc aarroouunndd tthheeeennddss ooff ggrraafftt• Layer of thrombus between the graft and aortic
wall135,136
• Graft displacement exposing thrombus layer ataortic neck
• Endoleak channel sealed by thrombus• Undetected endoleak• Intermittent endoleak channel136
• Very low flow endoleak channel
PPrreessssuurree ttrraannssmmiissssiioonn tthhrroouugghh ggrraafftt wwaallll• High graft porosity• Microleak through graft interstices137
• Transudation/exudation of fluid through graftfabric138
• Graft pulsatility/wall movements
PPrreessssuurree ttrraannssmmiissssiioonn ffrroomm bbrraanncchh vveesssseellss• Thrombus over orifice of internal mesenteric or
lumbar arteries
PPrreessssuurree bbuuiilldd--uupp ffrroomm fflluuiidd aaccccuummuullaattiioonn iinn ssiittuu• Graft infection• Thrombus fibrinolysis/hygroma139
• Genetic modulation• Enzymatic activity• Others
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 145

distal transverse aortic diameter, maximumcommon iliac diameter, and increasing proximalgraft size were significantly associated withstent graft migration.
Graft migration can be reduced through strictadherence to a particular stent graft’s instructionsfor use (IFU) when selecting patients. Aneurysmsthat have adequate and less angulated proximalaortic necks also decrease the likelihood of graftmigration. Precise graft placement adjacent to therenal arteries as well as the hypogastric arterydistally is equally important.19,37,72 Conservativemanagement may be acceptable if there is no evi-dence of endoleaks, aneurysm expansion, or signsof ongoing migration. Interventions for migra-tion include the placement of balloon-expandablestents, endograft cuffs, or open surgical repair.The practice of oversizing stents by 20% relativeto the proximal neck diameter is also aimed atpreventing graft migration.46 Balloon expansionof the proximal aortic neck may also improveproximal graft fixation. We examined 41 patientswho underwent EVAR with a balloon-expandableendograft and were followed for an average of31 months.82 Aortic neck diameters were mea-sured at the level of the lowest renal artery and5 mm distally. Proximal neck dilatation was
146 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(b)
(a)
Figure 9.5 (a) CardioMEMS antenna. (b) CardioMEMS wireless pressure sensor.
Figure 9.6 Endotension; enlarging aneurysm withoutevidence of endoleak.
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 146

defined as neck enlargement of 2.5 mm or more.To assess endograft migration, the distancebetween the superior mesenteric artery and theproximal end of the stent was measured. Stentmigration was defined as a change of 5 mm ormore. The maximum aneurysm diameter wasunchanged or decreased in 85% of this group ofpatients who had balloon-expandable endografts.The immediate postoperative proximal neckdiameter was 19 to 29 mm and was unchangedduring follow-up. None of the patients had sig-nificant proximal neck dilatation and none of thepatients developed significant endograft migra-tion. This study concludes balloon expandablestents are superior as a means of fixation.
Endografts with hooks, barbs, or supra-renalfixation devices have a lower rate of migration.For example, Malina et al reported that the addi-tion of suprarenal stents, hooks, and barbs ongrafts enhanced proximal fixation 10-fold, whilestents that rely on radial force and friction hadno impact on fixation, with the most secureproximal fixation device being pararenal barbedstents.70,83,84 An additional method of minimizingmigration is to increase the columnar strength ofthe endograft by adding longitudinal bars,although the efficacy of this method is less clear.
A vascular endostapling device has been devel-oped to attach the graft to the aortic wall. Thisdevice is introduced through a 13 Fr sheath. Anoptic fiber and endostaple are used to penetratethe endograft and aortic wall at a desired location.The endostaple is inserted, assumes its preformedshape, and behaves like a wire suture.85 Possibleapplications of this device include prevention ofgraft migration, sealing or preventing graft migra-tion, and expansion of EVAR to aneurysms with‘unfavorable’ necks. Other devices include anendostapling device which utilizes a motor drivennitinol screw to secure the endograft to the aorticwall.86
Stent fracture
The endograft prosthesis comprises a fabric anda metallic skeleton. Graft materials on the markettoday include polytetrafluoroethylene (PTFE)and Dacron®. Some grafts have metallic stentsonly at the proximal and distal ends. Others havea metallic exoskeleton throughout the graft. Themetal compounds used include nitinol, Elgiloy,and stainless steel. Nitinol is an alloy that is 55%nickel and 45% titanium. Stents made from thisalloy have shape memory and are self-expanding.
AORTIC ANEURYSMAL DISEASE 147
(a) (b)
Figure 9.7 (a) Stent graft. (b) Stent graft with migration.
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 147

Elgiloy (Elgiloy Limited Partnership, Elgin, IL)is 40% cobalt, 20% chromium, and 15% nickel.The remaining components include iron man-ganese, molybdenum mohybian nolinium, car-bon, and beryllium.87
Stent fractures occur due to stress fatigue onthe metallic stents. Sites where the graft is suturedto metallic stents are points of stress and canfracture. Kinking or sharp angulation of thestent can subject the stent graft to micromotionwith each cardiac cycle and place it at increasedrisk for stent fracture.88,89 Some stents possessendoskeletons held together by sutures. Thesesutures have the potential to break or becomeuntied. The endoskeleton can buckle and the tipscan come into contact with the graft, with resul-tant graft erosions and type III endoleaks.90 Manystent fractures can be diagnosed through plainabdominal films. Treatment options includeplacement of additional bare stents, additionalstent grafts, or open surgical repair.
Rupture
Rupture is the most devastating complication ofaortic aneurysms.53,91–93 The incidence of ruptureafter EVAR ranges from 0.2 to 1.0%.29,51,94–97
Analysis of EUROSTAR data concluded there arethree independent predictors of aneurysm rup-ture after EVAR: history of continuing aneurysmexpansion, proximal stent migration, and type IIIendoleak.98 Causes of rupture include migration,component separation, fabric erosions, and endo-leaks. Rupture after EVAR is usually treated withemergency open conversion, but secondary endo-grafting has also been reported (Figure 9.8).
Thrombosis
Graft limb occlusions after EVAR have beenreported to have an incidence of 0 to 15%.99–101 Ina series by Sampram et al, involving 703 patientsof a single institution, there was a graft limbocclusion incidence of 2.8%. Risk was determinedto be 2.7% at 1 year, 4.1% at 2 years, and 5.5% at3 years postrepair.102 Etiologies of graft limbocclusion include compression of the graft in theproximal neck, compression of the limb in anarrow distal aneurysm neck, kinking or com-pression of the limb, peripheral vascular disease
causing poor run-off, and limb twisting duringdeployment. Kinking can be due to excessive graftoversizing, tortuous iliac vessels, or the use of anunsupported endograft.19,103
To prevent thrombosis, narrow proximal aorticnecks should be preferentially treated with longbodied grafts. In cases of tortuous iliac arteries,fully supported flexible grafts should be used. Ifan iliac limb kinks, it can be stented to preventsubsequent occlusion. If one graft limb throm-boses, a possible solution is the creation of afemoral–femoral graft.19
Hip and buttock claudication
Hip and buttock claudication can occur from theocclusion of one or both hypogastric arteries. It canmanifest as pain in the region or as impotence.Occlusion can be inadvertent, such as covering
148 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a)
(b)
Figure 9.8 (a) CT scan demonstrating type I endoleak. (b) Type I endoleak and posterolateral aneurysm rupture.
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 148

by the graft limbs. Extension of the iliac limbs toexclude aneurysmal common iliac arteries andintentional coil embolization of the hypogastricarteries during graft deployment is another etiol-ogy. With the occlusion of these vessels bilater-ally, the collateral circulation for the left coloncan be compromised, with left colon ischemiaarising as a potential complication. There is areported incidence of 26 to 41% of hip and but-tock claudication after coil embolization of thehypogastric artery.104–109 In this situation, a surgi-cal bypass from the external iliac artery to theinternal iliac artery can be created, although rarelyindicated.110
Renal compromise due to the use of suprarenal stents
The development of endografts capable of sup-rarenal proximal fixation is a welcome addition tothe arsenal of devices at the disposal of endovas-cular specialists. Kalliafas et al observed a lowerrate of graft migration in suprarenally fixatedgrafts versus infrarenally fixated grafts (2.1% ver-sus 10.9%).112 Suprarenal fixation is accomplishedby having bare stents cross the orifices of therenal arteries, which permits blood flow into thesevessels. While there have been concerns aboutthe bare stents causing renal artery occlusion oremboli to the kidney this concern has not beenvalidated. Studies have demonstrated minimalflow disturbances.113–115 In one study by Burkset al, 192 patients underwent EVAR with addi-tional long (15 mm) uncovered Parodi/Palmazor Talent-LPS stent segments placed at the prox-imal attachment sites.116 Based on postoperativeimaging follow-up, 95 patients (49%) showed theuncovered stent at or above the level of the supe-rior mesenteric artery. In 23 patients (12%), thestent extended to the celiac artery. After an aver-age of 25 months of follow-up, serum creatininelevels were unchanged. Contrast-enhanced CTscans demonstrated no stenoses or occlusions inthe celiac, superior mesenteric, or renal arteries.In addition, there was no evidence of renal,hepatic, splenic, or intestinal infarctions. Themost important aspect regarding this potentialcomplication is deployment of the fabric-encasedportion of the stent graft as close to the level ofthe lower renal arteries as possible without
vessel occlusion. Accuracy of placement thushinges on operator experience, the delivery sys-tem, and the resolution of imaging equipment.
Access artery injury
The delivery of large endografts through dis-eased iliac arteries can lead to perforation anddissection. Prompt recognition and treatmentwith covered stents is essential for perforations.For dissections of access arteries, the use of self-expandable or balloon-expandable stents hasbeen highly effective. Transfemoral exposure andfemoral artery puncture can also be associatedwith pseudoaneurysms, seroma formation, andwound infection. Seromas form in approximately15% of cases but usually resolve spontaneously.Wound infection rates are low and stand atapproximately 2%.117 Inability to traverse the iliacarteries was historically the most common sourceof procedure failure.118,119 This phenomenon isnow rare. The routine use of stiff guidewires hasminimized this problem. The external iliac arter-ies are usually the most tortuous, but are also themost easily corrected. The combination of tortu-ous and calcified common iliac arteries is moredifficult, but still amenable with the use of a stiffguidewire (e.g. Amplatz) and a trackable deliverysystem. A trackable delivery sheath does not haveto be highly flexible, merely a smooth, taperedprofile.46
FACTORS IDENTIFYING HIGH-RISK PATIENTSFOR COMPLICATIONS OF EVAR
Female gender
Female gender is believed to be a high-risk factorfor complications, due to less favorable aortic neckanatomy. Women in general have shorter andwider aortic necks, more angulations, and smallercaliber iliac arteries. These variables decrease thenumber of women suitable for EVAR and alsomake femoral access more challenging.
Large initial AAA size
Large preoperative aortic aneurysm size is anotherknown predictor of complications from EVAR.These aneurysms are less likely to have favorable
AORTIC ANEURYSMAL DISEASE 149
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 149

neck anatomy by possessing wider, shorter,more angulated aortic necks.120 There is also apositive correlation between aneurysm size andthe incidence of preoperative co-morbidities.121,122
In one EUROSTAR series, 4-year outcomeswere less favorable for large and medium sizedaneurysms compared with smaller aneurysms(<5.4 cm) treated with EVAR.27,47,122 Over 4000patients who had undergone EVAR were ana-lyzed over 6 years. Patients were divided intothree groups based on aneurysm size: group A(n = 1962), 4.0 to 5.4 cm; group B (n = 1528), 5.5to 6.4 cm; group C (n = 902), 6.5 cm or larger.Device-related endoleaks were more frequentlyobserved in group C compared with groups Aand B (9.9% compared with 3.7% and 6.8%).Postoperatively, systemic complications weremore frequently present in group C (17.4%versus 12.0% in group A, and 12.6% in group B).Thirty day mortality was approximately twiceas high in group C compared with the othergroups combined (4.1% vs 2.1%). Late rupturewas also most frequent in group C. Follow-upresults at midterm were less favorable in groupsC and B compared with group A (freedom fromrupture, 90%, 98%, and 98% at 4 years in groupsC, B, and A, respectively). Aneurysm-relateddeath was highest in group C (88% freedom at4 years, compared with 95% in group B and 97%in A). The annual rate of aneurysm-related deathin group C was 1% in the first 3 years, but acceler-ated to 8.0% in the fourth year. It is clear fromthis study that large aneurysms after EVAR areassociated with increased rates of aneurysm-related death and rupture.
In one study by Sampram and the ClevelandClinic group103,123, it was observed that secondaryprocedures were more frequent in patients withlarger aneurysms and in patients who had re-ceived larger diameter aortic stents because ofproximal endoleaks at initial EVAR. The overallrisk for secondary intervention was 12% at 1 year,24% at 2 years, and 35% at 3 years. Aneurysm-related death after EVAR was 3.6% over 3 years.These data suggest a link between outcome andpreoperative AAA size, with better results inpatients with smaller aneurysms. Hence, an argu-ment can be made for treating aneurysms atsmaller sizes, which translates into earlier inter-vention. A randomized trial comparing outcome
for surveillance versus early stenting for thetreatment of small aneurysms is ongoing in theUnited States (PIVOTAL trial).
Neck angulation
Neck angulation is another risk factor for com-plications. Neck angulation is defined as the anglebetween the proximal aortic neck and the longi-tudinal axis of the aneurysm. Sternbergh et alstudied the adverse effects of aortic neck angula-tion through prospective data on 148 consecutiveEVAR repairs over 6 years.37 The risk of a patientexperiencing one or more adverse events was70%, 54.5%, and 16.6% in those with severe(greater than or equal to 60°), moderate (40 to59°), and mild (less than 40°) aortic neck angula-tion, respectively. In comparing patients withmoderate/severe neck angulation to mild neckangulation, adverse events included death within30 days (20% versus 0%), acute conversion toopen repair (20% versus 0%), aneurysm expan-sion (9.1% to 20% versus 1.7%), device migration(20% to 30% versus 3.3%), and type I endoleak(23.8% versus 8.3%). Aortic neck length anddiameter, age, and medical co-morbidities werenot significantly different between groups. Thestudy concluded that aortic neck angulation is animportant determinant of outcome after EVAR.
Difficult access arteries
Another patient factor to consider when evalu-ating for EVAR is the character of the accessarteries. Problems at the access sites not onlycompromise endograft insertion, but they alsomake endograft deployment at the target vesseldifficult. Tortuousity and calcification of theiliac and femoral vessels can increase the risk forcomplications. Atherosclerotic disease can alsolead to localized stenoses that pose problems fordeploying the endograft via a delivery sheath.Keeping these potential complications in mind,the surgeon can usually correct tortuous andcalcified vessels by using super-stiff guidewiresto traverse these difficult segments. Discretestenoses can be corrected with angioplasty.
Adjunctive techniques to negotiate tortuousvessels includes the ‘push-and-pull’ technique,which is done by simultaneously pulling on the
150 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 150

super-stiff guidewire while introducing the endo-graft. The tortuous vessel can also be stabilizedby applying external pressure on the access vesselor aneurysm.
COMPLICATIONS OF THORACIC ENDOVASCULAR GRAFTING (EVG)
Endovascular repair of thoracic aortic disease hasbeen applied to elective processes such as degen-erative aneurysms, mycotic aneurysms, pseudo-aneurysms, chronic dissections, and coarctationsof the aorta. Emergency applications include rup-tured thoracic aneurysms, traumatic injuries ofthe aorta, and acute type B aortic dissections.Thoracic endografting is a very appealing thera-peutic option because of its minimally invasivenature compared to open options. It avoids thecomplications of open repair, such as an openthoracotomy, cross-clamping of the aorta, andleft heart bypass. Perioperative mortality of EVGrepair of descending aneurysms ranges from3.5 to 12.5%.21,124–126
Spinal cord ischemia and paraplegia after endo-grafting of the thoracic aorta is relatively low,with rates ranging from 0 to 6%.21,124,127–130 Theconcern is obstruction of the anterior spinal arter-ies, which usually arise between the levels of T9and L1.131 These vessels may be occluded by theendograft. Mitchell et al have reported a higherincidence of paraplegia with simultaneous openabdominal aortic aneurysm repair and endovas-cular thoracic aneurysm repair.132 The etiologyof this increased incidence is due to the abdominalaorta being a major collateral blood source forthe spinal cord, once the artery of Adamkiewiczis occluded.131
To predict and prevent this complication, tem-porary interruption of the intercostal arteries hasbeen performed by placement of a retrievablestent graft in the descending thoracic aorta underevoked spinal cord potential monitoring.133 Ifchanges in amplitude or latency of evoked spinalcord potential are noted during temporary inter-ruption, surgical repair with re-implantation ofintercostal arteries may be necessary.
Endoleak in the thoracic aorta is relativelyuncommon. If present, the common types aretype I endoleaks, which need to be treatedpromptly upon discovery. Type II endoleaks are
rare and are usually secondary to patent inter-costal arteries.133 Stent migration is also a concern,because of the increased forces of systemic bloodflow in the thoracic aorta. It is recommendedthat a zone of attachment greater than or equal to2 cm be used when performing endovascularstent grafting in the thoracic aorta. This mini-mum length is comparatively longer than forEVAR.21,124,135
When performing endografting for thoracicaortic aneurysms, it is permissible to cover theleft subclavian artery with the graft in order toobtain an adequate seal. However, the potentialexists for complications pertaining to retrogradeendoleaks through the subclavian artery, as wellas ischemia of the left upper extremity. In suchcases, some have advocated transposition of theleft subclavian artery to the common carotidartery.124,127,130,132 If the right vertebral artery ispatent, some groups will deploy the thoracicstent over the left subclavian artery and performextra-anatomic reconstruction as needed.
METHODS TO DETECT/AVOID COMPLICATIONS
In order to avoid complications, the underlyingtheme throughout endovascular repair of the aortais careful patient selection. Successful EVARmandates precise measurements of aorto-iliacdimensions so that an appropriate endograft canbe chosen. Relative anatomic criteria for endovas-cular repair are an infrarenal proximal aorticneck at least 15 mm in length, neck diameter lessthan 26 mm, less than 60° angulation of theproximal neck, and no significant calcificationsproximal and distal to the aneurysm136 (Table 9.3).Various schemes are used for sizing endografts(Figure 9.9).
EMERGENCY ENDOVASCULAR AORTICANEURYSM REPAIR
See Table 9.4.
SUMMARY
The natural history of thoracic and abdominal aorticaneurysms is enlargement and eventual rupture.
AORTIC ANEURYSMAL DISEASE 151
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 151

While traditional therapy has consisted of opensurgical repair, newer technologies and rapidadvances are allowing patients the option of under-going endovascular stent grafting. This method
of therapy commits patients to lifetime imagingsurveillance because of complications inherentto stent grafting. The most commonly recognizedcomplications include endoleaks, stent migra-tion, and stent fracture, all of which can lead to continued aneurysm sac pressurization andpotential rupture. Other injuries include hip andbuttock claudication and access artery injury.Risk factors known to increase the risks of com-plications include female gender, large aneurysmsize, tortuous aortic necks, and difficult accessarteries.
While thoracic endografting has distinctadvantages in avoiding complications, such asthoracotomy and left heart bypass, there remainconcerns of spinal cord ischemia resulting inparaplegia, as well as compromised circulationto upper extremities from stenting over the leftsubclavian artery. As with abdominal aorticaneurysm repairs, endovascular stent graftingof the thoracic aorta has similar issues withendoleaks and device migration.
152 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Table 9.3 Relative anatomic abdominalaortic aneurysm criteria136
IInnffrraarreennaall aaoorrttaa aannaattoommyy• �15 mm of proximal neck (non-aneurysmal
aorta distal to lowest renal)• Proximal neck diameter less than 28 mm• Less than 60° angulation of proximal neck• No significant neck thrombus (<50%)• No excessive calcifications of proximal neck• Absence of indispensable inferior mesenteric
artery (IMA)
IIlliiaacc aarrtteerryy aannaattoommyy• Patent• Without severe angulations• Large caliber (to accommodate graft, 6–7 mm)
D1 Suprarenal aortic diameter
D2 Infrarenal aortic neck diameter
(a, proximal; b, mid; c, distal)
D3 Maximal aneurysm diameter
D4 Terminal aortic transverse diameter
D5 Common iliac artery (CIA) diameters
(a, right; b, left)
Length from lower renal artery to
H1 aneurysm neck
H2 distal aneurysm
H3 aortic bifurcation
H4 CIA bifurcation (a, right; b, left)
D1
D2
D3
D3a
D4
D5 a b
H1
H2
H3
H4a
H5b
a
b
c
Figure 9.9 Method for measuring aortic dimensions. Figure adapted from Mohan et al.82
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 152

REFERENCES
1. Gillum RF. Epidemiology of aortic aneurysm in theUnited States. J Clin Epidemiol 1995; 48: 1289–98.
2. Clouse WD, Hallett JW Jr, Schaff HV et al. Improvedprognosis of thoracic aortic aneurysms: a population-based study. JAMA 1998; 280: 1926–9.
3. Hagan PG, Nienaber CA, Isselbacher EM et al. Theinternational registry of acute aortic dissection(IRAD): new insights into an old disease. JAMA 2000;283: 897–903.
4. Kouchoukos NT, Dougenis D. Surgery of the thoracicaorta. N Engl J Med 1997; 336: 1876–88.
5. Pate JW, Richardson RL, Eastridge CE. Acute aorticdissections. Am Surg 1976; 42: 395–404.
6. Spitell PC, Spitell J, Joyce JW. Clinical features and dif-ferential diagnosis of aortic dissection: experience with236 cases. Mayo Clin Proc 1993; 68: 897–903.
7. Meszaros I, Morocz J, Szlavi J et al. Epidemiology andclinicopathology of aortic dissection. Chest 2000; 117:1271–8.
8. Ailawadi G, Eliason JL, Upchurch GR. Current conceptsin the pathogenesis of abdominal aortic aneurysms. J Vasc Surg 2003; 38: 584–8.
9. Hollier LH, Taylor LM, Ochsner J. Recommendedindications for operative treatment of abdominal aor-tic aneurysms. Report of a subcommittee of the JointCouncil of the Society for Vascular Surgery and theNorth American Chapter of the International Societyfor Cardiovascular Surgery. J Vasc Surg 1992; 15:1046–56.
10. Cambria RP, Clouse WD, Davison JK et al. Thoracoab-dominal aneurysm repair: results with 337 operationsperformed over a 15-year interval. Ann Surg 2002; 236:471–9.
11. Elefteriades JA, Hartleroad J, Gusberg RJ et al. Long-term experience with descending aortic dissection: the complication-specific approach. Ann Thorac Surg1992; 53: 11–20.
12. Kouchoukos NT, Daily BB, Rokkas CK et al. Hypother-mic bypass and circulatory arrest for operations on thedescending thoracic and thoracoabdominal aorta. AnnThorac Surg 1995; 60: 67–76.
13. Svensson LG, Crawford ES, Hess KR et al. Experiencewith 1509 patients undergoing thoracoabdominal aor-tic operations. J Vasc Surg 1993; 17: 357–68.
14. Parodi JC, Palmaz JC, Barone HD. Transfemoralintraluminal graft implantation for abdominal aorticaneurysms. Ann Vasc Surg 1991; 5: 491–9.
15. Parodi JC, Marin ML, Veith FJ. Transfemoral, endo-vascular stented graft repair of an abdominal aorticaneurysm. Arch Surg 1995; 130: 549–52.
16. Armon MP, Yusuf SW, Latief K et al. Anatomical suit-ability of abdominal aortic aneurysms for endovascularrepair. Br J Surg 1997; 84: 178–80.
17. Carpenter JP, Baum RA, Barker CF et al. Impact ofexclusion criteria on patient selection for endovascularabdominal aortic aneurysm repair. J Vasc Surg 2001;34: 1050–4.
18. Zarins CK, Wolf YG, Hill BB et al. Will endovascularrepair replace open surgery for abdominal aortic aneu-rysm repair? Ann Surg 2000; 232: 501–7.
AORTIC ANEURYSMAL DISEASE 153
Table 9.4 Equipment necessary for emergency endovascular aortic aneurysm repair
CC--aarrmm ddiiggiittaall fflluuoorroossccooppee wwiitthh ssuubbttrraaccttiioonn GGuuiiddeewwiirreessccaappaabbiilliittiieess aanndd ccoonnttrraasstt iinnjjeeccttoorr 0.035-inch Glidewire (180, 260 cm*)(portable or fixed system) Bentson
Lunderquist extra stiffAmplatz super stiff
CCaatthheetteerrss BBaalllloooonnssKumpe Cook Coda balloon up to 40 mmRIM BSC equalizer 40 mm*Cobra Cordis Maxi 15, 20, 25 mmMarker pigtail PTA balloon 12 mm diameterSos Omni Flush125 cm multi-purpose
SShheeaatthh SStteennttssCook 5, 7, 9, 12, 14*, 18, 20, 23 Fr Balloon-expandable (Palmaz)(10–15 cm long) Self-expanding (SMART)
AAA Stent grafts (Cook, Gore, Medtronic)
*Denotes for brachial approach.
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 153

19. Bown MJ, Fishwick G, Sayers RD. The post-operativecomplications of endovascular aortic aneurysm repair.J Cardiovasc Surg 2004; 45: 335–47.
20. Towne JB. Endovascular treatment of abdominal aorticaneurysms. Am J Surg 2005; 189: 140–9.
21. Orend KH, Scharrer-Pamler R, Kapfer X et al. Endovas-cular treatment in diseases of the descending thoracicaorta: 6-year results of a single center. J Vasc Surg2003; 37: 91–9.
22. Rutherford RB. Vascular Surgery. Philadelphia: ElsevierSaunders, 2005: 1468–9.
23. Pan JH, Lindholt JS, Suhova GK et al. Macrophagemigration inhibitory factor is associated with aneurys-mal expansion. J Vasc Surg 2003; 37: 628–35.
24. Sternbergh WC, Money SR. Hospital cost of endovas-cular versus open repair of abdominal aortic aneurysms:a multicenter study. J Vasc Surg 2000; 31: 237–44.
25. Van Marrewijk CJ, Fransen G, Laheij RJF et al.EUROSTAR collaborators: is type II endoleak afterEVAR a harbinger of risk? Causes and outcome of openconversion and aneurysm rupture during follow-up.Eur J Vasc Endovasc Surg 2004; 27: 128–37.
26. Verzini F, Cao P, De Rango P et al. Conversion to openrepair after endografting for abdominal aortic aneurysm:causes, incidence and results. Eur J Vasc EndovascSurg 2006; 31: 136–42.
27. EVAR trial participants. Endovascular aneurysm repairversus open repair in patients with abdominal aorticaneurysm (EVAR trial 1): randomised controlled trial.Lancet 2005; 365: 2179–86.
28. Laheij RJ, Buth J, Harris PL et al. Need for secondaryinterventions after endovascular repair of abdominalaortic aneurysm: intermediate-term follow-up resultsof a European collaborative registry (EUROSTAR). BrJ Surg 2000; 87: 1666–73.
29. Ohki T, Veith FJ, Shaw P et al. Increasing incidence ofmidterm and long-term complications after endovas-cular graft repair of abdominal aortic aneurysms: a noteof caution based on a 9-year experience. Ann Surg2001; 234: 323–35.
30. Schurink GW, Aarts NJ, Bockel JH. Endoleak after stentgraft treatment of abdominal aortic aneurysm: a meta-analysis of clinical studies. Br J Surg 1999; 86: 581–7.
31. Blankensteijn JD, de Jong SE, Prinssen M et al. DutchRandomized Endovascular Aneurysm Management(DREAM) Trial Group. Two-year outcomes after con-ventional or endovascular repair of abdominal aorticaneurysms. N Engl J Med 2005; 352: 2398–405.
32. Cao P, Verzini F, Parlani G et al. Clinical effect of abdom-inal aortic aneurysm endografting: 7-year concurrentcomparison with open repair. J Vasc Surg 2004; 40: 841–8.
33. Goueffic Y, Becquemin JP, Desgranges P et al. Midtermsurvival after endovascular versus open repair of infrarenalaortic aneurysms. J Endovasc Ther 2005; 12: 47–57.
34. White GH, Yu W, May J et al. Endoleaks as a compli-cation of endoluminal grafting of abdominal aorticaneurysms: classification, incidence, diagnosis, andmanagement. J Endovasc Surg 1997; 4: 152–68.
35. Broeders IAMJ, Blankensteijn JD, Gvakharia A et al.The efficacy of transfemoral endovascular aneurysmmanagement: a study of size changes of the abdominalaorta during mid-term follow-up. Eur J Vasc EndovascSurg 1997; 14: 84–90.
36. Matsumura JS, Moore WS. Clinical consequences ofperiprosthetic leak after endovascular repair of abdom-inal aortic aneurysm. J Vasc Surg 1998; 27: 606–13.
37. Sternbergh WC, Carter G, York JW et al. Aortic neckangulation predicts adverse outcome with endovascu-lar abdominal aortic aneurysm repair. J Vasc Surg2002; 35: 482–6.
38. Van Marrewijk C, Buth J, Harris PL et al. Significanceof endoleaks after endovascular repair of abdominalaortic aneurysms: the EUROSTAR experience. J VascSurg 2002; 35: 461–73.
39. Buth J, Laheij RJ. Early complications and endoleaks afterendovascular abdominal aortic aneurysm repair: reportof a multicenter study. J Vasc Surg 2000; 31: 134–46.
40. Moore WS, Rutherford RB. Transfemoral endovascularrepair of abdominal aortic aneurysms. Results of theNorth-American EVT phase I trial. J Vasc Surg 1996;23: 543–53.
41. Zarins CK, White RA, Schwarten D et al. AneuRx stent-graft versus open surgical repair of abdominal aorticaneurysms: multicenter prospective clinical trial. J VascSurg 1999; 29: 292–308.
42. Golzarian J, Dussaussois L, Abada HT et al. Helical CTof aorta after endoluminal stent-graft therapy: valueof biphasic acquisition. Am J Roentgenol 1998; 171:329–31.
43. McLafferty RV, McCrary BS, Mattos MA et al. The useof color-flow duplex scan for the detection of endoleaks.J Vasc Surg 2002; 35: 100–4.
44. Veith FJ, Baum RA, Ohki T et al. Nature and significanceof endoleaks and endotension: summary of opinionsexpressed at an international conference. J Vasc Surg2002; 35: 1029–35.
45. Chuter TA, Reilly LM, Kerlan RK et al. Endovascularrepair of abdominal aortic aneurysm: getting out oftrouble. Cardiovasc Surg 1998; 6: 232–9.
46. Chuter TA. Stent-graft design: the good, the bad andthe ugly. Cardiovasc Surg 2002; 10: 7–13.
47. Lederle FA, Wilson SE, Johnson GR et al. Variability inmeasurement of abdominal aortic aneurysms. J VascSurg 1995; 21: 945–52.
48. Gould DA, McWilliams R, Edwards RD et al. Aorticside branch embolization before endovascular aneurysmrepair: incidence of type II endoleaks. J Vasc IntervRadiol 2001; 12: 337–41.
154 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 154

49. Parry DJ, Kessel DO, Robertson I et al. Type IIendoleaks: predictable, preventable, and sometimestreatable? J Vasc Surg 2002; 36: 105–10.
50. Resch T, Ivancev K, Lindh M et al. Persistent collateralperfusion of abdominal aortic aneurysm after endovas-cular repair does not lead to progressive change inaneurysm diameter. J Vasc Surg 1998; 28: 242–9.
51. Harris PL, Vallabhaneni SR, Desgranges P et al.Incidence and risk factors of late rupture, conversion,and death after endovascular repair of infrarenal aorticaneurysms: the EUROSTAR experience. J Vasc Surg2000; 32: 739–48.
52. Hinchliffe RJ, Sing-Ranger R, Davidson JR et al. Ruptureof an abdominal aortic aneurysm secondary to type IIendoleak. Eur J Vasc Endovasc Surg 2001; 22: 563–5.
53. Politz JK, Newman VS, Stewart ME. Late abdominalaortic aneurysm rupture after AneuRx repair: a reportof three cases. J Vasc Surg 2000; 31: 599–606.
54. White R, Donayre C, Walot I et al. Abdominal aorticaneurysm rupture following endoluminal graft devel-opment: report of a predictable event. J Endovasc Ther2000; 7: 257–62.
55. Chuter TA, Faruqi RM, Sawhney R et al. Endoleakafter endovascular repair of abdominal aortic aneurysm.J Vasc Surg 2001; 34: 98–105.
56. Faries PL, Cadot H, Agarwal G et al. Management ofendoleak after endovascular aneurysm repair: cuffs,coils, and conversion. J Vasc Surg 2003; 37: 1155–61.
57. Vallabhaneni SR, Gilling-Smith GL, How TV et al.Aortic side branch perfusion alone does not accountfor high intra-sac pressure after endovascular repair(EVAR) in the absence of graft-related endoleak. Eur JVasc Endovasc Surg 2003; 25: 354–9.
58. Baum RA, Carpenter JP, Golden MA et al. Treatmentof type 2 endoleaks after endovascular repair of abdom-inal aortic aneurysms: comparison of transarterial andtranslumbar techniques. J Vasc Surg 2002; 35: 23–9.
59. Ellis PK, Kennedy PT, Collins AJ et al. The use ofdirect thrombin injection to treat a type II endoleakfollowing endovascular repair of abdominal aorticaneurysm. Cardiovasc Interv Radiol 2003; 26: 482–4.
60. Haulon S, Tyazi A, Willoteaux S et al. Embolization oftype II endoleaks after aortic stent-graft implantation:technique and immediate results. J Vasc Surg 2001; 34:600–5.
61. Kasirajan K, Matteson B, Marek JM et al. Techniqueand results of transfemoral superselective coil emboli-zation of type II lumbar endoleak. J Vasc Surg 2003;38: 61–6.
62. Krueger K, Zaehringer M, Gawenda M et al. Successfultreatment of a type-II endoleak with percutaneous CT-guided thrombin injection in a patient after endovas-cular abdominal aortic aneurysm repair. Eur Radiol2003; 13: 1748–9.
63. Chaikof EL, Blankensteijn JD, Harris PL et al.Reporting standards for endovascular aortic aneurysmrepair. J Vasc Surg 2002; 35: 1048–60.
64. Hinchliffe RJ, Hopkinson BR. Current concepts andcontroversies in endovascular repair of abdominalaortic aneurysms. J Cardiovasc Surg 2003; 44: 481–502.
65. Gilling-Smith G, Brennan J, Harris P et al. Endotensionafter endovascular aneurysm repair: definition, classi-fication, and strategies for surveillance and interven-tion. J Endovasc Surg 1999; 6: 305–7.
66. Gilling Smith GL, Martin J, Sudhindran S et al.Freedom from endoleak after endovascular aneurysmrepair does not equal treatment success. Eur J VascEndovasc Surg 2000; 19: 421–5.
67. Ohki T, Ouriel K, Silveira PG, Katzen B, White R,Criado F, Diethrich E. Initial results of wireless pres-sure sensing for endovascular aneurysm repair: TheAPEX Trial. J Vasc Surg 2007; 45: 236–42.
68. Buth J, Harris PL, Van Marrewijk C et al. The signifi-cance and management of different types of endoleaks.Semin Vasc Surg 2003; 16: 95–102.
69. Dubenec SR, White GH, Pasenau J et al. Endotension:a review of current views on pathophysiology andtreatment. J Cardiovasc Surg (Torino) 2003; 44: 553–7.
70. Resch T, Malina M, Lindblad B et al. The impact ofstent design on proximal stent-graft fixation in theabdominal aorta: an experimental study. Eur J VascEndovasc Surg 2000; 20: 190–5.
71. Ouriel K, Clair DG, Greenberg RK et al. Endovascularrepair of abdominal aortic aneurysms: device-specificoutcome. J Vasc Surg 2003; 37: 991–8.
72. Conners MS, Sternbergh WC, Carter G et al. Endograftmigration one to four years after endovascularabdominal aortic aneurysm repair with the AneuRxdevice: a cautionary note. J Vasc Surg 2002; 36: 476–84.
73. Zarins CK, Bloch DA, Crabtree T et al. Stent graftmigration after endovascular aneurysm repair: impor-tance of proximal fixation. J Vasc Surg 2003; 38: 1264–72.
74. Badran MF, Gould DA, Raza I et al. Aneurysm neckdiameter after endovascular repair of abdominal aorticaneurysms. Vasc Interv Radiol 2002; 13: 887–92.
75. Cao P, Verzini F, Parlani G et al. Predictive factors andclinical consequences of proximal aortic neck dilatationin 230 patients undergoing abdominal aorta aneurysmrepair with self-expandable stent-grafts. J Vasc Surg2003; 37: 1200–5.
76. Makaroun MS, Deaton DH. Is proximal aortic neckdilatation after endovascular aneurysm exclusion acause for concern? J Vasc Surg 2001; 33: S39–45.
77. Napoli V, Sardella SG, Bargellini I et al. Evaluation ofthe proximal aortic neck enlargement following endovas-cular repair of abdominal aortic aneurysm: 3-years expe-rience. Eur Radiol 2003; 13: 1962–71.
AORTIC ANEURYSMAL DISEASE 155
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 155

78. Resch T, Ivancev K, Brunkwall J et al. Distal migrationof stent-grafts after endovascular repair of abdominalaortic aneurysms. J Vasc Interv Radiol 1999; 10: 257–64.
79. Sternbergh C, Money S, Greenberg R et al. Influence ofendograft oversizing on device migration, endoleak,aneurysm shrinkage, and aortic neck dilation: resultsfrom the Zenith multicenter trial. J Vasc Surg 2004; 39:20–6.
80. Wever J, de Nie A, Blankensteijn D et al. Dilatation ofthe proximal neck of infrarenal aortic aneurysms afterendovascular AAA repair. Eur J Vasc Endovasc Surg2000; 19: 197–201.
81. Mohan IV, Harris PL, Van Marrewijk CJ et al. Factorsand forces influencing stent-graft migration after endo-vascular aortic aneurysm repair. J Endovasc Ther2002; 9: 748–55.
82. Malas MB, Ohki T, Veith FJ et al. Absence of proximalneck dilatation and graft migration after endovascularaneurysm repair with balloon-expandable stent-basedendografts. J Vasc Surg 2005; 42: 639–44.
83. Malina M, Lindblad B, Ivancev K et al. EndovascularAAA exclusion: will stents with hooks and barbs preventstent-graft migration? J Endovasc Surg 1998; 5: 310–17.
84. Greenberg RK, Lawrence-Brown M, Bhandari G et al.An update of the Zenith endovascular graft for abdom-inal aortic aneurysms: initial implantation and mid-term follow-up data. J Vasc Surg 2001; 33: S157–64.
85. Trout HH, Tanner HM. A new vascular endostaple: atechnical description. J Vasc Surg 2001; 34: 565–8.
86. Ohki T, Deaton DH, Condado JA. Aptus EndovascularAAA Repair System: Report of the 1-year follow-up ina first-in-man study. Endovascular Today; November2006: 29–36.
87. Criado FJ, Barnatan MF, Lingelbach JM et al. Abdominalaortic aneurysm: overview of stent-graft devices. J AmColl Surg 2002; 194: S88–97.
88. Harris PL, Brennan J, Martin J et al. Longitudinalaneurysm shrinkage following endovascular aorticaneurysm repair: a source of intermediate and latecomplications. J Endovasc Surg 1999; 6: 11–16.
89. Riepe G, Heilberger P, Umscheid T et al. Frame dislo-cation of body middle rings in endovascular stent tubegrafts. Eur J Vasc Endovasc Surg 1999; 17: 28–34.
90. Beebe HG, Cronenwett JL, Katzen BT et al; VanguardEndograft Trial Investigators. Results of an aorticendograft trial: impact of device failure beyond 12months. J Vasc Surg 2001; 33: S55–63.
91. Darling RC, Ozsvath K, Chang BB et al. The incidence,natural history and outcome of secondary interventionfor persistent collateral flow in the excluded abdominalaortic aneurysm. J Vasc Surg 1999; 30: 968–76.
92. Torsello GB, Klenk E, Kaspizak B et al. Rupture of abdominal aortic aneurysm previously treated byendovascular stent-graft. J Vasc Surg 1998; 28: 184–7.
93. Zarins CK, White RA, Fogarty TJ. Aneurysm ruptureafter endovascular repair using the AneuRx stent-graft.J Vasc Surg 2000; 31: 960–70.
94. Bernhard VM, Mitchell RS, Matsumura JS et al.Ruptured abdominal aortic aneurysm after endovas-cular repair. J Vasc Surg 2002; 35: 1155–62.
95. Datillo JB, Brewster DC, Fan C-M et al. Clinical failuresof endovascular abdominal aortic aneurysm repair.Incidence, causes, and management. J Vasc Surg 2002;35: 1137–44.
96. Makaroun MS, Chaikof E, Naslund T et al. Efficacy of abifurcated endograft versus open repair of abdominalaortic aneurysms: a reappraisal. J Vasc Surg 2002; 35:203–10.
97. Zarins CK, White RA, Moll FL et al. The AneuRx stentgraft: four-year results and worldwide experience 2000.J Vasc Surg 2001; 33: S135–45.
98 Harris P. Rupture after endovascular aneurysmrepair: implications for clinical practice. Presented atthe Congress of the International Society for Endovas-cular Specialists, 14 February 2001, Scottsdale, AZ.
99. Carpenter JP, Anderson WN, Brewster DC et al.Multicenter pivotal trial results of the Lifepath systemfor endovascular aortic aneurysm repair. J Vasc Surg2004; 39: 34–42.
100. Conners MS, Sternbergh WC, Carger G et al. Secondaryprocedures after endovascular aortic aneurysm repair.J Vasc Surg 2002; 36: 992–6.
101. Krajcer Z, Gilbert JH, Dougherty K et al. Success-ful treatment of aortic endograft thrombosis with rheolytic thrombectomy. J Endovasc Ther 2002; 9: 756–64.
102. Sampram ES, Karafa MT, Mascha EJ et al. Nature, fre-quency, and predictors of secondary procedures afterendovascular repair of abdominal aortic aneurysm.J Vasc Surg 2003; 37: 930–7.
103. Fairman RM, Baum RA, Carpenter JP et al; Phase IIEVT Investigators. Limb interventions in patientsundergoing treatment with an unsupported bifur-cated aortic endograft system: a review of the Phase IIEVT Trial. J Vasc Surg 2002; 36: 118–26.
104. Criado FJ, Wilson EP, Velazquez OC et al. Safety of coilembolization of the internal iliac artery in endovasculargrafting of abdominal aortic aneurysms. J Vasc Surg2000; 32: 684–8.
105. Cynamon J, Lerer D, Veith FJ et al. Hypogastric arterycoil embolization prior to endoluminal repair ofaneurysms and fistulas: buttock claudication, a recog-nized but possibly preventable complication. J VascInterv Radiol 2000; 11: 573–7.
106. Lee CW, Kaufman JA, Fan CM et al. Clinical outcomeof internal iliac artery occlusions during endovasculartreatment of aortoiliac aneurysmal diseases. J VascInterv Radiol 2000; 11: 567–71.
156 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 156

107. Lee WA, O’Dorisio J, Wolf YG et al. Outcome afterunilateral hypogastric artery occlusion during endovas-cular aneurysm repair. J Vasc Surg 2001; 33: 921–6.
108. Razavi MK, DeGroot M, Olcott C 3rd et al. Internaliliac artery embolization in the stent-graft treatment ofaortoiliac aneurysms: analysis of outcomes and compli-cations. J Vasc Interv Radiol 2000; 11: 561–6.
109. Sanchez LA, Patel AV, Ohki T et al. Midterm experi-ence with the endovascular treatment of isolated iliacaneurysms. J Vasc Surg 1999; 30: 907–13.
110. Parodi JC, Ferreira M. Relocation of the iliac arterybifurcation to facilitate endoluminal treatment of abdom-inal aortic aneurysms. J Endovasc Surg 1999; 6: 342–7.
111. Kalliafas S, Albertini JN, Macierewicz J et al. Stent-graft migration after endovascular repair of abdominalaortic aneurysm. J Endovasc Ther 2002; 9: 743–7.
112. Bove PG, Long GW, Shanley CJ et al. Transrenal fixa-tion of endovascular stent-grafts for infrarenal aorticaneurysm repair: mid-term results. J Vasc Surg 2003;37: 938–42.
113. Lau LL, Hakaim AG, Oldenburg WA et al. Effect ofsuprarenal versus infrarenal aortic endograft fixationon renal function and renal artery patency: a compara-tive study with intermediate follow-up. J Vasc Surg2003; 37: 1162–8.
114. Lobato AC, Quick RC, Vaughn PL et al. Transrenal fixa-tion of aortic endografts: intermediate follow-up of asingle-center experience. J Endovasc Ther 2000; 7: 273–8.
115. Burks JA Jr, Faries PL, Gravereaux EC et al. Endovas-cular repair of abdominal aortic aneurysms: stent-graftfixation across the visceral arteries. J Vasc Surg 2002;35: 109–13.
116. Slappy AL, Hakaim AG, Oldenburg WA et al. Femoralincision morbidity following endovascular aorticaneurysm repair. Vasc Endovasc Surg 2003; 37: 105–9.
117. May J, White GH, Waugh R et al. Adverse events afterendoluminal repair of abdominal aortic aneurysms: acomparison during two successive periods of time. J Vasc Surg 1999; 29: 32–9.
118. Moore WS, Kashyap VS, Vescera CL et al. Abdominalaortic aneurysm: a 6-year comparison of endovascularversus transabdominal repair. Ann Surg 1999; 230:298–306.
119. Albertini J, Kalliafas S, Travis S et al. Anatomical riskfactors for proximal perigraft endoleak and graft migra-tion following endovascular repair of abdominal aorticaneurysms. Eur J Vasc Endovasc Surg 2000; 19: 308–12.
120. Chaikof EL, Lin PH, Brinkman WT et al. Endovascularrepair of abdominal aortic aneurysms: risk stratifiedoutcomes. Ann Surg 2002; 235: 833–41.
121. Peppelenbosch N, Buth J, Harris PL et al. Diameter ofabdominal aortic aneurysm and outcome of endovas-cular aneurysm repair: does size matter? A report fromEUROSTAR. J Vasc Surg 2004; 39: 288–97.
122. Cambria RP, Brewster DC, Lauterbach SR et al.Evolving experience with thoracic aortic stent graftrepair. J Vasc Surg 2002; 35: 1129–36.
123. Sampram ES, Karafa MT, Mascha EJ, Clair DG,Greenberg RK, Lyden SP, O’Hara PJ, Sarac TP,Srivastava SD, Butler B, Ouriel K. Nature, frequency,and predictors of secondary procedures after endovas-cular repair of abdominal aortic aneurysm. J VascSurg 2003; 37: 930–7.
124. Dake MD, Miller DC, Semba CP et al. Transluminalplacement of endovascular stent-grafts for the treatmentof descending thoracic aortic aneurysms. N Engl JMed 1994; 331: 1729–34.
125. Greenberg R, Resch T, Nyman U et al. Endovascularrepair of descending thoracic aortic aneurysms: anearly experience with intermediate-term follow-up. J Vasc Surg 2000; 31: 147–56.
126. Grabenwoger M, Hutschala D, Ehrlich MP et al.Thoracic aortic aneurysms: treatment with endovas-cular self-expandable stent grafts. Ann Thorac Surg2000; 69: 441–5.
127. Gravereaux EC, Faries PL, Burks JA et al. Risk of spinal cord ischemia after endograft repair of thoracic aortic aneurysms. J Vasc Surg 2001; 34:997–1003.
128. Mitchell RS, Miller DC, Dake MD et al. Thoracic aorticaneurysm repair with an endovascular stent-graft: the‘first generation.’ Ann Thorac Surg 1999; 67: 1971–4.
129. White R, Donayre CE, Walot I et al. Endovascularexclusion of descending thoracic aortic aneurysm andchronic dissections: initial clinical results with theAneuRx device. J Vasc Surg 2001; 33: 927–34.
130. Ishimaru S, Kawaguchi S, Koizumi N et al. Preliminaryreport on prediction of spinal cord ischemia in endovas-cular stent graft repair of thoracic aortic aneurysm byretrievable stent graft. J Thorac Cardiovasc Surg 1998;115: 811–18.
131. Greenberg R, Resch T, Nyman U et al. Endovascularrepair of descending thoracic aortic aneurysms: anearly experience with intermediate-term follow-up. JVasc Surg 2000; 31: 147–56.
132. Thompson CS, Gaxotte VD, Rodriguez JA et al.Endoluminal stent grafting of the thoracic aorta: initialexperience with the Gore Excluder. J Vasc Surg 2002;35: 1163–70.
133. Dillavou ED, Muluk SC, Rhee RY et al. Does hostileneck anatomy preclude successful endovascular aorticaneurysm repair? J Vasc Surg 2003; 38: 657–63.
134. White GH. What are the causes of endotension? J Endovasc Ther 2001; 8: 454–6.
135. Gilling-Smith GL, Martin J, Sudhindran S et al. Freedomfrom endoleak after endovascular aneurysm repairdoes not equal treatment success. Eur J Vasc EndovascSurg. 2000; 19: 421–5.
AORTIC ANEURYSMAL DISEASE 157
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 157

136. White GH, May J, Petrasek P et al. Endotension: anexplanation for continued AAA growth after successfulendoluminal repair. J Endovasc Surg 1999; 6: 308–15.
137. Matsumura JS, Ryu RK, Ouriel K. Identification andimplications of transgraft microleaks after endovascu-lar repair of aortic aneurysm. J Vasc Surg 2001; 34:190–7.
138. Williams GM. The management of massive ultrafiltra-tion distending the aneurysm sac after abdominal aorticrepair with a polytetrafluoroethylene aortobiiliac graft.J Vasc Surg 1998; 28: 551–5.
139. Risberg B, Delle M, Eriksson E et al. Aneurysm sachygroma: a cause of endotension. J Endovasc Ther 2001;8: 447–53.
158 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter09.qxp 4/5/2007 2:46 PM Page 158

INTRODUCTION TO THE FREQUENCY ANDTYPE OF COMPLICATIONS
This chapter covers complications related toendovascular treatment of celiac, superior mesen-teric, renal, and occasionally inferior mesentericarteries. Systematic data on complications mainlyare available for renal artery stenting, only veryfew reports cover complications of mesentericartery interventions. The principle mechanisms ofcomplications for renal and mesenteric arteriesare very similar, thus this chapter mainly coversthe literature on renal arteries.
The occurrence of any complication describedin the literature on renal interventions is reported tobe between 3 and 36%.1–15 Particularly in historicalseries using the over-the-wire (OTW) approach7–9
without guiding catheters or long sheaths, com-plication rates above 10% were frequentlyobserved: the rate of minor complications was atmaximum 26%,7,10 the rate of major complicationswas reported to be between 1 and 14%,4–7,11–14 anda 30-day mortality rate of 1% due to renal arteryperforation, cholesterol embolization, acute renalfailure, and fatal bleeding at the access site wasobserved.15 These figures completely changed
with the introduction of coronary technologies.Complication rates below 3%16,17 seem realisticwhen low profile rapid exchange systems andrenal guiding catheters or sheaths are used.
Frequencies of complications during treatmentof celiac or mesenteric arteries are available onlyfrom small case series. The extent of ischemia ofthe related target organs mainly determines theimpact of complications in these vessel areas.Distal embolization from the celiac trunk and thesuperior mesenteric artery or acute occlusions ofthese vessels may result in ischemia of the stom-ach, small and large intestinal infarction, hepaticischemia, ischemic pancreatitis, or ischemic coli-tis. While this may occur infrequently for chronicdisease, in acute settings there is a greater chanceof bowel infarction and exploratory laparotomymay be indicated as a concurrent procedure. Formesenteric procedures, bowel infarctions werereported in up to 11% of the cases, with a peripro-cedure mortality rate of up to 4% and a frequencyof renal failure of also 4%.18,19 Acute thrombosiswas seen in 3% and additionally compromisedarterial perfusion due to severe spasm has beenreported in numerous cases.
10
Complications in renal and mesentericvascular interventionsMartin Schillinger and Thomas Zeller
Introduction to the frequency and type of complications • Factors identifying high-risk patients forcomplications • Complications of specific interventional steps and complications of specific interventional tools • Methods to detect potential complications – which diagnostic steps are neededroutinely to rule out or identify complications • Endovascular, surgical and/or medical techniques toresolve complications • Methods to avoid complications • Summary • Check list for emergencyequipment for interventions
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 159

Specific complications of renal and mesentericartery stenting include local complications at thetarget vessel segment like stent misplacement,arterial dissection or rupture, renal artery thrombo-sis, and perforation of the renal parenchyma, andrenal infarction as a potential consequence of allthese complications, as well as systemic compli-cations like cholesterol emboli, which refers to aworst case scenario after the intervention. Somepatients suffer multiple and repetitive emboli,intra- as well as extrarenal, until days after theprocedure. Finally, interventions can be compli-cated by renal failure, which can be due to localcomplications, embolization, or contrast agentinduced, and secondary nephrectomy – a ratherrare complication (below 1%) even in timeswhen low profile systems were not available.15
Stent misplacement
There are no data indicating the frequencies ofstent misplacement. From personal experiencethe frequency certainly is below 5%. Ideally anostial renal stent extends 1 to 2 mm into theaorta to firmly cover the ostium and to reducethe risk of recoil and restenosis at the renal ori-fice, but still enable repeat interventions in caseof restenosis. Precise placement of the stent iscrucial. Three factors may influence the preci-sion of stent placement. First, precise stentingcan be best achieved during apnea of the patientduring stent inflation. Second, in patients withtight and focal ostial lesions, predilation reducesthe risk of stent misplacement. Third, adequateprojection of the renal artery and the stenosis iscrucial.
Figure 10.1 demonstrates a case of stent mis-placement in a patient with inadequate angio-graphic projection during renal artery stenting.The initial result looks perfect in the posterior-anterior view, in fact the stent was misplacedand the ostium was not covered. The patientcame back with a high-grade restenosis and hadto undergo repeat angioplasty. The 25� LAOview indicates that the stent was initially mis-placed and did not cover the ostium (Figure 10.1).In contrast, Figure 10.2 shows an example of stentmisplacement with the stent protruding 5 mminto the lumen of the abdominal aorta. Althoughthe initial result is acceptable, repeat interventions
in this patient will be difficult: a wire may easilypass through the struts of the stent rather thanthrough the lumen, furthermore, the aortic edgeof the stent may be damaged or dislocated20 dur-ing later interventions in the renal or any otherproximal territory.
Dissection
Dissection of the renal artery may occur duringvirtually all phases of the intervention, particu-larly during wiring and dilation of the artery.Reported frequencies range from around 0 to8%.15 Diagnostic or guiding catheters may causedissection, particularly when advanced throughthe stenosis (Figure 10.3); wiring the artery caninitiate a dissection, stenting and postdilation maycause miniruptures and subsequent vessel dis-section. Leaving a dissection untreated is associ-ated with a high risk of early vessel thrombosis.Figure 10.3 shows a case with a large dissection,which could be resolved by bare stent implan-tation. Besides dissection of the renal artery,dissection of the aorta may occur both due tomanipulation with the guide or following stentimplantation with an incidence of 0 to 2.2%.15
These dissections can be left untreated as long asthe origin of the dissection is covered by the renalstent and as long as there is no retroperitonealbleeding or progressive enlargement of the dis-section. Follow-up by serial computed tomogra-phy investigations is mandatory to ascertainhealing of the leakage.
Rupture
Fortunately, this worst potential complication ofrenal and mesenteric artery stenting very rarelyoccurs (below 1%).15 Clinical signs of rupture areback, flank, or inguinal pain, tachycardia, andhypotension. Unexplained pain after ballooninflation or stenting always has to be followedby a thorough interrogation for rupture andbleeding. Ideally, the rupture should be recog-nized before the wire is removed, otherwise re-entry can be very difficult. The most devastatingcomplication which can hardly be resolved byendovascular techniques is a complete ruptureof the renal artery from the origin from the aorta.The risk for this complication seems to be higherin patients with circular heavy calcification of
160 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 160

(a)
(b)
(c)
(d)
Figure 10.1 Renal artery stenting in a case of bilateral ostial renal artery stenosis demonstrating the importance of coveringthe renal ostium – restenosis after 3 months due to suboptimal stent placement. (a) High grade bilateral renal arterystenosis. (b) Stent implantation in the right renal artery with apparently optimal result. However, the suboptimal placement ofthe stent – not completely covering the ostium of the renal artery – cannot be seen in this projection. (c) Moderate restenosisafter 3 months at the proximal edges of the stent. (d) Stent implantation in the left renal artery with excellent technical result.
COMPLICATIONS IN RENAL AND MESENTERIC VASCULAR INTERVENTIONS 161
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 161

162 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Prestenting Poststenting
Figure 10.2 Misplacement of a renal stent with the stent extending too much into the aorta. Clinically, no complicationswere observed in this patient.
Figure 10.3 Dissection of a renal artery after placement of a guiding catheter through the stenosis. The dissection couldbe resolved by stenting with a balloon-expandable bare metal stent.
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 162

the renal ostium, and when high pressure dilationis needed to dilate or expand the stent. In thiscase, the rupture site has to be immediately sealedwith a balloon and further with a covered stentgraft, otherwise most patients will need an emer-gency operation. When ruptures cannot be han-dled by endovascular treatment, the occlusionballoon has to be kept in place and the patienttransferred to the operating room. The ‘warmischemia’ time has to be reduced as much as pos-sible to avoid renal infarction and nephrectomy.Figure 10.4 shows an example of a complete rup-ture of a renal artery after balloon dilation. Theorifice of the artery was immediately sealed witha large balloon in the aorta. A covered stent thencould not be passed to the renal artery, thereforethe patient was transferred to the operating room.Besides rupture at the renal ostium, the arterymay also rupture more distally, particularly innon-compliant, calcified artery. Again, immediate
balloon occlusion and implantation of a stent graftis the treatment of choice.
Perforation
Manipulation with the guidewire in the subseg-mental arteries is the most frequent cause of per-forations, while perforation during passage of thestenosis occurs relatively seldom. This compli-cation is more frequent during recanalization ofchronic total occlusions. The choice of the wire aswell as a stable position of the tip of the wire dur-ing the entire intervention is crucial to reduce therisk for this complication. Figure 10.5 shows acase with a perforation of the renal parenchymaduring recanalization of a chronic total occlu-sion. The bleeding could be stopped by antago-nizing heparin with protamine and spontaneoustamponade. As a consequence of perforation,deleterious bleeding may occur and secondary
COMPLICATIONS IN RENAL AND MESENTERIC VASCULAR INTERVENTIONS 163
Figure 10.4 Rupture of the renal artery during balloon angioplasty of a left-sided ostial renal artery, stenosis, andsuccessful sealing of the rupture site using a large compliant balloon. (Courtesy of Dr P Waldenberger, Innsbruck, Austria.)
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 163

(partial) nephrectomy is a feared consequence.Figure 10.6 shows a case when perforation andbleeding resulted in secondary nephrectomy.
Thrombosis
Renal artery occlusion as a complication duringthe intervention is reported in 1 to 2.5% of theprocedures in the renal trunk, segmental arteryocclusion in 1 to 2%.15 However, most of theseacute occlusions can be successfully recanalizedduring the procedure and the rate of renal infarc-tion due to acute procedure-induced thrombosisis expected to be below 1%. Stent thrombosis veryrarely occurs with modern stents, adequate (dual)antiplatelet therapy including aspirin and athienopyridine, and a good final result after stent-ing (residual stenosis below 30%, no dissection).However, when dissections distal to the stentremain unrecognized, early stent thrombosis mayoccur despite adequate antiplatelet medication.Good quality final angiograms are thereforeimportant before removing the wire and the guide.
Embolization
Microemboli to the renal artery presumablyoccur in most interventions and may be thecause for renal deterioration in a considerablenumber of patients; unfortunately, data on the fre-quency and the true impact of this complication
are not available. Macroembolization was re-ported in up to 8% in early series; more recentdata indicate a macroembolization rate of around1%.15 Furthermore, besides the use of low profilecatheter material and atraumatic techniques, thereis no reliable technique to avoid microemboliza-tion. Current protection devices seem inade-quate for most renal or mesenteric procedures.
Cholesterol embolization is a worrying syn-drome and occurs especially in a diffuse athero-matous or aneurysmatic aorta. The syndromemay become evident days after the procedurewith an incidence of up to 3%. Signs of periph-eral embolization (Figure 10.7) as well as sys-temic inflammation and renal deterioration arecharacteristic for this potentially life-threateningcondition.
Spasm
Renal artery spasm can be induced by the wire,guiding catheter, balloon, or stent. Spasm lessfrequently occurs in calcified artery and mostlycan be resolved by local administration of 0.1 mgdiluted nitroglycerin or by papaverine in case ofmesenteric interventions. The most importantdifferential diagnosis is perforation and dissec-tion – which per se might induce severe spasmsand need mechanical stabilization by stentimplantation.
164 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 10.5 Perforation during recanalization of a chronic total renal artery occlusion. The bleeding could be stopped byantagonizing heparin with protamine and spontaneous tamponade.
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 164

Renal failure
Deterioration of renal function after renalartery interventions is reported in approximately15% of the patients.21 Several risk factors havebeen acknowledged and there exist some effec-tive strategies to minimize the risk for this com-plication. In contrast to other percutaneousinterventions – when renal dysfunction is a con-traindication for an intervention – renal dysfunc-tion can be a good indication to treat renal arterystenosis. Nevertheless, the patient and physicianhave to be aware that, particularly in cases withpre-existent renal impairment, there is much towin but at least as much to lose following a per-cutaneous renal treatment.
According to the Society of InterventionalRadiology, the overall threshold for major com-plications of percutaneous renal revasculariza-tion is 10%,15 realistically this rate can be reducedto below 3% in skilled hands. Thresholds15 for
30-day mortality (1%), secondary nephrectomy(1%), surgical salvage operation (2%), sympto-matic embolization (3%), main renal artery occlu-sion (2%), branch renal artery occlusion (2%),complicated access site hematoma (5%), and acuterenal failure (2%) also seem unacceptably highand certainly can be reduced by adequate train-ing and the use of proper materials.
FACTORS IDENTIFYING HIGH-RISK PATIENTSFOR COMPLICATIONS
Two major determinants of complications haveto be considered. First, patients’ comorbiditiesincluding age, pre-existent renal failure, conges-tive heart failure and diabetes mellitus. Second,anatomical factors of the renal arteries and theaccess route. Unfavourable anatomies include tor-tuous iliac arteries, heavy calcification and kink-ing of the aorta, steep angle of the renal artery
COMPLICATIONS IN RENAL AND MESENTERIC VASCULAR INTERVENTIONS 165
Figure 10.6 Renal main stem perforation during recanalization of a segmental artery occlusion which resulted insecondary nephrectomy.
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 165

origin, short trunk of the renal artery – i.e. earlybifurcation to segmental arteries, heavily calci-fied stenosis, or fresh thrombotic lesions, andfinally extended soft, mainly thrombus contain-ing plaques of the aorta.
Comorbidities
With increasing age, the degree of calcificationusually rises and the likelihood for arterialkinking and tortuosity increases. Furthermore,renal functional reserve naturally decreases withincreasing age, making patients more vulnera-ble for contrast-induced complications. Increasedage, per se, of course is not a contraindication fora renal or mesenteric intervention, but the inter-ventionist has to be aware that some specificmeasures like preprocedure hydration and MRangiography of the access route should be con-sidered mandatory in these patients.
Pre-existent renal failure frequently is the indica-tion to perform renal artery stenting. Particularlyin these patients, the benefit of the interven-tion can be striking; unfortunately, the risk forrenal failure following an intervention also isincreased. Again, preprocedure care, includingadequate hydration, administration of acetyl-cysteine (600 mg bidaily), and limiting the amountof contrast agent, is a cornerstone in the man-agement of these patients. The use of alternativecontrast agents like carbon dioxide or gadolin-ium alone or in combination with iodinated con-trast agents may reduce the risk of deteriorationof renal dysfunction.22,23
Congestive heart failure (CHF) is a frequentlyneglected risk factor for renal failure after percu-taneous interventions. The main impact of CHFon renal function is based on chronic renalhypoperfusion due to low cardiac output on theone hand as well as renal vasoconstriction fol-lowing enhanced sympathetic activity. Patientswith CHF require monitored fluid managementperiprocedure which has to balance hydrationin relation to urine volume and the risk of pul-monary congestion.
Diabetes mellitus increases the risk for complica-tions due to its impact on microvascular andmacrovascular disease. Microvascular renal dis-ease causes impaired renal function and elevatedrenovascular resistance, which is considered a riskfactor for non-response with respect to bloodpressure improvement after renal interventions.24
Macrovascular diabetic disease is characterizedby a tendency for extensive calcification of theaccess route, aorta, and renal arteries, whichincreases the risk for embolic complications.
Anatomic factors
Tortuous iliac arteries can complicate the accessand even if access through these arteries can beachieved, tortuosity reduces the steerability ofthe catheter material at the site of the target ves-sel. Preprocedure imaging with magnetic reso-nance imaging angiography helps to identifypatients with complicated access routes and inthese patients alternative routes like transradialor transbrachial access can be an adequate choice.The morphology of the aorta is a key determinantfor potential problems during the intervention.
166 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 10.7 Sign of peripheral embolization in a patientafter renal artery stenting.
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 166

Heavy calcification, multiple (ulcerated) plaques,and kinking of the aorta can cause complicationsduring positioning of the guiding catheter orsheath even before access to the target vessel hasbeen gained. Again preprocedure imaging andplanning of the intervention is crucial in thiscontext. Furthermore, specific atraumatic tech-niques for placement of the guiding catheter orsheath should be applied (which will be describedbelow). Usually, right renal arteries will be bestaccessed from the right transfemoral approachand left renal arteries from the left groin. Theeasiest access route for the celiac trunk and supe-rior mesenteric artery is from a transbrachial ortransradial approach. The angle of the renal arteryoriginating from the aorta usually is between 60and 90�; in patients with very steep angles, trans-femoral access can be difficult. However, in thesepatients, coming from above frequently is aneasy and safe solution and avoids the problemof unstable catheter back-up.
A short trunk of the renal artery due to an earlybifurcation to segmental arteries as well as bifur-cated lesions (Figure 10.8) can complicate renalprocedures. The use of multiple wires and thekissing balloon technique demands high inter-ventional skills, but enables safe treatment ofbifurcated lesions.
Unfavorable lesion morphology includes heav-ily calcified stenosis or fresh thrombotic lesions.Calcification can be a particular problem whenprimary stenting is anticipated. First, placementof the stent may be difficult – even low profilerapid exchange stents can get lost in patientswith very tight and rigid stenosis when predila-tion is not done adequately. Second, some lesionscan be resistant even to high pressure postdila-tion, causing a significant residual stenosis in thestented segment. In these patients the risk forstent thrombosis and restenosis is increased, andruptures have been reported when postdilation ofthe artery was done with very high pressures.
COMPLICATIONS IN RENAL AND MESENTERIC VASCULAR INTERVENTIONS 167
Figure 10.8 Double wire and kissing stent technique for treatment of a renal bifurcated lesion. (Courtesy of Dr P Waldenberger, Innsbruck, Austria.)
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 167

In these patients lesion preparation by predilation –eventually using cutting balloon angioplasty – canbe helpful to avoid these complications.
COMPLICATIONS OF SPECIFIC INTERVENTIONAL STEPS AND TOOLS
Placement of the guiding catheter or long sheath
Engaging the ostium of the renal artery has to bedone as atraumatically as possible. Particularly,plaque disruption of the aorta during the accessto the renal artery frequently may causeembolization. Most frequently, these are microem-bolic showers, both to the renal and peripheralarteries. In this context, cholesterol embolizationcan be a worst case scenario. It has been sug-gested that plaque rupture and delayed healingof the vulnerable plaque at the renal artery or inthe abdominal aorta causes these severe emboliccomplications. Treatment options for this com-plication are unclear, and different approacheshave been proposed: aggressive anticoagulationon the one hand, to inhibit further local throm-botic applications and support emboli resolution,as opposed to discontinuing any antithromboticdrugs on the other hand, to allow healing of thevulnerable plaque. Fatal courses of cholesterolemboli are relatively frequent, and as yet all rec-ommendations to prevent or treat this symptomare not evidence-based.
Manipulation with the guiding catheter orsheath may also initiate a dissection of the renalartery, celiac or mesenteric artery, or the aorta.This is a rather infrequent complication as longas dedicated materials with soft tips are usedand the tip of the guiding catheter or sheath iskept out of the orifice of the renal artery. In thiscontext, we recommend not inserting the tip of the guiding catheter or sheath through thestenosis.
Wire passage
Potential complications during this interven-tional phase are dissection of the plaque, plaqueshift and acute vessel thrombosis, and perforationof the renal parenchyma. Non-hydrophilic wireswith malleable soft tips (usually 0.014 inch) cer-tainly reduce the risk for these complications.
Predilatation
The risk for complications during predilatationis relatively small; usually undersized balloonsare used for plaque preparation. Potential compli-cations mainly include peripheral embolization,which remains asymptomatic in most patients.
Stenting
Implantation of the stent according to the nomi-nal diameter of the artery or with minimal over-sizing bears several possible risks. Rupture of theartery certainly is a rare but worst scenario.Other complications are dissection at the distaledge of the stent, acute stent thrombosis, and stentmisplacement. The risk for rupture and dissectionincreases with an increased stent-to-artery ratio;oversizing therefore should be limited to 10% ofthe reference vessel lumen. Acute stent thrombo-sis can be more or less completely avoided withadequate premedication with dual antiplateletinhibitors (clopidogrel or ticlopidine plus ASA)and low dose peri-intervention heparin (usually2000 to 5000 IU heparin) or bivalirudin.
Postdilatation
Since the recommended stents for renal arteriesare balloon expanding, postdilatation will not beneeded routinely. Aggressive postdilatation againbears the risk of rupture and dissection, particu-larly when the edges of the balloon are not keptstrictly within the margins of the stent. Whenchoosing the size of the postdilatation balloon,the interventionist has to be particularly carefulin patients with post-stenotic dilatations of therenal artery distal to a high-grade stenosis. Inthese patients, the stent and balloon have to fitto the size of the renal artery prior to the post-stenotic dilatation to reduce the risk of oversiz-ing and severe vessel injury.
METHODS TO DETECT POTENTIAL COMPLICATIONS – WHICH DIAGNOSTICSTEPS ARE NEEDED ROUTINELY TO RULE OUT OR IDENTIFY COMPLICATIONS
Angiography
It is still mandatory to be aware of the necessity tominimize the amount of contrast agent and for
168 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 168

adequate pre- and postintervention angiogramsof the entire renal artery and the kidney. The mainissues which have to be ascertained in the finalangiogram are a good local result, exclusion ofdissection, perforation, and bleeding. The latterin particular has to be excluded with certainty,as unrecognized and untreated bleeding mayendanger the patient’s organ and life.
Ultrasound
This has a limited role in excluding complicationsat the renal artery, but can be helpful as a rapidlyavailable technique to visualize renal infarct orparenchymous bleeding. Duplex ultrasound canbe helpful in excluding renal stent thrombosis.Unfortunately, renal arteries cannot be adequatelyvisualized by ultrasound in approximately 20%of the patients.
Computed tomography
This is the method of choice to exclude bleedingand infarcts. The main shortcoming of CT is theadditional amount of contrast agent needed toexclude bleeding complications.
ENDOVASCULAR, SURGICAL AND/ORMEDICAL TECHNIQUES TO RESOLVE COMPLICATIONS
Endovascular techniques
Most complications of renal and mesenteric arteryinterventions can be resolved by endovasculartechniques.
Balloon inflation
Balloons are effective for sealing ruptures or per-forations in all cases when a wire can be passed bythe site of the bleeding. The balloon should beinflated to low pressures only in a 1:1 balloon-to-artery ratio. It has to be checked angiographi-cally that the balloon adequately occludes the siteof perforation. Balloon inflation in patients withrupture always has to be combined with reversalof heparin using protamine. An initial inflationtime of 3 to 5 minutes usually helps to stabilizethe patient. In patients with massive bleeding andwhen the bleeding site cannot be passed with a
balloon, sealing of the ostium of the artery or eventhe aorta can be effective and life-saving as abridge to an emergency operation (Figure 10.4).In contrast to other peripheral vessels, dissectionsare usually treated by stent implantation ratherthan by prolonged balloon angioplasty only.
Bare stents
These are the methods of choice to resolve dis-sections (Figure 10.9) or residual stenosis afterballoon angioplasty in patients with fibromus-cular dysplasia or non-ostial stenosis, when bal-loon angioplasty alone was attempted. However,if dissection and perforation occur during theinitial wire passage, endovascular managementbecomes complex (Figure 10.10). The most criti-cal point is safe re-entry with the wire throughthe true lumen. As soon as this step has been
COMPLICATIONS IN RENAL AND MESENTERIC VASCULAR INTERVENTIONS 169
Figure 10.9 Wire-induced dissection of the renal arterytrunk which could be resolved by implantation of a balloon-expandable bare metal stent.
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 169

completed, bare stents (self-expanding or balloon-expandable) can be used to ensure a sufficientresult (Figure 10.10).
Covered stents
Recently, balloon-expandable and self-expandingcovered stent grafts in sizes and profiles adequatefor renal and mesenteric arteries became avail-able. These devices usually are more rigid thanbare metal stents. However, covered stents arevery effective in treating complications like rup-ture, bleeding, or aneurysms. Figure 10.11 showsan example of the use of a covered self-expandingstent graft in a patient with an aneurysm of the
right renal artery; it can be used in similar waysto cover perforations and bleeding sites.
Embolization
In cases with perforation of the renal parenchymawith the tip of the wire, antagonizing anticoagula-tion and immediate embolization of the perforatedsegmental artery with coils can save the patient’skidney. Adequately sized coils for vessels from 2 to 6 mm have to be available in the cath lab.
Aspiration and thrombolysis
Local thrombolysis is very effective for thetreatment of acute renal or mesenteric artery
170 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 10.10 Perforation and bleeding during wire passage for recanalization of an in-stent occlusion of a right renalartery (1, 2). Finally, the wire can be re-advanced through the true lumen (3) and a self-expanding stent is implanted tore-open the artery (4, 5).
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 170

thrombosis including stent thrombosis. Beforethrombolysis is initiated, aspiration thrombec-tomy can be attempted, using coronary aspira-tion catheters (like the Export or Pronto device).Urokinase as well as rt-PA can be used locallyvia perfusion catheters.
Surgical techniques
Secondary surgical procedures are reported in 1to 2.5% of cases in larger series.15 Uncontrolled
bleeding usually necessitates nephrectomy. Therate of complications of elective nephrectomy islow; emergency nephrectomy carries an opera-tive risk for major complications of 15 to 30%. In patients with complete rupture of the artery,emergency bypass surgery can resolve the problem,again at a risk for major complications rangingbetween 10 and 25%.
Medical approaches
Besides the use of thrombolysis, the interventionisthas to be familiar with antagonizing anticoagula-tion – e.g. heparin by administration of protamine.Figure 10.12 shows an example of a severe bleed-ing after perforation with the guidewire, whichcould be handled conservatively by antagonizinganticoagulation. Dosage of protamine is usuallyrecommended in a 1:1 ratio to heparin. In patientswith complex bleeding disorders, fresh frozenplasma and prothrombin complex concentratesmay be necessary.
METHODS TO AVOID COMPLICATIONS
Preprocedure work-up
Before starting the procedure, the interventionisthas to know the patient’s medical history, medica-tion and comorbidities, the degree of stenosis,anatomy of the aorta, and level of the renal ostium.In skilled hands, duplex ultrasound is the most ade-quate non-invasive method to assess the degree ofstenosis and hemodynamic significance of a renalartery. Unfortunately, duplex ultrasound will notgive adequate information on the access route inmany patients. MR angiography (MRA) seemsmost adequate to assess these anatomic condi-tions, although the degree of stenosis is frequentlyoverestimated by MRA. We recommend usingMRA in all patients with risk factors for extensiveatherosclerosis like elderly, diabetic patients,patients with known coronary or peripheral arterydisease, and patients with pre-existing renal dys-function, to minimize the amount of contrastagent. However, recent data indicate that particu-larly in patients with advanced renal insufficiencythe use of the MR-contrast agent Gadolinium maylead to severe systemic complications callednephrogenic systemic fibrosis and therefore has to belimited whenever possible.
COMPLICATIONS IN RENAL AND MESENTERIC VASCULAR INTERVENTIONS 171
Figure 10.11 Example of the use of a covered stent graft ina patient with a renal artery aneurysm. These devices canalso be applied to seal perforations or ruptures of the artery.
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 171

Medical pretreatment
Intravenous hydration of the patient with intra-venous saline solution starting the day before theintervention should be anticipated in all patientswith increased risk for renal failure includingthe elderly, diabetics, patients with CHF, andpatients with pre-existent renal dysfunction.Furthermore, data support the use of acetyl cys-teine, 600 mg bidaily, starting the day before theintervention and continuing until one day afterthe intervention. Finally, dual antiplatelet therapyhas to be given; in patients without pretreatmentof clopidogrel or ticlopidine we recommend 300 mgclopidogrel (1000 mg ticlopidine) as a loadingdose.
Choice of contrast agent
Iodinated contrast medium can result innephropathy. Iso-osmolar contrast agents likeiodixanol have been demonstrated to exhibit animproved renal safety profile compared to low-osmolar contrast agent.25 Therefore, the uniformuse of iso-osmolar contrast agents in patientsundergoing renal interventions is recommended.
Projection
Precise placement of the stent is crucial, for thispurpose the stenosis has to be adequately visu-alized during angiography. MRA can be helpfulto determine the best angiographic angle forangiography. In patients without MRA, we rec-ommend a 20 to 25� LAO projection as a standardview for renal interventions.
Low profile rapid exchange systems
Low profile rapid exchange (RX) or ‘monorail’systems are today’s standard for coronary inter-ventions, and RX therefore was formerly referredto as ‘coronary technique’, implicating the use ofguiding catheters and low profile devices. Tech-nologic improvements in renal artery interven-tions have substantially reduced the complicationrate in the past 5 years,6 and the introduction ofRX systems certainly contributed to this devel-opment. A significant reduction in fluoroscopyand procedure time was found when RX catheterswere used for renal stenting, with identical suc-cess and complication rates compared to the con-ventional over-the-wire coronary angioplastysystems.1 Besides the advantages for the inter-ventionist of comfortably handling shorter wires,the introduction of RX devices also enabled adecrease in the diameter of wires and size ofcatheters and stents. Data suggest that the use ofRX systems also translates into an improvedsafety of the procedure.16
Choice of wire
Passage through the stenosis can be done eitherwith a non-hydrophilic 0.035-inch wire (Bentson)using an atraumatic technique described by DrSos, or directly with non-hydrophilic 0.014-inchwires. During the intervention, non-hydrophilic
172 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 10.12 Bleeding due to guidewire perforation whichcould be managed conservatively by antagonizing heparinwith protamine.
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 172

0.014-inch wires with a stiff body and flexible andsoft tips should be used throughout. The tip of thewire has to be visualized during the entire proce-dure and should be kept in the segmental arter-ies without entering the subsegmental space. Theuse of hydrophilic glide wire should not be con-sidered for renal and mesenteric interventions.
Engaging the renal artery
An atraumatic technique to place the guidingcatheter or sheath and enter the renal artery is thekey for success in renal and mesenteric interven-tion. The technique displayed in Figure 10.13 wasdescribed by Dr Sos and is probably one of theeasiest and fastest ways to get safe access. Usinga small shepherd hook shaped catheter (Sos-omni)and a 0.035-inch non-hydrophilic guidewire(Bentson) the renal artery is approached frombelow. The guidewire is retracted in the diagnos-tic catheter until approximately 1 cm of the tipof the wire is extending out of the diagnosticcatheter. The catheter and the guidewire are thenadvanced cranially until the tip of the guidewirejumps laterally into the renal ostium. The catheteris then slightly retracted and the guidewireadvanced through the stenosis. In the coaxialtechnique, a guiding catheter or sheath can now besafely advanced to the renal ostium, the 0.035-inch wire is exchanged for a 0.014-inch renal wireand the diagnostic catheter can be removed.
If the traditional technique of direct cannula-tion of the renal artery ostium with the guidingcatheter is used, to avoid renal embolism prior toselective renal angiography, the guiding cathetershould be cleaned from debris by aspiration ofblood through the guiding catheter (‘proximalprotection’). This technique cleans the tip of theguiding catheter from debris collected duringthe engagement of the renal artery and thereforereduces the risk of renal embolism.
Pressure gradients
With adequate preprocedure work-up, mea-surement of pressure gradients usually is notnecessary, particularly if high-grade stenosis istreated. For pressure measurement, pressurewires rather than 4 Fr diagnostic catheters shouldbe used to reduce the risk for trauma, plaque
disruption, and acute occlusion of the arteryduring this diagnostic work-up.
Predilation
When low profile catheter systems are used,predilation is not mandatory any more. However,in short and ostial stenosis, when calcification issuspected, and in all cases when the interven-tionist is in any doubt about easy passage of thestent, predilation should be considered. There is
COMPLICATIONS IN RENAL AND MESENTERIC VASCULAR INTERVENTIONS 173
(a) (b)
(c)
(e)
(d)
Figure 10.13 Atraumatic approach for treatment of renalor mesenteric artery stenosis. (a) Using a small shepherdhook shaped catheter (Sos-omni) and a 0.035 non-hydrophilic guidewire (Bentson) the renal artery isapproached from below. (b) The guide wire is retracteduntil approximately 1 cm of the tip is extending out of thediagnostic catheter. (c) The catheter and the guidewire areadvanced cranially until (d) the tip of the guidewire jumpsinto the renal ostium. (e) The catheter is slightly retractedand the guidewire advanced through the stenosis. In thecoaxial technique, a guiding catheter can now be safelyadvanced to the renal ostium.
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 173

hardly any complication which may arise due topredilation with undersized balloons, but thisadditional step may significantly facilitate stentdeployment, reduce the risk for ‘jumping’ of thestent, and thus increase the safety of the proce-dure. In patients with very rigid stenosis, cuttingballoon angioplasty can help to prepare the plaqueand avoid high pressures during stent implanta-tion and postdilation.
Stenting
Precise sizing and placement of the stent are cru-cial. It is known from several studies that therisk for restenosis correlates with the diameterof the stent – larger stents have a lower risk forrestenosis. However, oversizing increases therisk for dissection and rupture and should not bedone to more than 10%. Stent length is also associ-ated with restenosis – as long as bare-metal stentsare used. Nevertheless, the length has to be ade-quate to cover the entire plaque and avoid distalplaque shift. Stent deployment is best done underthe patient’s apnea after expiration. The degree ofresidual stenosis has to be minimized to reducethe risks for stent thrombosis and restenosis.
Postdilatation
Postdilatation of balloon-expanding stents is notmandatory, but should be considered in patientswith a suboptimal result (> 10% residual steno-sis). The risk of rupture and bleeding increaseswith pressure, particularly after high-pressurepostdilatation a control angiogram should betaken, before the balloon is removed, especiallyif the patient is complaining of an acute onset ofback pain; in case of bleeding the balloon can berapidly re-inflated to seal the leakage.
Protection devices
Currently, no protection device adequatelydesigned for renal or mesenteric arteries is avail-able and the number of patients with an anatomysuitable for carotid protection devices is low.Furthermore, carotid protection devices mayintroduce the risk for additional complications – inparticular removal of the filter devices after
stenting sometimes can be challenging, when theretrieval catheter cannot be advanced throughthe stent. Therefore, current protection devicescannot be recommended for routine applicationsin the renal and mesenteric arteries.
Final angiography
We recommend to always perform two finalangiographic runs: one before the wire isremoved to exclude dissection, perforation, andbleeding, and a second run after removal of thewire to document the final result. In particular,the first run with the wire still in place is crucial,as re-entering the wire through a dissection orruptured artery can be very difficult. Angiogra-phy always has to be done during the procedurein case of unexplained back or flank pain to ruleout severe complications.
Knowing where to stop
Finally, stopping an intervention before theoccurrence of a complication is always prefer-able to the treatment of a potentially avoidablecomplication. Time is usually a good indicatorof how things are going during an intervention.The standard time for a renal or mesenteric ostialangioplasty is between 15 and 35 minutes frompuncture to closure – if these times are vastlyexceeded, stopping the procedure seems an ade-quate option.
SUMMARY
Renal and mesenteric artery interventions can beone of the safest and fastest peripheral interven-tions. Adequate indication, thorough preproce-dure work-up, choice of medication and materials,and atraumatic technique are the key issues forsuccess.
CHECK LIST FOR EMERGENCY EQUIPMENTFOR INTERVENTIONS
• covered stent grafts 4 to 7 mm in diameter and10 to 20 mm in length (balloon-expandable orself-expanding)
174 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 174

• large diameter balloons to seal the aorta• vascular coils suitable for vessels of 2 to 6 mm• 0.014-inch guidewire compatible aspiration
catheters• thrombolytics• protamine.
REFERENCES
1. Linnemeier TJ, McCallister SH, Lips DL et al. Radiationexposure: comparison of rapid exchange and conven-tional over-the-wire coronary angioplasty systems.Cathet Cardiovasc Diagn 1993; 30: 11–14.
2. Van Jaarsveld BC, Krijnen P, Pieterman H et al. Theeffect of balloon angioplasty on hypertension in athero-sclerotic renal-artery stenosis. N Engl J Med 2000; 342:1007–14.
3. Nordmann AJ, Logan AG. Balloon angioplasty versusmedical therapy for hypertensive patients with renalartery obstruction. Cochrane Database Syst Rev 2003:CD002944.
4. Zeller T, Frank U, Müller C et al. Stent-supportedangioplasty of severe atherosclerotic renal artery steno-sis preserves renal function and improves blood pressurecontrol: long-term results from a prospective registry of456 lesions. J Endovasc Ther 2004; 11: 95–106.
5. Zeller T, Müller C, Frank U et al. Survival after stentingof severe atherosclerotic ostial renal artery stenosis. J Endovascular Ther 2003; 10: 539–45.
6. Zeller T, Frank U, Müller C et al. Technological advancesin the design of catheters and devices used in renal arteryinterventions: impact on complications. J Endovasc Ther2003; 10: 1006–14.
7. Beek FJA, Kaatee R, Beutler JJ et al. Complications dur-ing renal artery stent placement for atherosclerotic ostialstenosis. Cardiovasc Interv Radiol 1997; 20: 184–90.
8. Rees CR, Palmaz JC, Becker GJ et al. Palmaz stent in ath-erosclerotic stenoses involving the ostia of renal arteries:preliminary report of a multicenter study. Radiology1991; 181: 507–14.
9. Bakker J, Goffette PP, Henry M et al. The Erasme study:a multicenter study on the safety and technical resultsof the Palmaz stent used for the treatment of atheroscle-rotic ostial renal artery stenosis. Cardiovasc Interv Radiol1999; 22: 468–74.
10. Van de Ven PJG, Kaatee R, Beutler JJ et al. Arterial stentingand balloon angioplasty in ostial atherosclerotic renova-scular disease: a randomized trial. Lancet 1999; 353: 282–6.
11. Bush RL, Najibi S, Macdonald J et al. Endovascularrevascularization of renal artery stenosis: technical andclinical results. J Vasc Surg 2001; 33: 1041–9.
12. Leertouwer TC, Gussenhowen EJ, Bosch JL et al. Stentplacement for renal arterial stenosis: where do westand? A meta-analysis. Radiology 2000; 216: 78–85.
13. Baumgartner I, Von Aesch K, DO D et al. Stent place-ment in ostial and nonostial atherosclerotic renal arte-rial stenosis: a prospective follow-up study. Radiology2000; 216: 489–505.
14. Dorros G, Jaff M, Jain A et al. Follow-up of primaryPalmaz–Schatz stent placement for atherosclerotic renalartery stenosis. Am J Cardiol 1995; 75: 1051–5.
15. Martin LG, Rundback JH, Sacks D et al. Qualityimprovement guidelines for angiography, angioplasty,and stent placement in the diagnosis and treatment ofrenal artery stenosis in adults. J Vasc Interv Rad 2003;14: S297–310.
16. Amighi J, Sabeti S, Dick P et al. Impact of rapidexchange vs. over-the-wire technique on procedure com-plications of renal artery angioplasty. J Endovasc Ther2005; 12: 233–9.
17. Zeller T, Frank U, Müller C et al. Predictors of improvedrenal function after percutaneous stent-supported angio-plasty of severe atherosclerotic ostial renal artery steno-sis. Circulation 2003; 108: 2244–9.
18. Kasirajan K, O’Hara PJ, Gray BH et al. Chronic mesen-teric ischemia: open surgery vs. percutaneous angio-plasty and stenting. J Vasc Surg 2001; 33: 63–71.
19. Sharafuddin MJ, Olson CH, Sun S et al. Endovasculartreatment of celiac and mesenteric arterial stenosis:applications and result. J Vasc Surg 2003; 38: 692–8.
20. Zeller T, Büttner HJ, Lorenz HM et al. Late aortic dislo-cation of a stent following stent angioplasty for ostialrenal artery stenosis. Cathet Cardiovasc Interv 2002; 56:416–20.
21. Sabeti S, Schillinger M, Mlekusch W et al. Contrastinduced acute renal failure in patients undergoing renalartery angiography vs. renal artery PTA. Eur J VascEndovasc Surg 2002; 24: 156–60.
22. Zeller T, Müller C, Frank U et al. Percutaneous translu-minal angioplasty using gadodiamide as an alterna-tive contrast agent in patients with contraindications toiodine-containing contrast agents. J Endovasc Ther 2002;9: 625–32.
23. Strunk H, Schild H, Mortasawi MA. Arterial interven-tional measures using carbon dioxide (CO2) as a contrastmedium. Rofo Fortschr Geb Rontgenstr Neue BildgebVerfahr 1992; 157: 599–600.
24. Radermacher J, Chavan A, Bleck J et al. Use of Dopplerultrasonography to predict the outcome of therapy forrenal artery stenosis. N Engl J Med 2001; 344: 410–17.
25. Aspelin P, Aubry P, Fransson SG et al. Nephrotoxiceffects in high-risk patients undergoing angiography.N Engl J Med 2003; 348: 491–9.
COMPLICATIONS IN RENAL AND MESENTERIC VASCULAR INTERVENTIONS 175
CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 175

CPVI_Chapter10.qxp 4/5/2007 2:47 PM Page 176

INTRODUCTION TO THE FREQUENCY ANDTYPE OF COMPLICATIONS
Aorto-iliac intervention is a commonly per-formed endovascular procedure and yet the datato indicate the prevalence of complications arefew. The problem is compounded by a lack ofuniformity in the definition of a complication ofendovascular intervention. Perhaps the best con-temporary data come from the second BIAS IIreport, which prospectively looked at outcomesin 2152 patients from 46 hospitals in the UnitedKingdom.1 That report detailed an overall peri-procedural complication rate of 5.7%. Compli-cations were more likely to occur in patients withcritical limb ischemia (CLI) compared to claudi-cation (18% vs 2.5%), but interestingly there wasno significant difference between those patientstreated with angioplasty or stents. Such infor-mation will be undoubtedly skewed by patientselection. More complex lesions are likely to havebeen treated by stent placement including theirprimary use in iliac occlusions rather than simplestenoses. In addition, there was a low rate (0%)of complications in patients treated as a day case,again reflecting good patient selection and anundoubted bias towards claudicants rather thanpatients with CLI.
The meta-analysis of aorto-iliac interventionperformed by Bosch et al detailed a systemiccomplication rate of 1%, a local (access and treat-ment site and embolization) complication rate of9%, a complication rate requiring intervention of5.2%, and a mortality rate of 0.3%.2
The Dutch iliac stent trial had prospectiveassessment and recorded an overall complica-tion rate of 5.7% in a group of patients who werepredominantly claudicants.3
Periprocedural complications can be assessedas occurring (a) at the access site, (b) at the treat-ment site, and (c) systemic, away from the treatedarea. Access-related issues have been describedin an earlier chapter.
Target site complications
Acute closure
The frequency of occlusion at the angioplastysite varies between 1 and 7% and does not seemto be related to the severity or location of thelesion.4 When management of a stenosis resultsin acute closure at the time of treatment themechanism is usually dissection. When closurefollows balloon dilatation of an occlusion then
11
Complications of aorto-iliac interventionDeepa Gopalan and Peter Gaines
Introduction to the frequency and type of complications • Factors identifying high-risk patients •Complications of specific interventional steps and tools • Methods to detect complications •Endovascular, surgical, and medical techniques to resolve complications • Check list for emergency equipment
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 177

vessel recoil may be responsible. Acute throm-bosis typically follows a primary mechanismthat limits flow (Figure 11.1). Spasm of sufficientintensity to close a diseased iliac artery must beextremely rare.
Delayed closure
Closure of the treatment site within a few dayseither follows a technically imperfect primarytreatment (a high-grade residual stenosis/dis-section or misplacement of a stent) or resultsfrom poor run-off below the treated segment.
Rupture
Arterial rupture during balloon angioplasty is apotentially life-threatening complication but,fortunately, it occurs in only about 0.5% ofcases.5,6 In the BIAS II data set the rupture ratewas 1.2% and entirely limited to stent place-ment. This is likely to be because stents will have
been placed to manage complex disease such asiliac occlusions.
Stent infection
Since the publication of the first suspected infec-tion associated with an endovascular stent byChalmers et al,7 the growing number of infectionsinvolving stent grafts represents an emergingproblem. However, it still remains a very rarecomplication of simple stents placed in the iliacvessels. An international enquiry by Fiorani et alestimated the frequency of endograft infectionto be about 0.4%.8 This estimate is, however, inexcess of our own experience. This report sug-gested that the development of endoprostheticinfection may be influenced by secondary adjunc-tive procedures, immunosuppression, treatmentof false aneurysms, and infected central lines.
Embolization
Inadvertent embolization distal to the targetvessel occurs in about 1–5% of procedures and ismost frequent when there is attempted recanal-ization of occluded segments9 (Figure 11.2).Within BIAS II this occurred as a complication of1% of cases.1
Cholesterol embolization
Prolonged catheter manipulation in a diseasedaorta can cause cholesterol plaques to gain entryinto peripheral or visceral circulation. It isassociated with a mortality rate of about 80%with poorly described and inadequate treat-ment options.10 Its development is heralded byleg pain with livedo reticularis despite palpablepulses. Outcome is poor despite any active inter-vention often resulting in confusion, renal failure,and death.11
FACTORS IDENTIFYING HIGH-RISK PATIENTS
• Whilst there is considerable discussionamongst interventionalists about which fac-tors result in high risk for endovascularintervention, there is little in the way of anevidence base.
178 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b)
Figure 11.1 (a) Acute iliac occlusion during an attemptedpuncture reversal on a restless patient. (b) Immediatestenting failed to re-establish flow and the patientsubsequently underwent surgery.
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 178

• Calcified lesions and tortuous anatomy makethe procedure more technically demandingand possibly therefore more liable to com-plications due to overly zealous attempts bythe interventionists.
• All plaques are ulcerated and therefore thisis a poor discriminator.
• Occlusions rather than stenoses have longbeen identified as resulting in a high risk ofdistal embolization, particularly when thelesion is long (e.g. longer than 6 cm) andmanaged by angioplasty rather than stenting.
• Rupture is much more common followingtreatment of occlusions rather than stenosis.1
This is possibly because frequently recanali-zation involves entering the ‘subintimal’plane that has a thinner outer aspect com-pared to intraluminal recanalization. Externaliliac occlusions are at higher risk of rupturedue to the poor adventitial support comparedto the common iliac artery. Patients takingsteroids may be at particularly high risk.12
• Diabetic patients are at increased risk ofcomplications because of poor renal function,extensive disease, and poor distal run-off.
• Plaque prolapse is a difficult subject. It wasonce considered mandatory to treat ostialcommon iliac artery disease with kissing bal-loons or stents. This is unnecessary as therisk of plaque prolapsing across into the con-tralateral iliac artery is low and can be appro-priately managed on the rare occasion that itis identified on the completion angiogram.13
Occasionally plaque does protrude into theinternal iliac artery, which is why in someinstitutions patients are warned against therisk of impotence.
COMPLICATIONS OF SPECIFIC INTERVENTIONAL STEPS AND TOOLS
Stenosis
Once access has been achieved from the ipsilat-eral groin the lesion is crossed with a guidewire.Hydrophilic wires in general are associated witha higher number of complications because theyhave less tactile feed-back, are more likely to liftplaque, pass subintimally, and cause inadver-tent dissection. It is our practice therefore to ini-tially use a straight wire directed by a curved(e.g. cobra) catheter. If this fails then we will usea hydrophilic wire.
We treat lesions with a non-compliant balloonwhose size is matched to the diameter of thenormal vessel. Oversizing the balloon runs therisk of arterial rupture. The experienced inter-ventionist will usually ‘eye-ball’ the angiogramand estimate balloon size. If the interventionistis not experienced they should either ask, assesssize from another imaging modality (e.g. gradu-ated catheter angiogram, duplex, CT, etc.).Balloons should be inflated with a manometersince they all have a recommended burst pres-sure, and failure to recognize this makes the inter-ventionist responsible for any complicationfollowing a burst balloon. Balloons tend to burstlongitudinally and therefore without sequelae.Occasionally the balloon will burst circumfer-entially. This makes removal out of the sheathmore difficult. In this situation it may be
COMPLICATIONS OF AORTO-ILIAC INTERVENTION 179
Figure 11.2 Distal embolus seen as filling defect atfemoral artery bifurcation.
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 179

necessary to increase the size of the sheath oreven use a guide catheter to close the balloon if itcannot be brought to the groin from the site ofrupture. Finally, surgery may be required.
Iliac stenoses are usually managed by angio-plasty rather than stent placement. If a stent ischosen then consideration should be given tothe type. Balloon-mounted stents are capable ofprecise placement and therefore we use them fordisease that impinges on the aortic bifurcationso that we do not overhang the opposite com-mon iliac artery. In addition, they can be quiteshort so that a focal lesion can be treated withoutcovering the internal iliac artery. Self-expandingstents are more difficult to place precisely, butcome as longer units and are flexible. For thesereasons we tend to use them when managingtortuous, long segments.
Aortic stenoses are usually treated with kiss-ing balloons since the long-term results aregood, the stenosis often impinges upon the iliacvessels, and the long-term patency of kissingstents is in doubt. In addition, a single large bal-loon will extend down the iliac artery causingrupture unless the stenosis is a long distancefrom the aortic bifurcation. Stent placement isdifficult in this area. Most self-expanding stentsare not big enough for the aorta and some do nothave the required radial force (e.g. Wallstent).Most balloon expandable stents are not largeenough. Those that are (e.g. Palmaz Extra Large)require a single large balloon and are there-fore impossible to place accurately when thestenosis is close to the aortic bifurcation. Stentsin the aorto-iliac segment have their own complications:
1. The stent may not be placed across thestenosis. If this occurs then a second stentshould be placed. There is usually little needto move the first stent.
2. If the stent covers the contralateral commoniliac artery there are two solutions. Ourpreference is to simply place the patient ondual antiplatelet treatment to try to restrictplatelet deposition on the exposed metal.Alternatively an attempt can be made toplace a second stent in the contralateral iliacartery to hold the offending first stent off theorifice.
3. Most balloon-expandable stents do not moveoff the delivery balloon until after deploy-ment. Should the stent move forwards thenit may not be possible to pass a 5 Fr balloonback into the stent. This can be remedied byexchanging the 035" wire for a 018" or 016",passing a 3 Fr balloon catheter into thestent and dilating. If further dilatation isrequired this can then be done using a 5 Frsystem.
4. If the partly expanded stent moves back offthe balloon this is a more difficult situation.It may be possible to bring the balloon backinto the stent and continue dilatation. If it isnot we have either retrieved the balloonfrom the contralateral femoral artery using asnare and cutting the hub off the balloon, orpassed a second 018" wire through the stentfrom the ipsilateral side and increased thediameter of the stent with a 3 Fr balloon.
5. Occasionally a self-expanding stent mayrestrict the retrieval of the delivery nosecone. Persistent jiggling may overcome this.If not, the outer delivery catheter can oftenbe advanced up to the nose cone. Finally,the stent can be dilated by a second accessfollowed by nose cone retrieval.
Occlusion
Occlusions have their own procedural complica-tions in addition to those described for stenoses.Approximately 40% of occlusions are crossedfrom the ipsilateral side. Commonly the wirecontinues to pass subintimally in the aortic wall,but this is invariably without consequence. Ifipsilateral recanalization fails then the wire loop(through-and-through) technique is required.14
This technique requires that a wire is passedantegradely across the occlusion, usually fromthe contralateral groin. This wire often re-entersthe channel formed by the first wire and thewire is then brought out through the ipsilateralgroin and the occlusion treated from the ipsilat-eral side. However, occasionally this second chan-nel remains independent and continues into thecommon femoral artery. We have elected in thissituation to treat the iliac disease from the con-tralateral side and leave the re-entry site in thecommon femoral artery alone.
180 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 180

Distal embolization is more common if theocclusion is predilated. We therefore stent alllesions primarily, followed by postdilatation.
Occasionally left brachial artery access helpsovercome technical difficulties related to aorto-iliac anatomy. Catheterization of the right brachialartery is undesirable because of the potentialembolic complications up the carotid artery.Brachial artery occlusion after percutaneousplacement of a 7 Fr sheath has been reported tooccur in 1.3% of cases.15 Limiting sheath size to5–6 Fr may mitigate this problem. Absent orweak pulsations, brachial pressure differential,or other features suggestive of possible proximalarterial stenosis or occlusion contraindicatebrachial artery catheterization. ‘Blind’ retrogradeadvancement of guidewire and catheter can alsolead to arrhythmia or ventricular perforationfrom intracardiac entry and, therefore, continu-ous fluoroscopic visualization and guidance aremandatory. Caution should be exercised whenapplying tension on a brachial-femoral guide-wire. A catheter should always be placed over thewire to protect the arch and proximal subclavianartery from the cheese-cutting effect of a tensed,rigid wire going across the aorto-subclavianjunction.
METHODS TO DETECT COMPLICATIONS
The diagnosis of complications at the time ofintervention requires a combination of clinicalassessment and appropriate imaging.
Procedural complications
Clinically, most dissections are uneventful anddo not require intervention. Occasionally thepatient will complain of pelvic pain or the ipsi-lateral limb may become acutely ischemic. Thediagnosis of dissection is usually made by a sub-sequent angiogram, although intravascular ultra-sound (IVUS) can be helpful in difficult cases.
Rupture results in acute blood volume loss.Typically the patient experiences pain that per-sists after deflation of the balloon associated withhypotension. The pulse rate normally increasesbut occasionally the clinical picture may mimica vagal episode with initial bradycardia. It iscommonly noted that the retroperitoneal blood
displaces the contrast-filled bladder to the con-tralateral side, and this can be clearly witnessedon fluoroscopy. The diagnosis can be confirmedby a quick angiogram following brisk resuscita-tion. Delayed rupture occasionally occurs. Theclinical features are again those of acute bloodloss and the diagnosis is best confirmed byemergency CT scan.
The diagnosis of embolization is made eitherby routine completion angiography or becausethe patient experiences ischemic pain on thetable. Common impaction sites are where arteriallumen narrows abruptly, e.g. areas of pre-existingatherosclerosis, and branching sites such asthe common femoral bifurcation and poplitealtrifurcation.
Delayed complications
Following apparently uncomplicated interven-tion, patients are observed by nursing personnel.The period of bed rest depends on the sheathsize, use of closure device, and status of accesssite. The patient’s clinical condition is monitoredfor evidence of bleeding, including access-sitehematoma, neurologic changes, and hypoten-sion by following standard instructions.
Delayed closure at the treatment site may notnecessarily result in an ischemic leg. If clinicalexamination confirms a weak or absent femoralpulse, and a decision has been made to inter-vene, then non-invasive imaging (usually US)will confirm the diagnosis.
The clinical manifestation of stent infectioncomprises localized pain, swelling, and ery-thema of the affected limb accompanied by rela-tively non-specific systemic symptoms like fever,generalized malaise, and abdominal or lumbarpain. Patients with aorto-enteric fistulas developgastrointestinal bleeding. Blood culture and peri-prosthetic drainage fluid may reveal the offend-ing organism, staphylococcus species being themost commonly implicated microbiologicalagent. CT is the imaging modality of choice andfacilitates the aspiration of infected fluid for cul-ture to confirm the diagnosis and to guide treat-ment. The role of MRI has yet to be clarifiedsince, whilst it can distinguish hematoma fromperigraft fluid and inflammatory changes in thepostoperative cases, images may well be too badly
COMPLICATIONS OF AORTO-ILIAC INTERVENTION 181
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 181

degraded by the presence of metallic stents.16
Radionuclide studies such as technetium orindium labelled leucocyte scanning are highly sen-sitive but relatively non-specific, and are there-fore usually reserved for those instances in whichimaging studies do not confirm or exclude thediagnosis of infection.17
ENDOVASCULAR, SURGICAL, AND MEDICALTECHNIQUES TO RESOLVE COMPLICATIONS
Some basic rules should be applied to limit thedevelopment of complications:
1. Interventionists should be trained appropri-ately, have sufficient work load to maintaincompetence, and continue with postgraduateeducation to justify their practice. Practi-tioners should be aware of their own andtheir unit’s limitations.
2. Heparin immediately after arterial accesswill limit thrombosis on the catheters, wires,devices, and treatment site.
3. Balloons should be sized appropriately toavoid rupture.
4. Stents should be sized appropriately toavoid misplacement.
5. To limit embolization, iliac occlusions shouldbe stented without predilatation.
6. The guidewire should not be removedacross the lesion until a decision has beenmade to stop the procedure.
7. Pain during dilatation indicates that furtherstretching may result in rupture.
It is our practice to treat the specific complica-tions in the following way.
Acute closure
• As indicated previously, the majority ofacute closures of the treatment site are dueto either recoil or dissection.
• The patient should be sufficiently anticoag-ulated so that fresh thrombus does not format the closure site.
• Vessel recoil is simply managed by theplacement of a stent in the usual manner.
• A small dissection flap is part of the angio-plasty process and when there is no impe-diment to flow does not require treatment.
A retrograde dissection formed by guide-wire manipulation often does not impedeflow and is not significant.
• Antegrade dissection is more harmful whenblood flow keeps the false lumen open,resulting in a hemodynamic problem.
• If the dissection in the iliac vessels is flowlimiting, it is best treated by a bolus ofheparin to limit thrombus formation (e.g.5000 IU) and immediate stent placement(Figure 11.3). Dissection may extend beyondthe treatment site such that careful angiog-raphy is required to define the extent priorto stent placement.
• Basic good interventional technique requiresthat the interventionist maintains a guide-wire across the treatment site until a decisionto stop has been reached. By doing so thereis always access to pursue further interven-tion or treat complications. If the guidewirehas been removed before the dissection isdiscovered it can be very difficult to recrossthe dissection site because the wire often per-sistently tracks back into the false lumen. Onthis occasion the dissection may be best tra-versed from the contralateral limb. If the dis-section involves the common femoral arteryalone or in combination with iliac artery dis-section then surgery may be required to com-pletely resolve the problem.
Delayed closure
The degree of resulting ischemia will determinethe nature and haste of intervention. If thepatient has a white acutely ischemic limb thenthere is little time for thrombolysis and immedi-ate surgical intervention is required. If the limbis acutely ischemic, but not white, and examina-tion would indicate that immediate interventionis not required then immediate heparinization tolimit clot formation with urgent endovascularintervention is reasonable. If the ipsilateral com-mon femoral artery was patent on ultrasoundthen this should be used for access. Angiogra-phy will confirm an acutely occluded iliac seg-ment and any fresh thrombus can be removedby aspiration, thrombolysis, mechanical throm-bectomy, or balloon embolectomy. Once theoffending lesion has been revealed this needs
182 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 182

appropriate intervention with either further bal-loon dilatation or stent placement. Some recentevidence would suggest that fresh occlusionsmay be treated by direct stent placement withoutthe need to initially remove the thrombus.18 Ifthe ipsilateral common femoral artery is occludedon ultrasound thrombosis is likely to be exten-sive and further imaging should be obtained,either by angiography from the contralateral sideor Computerised Tomographic Angiography(CTA)/Magnetic Resonance Angiography (MRA).The extent of thrombosis will then determinewhether endovascular or conventional surgicalrevascularization is required.
If the patient is asymptomatic or a claudicantit may be unreasonable to immediately intervenegiven the risks of thrombolysis or embolizationwhen dealing with fresh thrombus. In this situa-tion we delay any further intervention for sev-eral months. This allows the thrombus to matureand then a clinical decision can be taken as towhether intervention is required.
Arterial rupture
This is a clinical emergency. Once the clinicaldiagnosis has been made the patient should have:(a) rapid blood volume replacement (crystalloid
followed by colloid), (b) tamponade of the rup-ture by gently inflating a balloon across or proxi-mal to the tear, (c) reversal of anticoagulation, (d)analgesia. Once the clinical picture is stabilizedthen a covered stent should be placed across therupture site19,20 (Figure 11.4). Our preference is fora self-expanding stent graft since it makes littlesense to further increase the size of the hole byforcefully deploying a balloon-mounted stent.
Distal embolization
The decision as to whether to intervene dependsupon the mode of presentation. If, for example,the embolization was found to affect a single tib-ial vessel leaving two patent crural arteries with-out any clinical features of acute ischemia itcould reasonably be argued that no active inter-vention is required and the patient should simplybe given 24 hours’ anticoagulation to limit exten-sion of the thrombus. If, however, the embolusresulted in acute ischemia then active interven-tion is required following immediate anticoagula-tion. The nature of intervention will depend uponthe site of the embolus and local expertise. A com-mon femoral embolus is easily removed surgi-cally. We would treat more distal embolization bypercutaneous aspiration thromboembolectomy,
COMPLICATIONS OF AORTO-ILIAC INTERVENTION 183
(a) (b)
Figure 11.3 (a) Extensive dissection of the left iliac artery during a difficult femoral puncture. (b) Flow-limiting dissectionhas been successfully treated by insertion of a stent in the left external iliac artery.
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 183

which has a 90% success rate.21 Initially the punc-ture needs to be reversed into an antegrade posi-tion. Alternatively a separate puncture can bemade, but this provides two large holes to sub-sequently bleed from. A large bolus of heparinis then given (5000–7500 IU) to restrict furtherthrombosis. A wide-bore single endhole catheter(typically a 7–9 Fr guide catheter) is then placedipsilaterally and the embolus is removed by suc-tion. A removable valve is useful in preventingthe embolus from getting dislodged as it passesthrough the valve. If aspiration fails then we referpatients for surgical embolectomy because it isunlikely that thrombolysis will remove emboliconsisting of plaque.
Stent infection
Until there are data to the contrary, it seems sen-sible that an artery infected by a foreign bodyrequires removal. It is therefore our policy thatpatients receive antibiotics followed by appropri-ate surgery. The infrequency of this complicationand the problems associated with the overuse of
antibiotics in hospital practice mean that we donot routinely give antibiotic cover for simple iliacstent procedures.
CHECK LIST FOR EMERGENCY EQUIPMENT
Any responsible catheter laboratory performingintervention will have a range of balloons andstents to manage many of the complicationsdetailed. In addition, there should be the equip-ment available that will salvage an acute limb orlife-threatening complication. Such basics shouldinclude:
• resuscitation trolley with staff capable ofusing it
• covered stents WallgraftTM (Boston Scientific)or FluencyTM (CR Bard, Inc, Murray Hill, NJ)
• thrombolytic agents and mechanical throm-bectomy devices
• aspiration thromboembolectomy catheters(we recommend Cordis bright-tip 7–9 Frguide catheters and removable hemostaticvalves).
184 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b) (c)
Figure 11.4 (a) Extravasation of contrast medium secondary to iliac rupture noticed immediately following placement ofiliac stent. (b) Balloon tamponade whilst getting ready for placement of a covered stent. (c) Successful treatment of therupture with a covered stent.
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 184

REFERENCES
1. Gaines P, Moss JG et al. The British Society of Inter-ventional Radiology second BIAS report. Henley-on-Thames, Oxfordshire: Dendrite Clinical Systems Ltd,2005.
2. Bosch JL, Hunink MG. Meta-analysis of the results ofpercutaneous transluminal angioplasty and stent place-ment for aortoiliac occlusive disease. Radiology 1997;204(1): 87–96.
3. Tetteroo E, van der Graaf Y, Bosch JL et al. Randomisedcomparison of primary stent placement versus primaryangioplasty followed by selective stent placement inpatients with iliac-artery occlusive disease. Dutch IliacStent Trial Study Group. Lancet 1998; 351(9110): 1153–9.
4. Gardiner GA Jr, Meyerovitz MF, Stokes KR et al.Complications of transluminal angioplasty. Radiology1986; 159(1): 201–8.
5. Weibull H, Bergqvist D, Jonsson K et al. Complicationsafter percutaneous transluminal angioplasty in theiliac, femoral, and popliteal arteries. J Vasc Surg 1987;5(5): 681–6.
6. Schubart PJ. Arterial complications associated with theuse of balloon catheters. In: Bernhard VM, Towne JB,eds. Complications in Vascular Surgery, 2nd edn. NewYork: Grune & Stratton, 1985: 87–109.
7. Chalmers N, Eadington DW, Gandanhamo D et al. Casereport: infected false aneurysm at the site of an iliacstent. Br J Radiol 1993; 66(790): 946–8.
8. Fiorani P, Speziale F, Calisti A et al. Endovascular graftinfection: preliminary results of an international enquiry.J Endovasc Ther 2003; 10(5): 919–27.
9. Belli AM, Cumberland DC, Knox AM et al. The compli-cation rate of percutaneous peripheral balloon angio-plasty. Clin Radiol 1990; 41(6): 380–3.
10. Hawthorn IE, Rochester J, Gaines PA et al. Severe lowerlimb ischaemia with pulses: cholesterol embolisation –a little known complication of aortic surgery. Eur J VascSurg 1993; 7(4): 470–4.
11. Gaines PA, Cumberland DC, Kennedy A et al.Cholesterol embolisation: a lethal complication of vas-cular catheterisation. Lancet 1988; 1(8578): 168–70.
12. Lois JF, Takiff H, Schechter MS et al. Vessel rupture byballoon catheters complicating chronic steroid therapy.Am J Roentgenol 1985; 144(5): 1073–4.
13. Smith JC, Watkins GE, Taylor FC et al. Angioplasty orstent placement in the proximal common iliac artery: isprotection of the contralateral side necessary? J VascInterv Radiol 2001; 12(12): 1395–8.
14. Gaines PA, Cumberland DC. Wire-loop technique forangioplasty of total iliac artery occlusions. Radiology1988; 168(1): 275–6.
15. Criado FJ, Wilson EP, Abul-Khoudoud O et al. Brachialartery catheterization to facilitate endovascular graft-ing of abdominal aortic aneurysm: safety and rationale.J Vasc Surg 2000; 32(6): 1137–41.
16. Modrall JG, Clagett GP. The role of imaging techniquesin evaluating possible graft infections. Semin Vasc Surg1999; 12(4): 339–47.
17. Orton DF, LeVeen RF, Saigh JA et al. Aortic prostheticgraft infections: radiologic manifestations and implica-tions for management. Radiographics 2000; 20(4): 977–93.
18. Duc SR, Schoch E, Pfyffer M et al. Recanalization of acuteand subacute femoropopliteal artery occlusions withthe rotarex catheter: one year follow-up, single centerexperience. Cardiovasc Interv Radiol 2005; 28(5): 603–10.
19. Formichi M, Raybaud G, Benichou H et al. Rupture ofthe external iliac artery during balloon angioplasty:endovascular treatment using a covered stent. J Endo-vasc Surg 1998; 5(1): 37–41.
20. Allaire E, Melliere D, Poussier B et al. Iliac artery ruptureduring balloon dilatation: what treatment? Ann VascSurg 2003; 17(3): 306–14.
21. Cleveland TJ, Cumberland DC, Gaines PA. Percutaneousaspiration thromboembolectomy to manage the emboliccomplications of angioplasty and as an adjunct tothrombolysis. Clin Radiol 1994; 49(8): 549–52.
COMPLICATIONS OF AORTO-ILIAC INTERVENTION 185
CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 185

CPVI_Chapter11.qxp 4/5/2007 2:48 PM Page 186

INTRODUCTION TO THE FREQUENCY ANDTYPE OF COMPLICATIONS
Peripheral arterial disease of the lower extremi-ties affects approximately 8 million people in theUnited States, causing significant morbidity, suchas claudication and pain during ambulation and,ultimately, insufficient perfusion of the distalextremities that may yield ischemic ulcerationand gangrene. It is a marker for systemic arte-riosclerosis, and mortality in patients with clau-dication is significantly higher than in controls.1
The superficial femoral artery (SFA) is thelongest artery in the body and its geometry andelasticity are noticeably affected by the surround-ing musculature and its mobility and locationbetween two joints. Significant changes in arterialblood flow characteristics are seen in patientswith peripheral arterial disease with respect tothe span between the peak positive and negativeblood flow velocity in the femoral artery2 and,overall, the SFA’s structural and functionalproperties predispose it to arteriosclerosis, calci-fication, and ulceration, and the development offibrous plaques and local thrombus.3
Initial management of patients with peripheralarterial disease includes relief of symptoms and reduction in cardiovascular risk factors and may involve antiplatelet therapy, exercise,smoking cessation, and treatment of diabetes,hyperlipidemia, and hypertension. When medical
interventions fail to ameliorate symptoms,endovascular therapy is often considered a firstline of defense. Indeed, minimally invasive ther-apies have become established techniques fortreating vascular disease; initially with the wide-spread application of balloon angioplasty,4 andfollowed by the introduction of peripheral stents5
and atherectomy techniques.6
Standard angioplasty techniques have been in use for decades, but they are generally moreappropriate in the iliac vessels – where there isgood distal run-off, and lesions are usually steno-tic rather than occlusive. The difficulty in negoti-ating femoropopliteal lesions and the potential forembolic consequences has kept many awayfrom more distal territory. Balloon angioplastyis a controlled injury to the vessel wall, causingrupture and dissection of plaque, partial dissec-tion of the intima and media, and overstretchingof the vessel wall. The intrinsic coagulation path-way is activated, and platelet adhesion and throm-bus formation are encouraged; if fibroblastscontinue to form intercellular matrices, intimalhyperplasia continues unabated.7
The femoropopliteal segment is fairly straightand in general side branches are not relevantexcept for the deep femoral artery. The deepfemoral artery’s importance in maintaining viablecirculation to the leg cannot be underestimated.Compromise of the deep femoral artery can result
12
Femoropopliteal segmentRichard R Heuser
Introduction to the frequency and type of complications • Factors identifying patients at high risk forcomplications • Complications of specific interventional steps and tools • Diagnostic methods to detectpotential complications • Endovascular, surgical, and medical techniques to resolve complications •Methods to avoid complications • Summary • Check list for emergency equipment
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 187

in a true medical emergency in patients pre-senting with severe symptoms of critical limbischemia. This problem can be obviated by eitherthe use of atherectomy devices or a kissing bal-loon technique at the site of the common femoraland deep femoral junction. Embolization alsooccurs in this patient population, but it is under-recognized and by the time it is recognized eitherlarge particles have already been expelled or thereis the blue toe syndrome. Some investigatorsworking in this region have suggested usingembolic protection devices, but this has not beenwidely embraced clinically.
Endovascular stents were introduced to pre-vent residual stenosis, elastic recoil, and flow-limiting arterial dissection following balloonangioplasty. Initial reports of stenting for occlu-sive atherosclerotic disease in the femoropoplitealsegment were encouraging, with primary andsecondary patency rates of ~90% at 18 months.8
Unfortunately, intimal hyperplasia and in-stentrestenosis have since proven to be significantproblems affecting long-term patency.9 One of theproblems in stenting in the superficial femoraland popliteal region is that with movement inthe leg, there is external compression of the stentwhich can result in fracture, restenosis, or in somecases late thrombosis. While the TransAtlanticInter-Society Consensus (TASC) recommenda-tions for femoropopliteal stent placement do notindicate it should be a primary approach to theinterventional treatment of intermittent clau-dication,10 percutaneous stent placement intofemoropopliteal arteries has become a widelyaccepted therapeutic strategy when angioplastyfails due to residual stenosis or dissection.
FACTORS IDENTIFYING PATIENTS AT HIGH RISK FOR COMPLICATIONS
In general, it appears the risk factors for develop-ment of peripheral arterial disease mirror thosethat affect the success of treatment. In a recentstudy, male gender, diabetes mellitus, and chronicrenal failure were significant independent riskfactors for distal (rather than proximal) lowerextremity arterial vascular disease, with hyper-tension nearing statistical significance (p = 0.06).11
Accordingly, patients with diabetes have a higherrate of in-stent restenosis following endovascular
procedures,12 and diastolic hypertension and thepercent stenosis may predict immediate angio-plasty failure.13 In another more recent study,however, hypercholesterolemia was less preva-lent in patients with lesions below the knee andthere was no distinct association with arterialhypertension.14 While cigarette smoking has longbeen associated with risk for peripheral arte-riosclerosis15,16 and with vessel occlusion afterdeliberate extraluminal recanalization,17 one studyindicated that smoking 10 or more cigarettes dailywas associated with a reduced rate of intermedi-ate-term restenosis after lower-limb endovascularinterventions.18 Presenting symptoms – whetherthe patient had simple claudication or criticalischemia – also predict the success of interven-tion, with poorer outcomes in severely ischemicpatients.
Immediate causes of interventional failureinclude intimal dissection, elastic recoil of the ves-sel wall, and arterial rupture. Predictors of earlyclinical failure are advanced age, SFA occlusion,and the presence of residual stenosis, dissection,or occlusion. Many factors adversely affect mid-to long-term patency, including type of lesion,and length of lesion.19–22 In general, stenoses areassociated with better patency than occlusions;thrombosis of total occlusions is not uncommonand usually occurs within hours of the procedure.As a rule, focal stenoses are easier to treat thanlong-segment lesions. In addition, treatment ofconcentric lesions is often more successful thanthat of eccentric lesions. Overall, poor distal run-off correlates with worse outcomes. The absenceof calcification, dissection, or plaque rupture asjudged by intravascular ultrasound, and a resid-ual stenosis of less than 30%, is associated withimproved outcomes.23 Restenosis due to intimalhyperplasia and progression of atherosclerosisare the most common causes of late failures.
COMPLICATIONS OF SPECIFIC INTERVENTIONAL STEPS AND TOOLS
Endovascular procedures have many advantagesover open surgery – they can be performed underlocal anesthesia, are generally well tolerated bythe patient, and are usually associated with fewercomplications and shorter hospitalization andrecovery periods than surgery – but the risks of
188 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 188

minimally invasive procedures include emboliza-tion, dissection, thrombosis, perforation, bleed-ing, atherosclerotic stenosis and occlusion, andaneurysm and arteriovenous fistula development.
Imaging
While advances in preoperative imaging modal-ities such as magnetic resonance imaging (MRA)and duplex ultrasound arterial mapping areimpressive, their superiority over contrast angiog-raphy has not been clearly demonstrated. In par-ticular, the use of MRA in the infrapoplitealsegment resulted in both false negatives and falsepositives, and duplex exams were inadequatewhen low flow or severe arterial calcificationswere identified.24 As such, angiography is usedto define the disease distribution. Most angiogra-phy is performed with iodinated contrast agents,and low-osmolar agents are often used in periph-eral arterial studies to minimize discomfort. Theseagents carry a low risk of allergic reaction andvolume overload; however, renal toxicity variesaccording to patient characteristics, and thosewith renal insufficiency may require alternativecontrast.
Puncture site
Catheter-based angiography of the arterial systemis generally performed via the common femoralartery. Interventionists involved with treatingsuperficial femoral, deep femoral, or popliteal dis-ease, or below, should be widely familiar with theantegrade approach. The antegrade approachcan be difficult in obese patients and also can bedifficult with an inexperienced operator. Com-plications that can occur with antegrade passagecan be dissection, retroperitoneal hematoma, aswell as a possibility of an AV fistula or pseudo-aneurysm following the procedure. The con-tralateral approach is also an excellent and safeapproach in treating patients with SFA orpopliteal disease; however, this can be difficultwhen a patient has a very tortuous aorto-iliacjunction or if the patient is status postendolumi-nal grafting. The radial approach in patientswith femoral and popliteal disease is difficult,not because of technique but because of the lackof availability of long catheters, stents, etc.
Experience with the popliteal puncture tech-nique is essential when performing interventionsin this segment. Our experience with the poplitealapproach is to direct the needle by a contralateralsmall catheter injection with roadmapping tech-niques. This technique makes it possible for us tohave less likelihood of hematoma, dissection, etc.as we place the sheath. The risks of the techniqueinclude serious puncture site complications and,since the deep or superficial femoral artery lacksthis bony support, hemostasis may be difficult toachieve during arterial compression after catheterremoval if the puncture site is distal to thecommon femoral artery (Figure 12.1). Figure 12.2shows the same vessel after treatment with anatherectomy device (SilverHawkTM, FoxhollowTechnologies, Redwood City, CA); the patient’sankle brachial indices (ABIs) improved from 0.68to 1.02.
Wire passage
Passage of wires into the infrapopliteal regionmay initiate spasm and subsequent thrombosisin these small, sensitive vessels. Multiple lesionsshould be approached in a distal-to-proximalfashion.
FEMOROPOPLITEAL SEGMENT 189
Figure 12.1 This arteriogram of the right iliac and femoralartery depicts the stenosis in the right common femoralartery at the site of previous closure.
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 189

Ballooning/stenting
We still minimize stent usage in the infrapoplitealregion. Overinflation may be associated with rup-ture of theballoon catheter, while the use of over-sized balloons relative to the reference segmentmay also cause injury to the vessel wall. Abruptclosure is commonly caused by dissection from bal-loon angioplasty with superimposed thrombosis. Itoccurred in 2–4% of cases with balloon angioplastyin the prestent era. Clinical features associated withincreased risk of abrupt closure include diabetesmellitus, female gender, inadequate antiplatelettherapy, and advanced age. Long lesions, totalocclusions, and the presence of multivessel dis-ease may also increase the risk of abrupt closure.Signs and symptoms include pain, pallor, pulse-lessness, paresthesias, and coldness of the ex-tremity, and are similar to those seen with stentthrombosis.
Appropriate stent sizing is imperative to thesuccess of the procedures. When a stent is toosmall, migration of the device can occur from theproximal segment of the SFA into the commonfemoral artery. Distal embolization is anothercomplication that may be stent-related or pro-duced by the balloon angioplasty procedure.
In some cases, distal embolization may be treatedby thrombectomy alone; however, thrombolyticmanagement may also be appropriate. Con-traindications to thrombolysis include recentneurologic, thoracic, or abdominal surgery, recentstroke, evidence of active gastrointestinal orgenitourinary bleeding, central nervous systemmetastatic disease, and bleeding diathesis.
The superficial course of the artery and crossing of flexion points exposes the superficial femoral andpopliteal arteries to relevant biomechanical forces,including compression, torsion, and elongation, whichmay result in stent fracture. Multiple stent deploymentand stent overlap carry a higher risk of fracture andshould be avoided. The problem was minimized withthe advent of self-expanding nitinol stents. Finally, theimpact of fracture on long-term patency of the stent hasvaried among studies, and is not very well defined yet.
Other devices
Atherectomy/debulking
Atherectomy and debulking techniques mayimprove outcome, but the risks of dissection,embolic debris, and distal embolization arenotable.25,26 Likewise, mechanical thrombectomydevices may introduce similar complications dueto embolic debris.27
Cryoplasty
Cryoplasty has been used to administer a cold-induced injury to inhibit restenosis. Complica-tions during such procedures are uncommon,but patients who undergo successful cryoplastyshould still be monitored carefully following theprocedure. Signs of complications may includesevere leg pain, pallor, and absent pulses in thepopliteal artery and dorsalis pedis. An angiogramcan demonstrate problems such as abrupt closureof the SFA, spasm, dissection, or embolism.
Laser
Early laser interventions were plagued by com-plications resulting from thermal damage to sur-rounding tissue. Today, the use of ‘cool’ tip lasershas limited such problems. However, proceduralcomplications still include acute re-occlusion,perforation, and embolization.28
190 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 12.2 This is the same vessel as in Figure 12.1after treatment with the SilverHawkTM (Foxhollow) atherec-tomy device. Note the improvement in the stenosis; thepatient’s ABIs went from 0.68 to 1.02.
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 190

DIAGNOSTIC METHODS TO DETECTPOTENTIAL COMPLICATIONS
Physical exam
The physical exam should include evaluation offemoral-popliteal pulses and palpation of the pos-terior tibial vessels and dorsalis pedis. The mea-surement of ABI is also critical.
Imaging
Although contrast arteriography remains the goldstandard for evaluation of patients undergoinglower extremity revascularization,24 recurrentlesions are often readily detected byduplex ultra-sonography. Magnetic resonance angiography(MRA), computed tomography (CT), and angiog-raphy may also be useful.
ENDOVASCULAR, SURGICAL, AND MEDICALTECHNIQUES TO RESOLVE COMPLICATIONS
Thrombolysis/aspiration
When abrupt closure and/or stent thrombosis isdetected, angiography via contralateral accessis performed to determine the site and flow is re-established using one or more of the followingapproaches: selective thrombolysis below theaccess site, mechanical thrombectomy, and/orsuction thrombectomy. In some patients, admin-istration of a thrombolytic via an infusioncatheter may not be successful in restoring ade-quate flow, and the patient may continue to havesevere symptoms. Ultimately, femoropoplitealbypass surgery is sometimes necessary when thedeep femoral artery and common femoral arteryare affected.
Stent migration
When stent migration is detected, usually viaDoppler and angiography, a nitinol snare may beintroduced from a contralateral femoral approachto retrieve a misplaced stent.
Coil embolization
Coil embolization is rarely, if ever, indicatedin femoral popliteal intervention. In emergent
situations, such as a bleed or rupture, these com-plications are usually treated by prolonged bal-loon inflation or the use of a covered stent(Figures 12.3 and 12.4).
FEMOROPOPLITEAL SEGMENT 191
Figure 12.3 This arteriogram illustrates a right commonfemoral arteriovenous fistula in a patient who hadundergone multiple coronary interventions in the past. The patient presented with a loud right femoral bruit and mild claudication with normal ABIs.
Figure 12.4 The arteriovenous fistula was treatedsuccessfully with a Hemobahn covered stent (WL Goreand Associates, Flagstaff AZ).
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 191

Surgical intervention
Surgical intervention is indicated when the limbis threatened, and further endovascular inter-vention is not possible (Figure 12.5).
METHODS TO AVOID COMPLICATIONS
Imaging
Renal toxicity varies according to patient charac-teristics (renal status, presence of diabetes); thosewith renal insufficiency may require alternativecontrast. Digital imaging may allow smalleramounts of contrast material to be used and reduc-tion in the radiation exposure needed for eachimage. The use of the subtraction technique withdigital imaging may further improve the con-trast resolution. Nevertheless, multiple angio-graphic views are often required to show theseverity of a stenosis, and the measurement oftranslesional pressure gradients and the use ofintravascular ultrasound may be helpful adjuncts.
Recently, duplex-guided balloon angioplastyhas been described as a safe and effective tech-nique for renal patients that allows direct visual-ization of the puncture site, accurate selection ofthe proper size of balloon and stent, confirma-tion of the adequacy of the technique by hemo-dynamic and imaging parameters, and avoidanceof radiation.29
Approach
When treating lesions below the inguinal liga-ment, a contralateral retrograde or an ipsilateralantegrade access may be used. The contralateralapproach is often preferable because it avoidspotential complications such as dissection orhematoma formation that are sometimes seenwith the ipsilateral antegrade approach; also theantegrade approach is awkward and technicallychallenging for most catheterization labs. Theradial approach, though generally easier to per-form, is somewhat restrictive because many bal-loons, atherectomy devices, and stents are simplytoo short. Multiple lesions should be treated ina distal-to-proximal fashion.
Stent choice
Although balloon-expandable stents provideaccurate sizing, self-expanding stents are pre-ferred in the femoropopliteal region because oftheir flexibility and resistance to external forcesin superficial locations. Substantial flexing, suchas that occurring at a joint, may lead to compres-sion or kinking; using the shortest device possiblemay help avoid complications. The use of self-expanding nitinol stents appears to improvepatency.30,31 Stent compression and fracture,though reduced with self-expanding nitinolstents, are still risks when treating long lesions32
(Figures 12.6–12.9).The use of coil-shaped stents inside the treated
vessel may reduce local trauma by limiting thearea of the arterial wall covered by the stent, andself-expandable coil stents are often suitable fortortuous arteries and lesions of the femoral orpopliteal artery situated at flexion points or atlocations that may be subjected to external com-pression. Despite these merits, coil stents are not
192 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 12.5 This arteriogram of the left common femoralartery and bifurcation delineates a patient with a limb atrisk. Note the thrombotic occlusion at the bifurcation ofthe deep femoral artery. This patient will need immediaterevascularization, either percutaneously or via open surgery,otherwise, he will likely lose at least part of his limb.
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 192

FEMOROPOPLITEAL SEGMENT 193
(a) (b) (c)
(d) (e) (f)
Figure 12.6 (a) The angiogram shows multiple in-stent restenosis. (b) The native frame indicates that the stenoses arecorrelated to stent fractures. (c) After in-stent placement of a nitinol stent, and focal post-dilation with a 6/20 mmballoon (d–f), a good angiographic result could be achieved. From Heuser and Biamino, eds. Peripheral Vascular Stenting.London: Taylor & Francis, 2005.
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 193

appropriate in heavily calcified and eccentriclesions; conventional balloon-expandable stentsmay still be preferable in these cases. Someinterventionists use coronary drug eluting in theinfrapopliteal region. In most cases, these stentscan still thrombose and, because of their lack of
adequate tensile strength, may be compressed;the use of such stents in this region is still highlycontroversial and, as yet, investigational.
Prevention of stent thrombosis/distalembolization
The vascular biological response to stent place-ment in the peripheral circulation may be similarto that in the coronary circulation and, thus, thesame antiplatelet regimens used in the coronaryvessels are used in peripheral vascular stenting.Clopidogrel has replaced ticlopidine as a drug toprevent stent thrombosis in most centers becauseit is more easily administered and is generallyconsidered to have a safer hematologic profile.We currently prescribe 4 weeks of clopidogrelfollowing superficial femoral artery stenting,and aspirin is continued indefinitely.
Embolic protection devices have been used forsome time in percutaneous interventions in thecoronary and carotid arteries. More recently, filterand balloon occlusion devices have been used in
194 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
Figure 12.7 Balloon-expandable stent deformed by flexionat the groin. From Heuser and Henry, eds. Textbook ofPeripheral Vascular Interventions. London: Martin Dunitz,2004.
(a) (b)
Figure 12.8 (a) Thrombosed Palmaz® stent in the superficial femoral artery. (b) A different angle shows thepresence of pressure deformity of the stent. From Heuserand Henry, eds. Textbook of Peripheral VascularInterventions. London: Martin Dunitz, 2004.
Figure 12.9 This arteriogram illustrates a commonproblem in patients treated with femoral stents for a longocclusion in the SFA. New technology may reduce the re-occlusion rate in these patients.
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 194

the femoral and popliteal arteries to capture dis-lodged thromboembolic material during angio-plasty and stenting procedures placement – earlyresults (n = 5) indicate no apparent difficulties inplacing the devices and that all devices wereretrieved with substantial debris.26 Additionalstudy of both filter-type and balloon occlusiondevices appears warranted.
Prevention of restenosis
It has been suggested that debulking of lesionsmay enhance patency, and atherectomy and endo-vascular endarterectomy have been used in anattempt to improve outcomes (as seen previ-ously in Figures 12.1 and 12.2). The SilverHawkTM
coaxial system incorporating cutting and storagechambers (Foxhollow Technologies) has beenstudied in a registry, and there are early reportsof success in debulking short- and medium-lengthfemoropopliteal lesions.33 However, while thedevice’s debulking capabilities are not at issue,at least one investigative group urges caution,citing a notable risk of dissection, embolic debris,and distal embolization.26 Results with a mechan-ical thrombectomy device (Rotarex, StraubMedical, Wangs, Germany) have also beenreported, indicating successful treatment of acute,subacute, or chronic peripheral arterial throm-boembolic occlusions.27 However, the investiga-tors caution the device is not recommended foruse in heavily calcified lesions, and note that dis-tal embolizations occurred in 10 of 48 patients;six clinically relevant emboli required aspirationin this series.
Medical therapies aimed at interrupting orinhibiting intimal hyperplasia include heparin,low-molecular-weight heparin, aspirin, corti-coids, angiotensin-converting enzyme inhibitors,vascular endothelial growth factor, cyclosporin,and other agents. Use of preprocedural aspirinhas been shown to reduce abrupt closure dur-ing intervention. Traditionally, unfractionatedheparin has been used to prevent thromboticcomplications in peripheral interventions, butthe level of activated clotting time is not welldefined. Generally, a level of greater than 300seconds in the absence of a IIb/IIIa inhibitor hasbeen adopted in most centers. The effects ofadjunctive administration of abciximab have been
reported to have a favorable effect on patency andclinical outcome in patients undergoing complexfemoropopliteal catheter interventions with treat-ment effects of abciximab maintained at 6-monthfollow-up in one study.34 Observational studieswith the direct thrombin inhibitor, bivalarudin,indicate that it is safe, effective, and might offersome advantages over heparin such as earlysheath removal and possibly a lower major bleed-ing rate.35
The sirolimus-eluting stent (Cordis Endo-vascular, Miami Lakes, FL) was studied in theSIROCCO trials – most recently, investigatorsreported a trend for greater efficacy in thesirolimus-eluting stent group but there were nostatistically significant differences in any of thevariables between the bare and sirolimus-elutingstent groups.
Laser-assisted angioplasty has been shown tobe useful in recanalizing long SFA occlusions;however, maintaining patency and quality of lifehas been reported to require intensive surveil-lance and prompt repeat intervention.36 Steinkampand colleagues37 noted that, while initial recanal-ization was more successful with laser-assistedangioplasty, it did not appear to add any long-term benefit over balloon dilatation alone. Morerecently, a review of data from the Laser Angio-plasty for Critical Limb Ischemia (LACI) phase 1and 2 trials suggests excimer laser-assisted angio-plasty is a viable treatment strategy for patientswith critical limb ischemia who are otherwise notgood candidates for bypass surgery and havelimited options for other treatment.28
Endovascular radiotherapy in the endolumenof the femoropopliteal segment following per-cutaneous transluminal angioplasty has beenreported to prevent intimal hyperplasia in femo-ropopliteal arteries and improve patency insome studies.38,39 While these improvements inpatency rates after brachytherapy are encourag-ing, further study indicated endovascular bra-chytherapy did not diminish early vascularinflammation in response to angioplasty orstent implantation, and even induced a trendtoward an increased inflammatory response; theinvestigators concluded reduced rates of resteno-sis after brachytherapy cannot be explained byan anti-inflammatory radiation effect.40 Morerecently, it has been reported that while there
FEMOROPOPLITEAL SEGMENT 195
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 195

appear to be positive short-term effects of adjunc-tive endovascular brachytherapy, these are notsustained in the longer term and there is no sub-stantial clinical improvement in de novo or recur-rent femoropopliteal lesions at up to 5 years.41
Cryoplasty incorporates conventional balloonangioplasty and the currently available device(CryoVascular Systems, Los Gatos, CA) uses adouble balloon that administers a cold-inducedinjury at 6–8 atm of pressure. In a total of 102patients (of whom 31% were each diabetic andactive cigarette smokers), the technical successrate was 85.3% with a mean residual stenosisafter cryoplasty of 11.2% ± 11.2% (p < 0.05 vsbaseline). Clinical patency in this group was>80% during the 9-month surveillance period;primary patency determined by duplex US was70.1%.42
While results in the femoropopliteal region arenot yet available, intracoronary sonotherapy fol-lowing angioplasty has been performed usingserial ultrasound transducers operating at 1 MHz.Sonotherapy was applied safely and with highacute procedural success, but late lumen loss andneointimal growth were similar to conventionalPTCA approaches.43
Photodynamic therapy using up to 50 J/cm2
red light (635 nm) was delivered to the angio-plasty site via a laser fiber within the balloon in7 patients who had previously undergone con-ventional angioplasty at the same site and hadsymptomatic restenosis or occlusion between 2and 6 months.44 Outcome by duplex imagingindicated the median (interquartile range) peaksystolic velocity ratio across stenotic segmentswas 4.7 (3.7–5.7) before angioplasty and 1.4(1.0–1.8) at 6 months after intervention (p = 0.04)in this small group. At a mean of 48 months,none of the patients had critical limb ischemia orulceration and there were no arterial complica-tions; one developed mild, non-limiting claudi-cation 18 months after photodynamic therapy.45
SUMMARY
Peripheral arterial disease is a common maladyin aging populations that causes significant mor-bidity. The structural and functional propertiesof the distal arteries predispose them to arterioscle-rosis, calcification, and ulceration, and when risk
factor modification and medical interventionfail to improve symptoms of claudication and/or ischemia, endovascular therapy is often con-sidered. Although the TASC recommendationsfor femoropopliteal stent placement do not indi-cate it should be a primary approach to the inter-ventional treatment of intermittent claudication,stent placement for femoropopliteal arterial dis-ease is widely accepted to prevent residualstenosis, elastic recoil, and flow-limiting arterialdissection following balloon angioplasty. Stentprocedures have many advantages over opensurgery as they employ local anesthesia, aregenerally well tolerated, and result in shorterhospitalization and recovery periods. Neverthe-less, risks of minimally invasive proceduresinclude embolization, dissection, thrombosis, per-foration, bleeding, atherosclerotic stenosis andocclusion, and aneurysm and arteriovenousfistula development.
One of the questions many interventionistshave is when is it time to stop. In other words,when you have a dissection or a complicationwhen is the best time to decide to go back andtreat the patient at another time or considerreferral to surgery. It has been our experience inthe antegrade approach or the contralateralapproach to the SFA when the vessel is totallyoccluded or has a complex stenosis, that if there isa significant dissection that is not flow limitingor compromising the deep femoral artery and wehave been working to try to enter the true lumenfor a significant amount of time, this might bethe time to abandon the procedure. This patientmight be best served by coming back; the proce-dure can then be attempted via the poplitealapproach to more effectively treat this compli-cated lesion. We found this approach results inless radiation, less risk to the patient, and ahigher degree of success. This may also be a timeto share with a vascular surgical colleague theconsideration for the surgical approach or per-haps consider a referral to a more experiencedinterventionist. This would particularly be thecase with a thrombotic, calcific, or very resistantlesion. Some interventionists will consider bypasson a younger patient with this histopathology,particularly when there appears to be adequaterun-off and the vessel is occluded over a longdistance or heavily calcified.
196 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 196

Proper patient selection and appropriate imag-ing and selection of devices and adjuvant thera-pies are important determinants of the successof percutaneous interventions. Contrast arteri-ography remains the gold standard for evaluationof patients undergoing lower extremity revascu-larization, and self-expanding stents are preferredin the femoropopliteal region because of theirflexibility and resistance to external forces insuperficial locations. Medical therapy that limitsthe potential for embolization and thrombosis isan important adjunct, and embolic protectiondevices are beginning to be used in the femoraland popliteal arteries to capture dislodgedthromboembolic material during procedures.Prevention and treatment of restenosis, which isby far the most common complication of percu-taneous interventions, currently includes theuse of a variety of adjunctive therapies, includingdrug-eluting stents, local antiproliferative drugsgiven intraprocedurally, sonotherapy, photody-namic angioplasty, radiation therapy, and cry-oplasty. Most of these treatments are in therelatively early stages of development and testing,and it is not yet clear whether lasting protectionagainst restenotic lesions will be afforded. Atpresent, clinicians frequently rely on more thanone mode of therapy to treat critical ischemia andreduce the need for amputation in patients witharterial disease in the femoropopliteal segment.
Overall, the interventionist considering en-dovascular intervention in the femoropoplitealregion must be comfortable using contralateraland popliteal approaches and an antegrade sticktechnique. In addition, he or she must have expe-rience removing emboli and be skilled using avariety of wires, stents, and snares; filter deviceexperience may be useful as well. A close rela-tionship with a vascular surgeon is essential inmanaging complications such as vascular dis-section and perforation.
CHECK LIST FOR EMERGENCY EQUIPMENT
Emergency equipment that should be availablefor work in the femoral popliteal area includethe availability of coils for perforations, coveredstents, and an open mind to be able to think onyour feet. Sometimes interventionists let their egoget in the way, but a thoughtful approach with
the consideration of the patient first is always animportant policy.
• covered stent• coils• aspiration thrombectomy catheter• snares• thrombolytics.
REFERENCES
1. American Heart Association. Heart Disease and Stroke Sta-tistics – 2006 Update. Dallas, Texas. http://circ.ahajournals.org/cgi/content/abstract/CIRCULATIONAHA.105.171600v1 Accessed 18 January 2006.
2. Nesbitt E, Schmidt-Trucksass A, Il’yasov KA et al.Assessment of arterial blood flow characteristics in nor-mal and atherosclerotic vessels with the fast Fourierflow method. MAGMA 2000; 10: 27–34.
3. Davies MG, Waldman DL, Pearson TA. Comprehensiveendovascular therapy for femoropopliteal arterial ath-erosclerotic occlusive disease. J Am Coll Surg 2005; 201:275–96.
4. Gruentzig AR. Percutaneous transluminal coronaryangioplasty. Semin Roentgenol 1981; 16: 152–3.
5. Sigwart U, Puel J, Mirkovitch V. Intravascular stents toprevent occlusion and restenosis after transluminalangioplasty. N Engl J Med 1987; 316: 701–6.
6. Simpson JB, Selmon MR, Robertson GC et al. Trans-luminal atherectomy for occlusive peripheral vasculardisease. Am J Cardiol 1988; 61: 96–101G.
7. Lammer J. Femoropopliteal artery obstructions: fromthe balloon to the stentgraft. Cardiovasc Interv Radiol2001; 24: 73–83.
8. Henry M, Amor M, Beyar I et al. Clinical experiencewith a new nitinol self-expanding stent in peripheralartery disease. J Endovasc Surg 1996; 3: 369–79.
9. Gray BH, Sullivan TM, Childs MB et al. High incidenceof restenosis/reocclusion of stents in the percutaneoustreatment of long-segment superficial femoral arterydisease after suboptimal angioplasty. J Vasc Surg 1997;25: 74–83.
10. Dormandy JA, Rutherford RB. Management of periph-eral arterial disease (PAD), TASC Working GroupTransAtlantic Inter-Society Consensus (TASC). J VascSurg 2000; 31(Suppl): S1–296.
11. Rafetto JD, Montgomery J, Eberhardt et al. Differencesin risk factors for lower extremity arterial occlusive dis-ease. J Am Coll Surg 2005; 201: 918–24.
12. Abizaid A, Kornowski R, Mintz GS et al. The influenceof diabetes mellitus on acute and late outcomes follow-ing coronary stent implantation. J Am Coll Cardiol 1998;32: 584–9.
FEMOROPOPLITEAL SEGMENT 197
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 197

13. Dalsing MC, Cockerill E, Deupree R et al. Outcome pre-dictors in selection of balloon angioplasty or surgeryfor peripheral arterial occlusive disease, VeteransAdministration Cooperative Study No. 199. Surgery1991; 110: 636–43.
14. Diehm N, Shang A, Silvestro A et al. Association of car-diovascular risk factors with pattern of lower limb ath-erosclerosis in 2659 patients undergoing angioplasty.Eur J Vasc Endovasc Surg 2006; 31: 59–63.
15. Kannel WB, Higgins M. Smoking and hypertension aspredictors of cardiovascular risk in population studies.J Hypertens Suppl 1990; 8: S3–8.
16. Hiatt WR, Hoag S, Hamman RF. Effect of diagnosticcriteria on the prevalence of peripheral arterial disease:the San Luis Valley Diabetes Study. Circulation 1995;91: 1472–9.
17. London NJ, Srinivasan R, Naylor AR et al. Subintimalangioplasty of femoropopliteal artery occlusions: thelong term results. Eur J Vasc Surg 1994; 8: 148–55.
18. Schillinger M, Exner M, Mlekusch W et al. Effect ofsmoking on restenosis during the 1st year after lower-limb endovascular interventions. Radiology 2004; 231:831–8.
19. Matsi PJ, Manninen HI, Vanninen RL et al.Femoropopliteal angioplasty in patients with claudica-tion: primary and secondary patency in 140 limbs with1–3 year follow up. Radiology 1994; 191: 727–33.
20. Hunink MG, Wong JB, Donaldson MC et al. Revas-cularization for femoropopliteal disease; a decision andcost-effectiveness analysis. JAMA 1995; 274: 165–71.
21. Strecker EP, Boos IB, Gottmann D. Femoropoplitealartery stent placement: evaluation of long-term success.Radiology 1997; 205: 375–83.
22. Clark TW, Groffsky JL, Soulen MC. Predictors of long-term patency after femoropopliteal angioplasty: resultsfrom the STAR registry. J Vasc Interv Radiol 2001; 12:923–33.
23. Vogt KC, Just S, Rasmussen JG et al. Prediction of out-come after femoropopliteal balloon angioplasty byIVUS. Eur J Vasc Endovasc Surg 1997; 13: 563–8.
24. Hingorani A, Ascher E, Markevich N et al. A compari-son of magnetic resonance angiography, contrast arteri-ography, and duplex arteriography for patients undergoinglower extremity revascularization. Ann Vasc Surg 2004;18: 294–301.
25. Wholey MH, Suri R, Potoak D et al. Plaque excision in2005 and beyond: issues of the past have yet to beresolved. Endovasc Today, August 2005: 40–4.
26. Wholey MH, Toursarkissian B, Postoak D et al. Earlyexperience in the application of distal protectiondevices in treatment of peripheral vascular disease ofthe lower extremities. Cathet Cardiovasc Interv 2005;64: 227–35.
27. Duc SR, Schoch E, Pfyffer M et al. Recanalization ofacute and subacute femoropopliteal artery occlusions
with the rotarex catheter: one year follow-up, singlecenter experience. Cardiovasc Interv Radiol 2005; 28:603–10.
28. Laird Jr JR, Reiser C, Biamino G et al. Excimer laserassisted angioplasty for the treatment of critical limbischemia. J Cardiovasc Surg (Torino) 2004; 45: 239–48.
29. Ascher E, Marks NA, Schutzer RW et al. Duplex-guided balloon angioplasty and stenting for femoro-popliteal arterial occlusive disease: an alternative inpatients with renal insufficiency. J Vasc Surg 2005; 42:1108–13.
30. Lugmayr HF, Holzer H, Kastner M et al. Treatment ofcomplex atherosclerotic lesions with nitinol stents inthe superficial femoral and popliteal arteries: a midtermfollow-up. Radiology 2002; 222: 37–43.
31. Sabeti S, Schillinger M, Amighi A et al. Primarypatency of femoropopliteal arteries treated with nitinolversus stainless steel self-expanding stents: propensityscore-adjusted analysis. Radiology 2004; 232: 516–21.
32. Scheinert D, Scheinert S, Sax J et al. Prevalence and clin-ical impact of stent fractures after femoropoplitealstenting. J Am Coll Cardiol 2005; 45: 312–15.
33. Zeller T, Rastan A, Schwarzwalder U et al. Percutaneousperipheral atherectomy of femoropopliteal stenosesusing a new-generation device: six-month results froma single-center experience. J Endovasc Ther 2004; 11:676–85.
34. Dorffler-Melly J, Mahler F, Do DD et al. Adjunctiveabciximab improves patency and functional outcome inendovascular treatment of femoropopliteal occlusions:initial experience. Radiology 2005; 237: 1103–9.
35. Katzen BT, Ardid MI, MacLean AA et al. Bivalirudin asan anticoagulation agent: safety and efficacy in periph-eral interventions. J Vasc Interv Radiol 2005; 16: 1183–7.
36. Scheinert D, Laird JR Jr, Schroder M et al. Excimerlaser-assisted recanalization of long, chronic superficialfemoral artery occlusions. J Endovasc Ther 2001; 8:156–66.
37. Steinkamp HJ, Rademaker J, Wissgott C et al. Percuta-neous transluminal laser angioplasty versus balloondilation for treatment of popliteal artery occlusions. J Endovasc Ther 2002; 9: 882–8.
38. Minar E, Pokrajac B, Maca T et al. Endovascularbrachytherapy for prophylaxis of restenosis afterfemoropopliteal angioplasty: results of a prospective,randomized study. Circulation 2000; 102: 2694–9.
39. Krueger K, Landwehr P, Bendel M et al. Endovasculargamma irradiation of femoropopliteal de novo stenosesimmediately after PTA: interim results of prospectiverandomized controlled trial. Radiology 2002; 224:519–28.
40. Schillinger M, Mlekusch W, Wolfram RM et al.Endovascular brachytherapy: effect on acute inflamma-tory response after percutaneous femoropopliteal arter-ial interventions. Radiology 2004; 230: 556–60.
198 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 198

41. Diehm N, Silvestro A, Do DD. Endovascular brachyther-apy after femoropopliteal balloon angioplasty fails toshow robust clinical benefit over time. J Endovasc Ther2005; 12: 723–30.
42. Laird J, Jaff MR, Biamino G et al. Cryoplasty for thetreatment of femoropopliteal arterial disease: results ofa prospective, multicenter registry. J Vasc Interv Radiol2005; 16: 1067–73.
43. Regar E, Thury A, van der Giessen WJ et al. Sonother-apy, antirestenotic therapeutic ultrasound in coronary
arteries: the first clinical experience. Cathet CardiovascInterv 2003; 60: 9–17.
44. Jenkins MP, Buonaccorsi GA, Raphael M et al. Clinicalstudy of adjuvant photodynamic therapy to reducerestenosis following femoral angioplasty. Br J Surg 1999;86: 1258–63.
45. Mansfield RJ, Jenkins MP, Pai ML et al. Long-termsafety and efficacy of superficial femoral artery angio-plasty with adjuvant photodynamic therapy to preventrestenosis. Br J Surg 2002; 89: 1538–9.
FEMOROPOPLITEAL SEGMENT 199
CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 199

CPVI_Chapter12.qxp 4/5/2007 2:48 PM Page 200

INTRODUCTION TO THE FREQUENCY AND TYPE OF COMPLICATIONS WITHTIBIOPERONEAL INTERVENTIONS
Until recently, scepticism was often expressedconcerning the feasibility, effectiveness, andlong-term results of catheter revascularizationfor treatment of infrapopliteal disease. Further-more, endovascular interventions of the tibialarteries are often viewed as high risk and proneto failure, with fear of enduring the consequen-ces of a limb-threatening complication. Thereforethe accepted indication for below-knee endovas-cular interventions remains primarily the treat-ment of critical or limb-threatening ischemia,1
while isolated infrapopliteal endovascular inter-vention is rarely indicated in patients with inter-mittent claudication.2 An additional importantindication for below-knee angioplasty is toimprove run-off and subsequent long-term pat-ency after femoropopliteal angioplasty/stentingor bypass grafting.
Patients with critical limb ischemia often havemultilevel disease with multiple lesions also inthe crural vessels, with the consequence of tech-nically demanding surgical procedures requiringfemorodistal and even pedal bypasses with aperioperative mortality rate of up to 6% in these
mostly high-risk patients.3 The risks of surgeryhave led together with the improved technologyand the growing literature demonstrating theefficacy of endovascular treatment for criticallimb ischemia (CLI) to a steadily increasing appli-cation also in the infrapopliteal arteries. How-ever, experience of the interventionalist is evenmore important than in other regions of thelower leg arteries, and the infrapopliteal vascu-lar bed should definitely not be approached bythe novice endovascular interventionalist.
Patients with CLI are usually older than aver-age, have an increased prevalence of diabetes,and often have associated advanced cardiac andcerebrovascular disease. Patients with infrapop-liteal lesions alone or in conjunction with femo-ropopliteal disease are amongst those with thehighest likelihood of coronary heart disease.Furthermore, these patients usually have a lot of comorbidities, identifying them as high-riskpatients. The natural history of patients withrest pain alone carries a 5-year mortality rate ofabout 50%.
In general, the rate of complications reportedin the literature for infrapopliteal endovascularinterventions is astonishingly low concerningthese mainly high-risk patients. This may be due
13
Complications of tibioperoneal interventionsErich Minar and Lanfroi Graziani
Introduction to the frequency and type of complications with tibioperoneal interventions • Factors identifying patients at high risk for complications • Complications of specific interventional steps andtools • Methods to detect potential complications • Techniques to resolve complications • Methods toavoid complications • Summary • Check list for emergency equipment for interventions in this specificvessel area
CPVI_Chapter13.qxp 4/5/2007 2:49 PM Page 201

to a rather restrictive indication in the past andto the fact that – because of the fear of limb-threatening complications – in most institutionsthese interventions have been performed by themost experienced physician.
Complications are reported to occur in 2–6%of cases, and in most series complications atthe access site are the most common.1,4–10 Themortality rate is very low and mainly due tothe cardiovascular comorbidity. In the study bySoder et al,4 the mortality rate after infrapop-liteal balloon angioplasty was 1.8%, comparingfavorably to the mostly higher perioperativemortality rate for distal bypass surgery. Dorroset al6 studied a consecutive series of 284 patientstreated for critical limb ischemia. They observed2 (0.7%) in-hospital deaths, and 1 (0.4%) wasprocedurally related. Emergency vascular surg-ery became necessary in 3 patients (1%).
Another typical complication is developmentof transient contrast-induced acute renal failure,due to the high prevalence of diabetes in thesepatients. In the series of Dorros et al,6 20 patients(7%) developed this complication.
Arterial occlusions may occur due to dissec-tion, spasm, or distal embolization. However,the reported incidence is low, at <3%. The embo-lic occlusion of distal tibial or pedal arteriesmay severely deteriorate the already existingischemia. Arterial perforations can occur in upto 3%. These are caused either by the guidewire –inadvertent placement in a small collateral ves-sel – or at the site of angioplasty, leadingto vessel rupture in the most severe cases.Major local bleeding may cause compartmentsyndrome.
FACTORS IDENTIFYING PATIENTS ATHIGH RISK FOR COMPLICATIONS
Antegrade vascular access is generally associ-ated with an increased risk of complicationsincluding severe hematoma, retroperitonealbleeding, and errant positioning of the sheath.Since this approach is preferred by many inter-ventionalists in patients scheduled for infra-popliteal interventions, a higher rate of accesssite complications has to be expected, especiallyin obese patients and in patients with severevessel wall calcification. Diabetics are generally
at increased risk due to the presence of diffuselydiseased calcified vessels and due to diabeticnephropathy. The presence of end-stage renaldisease has not only a negative prognostic effecton the patency of endovascular interventions,but is also associated with a higher complicationrate due to the mostly unfavorable anatomicsituation with long-distance lesions and severecalcification. Since many of these patients arealso poor surgical candidates, an endovascu-lar treatment is often done as the last optiondespite this increased risk. Brosi et al11 reported nomajor periprocedural complications or in-hospitaldeaths in a series of 38 patients.
COMPLICATIONS OF SPECIFIC INTERVENTIONAL STEPS AND TOOLS
Crossing even long-distance stenoses can usu-ally be done without major problems also in theinfrapopliteal vessels. However, tibial vesselshave a significant propensity for spasm, espe-cially in younger patients without calcification.Since spasm may simulate dissection, its evalua-tion can be difficult.
The use of hydrophilic guidewires increasesthe risk of unintended subintimal passage andof perforation at the lesion site or of small collat-eral vessels. Balloon angioplasty can cause dis-section, especially in severely calcified vessels.Furthermore, an inadequate luminal openingincreases the risk of acute re-occlusion.
Stenoses and short occlusions can usually becrossed intraluminally. However, in longerocclusions subintimal recanalization may becomenecessary. The principle of this technique, pio-neered in the United Kingdom,12 is to deliber-ately create a dissection with a hydrophilicguidewire with extension of the dissection untilthe wire re-enters the patent distal artery. Theangioplasty balloon is inflated in the subintimalspace. An occlusion is considered suitable forattempted subintimal recanalization if there is a patent distal arterial segment. However, inpatients with critical limb ischemia and only oneopen distal vessel, special care has to be taken toavoid dissection beyond the distal open segmentto preserve the possibility for distal vascularsurgery in case of failed endovascular recanaliza-tion. Complications such as distal embolization
202 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter13.qxp 4/5/2007 2:49 PM Page 202

or perforation occur in approximately 5% ofcases.13 Hayes et al14 have reported that the riskof perforation is significantly increased withsubintimal angioplasty.
Treatment of proximal thrombotic or embolicocclusions with thrombolytic agents may causefurther distal embolization (see also Figure 13.2)Patients may also experience increased painduring thrombolysis caused by embolizationinto distal arteries or into muscle vessels.
Several new methods are currently underclinical investigation for recanalization of com-plex lesions or for prevention of restenosis.15
At least some of these approaches have thepotential to become established adjunctive inter-ventional methods in the infrapopliteal terri-tory. The use of the cutting balloon in theinfrapopliteal vessels was associated with a 20%rate of intimal dissection and inadequate hemo-dynamic result, necessitating use of adjunctivestenting.16 At present, they may have niche
indications such as treating ostial lesions orlesions from intimal hyperplasia.
Atherectomy devices are increasingly usedalso in the below-knee arteries. Results of treat-ment of such lesions in the TALON (TreatingPeripherals with Silverhawk: Outcomes Collec-tion) registry were reported recently.17 The rateof perforation or embolization was reported tobe low, at <2%. Zeller et al18 reported 1 (3%) pro-cedural complication, in which an intermittentocclusion of the target vessel occurred after anunsuccessful attempt to cross the lesion with theatherectomy device.
Laser-assisted angioplasty has been widelyused for treatment of critical limb ischemia.Laird et al19 have reported favorable resultswith a low complication rate. However, no datawere reported separately for the lower legarteries.
Until recently, stenting of the crural vesselswas only recommended in case of complication,
COMPLICATIONS OF TIBIOPERONEAL INTERVENTIONS 203
(a) (b) (c) (d)
Figure 13.1 (a) Angiography demonstrating a focal stenosis of the anterior tibial artery (ATA) associated with stenosis ofthe tibioperoneal trunk and short-segment occlusion of the posterior tibial and long-distance occlusion of the peronealartery. It was planned to recanalize the anterior and posterior tibial artery. (b) After angioplasty of the ATA by a monorail2.5 × 20 mm coronary-type balloon catheter, inflated at 12 atm for 180 seconds, control angiography demonstratedrupture of the vessel at the angioplasty site. (c) Inflation of a long over-the-wire balloon for 3 minutes at 6 atm. Furthercompression was done externally by suprasystolic inflation of a blood pressure cuff at the level of the perforation. (d) The control angiogram demonstrates no further contrast extravasation.
CPVI_Chapter13.qxp 4/5/2007 2:49 PM Page 203

204 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a) (b)
(c) (d)
Figure 13.2 (a) Subacute embolic occlusion of the popliteal trifurcation. (b) Treatment by aspiration thrombembolectomy.(c) Angiographic control demonstrates further embolization – due to thrombus fragmentation – in the distal anterior tibialartery. At this level the thrombus was aspirated using a 6 French coronary guiding catheter. (d) Final angiographydemonstrating an optimal result with no residual thrombus at the popliteal trifurcation and anterior tibial artery with directflow to the foot.
CPVI_Chapter13.qxp 4/5/2007 2:49 PM Page 204

COMPLICATIONS OF TIBIOPERONEAL INTERVENTIONS 205
e.g. dissection. However, recently studies havealso been published concerning stent implanta-tion for the treatment of focal infrapopliteallesions to improve long-term patency.9,20,21 Nosite-specific complications were reported. Thechoice of the appropriate stent has been unclearuntil now. While in other vascular regions self-expanding or balloon-expandable stents arerecommended, currently no clear recommen-dations can be given for the crural vessels. Dueto limited availability of self-expanding stentswith an appropriate dimension, mainly balloon-expandable coronary stents are currently used.Such balloon-expandable stents can be usedwithout problems, since the course of the tibialand peroneal arteries is relatively protected.Furthermore, until now there have been noreports concerning compression from outsideforces of a balloon-expandable stent implantedin the infrapopliteal vessels.
METHODS TO DETECT POTENTIAL COMPLICATIONS
Preinterventional angiogram is the optimalmethod to identify good candidates for endo-vascular treatment. However, even in cases ofunfavorable morphology, it is often necessary torecommend primary endovascular treatmentdue to the risks of surgery, especially in high-risk patients. An optimal angiogram of the distaltibial and crural vessels is obligatory to recog-nize patency of the distal segments and to detecta new occlusion caused by the intervention. Atthe end of the intervention, an angiogram with along series is necessary to recognize even smallperforations.
The postinterventional follow-up is primarilydone clinically for evaluation of improvementor further deterioration of limb ischemia.Control of the patency can be done by duplexsonography. However, in cases of severe calcifi-cation, morphologic judgment may be impossi-ble. In these cases one has to rely on the flowpattern in the distal tibial or pedal arteries. Inour laboratory we avoid immediate – for about 4 weeks – measurement of ankle pressure withsuprasystolic inflation of a cuff in patients withintervention in the distal lower leg arteries.
TECHNIQUES TO RESOLVE COMPLICATIONS
Dissections can effectively be treated by stentimplantation. Perforation requires temporaryballoon occlusion for a few minutes. Further-more, inflation of a blood pressure cuff in theregion of the vessel perforation can also be rec-ommended to support rapid sealing of the per-foration (see Figure 13.1). Coil embolization israrely necessary. If control angiography demon-strates further blood extravasation, implantationof a bare metal or even covered stent may becomenecessary. In case of arterial wall rupture causedby extraluminal position of the balloon or atherec-tomy devices, prolonged balloon inflation maynot be sufficient and implantation of a coveredstent is then the treatment of choice. Reversal ofthe anticoagulation should be avoided becauseof the risk of thrombotic occlusion. Distal embolicocclusions usually respond to thrombolysis(‘lacing’ of the clot may shorten the duration timeof necessary thrombolysis and support furtheraspiration) and/or aspiration thrombectomy(Figure 13.2). Some authors also recommend useof a mechanical thrombectomy device (such asthe AngioJet). In the case of persistent occlu-sion caused by atheromatous debris stent implan-tation can be recommended to re-establish flow.
METHODS TO AVOID COMPLICATIONS
Use of modern devices (fine wires and small,low-profile balloon catheters adopted fromcoronary technology) and great operator experi-ence are the best prerequisites to avoid majorcomplications.
An antegrade approach is preferred by manyinterventionalists since it is often the easiestapproach for intervention in the crural arteries.However, this increases the risk of access sitecomplications. Therefore a 4 Fr sheath should beused when simple balloon angioplasty – or eventhe placement of small stents – is planned. Thismakes subsequent hemostasis safer and simpler.In obese patients and in patients with severe cal-cification at the puncture site, the contralateralapproach should be chosen primarily. The use ofnon-kinking sheaths, guiding catheters, and low-profile balloons enables successful interventionfrom the contralateral approach in most cases.
CPVI_Chapter13.qxp 4/5/2007 2:49 PM Page 205

Furthermore, a long 5 Fr sheath can be used as aguiding catheter. The use of a distally placedguiding catheter may be of value to provideproximal support with the use of rapid exchangecatheters.
In case of technical failure with inability tocross the lesion with the guidewire, a retro-grade tibial access using a micropuncture kit is recommended as a possible alternativeapproach.22 However, this percutaneous accessrequires sufficient caliber of the anterior or pos-terior tibial artery below the ankle. Furthermore,this kind of intervention should only be tried byan experienced operator, since potential com-plications may damage the single patent run-offvessel and worsen surgical options due to lackof identifiable distal anastamotic sites. Since theinfra-popliteal arteries are sensitive to manipu-lation with a risk of spasm, liberal use ofantispasmodic agents (such as an intra-arterialbolus application of 0.1–0.2 mg nitroglycerin,30–60 mg papaverine, 12.5 mg tolazoline, or 10mg nifedipine orally) is often recommended atthe beginning of the procedure to avoid the riskof severe spasm leading to thrombosis. Strictanticoagulation with heparin (5000 IU at thebeginning of the procedure and eventual fur-ther application after control of the activatedclotting time (ACT) in prolonged interventions)is obligatory.
Coronary 0.014-inch wires are recommendedto cross stenotic lesions, especially for very distallesions. In case of occlusion, the use of hydro-philic 0.018-inch wires may become necessary.Since hydrophilic wires have a higher risk forperforation, they should be used with specialcaution and exchanged for a standard wire aftersuccessful passage of the lesion. Furthermore,the distal tip of the guidewire should always bekept in view to avoid perforation by inadvertentplacement in a collateral vessel.
Treatment of long-distance lesions should bedone with balloon lengths up to 12 cm to avoidrepeated inflations. In long lesions we prefer to use the Amphirion balloon catheter. This is a small-diameter, long balloon with excellenttrackability, designed specifically for the tibialarteries. The Amphirion is available in diametersranging from 1.5 to 4 mm, with lengths up to 12 cm with a 0.014-inch platform. The 0.018-inch
wire compatible Cordis Savvy is another popu-lar balloon for infrapopliteal vessels.
The appropriate choice of balloon size accord-ing to the diameter of the artery is of criticalimportance to avoid severe dissections or vesselperforation/rupture. In severely calcified arteries,predilation with a smaller balloon can be recom-mended to reduce the risk of vessel perforation.
Despite the lack of studies concerning opti-mal antithrombotic treatment during and afterinfrapopliteal interventions, a combined anti-platelet therapy with aspirin and clopidogrel/ticlopidin can be recommended due to the simi-lar diameters of the tibial and coronary arteries,and the proven efficacy of this regimen aftercoronary interventions. Such treatment seemsespecially important after stent implantation.
SUMMARY
Treatment of critical limb ischemia is the onlygenerally accepted indication for below-kneeendovascular interventions. The risks of surgeryin these mostly high-risk patients (diabetics,renal insufficiency) have led, together with theimproved technology, to a steadily increasingapplication of endovascular interventions in theinfrapopliteal arteries as well.
Complications are reported to occur in 2–6%of cases, and in most series complications atthe access site are the most common. A 4 Frsheath should be used for the antegradeapproach when simple balloon angioplasty – oreven the placement of small stents – is planned.The use of modern devices (fine wires and small,low-profile balloon catheters adopted fromcoronary technology) and great operator experi-ence are the best prerequisites to avoid majorcomplications.
Coronary 0.014-inch wires are recommendedto cross stenotic lesions, especially for very distallesions. In case of occlusion, the use of hydro-philic 0.018-inch wires may become necessary.The use of hydrophilic guidewires increases therisk of unintended subintimal passage and ofperforation at the lesion site or of small collat-eral vessels. The appropriate choice of balloonsize according to the diameter of the artery is ofcritical importance to avoid severe dissections orvessel perforation/rupture.
206 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter13.qxp 4/5/2007 2:49 PM Page 206

Dissections can effectively be treated by stentimplantation. Perforation requires temporaryballoon occlusion for a few minutes.
A combined antiplatelet therapy with aspirinand clopidogrel/ticlopidin should be applied.
CHECK LIST FOR EMERGENCYEQUIPMENT FOR INTERVENTIONSIN THIS SPECIFIC VESSEL AREA
• covered stent• thrombolytics• aspiration thrombectomy catheter• coils.
REFERENCES
1. Tsetis D, Belli AM. The role of infrapopliteal angio-plasty. Br J Radiol 2004; 77: 1007–15.
2. Krankenberg H, Sorge I, Zeller T et al. Percutaneoustransluminal angioplasty of infrapopliteal arteries inpatients with intermittent claudication: acute and one-year results. Cathet Cardiovasc Interv 2005; 64: 12–17.
3. Pomposelli FB, Marcaccio EJ, Gibbons GW et al. Dorsalispedis arterial bypass: durable limb salvage for footischemia in patients with diabetes mellitus. J Vasc Surg1995; 21: 375–84.
4. Soder HK, Manninen HI, Jaakkola P et al. Prospectivetrial of infrapopliteal artery balloon angioplasty forcritical limb ischemia: angiographic and clinical results.J Vasc Interv Radiol 2000; 11: 1021–31.
5. Lofberg AM, Lorelius LE, Karacagil S. The use ofbelow-knee percutaneous transluminal angioplastyin arterial occlusive disease causing chronic criticallimb ischemia. Cardiovasc Interv Radiol 1996; 19:317–22.
6. Dorros G, Jaff M, Dorros AM et al. Tibioperoneal (out-flow lesion) angioplasty can be used as primary treat-ment in 235 patients with critical limb ischemia. Five yearsfollow-up. Circulation 2001; 104: 2057–62.
7. Faglia E, Dalla Paola L, Clerici G et al. Peripheral angio-plasty as the first-choice revascularization procedure indiabetic patients with critical limb ischemia: prospec-tive study of 993 consecutive patients hospitalized andfollowed between 1999 and 2003. Eur J Vasc EndovascSurg 2005; 29: 620–7.
8. Mishkel G, Goswami M. A practical approach to endovas-cular therapy for infrapopliteal disease and the treatmentof critical leg ischemia: savage or salvage angioplasty? J Invas Cardiol 2005; 17: 45–51.
9. Rand T, Basile A, Cejna M et al. PTA versus carbofilm-coated stents in infrapopliteal arteries: pilot study.Cardiovasc Interv Radiol 2006; 29: 29–38.
10. Bosiers M, Hart J, Deloose K et al. Endovascular therapyas the primary approach for limb salvage in patients withcritical limb ischemia: experience with 443 infrapoplitealprocedures. Vascular 2006; 14: 63–9.
11. Brosi P, Baumgartner I, Silvestro A et al. Below-the-kneeangioplasty in patients with end-stage renal disease.J Endovasc Ther 2005; 12: 704–13.
12. Bolia A, Sayers R, Thompson M et al. Subintimal andintraluminal recanalization of occluded crural arteriesby percutaneous balloon angioplasty. Eur J Vasc Surg1994; 8: 214–19.
13. Vraux H, Hammer F, Verhelst R et al. Subintimalangioplasty of tibial vessel occlusions in the treatmentof critical limb ischemia: mid-term results. Eur J VascEndovasc Surg 2000; 20: 441–6.
14. Hayes PD, Chokkalingam A, Jones R et al. Arterial per-foration during infrainguinal lower limb angioplastydoes not worsen outcome: results from 1409 patients. J Endovasc Ther 2002; 9: 422–7.
15. Morshedi-Meibodi A, Dieter R. Endovascular treatmentof infrapopliteal lesions. An overview of the promisingapproaches to treating CLI and the role of debulkingdevices. Endovasc Today 2006; 5: 43–9.
16. Ansel G, Sample N, Botti C Jr et al. Cutting balloonangioplasty of the popliteal and infrapopliteal vesselsfor symptomatic limb ischemia. Cathet CardiovascInterv 2004; 61: 1–4.
17. Rubin BG. Plaque excision in the treatment of periph-eral arterial disease. Perspect Vasc Surg Endovasc Ther2006; 18: 47–52.
18. Zeller T, Rastan A, Schwarzwalder U et al. Midtermresults after atherectomy-assisted angioplasty of below-knee arteries with use of the Silverhawk device. J VascInterv Radiol 2004; 15: 1391–7.
19. Laird J, Zeller T, Gray B et al. Limb salvage followinglaser-assisted angioplasty for critical limb ischemia:results of the LACI multicenter trial. J Endovasc Ther2006; 13: 1–11.
20. Scheinert D, Biamino G, Schmidt A. Preliminary experi-ence with DESs in tibial arteries. Endovasc Today 2006;5: 60–2.
21. Siablis D, Kraniotis P, Karnabatidis D et al. Sirolimus-eluting versus bare stents for bailout after suboptimalinfrapopliteal angioplasty for critical limb ischemia: 6-month angiographic results from a nonrandomizedprospective single-center study. J Endovasc Ther 2005;12: 685–95.
22. Botti CF, Ansel GM, Silver MJ et al. Percutaneous retro-grade tibial access in limb salvage. J Endovasc Ther2003; 10: 614–18.
COMPLICATIONS OF TIBIOPERONEAL INTERVENTIONS 207
CPVI_Chapter13.qxp 4/5/2007 2:49 PM Page 207

CPVI_Chapter13.qxp 4/5/2007 2:49 PM Page 208

INTRODUCTION TO THE FREQUENCY ANDTYPE OF COMPLICATIONS
Interventional radiology in failing hemodialysisfistulas and grafts has been – in the meantime –accepted as a valid alternative to surgical revi-sion. The literature does not show a significantdifference concerning technical outcome, com-plication rate, and follow-up patency betweensurgical revision and an interventional radio-logic approach.1–3 Most procedures are safe, easyto perform, and benign in outcome. In the major-ity of cases a transvenous access is used, severebleeding complications therefore remain rare.Nevertheless, there are typical complications inpercutaneous interventions in dialysis connec-tions; the type, rate, and severity depend on theunderlying problem, the method of treatment,and the means of access. Furthermore – albeitstill very rare – there are some typical complica-tions that are potentially life-threatening or dis-abling, such as pulmonary embolism, paradoxicarterial embolism, and septicemia. Others occurthat require surgical repair.
Most shunt procedures are performed as anacute and emergency treatment, but in con-scious and informable patients, raising open and
sometimes delicate questions about the ways inwhich patient information and consent shouldbe approached. As related questions, however,depend on the jurisdiction of each individualcountry, it is difficult to give clear answers inthat complex field.
General complication rate
It is somewhat difficult to give a uniform overviewabout complication rates from the literature asthey are reported and classified in heterogeneousways. Some authors, for example, count venousruptures among complications, while othersregard them as technical failures that require fur-ther treatment, but not as complications.
Nevertheless, most of the complications thathave been reported are relatively benign and donot require further surgical or medical treatment.Life-theatening situations such as clinically signif-icant pulmonary embolism or paradoxic arterialembolism may occur, but due to the underlyingcharacter of the shunt failure they are typicallyassociated with treatment of shunt thrombosis.
There is scant literature dealing exclusivelywith the rate of complications of percutaneous
14
Complications in the percutaneousmanagement of failing hemodialysisfistulas and graftsDierk Vorwerk
Introduction to the frequency and type of complications • Complications of specific interventional stepsand tools • Acute complications • Methods to avoid complications • Conclusion • Check list foremergency equipment
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 209

shunt treatment. Beathard et al4 reported on alarge collection of data from 14 067 cases thatwere treated in different ways, including bothshunt thromboses and stenosis. They found atotal rate of 3.54% for complications in general;3.26% were classified as minor while 0.28% wereclassified as major. Turmel-Rodrigues et al5
reported on a mixed group of 1118 shunt proce-dures. They found a rate of 2% for major compli-cations such as uncontrollable rupture with fistulaloss (2 cases), formation of pseudoaneurysms atthe site of dilatation or puncture requiring surgery(5 cases), infection and bacteremia (5 cases),severe hematoma requiring surgical evacuation(2 cases), pulmonary embolism (1 case), mesen-teric infarction (1 case), significant blood loss (1 case), iododermitis (2 cases), metabolic acidosis(1 case), and pulmonary edema (1 case). However,they did not count arterial embolism duringdeclotting as a complication as they claimed thatall events were treated by aspiration. Technicalproblems occurred with venous rupture in 83cases (7.7%), with the highest rate in upper armfistulas. Venous ruptures were partly treated bystent placement, with two events of stent dis-lodgement requiring retrieval.
Thrombosed shunts
Complications seem to be more frequent inshunt declotting techniques. Sofocleous et al6
found 48 complications among 579 cases ofpercutaneous shunt treatment in grafts (8.5%).These included 12 venous ruptures, 4 graft dis-sections, 7 small hematomas, 12 graft extravasa-tions and one distant hematoma, 8 arterial emboli,2 pulmonary emboli, one intestinal angina, andone death related to the procedure. While themajority was related to bleeding complicationsat the site of access or dilatation, some very typ-ical complications for thrombectomy proce-dures did occur – although in a relatively smallamount of 2%.
Lazzaro et al7 compared mechanical throm-bectomy using the percutaneous thrombectomydevice (PTD) device as a sole instrument formechanical thrombectomy with a historical groupwhere the PTD device together with a Fogartyballoon was used in order to remove the arterialplug and to pull it into the graft. They had a rate
of 6% of arterial emboli in the PTD alone groupversus 2% in the PTD Fogarty group. Venousrupture occurred in 6% versus 2% and one caseof sepsis was found. This counted for a total of 9complications out of 104 procedures (9%).
Turmel-Rodrigues et al8 described one case ofpulmonary embolism, one subacute pseudoaneu-rysm, one significant blood loss, and 5 venousruptures in 93 cases of thrombectomy of nativefistulas (8% including venous rupture, 3% with-out). Myayama et al9 described minor complica-tions in 20% of 26 patients with thrombosedBrescia–Cimino fistulas, but this included proce-dural events such as venous rupture in 12% anddevelopment of a hematoma in 8%. Liang et al10
reported just 2 cases of venous rupture and 2cases of radial arterial emboli in a group of 42thromboses of Brescia–Cimino fistulas treatedby percutaneous means, which counts for a totalcomplication rate of 10%, or 5% excludingvenous rupture. Rajan and Clark11 found 2 com-plications among 30 treatments for thrombosisof native fistulas: one small hematoma and onesmall pseudoaneurysm (7% in total).
COMPLICATIONS OF SPECIFIC INTERVENTIONAL STEPS AND TOOLS
Barth et al12 did not find significant differences incomplications comparing random hydrodynamicthrombectomy and spray lysis in thrombosedhemodialysis grafts. Vesely et al13 compared rhe-olytic thrombectomy using the AngiojetTM devicewith surgery in the treatment of thrombosedgrafts in a randomized trial with 153 treatmentsenrolled. They did not find a significant differ-ence in the complication rate, with 14.6% in theAngiojetTM group and 14.1% in the surgery group.
Immature fistulas
In the percutaneous treatment of immature fistulas, an overall complication rate of 4%, withminor complications in 3% and major complica-tions in 1%, was described by Beathard et al14
analyzing procedural results of 100 cases. Turmel-Rodrigues et al15 described two significant compli-cations out of 69 procedures including bacteremiaand a pseudoaneurysm formation (2.8%). Theyalso described 9 cases of venous rupture (n = 13%)
210 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 210

where 2 required further treatment by place-ment of a stent graft.
Transarterial access
Most authors use a transvenous access to treatshunt failure. There are few references availablewhere a transbrachial arterial access was used asthe primary access technique. In those, a higherrisk of bleeding complications is likely. Manninenet al16 reported a complication rate of 12% exclu-sively dealing with access problems, including 6 minor hematomas but 4 pseudoaneurysms of the brachial artery and 2 persistent arterialbleedings, of whom 4 needed surgical treatment.According to Trerotola and Turmel-Rodrigues17
therefore, transarterial access should remainreserved to special cases where a transvenousaccess is not possible or failed.
ACUTE COMPLICATIONS
Technical complications
Venous rupture at the site of balloon inflation isa relatively frequent technical complication andoccurs in 2 to 8% of cases.6,8,11 It is more frequent
in the treatment of immature fistulas, occurringin up to 13%. Venous stenoses in shunts andgrafts are frequently more rigid than in arteriesand formed by scarring tissue. However, venousrupture is unpredictable but occurs more fre-quently in upper arm veins than in lower armveins.5
Usually rupture is benign and extravasation isself-limiting in the majority of cases (Figure 14.1).The primary means of treatment is prolongedballoon inflation at the site of rupture. If this isnot sufficient, or rupture is flow-limiting, the useof native stents is recommended; some authorsalso prefer the use of stent grafts instead. In ourown experience, the use of stent grafts as theonly effective means to treat a ruptured vein isvery rarely necessary, but polytetrafluoroethylene(ePTFE)-coated stent grafts may be used as analternative to native stents as they seem to bepromising concerning their tendency of restenosis.
Rajan et al11 used Wallstents to treat venousrupture in 9 of 414 angioplasties, indicating astent rate of 2%. Turmel-Rodrigues et al5 usedstents and stent grafts in 16 of 83 venous rup-tures (18%). Related to all interventions, thestent rate was about 1.5% for venous rupture(Figure 14.2).
(a)
(b)
Figure 14.1 Venous rupture. (a) Native lower arm fistula with a stenosis in the proximal vein. (b) After PTA, venousrupture (arrow) occurs, that was successfully treated by prolonged PTA.
COMPLICATIONS IN THE PERCUTANEOUS MANAGEMENT OF HEMODIALYSIS 211
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 211

Venous dissection (Figure 14.3) with compro-mise of the venous lumen but no blunt extravasa-tion may occur as a variation of venous ruptureand may require stent placement. Both venousrupture and venous perforation, which mayoccur during an attempt to cross a tight stenosis,may lead to a complete blockage of the venouslumen, making recanalization from the same
approach impossible. In such a case, a secondaccess from the opposite venous segment – orfrom an arterial approach if the dissection hap-pens close to the anastomosis – should be used.
Arterial dissection is a very rare event andshould be treated similarly as in all peripheralarteries by prolonged balloon angioplasty even-tually combined with stent placement.
212 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a)
(b)
Figure 14.2 Venous rupture and stent. (a) Rupture of the upper cephalic vein after PTA. (b) After stent implantationfollowing unsuccessful prolonged PTA, rupture is sealed (arrow).
(a) (b) (c)
Figure 14.3 Venous dissection in an occluded forearm fistula. (a) After retrograde cannulation of the lower cephalic veinthe guidewire is not able to enter into the artery crossing the occlusion. (b) After contrast an extravasal depot of contrastis seen, indicating dissection. (c) Repeat cannulation finally enters into an endoluminal pathway and into the radial artery.
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 212

In some stenoses, conventional balloons donot open completely despite high pressures upto 18 atm. This may lead to incomplete openingof the lesion and residual stenosis (Figure 14.4).In those cases, high pressure balloons that maybe dilated up to 30 and 40 atm may be used aswell as cutting balloons.18 Cutting balloons donot improve long-term patency in a generalshunt population but offer a technical option incases with rigid stenoses.18,19
Bleeding problems
Bleeding may occur at different locations. It mayfollow venous rupture and is self-limiting inmost of these incidences. From our experience,bleeding may be more severe in upper arm veinruptures, as skin and subcutaneous tissue maybe looser than at the forearm. The same is truefor bleeding from the point of access. As espe-cially for thrombectomy, larger diameter sheathssuch as 8 Fr are used, bleeding control is some-times time-consuming and difficult.
We routinely use subcutaneous purse stringsutures to narrow the puncture channel and toreduce bleeding time.20 This works very well in areas with scarring tissue, which is almostalways present in puncture areas of shunts inuse for a long time. In patients with immatureshunts, however, or patients with very loosesubcutaneous tissue, this method may fail andmassive bleeding may occur. Prolonged com-pression and sometimes surgical evacuationmay then become necessary.
As a sequela of bleeding or rupture, late for-mation of a pseudoaneurysm eventually occurs.
Embolization
Arterial embolization
Arterial embolization rarely occurs duringrecanalization of lower arm arteriovenous fistulas.Antegrade flow from the feeding artery usuallyprevents dislodgement of thrombus materialinto the radial artery.
COMPLICATIONS IN THE PERCUTANEOUS MANAGEMENT OF HEMODIALYSIS 213
(a)
(b)
(c)
Figure 14.4 Rigid stenosis. (a) Stenosis of the lower cephalic vein in a native fistula. (b) By use of a conventionalballoon, the stenosis does not open completely, despite pressures of 18 atm. (c) Cutting balloon completely opens atthe stenotic side, overcoming the rigid stenosis.
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 213

More often, arterial embolization occurs whentreating an upper arm brachiocephalic shunt ofimplant grafts. The nature of the arterial anasto-mosis to a bigger arterial vessel as a side-to-endanastomosis facilitates dislodgement of throm-bus material into the brachial artery. Its rate isrelatively high. Lazzaro et al7 described a rate of2 to 6% using the PTD device. Smits et al foundthree arterial emboli in 68 treatments using dif-ferent mechanical devices (4%).21
Some of these emboli may remain asympto-matic. It is, however, recommended to removethem as early as possible as in most dialysispatients peripheral arteries are delicate. In upperarm native fistulas, treatment is relatively easyby retrograde puncture of the upper cephalicartery. By this access a guidewire is inserted intothe brachial artery in an antegrade fashion and asuitable manual aspiration catheter is guidedclose to the point of embolic occlusion. The throm-bus is then sucked out from the artery and dis-lodged into the vein or outside of the bodythrough the sheath. A sheath with a removablehub is recommended.
In implant grafts, removal of arterial emboli isusually more difficult due to the very acuteangulation between the arterial graft limb andthe brachial artery. Trerotola et al7 described asimple backbleeding technique where the brachialartery proximal to the arterial graft anastomosisis occluded by a balloon while the patient startsexercising his ipsilateral hand. By collaterals areversed flow is created that dislocates theembolus into the graft out of the artery.
If this approach fails, aspiration embolec-tomy can be performed (Figure 14.5). For thispurpose, a kink-resistant cross-over sheath(6–7 Fr) is guided across the arterial anasto-mosis through which an aspiration cathetercan be safely introduced without the risk ofkinking.
Pulmonary embolism
Pulmonary embolization (PE) rarely becomessymptomatic in patients undergoing shunt andgraft declotting procedures. However, singleevents are reported from many series and thereis also the description of fatal outcome.22
Smits et al21 described one case out of 68(1.5%) with symptomatic PE; Sofocleous et al6
did not describe a single case among 579 ses-sions and Turmel-Rodrigues et al5 found onecase out of 1118 treatments (0.09%). However,there is also a certain subset of patients whoexperience silent events of PE without becomingsymptomatic.
Petronis et al23 performed perfusion scansbefore and after mechanical thrombectomy in 13 patients but found signs of new filling defectsin only one patient. Smits et al21 analyzed 23 oftheir patients in the same way before and aftermechanical or pharmacomechanical thrombec-tomy and found signs of PE in 8 cases (35%).
It is questionable whether thrombolysis in-stead of mechanical thrombectomy prevents PE.In an animal experimental setting, Trerotola et al24 have tested mechanical thrombectomyusing the PTD device against spray lysis andfound signs of PE in lung scans after recanaliza-tion of grafts in 18% of dogs in the PTD groupbut in 91% of the spray-lysis group. However,Kinney et al25 compared spray lysis with uroki-nase versus spray lysis with heparin saline solu-tion only in 27 patients. They found signs ofnew PE in 18% of patients where urokinase wasused but – significantly more – in 64% whereheparinized saline was used. All cases remainedclinically silent. Interestingly enough, they com-pared baseline perfusion lung scans with thoseafter treatment and described abnormal baselinescans in 70.4%. These findings state the oldknowledge that patients with arterio-verious fis-tulas and grafts frequently experience events ofPE even without shunt thrombosis.
Harp et al26 investigated whether recurrentthrombectomy treatment may lead to chronicpulmonary hypertension potentially due to silentrecurrent embolization. They compared patientswith one or more thrombectomies to healthy per-sons and those with end-stage renal disease butno thrombectomies. They found a higher inci-dence for pulmonary hypertension in patientswith end-stage renal disease, but no incidence of a higher rate in patients having undergonethrombectomy treatment.
To conclude, there is a small but existing risk of symptomatic pulmonary embolism afterthrombectomy in shunts. There seems to be an
214 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 214

even higher risk to experience silent PE which –from our current knowledge – is not likely tolead to late complications. Unfortunately, singlecases have been reported who developed para-doxal cerebral emboli or mesenteric schemiawhich may result from paradoxal thrombus dis-lodgement. Besides case reports on paradoxalcerebral emboli,27,28 Turmel-Rodrigues et al5
reported one case of mesenteric infarction out of1118 treatment sessions (0.09%) and Sofocleouset al6 described one case of mesenteric anginaout of 579 cases (0.14%).
Infection
Infection and septicemia may complicate treat-ment of shunt thrombosis in some cases. If alocal infection is apparent, percutaneous inter-vention is contraindicated. In some cases, how-ever, infection is not apparent, the site developsinfection after intervention, or part of the occlud-ing material is superinfected. In those cases,septicemia may occur. Turmel-Rodrigues et aldescribed 5 cases out of 1118 interventions
(0.45%).5 Very rarely, a stent may undergo sec-ondary infection. There is one case report pub-lished on a superinfected stent in the subclavianvein of a dialysis patient.28
Stent complications
After a stent has been placed, complications arerare. Acute stent thrombosis in central or upperarm veins is extremely rare as a sufficient flowusually keeps them patent. In grafts, rethrombo-sis also involves a stent at the venous anastomo-sis if early graft thrombosis takes place.
Stent dislocations from central veins into theright heart or the pulmonary circulation havebeen described, but remain rare, if the stent islong enough to make enough contact with thevenous wall and is of a sufficient diameter.
METHODS TO AVOID COMPLICATIONS
Due to the variety and different nature of the com-plications, avoidance is sometimes difficult. Ofcourse, general rules of percutaneous intervention
COMPLICATIONS IN THE PERCUTANEOUS MANAGEMENT OF HEMODIALYSIS 215
(a)
(b) (d)
(c)
Figure 14.5 Arterial embolization. (a) Angiographic appearance of the arterial anastomosis of an implant shunt. Shunt isstill occluded but brachial artery is open. (b) After mechanical thrombectomy, brachial artery is occluded by an embolus(arrow) but shunt flow is partly restored. (c) A kink-resistant cross-over sheath with removable hub has been introducedinto the brachial artery (arrow) through which a 6 Fr aspiration catheter was advanced. (d) After aspiration, brachial arteryis patent again. Note residual clot in the proximal loop.
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 215

need to be obeyed, for example no gross oversiz-ing of balloons and no advertent massive forceshould be obtained. Venous rupture, however, isdifficult to predict and is not strictly related tohigh pressures. Thus, it is recommended not toapply high pressure onto a resistant stenosisbecause otherwise the intervention might fail.
If mechanical instruments for thrombectomyare used they should be over-the-wire instru-ments to prevent perforation or rupture. Ruptureis usually simple to control either by prolongeddilation, stent, or stent graft placement.
Bleeding problems are also unpredictable inmost cases. In patients with immature shunts,however, or patients with very loose subcuta-neous tissue, a subcutaneous string purse sutureshould be avoided or used with care, not tooversee larger subcutaneous bleeding. In rareinstances, surgical assistance is required.
Inadvertent arterial embolization in implantloop shunts and upper arm shunts is mostly dueto incautious injection of contrast medium intothe graft or the vein without sufficient outflow.With increased pressure, parts of the thrombusmight then be squeezed out of the graft into theopen artery. Thus, imaging of partially blockedgrafts should always be performed as antegradeangiography from an arterial injection point.Also, manipulations within a thrombus requirethe use of straight or slightly curved cathetersand wires; J-shaped instruments may push partsof the thrombus into the artery.
Venous and pulmonary embolization is – unlessno paradoxal embolization occurs – relativelybenign if the thrombus remains small. To pre-vent dislodgement of larger portions of orga-nized thrombus, it is recommended to place atourniquet around the upper arm during throm-bectomy and to clear the vein as completely aspossible from remaining clots up to this pointbefore venous outflow is opened again.
CONCLUSION
Stenosis and thrombosis of hemodialysis fistu-lae and grafts represent the most frequent com-plications of hemodialysis accesses.
In conclusion, mechanical thrombectomywith all its variations proved to be an effectivepercutaneous method for thrombectomy in
hemodialysis grafts and native fistulas, achievingresults comparable to alternative methods such aslysis therapy. What particular type of treatmentshould be used depends on the experience ofeach operator, the clinical situation, the extent ofthrombosis, and the type and age of the occlusion.
Percutaneous techniques have become theapproach of first choice in many institutionsand surgical thrombectomy has been limited tospecial cases. Outcome in the overwhelmingmajority of cases is benign and the nature ofcomplications is usually minor and simple totreat by percutaneous means. Complicationsexist, however, but should not prevent interven-tional radiologists from being active in thisinteresting field of interventional radiology.
CHECK LIST FOR EMERGENCYEQUIPMENT
In order to be sufficiently prepared for the man-agement of complications the following instru-ments should be in stock:
For venous ruptureself-expanding stents (8–12 mm), stent grafts(8–12 mm), preferably self-expanding.
Arterial embolizationaspiration catheters, equipment for thrombolysis,stable and long cross-over sheath (8 or 9 Fr).
Venous thrombus removalAspiration catheters (8–9 Fr), thrombectomydevices, tourniquets.
As dialysis patients are usually older, multimor-bid, and of fragile constitution, a structure foremergency treatment and the possibility of in-house admission should be available.
REFERENCES
1. Dapunt O, Feurstein M, Rendl KH et al. Transluminalangioplasty versus conventional operation in the treat-ment of haemodialysis fistula stenosis: results from a5-year study. Br J Surg 1987; 74(11): 1004–5.
2. McCutcheon B, Weatherford D, Maxwell G et al. A pre-liminary investigation of balloon angioplasty versussurgical treatment of thrombosed dialysis access grafts.Am Surg 2003; 69(8): 663–7; discussion 668.
3. Uflacker R, Rajagopalan PR, Selby JB et al; Investigators ofthe Clinical Trial Sponsored by Microvena Corporation.
216 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 216

Thrombosed dialysis access grafts: randomized com-parison of the Amplatz thrombectomy device and sur-gical thromboembolectomy. Eur Radiol 2004; 14(11):2009–14.
4. Beathard GA, Litchfield T; Physician Operators Forumof RMS Lifeline, Inc. Effectiveness and safety of dialysisvascular access procedures performed by interven-tional nephrologists. Kidney Int 2004; 66(4): 1622–32.
5. Turmel-Rodrigues L, Pengloan J, Baudin S et al.Treatment of stenosis and thrombosis in haemodialysisfistulas and grafts by interventional radiology. NephrolDial Transplant 2000; 15(12): 2029–36.
6. Sofocleous CT, Schur I, Koh E et al. Percutaneous treat-ment of complications occurring during hemodialysisgraft recanalization. Eur J Radiol 2003; 47(3): 237–46.
7. Lazzaro CR, Trerotola SO, Shah H et al. Modified use ofthe arrow-trerotola percutaneous thrombolytic devicefor the treatment of thrombosed hemodialysis accessgrafts. J Vasc Interv Radiol 1999; 10(8): 1025–31.
8. Turmel-Rodrigues L, Pengloan J, Rodrigue H et al.Treatment of failed native arteriovenous fistulae forhemodialysis by interventional radiology. Kidney Int2000; 57(3): 1124–40.
9. Miyayama S, Matsui O, Taki K et al. OccludedBrescia–Cimino hemodialysis fistulas: endovasculartreatment with both brachial arterial and venous accessusing the pull-through technique. Cardiovasc IntervRadiol 2005; 28(6): 806–12.
10. Liang HL, Pan HB, Chung HM et al. Restoration ofthrombosed Brescia–Cimino dialysis fistulas by usingpercutaneous transluminal angioplasty. Radiology2002; 223(2): 339–44.
11. Rajan DK, Clark TW. Patency of Wallstents placed atthe venous anastomosis of dialysis grafts for salvage ofangioplasty-induced rupture. Cardiovasc Interv Radiol2003; 26(3): 242–5.
12. Barth KH, Gosnell MR, Palestrant AM et al. Hydro-dynamic thrombectomy system versus pulse-spraythrombolysis for thrombosed hemodialysis grafts: a multicenter prospective randomized comparison.Radiology 2000; 217(3): 678–84.
13. Vesely TM, Williams D, Weiss M et al. Comparison ofthe Angiojet rheolytic catheter to surgical thrombec-tomy for the treatment of thrombosed hemodialysisgrafts. Peripheral AngioJet Clinical Trial. J Vasc IntervRadiol 1999; 10(9): 1195–205.
14. Beathard GA, Arnold P, Jackson J et al; PhysicianOperators Forum of RMS Lifeline. Aggressive treatmentof early fistula failure. Kidney Int 2003; 64(4): 1487–94.
15. Turmel-Rodrigues L, Mouton A, Birmele B et al.Salvage of immature forearm fistulas for haemodialysis
by interventional radiology. Nephrol Dial Transplant2001; 16(12): 2365–71.
16. Manninen HI, Kaukanen ET, Ikaheimo R et al. Brachialarterial access: endovascular treatment of failingBrescia–Cimino emodialysis fistulas – initial successand long-term results. Radiology 2001; 218(3): 711–18.
17. Trerotola SO, Turmel-Rodrigues LA. Off the beatenpath: transbrachial approach for native fistula interven-tions. Radiology 2001; 218(3): 617–19.
18. Vorwerk D, Gunther RW, Schurmann K et al. Use of acutting balloon for dilatation of a resistant venousstenosis of a hemodialysis fistula. Cardiovasc IntervRadiol 1995; 18(1): 62–4.
19. Vesely TM, Siegel JB. Use of the peripheral cutting bal-loon to treat hemodialysis-related stenoses. J VascInterv Radiol 2005; 16(12): 1593–603.
20. Vorwerk D, Konner K, Schurmann K et al. A simpletrick to facilitate bleeding control after percutaneoushemodialysis fistula and graft interventions. CardiovascInterv Radiol 1997; 20(2): 159–60.
21. Smits HF, Van Rijk PP, Van Isselt JW et al. Pulmonaryembolism after thrombolysis of hemodialysis grafts. J Am Soc Nephrol 1997; 8(9): 1458–61.
22. Swan TL, Smyth SH, Ruffenach SJ et al. Pulmonaryembolism following hemodialysis access thrombolysis/thrombectomy. J Vasc Interv Radiol 1995; 6(5): 683–6.
23. Petronis JD, Regan F, Briefel G et al. Ventilation-perfusion scintigraphic evaluation of pulmonary clotburden after percutaneous thrombolysis of clotted hemo-dialysis access grafts. Am J Kidney Dis 1999; 34(2): 207–11.
24. Trerotola SO, Johnson MS, Schauwecker DS et al.Pulmonary emboli from pulse-spray and mechanicalthrombolysis: evaluation with an animal dialysis-graftmodel. Radiology 1996; 200(1): 169–76.
25. Kinney TB, Valji K, Rose SC et al. Pulmonary embolismfrom pulse-spray pharmacomechanical thrombolysis ofclotted hemodialysis grafts: urokinase versus heparinizedsaline. J Vasc Interv Radiol 2000; 11(9): 1143–52.
26. Harp RJ, Stavropoulos SW, Wasserstein AG et al.Pulmonary hypertension among end-stage renal failurepatients following hemodialysis access thrombectomy.Cardiovasc Interv Radiol 2005; 28(1): 17–22.
27. Owens CA, Yaghmai B, Aletich V et al. Fatal paradoxicembolism during percutaneous thrombolysis of a hemo-dialysis graft. Am J Roentgenol 1998; 170(3): 742–4.
28. Briefel GR, Regan F, Petronis JD. Cerebral embolismafter mechanical thrombolysis of a clotted hemodialy-sis access. Am J Kidney Dis 1999; 34(2): 341–3.
29. Guest SS, Kirsch CM, Baxter R et al. Infection of a sub-clavian venous stent in a hemodialysis patient. Am JKidney Dis 1995; 26(2): 377–80.
COMPLICATIONS IN THE PERCUTANEOUS MANAGEMENT OF HEMODIALYSIS 217
CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 217

CPVI_Chapter14.qxp 4/5/2007 2:49 PM Page 218

INTRODUCTION
Various interventions are performed in thevenous system. In general the intervention isperformed to restore blood flow through astenotic or occluded vein segment. Depending onthe location, the chronicity, and the cause ofthe obstruction, thrombolysis, angioplasty, orstenting is performed. In contrast to the arterialsystem, vein closure is rarely performed. Excep-tions are embolizations of insufficient gonadalveins or occlusion of varicose veins in the leg.Unfortunately the literature about venous inter-vention is scarce and reports about complica-tions are even more infrequent and consist mostlyof case reports or small series. The largest num-bers are available in angioplasty of the venousanastomosis of hemodialysis grafts. A largeseries reported 14 (2%) ruptures in 683 proce-dures.1 The lack of reported adverse events couldbe interpreted to suggest that venous interven-tions are comparably safe. The goal of this chap-ter is to address complications specific to venousintervention and how to resolve them.
The complications in the venous system differfrom the arterial system mainly because of thelack of high blood pressure. There are hardly anysubstantial venous access site bleedings despitethe use of remarkably large access sheaths. Incases of bleeding from an access site, manualcompression is usually all that is needed. In caseof a severe access site bleeding an inadvertent
injury to the adjacent artery must be considered.With the use of ultrasound guidance the venousaccess complications can be markedly reduced.2,3
Because of the low pressure in the venous sys-tem severe bleeding complications are uncom-mon and often associated with an additionalproblem such as coagulopathy or bleeding into acavity.
Access site thrombosis was reported to bebetween 2 and 28% for filter placement.4 Thesenumbers include data from the time when theintroducer systems were considerably largerthan today. With the smaller introducer profilethe rate has dropped to the point where it is nolonger reported in most publications.
Unlike the arterial system, the venous systemconsists of an extensive network of collaterals.The collateral venous network can compensatefor many segmental venous occlusions or throm-boses. Often a segmental vein occlusion does notcause any clinical symptoms and is therefore notnecessarily perceived as a complication. The dif-ference in the vein wall configuration comparedto the arterial wall results in different types ofcomplications if damaged. Dissections, quitecommon in the arterial system, are very uncom-mon in veins. A case report describes a rare cir-cumstance of a venous dissection caused by amalpositioned return needle during dialysis.5
Vein injuries rather manifest as perforation, rup-ture, or occlusion instead.
15
Venous interventionsC Binkert
Introduction • Factors identifying patients at high risk for complications • Complications of specificsteps and tools • Methods to detect potential complications • Techniques to resolve complications •Methods to avoid complications • Summary • Check list for emergency equipment
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 219

FACTORS IDENTIFYING PATIENTS AT HIGH RISK FOR COMPLICATIONS
Patients with severe comorbidities such as coro-nary artery disease, congestive heart failure, orchronic obstructive pulmonary disease have an increased risk for any procedure includingvenous intervention. However, because alterna-tive surgeries carry an even higher risk for thesepatients, endovascular intervention is generallythe better option for these patients. Besides thegeneral medical conditions, there are some spe-cific factors which can increase the risk of venousinterventions. These factors include all condi-tions which increase the risk of bleeding. Anincreased bleeding risk is most commonly sec-ondary to anticoagulation. In these cases wait-ing till the bleeding risk is back to normal is oftenthe best choice. Other reasons for a prolongedbleeding time are liver failure or less commonhereditary coagulopathies. In the latter instances,correction of the bleeding risk with fresh frozenplasma or specific factors is indicated. The oppo-site, a hypercoagulopathy, can also increase therisk of venous intervention by causing thrombo-sis during intervention. Careful administrationof heparin is advisable in these cases, includingmonitoring the heparin effect with repeat mea-surements of the activated clotting time (ACT).
Vein wall weakness can also lead to anincreased risk of vein rupture during interven-tions. Chronic steroid treatment, recent surgery,or ablation6 can weaken the venous wall. In caseof recent surgery, the risk will decrease over time,therefore waiting 2–4 weeks before intervening inan area of prior surgery is advisable. In case ofchronic steroid use, careful manipulation ofmaterial through the veins is important in orderto avoid complications such as a vein rupture(Figure 15.1). In case of additional risk factors, therisks and benefits of a venous intervention haveto be evaluated individually before proceeding.
COMPLICATIONS OF SPECIFIC STEPS AND TOOLS
Similar to arterial revascularization, the firststep to re-open a vein is to advance a wirethrough the obstruction. This step itself hardlyever causes any problems because the hole,even in the wrong place, is too small to cause a
significant hemorrhage. This is still true when asharp recanalization technique is used. Forsharp recanalizations typically a 21 gauge metal-lic mandrel is used through which a sharp styletcan be passed (Cook).7 Sharp recanalizations havea high-risk of severe hemodynamic complica-tions, including hemothorax and/or pericardialtamponade (Figure 15.2). A recent report of 12patients treated with sharp recanalization showedmajor complications in 3 patients (25%).7 Afterguidewire placement the next step is usually toadvance a catheter, most commonly a 5 Frenchcatheter, through the obstruction. Through thecatheter a venogram is typically performed toconfirm the appropriate position of the catheterbeyond the obstruction. If a wrong path is recog-nized at this point, simply pulling the catheterand abandoning the procedure can prevent a seri-ous complication. The critical step is the inflationof the balloon to open up the obstruction.
During angioplasty a vein can rupture(Figure 15.3). Possible causes for a vein ruptureare balloon oversizing or a rupture of the bal-loon itself.8 The burst of a balloon can damage thesurrounding vessel wall, which is also describedin the coronary literature.9,10 It is advisable to usean inflating device to monitor the balloon pres-sure, and high-pressure balloons, in case of aresistant stenosis. An area of increased risk ofrupture is the cephalic arch (Figure 15.4). Onearticle described a 6% rupture rate at the cephalicarch during angioplasty.11 Besides rupture of thevein, the step of balloon inflation can cause asubstantial amount of bleeding if the course of the guidewire was extraluminal. Figure 15.2illustrates how the step of angioplasty of anextraluminal path can cause an immediate severecomplication, while nothing happened when theguidewire and catheter were advanced.
Balloon angioplasty is usually the treatmentof choice in the venous system. In certaininstances, angioplasty alone is not enough, how-ever. Such instances are immediate recoil,extrinsic compression, or rare cases of dissec-tion after angioplasty. In these cases the place-ment of a stent can be helpful. Generallyself-expanding stents are preferred over balloon-expanable stents in the venous system in orderto adapt to the changing vein diameter duringrespiration and to avoid irreversible collapse
220 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 220

by compression. The use of self-expandable niti-nol stents is somewhat limited by the availablesizes. The largest diameter available is 14 mm fromdifferent companies (Luminex, Bard Peripheral;Zilver, Cook, or Smart, Cordis). For larger diam-eters alternatively the WallstentTM from BostonScientific (up to 24 mm) or the Gianturco-RoschZTM stent from Cook (up to 35 mm) can be used.As a side note for interventionalists in the US:the nitinol stents are approved for biliary useand the larger stents for tracheo-bronchial use.
While rupture during angioplasty is the most feared complication during venous revas-cularization, stenting has its own complications.
Stent complications include collapse, fracture,migration, thrombosis, and perforation. Col-lapses or fractures most commonly occur whenthe stent is repeatedly compressed, for examplein the subclavian vein between the first rib andthe clavicle.12 Migration is most likely whenstents are undersized or when using Wallstents.Wallstents have a tendency to migrate whenthe edges of the stent are not well embedded(Figure 15.5). Retrieval of a migrated Wallstentis illustrated in Figure 15.5. Similar Wallstentretrieval is also described in the literature.13 Thesharp edges of the Wallstent can cause damageto the vessel wall, which is most dangerous close
VENOUS INTERVENTIONS 221
(a)
(c)
(b)
(d)
Figure 15.1 56-year-old man with heart–lung transplant 8 years previously. He developed renal insufficiency secondary tocyclosporine therapy. He presented for tunneled hemodialysis catheter. During insertion of the peel-away sheath theguidewire was bent and dilator pointed into the mediastinum. A quick hand-injected venogram showed regular flow ofcontrast through the brachiocephalic vein (a). Because of pain and an episode of hypotension a few hours later a CT wasperformed showing rupture of the left brachiocephalic vein (arrow, b) and a mediastinal hematoma with air from therecent catheter placement (c). The rupture in the trajectory of the traumatically inserted dilator is better visualized oncoronal reconstruction (arrow, d). The patient was admitted to ICU for observation. He did well without any furtherintervention and left the hospital 2 days later.
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 221

222 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a)
(d)
(b) (c)
Figure 15.2 43-year-old woman with cystic fibrosis and head swelling secondary to chronic SVC occlusion. Initialvenogram shows a short occlusion of the right brachiocephalic vein (a). Sharp recanalization was performed and the wirewas snared in the SVC to achieve through-and-through access (b). After angioplasty to 8 mm the patient developed acardiac tamponade. The balloon was re-inflated and an emergency pericardiocentesis was performed. The patientstabilized and a 14/40 mm Wallgraft was placed with the intention to cover the rupture site, but follow-up venographycontinued to show contrast leaking into the pericardium (c). A balloon was re-inflated and the patient was brought to theoperating room where open repair was perfomed. Strangely, the Wallgraft was found to end in the pericardium without ahole in the heart or SVC (d). The patient recovered well from a cardiovascular perspective, but she could not beextubated secondary to her underlying lung disease and expired 27 days later.
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 222

to the heart. Damage to the superior vena cavaor right atrium can lead to cardiac tamponade,which can be fatal14 if not immediately decom-pressed with a pericardial drain.15 Cardiac tam-ponade can occur even 6 months after Wallstentplacement.16 Venous perforation can also occurwhen two stents are compressing the tissue inbetween. This condition led to two fatal outcomeswith simultaneous caval and esophageal stentplacement.17
Balloons and stents are the most commonlyused tools for venous intervention. Other toolsinclude caval filters and coils. Possible filtercomplications include filter migration,18 filterfracture, caval penetration with injury to adjacentstructures such as the aorta19 or duodenum,20 orcaval occlusion.21 The incidence of these compli-cations is likely higher because many of themare asymptomatic and go undetected.
As mentioned earlier, embolization of veins israrely performed. Particulate embolization isnot feasible because in the venous system theblood flow runs from small to large vessels andparticles would end up in the pulmonary circu-lation when released into the vein. Coil emboliza-tion is occasionally performed. One area of such
embolization is insufficient gonadal veins.22
There is a chance that a coil could dislodge withthe flow to the pulmonary arteries. A single coilinto the pulmonary artery would likely beasymptomatic. However, snare retrieval can beattempted to avoid the risk of pulmonary arterythrombosis. The snare technique is widely usedto remove foreign bodies from the pulmonarycirculation.23,24
Endovascular thrombectomy of acute deepvein thrombosis, despite being controversial, is increasingly performed. Thrombectomy caneither be performed mechanically or pharmaco-logically,25 or in a combined technique using thepower-pulse spray technique.26 The complicationsof mechanical thrombectomy are rupture of thevein similar to angioplasty. Catheter-directedthrombolysis has additional risks of local or dis-tant bleeding. In a study of 473 patients, majorbleedings were reported in 11%.27 Most of themajor bleeds were either at the venous insertionsite or in the retroperitoneum. However, in thesame study two intracranial hemorrhages (0.4%),one of them fatal, occurred. More recently, smallerstudies report no major complication using com-bined mechanico-pharmacologic techniques.25,26
VENOUS INTERVENTIONS 223
(a) (b) (c)
Figure 15.3 44-year-old woman with persistent left leg swelling. Initial venogram shows a high-grade stenosis of theexternal iliac vein close to the internal iliac vein inflow (a). After angioplasty to 10 mm the vein ruptured with diffuseextravazatioin into the surrounding tissues (b). A bare stent (Smart 12/40 mm) was placed to seal the rupture (c). Thepatient left the hospital after an overnight observation.
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 223

With either mechanical or pharmacologic throm-bectomy there is a risk of pulmonary embolism.In a larger series symptomatic pulmonary embo-lisms were seen in 6 patients (1%), one fatal.27
With the availability of retrievable filters manyinterventionalists place an optional caval filterprophylactically before thrombus removal. Ithas been shown that retrievable filter can effec-tively avoid new pulmonary embolism duringtreatment of deep vein thrombosis.28 Filter place-ment is maybe even more important whenusing newer, more aggressive thrombolysis tech-niques. Recently a case with a large pulmonary
embolism after power-pulse spray thrombolysiswas reported.29
METHODS TO DETECT POTENTIAL COMPLICATIONS
Before discussing methods to detect complica-tions, it should be emphasized that good imag-ing before an intervention can help to minimizecomplications during the intervention. Contrast-enhanced cross-sectional imaging (CT and/orMRI) helps proper planning of the interventionincluding determination of the best access site,
224 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
(a)
(c) (d)
(b)
Figure 15.4 52-year-old man on hemodialysis. He presented with a central stenosis of a left brachio-cephalic graft (a).During angioplasty to 6 mm a tight waist was seen (arrow, b). After angioplasty the cephalic vein ruptured (c). Prolongedballoon inflation for 10 minutes was unsuccessful, therefore an 8/40 mm Wallgraft was placed which sealed the rupture(d). The stent graft was patent at 3 months’ follow-up.
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 224

VENOUS INTERVENTIONS 225
(a)
(c)
(e) (f)
(d)
(b)
Figure 15.5 60-year-old woman with end-stage renal disease and left arm AV access. A 16 mm Wallstent was placed inthe left brachiocephalic vein (a). The Wallstent opened the stenosis well, but remained in a funnel shape with the centralstruts not engaging the subclavian vein. Shortly after placement the Wallstent started to migrate towards the right atrium(b) and a little later the stent was in the right atrium (c). A gooseneck snare was then advanced around the stent (d) andclosed at the center of the Wallstent (e). The Wallstent was then removed through the femoral access (f). The patienthad no sequelae from the procedure. In a further procedure the left brachiocephalic vein was stented using a self-expandablenitinol stent. Courtesy of R Torrance Andrews, MD; University of Washington.
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 225

assessment of the cause of the obstruction, andthe strategy to cross the lesion. In addition, thevein diameter and the length of the stenosis/occlusion can be measured, which helps in selec-tion of the appropriate balloon or stent before theprocedure.
At the beginning of any complex case a scoutfilm should be taken in order to better recognizechanges during the intervention. Venographyshould be performed using a power injectorin order to properly fill the vein. A low-volumehand injection can miss even a quite large rup-ture easily (Figure 15.1). Hemodynamic moni-toring is of limited use for early detection ofvenous complications. Unlike in the arterial sys-tem, venous bleeding is usually slow and signif-icant blood loss occurs over longer periods oftime. Exceptions are bleeding into the peri-cardium, as shown in Figure 15.2, which resultedin immediate cardiac arrest.
If in doubt, cross-sectional imaging should beperformed to assess an ongoing problem.15 Asillustrated in Figure 15.1, a rupture of a centralvein with a large hematoma was missed onhand-injected venography. The patient remainedhemodynamically stable, but was admitted tothe intensive care unit for observation.
TECHNIQUES TO RESOLVE COMPLICATIONS
Bleeding is the most common complication fromvenous interventions. The treatment of bleedingranges from observation (Figure 15.1) to emer-gency surgery (Figure 15.2). It can be difficult tochoose the appropriate method because venousbleeds can develop over time. It is important forthe interventionalist to have pre-thought strate-gies in place to quickly control the acute bleedingbefore contemplating further treatment options.These automatisms include immediate re-inflationof the angioplasty balloon at the site of bleedingor manual compression if applicable. These ini-tial measures can sometimes be all that is neededto control the bleeding, but more importantlythey give time to rethink the options for furthersteps. Prolonged balloon inflation, typically withthe same balloon used for angioplasty, is a sim-ple first step. The success of prolonged ballooninflation for rupture hemodialysis access wasreported at 29%.30
If prolonged balloon inflation is not successfula bare1 or covered stent can be placed to coverthe rupture or bleeding site (Figure 15.4). Self-expandable stents are preferable over balloon-expandable stents to adopt to the changing sizeof a vein during respiration and to exert a con-tinuous force for optimal wall adaptation. Thestent length should be chosen to cover the rup-ture site by at least 2 cm on each side. Whenusing a bare or covered stent appropriate over-sizing of the device is important. Oversizing by10–20% or 2–3 mm is recommended. Too muchoversizing can be a problem for bare and cov-ered stents. If a bare stent is too oversized theincreased radial force could potentially lead to aworsening of the vein rupture. When using a toooversized covered stent there is a risk that thecover material will not fully adapt to the veinwall. If redundancy of the cover material persiststhe rupture may not be sealed properly, Similarto the nitinol bare stents, the available sizes ofself-expanding covered stents are limited to adiameter of 10 mm Fluency (Bard Peripheral),13 mm Viabahn (Gore) or 14 mm Wallgraft(Boston Scientific). Alternatively a piece of anaortic stent graft can be used.31
In contrast to bleeding issues, venous throm-bosis can occur during venous interventions. Thisis most common when working in an arterio-venous access graft, because the graft has no sidebranches. Native veins hardly ever thromboseduring a procedure, especially when appropriateanticoagulation with heparin is used. However,acute stent thrombosis has been described.32 Incase a thrombosis occurs, mechanical or phar-macologic thrombolysis can be performed toresolve the clot. Because of the acuity of the clot,dissolution of the clot is typically fairly easy.The simplest way is to spray a thrombolytic agentinto the fresh clot. A very practical way is to usea vial of 2 mg alteplase (Cathflow Activase,Genentech, South San Francisco, CA) which wasdesigned for central catheter lysis. Expensivemechanical devices are rarely needed to dissolveacute thrombosis which occurs during a proce-dure. In case of thrombosis it is important tomake sure the patient is appropriately anticoag-ulated with heparin. The use of an activatedclotting time can be helpful to adjust the correctheparin dose. In addition, it is important to try
226 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 226

to treat the underlying problem, which is likely avenous obstruction or a hypercoagulable situa-tion, in order to avoid rethrombosis.
Despite the advancement in endovasculartechnology open surgical solutions should alwaysbe considered. In certain cases, such as in the casedescribed in Figure 15.2, open surgery is the life-saving solution. In other circumstances, surgicaloptions can possibly be less invasive and quickerthan an endovascular approach. An examplewould be a foreign body stuck in the commonfemoral vein. Endovascular options would likelyrequire another large access, whereas surgicalremoval is straightforward. A good collaborationbetween the interventionalist and surgeon isimportant, especially if riskier central vein inter-ventions are performed.
METHODS TO AVOID COMPLICATIONS
Careful planning of every intervention is the bestway to prevent complications. Planning shouldinclude as many technical details of the inter-vention as possible, including special patient fac-tors such as comorbidities, prior interventions orsurgeries, and anatomic details. Ideally, alterna-tive plans should be developed for every step ofthe intervention. In the way of: ‘what if?’ A well-defined strategy makes it easier to stop and adaptduring a case when things are not going the waythey are supposed to go. During the planningthe achievability of the intervention should beassessed and alternative options should be con-sidered. The interventionalist should always keepin mind that doing nothing is also an option,especially if the patient is not very sympto-matic. For venous intervention the endovascularapproach is often less invasive and as effective assurgery. However, there are situations where thesurgical option is preferable. The best example isthe venous thoracic outlet syndrome, also calledthe Paget–von Schrötter syndrome. In this con-dition the subclavian vein is compressed betweenthe first rib and the clavicle. This condition, whichwould better be named thoracic inlet syndrome,is best treated with surgical resection of the com-pressing bone structure. Stenting of the subcla-vian vein has a high risk of stent malfunctioning,especially in young and active individuals, andshould therefore be avoided.12
SUMMARY
Venous interventions are overall safe and effec-tive. The key to avoid complications is good pre-procedural planning, assessment of every singlestep during the procedure, and automatisms incase a complication occurs. If a problem such asan extraluminal guidewire is recognized early, apossible complication can be avoided. Automa-tisms such as re-inflating the balloon or manualcompression can help to gain time to decideabout the next step. Most complications can bedealt with by endovascular means. Nevertheless,a surgical back-up is important, especially whenworking in the central venous system close tothe heart.
CHECK LIST FOR EMERGENCY EQUIPMENT
Large diameter angioplasty balloons
• 12–26 mm Atlas PTA Dilation catheter (BardPeripheral, Tempe, AZ).
Occlusion balloons
• 20–40 mm Equalizer (Boston Scientific,Natick, MA).
Large bare stents
• 16–24 mm Wallstent (Boston Scientific,Natick, MA).
• 20–35 mm Gianturco Rosch Z stent (Cook,Bloomington, IN).
Covered stents
• 10–14 mm Wallgraft (Boston Scientific,Natick, MA).
Aortic stent graft extensions
• 23, 26, 28.5 mm aortic extender (Excluder,WL Gore & Associates, Inc, Flagstaff, AZ)
• 22–32 mm main body extension (Zenith,Cook, Bloomington, IN).
Large diameter sheath to accommodate abovedevices
• 16–24 Fr Check-Flo introducers (Cook,Bloomington, IN).
Snares
• 15 mm and 25 mm Amplatz Goose NeckSnare (ev3, Plymoth, MI)
VENOUS INTERVENTIONS 227
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 227

• 12–20 mm and 18–30 mm EN snare (intervMedical Device Technologies, Inc, Gainesville,FL).
Retrievable filters for protection during throm-bolysis
• Recovery G2 (Bard Peripheral, Tempe, AZ)• Gunther Tulip (Cook, Bloomington, IN)• Optease (Cordis, Miami Lakes, FL).
Thrombolytics
• 2 mg alteplase (Cathflow Activase, Genen-tech, South San Francisco, CA).
REFERENCES
1. Welber A, Schur I, Sofocleous CT et al. Endovascularstent placement for angioplasty-induced venous rup-ture related to the treatment of hemodialysis grafts. J Vasc Interv Radiol 1999; 10: 547–51.
2. Bansal R, Agarwal SK, Tiwari SC et al. A prospectiverandomized study to compare ultrasound-guided withnonultrasound-guided double lumen internal jugularcatheter insertion as a temporary hemodialysis access.Ren Fail 2005; 27: 561–4.
3. Koroglu M, Demir M, Koroglu BK et al. Percutaneousplacement of central venous catheters: comparing theanatomical landmark method with the radiologicallyguided technique for central venous catheterizationthrough the internal jugular vein in emergent hemodial-ysis patients. Acta Radiol 2006; 47: 43–7.
4. Kinney TB. Update on inferior vena cava filters. J VascInterv Radiol 2003; 14: 425–40.
5. Salgado OJ, Chacon RE, Alcala A et al. Vein wall disse-cion: a rare puncture-related complication of brachio-cephalic fistula. Gray-scale and color Doppler sonographicfindings. J Clin Ultrasound 2005; 33: 464–7.
6. Oshima K, Takahashi T, Ishikawa S et al. Superior venacava rupture caused during balloon dilation for treat-ment of SVC syndrome due to repetitive catheter abla-tion – a case report. Angiology 2006; 57: 247–9.
7. Lang EV, Reyes J, Faintuch S et al. Central venousrecanalization in patients with short gut syndrome:restoration of candidacy for intestinal and multivisceraltransplantation. J Vasc Interv Radiol 2005; 16: 1203–13.
8. Borstlap AC, Lampmann LE. Balloon rupture and arte-riovenous communication – a rare complication oftransluminal angioplasty. Vasa 1993; 22: 352–4.
9. Dev V, Kaul U, Mathur A. Pin hole balloon ruptureduring coronary angioplasty causing dissection andocclusion of the coronary artery. Ind Heart J 1991; 43:393–4.
10. Alfonso F, Perez-Vizcayno MJ, Hernandez R et al.Clinical and angiographic implications of balloon
rupture during coronary stenting. Am J Cardiol 1997;80: 1077–80.
11. Rajan DK, Clark TW, Patel NK et al. Prevalence andtreatment of cephalic arch stenosis in dysfunctionalautogenous hemodialysis fistulas. J Vasc Interv Radiol2003; 14: 567–73.
12. Phipp LH, Scott DJ, Kessel D et al. Subclavian stentsand stent-grafts: cause for concern? J Endovasc Surg1999; 6: 223–6.
13. Sanchez RB, Roberts AC, Valji K et al. Wallstent mis-placed during transjugular placement of an intrahepaticportosystemic shunt: retrieval with a loop snare. Am JRoentgenol 1992; 159: 129–30.
14. Martin M, Baumgartner I, Kolb M et al. Fatal pericardialtamponade after Wallstent implantation for malignantsuperior vena cava syndrome. J Endovasc Ther 2002; 9:680–4.
15. Brant J, Peebles C, Kalra P et al. Hemopericardium aftersuperior vena cava stenting for malignant SVC obstruc-tion: the importance of contrast-enhanced CT in theassessment of postprocedural collapse. CardiovascInterv Radiol 2001; 24: 353–55.
16. Smith SL, Manhire AR, Clark DM. Delayed spontaneoussuperior vena cava perforation associated with a SVCwallstent. Cardiovasc Interv Radiol 2001; 24: 286–7.
17. Binkert CA, Petersen BD. Two fatal complications afterparallel tracheal-esophageal stenting. Cardiovasc IntervRadiol 2002; 25: 144–7.
18. Izutani H, Lalude O, Gill IS et al. Migration of an infe-rior vena cava filter to the right ventricle and literaturereview. Can J Cardiol 2004; 20: 233–5.
19. Putterman D, Niman D, Cohen G. Aortic pseudo-aneurysm after penetration by a Simon nitinol inferiorvena cava filter. J Vasc Interv Radiol 2005; 16: 535–8.
20. Feezor RJ, Huber TS, Welborn MB 3rd et al. Duodenalperforation with an inferior vena cava filter: an unusualcause of abdominal pain. J Vasc Surg 2002; 35: 1010–12.
21. Athanasoulis CA, Kaufman JA, Halpern EF et al.Inferior vena caval filters: review of a 26-year single-center clinical experience. Radiology 2000; 216: 54–66.
22. Reyes BL, Trerotola SO, Venbrux AC et al. Percutaneousembolotherapy of adolescent varicocele: results and long-term follow-up. J Vasc Interv Radiol 1994; 5: 131–4.
23. Savage C, Ozkan OS, Walser EM et al. Percutaneousretrieval of chronic intravascular foreign bodies. Cardio-vasc Interv Radiol 2003; 28: 28.
24. Egglin TK, Dickey KW, Rosenblatt M et al. Retrieval ofintravascular foreign bodies: experience in 32 cases.Am J Roentgenol 1995; 164: 1259–64.
25. Lee KH, Han H, Lee KJ et al. Mechanical thrombectomyof acute iliofemoral deep vein thrombosis with use ofan arrow-trerotola percutaneous thrombectomy device.J Vasc Interv Radiol 2006; 17: 487–95.
26. Allie DE, Hebert CJ, Lirtzman MD et al. Novel simul-taneous combination chemical thrombolysis/rheolytic
228 COMPLICATIONS IN PERIPHERAL VASCULAR INTERVENTIONS
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 228

thrombectomy therapy for acute critical limb ischemia:the power-pulse spray technique. Cathet CardiovascInterv 2004; 63: 512–22.
27. Mewissen MW, Seabrook GR, Meissner MH et al.Catheter-directed thrombolysis for lower extremity deepvenous thrombosis: report of a national multicenterregistry. Radiology 1999; 211: 39–49.
28. Yamagami T, Kato T, Iida S et al. Gunther tulip inferiorvena cava filter placement during treatment for deepvenous thrombosis of the lower extremity. CardiovascInterv Radiol 2005; 28: 442–53.
29. Tsai J, Georgiades CS, Hong K et al. Presumed pulmonaryembolism following power-pulse spray thrombectomy
of upper extremity venous thrombosis. CardiovascInterv Radiol 2006; 18: 18.
30. Rundback JH, Leonardo RF, Poplausky MR et al. Venousrupture complicating hemodialysis access angioplasty:percutaneous treatment and outcomes in seven patients.Am J Roentgenol 1998; 171: 1081–4.
31. Castelli P, Caronno R, Piffaretti G et al. Emergencyendovascular repair for traumatic injury of the inferiorvena cava. Eur J Cardiothorac Surg 2005; 28: 906–8.
32. de Gregorio Ariza MA, Gamboa P, Gimeno MJ et al.Percutaneous treatment of superior vena cava syn-drome using metallic stents. Eur Radiol 2003; 13:853–62.
VENOUS INTERVENTIONS 229
cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 229

cpvi_chapter15.qxp 4/5/2007 2:50 PM Page 230

abciximab 55, 73, 76, 77, 130–1, 195abdominal aortic aneurysms (AAAs)
endovascular treatment 139–40see also endovascular aortic aneurysm
repair (EVAR)open surgical repair 139size and outcome 149–50
access site(s)arterial and venous 51closure 66–7evaluation 21location and risk of complications 55–6, 65, 65,
66, 103–4see also specific interventions
access site complications 51–69, 149closure device-associated 56, 57detection methods 56–7, 58emergency equipment checklist 67frequency 51manual compression-associated 56prevention 65–7, 65, 66risk factors 55–6treatment options 57–8
coil embolization 63, 65compression 58stent graft implantation 59–63, 63, 64stent implantation 57, 59thrombin injection 58–9, 61, 62vascular surgery 58
typesarteriovenous fistulas 54, 54blood loss 52–3, 52infection 53pseudoaneurysms 53, 53, 54vessel dissection/occlusion 54
venous interventions 219acetylcysteine (ACC) 31, 35, 172acetylsalicylic acid see aspirinacute renal failure (ARF)
cholesterol emboli and 33see also contrast media induced acute renal
failure (CM-ARF)acute vessel occlusion 10
adenosine antagonists 31age and renal/mesenteric artery intervention
complications 166ALARA principle 39, 42allergies
iodinated contrast media 17, 34, 111streptokinase 81, 82, 93
amiodarone 23anemia 17, 30, 30AneuRx trial 145aneurysms
carotid 100, 101intracranial 110renal artery 170, 171see also endovascular aortic aneurysm
repair (EVAR)angiography
access site complication detection 57first performance of 40needle 66rotational 44–5see also radiotoxicity; specific vessel areas
Angiojet device 210angioplasty complications
frequency after elective procedures 3–4, 4, 15target site 4–6, 5, 6, 7see also balloon angioplasty; specific vessel
areas/scenariosAngioseal device 56, 57anistreplase 84anti-arrhythmic drugs 23anticoagulant drugs 23, 72, 73–5
see also specific drugsantiplatelet drugs 4–5, 55, 72
see also specific drugsantispasmodic drugs 206antithrombotic drugs 72
see also specific drugsaortic access complications 103–4aortic aneurysmal disease repair
open surgery 139see also endovascular aortic aneurysm repair
(EVAR)
Index
Page numbers in italics refer to tables and figures.
cpvi_index.qxp 4/5/2007 3:29 PM Page 231

aortic aneurysm rupture 148aortic dissection 98, 99, 139aortic morphology
neck angulation and EVAR complications 150and renal artery intervention complications 166–7
aortic stenosis 179–80aortic stent graft extensions 26aorto-iliac intervention complications 177–85
avoidance 182detection
delayed complications 181–2procedural complications 181
emergency equipment checklist 184frequency 177identification of high risk patients 178–9specific steps and tools
occlusion 180–1stenosis 179–80
target site 177–8, 178, 179treatment
acute closure 182, 183arterial rupture 183, 184delayed closure 182–3distal embolization 183–4stent infection 184
aorto-iliac occlusions 180–1argatroban 17, 75arterial access sites 51
see also access site complicationsarteriovenous (AV) fistulas 5, 6, 54, 54artificial coagulation disorders and access site
complications 55aspiration thrombectomy 25, 171, 183–4, 214, 215aspirin
adverse effects 55, 71–2dosage 71, 77intolerance 72platelet inhibitory effects 71resistance 72reversal of effects 77, 78
Asymptomatic Carotid Atherosclerosis Study(ACAS) 97
atherectomy device use 189, 190, 190, 195, 203atherosclerosis as systemic disease 13atropine 23, 56axillary access 55
bail-out equipment 22–6balloon angioplasty
cutting balloon 25, 203, 213, 213development 3dissection after 5, 6rupture during 6, 7, 9–10, 178
vein rupture 220, 223, 224
ultrasound-guided 192see also specific vessel areas/scenarios
balloons 25beta-blockers 17, 18BIAS II report 177, 178bivalirudin 5, 17, 23, 74, 195bleeding complications of pharmacologic
interventionsabciximab 73, 76aspirin 71avoidance 77clopidogrel 72–3diagnostic methods 76direct thrombin inhibitors 74heparin 74thrombolysis 75, 81treatment 76–7, 78
blood loss, access site 52–3, 52bowel infarctions after mesenteric artery
interventions 159brachiocephalic access complications 103–4brachiocephalic (innominate) artery 118–19brachytherapy after femoropopliteal angioplasty
195–6buttock claudication 148–9
cancer risk from diagnostic X-rays 41–2CAPRIE trial 72cardiac tamponade 223CardioMEMS pressure sensor 144, 146cardiovascular comorbidity
prevalence 13–14risk evaluation
data in the literature 14–15recommendations 15
care standards 21–2carotid angioplasty and stenting (CAS), patient
preparation 103carotid angioplasty and stenting (CAS) complications
atherosclerotic carotid artery disease 97avoidance methods 112–13detection 11emergency equipment checklist 113–14high risk patients 100–3, 102intracranial complications 108–10, 109, 110low risk patients 103non-atherosclerotic carotid artery disease 97–8
dissection 98fibromuscular dysplasia 98–9, 100pseudoaneurysm/aneurysm 100, 101
risk scores 14specific interventional steps
aortic/brachiocephalic access 103–4distal embolic protection 105–8
232 INDEX
cpvi_index.qxp 4/5/2007 3:29 PM Page 232

femoral artery access 103guide catheter placement 104–5, 105
systemic complications 110–11treatment 111–12
carotid arteryacute occlusion during stent implantation 10dissections 98preoperative investigations 15vasospasm 107
carotid endarterectomy (CEA) 97, 101catheters, choice of 24caval filters
complications with 223retrievable 26, 224
celiac artery interventions, frequency ofcomplications 159
cephalic arch rupture 220, 224cholesterol embolization 7, 33, 164, 166, 168, 178cigarette smoking and endovascular intervention
complications 188clopidogrel 72–3, 194
dosage 77reversal of effects 77, 78
closure devicescomplications 56, 57use of 66–7
CM-ARF see contrast media induced acute renalfailure (CM-ARF)
coagulation disorder patients 16–17, 55coil embolization
causing hip/buttock claudication 149clinical use 63, 65, 77, 170, 191, 223coil types 25
coil stents 192, 194collateral (type II) endoleaks 141, 142–3, 143compartment syndromes 10, 53complications in peripheral vascular interventions
3–12classification 9device-related 8distal to the target site 6–7frequency 3–4, 4prevention 8–9site of angioplasty 4–6, 4, 5, 6, 7systemic 7vascular access site 4, 4, 5worst scenarios 9–11see also specific complications and vessel areas
compression of puncture sitesmanual 56, 58ultrasound guided 58
computed tomography (CT)assessment of postinterventional bleeding 57endoleak detection 141
congestive heart failure (CHF) and renal function 166contrast media, allergic reactions to 17, 34, 111contrast media induced acute renal failure (CM-ARF)
10, 27–37, 111clinical importance 27–8, 28definition 27frequency 28–9, 29prevention
drugs 31intravenous hydration 30–1postinterventional hemodialysis/hemofiltration
31–3, 33strategy 35
risk factors 29–30treatment 34
contrast media induced complications (non-ARF) 34coronary heart disease (CHD) prevalence in PAOD
patients 13–14crash carts 23creatinine 16critical limb ischemia (CLI)
laser-assisted angioplasty 195see also tibioperoneal intervention complications
cryoplasty 190, 196CURE trial 72cutting balloons 25, 203, 213, 213
danaparoid 17deep femoral artery 187–8deep venous thrombosis (DVT)
due to vessel compression by hematomas 52–3thrombectomy 223–4thrombolytic therapy 85, 87–9, 223–4
dehydration and CM-ARF 29–30deterministic risks 40device-related complications 8diabetes mellitus patients
cardiovascular risk evaluation 15CM-ARF risk 30, 30peri-interventional management 16risk during renal artery interventions 166risk during tibioperoneal interventions 202
direct thrombin inhibitors 74–5, 78dissection
as access site complication 54after balloon angioplasty 5, 6aortic 98, 99, 139avoidance at distal sites 6carotid 98hemodialysis fistula complication 212, 212iliac artery 182, 183renal artery 160, 162, 168, 169, 169subclavian artery 119, 124, 125–6, 125, 127vertebral artery 119, 125, 127
INDEX 233
cpvi_index.qxp 4/5/2007 3:29 PM Page 233

distal embolic protection (DEP)complications in carotid stenting 105–8see also embolic protection devices
distal embolizationduring thrombolytic therapy 92see also embolization; specific vessel areas/scenarios
dopamine 23dose area products (DAPs)
definition 40variations in 39, 40
drugsemergency use 22–3implicated in CM-ARF 30see also specific drugs
duplex-guided balloon angioplasty in renal patients 192
duplex sonographyaccess site assessment 21, 56–7, 58endoleak detection 141pseudoaneurysm detection 76renal artery 169, 171subclavian artery 128vertebral artery 128, 129
Dutch Randomized Endovascular AneurysmManagement (DREAM) trial 140
effective dose (ED) 40Ehlers–Danlos syndrome 99, 103elective angioplasty, frequency of complications 3–4Elgiloy 148embolectomy see thrombectomyembolic protection devices 26, 106–8, 131, 194–5,
223, 224embolization
aorto-iliac interventions 178, 183–4cholesterol 7, 33, 164, 166, 168, 178during thrombolytic therapy 92external carotid artery interventions 104–5femoropopliteal interventions 188, 194–5hemodialysis fistulas and grafts 213–14, 215liquid embolization agents 25peripheral 6–7, 8renal artery interventions 164, 168subclavian and vertebral artery interventions
127, 130–1tibioperoneal interventions 202, 203, 204, 205of veins 223see also coil embolization
EmboShield 106, 107emergency drugs 22–3emergency tools 23–4
see also specific vessel areas/scenariosendoleaks 140–1
classification system 141
types I-IV 141–4, 142, 143, 144type V 144–5, 145, 146
endotension (type V endoleak) 144–5, 145, 146endovascular aortic aneurysm repair (EVAR)
advantages 139–40anatomic criteria 151, 152aneurysm-related death rates 140emergency equipment 153measurement of aortic dimensions 152secondary intervention rates 140
endovascular aortic aneurysm repair (EVAR)complications 139–58
access artery injury 149avoidance methods 151, 152endoleaks 140–1
classification system 141diagnosis 141types I-IV 141–4, 142, 143, 144type V (endotension) 144–5, 145, 146
hip and buttock claudication 148–9renal compromise with suprarenal stent use 149risk factors 149–51rupture 148, 148stent fracture 147–8stent migration 147
frequency 145prevention 146–7risk factors 145–6
thoracic aortic disease 151thrombosis 148
endovascular therapyevolution of 3risk evaluation 13–19
entrance skin air kerma (ESAK) 39–40entrance skin radiation dose 40EPIC trial 73epinephrine 22–3European Imaging in Carotid Angioplasty and Risk
of Stroke (ICAROS) study 106EUROSTAR registry 144–5, 148, 150EVAR see endovascular aortic aneurysm repairexcimer laser angioplasty (ELCA) of renal in-stent
restenoses 43, 43external carotid artery (ECA)
embolism 104–5wire perforation 104, 105
femoral artery access, carotid stenting 103femoropopliteal intervention complications 187–99
avoidance methodsapproach choice 192imaging techniques 192patient selection 192restenosis prevention 195–6
234 INDEX
cpvi_index.qxp 4/5/2007 3:29 PM Page 234

stent choice 192–4, 193, 194stent thrombosis/distal embolization prevention
194–5causes of interventional failure 188detection 191emergency equipment checklist 197risk factors 188specific steps and tools 188–9
imaging 189puncture site 189wire passage 189stenting/ballooning 190other devices 190
treatment 191–2, 191type and frequency 187–8when to stop 196
fenoldopam 31fibrinolytic therapy
characteristics of agents 83contraindications 81, 82see also thrombolytic therapy
fibromuscular dysplasia (FMD) 98–9, 100, 103, 122filter devices 26, 106–8, 131, 194–5, 223, 224fluids 23fondaparinux 17foot microemboli 7, 8
glomerular filtration rate (GFR) 16glycoprotein (Gp) IIb/IIIa inhibitors 23, 73, 75, 77, 78graft-related endoleaks (types I and III) 141–2, 141,
142, 143, 144
heart failure 15hematomas as access site complications 51, 52–3, 52hemodialysis fistulas and grafts, complications of
percutaneous management 209–17arterial embolization 213–14, 215avoidance methods 215–16bleeding problems 213emergency equipment checklist 216frequency and types 209–10immature fistulas 210–11infection 215pulmonary embolism 214–15stent complications 215technical complications 211–13, 211, 212, 213thrombosed graft treatment 210transarterial access complications 211
hemodialysis/hemofiltrationprevention of CM-ARF 31–3, 33treatment of CM-ARF 34
heparindosage 23DVT treatment 87
low molecular weight 55, 74, 78monitoring 23, 76neutralization with protamine 23, 77, 78, 171pulmonary embolism treatment 89–90, 90, 91unfractionated 73–4, 77, 77, 78
heparin-induced thrombocytopenia 17hip claudication 148–9hirudin 74hydration, preintervention 172hypersensitivity reactions to contrast media 34hypertensive patients, peri-interventional
management 16hyperthyroidism 34
iliac arterydissection 182, 183rupture 183, 184stenosis 179–80tortuosity and access difficulties 166see also aorto-iliac intervention complications
ilipsoas hematomas 52imaging techniques
bleeding complication detection 76–7endoleak detection 141preprocedure assessment 21–2see also specific techniques
infectionsaccess site 53hemodialysis patients 215stent 8, 178, 181, 184, 215
innominate artery 118–19International Study of Unruptured Intracranial
Aneurysms (ISUIA) 110intracoronary sonotherapy 196intracranial aneurysms 110intracranial complications of carotid stenting
108–10, 109, 110, 112, 113intracranial hemorrhage (ICH) 109–10, 110,
112, 113intravascular ultrasound (IVUS) 129iodinated contrast media, allergic reactions 17,
34, 111iodine-induced thyrotoxicosis 16iodixanol 29, 29, 30, 34, 172iohexol 29, 29, 34iomeprol 29iopamidol 29, 30, 34iopentol 29, 29iopromide 29, 34iotrolan 34ioxilan 29, 29ischemia during endovascular treatment 10
see also specific vessel areas/scenariosischemic stroke, thrombolytic therapy 90–1
INDEX 235
cpvi_index.qxp 4/5/2007 3:29 PM Page 235

236 INDEX
kidney diseasepreoperative identification 15–16see also renal and mesenteric artery intervention
complications
Laser Angioplasty for Critical Limb Ischemia (LACI)trials 195
laser-assisted angioplasty 190, 195, 203lepirudin 17, 74limb ischemia
laser-assisted angioplasty 195thrombolytic therapy 86–7, 87, 88, 89see also tibioperoneal intervention complications
liquid embolic agents 25low molecular weight heparins (LMWH) 55, 74, 78lung disease, preoperative identification 15
magnetic resonance angiography (MRA)endoleak detection 141infrapopliteal segment 189renal artery 171, 172
manual compression of puncture sites 56, 58MATCH trial 72medical history 21mesenteric artery interventions
frequency and types of complications 159–60see also renal and mesenteric artery intervention
complicationsmetformin 16microembolization 7, 8monorail (rapid exchange; RX) systems 172myocardial infarction
carotid stenosis patients 100, 111perioperative 14
needles, choice of 65nephrectomy 171nephrogenic systemic fibrosis 171nifedipine 131nitinol 147nitroglycerin 23North American Symptomatic Carotid
Endarterectomy Trial (NASCET) 97, 110
occlusion balloons 25oral anticoagulation 74
Paget–von Schrötter syndrome (venous thoracicoutlet syndrome) 227
pain control 18paraplegia after thoracic endovascular grafting 151patient care standards 21–2PercuSurge device 106, 107percutaneous thrombolytic device (PTD) 210, 214
peripheral arterial occlusive disease (PAOD)mortality rate 14prevalence of cardiovascular comorbidity 13–14
peripheral embolization 6–7, 8pharmacologic interventions
avoidance of complications 77contraindications 75, 75detection and treatment of complications 76–7,
76, 78reversal of effects 77, 78see also specific drugs
photodynamic therapy 196PIVOTAL trial 150plasmin 81–2plasminogen 82platelet counts and access site complications 55platelet glycoprotein (GP) IIb/IIIa receptor
inhibitors 23, 73, 75, 77, 78popliteal access
arteriovenus fistula risk 54puncture technique 65, 189
popliteal fossa, compartment syndrome 10, 11postphlebitic syndrome 87, 93pressure bandage use 67PROACT II study 90procoagulant substances 23PROMPT study 73prostatic hypertrophy 16protamine 23, 77, 78, 171protection devices 26
see also specific devicesprothrombin complex concentrate 23prourokinase 90Prourokinase versus Urokinase for Recanalization of
Peripheral Occlusions: Safety and Efficacy(PURPOSE) trial 84
proximal balloon occlusion systems 26pseudoaneurysms 53, 53, 54
carotid 100detection and treatment 76–7, 76, 77, 100
pulmonary disease, preoperative identification 15pulmonary embolism (PE)
avoidance using retrievable filters 224following hemodialysis access declotting 214–15thrombolytic therapy and 87, 89–90, 90, 93
puncture technique 65–6
radiotherapy after femoropopliteal angioplasty 195–6radiotoxicity 39–47
deterministic effects 39, 40–1, 40, 41diagnosis and therapy 45–6operator exposure 45, 45prevention measures 42–5, 42, 43, 44relevant definitions 39–40
cpvi_index.qxp 4/5/2007 3:29 PM Page 236

risk factors 42stochastic effects 41–2training in radiation reducing techniques 46variation in patient radiation exposure 39, 40
rapid exchange (RX) systems 172renal disease, preoperative identification 15–16renal and mesenteric artery intervention
complications 159–75avoidance methods
preprocedure 171–2atraumatic technique 173, 173choice of wire 172–3pressure measurement 173stent deployment 173–4protection devices 174final angiography 174use of rapid exchange systems 172
detection methods 168–9emergency equipment checklist 174–5frequency and types 159–60, 165
dissection 160, 162, 168, 169, 169perforation 163–4, 164, 165renal failure 165rupture 9–10, 160, 163, 163spasm 164stent misplacement 160, 161, 162thrombosis/embolization 164, 166
identification of high risk patientsanatomic factors 165–6, 166–8comorbidities 165, 166
specific steps and tools 168treatment
endovascular 169–71, 169, 170, 171medical 171surgical 171
REPLACE-2 trial 74reteplase (r-PA)
bleeding complications 85, 85, 86characteristics 83DVT treatment 85, 89
retinal embolism 104, 105retrieval devices 25retroperitoneal bleeding 52rheolytic thrombectomy 24–5, 210risk identification before endovascular intervention
13–19, 21importance 13minimal program 18non-vascular comorbidity 15–17vascular comorbidity 13–15
risk reduction using drugs 17–18rotational angiography 44–5rupture 9–10
see also specific vessel areas/scenarios
seizures during carotid interventions 110–11Seldinger technique 65–6sharp recanalization 220, 222sheaths
choice of 24size and risk of complications 55
SilverHawk system 190, 195, 203sirolimus-eluting stents 195skin reactions to radiation 40–1, 40, 41snares 25, 223sonotherapy 196spasm
brachiocephalic vessels 131carotid artery 107renal artery 164tibial vessels 202, 206
spinal cord ischemia after thoracic endovasculargrafting 151
statins 17–18stenosis, aorto-iliac 179–80stent graft implantation for access site complications
59–63, 63, 64Stenting and Angioplasty with Protection in Patients
at High Risk for Endarterectomy (SAPPHIRE)trial 97, 111
stent(s)covered 25, 170, 171fracture 147–8implantation for access site complications 59infection 8, 178, 181, 184, 215migration after EVAR 145–7, 147misplacement in renal artery interventions 160,
161, 162selection
femoropopliteal region 192–4, 193, 194subclavian region 125
sirolimus-eluting 195suprarenal 149thrombosis 5, 91, 164, 168, 194, 215types and uses 25–6venous intervention complications 221, 223, 225see also specific vessel areas/scenarios
STILE trial 87stochastic risk 40streptokinase
allergic reactions to 81, 82, 93characteristics 83contraindications 82pharmacokinetics 82, 84
strokeas complication of carotid stenting 104, 108thrombolytic therapy 90–1
subclavian artery endovascular interventionsaccess site choice 122, 124
INDEX 237
cpvi_index.qxp 4/5/2007 3:29 PM Page 237

subclavian artery endovascular interventions(Continued)
indications for 117, 118physiologic protection mechanism 127stent selection 125wire selection 124–5
subclavian artery intervention complications 117–38avoidance 120, 131, 131detection
preoperative assessment 128, 128operative assessment 128–9
emergency equipment checklist 132–3follow-up 132frequency and type 117–18, 119, 121–2identification of high risk patients 118–19, 132specific steps and tools 122–8, 125, 126, 127
dissection 119, 124, 125–6, 125, 127thrombosis/embolization 126–7wall injuries 126, 127
treatmentarterial spasm 131perforations 129–30thromboses/emboli 130–1
subintimal recanalization 202–3superficial femoral artery (SFA) 187
Takayasu’s arteritis 122TALON (Treating Peripherals with Silverhawk:
Outcomes Collection) registry 203tenecteplase (TNK) 83, 86theophylline 31thoracic aortic aneurysms
endovascular grafting (EVG) 151incidence 139indications for endovascular repair 140open surgical repair 139see also endovascular aortic aneurysm repair
(EVAR) complicationsthrombectomy, mechanical
DVT 223–4femoropopliteal artery occlusions 195hemodialysis shunt thrombosis 210rheolytic thrombectomy 24–5, 210see also aspiration thrombectomy
thrombin inhibitors, direct 74–5, 78thrombin injection 58–9, 61, 62, 77thrombolysis catheters 24Thrombolysis or Peripheral Arterial Surgery
(TOPAS) trial 84, 87Thrombolysis and Thrombin Inhibition in
Myocardial Infarction (TIMI) 9B trial 74thrombolytic therapy
contraindications 75, 81, 82during venous interventions 226
DVT 85, 87–9, 223–4hemodialysis access declotting 214renal and mesenteric artery thrombosis 170–1
thrombolytic therapy complications 81–96clinical application-related
acute ischemic stroke 90–1acute limb ischemia 86–7, 87, 88, 89, 203DVT 85, 87–9, 223–4pulmonary embolism 87, 89–90, 90, 93stent thrombosis 91
detection 91–2fibrinolytic agent-related 81–2, 83
reteplase 85, 85, 86streptokinase 81, 82–4, 93tenecteplase 86tissue plasminogen activator 84–5, 85urokinase 84, 85, 85
management 92–3types 81
thrombosisafter EVAR 148haemodialysis shunt 210renal artery interventions 164stent 5, 91, 164, 168, 194, 215subclavian artery interventions 126–7venous 226–7see also deep venous thrombosis (DVT)
thyrotoxicosis, iodine-induced 16, 34tibioperoneal intervention complications 201–7
avoidance 205–6detection 205emergency equipment checklist 207frequency 201–2identification of high risk patients 202specific steps and tools 202–5, 203, 204treatment 203, 204, 205
tibioperoneal interventions, indications 201tissue plasminogen activator (t-PA)
acute ischemic stroke treatment 90–1characteristics 83complications 84–5, 85DVT treatment 88–9limb ischemia treatment 86–7, 87, 88, 89
tourniquets 23tracheostomy sets 23transbrachial access 55, 65transfemoral access 55, 65transradial access 55, 56, 65, 65, 66Treating Peripherals with Silverhawk: Outcomes
Collection (TALON) registry 203
ultrasonographyaccess site assessment 21, 56–7, 58balloon angioplasty guidance in renal patients 192
238 INDEX
cpvi_index.qxp 4/5/2007 3:29 PM Page 238

compression guidance 58endoleak detection 141intravascular 129pseudoaneurysm detection 76renal artery 169, 171subclavian artery 128thrombin injection guidance 77vertebral artery 128, 129
unfractionated heparin (UFH) 73–4, 77, 77, 78urokinase
characteristics 83, 84combined with abciximab 73complication rates 84, 85, 85DVT treatment 88–9limb ischemia treatment 86–7, 87, 88, 89
urologic disorders 16
vascular surgery 58, 84, 87, 139, 227vasodilators 23vasopressin 23vasopressors 22–3vasovagal reflex induction by manual
compression 56vena caval filters see caval filtersvenous access sites 51, 219
see also access site complicationsvenous dissection 212, 212venous filters 26venous intervention complications 219–29
detection 226emergency equipment checklist 227–8prevention 224, 226, 227risk factors 220specific steps and tools 220–4
guidewire placement 220, 222
angioplasty 220–1, 222, 223, 224stenting 221, 223, 225coil embolization 223filter complications 223thrombectomy 223–4
treatmentof bleeding 226open surgery 227of thrombosis 226–7
types 219venous rupture
general venous interventions 220, 221, 223, 224hemodialysis access interventions 211, 211,
212, 216venous thoracic outlet syndrome 227vertebral artery, anatomic classification of segments
119, 124vertebral artery intervention complications 117–38
detectionpreoperative assessment 128, 128operative assessment 128–9
emergency equipment checklist 132–3follow-up 132frequency and type 117–18, 119, 123identification of high risk patients 119–20,
122, 132specific steps and tools 125–8, 127treatment 129–31
vessel rupture see rupturevitamin K antagonists, reversal of effects 78
wires, choice of 24, 66see also specific interventions
X-rays, cancer risk from 41–2
INDEX 239
cpvi_index.qxp 4/5/2007 3:29 PM Page 239

cpvi_index.qxp 4/5/2007 3:29 PM Page 240