Embed Size (px)
Citation preview

RRP =Recurrent Rectal Prolapse
Colo‐rectal unit
Surgery department
“Soroka” Medical center
Dr. Ruthie Gold‐Deutch
Dr. Ilia Pinsk

First Admission‐ 9/2010First Admission 9/2010
ld f l30 years old female
Lives in Psychiatric institution‐ “Rotem house”
Epilepsy s/p Head trauma in childhoodEpilepsy s/p Head trauma in childhood
Schizo‐affective disorder
Personality disorder –Cluster B – Borderline Histrionic‐Regular medication
Obsessive recurrent coughs for years
Rectal prolapse –Rectal bleeding‐Anemia
N iNo pregnancies
Altemeier Operation ‐ Perineal rectosigmoidectomy – First operation ‐9/10
Uneventful postoperative courseUneventful postoperative course
9/12/2010Second admission 9/12/2010Second admission ‐
l lRecurrent rectal prolapse
Rectal bleeding and pain
Difficulty emptyingDifficulty emptying
Abdominal pain
Physical examination‐ Full rectal prolapse –reducible , rectal bleeding
Altemeier Operation –Perineal rectosigmoidectomy‐ Second operation –
16/12/201016/12/2010
Anterior and posterior Puborectalis muscle plication
Uneventful postoperative courseUneventful postoperative course

Third admission 2/4/2011Third admission ‐2/4/2011
l lRecurrent rectal prolapse
Fecal incontinence
Rectal bleedingRectal bleeding
Physical examination‐ Full rectal prolapse –reducible , rectal bleeding
Patulus anus
Anal sphincter –no tonus
??
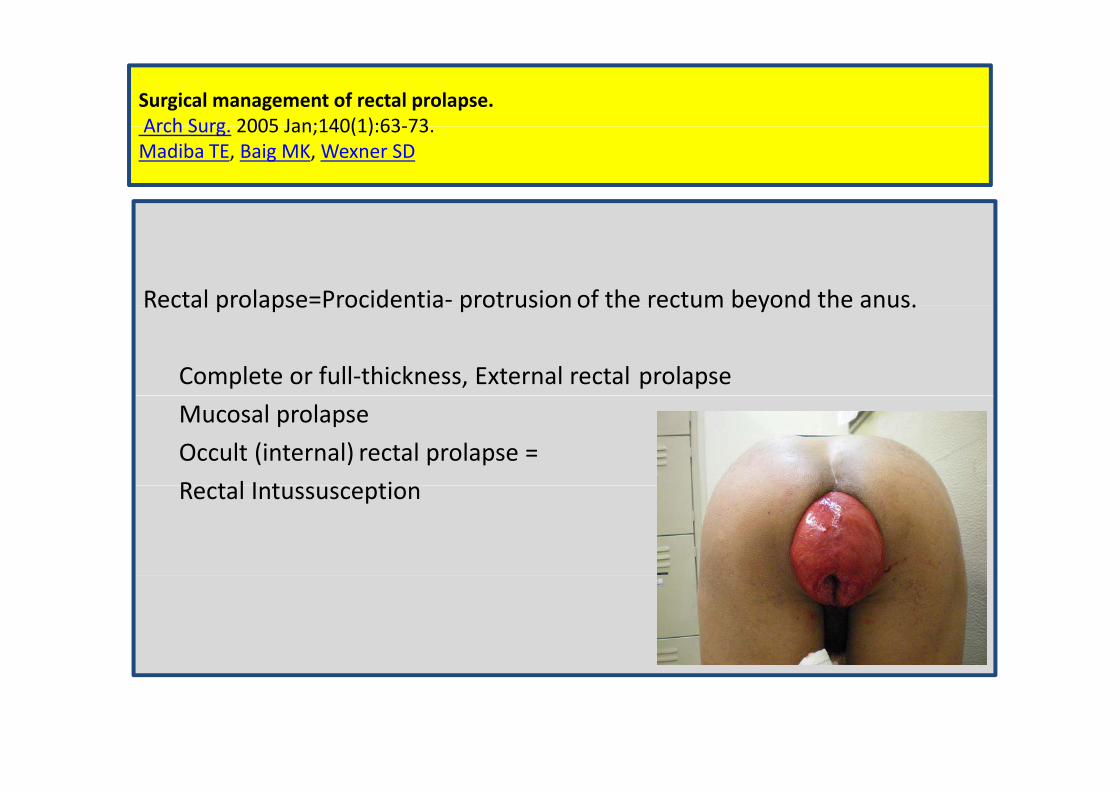
Surgical management of rectal prolapse.7363):1(140Jan;2005Arch Surg . 73‐63):1(140Jan;2005 Arch Surg.
SDWexner, MKBaig, TEMadiba
Rectal prolapse=Procidentia‐ protrusion of the rectum beyond the anus.Rectal prolapse Procidentia protrusion of the rectum beyond the anus.
Complete or full‐thickness, External rectal prolapse
Mucosal prolapse
Occult (internal) rectal prolapse =
R t l I t tiRectal Intussusception
Pelvic Organ ProlapseI. Kuncharapu, B.A. Majeroni , D. W. Johnson.Am Fam Physician. 2010 May 1;81(9):1111‐1117.
Ri k F t f t l P lRisk Factors for rectal ProlapseGeneral factors Advancing ageI i b d i dIncreasing body mass indexMenopauseLow socioeconomic statusI d i t bd i lIncreased intra‐abdominal pressure
Chronic cough caused by smoking, chronic lung diseasestraining with chronic constipation or repeated heavy liftingObstetricCurrent pregnancy, previous prolonged labor, instrumental delivery, episiotomyincreasing parity, weight of babiesPrevious surgeryHysterectomy, previous prolapse surgery(Cesarean delivery may not prevent prolapse)

Habit Cough, Tic Cough, and Psychogenic Cough in Adult and Pediatric Populations ACCP Evidence‐Based Clinical Practice GuidelinesR. S. Irwin, W.B. Glomb, A.B. Chang. Chest, January 2006 vol. 129 no. 1 suppl 174S‐179S
Diagnoses of habit cough or psychogenic cough can be made only after an
extensive evaluation is performed that includes ruling out tic disorders andextensive evaluation is performed that includes ruling out tic disorders and
uncommon causes of chronic cough, and when cough improves with
behavior modification or psychiatric therapy.

Surgical management of rectal prolapse.SDWexner, MKBaig, TEMadiba
. 73‐63):1(140Jan;2005 Arch Surg.
Aims of surgicalmanagement –
• Restoring physiology by correcting the prolapseRestoring physiology by correcting the prolapse
• Improving continence and/or constipation
• With acceptablemorbidity/mortality and recurrence rates.
Treatment of RP
to narrow to encircle??to suspend to plicate
to wrap to resect
to fix

Surgical management of RP
Perineal approachesAbdominal approaches open/laparoscopy
Suture RectopexyDelorme procedure perineal rectosigmoidectomy
Prosthetic or Mesh Posterior RectopexyRipstein Procedure (Anterior
(Altemeier operation)+/‐LevatorplastyThiersch procedure‐ anal encirclement Ripstein Procedure (Anterior
Sling Rectopexy)encirclement
Resection Rectopexy‐Frykman‐Goldberg procedure
Laparoscopic Rectopexy
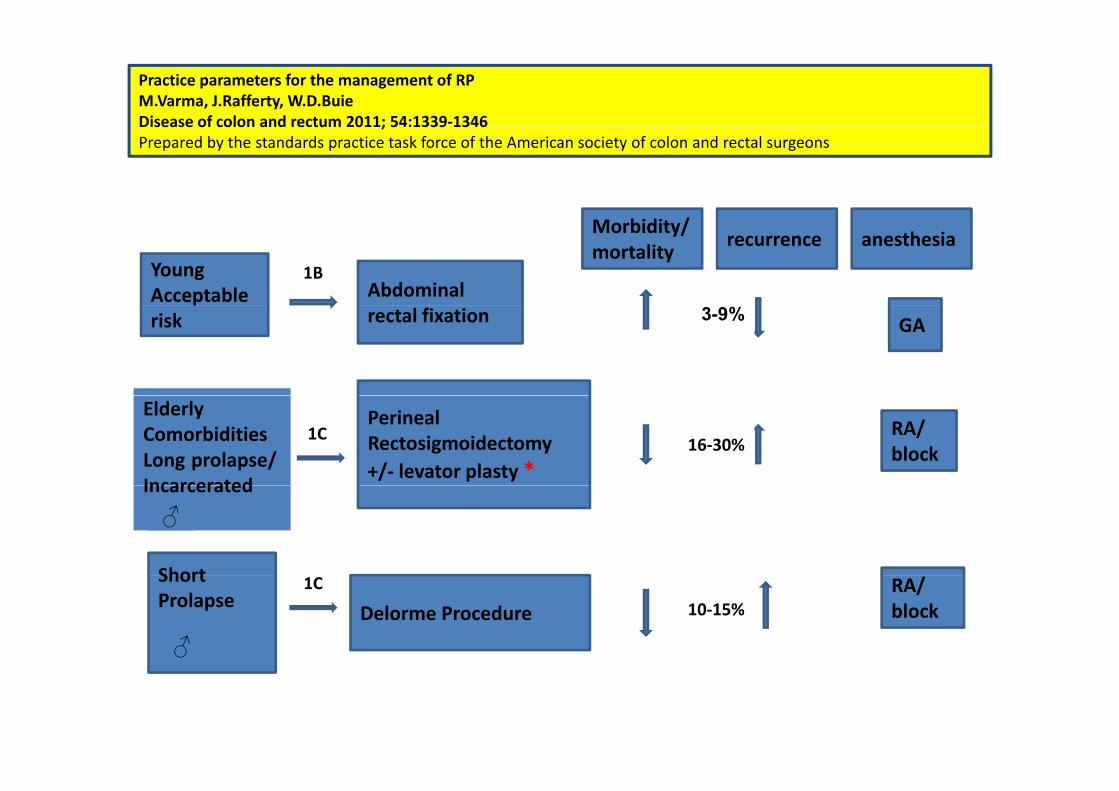
Practice parameters for the management of RPM.Varma, J.Rafferty, W.D.BuieDisease of colon and rectum 2011; 54:1339‐1346Disease of colon and rectum 2011; 54:1339 1346Prepared by the standards practice task force of the American society of colon and rectal surgeons
YoungAcceptable Abdominal
recurrenceMorbidity/ mortality
anesthesia
1B
risk rectal fixation GA3-9%
PerinealRectosigmoidectomy+/‐ levator plasty *
ElderlyComorbidities
prolapse/ LongIncarcerated
RA/block16‐30%
1C
Short
Incarcerated
♂
ShortProlapse Delorme Procedure
RA/block
1C10‐15%
♂
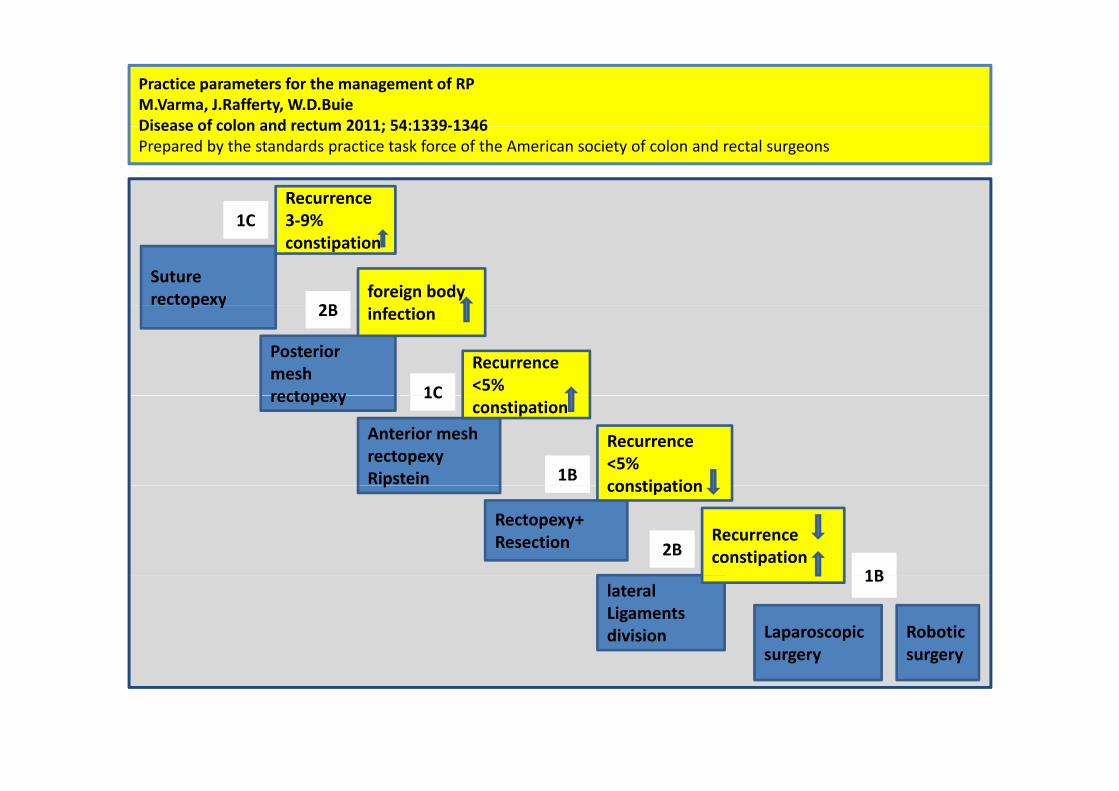
Practice parameters for the management of RPM.Varma, J.Rafferty, W.D.BuieDisease of colon and rectum 2011; 54:1339‐1346Disease of colon and rectum 2011; 54:1339‐1346Prepared by the standards practice task force of the American society of colon and rectal surgeons
Recurrence3 9%1C
Suture rectopexy foreign body
3‐9%constipation
1C
2Bp y
Posterior mesh rectopexy
infection
Recurrence <5% 1C
2B
rectopexy
Anterior mesh rectopexyRipstein
Recurrence <5% constipation
constipation
1B
1C
Rectopexy+Resection
p
Recurrence constipation
constipation
2B1B
lateral Ligamentsdivision Laparoscopic
surgery
1B
Robotic surgery
Treatment for RRP‐?What Is the Next Good Option?
? !Perineal approach Abdominal approach
? !Perineal approach Abdominal approach
? !? !

Recurrent Rectal Prolapse‐What Is the Next Good Option?A J Pikarsky J S Joo S D Wexner E G Weiss J J Nogueras F Agachan A IroatulamA.J. Pikarsky, J.S. Joo, S.D. Wexner, E.G. Weiss, J.J. Nogueras, F. Agachan, A. Iroatulam. Dis Colon Rectum, 2000 ;43: 1273‐6
Aim –To assess the clinical and functional outcome of surgery for RRP and
compare it to patients who underwent an initial operation for rectal p p p
prolapse.

Recurrent Rectal Prolapse‐What Is the Next Good Option?A.J. Pikarsky, J.S. Joo, S.D. Wexner, E.G. Weiss, J.J. Nogueras, F. Agachan, A. Iroatulam. y, , , , g , g ,Dis Colon Rectum, 2000 ;43: 1273‐6
115
27 27

Recurrent Rectal Prolapse‐What Is the Next Good Option?A.J. Pikarsky, J.S. Joo, S.D. Wexner, E.G. Weiss, J.J. Nogueras, F. Agachan, A. Iroatulam. Dis Colon Rectum 2000 ;43: 1273 6Dis Colon Rectum, 2000 ;43: 1273‐6

Recurrent Rectal Prolapse‐What Is the Next Good Option?A.J. Pikarsky, J.S. Joo, S.D. Wexner, E.G. Weiss, J.J. Nogueras, F. Agachan, A. Iroatulam. Dis Colon Rectum, 2000 ;43: 1273‐6

Recurrent Rectal Prolapse‐What Is the Next Good Option?A J Pikarsky J S Joo S D Wexner E G Weiss J J Nogueras F Agachan A IroatulamA.J. Pikarsky, J.S. Joo, S.D. Wexner, E.G. Weiss, J.J. Nogueras, F. Agachan, A. Iroatulam. Dis Colon Rectum, 2000 ;43: 1273‐6
ll fOverall success rate for RRP ‐ 85.2 %
Conclusions‐
• The outcome of surgery for rectal prolapse is similar in cases ofThe outcome of surgery for rectal prolapse is similar in cases of
primary or recurrent prolapse.
• The same surgical options are valid in both scenarios
• Perineal procedures for RRP had as good a success rate as was found after
primary prolapse repair
R l b d b i d bili i d• Recurrent prolapse may be caused by inadequate mobilization and
resection of the redundant rectum and sigmoid in perineal
proctosigmoidectomy or incomplete mucosectomy in Delorme'sproctosigmoidectomy or incomplete mucosectomy in Delorme s
procedure.

Surgical Treatment of RRPA Thirty‐Year Experience G .R. Hoot , T. L. Hull, V. W. Fazio. Dis Colon Rectum, March 1997; Vol. 40(3):270‐2
Perineal Approach9 pt’s
Abdominal approach15 pt’s
RRP 24 pt’s24 pt s
4 Perineal Approach 25 Abdominal approach
1963‐1993Median age was 56 (range, 18‐88) y Median follow‐up 6.75 (range, 0.08‐ 17) yMedian duration to recurrence 2 yy10 recurrence (34 %) within 7 months
Surgical Treatment of RRPA Thirty‐Year Experience G .R. Hoot , T. L. Hull, V. W. Fazio. Dis Colon Rectum, March 1997; Vol. 40(3):270‐2
Aims‐
1) To examine the possible causal factors for recurrence including possible1) To examine the possible causal factors for recurrence, including possible
technical factors
2) To examine the treatment options available and how they are affected by
initial prolapse surgery
3) To examine the outcome after surgery for RRP
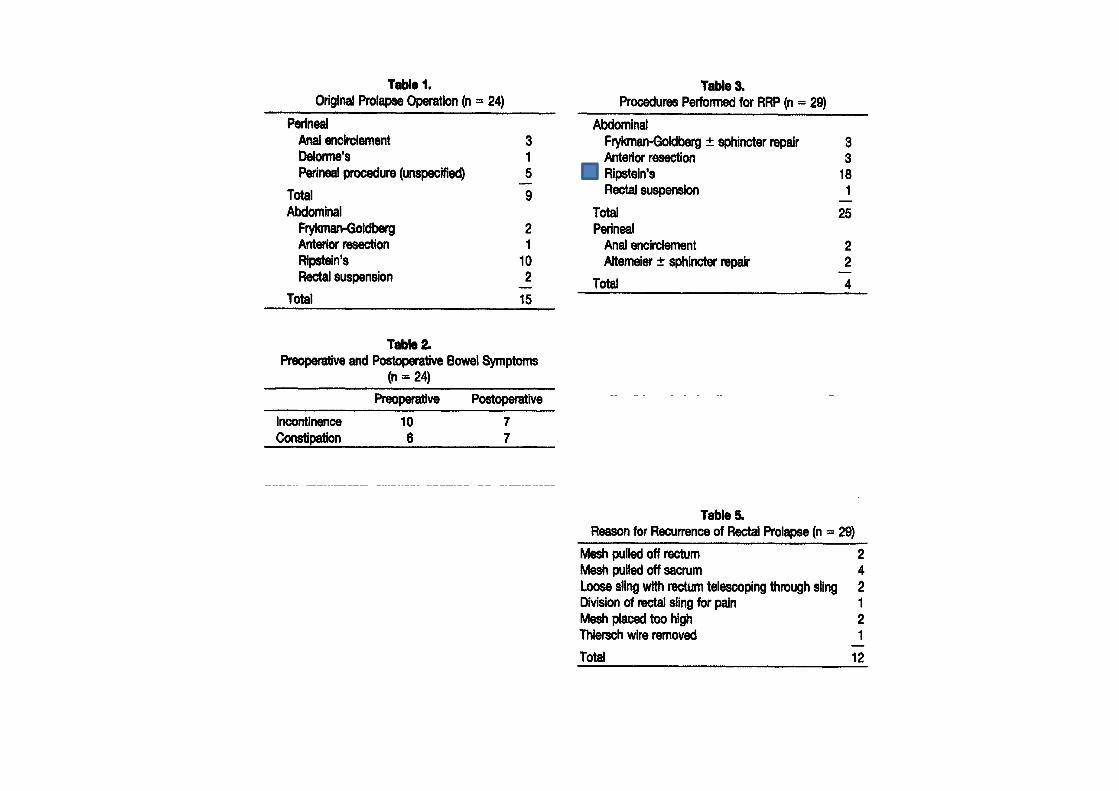

Surgical Treatment of Recurrent Complete Rectal ProlapseA Thirty‐Year Experience G .R. Hoot, T. L. Hull, V. W. Fazio. Dis Colon Rectum, March 1997; Vol. 40(3):270‐2
Conclusions‐
• It is assumed that the similar pathophysiology is occurring with RRP asIt is assumed that the similar pathophysiology is occurring with RRP as with the first occurrence
• Abdominal approach has a lesser recurrence rate than the perinealh fapproach for RRP
• Failure of the mesh was the most common identifiable reason for failure
• Preoperative incontinence and constipation were largely unchanged byPreoperative incontinence and constipation were largely unchanged by
RRP operation (60%)
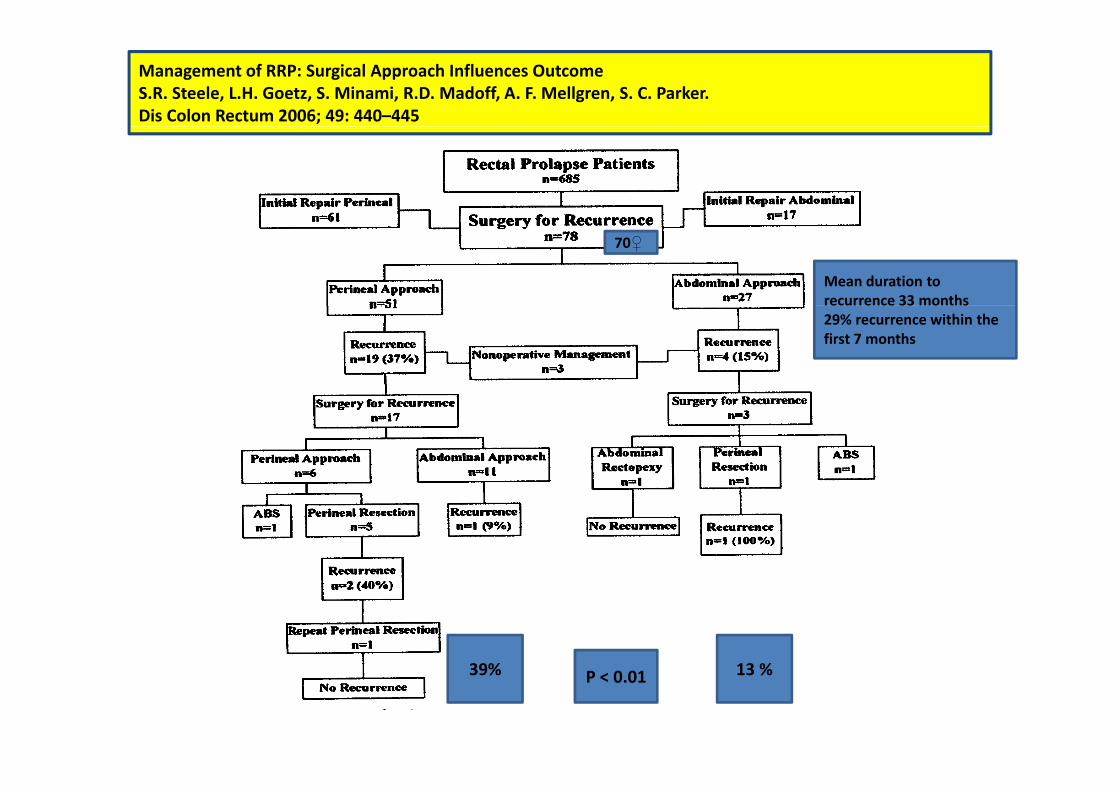
Management of RRP: Surgical Approach Influences OutcomeS.R. Steele, L.H. Goetz, S. Minami, R.D. Madoff, A. F. Mellgren, S. C. Parker.Dis Colon Rectum 2006; 49: 440–445
70♀
Mean duration to recurrence 33 months29% recurrence within the first 7 months
13 %39% 13 %39% P < 0.01
Management of RRP: Surgical Approach Influences OutcomeS R Steele L H Goetz S Minami R D Madoff A F Mellgren S C ParkerS.R. Steele, L.H. Goetz, S. Minami, R.D. Madoff, A. F. Mellgren, S. C. Parker.Dis Colon Rectum 2006; 49: 440–445
Conclusions‐
Recurrence rates are lower after an abdominal vs perineal repairRecurrence rates are lower after an abdominal vs. perineal repair
• More accurate determination of whether to resect or pull up and fixate
additional redundant bowel that may otherwise prolapse
Same benefits persist in recurrent prolapse surgery
E h i i h RRP h ld b i di id ll d d bd i lEach patient with RRP should be individually assessed, and suggest abdominal
repair if the his risk profile permits it.

Management of RRP: Surgical Approach Influences OutcomeS R Steele L H Goetz S Minami R D Madoff A F Mellgren S C ParkerS.R. Steele, L.H. Goetz, S. Minami, R.D. Madoff, A. F. Mellgren, S. C. Parker.Dis Colon Rectum 2006; 49: 440–445
Abdominalapproach
Perinealapproach
45N f li ti 45No. of complications
20Anastomotic stricture
13Anastomotic leak/abscess
11Severe constipation 11Severe constipation
01Intractable diarrhea
1510Overall complication %
Management of RRP: Surgical Approach Influences OutcomeS R Steele L H Goetz S Minami R D Madoff A F Mellgren S C ParkerS.R. Steele, L.H. Goetz, S. Minami, R.D. Madoff, A. F. Mellgren, S. C. Parker.Dis Colon Rectum 2006; 49: 440–445
6 pt’s developed anastomotic complications → stricture, leak
h ld b f l f• Surgeon should be wary to perform an Altemeier operation after a
rectosigmoid resection has been performed (or Vice versa).
This could leave a devascularized segment of rectumThis could leave a devascularized segment of rectum
• Recommend to preserve the Superior Hemorrhoidal artery in cases of
resection/rectopexy.

Management of RRPS A Fengler R K Pearl M L Prasad C P Orsay J R Cintron E Hambrick H AbcarianS. A. Fengler, R. K. Pearl, M. L. Prasad, C.P. Orsay, J. R. Cintron, E. Hambrick, H. AbcarianDis Colon Rectum, July 1997; Vol.40 (7): 832‐4
14 pt’s (11♀) Age from 22 ‐ 92 years (mean‐ 68y)Age from 22 92 years (mean 68y)
Underwent operative correction of RRP (1984 ‐1993)Average time to recurrence was 14 months (range‐ 6‐60m)
Average length of follow‐up ‐50 months (range, 9‐115m)
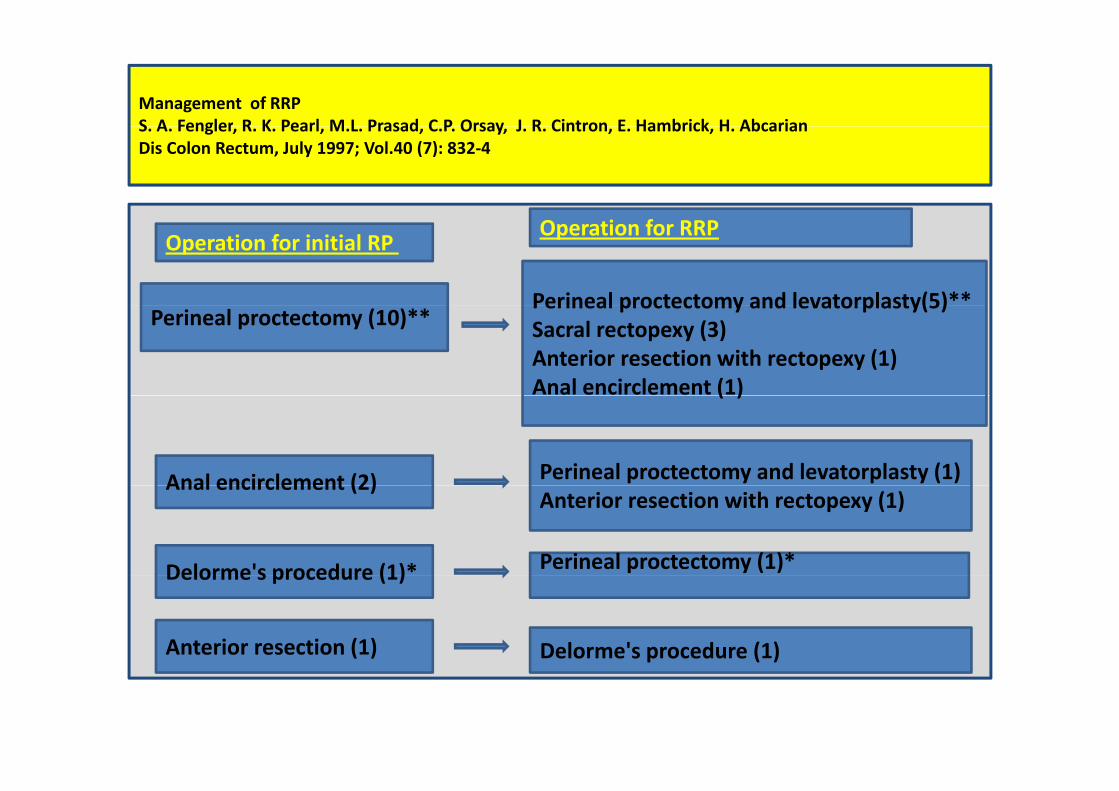
Management of RRPS A Fengler R K Pearl M L Prasad C P Orsay J R Cintron E Hambrick H AbcarianS. A. Fengler, R. K. Pearl, M.L. Prasad, C.P. Orsay, J. R. Cintron, E. Hambrick, H. AbcarianDis Colon Rectum, July 1997; Vol.40 (7): 832‐4
Perineal proctectomy and levatorplasty(5)**
Operation for initial RP Operation for RRP
Perineal proctectomy (10)**Perineal proctectomy and levatorplasty(5)Sacral rectopexy (3) Anterior resection with rectopexy (1)Anal encirclement (1)( )
Anal encirclement (2) Perineal proctectomy and levatorplasty (1)Anal encirclement (2)Anterior resection with rectopexy (1)
Delorme's procedure (1)* Perineal proctectomy (1)*Delorme s procedure (1)
Anterior resection (1) Delorme's procedure (1)

Management of Recurrent Rectal ProlapseS A Fengler R K Pearl M L Prasad C P Orsay J R Cintron E Hambrick H AbcarianS. A. Fengler, R. K. Pearl, M. L. Prasad, C. P. Orsay, J. R. Cintron, E. Hambrick, H. AbcarianDis Colon Rectum, July 1997; Vol.40 (7): 832‐4
l h f l ’Slough of rectal mucosa ‐1 pt’
Underwent AR with rectopexy for RRP after perineal proctectomy with
levatorplastylevatorplasty
Ischemia of the rectal segment between the two anastomoses.
Unless the previous anastomosis is resected in a procedure for RRP,
resectional procedures should be avoided.
No ischemic segment will be present if another perineal proctectomy is
f dperformed
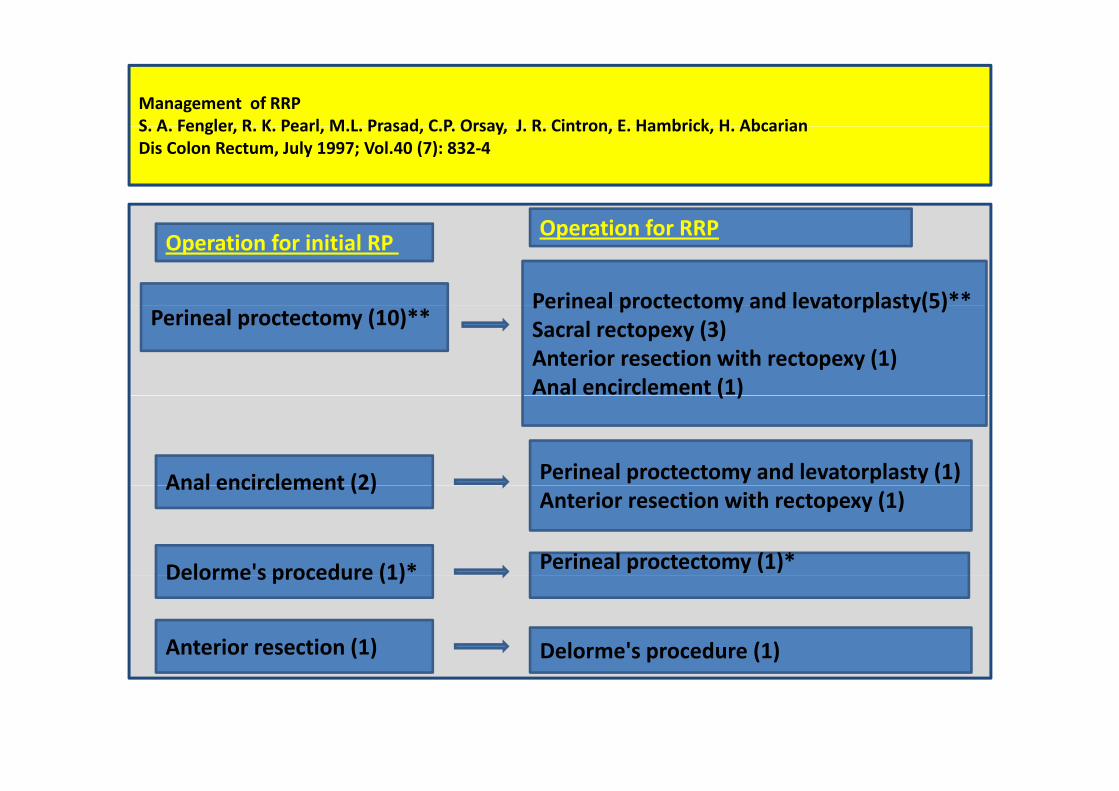
Management of RRPS A Fengler R K Pearl M L Prasad C P Orsay J R Cintron E Hambrick H AbcarianS. A. Fengler, R. K. Pearl, M.L. Prasad, C.P. Orsay, J. R. Cintron, E. Hambrick, H. AbcarianDis Colon Rectum, July 1997; Vol.40 (7): 832‐4
Perineal proctectomy and levatorplasty(5)**
Operation for initial RP Operation for RRP
Perineal proctectomy (10)**Perineal proctectomy and levatorplasty(5)Sacral rectopexy (3) Anterior resection with rectopexy (1)Anal encirclement (1)( )
Anal encirclement (2) Perineal proctectomy and levatorplasty (1)Anal encirclement (2)Anterior resection with rectopexy (1)
Delorme's procedure (1)* Perineal proctectomy (1)*Delorme s procedure (1)
Anterior resection (1) Delorme's procedure (1)

Management of Recurrent Rectal ProlapseS A Fengler R K Pearl M L Prasad C P Orsay J R Cintron E Hambrick H AbcarianS. A. Fengler, R. K. Pearl, M. L. Prasad, C. P. Orsay, J. R. Cintron, E. Hambrick, H. AbcarianDis Colon Rectum, July 1997; Vol.40 (7): 832‐4
Conclusions‐
• Surgical management of RRP can be expected to alleviate the prolapseSurgical management of RRP can be expected to alleviate the prolapse,
but not necessarily fecal incontinence.
• Perineal proctectomies can be safely repeated.
• Despite the familiarity and high success rate of abdominal approaches in
the repair of rectal prolapse, it is advisable to opt for a perineal approach
i hi h i k iin high‐risk patients.
• Advised that surgeons choose the procedure with which they are most
familiarfamiliar.

Practice parameters for the management of rectal prolapseM.Varma, J.Rafferty, W.D.BuieDisease of colon and rectum 2011;54:1339‐1346Prepared by the standards practice task force of the American society of colon and rectal surgeons
TRUS – sphincters defect
Anal manometryAnal manometry
PNTML
Defecography
Colonoscopy
CTT
(b i )(barium enema)
Urodynamics
Practice parameters for the management of rectal prolapseM.Varma, J.Rafferty, W.D.BuieDisease of colon and rectum 2011;54:1339‐1346Prepared by the standards practice task force of the American society of colon and rectal surgeons
Physiologic testing ‐
• To identify other important pelvic floor pathologyTo identify other important pelvic floor pathology.
• To assess functional disorders – Incontinence (60%)
Constipation (15% ‐ 65%)
• Preoperative manometric /EMG findings serves as reliable predictors of
i f i i dipostoperative function in some studies
• Anorectal physiology studied rarely change the operative strategyAnorectal physiology studied rarely change the operative strategy
but they can guide treatment for associated functional abnormalities
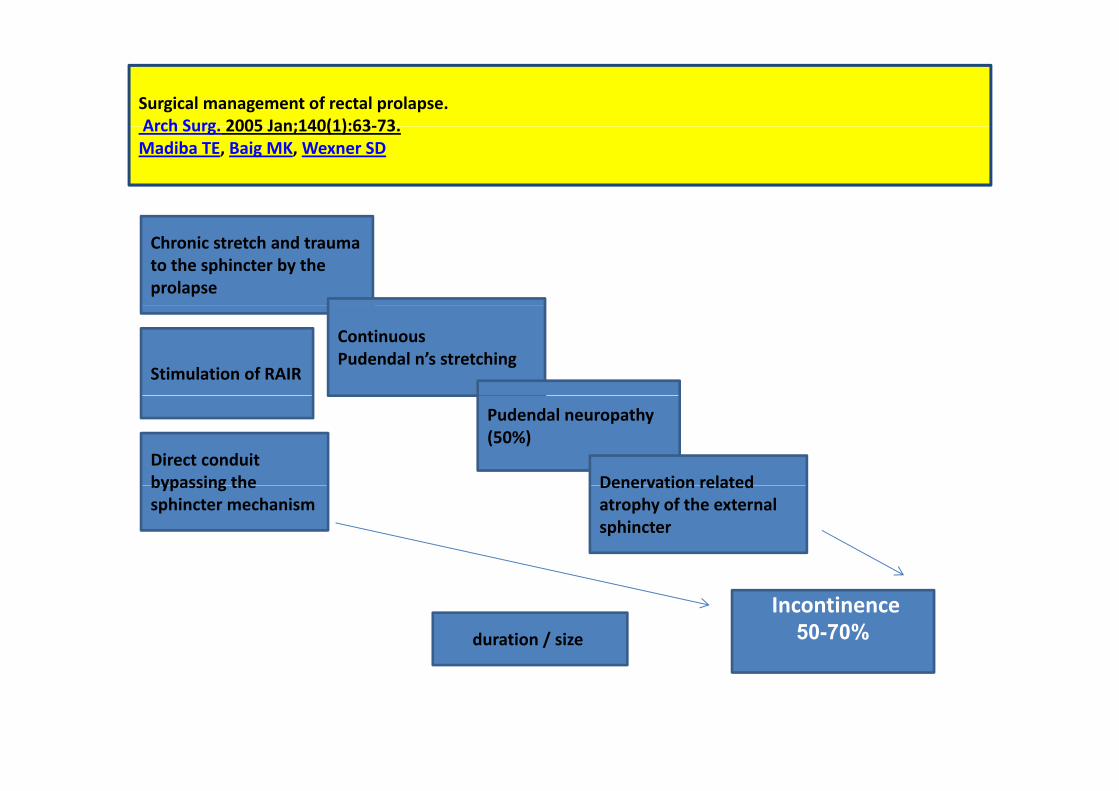
Surgical management of rectal prolapse.Arch Surg 2005 Jan;140(1):63‐73Arch Surg. 2005 Jan;140(1):63‐73. Madiba TE, Baig MK, Wexner SD
Chronic stretch and trauma to the sphincter by the prolapse
Continuous Pudendal n’s stretching
Stimulation of RAIR
Pudendal neuropathy (50%)
Denervation relatedDirect conduit bypassing the Denervation related
atrophy of the external sphincter
bypassing the sphincter mechanism
Incontinence50-70%duration / size

Surgical management of rectal prolapse.Madiba TE, Baig MK, Wexner SDArch Surg. 2005 Jan;140(1):63‐73.
In general patients with incontinence secondary to rectal prolapse will g p y p p
have improvement 2‐3 months after operation
P ti A l M t P di t C ti Aft P i l P t t f R t l P lPreoperative Anal Manometry Predicts Continence After Perineal Proctectomy for Rectal ProlapseS. C. Glasgow, E. H. Birnbaum, I J. Kodner, J. W. Fleshman, D. W. Dietz.Dis Colon Rectum 2006; 49: 1052–1058
Despite recovery of anal sphincteric tone in many patients after repair of the
prolapse, fecal Incontinence persists in at least one‐third of patients in most
large series independent of surgical approach.
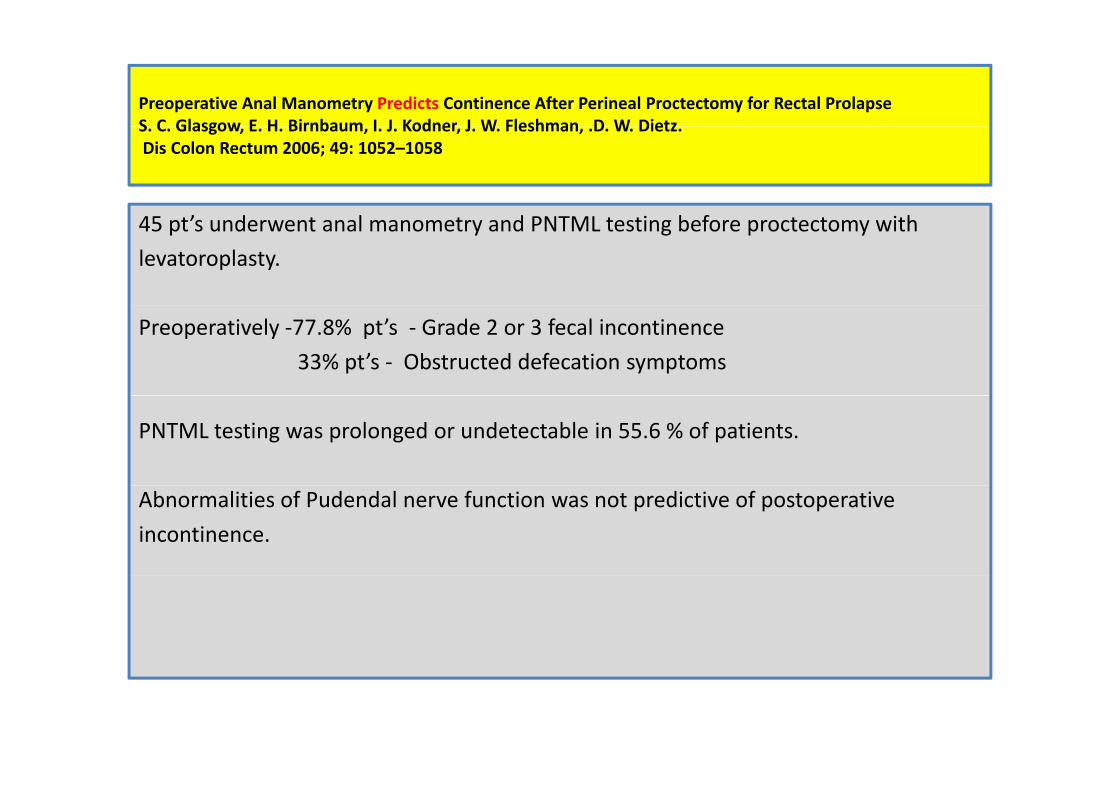
Preoperative Anal Manometry Predicts Continence After Perineal Proctectomy for Rectal ProlapseS C Glasgow E H Birnbaum I J Kodner J W Fleshman D W DietzS. C. Glasgow, E. H. Birnbaum, I. J. Kodner, J. W. Fleshman, .D. W. Dietz.Dis Colon Rectum 2006; 49: 1052–1058
’ d l d i b f i h45 pt’s underwent anal manometry and PNTML testing before proctectomy with
levatoroplasty.
Preoperatively ‐77.8% pt’s ‐ Grade 2 or 3 fecal incontinence
33% pt’s ‐ Obstructed defecation symptoms
PNTML testing was prolonged or undetectable in 55.6 % of patients.
Abnormalities of Pudendal nerve function was not predictive of postoperative
incontinence.

Preoperative Anal Manometry Predicts Continence After Perineal Proctectomy for Rectal ProlapseS C Glasgow E H Birnbaum I J Kodner J W Fleshman D W DietzS. C. Glasgow, .E. H. Birnbaum, I. J. Kodner, J. W. Fleshman, D. W. Dietz.Dis Colon Rectum 2006; 49: 1052–1058
Incontinence rate, 10 vs. 54 %; P = 0.004
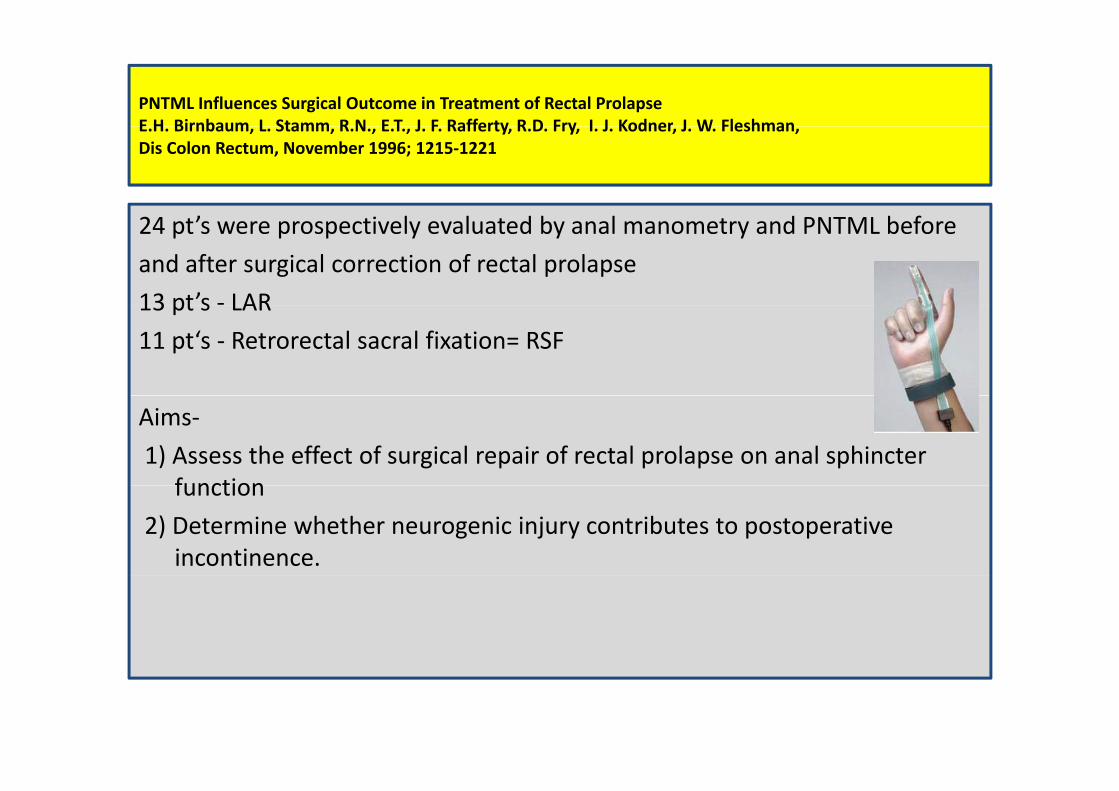
PNTML Influences Surgical Outcome in Treatment of Rectal ProlapseE H Birnbaum L Stamm R N E T J F Rafferty R D Fry I J Kodner J W FleshmanE.H. Birnbaum, L. Stamm, R.N., E.T., J. F. Rafferty, R.D. Fry, I. J. Kodner, J. W. Fleshman, Dis Colon Rectum, November 1996; 1215‐1221
’ l l d b l d b f24 pt’s were prospectively evaluated by anal manometry and PNTML before
and after surgical correction of rectal prolapse
13 pt’s ‐ LAR13 pt s LAR
11 pt‘s ‐ Retrorectal sacral fixation= RSF
Aims‐
1) Assess the effect of surgical repair of rectal prolapse on anal sphincter functionfunction
2) Determine whether neurogenic injury contributes to postoperative incontinence.
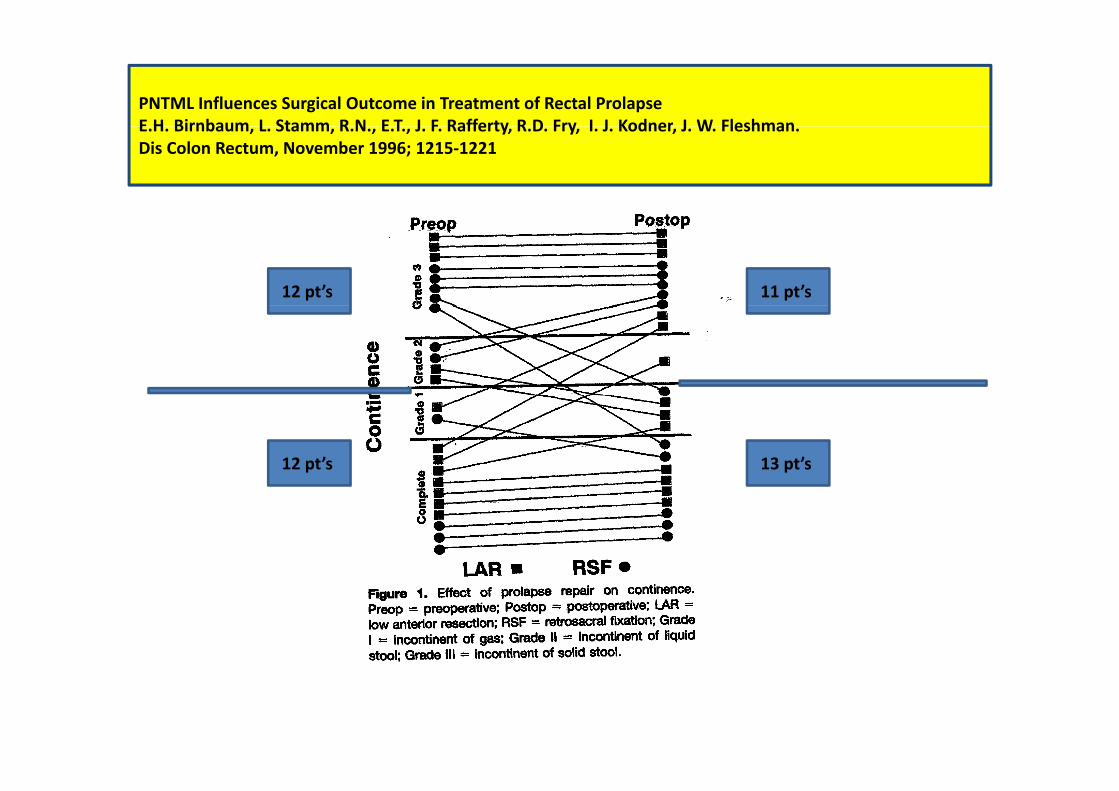
PNTML Influences Surgical Outcome in Treatment of Rectal ProlapseE H Birnbaum L Stamm R N E T J F Rafferty R D Fry I J Kodner J W FleshmanE.H. Birnbaum, L. Stamm, R.N., E.T., J. F. Rafferty, R.D. Fry, I. J. Kodner, J. W. Fleshman.Dis Colon Rectum, November 1996; 1215‐1221
12 pt’s 11 pt’s
12 pt’s 13 pt’s

PNTML Influences Surgical Outcome in Treatment of Rectal ProlapseE.H. Birnbaum, L. Stamm, R.N., E.T., J. F. Rafferty, R.D. Fry, I. J. Kodner, J. W. Fleshman., , , , y, y, ,Dis Colon Rectum, November 1996; 1215‐1221
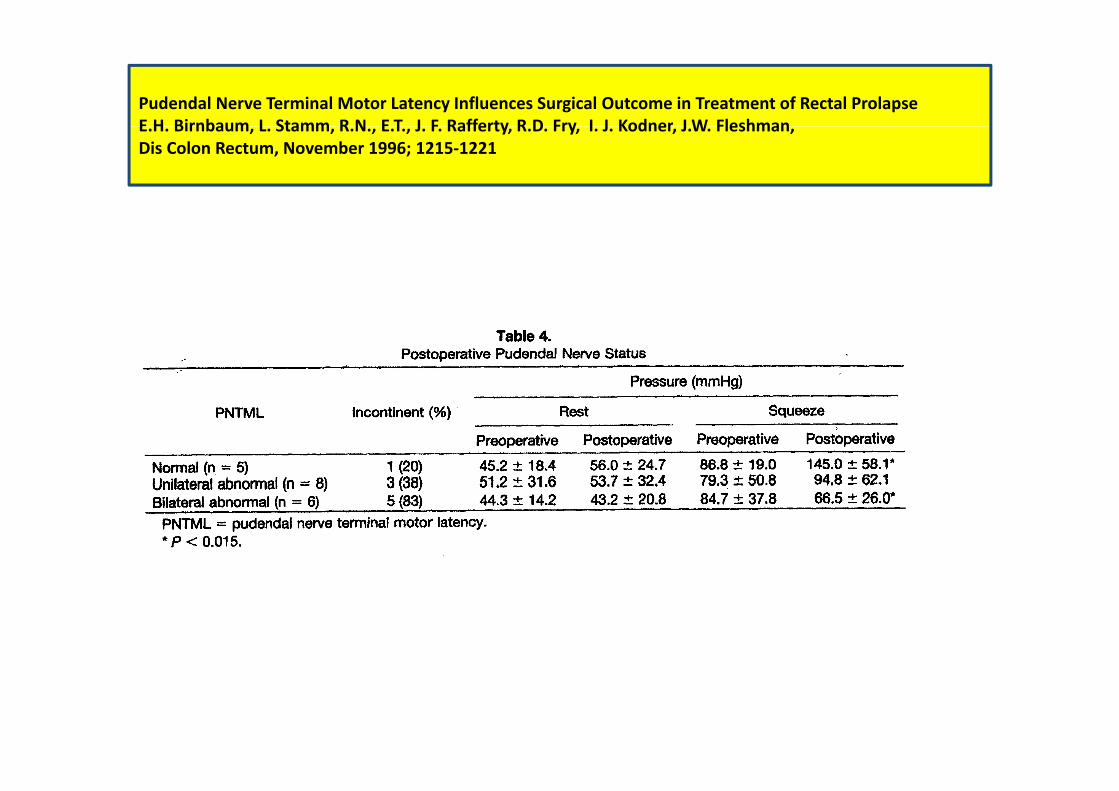
Pudendal Nerve Terminal Motor Latency Influences Surgical Outcome in Treatment of Rectal ProlapseE H Birnbaum L Stamm R N E T J F Rafferty R D Fry I J Kodner J W FleshmanE.H. Birnbaum, L. Stamm, R.N., E.T., J. F. Rafferty, R.D. Fry, I. J. Kodner, J.W. Fleshman, Dis Colon Rectum, November 1996; 1215‐1221

Third admission 2/4/2011Third admission ‐2/4/2011
Inter‐Sphincteric Proctectomy + end colostomy – Third operation – 3/4/2011
Uneventful postoperative course

Inter sphincteric proctectomyInter‐sphincteric proctectomy