-
8/4/2019 Lymph Nodes in Oral Cancer
1/11
Lymph Node Density Is a Significant
Predictor of Outcome in PatientsWith Oral CancerZiv Gil, MD,
PhD1; Diane L. Carlson, MD2; Jay O. Boyle, MD1; Dennis H. Kraus,
MD1; Jatin P. Shah, MD1;
Ashok R. Shaha, MD1; Bhuvanesh Singh, MD1; Richard J. Wong, MD1;
and Snehal G. Patel, MD1
BACKGROUND: The impact of lymph node metastases on prognosis in
patients with oral cavity squamous
cell carcinoma (OSCC) has been well recognized. However,
accurate stratification of risk for recurrence
among patients with lymph node metastases is difficult based on
the existing staging systems. In the cur-
rent study, the utility of lymph node density (LND) was
evaluated as an alternative method for predictingsurvival. METHODS:
Three hundred eighty-six patients who underwent neck dissection
were included. The
median follow-up was 67 months. Five-year overall survival (OS),
disease-specific survival (DSS), and
locoregional failure (LRF) rates were calculated using the
Kaplan-Meier method. LND (number of positive
lymph nodes/total number of excised lymph nodes) and
tumor-node-metastasis (TNM) staging variables
were subjected to multivariate analysis. RESULTS: Using the
median (LND0.06) as the cutoff point, LND
was found to be significantly associated with outcome. For
patients with LND 0.06, the OS was 58 per-
cent versus 28 percent for patients with LND >0.06 (P <
.001). Similarly, the DSS for patients with LND
0.06 was 65 percent and was 34 percent for those with LND
>0.06 (P < .001). On univariate analysis,
pathologic T and N classification, extracapsular spread, and LND
were found to be significant predictors of
outcome (P< .001). However, on multivariate analysis, LND
remained the only independent predictor of OS
(P .02; hazards ratio, 2.0), DSS (P .02; hazards ratio, 2.3),
and LRF (P .005; hazards ratio, 4.1). LND
was also found to be the only significant predictor of outcome
in patients receiving adjuvant radiotherapy
(P < .05). Within individual subgroups of pN1 or pN2
patients, LND reliably stratified patients according to
their risk of failure (P < .05). CONCLUSIONS: After surgery
for OSCC, pathologic evaluation of the neck
using LND was found to reliably stratify the risk of disease
recurrence and survival. Cancer 2009;115:570010.
VC 2009 American Cancer Society.
KEY WORDS: squamous cell carcinoma, head and neck, tongue,
survival, neck dissection.
Squamous cell carcinoma of the oral cavity (OSCC) is one of the
common malignant tumors of the
head and neck worldwide. The management of OSCC is largely
surgical and adjuvant treatment including
radiotherapy or chemoradiation is used for patients with
advanced stage tumors.1,2 Because adjuvant
therapy may induce severe toxic effects, a significant challenge
is to find a reliable method for stratifying
patients for the risk of tumor recurrence immediately after
surgery.
Received: September 23, 2008; Revised: November 25, 2008;
Accepted: January 5, 2009
Published online August 18, 2009 in Wiley InterScience
(www.interscience.wiley.com)
DOI: 10.1002/cncr.24631, www.interscience.wiley.com
Corresponding author: Ziv Gil, MD, PhD, Skull Base Service,
Department of Otolaryngology Head and Neck Surgery, Tel Aviv
Sourasky Medical
Center, Tel Aviv 64239, Israel; Fax (011) 972-3-6973543;
[email protected].
1Department of Surgery, Memorial Sloan-Kettering Cancer Center,
New York, New York; 2Department of Pathology, Memorial
Sloan-Kettering Cancer
Center, New York, New York
We thank Nancy Bennett for her editorial assistance and Maria
Coleman and Dr. Pen-Yuan Chu for their assistance in collecting the
data.
5700 Cancer December 15, 2009
Original Article
-
8/4/2019 Lymph Nodes in Oral Cancer
2/11
The conventional tumor-node-metastasis (TNM)
staging system quantifies lymph node disease according to
the number, size, and laterality of positive cervical lymph
nodes.3 This system factors the lymph node status into
6 categories: N0, N1, N2a, N2b, N2c, and N3. The pres-ence of 1
or more positive lymph nodes is a significant pre-
dictor of poor outcome. However, modern studies using
multivariate analysis report that, among patients with posi-
tive neck metastases, lymph node stage does not necessarily
predict prognosis, especially after adjuvant
radiotherapy.4-8
The extent of neck dissection, surgical technique,
and the level of histopathologic scrutiny determine the
degree to which the regional lymph nodes are examined
for neck metastasis and, hence, the probability of identify-
ing metastasis in lymph nodes at risk.9,10 Therefore, these
factors can be expected to determine the pN status (nega-tive or
positive) and the pN stage of the neck disease.
Recently, lymph node density (LND) (the number of pos-
itive lymph nodes/total number of excised lymph nodes)
has emerged as an alternative staging system for predicting
survival after surgery for carcinoma of the bladder11 and
esophagus.12 In this system, the ratio of positive lymph
nodes to the total number of excised lymph nodes was
found to be superior to conventional TNM lymph node
staging in predicting survival.13,14 Because limited lymph
node dissection may result in pathologic understaging,
LND attempts to compensate for this factor by recapitu-
lating 2 pieces of information: the extent of cancer spread
to the neck (number of positive lymph nodes) and the
extent of surgical lymph node clearance or sampling (total
number of lymph nodes removed during surgery). The
purpose of this study was to evaluate the utility of LND as
a potential prognostic predictor in patients with OSCC.
MATERIALS AND METHODS
Patients and Methods
Our study cohort included 386 patients treated with pri-
mary surgery, with or without adjuvant radiotherapy,
between 1986 and 1996 for OSCC. During this period,
adjuvant chemoradiotherapy was not yet used. Thus, this
provides a relatively more uniform cohort of patients than
could be expected from more recent years. All patients
underwent a standardized modified radical neck dissec-
tion involving levels I to IV or I to V as described by the
American Head and Neck Society.15 The type of neck dis-
section was prespecified in all patients before surgery. One
hundred ninety-five patients (50.5 percent) died of their
disease, 15 (3.9 percent) of them with distant metastases.
Table 1 presents demographic and clinical data on thesepatients.
The follow-up interval ranged from 4 to 184
months, with a median of 67 months.
Histopathologic Analysis
Lymph nodes were evaluated for metastasis by patholo-
gists at the Memorial Sloan-Kettering Cancer Institute.
All specimens were re-analyzed and evaluated by a single
pathologist (D.L.C.) who was blinded to the pathology
report. Overall, 5877 lymph nodes were evaluated, 457 of
which were positive.Specimen dissection and tissue sampling of
the pri-
mary tumor were performed in accordance with the cur-
rent guidelines for the histopathologic assessment of head
and neck cancer carcinoma.16 Neck dissection specimens
were submitted en block with metal tags attached desig-
nating the levels. Lymph nodes were detected by palpa-
tion. All lymph nodes identified by the pathologist were
submitted for analysis. Lymph nodes were defined as
aggregates of encapsulated lymphoid tissue of any size,
which had a peripheral sinus. Extracapsular spread (ECS)
was defined as tumor extension beyond the lymph node
capsule with a desmoplastic stromal response. Each lymph
node was sectioned every 2 mm, put in a different cassette,
and embedded in paraffin. Sectioning was performed at
200-lm intervals into the block. Lymph nodes with ECS
were representatively sectioned. There were 95 patients
with 173 lymph nodes that had evidence of ECS. Of
those, 100 lymph nodes (58 percent) had microscopic
extracapsular extension and 73 (42 percent) demonstrated
macroscopic extension.3
Statistical Analysis
Five-year overall survival (OS), disease-specific survival
(DSS), and locoregional control rates were calculated
using the Kaplan-Meier method, and the difference in
survival rate was assessed by the log-rank test.17 OS was
measured from the date of surgery to the date of death or
last follow-up. For DSS, the patients who died from
causes other than OSCC were censored at the time of
Lymph Node Density and Survival in Oral Cancer/Gil et al
Cancer December 15, 2009 5701
-
8/4/2019 Lymph Nodes in Oral Cancer
3/11
death. The variables that had prognostic potential sug-
gested by univariate analysis were subjected to multivari-
ate analysis with the Cox proportional hazards regression
model.18 All statistics were 2-sided (JMP; SAS Institute
Inc, Cary, NC). A value ofP< .05 was considered to indi-
cate statistical significance. Variables used to stratify
lymph node metastases included the total number of
lymph nodes dissected, the number of positive lymph
nodes, pN stage (pN0, pN1, pN2a, pN2b, pN2c, and
pN3), ECS of tumor, and the LND. The sixth edition of
the TNM staging system for OSCC was used for staging.3
LND distribution was evaluated as a continuous variable,and the
active data plot was best fitted by 4 Gaussian
equations using chi-square analysis (Microcal Origin;
Microcal Software Inc, Northampton, Mass). For analysis
of outcome, an LND cutoff point of or > the median
distribution (LND0.06) was used. Other cutoff points
tested were the intersection of the first and second Gaus-
sian equations (LND 0.05), the second and third Gaus-
sian equations (LND 0.076), or the third and fourth
Gaussian equations (LND 0.1). The 0.06 cutoff was
selected because the results of exploratory analysis demon-
strated no significant survival advantages over the otherratios,
except for risk stratification among a subgroup of
patients with pN2 disease and those undergoing therapeu-
tic neck dissections, for whom a cutoff point of 0.1 was
found to be a better predictor of outcome. Correlation
analysis was performed using Pearson regression
coefficient.
The study was approved by the institutional review
board committee.
RESULTSKaplan-Meier estimates of 5-year OS and DSS rates
were
61 percent and 70 percent, respectively. The management
and outcome of the entire cohort of 386 patients included
in the current study is summarized in Figure 1. On histo-
pathologic examination, 167 (43 percent) of the patients
had lymph node-positive disease. The 5-year OS rate for
patients with pathologically negative neck lymph nodes
was 76 percent and that for patients with positive lymph
nodes was 42 percent (P< .0001). The 5-year DSS of
patients with pathologically negative neck lymph nodes
was 85 percent and that for patients with positive lymph
nodes was 50 percent (P< .0001). Figure 2 shows the
Kaplan-Meier curves of OS and DSS according to the
lymph node (N) status.
Patients were further analyzed on the basis of the
pathologic status of their lymph nodes at the time of sur-
gery using the American Joint Committee on Cancer
(AJCC) TNM classification system. There were 219
patients with pN0 disease (57 percent), 72 patients with
Table 1. Patient Demographics
Variable No. ofPatients
%
Mean age, y 58 14 (range, 14-88) 386 100
Gender Male 227 59Female 159 41
Tobacco exposure No 54 33
Yes 258 67
Alcohol exposure No 68 18
Yes 189 82
Site Oral tongue 175 45
Floor of mouth 79 20
Upper gum 4 1
Lower gum 66 17
Hard palate 2 1
Retromolar trigone 36 9
Buccal mucosa 24 6
Treatment Surgery 162 42
Surgery and
adjuvant radiation
224 58
Type of neckdissection
Elective 264 68Therapeutic 122 32
Extent of neck
dissection
Selective neck
dissection
229 59
Modified radical
neck dissection
65 17
Radical neck
dissection
50 13
Bilateral neck
dissection
46 12
T classification 1 56 15
2 168 44
3 70 18
4 92 24
N classification N0 219 57
N1 72 19
N2a 2 1N2b 83 22
N2c 8 2
N3 2 1
Overall TNM stage I 44 11
II 103 27
III 90 23
IV 149 39
Follow-up of all
patients, mo
Mean: 65 49 219 57
Median: 67
Range: 4-184
Follow-up of
N patients, mo
Mean: 51 48 167 43
Median: 24
Range: 4-184
indicates positive; TNM, tumor-node-metastasis.
Original Article
5702 Cancer December 15, 2009
-
8/4/2019 Lymph Nodes in Oral Cancer
4/11
pN1 disease (18.5 percent), 93 patients with pN2 disease
(24 percent), and 2 patients with pN3 disease (0.5 per-
cent). The group of patients with N-positive disease
(n167) was analyzed to identify prognostic predictors
that reliably stratify the risk for adverse outcome within
this group. Among these patients, the number of lymph
nodes removed ranged from 6 to 114 (mean, 35 19
lymph nodes) and the number of positive lymph nodes
was between 1 and 22 (mean, 2.72.8 lymph nodes).
LND was calculated as the ratio of positive lymph nodes
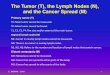
to the total number of lymph nodes removed. The distri-
bution of LND among the study population is shown in
Figure 3A. The LND frequency distribution could be reli-
ably fit by 4 Gaussian equations (P< .05). The median
LND was 0.06. The remainders of the parameters for
each of the 4 Gaussian equations are depicted in Figure
3A. The distribution of LND according to pN classifica-
tion is shown in Figure 3B. In the pN1 group (n 72),
the mean LND was 0.05 0.03 (range, 0.018-0.19); in
the pN2 group (n93), the mean LND was 0.12 0.09
(range, 0.01-0.5); and in the N3 group (n2), the mean
LND was 0.19 0.18 (range, 0.06-0.32). Statistical anal-
ysis demonstrated a significant difference in LND distri-
bution between the different pN classification groups (P
< .0001).
We next investigated whether an LND model can be
used to predict patient outcome. On univariate analysis,
pathologic T classification, pN classification, ECS, num-
ber of positive lymph nodes, and LND were found to be
significant predictors of outcome (P< .001). The total
number of excised lymph nodes was not found to be asso-
ciated with survival. An increase in the pN classification
was associated with decreased 5-year OS and DSS rates
(Fig. 4A and 4B, respectively). Similar to pN classifica-
tion, LND was also found to be significantly associated
with 5-year OS and DSS (Figs. 4C-4F). For patients with
LND0.06, the 5-year OS rate was 58 percent, versus 28
percent for patients with LND>0.06 (P< .001), as dem-
onstrated by the Kaplan-Meier curves. Similarly, the 5-
year DSS rate was 65 percent for patients with LND
0.06, versus 34 percent for patients with LND>0.06 (P
< .001). Based on the frequency distribution of LND,
FIGURE 2. Kaplan-Meier curves of overall and disease-spe-
cific survival are shown according to the lymph node (N)
sta-
tus. The difference in the survival rate was assessed using
the
log-rank test (P < .0001). Red line indicates pathologic
neck
status (pN) negative (-); green line, pN positive ().
FIGURE 1. The (A) management and (B) outcome of 386
patients who participated in the study are shown. cN indi-
cates clinical lymph node (N) status (negative [-] or
positive
[]); pN, pathologic neck status (negative or positive); END,
elective neck dissection; TND, therapeutic neck dissection;
OS, overall survival; DSS, disease-specific survival.
Lymph Node Density and Survival in Oral Cancer/Gil et al
Cancer December 15, 2009 5703
-
8/4/2019 Lymph Nodes in Oral Cancer
5/11
analysis was performed with the data set using an LND
separation point of 0.05, 0.076, and 0.1. These analyses
yielded similar results (P< .001).
To investigate whether LND predicts the prognosis
of patients with positive cervical lymph nodes, we first
cre-
ated a multivariate model with all relevant variables except
LND and then added LND to the model. The variables
compared were T classification, pN classification, overall
pathologic stage, ECS, total number of lymph nodes
excised, and total number of positive cervical lymph
nodes. On the first model (without LND), pN classifica-
tion was found to be the only significant predictor of OS
(P .03) and DSS (P .04). However when LND with a
separation point of 0.06 (median value) was introduced to
the multivariate model, the only significant predictor of
outcome was LND (OS, P .02; DSS, P .02; and
locoregional control, P .005), whereas the traditional
variables were not found to be independent predictors of
survival (Tables 2-4). In all analyses (of OS, DSS, and
locoregional control), the whole model proportional haz-
ards fits (-log likelihood and Pvalue) were better for the
model including LND than the model without LND
(Table 5). Similarly, when classification of the neck dis-
ease to N1, N2 and N3, was added to the model as an in-
dependent variable instead of pN classification, LND
remained the only significant predictor of outcome. In
addition, when patients with pN2 and pN3 disease were
grouped together, LND remained the only significant in-
dependent predictor of outcome (P< .05). We also used
3 other separation points in this analysis, as suggested by
the Gaussian function fit of the LND distribution: 0.05,
0.076, and 0.1. These analyses yielded similar results;however,
the 0.1 cutoff did not reach statistical signifi-
cance on multivariate analysis for DSS.
To further assess the ability of LND to predict treat-
ment response in a more homogeneous population and to
account for the potential impact of adjuvant treatment,
only those patients who receive postoperative radiother-
apy were subjected to multivariate analysis (n154).
Also in this subpopulation, LND was found to be the only
independent predictor of outcome on multivariate analy-
sis (P< .05).
The majority of the patients without clinical orradiologic
evidence of neck metastases (N-) underwent
selective neck dissection involving levels I to IV (80 per-
cent). The remaining patients underwent comprehensive
neck dissection. For patients with clinical evidence of
lymph node metastases (N), we performed a modified
radical neck dissection involving levels I to V in 84 per-
cent of the patients. Table 6 shows the different levels
dis-
sected in patients undergoing elective or therapeutic neck
dissection. The multivariate analysis was repeated for elec-
tive neck dissections (clinically negative necks) and thera-
peutic neck dissections (clinically positive necks)
separately. LND was found to be the most significant pre-
dictor of outcome for patients undergoing elective neck
dissection (P< .004). For therapeutic neck dissections,
none of the variables reached statistic significant when a
LND of 0.06 was used as the cutoff point. However,
when a separation point of 0.1 was used, LND remained
the only significant predictor of outcome (P< .04). Table
6 shows an increase in the yield of positive lymph nodes
and in the overall number of lymph nodes when therapeu-
tic neck dissection was used compared with elective neck
dissection (P< .0001), with no change in LND noted.
Finally, individual pN subgroups (pN1 alone or
pN2 alone) were stratified by LND at a cutoff of 0.06
using Kaplan-Meier analysis and the log-rank test. This
analysis demonstrates the ability of LND to predict OS (P
< .0002) and DSS (P< .001), even in the subgroup of
patients with pN1 disease. Similar results were found for
cutoff points of 0.05, 0.076, and 0.1 (P< .05). In the
pN2 subgroup, the ability of LND to predict OS and
FIGURE 3. The distribution of lymph node density (LND)
among the patients with positive neck lymph nodes is shown.
(A) The LND frequency distribution could be reliably fit by
4
Gaussian equations (P< .05). The median LND was 0.06. The
rest of the parameters for each 1 of the 4 Gaussian
equations
are depicted. (B) The distribution of LND according to
patho-
logic neck status (pN) classification is shown. Statistical
anal-
ysis demonstrated significant differences in LND
distribution
between the different pN classification groups (P<
.0001).
Original Article
5704 Cancer December 15, 2009
-
8/4/2019 Lymph Nodes in Oral Cancer
6/11
DSS was significant only for a cutoff point of 0.1. The
pN3 subgroup consisted of only 2 patients and therefore
was not included in this type of analysis. Figure 5 shows
the ability of LND to distinguish between low-risk and
high-risk patients within individual pN classification
subgroups.
DISCUSSION
Resection of the primary tumor with an appropriate neck
dissection is considered the standard of care for patients
with OSCC. Analysis of the patterns of failure in patients
with oral cancers reveals that approximately 33% of them
will fail due to regional metastases.7,19-21 Some of the
risk
factors for recurrence include T classification, surgical
margin status, depth of invasion, and major nerve inva-
sion.22 In addition, 1 of the most significant prognostic
factors in this population is the presence of neck metasta-
sis.19,23 Lymph node status and the number of positive
lymph nodes are primarily based on the lymph node sam-
pling procedure (ie, neck dissection) and secondarily on
examination by the pathologist. It was shown that cervical
metastases are more likely to be found for a lymph node
yield>20.9,10
Obviously, 1 of the weaknesses of the current study
is inconsistency in the analysis of the pathologic speci-
mens. In the current study cohort, the mean number of
lymph nodes removed was 35, with a standard deviation
FIGURE 4. The 5-year overall survival and disease-specific
survival rates as calculated using the Kaplan-Meier method in
patients
with positive cervical lymph nodes are shown (A and B) using the
tumor-node-metastasis (TNM) lymph node classification (P30
No. of positive lymph nodes 1 .57
>1
HR indicates hazards ratio; 95% CI, 95% confidence interval;
TNM, tumor-
node-metastasis.
Table 3. Multivariate Analysis of Prognostic Factors for
Overall Survival
Variable P HR 95% CI
T classification 1 .656
2
3
4
N classification N0 .22
N1
N2a
N2b
N2c
N3
Overall TNM stage I .95
II
IIIIV
Extracapsular spread No .6
Yes
Lymph node density 0.06 .02 2.0 1.1-3.5
>0.06
Total no. of lymph nodes 1-30 .36
>30
No. of positive lymph nodes 1 .19
>1
HR indicates hazards ratio; 95% CI, 95% confidence interval;
TNM, tumor-
node-metastasis.
Table 4. Multivariate Analysis of Prognostic Factors for
Locoregional Disease-Free Survival
Variable P HR 95% CI
T classification 1 .29
23
4
N classification N0 .24
N1
N2a
N2b
N2c
N3
Overall TNM stage I .31
II
III
IV
Extracapsular spread No .4
Yes
Lymph node density 0.06 .005 4.1 1.5-11.8
>0.06Total no. of lymph nodes 1-30 .12
>30
No. of positive lymph nodes 1 .62
>1
HR indicates hazards ratio; 95% CI, confidence interval; TNM,
tumor-node-
metastasis.
Table 5. Multivariate Analysis of Prognostic Factors for
Distant Metastases Disease-Free Survival
Cox Regression Model Without LND With LND
Overall survival
-Log likelihood 6.05 8.5
P .06 .01
Disease-specific survival
-Log likelihood 8.25 10.87
P .01 .0028
Locoregional control
-Log likelihood 3.14 7.1
P .4 .04
LND indicates lymph node density.
Original Article
5706 Cancer December 15, 2009
-
8/4/2019 Lymph Nodes in Oral Cancer
8/11
in the number of lymph nodes retrieved from the speci-
mens in the current study are, therefore, similar to other
studies. Furthermore, even after we excluded cases with
-
8/4/2019 Lymph Nodes in Oral Cancer
9/11
conventional lymph node staging.11,12,14,26,27 Simple to
calculate, LND is a ratio of the number of positive lymph
nodes divided by the total number of lymph nodes exam-
ined by the pathologist. It was postulated that LND may
have a greater prognostic value, because it takes into
con-sideration 3 factors: 1) tumor factors (number of positive
lymph nodes), 2) treatment factors (number of lymph
nodes removed during neck dissection), and 3) staging
factors (completeness of the sampling procedure, includ-
ing those related to the surgeon and pathologist). This
model proposes, for example, that a patient with 1 posi-
tive lymph node among 20 examined (LND 0.05) has a
better prognosis than a patient with 1 positive lymph
node out of 5 excised lymph nodes (LND0.2).
Although both patients will have the same pN classifica-
tion, the latter patient is more likely to have positivelymph
nodes left behind and therefore would be under-
staged by the conventional TNM system. Thus, the
patient with a higher ratio is expected to fare worse than
the patient with a lower ratio, although each has a similar
number of positive lymph nodes examined.
In the current study, we have evaluated for the first
time, to our knowledge, the value of LND in comparison
with the conventional staging system to determine its abil-
ity to predict OS, DSS, and locoregional recurrence-free
survival in patients undergoing neck dissection. Using
multivariate analysis, we found that, in patients with posi-
tive cervical lymph nodes, LND is superior to the conven-
tional N classification system (AJCC) in predicting OS,
DSS, and locoregional control. Our data also indicated
that LND is superior to T classification, ECS, overall
stage, and number of positive lymph nodes in predicting
survival. Within the subgroups of patients with pN1 or
pN2 neck disease, LND reliably distinguished between
low-risk and high-risk patients. Most importantly, multi-
variate analysis also demonstrated that LND is a better
predictor than conventional N classification for predicting
treatment failure in 3 groups of patients: those under-
going elective neck dissection, those undergoing therapeu-
tic neck dissection, and those receiving adjuvant
radiotherapy.
Recent studies have demonstrated slight improve-
ments in 5-year survival rates after adjuvant concurrent
chemoradiotherapy over radiotherapy alone for patients
with advanced head and neck SCC.1 However, due to the
significant morbidity of adding chemotherapy to radio-
therapy, considerable controversy remains regarding the
pathologic tumor characteristics that predict the need for
more aggressive adjuvant treatment. Furthermore, a
recent meta-analysis suggested that ECS and microscopi-
cally involved surgical margins, not pathologic N
classifi-cation, may serve as predictors of outcome and,
therefore,
can potentially help determine the type of adjuvant treat-
ment needed.8 The data from the current study indicate
that LND may be useful as an adjunct to the conventional
staging system in clinical studies investigating the role of
adjuvant therapy after surgery for patients with OSCC.
The LND ratio introduces into the equation the
expected variability in the extent of lymph node dissection
and may be even more important when surgeons perform
varying degrees of lymph node dissection. The value of
LND was studied in our institution, in which a standardneck
dissection is performed. For patients undergoing
very limited neck dissections and with very poor lymph
node yields, it is expected that LND will be higher than
that reported in the current study. Whether LND will
remain a significant predictor of outcome when different
techniques or types of neck dissection are used awaits fur-
ther evaluation.
Collinearity may exist when there are high correla-
tions among sets of independent variables.28 It is also
known that, when the collinearity is extreme (correlation
coefficiency R>0.85), the numeric accuracy of the multi-
variate model can be affected.29 Therefore, we studied the
correlation between LND and pN classification or the
number of positive lymph nodes using regression analysis.
In this analysis, the correlations were low (R 0.4
between LND and pN classification and R 0.6 between
LND and number of positive lymph nodes). These results
preclude profound effects on the multivariate model.29
We also found no significant correlation between the total
number of excised lymph nodes (positive and negative)
and the number of positive lymph node in the specimen
(R 0.3). This precludes the possibility of an inherent
bias in the number of lymph nodes removed during sur-
gery (ie, if the surgeon decides on the number of lymph
nodes to be resected during surgery, when there are multi-
ple positive lymph nodes).
Although the current study data provide a strong
argument in favor of lymph node ratios to stratify risk of
disease recurrence, other factors related to lymph node
status such as the size and volume of the occupied lymph
Original Article
5708 Cancer December 15, 2009
-
8/4/2019 Lymph Nodes in Oral Cancer
10/11
node, lymph node site, presence of occult micrometastases
discovered by molecular methods, and extent of ECS may
also be significant predictors of outcome and their inter-
play needs elaboration. Furthermore, the results of the
current study represent a single institutional experience,with a
relatively high median number of lymph nodes
examined by our pathologist (N30). Thus, it does not
necessarily comply with more limited dissections, in which
a denominator (total number of excised lymph nodes) of
-
8/4/2019 Lymph Nodes in Oral Cancer
11/11
23. Mamelle G, Pampurik J, Luboinski B, Lancar R, Lusinchi A,
Bosq J. Lymph node prognostic factors in head andneck squamous cell
carcinomas. Am J Surg. 1994;168:494-498.
24. Agrama MT, Reiter D, Topham AK, Keane WM. Node
counts in neck dissection: are they useful in outcomesresearch?
Otolaryngol Head Neck Surg. 2001;124:433-435.
25. Jose J, Coatesworth AP, MacLennan K. Cervical metastasesin
upper aerodigestive tract squamous cell carcinoma: histo-pathologic
analysis and reporting. Head Neck. 2003;25:194-197.
26. Kassouf W, Leibovici D, Munsell MF, Dinney CP, Gross-man HB,
Kamat AM. Evaluation of the relevance of lymph
node density in a contemporary series of patients under-going
radical cystectomy. J Urol. 2006;176:53-57; discus-sion 57.
27. Roder JD, Busch R, Stein HJ, Fink U, Siewert JR. Ratio
ofinvaded to removed lymph nodes as a predictor of survival
in squamous cell carcinoma of the oesophagus. Br J
Surg.1994;81:410-413.
28. Fraser GE, Stram DO. Regression calibration in studieswith
correlated variables measured with error. Am J Epide-miol.
2001;154:836-844.
29. Smith KR, Slattery ML, French TK. Collinear nutrientsand the
risk of colon cancer. J Clin Epidemiol. 1991;44:715-723.
Original Article
5710 Cancer December 15, 2009