The management of recurrent pelvic malignancy
Pete Sagar
The General Infirmary at Leeds
England




Things could be worse


EXCLUSIVE: SHANE'S AT IT AGAINCheat Aussie star's two-month affairBy Megan Lloyd Davies And Richard Smith
MESSAGES: Warne sent a string of texts
TWO-timing Shane Warne has been caught cheating with ANOTHER woman.


Presentation
• PAIN


The problem
• 8-10 000 cases annually of rectal cancer in the UK
• Local pelvic recurrence in 5-15%

Treatment – radiotherapy/chemotherapy
• Good initial palliation
• Long term survivors are rare
• Reserved for end stage disease
Treatment- surgery
• Multimodality therapy
• Team approach essential
• Technical demands

Preoperative assessment
• Biopsy to confirm diagnosis
• CT chest and abdomen
• MRI pelvis
• EUA
• Fitness for operation

The Leeds MDT meeting

Accommodation for relatives

Accommodation for relatives (NHS)

Patterns of pelvic invasion
• Localised type
• Sacral invasion
• Pelvic side wall invasion

Localized type
• Recurrent tumour is localized to the adjacent tissues or connective tissue

Peri-anastomotic recurrence

Perineal recurrence

Mucinous adenocarcinoma

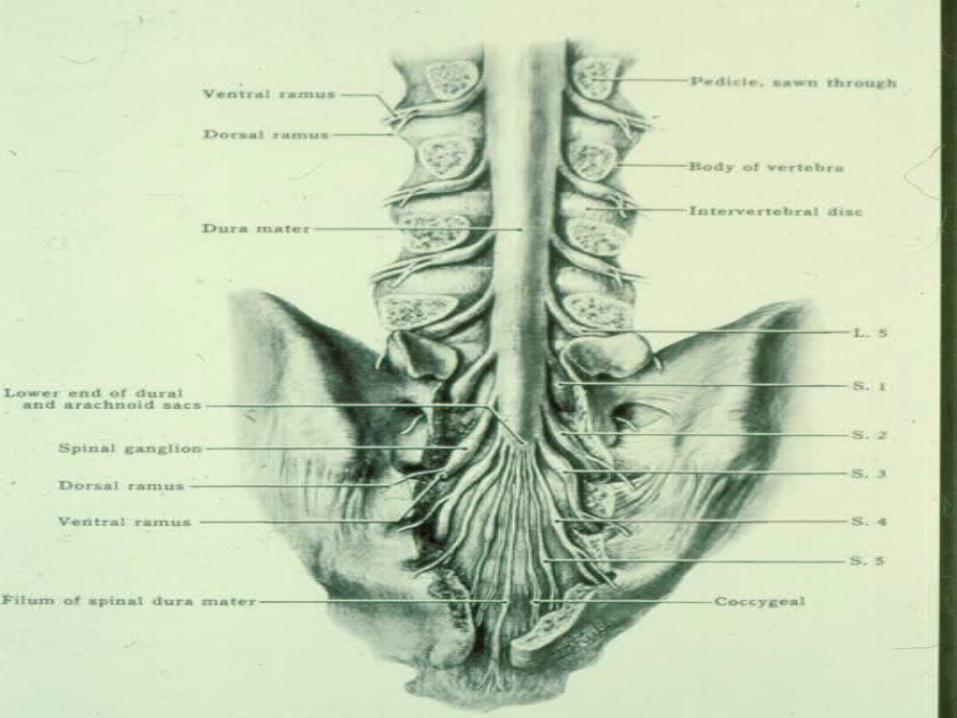
Sacral invasion
• Recurrent tumour invades the lower sacrum (S3, S4, S5) or coccyx

Chordoma with sacral invasion

Sacral invasion- gadolinium enhanced

Lateral invasion
• Recurrent tumour invades pelvic side wall

Pelvic side wall invasion

Vesico-ureteric junction

Planes of attack

APR+S vs TPE+S

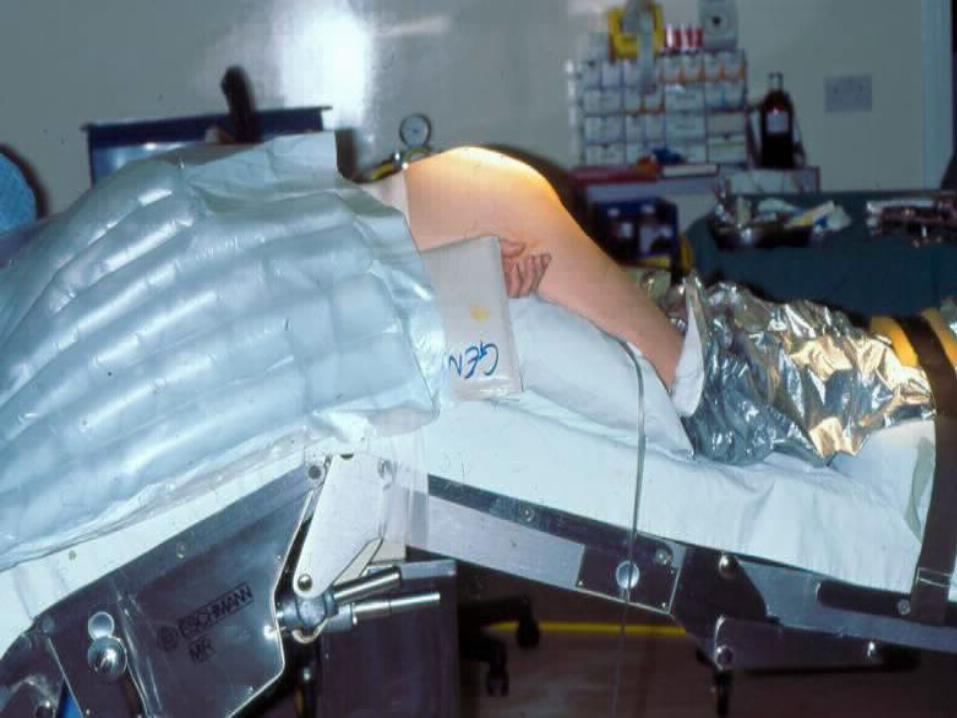





Rectus abdominus flap


Anatomical points



When not to operate

Choose your patient!

Contraindications
• Extrapelvic disease
• Invasion of S1 or S2
• Invasion through greater sciatic notch
• Extensive pelvic side wall involvement
• ASA IV-V

Para-aortic nodal involvement

Greater sciatic notch involvement

Surgical intervention contraindicated

Extension through both greater sciatic foramina

Technical tips

Perianastomotic recurrence

Peri-anastomotic recurrence
• Residual mesentery
• Anticipate tearing around the anastomosis
• Beware the medial course of the ureters

Anterior invasion into bladder
Anterior spread
• Trial dissection
• Plane anterior to the bladder
• APER
• Involve the urologist
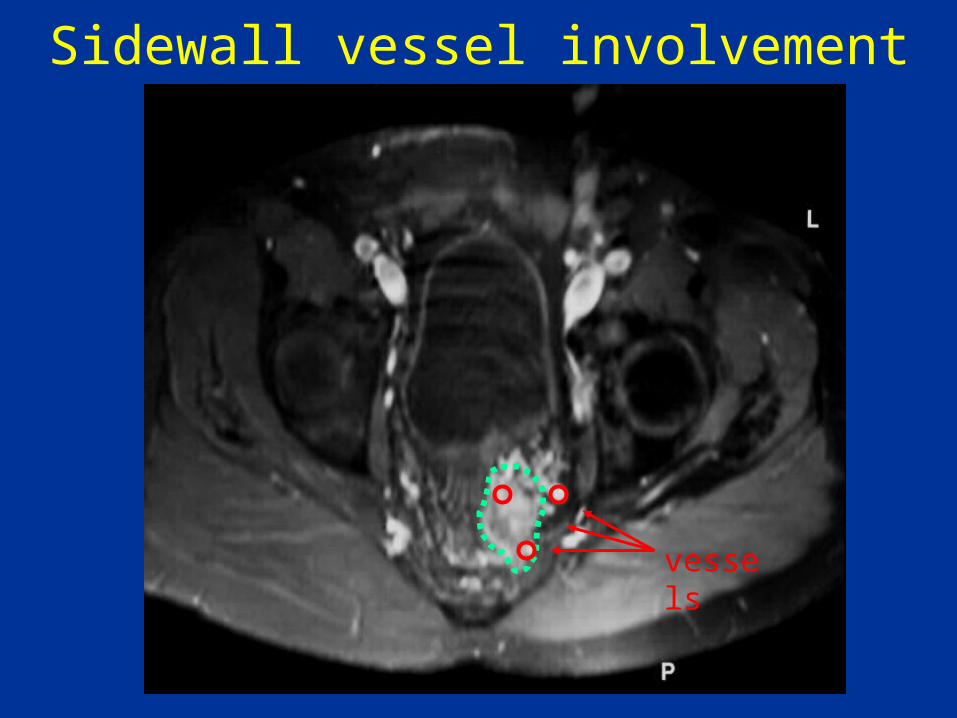
Sidewall vessel involvement
vessels

Pelvic side wall
• BLEEDING
• Suture
• Fibrillar surgicell
• Argon beamer
• Be prepared to pack

Presacral space, no direct invasion

Pre-sacral mass
• Control iliac vessels before dissection of mass
• Incise peritoneum and develop plane between mass and sacrum
• Beware spongy tumour

Direct invasion into the sacrum

Direct invasion of the sacrum
• Choose level of sacrectomy carefully
• Frozen section
• Beware bleeding from pre-sacral veins

Posterior
exenteration
35%

30%
Total
exenteration

Resection of mass alone
15%

9%
Gynaecological clearance

7%
Anterior
exenteration
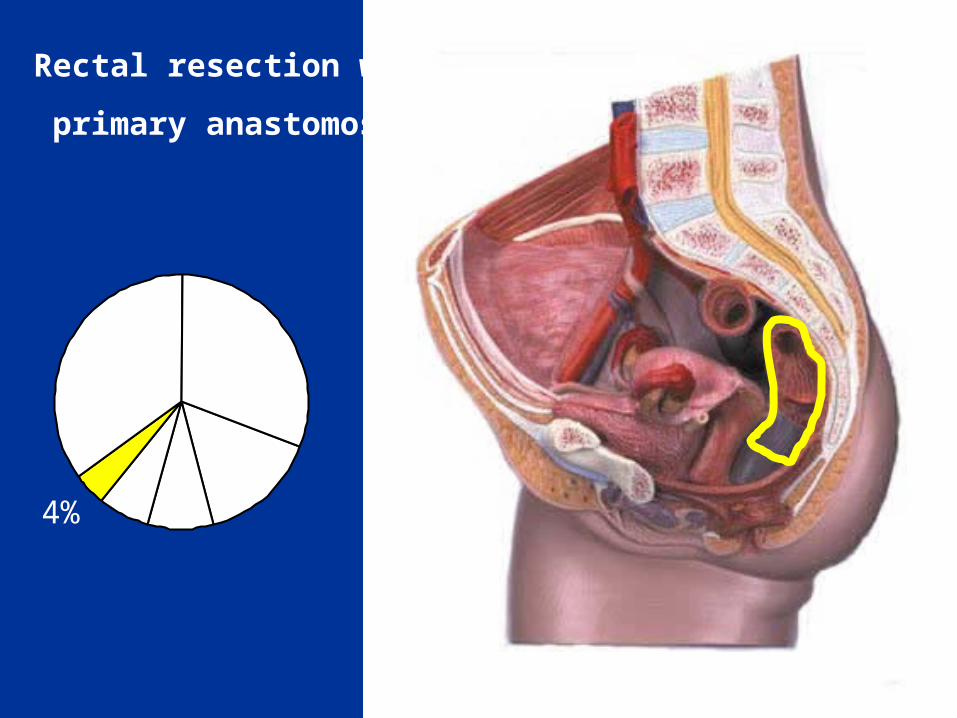
Rectal resection with
primary anastomosis
4%

Sacrectomy
16%

Cumulative survival R0 vs R1 resections


Outcome
• One third will live five years
• One third will recur locally (?re-operate)
• One third will die of disseminated disease

Conclusion
• Multidisciplinary management
• Surgery prime modality
• Surgical team approach essential



ENGLAND WIN THE ASHES



Intra-operative radiotherapy
• Delivery of high biological equivalent
• Dose limiting structures are displaced
• 45-60 Gy EBRT pre op
• Deliver remainder at operation





Best practice?



1-507-284-2511
Recommended