Embed Size (px)
Citation preview

Molecular Staging of Lymph Nodes from Patients
with Esophageal Adenocarcinoma
Liqiang Xi,1,5 James D. Luketich,1,3 Siva Raja,1
William E. Gooding,2,3 Virginia R. Litle,1,5
Michael C. Coello,1 Sydney D. Finkelstein,4
Melissa L. Chestney,1 Rodney J. Landreneau,1,3
Steven J. Hughes,1,3 and Tony E. Godfrey1,3,5
Departments of 1Surgery and 2Biostatistics, University of Pittsburgh;The 3University of Pittsburgh Cancer Institute; 4Redpath IntegratedPathology, Pittsburgh, Pennsylvania; and 5Mount Sinai School ofMedicine, New York, New York
ABSTRACT
Purpose: This study was designed to evaluate molecular
markers for the detection of micrometastasis in esophageal
adenocarcinoma, define algorithms to distinguish positive
from benign lymph nodes and to validate these findings in an
independent tissue set and in patients with pN0 esophageal
adenocarcinoma.
Experimental Design: Potential markers were identified
through literature and database searches. All markers were
analyzed by quantitative reverse transcription (QRT)-PCR
on a limited set of primary tumors and benign lymph nodes.
Selected markers were further evaluated on a larger tissue
set and classification algorithms were generated for individ-
ual markers and combinations. Algorithms were statistically
validated internally as well as externally on an independent
set of lymph nodes. Selected markers were then used to
identify occult disease in lymph nodes from 34 patients with
pN0 esophageal adenocarcinoma.
Results: Thirty-nine markers were evaluated, six
underwent further analysis and five were analyzed in the
external validation study. Two markers provided perfect
classification in both the screening and validation sets,
although parametric bootstrap analysis estimated 2% to
3% optimism in the observed classification accuracy. Several
marker combinations also gave perfect classification in the
observed data sets, and estimates of optimism were lower,
implying more robust classification than with individual
markers alone. Five of thirty-four patients with esophageal
adenocarcinoma had positive nodes by multimarker QRT-
PCR analysis and disease-free survival was significantly
worse in these patients (P = 0.0023).
Conclusions: We have identified novel QRT-PCR
markers for the detection of occult lymph node disease in
patients with esophageal adenocarcinoma. The objective
nature of QRT-PCR results, and the ability to detect occult
metastases, make this an attractive alternative to routine
pathology.
INTRODUCTION
At the time of diagnosis, many patients with esophageal
adenocarcinoma already have distant metastatic disease, and
thus, surgical resection is not an option. For earlier stage patients,
however, surgery offers the best hope for long-term cure. In these
patients, the most important prognostic factor is the involvement
of regional lymph nodes. Five-year survival for patients with any
lymph node involvement averages < 25%, whereas survival in
node-negative patients is 55% to 65% (1, 2). These low survival
rates reflect the limitations of surgical treatment in an aggressive
and frequently systemic disease for which current chemotherapy
regimens are ineffective. In lymph node–negative patients,
surgical resection alone should theoretically result in cure.
Clearly this is not the case, suggesting that many patients may
have pathologically occult lymph node involvement or hema-
togenous tumor spread with clinically occult distant metastases.
Indeed, many recent studies have shown the presence of occult
metastases in lymph nodes from patients with esophageal cancer
staged as pathologically node-negative (pN0; refs. 3–14). These
studies indicate that 1% to 17% of histologically negative lymph
nodes and 11% to 50% of pN0 patients have nodal metastases that
are missed by routine pathologic evaluation. Furthermore, of the
studies that include clinical follow-up data (3–10, 15), all but
one (15), show a significant correlation of occult lymph node
disease with poor outcome.
In the majority of reported studies, occult metastases have
been detected using additional sectioning of formalin-fixed
lymph nodes, followed by immunostaining with pan-cytokeratin
antibodies. From the literature on several tumor types, it seems
that both increased tissue sampling and the addition of
immunohistochemistry contribute to increased lymph node
metastasis detection rates (7, 8, 10, 16–28). Unfortunately, such
detailed lymph node analysis remains restricted to diseases such
as breast cancer and melanoma where the use of sentinel lymph
node biopsy greatly reduces the number of nodes to be examined.
In breast cancer, however, significant discordance has been
reported for interpretation of sentinel lymph nodes by different
pathologists (29), indicating that pathologic examination is a
difficult and subjective process when small volumes of tumor are
involved. In esophageal cancer, > 20 lymph nodes are typically
removed, and therefore, detailed pathologic analyses of each
node with immunohistochemical staining is not feasible. In a
Received 4/27/04; revised 10/20/04; accepted 11/3/04.Grant support: NIH/National Cancer Institute CA90665-01 researchgrant, the Veterans Administration Pittsburgh Health Care System, anda cooperative research and development agreement with Cepheid(Sunnyvale, CA).The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely toindicate this fact.Note: Supplementary data for this are available at Clinical CancerResearch Online (www.mssm.edu/labs/godfrt01/index.html).Requests for reprints: Tony E. Godfrey, Mount Sinai School ofMedicine, One Gustave L. Levy Place, Box 1668, New York,NY 10029. Phone: 212-659-9082; Fax 212-849-2523; E-mail: [email protected].
D2005 American Association for Cancer Research.
Vol. 11, 1099–1109, February 1, 2005 Clinical Cancer Research 1099
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

different approach, several groups have recently shown that
molecular staging, using reverse transcription (RT)-PCR, can also
detect occult lymph node metastasis in cancer patients. In these
studies, RT-PCR typically gives positive results in 6% to 49% of
lymph nodes and 50% to 100% of pN0 patients (11, 13, 14). This
high frequency of positive results in pN0 patients, many of whom
do not recur, has led to criticism of the RT-PCR technique on the
basis of poor specificity. To overcome this problem, most
investigators have begun to use quantitative RT (QRT)-PCR for
detection of occult metastasis. In esophageal cancer patients, we
recently reported that QRT-PCR allowed us to obtain high
(f90%) sensitivity for predicting disease recurrence in node-
negative patients, although still maintainingf90% specificity. In
our study, we quantified expression of carcinoembryonic antigen
(CEA), a somewhat generic adenocarcinoma marker, to achieve
these results. However, recent studies in breast and lung cancer
have identified genes that are considerably superior to CEA for
detecting lymph node metastases. Thus, the goal of this study was
to identify and test potential molecular markers for detection of
occult lymph node metastasis in esophageal adenocarcinoma.
MATERIALS AND METHODS
Identification of Potential Markers. An extensive
literature and public database survey was conducted to identify
any potential markers relevant to esophageal adenocarcinoma.
Resources for this survey included PubMed, OMIM, UniGene
(http://www.ncbi.nlm.nih.gov/), GeneCards (http://bioinfo.
weizmann.ac.il/cards), and CGAP (http://cgap.nci.nih.gov). Our
survey criteria were somewhat flexible but the goal was to
identify genes with moderate to high expression in esophageal
adenocarcinoma and low expression in normal lymph nodes. In
addition, genes reported to be up-regulated in esophageal
adenocarcinoma and genes with restricted tissue distribution
were considered potentially useful. Finally, genes reported to be
cancer-specific, such as the cancer testis antigens and hTERT,
were evaluated.
Tissues and Pathologic Evaluation. Tissue specimens
were obtained from tissue banks at the University of Pittsburgh
Medical Center through Institutional Review Board approved
protocols. One half of each lymph node, and a small piece of
each primary tumor, were snap-frozen in liquid nitrogen and later
embedded in optimal cutting temperature compound (oct) for
frozen sectioning and RNA isolation. The remaining tissue was
used for routine diagnostic pathology evaluation. Twenty 5-Amsections were cut from each frozen tissue piece for RNA
isolation. In addition, sections were cut and placed on slides for
H&E and immunohistochemical analysis at the beginning,
middle (between the 10th and 11th sections for RNA), and end
of the sections for RNA isolation. All three H&E slides from
each specimen underwent pathological review to confirm
presence of tumor, percentage of tumor, and to identify the
presence of any contaminating tissues (such as esophagus or
lung tissue on a lymph node). All of the unstained slides were
stored at �20jC. Immunohistochemistry evaluation was done
using the AE1/AE3 antibody cocktail (DAKO, Carpinteria, CA),
and Vector Elite ABC kit and Vector AEC Chromagen (Vector
Laboratories, Burlingame, CA). Immunohistochemistry was
used as needed to confirm the H&E histology. Only tissues on
which diagnostic pathology and frozen section pathology that
were concordant were included in the screening tissue sets.
Patients with Esophageal Adenocarcinoma. A total of
314 lymph nodes were analyzed from thirty four consecutive,
consenting patients (median 8.5 nodes per patient) with
esophageal adenocarcinoma. All patients signed informed
consent for this study using protocols and consent forms
approved by the University of Pittsburgh Institutional Review
Board. The final pathology staging, recurrence status, and other
clinical information on these patients is shown in Table 1.
Recurrence information was obtained by review of clinical charts
and electronic medical records by three of the authors (J.D.
Luketich, V.R. Litle, and M.C. Coello).
Marker Screening. The screening was conducted in two
phases. All potential markers entered the primary screening
phase and expression was analyzed in six primary esophageal
cancers and 10 benign lymph nodes obtained from patients
without cancer (five RNA pools with two lymph node RNAs per
pool). Markers that showed good characteristics for lymph node
metastasis detection (i.e., high expression in primary tumors and
low expression in benign lymph nodes) passed into the
secondary screening phase. The secondary screen consisted of
expression analysis on 18 primary tumors, 20 histologically
positive lymph nodes, and 21 benign lymph nodes from
21 patients without cancer (referred to as the screening tissue
set). All tumors and positive lymph node samples were from
independent patients.
Marker Validation. To externally validate the classifica-
tion accuracy of markers tested in the secondary screen, an
independent, validation, set of lymph nodes was analyzed. The
validation set consisted of 32 benign lymph nodes from patients
without cancer and 24 pathology-positive lymph nodes obtained
from patients undergoing surgery for esophageal adenocarcino-
ma. Diagnostic pathology and frozen section pathology were
concordant on all nodes in the validation set. In addition, we also
analyzed 14 lymph nodes from esophageal cancer patients which
were determined to be positive on routine diagnostic pathology
but were negative by our own pathology (H&E and immuno-
histochemistry) on the frozen tissue piece (discordant lymph
node set). As with the screening set, all lymph nodes were from
independent patients.
RNA Isolation and cDNA Synthesis. RNA was isolated
using the RNeasy minikit (Qiagen, Valencia, CA) essentially as
described by the manufacturer. The only modification was that
we doubled the volume of lysis reagent and loaded the column in
two steps. This was found to provide better RNA yield and
purity. All RNAs were DNase-treated using the DNA-free kit
from (Ambion, Austin, TX) and reverse transcription was done
in 100 AL reaction volumes with random hexamer priming and
Superscript II (Invitrogen, Carlsbad, CA) reverse transcriptase
(30). For the primary screen, two reverse transcription reactions
were done, each with 1,000 ng of RNA. The cDNAs were
combined and quantitative PCR (QPCR) was done using the
equivalent of 20 ng RNA per reaction. For the secondary screen,
the RNA input for primary tumors and positive nodes was 1,200
ng per RT reaction and 20 ng per QPCR reaction, but this was
increased to 2,000 ng per RT reaction and 80 ng per QPCR
reaction for the benign nodes in order to improve sensitivity for
detection of low background expression.
RT-PCR of Lymph Nodes from Patients with Esophageal Cancer1100
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

Quantitative PCR. All QPCR reactions were done on
the ABI Prism 7700 Sequence Detection Instrument (Applied
Biosystems, Foster City, CA). Relative expression of the
marker genes was calculated using the y-CT methods
previously described (30, 31) and with h-glucuronidase as
the endogenous control gene. All assays were designed for use
with 5V nuclease hybridization probes although the primary
screening was done using SYBR Green quantification in order
to save on costs. Assays were designed using the ABI Primer
Express Version 2.0 software, and where possible, amplicons
spanned exon junctions in order to provide cDNA specificity.
In addition, all primer pairs were tested empirically for
amplification from 100 ng of genomic DNA and primers were
redesigned when necessary. With the exception of cytokeratin
19 (CK19), cDNA-specific primer sets were successfully
identified for all genes in this study. Finally, optimal annealing
temperature was determined by testing primers for generation
of a single band on gels using cDNA templates and annealing
temperatures of 60jC, 62jC, and 64jC. Further details
describing our methods for primer design and testing have
recently been published (32). PCR efficiency was estimated
using SYBR green quantification prior to use in the primary
screen. Further optimization and more precise estimates of
efficiency were done with 5V nuclease probes for all assays
used in the secondary screen.
A mixture of the Universal Human Reference RNA
(Stratagene, La Jolla, CA) and RNAs from human placenta,
thyroid, heart, colon, PCI13 cell line, and SKBR3 cell line
served as a universal positive expression control for all the genes
in the marker screening process. Tissue RNAs were batched for
reverse transcription and the positive control RNA was included
in each batch. Batches of cDNAs were then analyzed by QPCR
Table 1 Clinical characteristics of the 34 patients with esophageal adenocarcinoma studied for occult disease
PatientID
Tumorstage
Nodestage
Metastasisstage
Finalstage
Neoadjuvanttherapy
QRT-PCRresults
Recurrencesite
Follow-uptime (months)
1 T3 N0 M0 IIA yes Neg none 26.62 T1 N0 M0 I no Neg none 24.23 T3 N0 M0 IIA yes Neg adrenal
metastasis,liver
26.7
4 T3 N0 M0 IIA yes Pos* celiaclymph nodes,liver, brain
18.0
5 T3 N0 M0 IIA yes Neg pleural fluid 7.96 T1 N0 M0 I no Neg none 25.47 T3 N0 M0 IIA no Neg none 27.78 Tis N0 M0 0 no Neg none 28.39 T1 N0 M0 I yes Neg none 23.710 T1 N0 M0 I no Neg none 4.311 T1 N0 M0 I no Neg none 25.512 T3 N0 M0 IIA no Neg none 26.113 T2 N0 M0 IIA no Neg none 22.314 T1 N0 M0 I no Neg none 5.615 T1 N0 M0 I no Neg none 23.516 T0 N0 M0 0 yes Neg stomach 11.617 T2 N0 M0 IIA yes Neg pleural fluid,
pericardium7.9
18 T1 N0 M0 I no Pos liver, abdomen,carcinomatosis
12.1
19 T1 N0 M0 I no Neg none 14.420 T1 N0 M0 I yes Pos liver 11.421 T0 N0 M0 0 yes Neg none 20.822 T0 N0 M0 0 yes Neg none 11.623 T1 N0 M0 I no Neg none 18.124 T0 N0 M0 0 yes Neg none 17.225 T3 N0 M0 IIA no Pos none 17.926 T1 N0 M0 I no Neg none 5.427 T2 N0 M0 IIA no Neg none 12.128 T2 N0 M0 IIA yes Pos retroperitoneal,
celiac, superiormesenteri arterylymph nodes
7.0
29 Tis N0 M0 0 no Neg none 8.430 T0 N0 M0 0 yes Neg brain/central
nervous system13.6
31 T2 N0 M0 IIA no Neg none 12.432 T0 N0 M0 0 yes Neg none 11.633 T1 N0 M0 I no Neg none 9.534 T3 N0 M0 IIA no Neg none 6.7
*This patient had two nodes positive by QRT-PCR.
Clinical Cancer Research 1101
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

one gene at a time on 96-well plates. Thus, the positive control
RNA acted as a control for both reverse transcription and QPCR
of each batch. The positive control was not used for calculation
of relative expression.
Quantification with SYBR Green (Primary Screen).
For SYBR Green I-based QPCR, each 50 AL reaction contained
1� TaqMan buffer A (Applied Biosystems), 300 nmol/L each
deoxynucleotide triphosphate, 3.5 mmol MgCl2, 0.06 units/ALAmplitaq Gold (Applied Biosystems), 0.25� SYBR Green I
(Molecular Probes, Eugene, OR), and 200 nmol/L each primer.
The amplification program comprised two stages with an initial
95jC Taq activation stage for 12 minutes followed by 40 cycles
of 95jC denaturation for 15 seconds, 60jC, 62jC, or 64jCanneal/extend for 60 seconds and a 10-second data collection
step at a temperature 2jC to 4jC below the Tm of the specific
PCR product being amplified (ref. 33; more information on this
technique is provided in the Supplementary Methods available
online at www.mssm.edu/labs/godfrt01/index.html). After am-
plification, a melting curve analysis was done by collecting
fluorescence data while increasing the temperature from 60jC to
95jC over 20 minutes.
Quantification with 5V Nuclease Probes (Secondary
Screen). Probe-based QPCR was done as described previously
(12, 31). Briefly, reactions were done with a probe concentration
of 200 nmol/L and a 60-second anneal/extend phase at 60jC for
h-GUS, CK19, and CK20, 62jC for CK7 and Villin 1, and
64jC for CEA and TACSTD1. The sequences of primers and
probes (purchased from IDT, Coralville, IA) for genes evaluated
in the secondary screen are available in Supplemental Table 1 at
www.mssm.edu/labs/godfrt01/index.html. The primer sequences
for markers used in the primary screen will be provided upon
request.
Quantitative PCR Analysis. In the primary screen, data
from the melt curve was analyzed using the ABI Prism 7700
Dissociation Curve Analysis 1.0 software (Applied Biosystems).
The first derivative of the melting curve was used to determine
the product Tm as well as to establish the presence of the specific
product in each sample. In general, samples were analyzed in
duplicate PCR reactions and the average C t value was used in
the expression analysis. However, in the secondary screen,
triplicate reactions were done each individual benign node and
the lowest C t value was used to calculate relative expression and
thus obtain the highest (most conservative) estimate of
background expression for the sample.
Statistical Analysis
Generation of Prediction Rules. Six markers that passed the
secondary screen were evaluated individually and in combination
with other markers. The characteristics used to evaluate markers
were sensitivity, specificity, classification accuracy, and the area
under the ROC curve. For individual markers, a cutoff value was
determined that maximized the classification accuracy (proportion
of lymph nodes correctly classified). In cases where classification
accuracy was 100%, the cutoff was set at the midpoint between the
highest expressing benign node and the lowest expressing,
histologically positive node. Markers were also combined into
pairs and for lymph node classification and a linear prediction rule
was generated for each pair. The rule was equivalent to the linear
predictor that equalized the fitted probabilities above and below
the linear boundary. That is, points on the boundary line had a
predicted probability midway between the numerical scores
assigned to positive and negative nodes. For example, if positive
nodes were assigned a score of 2 and benign nodes a score of 1,
predicted scores > 1.5 were classified as positive.
Internal Validation of Prediction Rules. Properties of single
and paired marker prediction rules were investigated by
examining the distributional properties of the observed marker
expression levels and by applying parametric bootstrap valida-
tion. Data were simulated from the lognormal and bivariate log-
normal distributions using moment estimators for mean, variance,
and correlation between marker pairs. One thousand parametric
samples of the original data were obtained and the prediction for
each bootstrap sample was applied to the original data. The
difference between the observed classification accuracy and
the average bootstrap classification accuracy was used to estimate
the optimism in the resubstitution prediction rules (34).
External Validation of Prediction Rules. External vali-
dation of the prediction rules generated in the secondary
screen was done on an independent set of benign lymph nodes
(n = 32) and positive lymph nodes (n = 24) from patients with
esophageal cancer. The prediction rules for individual
markers and marker combinations were applied to data from
the validation set and classification characteristics were
calculated.
RESULTS
Primary Screen. Our literature and database surveys
identified a total of 39 genes for evaluation in the primary screen.
All of these genes were analyzed for expression in six primary
esophageal tumors and 10 benign lymph nodes. Median relative
expression (relative to the endogenous control gene) in the
primary tumors and in benign nodes was calculated for each
gene in the primary screen and is reported in Table 2. In addition,
we also calculated the ratio of relative expression between the
lowest expressing tumor and the highest expressing benign node
and between the median expression in tumors and the highest
expressing benign node. Some genes, such as CK20, had no
detectable expression in benign nodes and therefore ratios could
not be calculated. With the exception of CK20, however, all
genes with undetectable expression in benign nodes also have
very low median expression in the primary tumors and as a
result, these genes are unlikely to be sensitive markers for
detection of occult disease.
When using median expression in the tumors as the
numerator, six genes (TACSTD1, CK19, CK7, CEA, Villin 1,
and CDX1) clearly stand out as having tumor/benign node ratios >
1,000. When the minimum difference between tumors and benign
nodes is calculated as a ratio (lowest tumor/highest benign node),
all of these genes still distinguish tumors from benign nodes very
well. CDX1 however does not seem to be quite as good as the
other five genes because it has a minimum-fold ratio of only 68.7
versus >234 for the other five genes. Based on this data, CEA,
CK7, TACSTD1, CK19, and Villin 1 were chosen for analysis in
the secondary screen. In addition, CK20 was analyzed in the
secondary screen based on the finding that it was moderately
expressed in tumors but undetectable in benign nodes. Detailed
data on genes in the primary screen that were not analyzed in the
secondary screen will be made available on request.
RT-PCR of Lymph Nodes from Patients with Esophageal Cancer1102
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

Secondary Screen. Histologic evaluation of the 18 pri-
mary adenocarcinoma specimens used in the secondary screen
revealed a median tumor percentage of 70% with a range of 5%
to 100%. Similarly, in the 20 histologically positive nodes, the
median tumor percentage was 50% with a range of 2% to 100%.
The relative expression profiles of the markers selected for the
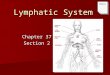
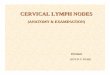
secondary screen are shown in Fig. 1. The data shows that these
markers are expressed in positive lymph nodes as well as in
primary tumors indicating that metastatic tumor cells continue to
express these markers. Interestingly, however, analysis of the
percentage of tumor cellularity compared with marker expres-
sion level revealed only weak associations in all cases except
TACSTD1. Figure 1 also indicates the relative expression cutoff
values that provide the most accurate classification of histolog-
ically positive and negative nodes. Of the six markers chosen
from our original screen, all but CK7 was able to classify
positive and negative lymph nodes with > 95% accuracy in the
secondary screen (Table 3). Furthermore, two markers, CK19
and TACSTD1, provided perfect classification. Of these two,
however, the distribution of expression levels in positive and
negative nodes is less variable for TACSTD1 than for CK19 and
the difference between the distributions is greater for TACSTD1.
Thus, one may expect that on a larger sample set, TACSTD1
would prove superior to CK19. In an attempt to address this
issue, we did an internal marker validation using parametric
bootstrap analysis to estimate the optimism in our observed
classification accuracy. Essentially, the expression distribution
observed in positive and negative lymph nodes was statistically
modeled (as illustrated in Fig. 1B and C) and 41 new data
points (20 positive and 21 negative) were artificially generated.
The most accurate cutoff value calculated from the artificial
data points was then applied to the original 41 data points and
the classification accuracy was determined. This was
repeated 1,000 times and the average values for classification
Table 2 Primary screen data on relative expression of potential markers in esophageal adenocarcinoma specimens and benign lymph nodes
MarkerAccessionnumber
Mediantumor
Medianbenign node
Highestbenign node
Lowest tumor/highestbenign node
Median tumor/highestbenign node
TACSTD1 NM_002354 126.5271 0.009753 0.049549 505.0 2,553.6TM4SF3 NM_004616 54.36396 0.025295 0.136787 39.8 397.4CK19 NM_002276 31.30345 0.003691 0.018163 504.2 1,723.5CK18 NM_000224 11.81054 0.033609 0.073557 30.0 160.6CK7 NM_005556 7.063151 0.000953 0.003162 234.7 2,233.8MMP7 NM_002423 5.607552 0.009453 0.099098 0.1 56.6CEA NM_004363 3.339841 0.000175 0.00027 1,964.2 12,369.8PVA NM_001944 2.888319 —* 0.021197 1.8 136.3Villin 1 NM_007127 2.288635 0.000288 0.000433 2,010.5 5,285.5SCCA1/2 NM_006919 1.825825 0.000014 0.015571 1.8 117.3Survivin NM_001169 0.790635 0.022251 0.113834 0.7 6.9CK20 NM_019010 0.767534 —y —y 1 1MAGEA3 NM_005362 0.319258 0.000328 0.001271 0.01 251.2c-MET NM_000245 0.307788 0.020617 0.039692 5.1 7.8MAGEA2 NM_005361 0.117915 —* 0.000279 0.04 422.6CDX1 NM_001804 0.099384 0.000003 0.000016 68.7 6,211.5bHCG NM_000737 0.029632 0.001616 0.009005 1.1 3.3NIS NM_000453 0.026305 0.003933 0.016232 0.6 1.6PTHrP NM_002820 0.019655 0.001186 0.004425 0.5 4.4NTS NM_006183 0.016921 0.532185 2.321408 0.00003 0.007hTERT NM_003219 0.01441 0.012648 0.026645 0.2 0.5MAGEA12 NM_005367 0.00929 0.000103 0.000404 0.002 23.0BRDT NM_001726 0.005306 0.000065 0.00035 0.003 15.2LDHC NM_017448 0.003147 —* 0.016402 0.1 0.2ITGB4 NM_000213 0.001867 0.000038 0.000063 13.3 29.6TITF1 NM_003317 0.001649 0.00132 0.007625 0.01 0.2GAGE1 NM_001468 0.001016 0.000221 0.002159 0.0005 0.5CK14 NM_000526 0.000917 —y —y 1 1MAGEA1 NM_004988 0.000524 —y —y —z 1KRTHB1 NM_002281 0.000417 —* 0.000165 0.2 2.5MAGEA4 NM_002362 0.000295 —y —y —z 1SSX2 NM_003147 0.000209 —y —y —z 1MAGEA10 NM_021048 0.000063 —y —y —z 1SGY-1 NM_014419 0.000054 0.000134 0.000605 0.002 0.1STX NM_006011 0.000054 0.00003 0.000194 0.005 0.3SSXux 0.000044 —y —y —z 1GAGEux —* —* 0.000126 —z —zMAGEA8 NM_005364 —* —y —y —z —zNY-ESO-1 NM_001327 —* —* 0.002036 —z —z
NOTE. Genes in boldface were analyzed further in the secondary screen. ‘‘Median tumor’’ and ‘‘Median benign node’’ indicates the medianexpression level in primary tumors and benign nodes.
*Three or more samples were at the nondetectable level in 40-cycle QPCR.yAll samples tested were at the nondetectable level in 40-cycle QPCR.zLowest or median expression levels of tumor were at nondetectable levels in 40-cycle QPCR.xUniversal design to amplify all submembers in the gene family.
Clinical Cancer Research 1103
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

Fig. 1 A, secondary screen data showing the expression profiles of selected markers in primary esophageal tumors (T), histologically positivelymph nodes (PN), and benign lymph nodes (BN). Open, light blue diamonds, samples where expression of CK20 was undetectable at 40 PCRcycles. The expression levels for these six samples were artificially calculated using a CK20, C t value of 40 cycles. B and C, examples illustratingthe approach used for analysis of data from the secondary marker screen. B, data obtained from Villin 1 and CEA; C, data from CK19 andTACSTD1. In each example, the top left graph shows the observed expression data for the selected gene on the 41 lymph nodes in the secondaryscreen, along with the most accurate cutoff value for lymph node classification. The bottom left graphs illustrate how lymph node classification wasanalyzed using combinations of marker pairs. In this case, the prediction rule used to classify nodes was calculated such that it split the region intotwo zones of equal prediction probability as described in Materials and Methods. For the top and bottom right graphs, the distribution characteristicsof expression in the positive and negative nodes were statistically modeled for each marker, or marker combination, based on the observedexpression data. Two hundred simulated positive and negative nodes were then randomly drawn from populations with these modeled distributionsand plotted. These plots illustrate how the cutoff values and prediction rules calculated from the observed data may be expected to fare when a largernumber of nodes is examined and more extreme values of expression levels are observed. This distribution modeling and resampling approach wasalso used in the calculation of parametric bootstrap estimates shown in Table 3. B, although CEA and Villin 1 were imperfect discriminators bythemselves, combining their information improves prediction in both the observed and simulated data. The larger dispersion seen in the simulatedpositive nodes reflects the lower correlation, and greater variance, found with these two markers and in positive lymph nodes in general. Among theindividual markers, TACSTD1 and CK19, yielded the best empirical discrimination and this also held up well in the simulated data. In addition toyielding the best single marker prediction properties, CK19 and TACSTD1 also benefit from being highly correlated with one another. Highercorrelation tends to limit variability in the bivariate distribution.
RT-PCR of Lymph Nodes from Patients with Esophageal Cancer1104
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

characteristics on the original 41 lymph nodes were calculated
(Table 3, bootstrap estimates). Because the parametric method
takes into account the distribution in the observed data, markers
with tighter and more separated distributions should fare better
in this analysis. Overall, the estimates of optimism were quite
low (2-5%), indicating that robust classification of lymph nodes
should be possible with these markers. Individually, CK19 and
TACSTD1 were again the best markers with estimated
classification accuracies of 97% and 98%, respectively.
In addition to analyzing individual markers, we also
evaluated lymph node classification using paired marker
combinations. Marker pairs were evaluated by plotting graphs
similar to those in Fig. 1B and C (bottom left), and then
mathematically calculating a linear cutoff that was midway
between the positive and negative lymph node distributions.
Classification accuracy obtained for all marker combinations
using this approach are shown in Table 3 (observed data). All
combinations achieved accuracies of 98% or greater but, as with
the individual markers, this is likely to be optimistic. However,
parametric bootstrap analysis estimated that, on average,
classification accuracy dropped <1% compared with the
observed data when using marker combinations (Table 3,
parametric bootstrap estimates).
External Marker Validation. To perform a more robust
evaluation of the cutoff values and prediction rules generated in
the secondary screen, five markers (CK7 was omitted due to
poor classification characteristics in the secondary screen) were
further evaluated in an independent, validation set of positive
and benign lymph nodes. Pathology analysis of the 24 positive
nodes in this set determined that the median tumor percentage
was 80% with a range of 2% to 100%. In general, application
of the cutoff values and prediction rules to the validation set
resulted in classification characteristics of individual markers
that were very similar to those estimated by the parametric
bootstrap analysis used for internal validation in the
secondary screen (Supplemental Table 2 and Fig. 2). The
two clear exceptions to this were Villin 1 and CK20, where
the specificity was clearly worse than in the secondary screen
and as a result, overall classification accuracy dropped by 7%
to 10% compared with the bootstrap estimate data from the
secondary screen. TACSTD1 and CK19 once again stood out
as the best individual markers with 100% accuracy in this set.
All combinations of marker pairs resulted in classification
accuracy > 92%, even those including Villin 1, and 7 of the
10 combinations gave perfect, 100% classification in the
validation set.
Analysis of Nodes with Discordant Pathology. As part
of our ongoing studies on esophageal cancer, we have now
analyzed over 600 lymph nodes using the markers described in
this study. Of these nodes, we have found 14 where the half of
the lymph node sent for diagnostic pathology was positive, but
our own pathology (including immunohistochemistry) on the
frozen lymph node half was inconclusive. One pathologist called
our sections from all 14 nodes negative, whereas a second
pathologist thought that 8 of the nodes were positive. Two
additional pathologists were asked to review these cases and
come to a consensus opinion. Their examination concluded that
3 of the 14 nodes were positive and these 3 were among the
8 identified by the second pathologist. Two of these three nodes
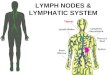
were positive based on QRT-PCR for multiple markers (Fig. 2),
whereas the third node was positive only by QRT-PCR for
CK20.
Table 3 Individual and marker pair classification characteristics on positive and benign lymph nodes in the secondary screen
Observed data Parametric bootstrap estimates*
Markers Sensitivity SpecificityClassificationaccuracy Sensitivity Specificity
Classificationaccuracy
CEA 0.95 0.95 0.98 0.95 0.93 0.93CK7 0.95 0.86 0.94 0.90 0.82 0.89CK19 1.0 1.0 1.0 1.0 0.99 0.94CK20 1.0 0.95 0.995 0.98 0.98 0.92TACSTD1 1.0 1.0 1.0 1.0 0.96 0.99Villin 1 0.95 0.95 0.98 0.95 0.92 0.93CEA + CK7 0.95 1.0 0.98 0.93 0.99 0.96CEA + CK19 0.95 1.0 0.98 0.97 0.99 0.98CEA + CK20 0.95 1.0 0.98 0.97 0.99 0.97CEA + TACSTD1 1.0 1.0 1.0 0.99 1.0 0.99CEA + Villin 1 0.95 1.0 0.98 0.95 1.0 0.98CK7 + CK19 1.0 1.0 1.0 0.99 0.99 0.99CK7 + CK20 0.95 1.0 0.98 0.93 0.99 0.97CK7 + TACSTD1 1.0 1.0 1.0 0.99 1.0. 0.99CK7 + Villin 1 0.95 1.0 0.98 0.95 0.99 0.98CK19 + CK20 0.95 1.0 0.98 0.97 0.99 0.98CK19 + TACSTD1 1.0 1.0 1.0 0.99 1.0 0.99CK19 + Villin 1 1.0 1.0 1.0 0.99 0.99 0.99CK20 + TACSTD1 1.0 1.0 1.0 0.99 1.0 0.99CK20 + Villin 1 0.95 1.0 0.98 0.94 1.0 0.97TACSTD1 + Villin 1 1.0 1.0 1.0 0.99 1 0.99
*Classification characteristics are calculated based on the observed data from 41 lymph nodes (left side of table) and also using parametricbootstrap analysis (right side). One thousand parametric bootstrap samples of 41 lymph node marker pair expression levels were generated and foreach new sample, a new decision rule was devised to split the region into two zones of equal prediction probability as described in Materials andMethods (total of 1,000 decision rules). The bootstrap estimates are the average prediction properties from classifying the original 41 lymph nodes1,000 times.
Clinical Cancer Research 1105
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

Correlation of QRT-PCR Analysis with Survival in pN0Patients. Three hundred and fourteen lymph nodes from
34 patients with pN0 esophageal adenocarcinoma were analyzed
by QRT-PCR for CK19 and TACSTD-1. Using the cutoff
generated in the secondary screen for the CK19/TACSTD-1
combination, six nodes from five patients were classified as
positive by QRT-PCR. Even with limited follow-up time, Kaplan-
Meier analysis showed that QRT-PCR-positive patients had a
significantly worse disease-free survival than QRT-PCR negative
patients (P = 0.0023, log-rank test; Fig. 3). Future analyses on
larger patient sets, and with more follow-up, are required to see if
this preliminary finding remains true in multivariate analyses.
DISCUSSION
The current tumor-node-metastasis staging system identifies
groups of cancer patients who are expected to have similar
outcome probabilities, thus allowing physicians to make
appropriate decisions regarding treatment options. Unfortunately,
within these stage groupings, the outcome for any individual
patient can still be very different from the overall prognosis of
the group. In esophageal cancer, the patients most affected by
such limitations of the current staging system are those with
localized, lymph node–negative tumors. Despite potentially
curative surgical resection, 30% to 40% of these patients will
suffer recurrence and succumb to their disease. In previous work,
we have shown that analysis of lymph nodes using QRT-PCR
can identify pathologically occult lymph node metastases and
that this correlates with disease recurrence (12). Extending this
work, the goal of our current study was to identify, screen, and
validate the best mRNA-based molecular markers for detection
of lymph node metastases in esophageal adenocarcinoma.
Marker Identification. CEA (CEACAM5) is a cell
adhesion molecule that is frequently found in adenocarcinomas
of endodermally derived digestive system epithelia. Historically,
CEA has been the marker of choice for identifying adenocar-
cinoma of the gastrointestinal tract and was among the first
markers to be used for RT-PCR analysis of lymph nodes.
TACSTD1, also known as EPCAM, EGP-2, KS1/4, GA-733-2,
and MIC-18 is a human cell surface antigen that is defined by the
monoclonal antibody AUAI. TACSTD1 is also the antigen for
the antibody Ber-Ep4 and, as such, has been used in several
studies to detect lymph node micrometastases in a variety of
tumor types (23, 35, 36). A recent study has also shown that
TACSTD1 is a good RT-PCR-based marker for identification of
lymph node micrometastases in non–small cell lung cancer (37).
CK19 is an acidic keratin that is expressed at high levels in
many epithelial tissues and their derived tumors. CK19 is one of
the keratins targeted by the AE1/AE3 antibody cocktail and, as
such, is frequently used by pathologists for immunohistochemical
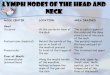
Fig. 2 Analysis of the 56 lymph nodes in the validation set and the 14 lymph nodes with discordant pathology. Top, data on five individual geneexpressions observed in benign, discordant, and positive nodes. The horizontal line indicates the most accurate cutoff value calculated from thesecondary screen and applied to this independent data set. Bottom, validation set data for the same two marker pair combinations illustrated in Fig. 1Band C (CK19/TACSTD1 and CEA/Villin 1). As with the individual markers, the diagonal black line indicates the decision rule generated from thesecondary screen data, applied to the validation set. Classification characteristics of the individual markers and all marker combinations are reported inSupplemental Table 2.
RT-PCR of Lymph Nodes from Patients with Esophageal Cancer1106
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

detection or confirmation of lymph node metastases in many
cancer types. CK19 has also been used in many RT-PCR-based
studies to detect occult lymph node disease in breast cancer
(35, 38, 39). Unfortunately, this gene has at least two pseudogenes
that make it difficult to develop a cDNA-specific assay. As a
result, the utility of this marker may be limited in clinical settings
given the potential for false-positive results. Cytokeratin 7 (CK7,
KRT7) is a type II keratin of simple, nonkeratinizing epithelia and
is typically found in tissues such as the epidermis, bronchus, and
mesothelium. As such, CK7 would not typically be considered as
a marker for esophageal adenocarcinoma. The last two markers,
CK20 and Villin 1, are generally associated with colonic
epithelium. Cytokeratin 20 (CK20, KRT20) is an integral,
intermediate filament component and is a major cytoskeletal
keratin of the intestinal epithelium. CK20 has been used
frequently in RT-PCR studies to detect occult metastases in colon
cancer patients but has not been used previously in esophageal
cancer. Villin 1 is a major structural component of the brush border
cytoskeleton. It is a calcium-regulated, actin-binding protein that
is specifically expressed in simple epithelia of some tissues of the
gastrointestinal and urogenital tracts. Because esophageal adeno-
carcinoma is thought to arise from an intestinal type, glandular
metaplasia of the normal squamous epithelium, the finding that
CK20 and Villin 1 are potentially useful markers for this disease is
novel but not surprising.
Lymph Node Classification. Data generated in the
screening and validation process indicate that TACSTD1 and
CK19 are the best individual markers for classification of positive
and benign lymph nodes in esophageal adenocarcinoma. Both
markers showed 100% classification accuracy in the secondary
screen, and internal validation resulted in estimated accuracies of
98% and 97%, respectively. Furthermore, when the cutoff values
from the secondary screen were applied to an independent
validation set of lymph nodes, these markers again showed 100%
classification. Indeed, the classification accuracy observed for all
markers in the validation study was very similar to that seen in the
secondary screen, indicating that robust and accurate classifica-
tion of lymph nodes by QRT-PCR is feasible. In our study,
however, the majority of positive lymph nodes examined
contained a large percentage of tumors (only seven nodes
contained < 5% tumor) and were easily identified by routine
pathology. Thus, the extremely high sensitivity and specificity
observed in our data may not be reflected upon analysis of node-
negative patients for the presence of micrometastatic disease.With
this in mind, and because it is highly unlikely that classification
accuracy with any individual marker will remain 100% when a
larger number of nodes are examined, we also analyzed
classification characteristics using combinations of marker pairs.
By combining individual markers we hoped to increase the
separation between positive and negative lymph node distribu-
tions and therefore obtain more reliable and sensitive lymph node
classifications. When combining markers with less than perfect
classification characteristics, we found that the combination
frequently improved the observed classification accuracy beyond
that of either individual marker alone. When comparing bootstrap
estimates of accuracy between individual markers and marker
combinations, the combinations were better than either individual
marker in all cases (average 2.5% improvement). Furthermore, the
bootstrap estimates of optimism in the individual markers ranged
from 2% to 5%, whereas on marker pairs, the optimism was only
0% to 2%. Finally, analysis of the independent, validation lymph
node set resulted in perfect classification for 7 of the 10 marker
combinations tested. These data indicate that combining the
classification characteristics of two markers is likely to result in
more robust lymph node classification, in particular when
examining nodes for micrometastatic disease.
Statistical Approach. In this study, the decision rules for
both single and double markers have been rigorously validated.
Internal validation consisted of parametric resampling of lymph
node expression data to simulate sampling variability. The
decision rules were further tested in an independent test set of
lymph nodes from patients at our institution. Thus, we are
confident of the reproducibility of classification at our institution
and in our laboratory. This process should be considered only the
first step in a series of more thorough efforts to generalize RT-
PCR-based methods of lymph node analysis. A continuum of
increasingly diverse settings needs to be introduced for full
evaluation of the generalizability of our ability to discriminate
and predict nodal status (40). These include obtaining lymph
nodes from patients at other institutions and evaluating QRT-PCR
in the hands of other pathologists and laboratory technicians.
Clinical Translation. The clinical utility of RT-PCR
staging of lymph nodes relies on the assumption that RT-PCR
will eventually prove superior to routine pathology, either by
detecting occult disease in pN0 patients or by providing an
objective analysis to help overcome the subjectivity and
discordance observed in current pathologic examination. Our
work lays the foundation for these studies because we have
identified appropriate markers and defined the classification
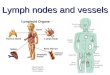
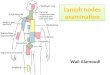
Fig. 3 Kaplan-Meier disease-free survival curves for 34 patients withpN0 esophageal adenocarcinoma. Patients were stratified into occultdisease-positive and occult disease-negative groups based on QRT-PCRdata for CK19 and TACSTD1 using the cutoff algorithms developed inthe marker screening phase. QRT-PCR-positive patients had a signifi-cantly worse disease-free survival than QRT-PCR-negative patients (P =0.0023, log-rank test). Note that patient 25 was censored at 17.9 monthsand patient 4 recurred at 18.0 months. Hence, the survival curve drops tozero despite one QRT-PCR-positive patient who did not suffer recurrencein this study.
Clinical Cancer Research 1107
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

criteria to be applied to lymph nodes from patients with
esophageal adenocarcinoma. The detection of occult lymph
node disease, and subsequent improved patient staging, could
have significant consequences for the treatment of esophageal
cancer. For example, although chemotherapy has failed to show
a proven benefit in any large, randomized, well-controlled study
(41, 42), there is now increasing interest in nonfluorouracil-
containing regimens that seem to be better tolerated by patients
(43). Specifically, an ongoing Eastern Cooperative Oncology
Group trial is investigating platinum-based regimens in combi-
nation with either irinotecan or paclitaxel. These therapies are
most likely to benefit patients with minimal residual disease,
such as patients with micrometastatic involvement of regional
lymph nodes. Furthermore, a major benefit of more accurate
staging may actually be in our ability to identify the low risk,
truly node-negative patients and spare them the potential
morbidity of unnecessary chemotherapy.
Surgical approach and extent of lymph node dissection may
also be determined by the lymph node status, with some surgeons
advocating extensive lymph node dissection in node-positive
patients. Furthermore, there is reasonably strong evidence that
patients with extensive lymph node involvement have a worse
prognosis (1, 7, 44) and that curative surgery may not be possible
in this group. These findings have led to a push for the revision of
the tumor-node-metastasis staging system in esophageal cancer to
include an N2 stage for patients with extensive lymph node
disease. Along these lines, identification of occult lymph node
metastases in patients determined to be N0 by routine histology
could help distinguish them from truly node-negative patients.
The former subgroup might possibly benefit from more extensive
nodal dissection, whereas the latter group may achieve curative
resection with less aggressive surgical resection. On the other
hand, among node-positive patients, the presence of occult nodal
disease could identify those patients with more extensive nodal
involvement (the proposed N2 patients) who might derive a better
quality of life from less invasive surgery and/or palliative or
systemic treatments rather than from a relatively morbid, and
ultimately unsuccessful, radical surgery. Thus, the detection of
occult lymph node metastasis could play an important role in
future staging and treatment options for pathologically node-
positive as well as node-negative patients.
ACKNOWLEDGMENTSWe thank Drs. Alyssa Krasinskas, Kenneth McCarty, Jr., and Susan
Silver for reviewing slides on discordant tissues.
REFERENCES1. Korst RJ, Rusch VW, Venkatraman E, et al. Proposed revision of thestaging classification for esophageal cancer. J Thorac Cardiovasc Surg1998;115:660–9.
2. Ando N, Ozawa S, Kitagawa Y, Shinozawa Y, Kitajima M.Improvement in the results of surgical treatment of advanced squamousesophageal carcinoma during 15 consecutive years. Ann Surg 2000;232:225–32.
3. Izbicki JR, Hosch SB, Pichlmeier U, et al. Prognostic value ofimmunohistochemically identifiable tumor cells in lymph nodes ofpatients with completely resected esophageal cancer. N Engl J Med 1997;337:1188–94.
4. Mueller JD, Stein HJ, Oyang T, et al. Frequency and clinical impact of
lymph node micrometastasis and tumor cell microinvolvement in patientswith adenocarcinoma of the esophagogastric junction. Cancer2000;89:1874–82.
5. Natsugoe S, Mueller J, Stein HJ, Feith M, Hofler H, Siewert JR.Micrometastasis and tumor cell microinvolvement of lymph nodesfrom esophageal squamous cell carcinoma: frequency, associatedtumor characteristics, and impact on prognosis. Cancer 1998;83:858–66.
6. Matsumoto M, Natsugoe S, Nakashima S, et al. Clinical significanceof lymph node micrometastasis of pN0 esophageal squamous cellcarcinoma. Cancer Lett 2000;153:189–97.
7. Bonavina L, Ferrero S, Midolo V, Buffa R, Cesana B, Peracchia A.Lymph node micrometastases in patients with adenocarcinoma of theesophagogastric junction. J Gastrointest Surg 1999;3:468–76.
8. Nakamura T, Ide H, Eguchi R, Hayashi K, Ota M, Takasaki K.Clinical implications of lymph node micrometastasis in patients withhistologically node-negative (pN0) esophageal carcinoma. J Surg Oncol2002;79:224–9.
9. Komukai S, Nishimaki T, Watanabe H, Ajioka Y, Suzuki T,Hatakeyama K. Significance of immunohistochemically demonstratedmicrometastases to lymph nodes in esophageal cancer with histologicallynegative nodes. Surgery 2000;127:40–6.
10. Vazquez-Sequeiros E, Wang L, Burgart L, et al. Occult lymph nodemetastases as a predictor of tumor relapse in patients with node-negativeesophageal carcinoma. Gastroenterology 2002;122:1815–21.
11. Kijima F, Natsugoe S, Takao S, et al. Detection and clinicalsignificance of lymph node micrometastasis determined by reversetranscription-polymerase chain reaction in patients with esophagealcarcinoma. Oncology 2000;58:38–44.
12. Godfrey TE, Raja S, Finkelstein SD, Gooding WE, Kelly LA,Luketich JD. Prognostic value of quantitative reverse transcription-polymerase chain reaction in lymph node-negative esophageal cancerpatients. Clin Cancer Res 2001;7:4041–8.
13. Kassis ES, Nguyen N, Shriver SP, Siegfried JM, Schauer PR,Luketich JD. Detection of occult lymph node metastases in esophagealcancer by minimally invasive staging combined with moleculardiagnostic techniques. JSLS 1998;2:331–6.
14. Luketich JD, Kassis ES, Shriver SP, et al. Detection of micro-metastases in histologically negative lymph nodes in esophageal cancer.Ann Thorac Surg 1998;66:1715–8.
15. Glickman JN, Torres C, Wang HH, et al. The prognostic significanceof lymph node micrometastasis in patients with esophageal carcinoma.Cancer 1999;85:769–78.
16. Cote RJ, Peterson HF, Chaiwun B, et al. Role of immunohisto-chemical detection of lymph-node metastases in management of breastcancer. International Breast Cancer Study Group. Lancet 1999;354:896–900.
17. Fisher ER, Swamidoss S, Lee CH, Rockette H, Redmond C,Fisher B. Detection and significance of occult axillary node metastases inpatients with invasive breast cancer. Cancer 1978;42:2025–31.
18. Jannink I, Fan M, Nagy S, Rayudu G, Dowlatshahi K. Serialsectioning of sentinel nodes in patients with breast cancer: a pilot study.Ann Surg Oncol 1998;5:310–4.
19. Isozaki H, Okajima K, Fujii K. Histological evaluation of lymphnode metastasis on serial sectioning in gastric cancer with radicallymphadenectomy. Hepatogastroenterology 1997;44:1133–6.
20. Chen ZL, Perez S, Holmes EC, et al. Frequency and distribution ofoccult micrometastases in lymph nodes of patients with non-small celllung carcinoma. J Natl Cancer Inst 1993;85:493–8.
21. Dobashi K, Sugio K, Osaki T, Oka T, Yasumoto K. Micro-metastatic P53-positive cells in the lymph nodes of non-small cell lungcancer: prognostic significance. J Thorac Cardiovasc Surg 1997;114:339–46.
22. Maruyama R, Sugio K, Mitsudomi T, Saitoh G, Ishida T,Sugimachi K. Relationship between early recurrence and micrometa-stases in the lymph nodes of patients with stage I non-small-cell lungcancer. J Thorac Cardiovasc Surg 1997;114:535–43.
RT-PCR of Lymph Nodes from Patients with Esophageal Cancer1108
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

23. Kubuschok B, Passlick B, Izbicki JR, Thetter O, Pantel K.Disseminated tumor cells in lymph nodes as a determinant for survivalin surgically resected non-small-cell lung cancer. J Clin Oncol 1999;17:19–24.
24. Osaki T, Oyama T, Gu CD, et al. Prognostic impact of micro-metastatic tumor cells in the lymph nodes and bone marrow of patientswith completely resected stage I non-small-cell lung cancer. J Clin Oncol2002;20:2930–6.
25. Gu CD, Osaki T, Oyama T, et al. Detection of micrometastatic tumorcells in pN0 lymph nodes of patients with completely resected nonsmallcell lung cancer: impact on recurrence and Survival. Ann Surg 2002;235:133–9.
26. Motomura K, Komoike Y, Inaji H, et al. Multiple sectioning andimmunohistochemical staining of sentinel nodes in patients with breastcancer. Br J Surg 2002;89:1032–4.
27. Wong SL, Chao C, Edwards MJ, Simpson D, McMasters KM. Theuse of cytokeratin staining in sentinel lymph node biopsy for breastcancer. Am J Surg 2001;182:330–4.
28. Veronesi U, Zurrida S, Mazzarol G, Viale G. Extensive frozensection examination of axillary sentinel nodes to determine selectiveaxillary dissection. World J Surg 2001;25:806–8.
29. Roberts CA, Beitsch PD, Litz CE, et al. Interpretive disparity amongpathologists in breast sentinel lymph node evaluation. Am J Surg 2003;186:324–9.
30. Godfrey TE, Kim S-H, Chavira M, et al. Quantitative mRNAexpression analysis from formalin-fixed, paraffin-embedded tissues using5V nuclease quantitative RT-PCR. J Mol Diagn 2000;2:84–91.
31. Tassone F, Hagerman RJ, Taylor AK, Gane LW, Godfrey TE,Hagerman PJ. Elevated Levels of FMR1 mRNA in Carrier Males: a newmechanism of involvement in the fragile-X syndrome. Am J Hum Genet2000;66:6–15.
32. Godfrey TE, Kely LA. Development of quantitative RT-PCR assaysfor measuring gene expression. In: Phouthone K, Grant SG, editors.Molecular Toxicology Protocols. Humana Press; 2004.
33. Morrison TB, Weis JJ, Wittwer CT. Quantification of low-copy
transcripts by continuous SYBR Green I monitoring during amplifica-tion. BioTechniques 1998;24:954–8, 960, 962.
34. Efron B, Tibshirani RJ. An introduction to the bootstrap. BocaRaton: Chapman & Hall/CRC; 1994.
35. Schroder CP, Ruiters MH, de Jong S, et al. Detection ofmicrometastatic breast cancer by means of real time quantitativeRT-PCR and immunostaining in perioperative blood samples andsentinel nodes. Int J Cancer 2003;106:611 – 8.
36. Takes RP, Baatenburg de Jong RJ, Wijffels K, et al. Expressionof genetic markers in lymph node metastases compared withtheir primary tumours in head and neck cancer. J Pathol 2001;194:298–302.
37. Mitas M, Cole DJ, Hoover L, et al. Real-time reverse transcription-PCR detects KS1/4 mRNA in mediastinal lymph nodes from patientswith non-small cell lung cancer. Clin Chem 2003;49:312–5.
38. Mitas M, Mikhitarian K, Walters C, et al. Quantitative real-time RT-PCR detection of breast cancer micrometastasis using a multigene markerpanel. Int J Cancer 2001;93:162–71.
39. Aerts J, Wynendaele W, Paridaens R, et al. A real-time quantitativereverse transcriptase polymerase chain reaction (RT-PCR) to detectbreast carcinoma cells in peripheral blood. Ann Oncol 2001;12:39–46.
40. Justice AC, Covinsky KE, Berlin JA. Assessing the generalizabilityof prognostic information. Ann Intern Med 1999;130:515–24.
41. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF. Rising incidence ofadenocarcinoma of the esophagus and gastric cardia. JAMA1991;265:1287–9.
42. Blot WJ, McLaughlin JK. The changing epidemiology of esophagealcancer. Semin Oncol 1999;26:2–8.
43. Anderson SE, Minsky BD, Bains M, Kelsen DP, Ilson DH.Combined modality therapy in esophageal cancer: the memorialexperience. Semin Surg Oncol 2003;21:228–32.
44. Lerut T, Coosemans W, Decker G, et al. Extracapsular lymph nodeinvolvement is a negative prognostic factor in T3 adenocarcinoma ofthe distal esophagus and gastroesophageal junction. J ThoracCardiovasc Surg 2003;126:1121–8.
Clinical Cancer Research 1109
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from

2005;11:1099-1109. Clin Cancer Res Liqiang Xi, James D. Luketich, Siva Raja, et al. Esophageal AdenocarcinomaMolecular Staging of Lymph Nodes from Patients with
Updated version
http://clincancerres.aacrjournals.org/content/11/3/1099
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/11/3/1099.full#ref-list-1
This article cites 42 articles, 4 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/11/3/1099.full#related-urls
This article has been cited by 5 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/11/3/1099To request permission to re-use all or part of this article, use this link
Cancer Research. on November 24, 2020. © 2005 American Association forclincancerres.aacrjournals.org Downloaded from