Embed Size (px)
DESCRIPTION
This E book describes various malignant lesions involving hypopharyngeal area and the various management modalities available to manage the same.
Citation preview

Hypopharyngeal malignancy And its management By drtbalu
2009
drtbalu www.drtbalu.co.in
1/1/2009

Hypopharyngeal malignancy
By
Dr. T. Balasubramanian M.S. D.L.O.
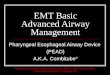
Anatomy: Hypopharynx is the area between the oropharynx superiorly and
oesophagus inferiorly, excluding the larynx. Technically speaking this area includes
1. Both pyriform fossae, 2. Post cricoid region and 3. Posterior pharyngeal wall.
Diagram showing Hypopharynx

Hypopharynx is composed of 4 layers:
1. Mucosal inner lining composed of stratified squamous epithelium
2. Fibrous layer of pharyngeal aponeurosis
3. Muscular layer formed by middle and inferior constrictors
4. Outer layer of fascia, derived from the buccopharyngeal fascia
Posteriorly the Hypopharynx is separated from the prevertebral fascia (this fascia
covers the prevertebral muscles) by a thin layer of areolar tissue. This potential
space is known as retropharyngeal space.
Weak areas of Hypopharynx: Knowledge of weak areas of Hypopharynx will
enable better understanding of tumor spread from this area.
1. The constrictor muscles are thin, especially the superior constrictor. Hence
there is very little resistance to tumor spread via this area.
2. At the junction of inferior constrictor and cricopharyngeas muscle there is
another area of weakness (Killian’s dehiscence).
3. In the lateral pharyngeal wall, where the middle and inferior constrictors
join just below the hyoid bone, there is another weak area.
4. The lateral pharyngeal wall contains the thyrohyoid membrane, through
which the superior laryngeal vessels traverse. This area may facilitate direct
lateral extension of the tumor.
Bulges seen in Hypopharynx: Normally bulges may be seen in the Hypopharynx.
These bulges should be differentiated from tumor mass. The superior horn of
thyroid cartilage sometimes protrudes into the mucosa of lateral pharyngeal wall
causing a confusion submucosal mass. These are usually symmetrical and bilateral.
Large osteophytes on the anterior surface of cervical vertebrae may protrude into
the posterior pharyngeal wall and may be mistaken for a tumor. This is especially
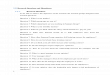
common in old patients.

Figure showing pyriform fossa
Marginal area: This is formed by aryepiglottic folds bilaterally and bridges the
larynx and Hypopharynx. This area is usually considered to be part of Supraglottis.
Nerve supply: The sensory nerve supply to Hypopharynx is via the internal branch
of the superior laryngeal nerve which runs along the anterior wall of pyriform fossa.
Referred Otalgia from Hypopharyngeal growth is due to this nerve.
Features of tumors of Hypopharynx:
1. Tumors of Hypopharynx usually present late in the course of the disease.
2. These tumors are usually aggressive in nature.
3. Tumors of this area usually metastasize to the neck nodes
4. Most of the tumors of this area are large at the time of presentation
5. Submucosal tumor spread is common

6. More than 95% of cancers of Hypopharynx are squamous cell carcinomas
7. Commonly involves patients in their 6th
and 7th
decades (except post cricoid
growth)
8. Even though tumors of this area cause swallowing difficulties, patients
circumvent it by making minor modifications to diet. They rarely seek help
during the early stages of growth.
9. Genetic polymorphism of enzymes that activate tobacco related
protocarcinogens
Etiology:
1. Smoking
2. Alcohol consumption
3. Combination of smoking and alcohol consumption multiplicative
4. Post cricoid and esophageal cancers may be influenced by dietary factors
5. Exposure to welding fumes
6. Radiation exposure
7. Exposure to polycyclic hydrocarbons
8. Deficiency of DNA repair mechanisms commonly associated with Xeroderma
pigmentosa, Bloom’s syndrome, and Fanconi anaemia may predispose to
Hypopharyngeal malignancy.
Epidemiology of post cricoid growth is found to be different from that of other
Hypopharyngeal tumors. It is more common in women and is associated with
Patterson – Brown Kelly syndrome. 30% of patients with Patterson – Brown Kelly
syndrome are associated with post cricoid growth.
Cancers of pyriform fossa:
Pyriform fossa is the most commonly involved site in Hypopharyngeal tumors. It
accounts for more than 65% of Hypopharyngeal malignancies.
It is a potential space that lies on either side of the larynx. They are two in number.
It is shaped like a pyramid with the base pointing above and the apex below. They
belong to the Hypopharyngeal area of the pharynx. It has two parts; the shallow
upper part and a deeper lower part.
Boundaries: The pyriform fossa is bounded laterally by the mucosa covering the
lamina of the thyroid cartilage. Medially it is bounded by the aryepiglottic fold and
arytenoid cartilages above and the cricoid cartilage below. Superiorly it is bounded
by the lateral glosso epiglottic fold (Pharyngoepiglottic fold), inferiorly it continues
with the oesophagus.

Features of pyriform fossa:
1. This is a hidden area which is difficult to examine
2. This area is richly endowed with lymphatics
3. Pyriform fossa tumors are known to metastasize to lymph nodes pretty early
4. Malignant tumors in this area cause referred Otalgia
5. These tumors are aggressive
6. Submucosal spread of tumor is common
7. Commonest tumor of this region is squamous cell carcinoma
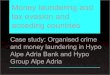
8. True Dysphagia is a fairly late symptom in pyriform fossa growth
Picture showing pyriform fossa growth

Clinical features:
1. In early stages of pyriform fossa growth, patients rarely seek help because it
just presents with sticky sensation in the throat. Depending on the rate of
progression of growth, Dysphagia may eventually occur. Dysphagia initially
starts off for solid foods and eventually the patient finds it difficult to
swallow even liquids.
2. Hoarseness of voice: Possibly due to secondary laryngeal invasion /
involvement of recurrent laryngeal nerve due to post cricoid extension.
3. Neck masses due to nodal metastasis. Hypopharynx is richly supplied with
lymphatics, hence early metastasis to cervical nodes is common.
4. Odynophagia is also one of the presenting features of pyriform fossa growth.
5. Patients are usually under nourished because of Dysphagia
6. Referred Otalgia
7. Unusual symptom can occur rarely in pyriform fossa tumors
8. Since pyriform fossa is a distensible space, the tumor will have to enlarge to a
large size to become symptomatic.
Spread of pyriform fossa tumors:
1. The tumor may spread medially to involve the larynx. The vocal cord may
become fixed due to involvement of cricoarytenoid muscles.
2. Lesions in lateral pyriform fossa may spread over the mucosal surface and
extend superiorly along the lateral pharyngeal wall.
3. They may grow posteriorly to involve the posterior wall of Hypopharynx and
may even reach the opposite pyriform fossa (Horse shoe growth).
4. Tumors of lateral wall of pyriform fossa may exit laterally through
thyrohyoid membrane, presenting itself as a lateral neck mass. This should
be differentiated from cervical neck node metastasis.

Figure showing routes of spread from pyriform fossa
Thyroid cartilage involvement:
Thyroid cartilage becomes involved by direct invasion. Common areas of thyroid
cartilage involvement are the posterior and superior margins. Studies have shown
that thyroid cartilage invasion was found in nearly 25% of patients with pyriform
fossa malignancy.
Thyroid gland involvement:
Thyroid gland may be involved if the tumor spreads directly through the thyroid
cartilage, or from the tumor exiting the larynx through the thyrocricoid membrane
more posteriorly.

Post cricoid growth:
Anatomy: Post cricoid region includes mucosa and submucosa extending from the
inferior aspect of arytenoids to the bottom of cricoid cartilage.
Post cricoid tumors account for nearly 20% of Hypopharyngeal malignancy. This
area may be commonly involved by tumors spreading from the apex of pyriform
fossa, or it may be a separate lesion on its own. Tumors involving this area may
remain asymptomatic until they become extremely large compromising swallowing.
Tumors of post cricoid area are prone for circumferential growth.
Features of post cricoid growth:
1. Present late
2. Carries poor prognosis as nutritional status of the patient is compromised
3. This area is very rich in lymphatics and vascular network making metastasis
as the order of the day
4. Very common in females (tends to affect them very early in their life)
Etiology:
1. Plummer Vinson syndrome: The syndrome of iron deficiency anaemia /
esophageal web is commonly associated with increased incidence of post
cricoid growth (about 20%).
2. Synergistic effects of tobacco and alcohol has also been documented
Diagnosis:
Indirect laryngoscopy is one way of examining the larynx and its surrounding
structures. It will give a rough idea about the size and extent of the tumor mass.
Endoscopic assessment of Hypopharyngeal tumors:
1. Patient should be adequately anesthetized, relaxed and absolutely still.
2. Using a direct laryngoscope the following folds are carefully examined:
Pharyngoepiglottic folds, aryepiglottic folds and glosso epiglottic folds.
3. Using a pharyngoscope the following areas should be examined: Base of
tongue, pyriform fossa, Post cricoid and posterior pharyngeal wall.
4. The lower limit of the tumor must be assessed using Oesophagoscopy. This is
crucial for surgical planning.

5. Ascertain whether the tumor moves freely on prevertebral fascia. Fixity to
prevertebral fascia is a contraindication for surgery.
6. Using a laryngoscope the Subglottic area and the upper portion of trachea
should be carefully examined.
7. Several biopsies are taken from the margin of the tumor mass
8. A full Bronchoscopy should be performed.
Role of imaging in Hypopharyngeal tumors:
CT scans:
1. CT scans are useful in delineating tumor extent.
2. It also helps in assessing tumor involvement of thyroid cartilage.
3. It helps to evaluate cricoid cartilage invasion.
4. Tongue base involvement.
5. Cervical nodal metastasis can be clearly assessed.
6. Contrast CT help in accurate assessment of nodal metastasis.
CT scan showing pyriform fossa mass

MRI scan:
1. It helps in assessing tongue base extension.
2. It is superior to CT in examining muscular planes.
Histology:
Squamous cell carcinoma is the commonest histological type seen in Hypopharynx.
Other tumor types include: adenocarcinomas, lymphomas, and mucosal melanomas.
Staging of Hypopharyngeal tumors:
Staging of Hypopharyngeal tumors is very vital in deciding the optimal
management modality. It also helps in the assessment of prognosis.
The staging system used is derived from the American Joint Committee on Cancer.
This was updated in 2002.
Primary tumor:
Tx: Primary tumor cannot be assessed
T0: No evidence of primary tumor
Tis: Carcinoma in situ
T1: Tumor limited to one subsite and is less than 2cm in the largest dimension
T2: Tumor limited to more than one subsite of Hypopharynx with the mass
measuring more than 2cm and less than 4 cm in the largest dimension. The larynx
should not be fixed.
T3: Tumor measuring more than 4cm in the greatest dimension / fixity of larynx
T4a: Tumor invades cartilage / bone / thyroid gland / esophagus
T4b: Tumor invades prevertebral fascia / carotid sheath / mediastinal structures
(Subsites include pyriform fossa, postcricoid area, and posterior pharyngeal wall)

Regional Nodes:
Nx: Regional nodes could not be assessed
N0: No cervical nodal metastasis
N1: Metastasis confined to a single ipsilateral node (size less than 3cm in greater
dimension)
N2: Metastasis confined to a single ipsilateral node (size greater than 3cm and less
than 6cm in the greatest dimension)
N2a: Metastasis to a single ipsilateral node (size more than 3 cm and less than 6
cm in the greatest dimension)
N2b: Metastasis to multiple ipsilateral nodes but none of them more than 6cm in
the greatest dimension
N2c: Metastasis to bilateral nodes / contralateral nodes (none of them more than
6 cm in the greatest dimension)
N3: Metastasis to cervical node (size more than 6cm in the greatest dimension)
Distant metastasis:
Mx: Distant metastasis cannot be assessed
M0: No regional metastasis
M1: Distant metastasis
AJCC stage groups:
Stage 0 - Tis, N0, M0
Stage I - T1, N0, M0
Stage II - T2, N0, M0
Stage III
o T3, N0, M0
o T1, N1, M0
o T2, N1, M0
o T3, N1, M0
Stage IVA
o T4a, N0, M0
o T4a, N1, M0
o T1, N2, M0
o T2, N2, M0

o T3, N2, M0
o T4a, N2, M0
Stage IVB
o T4b, any N, M0
o Any T, N3, M0
Stage IVC - Any T, any N, M1
Biopsy from the lesion should be taken at multiple sites along the edge of the mass.
Picture showing biopsy being taken

Treatment:
About a quarter of patients with Hypopharyngeal growth are not treatable
on presentation.
Advancing age and poor nutritional status add to the problem.
Pyriform fossa tumors with extension into the posterior 1/3 of tongue are
virtually inoperable
Post cricoid tumor fixed to the prevertebral fascia is again in operable
Patients who belong to the surgically untreatable group may be considered
for palliative radiotherapy
Chemotherapy has virtually no role as a single treatment modality
Stage
Pyriform fossa
Posterior pharyngeal
wall
Post cricoid
Stage I
Stage II
Stage III
Stage IV
Primary RT / Surgery
Primary RT / Surgery
Surgery and post op
RT
Surgery and post op
RT
Primary RT / Surgery
Primary RT / Surgery
Surgery and post op RT
Surgery and post op RT
Primary RT / Surgery
? Primary RT / Surgery
and post op RT
Surgery and post op RT
Surgery and post op RT

Inclusion criteria for primary radiotherapy:
1. Vertical length of the tumor should not exceed 5 cm
2. Vocal cords should be mobile
3. N0 neck.
If a tumor does not fulfill these criteria, then the patient should be submitted to
surgery if age and general condition are favorable.
It should also be accepted that radiotherapy when used for small volume disease is
an excellent form of radical therapy. It has also the added advantage of avoiding
laryngectomy.
The total prescribed doses used for primary radiotherapy are 70-72 Gy. Prescribed
doses for postoperative regimens are 60-66 Gy, depending on the pathologic margin
status. The dose per fraction in head and neck tumors should be 200 cGy when daily
radiotherapy is used alone. Dose reductions to 180 cGy or less (ie, 120 cGy twice a
day) can be used if the fractionation schedule is altered or radiation is combined
with chemotherapy. When IMRT is used, these doses can be delivered by
sequentially reducing the volume of irradiation, as has been done with traditional
nonconformal techniques. With this serial cone-down technique, more conventional
radiotherapy doses per fraction are used.
Radiotherapy regimens:
Radiation therapy oncology group has approved the following radiotherapy
regimens:
1. Standard fractionation at 2 Gy per fraction per day, 5 days per week to 70
Gy per 35 fractions for 7 weeks
2. Hyperfractionation at 1.2 Gy per fraction, twice daily, 5 days per week to
81.6 Gy per 68 fractions for 7 weeks
3. Accelerated fractionation with a split at 1.6 per fraction, twice daily, 5 days
per week to 67.2 Gy per 42 fractions for 6 weeks, including a 2-week rest
after 38.4 Gy
4. Accelerated fractionation with concomitant boost at 1.8 Gy per fraction per
day, 5 days per week and 1.5 Gy per fraction per day to the boost field as a
second daily treatment for the last 12 treatments
One of the difficulties of irradiation in these patients is the occurrence of ulcers in
post cricoid region which could turn out to be negative in a biopsy. These patients
demonstrate a high rate of recurrence in the post cricoid region at a later date.
Hence the presence of ulcer in the postcricoid region in an irradiated patient should
be assumed to represent a recurrent disease.

Surgery:
In most patients it is possible to resect the involved part of pharynx together with
larynx. Enough pharyngeal mucosa can be preserved to facilitate primary closure.
In irradiated patients there may not be enough pharyngeal mucosa to facilitate
primary repair. In these patients flaps may be used to repair the lesion.
Partial Laryngopharyngectomy:
Tumors that arise from the medial wall of pyriform fossa with limited extension to
the aryepiglottic folds can be managed by this procedure. Invasion of thyroid
cartilage is a contraindication for this surgical procedure.
Procedure:
1. Performed under general anesthesia.
2. Skin flaps are elevated in the subplatysmal plane.
3. The larynx and pharynx are mobilized by dissecting medial to the
sternomastoid muscles.
4. A tracheostomy is performed
5. Pharynx is entered through the valleculae on the side opposite to that of the
tumor
6. Entry into the preepiglottic space must be avoided at all costs
7. Pharyngeal mucosa is divided from side to side immediately above the hyoid
bone
8. A cricopharyngeal myotomy should be performed before closure

Figure showing the line of resection in partial Laryngopharyngectomy
Total pharyngolaryngectomy:
This surgery is indicated in patients with extensive carcinoma of pyriform fossa,
where primary pharyngeal repair is impossible.
Procedure:
1. The larynx and pharynx are mobilized by dissection medial to the carotid
sheath on each side
2. The superior thyroid pedicle are identified and divided on both sides.
3. Inferior thyroid artery on the side of the tumor is also divided.
4. In case of post cricoid tumors both lobes of thyroid gland should be excised
in continuity with the primary mass
5. Trachea is divided at the level of 4th
tracheal ring and a permanent
tracheostome is fashioned.
6. Upper end of oesophagus is palpated to identify the lower end of the tumor.
7. Three cm below the palpated point vicryl stay sutures are placed through
esophageal muscular wall and the esophagus is divided immediately below it.
8. Pharynx is divided at its upper end.
9. Wound is washed, and hemostasis is obtained.
10. Pharyngeal repair may be completed by using a free jejunal transfer
In post cricoid tumors a Total laryngo pharyngo oesophagectomy can be performed
using gastric pull up to repair the resected pharynx.
Block neck dissection can be resorted to for clearing involved neck nodes.
Tumors of posterior pharyngeal wall:
Because of its size and frequent association with enlarged nodes, tumors of posterior
pharyngeal wall do not do well with radiotherapy.
Lateral pharyngotomy can be resorted to in tumors of posterior pharyngeal wall.

Resection line of lateral pharyngotomy
Procedure:
1. Access to larynx and pharynx is achieved by retracting sternomastoid muscle
laterally and dissecting medial to the carotid sheath.
2. Using diathermy, the suprahyoid muscles are divided.
3. Mucosa is divided with scissors and the pharynx is entered through
valleculae
4. A retractor is inserted through the incision into the pharynx and the
epiglottis is retracted anteriorly
5. Tumor in the posterior wall of pharynx becomes visible and can be examined
and resected in toto.
6. Forearm flaps can be used to perform pharyngeal repair.

Prognostic factors:
1. Age: The survival rate usually declines as the age increases. However, 50%
or more of the patients who present when younger than 40 years (1-3%) have
stage IV disease.
2. Sex: Women usually present with earlier-stage disease and have a higher
survival rate after therapy.
3. Karnofsky performance score: Patients with a poor Karnofsky performance
score (KPS) usually have poorer outcome due to weight loss, cachexia,
malnutrition, and anemia.
4. Tumor-related factors that influence prognosis include the following:
Stage: Increasing T and N stages indicate poor prognosis.
Histology: Pathologic factors such as positive surgical margins or
tumor persistence in a radiation field after definitive treatment
adversely affect survival.
Location: Aryepiglottic fold and pyriform fossa tumors on the medial
wall are usually smaller and more localized and have higher cure
rates.
Cross-sectional tumor volume: Several studies have demonstrated an
inverse relationship between the primary tumor volume, as assessed
with cross-sectional imaging (e.g., CT scanning), and local control
rates. In several independent studies, this has been more consistently
reported in patients treated with radiotherapy but has also been
reported in patients who underwent surgery at the primary site.