HIVCOUNSELOR
PERSPECTivESVolume 3 Number 4 August 1993Written and Produced by the UCSF AIDS Health Projectfor the California Department of Health Services, Office of AIDS
HIV TESTSWhen researchers were seeking a way to identify HIV infection in the early 1980s, they found the most effective test to be
one that detected the presence of antibodies to HIV The enzyme-linked immunosorbent assay (ELISA) was approved for usein 1985. Based on its cost-effectiveness and high rate of accuracy, the use of the ELISA, combined with a supplemental testwhen a blood sample is reactive, has remained the standard in HIV testing.1 Other tests for HIV antibody and antigen havebeen developed as demand for testing has increased and as quicker and more cost-effective testing methods have beensought.
This issue of PERSPECTIVES offers an overview and an update of conventional testing methods, and presents researchon new tests that detect HIV antibodies or antigen. The Implications for Counseling section explains how counselors candiscuss the roles of current tests and prospects for other tests.
Research UpdateWhen someone is infected with
HIV, the body responds by developing antibodies to the virus, usually within six to eight weeks afterinfection. For a few people, it maytake three to six months for thebody to produce antibodies. Usingconventional testing methods, aperson is considered positive forHIV infection if blood samples arereactive in each of a series of teststhat detect antibodies. When aninitial ELISA test is reactive, it isrepeated once or twice. If a repeattest is positive, it is followed with asupplemental test, either theWestern blot test or immunofluorescence assay (IFA).1
ELISAThe ELISA is considered the best
available screening because of its
low cost, standardization, high reliability, and relatively quick turnaround.2 Numerous versions ofthis test have been licensed by theFood and Drug Administrationsince 1985. The price of each ELISAtest kit can be less than $2. Addingequipment, labor and other overhead needed to conduct an ELISA,the total cost of each test rangesfrom $12 to $20. Costs of performing an ELISA vary based on several factors, including locale and thenumber of tests conducted.
In recent years, refinementshave been made to the ELISA toprevent cross-reactions to antibodies other than HIV and to preventother false results. Currently, mostversions of the ELISA use inactivated HIV viral proteins - or HIV
antigen - isolated from cell cultures. Advanced technology isbeing used to make synthetic HIVantigens that are even more sensitive and specific.3 In a recent studyof the ELISA's reliability and accu-
Inside This Issue
7 Research Update
3 Non-Blood Tests, HomeCollection
4 AIDS-Like Symptoms without HIV
5 Implications for Counseling
7 Case Study
8 Test Yourself
8 Using PERSPECTIVES

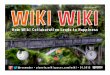
Estimated Costs of HIV Antibody Tests
responds to a test, human laboratory errors, or health conditions suchas hemophilia, autoimmune disorders, and alcohol-related hepatitis.5
Because false positive results canoccur, a supplemental test isalways necessary to conclude thatHIV antibodies are present and tomake a diagnosis of HIV infection.
Western Blot and IFAThe Western blot is the most
commonly used supplemental test.Compared to the ELISA, it is moreexpensive, takes a longer time toperform, requires greater technicalprecision, and is more difficult tointerpret. (i The total cost of performing a Western blot test isabout $40, which includes about$24 for each test kit. As a supplemental test, the overall sensitivityand specificity of the Western blotare considered to be high, at 99.3%and 91.6%, respectively, as analyzed recently by the Centers forDisease Control and Prevention(CDC).4
There has been some controversy regarding interpretation of theWestern blot and what are considered inconclusive readings. TheCDC has set specific guidelinesregarding the interpretation ofresults. Interpretation of Westernblot results involves reading several bands of reactivity that appearon a test strip. In order for a resultto be considered positive, reactivityto certain bands must occur. For a
Manufacturer'sprice of each test
Enzyme-linked ImmunosorbentAssay (ELISA)
Murex SUDS
Recombigen Latex Agglutination
Immunofluorescence Assay (lFA)
Western Blot
racy it was found to have a sensitivity of 99.7(70.4 Sensitivity refers tothe rate of false negative results: inthe case of the ELISA this meansthat 99.7% of test samples werecorrectly diagnosed as positivewhen antibodies were present, andthat 0.3% of test samples - or 3 in1,000 - were falsely diagnosed bythe ELISA as negative when HIVantibodies were actually present.The test's specificity was 98.5%.Specificity refers to the rate of falsepositive results: in the case of theELISA, this means that 98.5% ofnegative test samples were correctly diagnosed as negative, and that1.5% of the tests produced positiveresults when antibodies were notpresent.
Nonreactive results can occur insomeone with HIV infection whentesting is done before the body hasproduced antibodies to HIV - atime known as the "window period" - or when a person is late inthe course of AIDS, at which timethe body may stop producing antibodies. In addition, some ELISAsare specific only to antibodies toHIV-1, which is the primary strainof HIV infection found in theUnited States. Another virus, HIV2, is found in some African countries, but very rarely in the UnitedStates.
False positive screening results,on the rare occasions they occur,may result from biological variations in the way a blood sample
$2
$6-$9
$5
$76
$24
Total cost toperform test(includes price of test)
$72-$20
$7-$70
$75-$20
$25
$40
result to be negative, it is necessarythat no viral-specific bands showreactivity. In some cases, reactivitywill occur, but not to the specificbands required for a positive reading. This result is called "indeterminate" and the overall result iscalled inconclusive. It is possiblethat this occurrence could signifyearly HIV infection or an earlystage of seroconversion, or it couldindicate infection with HIV-2. 3
However, quite often when thesebands appear, HIV is not present?When a result is inconclusive, anew blood sample is needed fromthe client.8 This step is required byCalifornia law.
While the Western blot has beenthe most commonly used supplemental test in most parts of thecountry, the IFA is generally considered to be at least as reliable asthe Western blot, and it is morewidely used in public health testing in California. A commericalversion of the IFA received federalapproval to be marketed in 1992.For several years prior to this,California officials distributed a"homemade" version of the IFA tolocal labs.
The IFA is less expensive andeasier to perform than the Westernblot. The total cost to perform eachIFA is about $25, including $16 fortesting reagents. With an IFA, HIVantigens are fixed on a slide andincubated with the test sample.Another antibody is added thatreacts to the first complex.Fluorescent spots will appear onthe slide if HIV antibodies are present, indicating a positive result.
Using conventional testingmethods, results generally takefrom a week to as long as a monthto be reported to clients. Waits areoften greater in some rural areas,where test samples must often besent to a second lab for supplemental testing.
Rapid TestsThere are other methods either

now available or being developedto detect HIV infection. Recently,there has been increased focus onthese tests, particularly those thatcan be performed relatively quickly and easily outside a laboratory.9,lO In some cases, these tests arebeing considered as possible supplements or replacements to conventional testing methods.
With some rapid methods, testresults could be available the sameday blood is drawn, perhaps within an hour. 10,11 However, becausepositive results need to be confirmed with a more complex testlike the IFA or Western blot, bothof which require a laboratory,clients could not receive positive
results during the same visit.9
Currently, only two rapid testshave been licensed for use by theFDA. Other tests are being developed and may receive approvalduring the next several years. Forthe most part, all tests that havebeen approved or are awaitingapproval claim sensitivity andspecificity comparable to or greaterthan the ELISA.9,lO,11
The cost of most rapid tests issomewhat higher than for anELISA. The price of some rapidtests that have been approved isaround $5 each, and prices offuture tests are expected to be similar. However, unlike the ELISA, lit-
tIe equipment is required for somerapid tests. Rapid tests are nowbeing developed that do notrequire refrigeration or a reliableelectrical power source.
The following rapid tests havebeen approved for use:
Recombigen Latex AgglutinationTest. In 1988, the FDA approvedthe Recombigen HIV-1latex agglutination test, which can produce aresult within five minutes. This testis the first to use genetically engineered pieces of HIV antigen,which reduces cross-reactivity andnonreactivity that can cause falsepositive or false negative results. Alarge study found the sensitivity ofthe latex agglutination test to be
Related Issue: Non-Blood Tests, Home CollectionRapid HIV blood tests are just one area of devel
opment for HIV diagnostic tests. Other research isexploring tests of urine, saliva and mucous membrane samples to detect HIV. These procedures areless invasive than blood tests, and some health careworkers see these techniques as advantageousbecause they reduce the risk of infection from jobrelated needle sticks. These tests are also less costly,and they eliminate for clients the pain and inconvenience of providing blood samples.3
A recent study of a saliva test found specificityabove 99% and sensitivity at 96.2%, and a study offluid from nasal and gum mucosa showed a 99.8%sensitivity rate and a 99.5% specificity rate. 16
However, these techniques have not been studied asthoroughly as the ELISA test and therefore are considered relatively unproven.l7 There are also storageand handling concerns, including temperature andhumidity requirements, related to these testing techniques. It is unlikely that testing programs willswitch to saliva, urine, or mucous membrane testsuntil they are conclusively proven to be as accurateas what is already available.
Home-Collection TestsTesting methods by which someone can obtain a
sample in his or her own home are also being investigated, but these have not been approved for use,and it is not clear when they may be approved.Protocols for home-collection testing vary. A com-
monly proposed method is that a person would takea blood sample with a finger stick, then send thesample to a lab for analysis. Notification of resultswould be done by telephone, which would involvesome form of counseling, including referrals to localservice providers.9,17
Among the advantages of home-collection testingmethods cited by supporters are that the client cantest in private and maintain anonymity because thetest sample is identified only by code number; thecost of the test is lower than it would be if testingwere performed in a physician's office or clinic; andthere is no wait required before testing. Home-collection tests may be useful for people with little orno history of HIV infection risks because these people may have less need for risk assessment andhealth education counseling. Nearly 64% of peoplewho received services at Alternative Test Site CATS)programs in California during 1992 had little or noHIV risk behaviors. The seroprevalence rate for thisgroup was 0.3%.18 It is argued that home-collectiontests for these clients would preserve scarce publictesting funds for people at higher risk.
Despite these advantages, ethical and counselingconcerns are perhaps the biggest obstacles to theapproval of home-collection tests. 3 Opponents areconcerned that phone counseling may not offer thesupport people need to deal with a positive result,and that clients may receive little if any individualized risk assessment or risk-reduction education.9

99.4%, and the specificity, 99.6%.9However, a recent study of this testfound its sensitivity to be as low as92%.12 The latex agglutination testis not widely used because manybelieve it is not as simple to use orinterpret as the ELISA.9,12
Murex Suds. The Murex SUDStest, approved in 1992, has receivedwide attention. This test is manually performed and relatively easy tointerpret. While it takes as little as10 minutes to perform the test, thiscan occur only after an extendedperiod, perhaps up to one hour, toprepare test samples. Like therapid latex agglutination test, theMurex SUDS test uses a mixture oflatex particles coated with recombinant protein antigens. If antibodies are present in the blood, plasma, or serum being used, a blue
dot appears on a hand-held, disposable testing unit. If a result isnegative, no color will appear onthe test unit.
If a blue dot appears, the test isrepeated in duplicate. If repeatedly positive, a supplemental test isperformed to verify the result. TheMurex test includes several safeguards, such as a negative controlarea that remains white whenchemicals used to perform the testare properly administered. Inaddition, control samples areused. Murex company researchersclaim the test has a 99.9% sensitivity rate and a 99.9% specificityrate. ll The sensitivity rate is basedon tests of 839 specimens frompeople with AIDS, with one person falsely testing negative. Thespecificity rate is based on randomtests of 5,169 blood donor sam-
pIes. Of those tested, 18 falselytested positive. ELISA tests of thesame samples did not produce anyfalse results.11
Detecting HIV DirectlyWhile tests discussed above
detect infection based on the presence of antibodies - an indirectmethod - other tests detect thevirus directly. These methods maybe helpful at very early stages ofinfection in some situations when aWestern Blot result is indeterminate. For instance, there are someELISA-based tests that use HIVantibodies to detect HIV antigens,such as p24. This method producesvery few false positive results.However, the incidence of falsenegative results tends to be high,especially in HIV-infected peoplewho are asymptomatic.13
Related Issue: AIDS-Like Symptoms without HIVIn 1992, a variety of reports within the medical
community and media suggested that scientists haddetected an AIDS-like condition that occurred in theabsence of HIV infection. These reports raised concern about the usefulness of HIV testing.
The issue first gained broad attention when aresearcher at the University of California at Irvinereleased a report suggesting that a virus known asthe "human intracisternal virus" had caused anAIDS-like disease in an older woman.19 The releaseof this report coincided with last year's InternationalConference on AIDS. In an emergency session atthis conference, researchers discussed cases fromaround the world of severe immunosuppressionwithout HIY. These cases included five people inNew York and others identified by the Centers forDisease Control and Prevention (CDC). The CDCcalled for a more formal meeting later in 1992 thatresulted in the CDC's formal characterization of thisform of immunosuppression in the absence of HIVinfection as idiopathic CD4+ T-Iymphocytopenia, orICL.
Based on the CDC's characterization, a diagnosisof ICL is made when a person has repeated T-helpercell counts below 300, or fewer than 20% of all Tcells; tests negative for HIV infection; and has no
other apparent cause for immune deficiency.20Reports of a non-HIV, AIDS-like condition
some type of acquired immunodeficiency - haveappeared in medical literature at least since 1983.Characteristics of people with ICL are varied: theyrange from age 18 to 70, they are heterosexual andhomosexual, and they are of various ethnic origins.1R People with ICL most often have been whiteand female. More than half have reported no riskfactors for HIV infection.
The CDC has found about 60 possible cases ofICL in the United States. The number of deaths inthe group as a whole is low; only one of 30 investigated cases had died, and this death was not attributed to ICL. In a report following the CDC's meeting, researchers found no common pattern ofbehavioral risk among these cases, and no convincing evidence of a transmissible virus as the cause ofICL.19,20
Once research established ICL as distinct fromAIDS, less attention has been paid to it. This is likelybecause so few people are afflicted with ICL20 andthose with ICL, despite T-helper cell depletion, showrelatively stable T-helper cell counts over time. 21
Furthermore, unlike HIV, it does not appear that ICLcan be transmitted through the blood supply.

In addition, the polymerasechain reaction (PCR) can detecttiny amounts of specific HIV DNA.This test produces high rates offalse positive results and is usedmainly for research. [For moreinformation on the PCR test, referto the "Silent I:riJection" issue ofPERSPECTIVES, Vol. I, No.2; June1991.]
Future Testing ProtocolsSome researchers speculate that
with continued development ofrapid tests and continued improvements in ELISA tests, the Westernblot or IFA may be replaced in thetesting protocol by a three-testseries consisting of multiple ELISAtests, along with rapid and "simple" tests. Simple tests are similar
to rapid tests in that they do notneed sophisticated equipment, yetthey take longer than rapid tests toperform. The World HealthOrganization (WHO) cites researchthat has found combinations ofELISA, rapid and simple tests provide results at least as reliable asthe ELISA and Western blot combination and at a much lower COSt.14
Implications for CounselingIt has always been necessary for
counselors to assure clients aboutthe accuracy of HIV testing. Thedevelopment of improved versions of existing tests, such as theELISA, as well as entirely newtests and testing methods, hasallowed counselors to provideeven greater assurance and detailabout the scientific merit of testingprocedures.
ReliabilityMake sure clients understand
that HIV testing is accurate. Onrare occasions when asked forgreater detail, it may be useful toexplain the sensitivity and specificity of the test, and the meaningof these terms. Even after hearingthis, some clients may still questionthe reliability of common testingmethods. Assist these clients intwo ways: explain the testingoptions that are available, andexplore the reasons - and the feelings surrounding these - that theclient may have for distrusting thetest.
If asked about options, explainthat other tests, for instance thepolymerase chain reaction (PCR)or p24 antigen tests, can detecteither virus or viral particles, butthat these tests have significantlimitations. If the PCR test is discussed, explain that this test isconsidered a research tool and canproduce high rates of false positiveresults. If the p24 antigen test is
discussed, explain that this test haslittle use as an HIV test except atvery early stages of infection. Ifappropriate and available, offerreferrals to clients who ask forthem.
Clients who raise questionsabout the accuracy of existing testing methods, and are not satisfiedwith answers they receive, may
A Counselor's Perspective
"It's great to know thatrapid tests are promising,and could benefit the testing process. But, I need toremember that rapid tests
do not take away from theneed for thorough riskassessment and basic
health education."
not be satisfied with any test.There may be a variety of reasonsfor this attitude. For instance,these people may have recentlyengaged in unsafe sex with anHIV- infected partner and may beconvinced they too are infected;they may have peers with HIVand cannot imagine how theycould escape infection; or they
may be unable to accept any information unless it is absolute. Lesscommonly, a client may also sufferfrom a chronic mental illness andhold the delusion that he or she isinfected with HIV or has AIDSdespite laboratory evidence to thecontrary.
Explore the client's reasons fortesting and his or her reasons fordistrust. Continue to explore theclient's discomfort as long asprogress is being made. If itappears the client is unable toprogress in this discussion, it maybe appropriate to review with theclient the exchange that has takenplace and the client's response, andthen refer the client for additionalcounseling.
Waiting for ResultsIn most settings, clients receive
test results two weeks after testing.Waits such as this are often viewedas a useful time that allows clientsto understand the consequences ofthe test, respond to informationpresented in pre-test counseling,and prepare for a result. The period may also allow a person time toconsider the seriousness of his orher risk behaviors and makebehavioral changes.
Some counselors see the waiting period as too long and asharmful to the client. They arguethat the prolonged period ofuncertainty makes the testingprocess appear mystical, leads to

undue anxiety, and gives theclient little control while awaitingthese momentous results. Someclients report experiencing thewait as agonizing.
Be familiar with the protocol ofthe testing process from the timeblood is drawn until results aredisclosed, and explain this to theclient. Explain that results cannotbe reported immediately becausea series of tests must be conducted, and acknowledge that thelength of the process may be difficult for clients. Acknowledge andempathize with clients' frustratiems. For clients who display anxiety about managing their liveswhile awaiting their results, discuss techniques to reduce stressand gain support during this period. [See the Case Study on page 7to learn more about these techniques.]
When clients express an urgentneed to obtain test results, learn
A Counselor's Perspective
//Some clients don't
want to believe they are
unin fected. No test and
nothing that I say will con-
vince them. Discussions
with these clients can be
frustrating and anxiety
provoking for me, and I
know to avoid power
struggles. Instead, I
explore, as rm able, the
source of the client's con
cern, and then make the
best follow-up referral
that I can.//
more about the source of theurgency. It may be that the clientrecently engaged in unsafe behavior. If this is the case, explain thepossible need to return for a follOw-up test because he or shemay be in the infection "windowperiod," the time during whichHIV antibodies have not yetdeveloped in someone who isinfected.
Clients may express a need toreceive a result quickly based onthe belief that it is necessary toimmediately begin drug treatment.If the client has not had symptomsof disease, explain that it is highlyunlikely a two-week wait will havea detrimental effect on health. Ifthe client has symptoms of disease,discuss these and recommendmedical care.
When clients clearly expressthat they are unwilling to wait forresults and wish to test elsewhereto avoid the conventional waitingperiod, provide referrals for testing options. In most parts ofCalifornia, physicians provide testresults in as few as two or threedays. In some places, turnaroundcan be as short as one day. Explainthat when clients test through aphysician or elsewhere they maycompromise confidentiality oranonymity, and they will mostlikely pay a fee. Explain the significance of these effects, andadvise clients that some providersoffer testing with little, if any,counseling.
Rapid TestsWhile some people hope that
rapid tests, such as the MurexSUDS, can be used in mainstreamclinical settings to save money andtherefore allow for more intensivecounseling, there are several drawbacks to these tests. For instance,state law requires supplementaltesting - which is not rapid before a positive result is disclosed. In addition, the Murex testrequires refrigeration and equip-
A Counselor's Perspective
"I'd like to see testing
methods that are quicker
and more cost-effective.
But, I need to know that
any new methods are as
effective as current meth
ods and that they do not in
any way jeopardize the
counseling process. //
ment not commonly found at mosttest sites. Rapid tests also requiretraining for those performing thetests.
The likely discrepancy betweendisclosure procedures for negativeresults and positive results hasprompted resistance to the use ofrapid tests. One concern is relatedto fears that the method of delivering rapid test results inadvertantlyidentifies those who are infected.Because a person who tests negative to a rapid test would need tovisit the test site only once, it couldbe inferred that those who are notimmediately given results areinconclusive or positive. Becauseof this, it is not advisable to establish post-test negative counselingin a distinguishably different contextfrom post-test positive counseling.
Despite these limitations, someareas - for instance where fewpeople are being tested and HIVseroprevalence is low - couldbenefit from a rapid test. It is useful for counselors to consider thepossibilities for rapid tests becausefuture development of a rapid supplemental test or the use of a seriesof rapid or ELISA tests in place ofWestern blot or IFA testing maymake these alternatives moreviable.

Case StudyMark, who is 35, says during pre-test counseling that waiting two weeks for results will cause him too much anxiety. He
wants the test counselor to either produce a result in a shorter period or refer him to someone who can. Mark tested oncebefore in 1988. His history of risk is unclear, but it appears he has had unsafe sex several times in the past two years.
Acknowledge Mark's request for a test settingwith a more rapid turnaround of results, and validate the difficulty some people have in waiting. IfMark states that he cannot tolerate waiting and isclear he wants to test elsewhere, refer him to physicians or others who can provide results in a shorterperiod. If the current setting provides an option forquicker turnaround of results, offer this. Explainthe value of the anonymity or confidentiality offeredin the current setting as well as dangers of a testresult appearing on a person's medical record.
If Mark chooses to test in the current setting,learn more about how he perceives the wait periodand why this period is particularly difficult. Explorestrategies that could help him alleviate his anxietyand make the wait more acceptable.
Explain telephone support services, such as AIDShotlines and crisis support lines, and offer referrals.Discuss the social support available in Mark's life,to determine if this is a resource for him. Learn howMark has dealt with stressful events before. If these
coping skills have been healthy, explore how hemight use them now. Explain and offer writteninformation about stress-management techniquesand dealing with the waiting period. Emphasizehow Mark may benefit from avoiding stressful situations. Recommend that he avoid alcohol and otherdrugs during the period because they may elevateanxiety.
Perform a more thorough assessment of riskbehaviors Mark has engaged in over the last twoyears, especially those of recent months. His anxietyabout the wait may be directly related to his perceived risk for being infected. If Mark is able tounderstand the relationship of his anxiety to hisunsafe sex, he may be more motivated to avoidunsafe sex in the future. To help him avoid unsafesex and anxiety, Mark may benefit from risk-reduction counseling or group support sessions. While hemay not be able to receive this support before learninghis result, taking steps to seek it may relieve someanxiety.
References1. Centers for Disease Control: Public HealthService guidelines for counseling and antibody testing to prevent HIV infection andAIDS. MMWK 1987; 36: 5D93.
2. Schwartz JS, Kinosian BP, Pierskalla WI',et al. Strategies for screening human immunodeficiency virus antibody. JOl/l'1lal of theAmerican Medical Association. 1988; 259: 2574.
3. Sloand EM, Pitt E, Chiarello RJ, et al. HIVtesting. state of the art. JOl/rnal of theAmerican Medical Association. 1991; 266: 2D.
4. Centers for Disease Control. Update: serological testing for HIV-l antibody. MMWR.1990; 39(22): 38D-383.
5. Bylund OJ, Ziegner UH, Hopper DG.Review of Testing for Human Immunodeficiency Virus. Clinic in LaboratoryMedicine. 1992; 12(2): 305-333.
6. O'Gorman MR, Weber 0, Landis SE, et al.Interpretive criteria of Western Blot assay forserodiagnosis of human immunodeficiencyvirus type 1 infection. Archives of PathologicalLaboratory Medici1ze. 1991; 115: 26.
7. Jackson JB, MacDonald KL, Caldwell J, etal. Absence of HIV infection in blood donors
with indeterminate Western Blot tests forantibody to HIV-1. New England Joul'1lal ofMedicine. 1990; 322: 217.
8. Center for Disease Control. Interpretationand use of Western blot assay for serodiagnoses of human immunodeficiency virustypel infection. Morbidity and MortalityWeekly Report. 1989; 38(Suppl. 7): 1-7.
9. Kelly EB. The Search for a rapid HIV test.AIDS Patient Care. February 1990: 25-28.
10. Malone JD, Smith ES, Sheffiel F, et al.Comparative evaluation of six rapid serological tests for HIV-1 antibody. Journal ofAcql/ired Immune Deficiency Syndrome. 1993.6(2): 115-119.
11. Murex SUDS HIV-1 Test. Product labeling, package insert. 1992.
12. Riggin CH, Chenet-Monte C. I !IV testingby Latex Agglutination. Clinical MicrobiologyNewsletter. 1990; 12: 35.
13. Gauthier DK, Turner J. Anti-HIV antibodytesting: procedures and precautions. AmericanJOl/mal of Infection Control. 1989; 17: 14.
14. Tamashiro II, Maskill W, Emmanuel J, etal. Reducing the cost of HIV antibody testing. Lancet. 1993; 342: 87-9D.
15. Fitchen JH. Efficacy of OraSure fluid forH1V-1 antibody screening. Presentation at theNew York Academy of Science meeting,"Saliva as a Diagnostic Fluid." Oct. 22-25, 1992.
16. Hunt RJ, Connel J, Christofinis G, et al.The testing of saliva samples for HIV-1 antibodies: reliability in a non-clinic setting.Genitol/rinary Medicine. 1993; 69(1): 29-30.
17. Helig S. Controversy surrounds hometests for the AlDS virus. California Physician.June 1990: 30-33.
18. Department of Health Services, Office ofAIDS, HIV Testing Unit. Califomia HIVTesting and Counseling Annual Report,January-December 1992. Sacramento:Department of Health Services, 1993.
19. Fauci AS. CD4+ T-Iymphocytopeniawithout HIV infection- no lights, no camera,just facts. New England Journal of Medicine1993; 328: 429-43D.
20. World Health Organization. PressRelease, September 29,1993.
21. Duncan RA, Fordham von Reyn C, et al.Idiopathic CD4+ T-Iymphocytopenia- fourpatients with opportunistic infections and noevidence of HIV infection. New EnglandJOlll'1lal of Medicine 1993; 328: 393-398.

Test Yourself on HIV TestsTest Yourself on HIV Tests:
1. True or False: The ELISA testused in 1993 is no different fromthe ELISA first approved in 1985.
2. True or False: A positive ELISAtest alone is sufficient to determineHIV infection.
3. True or False: The occurrence ofa condition known as IeL, whichdepletes T-helper cell counts in theabsence of HIV and symptoms ofillness, has proven to be very rare,to have no link to HIV, and not tobe a new, transmissible virus.
4. True or False: A test's sensitivityrefers to the rate of test samplescorrectly diagnosed as positivewhen antibodies are present, and itindicates the rate of false negativeresults that are produced.
5. What is the sensitivity of theELISA test? a) 50%, b) 100%, c)99.7%, d) 20%.
6. True or False: It is widelybelieved that rapid tests will soonmake all other tests obsolete.
7. True or False: There are few, if
any drawbacks to home HIV testing.
8. Rapid tests may have restrictedusefulness for which of the following reasons? a) they require a nonrapid confirmatory test when aresult is positive, b) test sites maynot have appropriate facilities toperform a test, c) their results arehighly suspect, d) a and b are correct.
Discussion Questions
1. How can counselors discuss thereliability and accuracy of testssuch as the ELISA in simple termsand in ways that do not confusethe client?
2. How can counselors validatethe effectiveness of the ELISA andother tests with clients who statethat tests are imperfect and therefore their results invalid?
3. How can counselors deal withtheir personal frustrations relatedto the delay between the time a testis performed until results arereported?
4. What implications, if any, do
rapid tests have on the counselingand testing process currently, andwhat implications might such testshave in the future?
Answers to Test Yourself1. False. Versions of the ELISA have beenimproved continually since 1985.
2. False. A positive ELISA test must be validated by a Western Blot or other supplementaltest.
3. True.
4. True.
5. C. The ELISA has a sensitivity of 99.7%.
6. False. It is generally believed that rapidtests may be useful in some settings, but forthe foreseeable future, their usefulness is limited.
7. False. There are significant drawbacks tohome HIV testing, including their reliabilityand accuracy, and concerns related to counseling.
8. D. Both a and b are correct.
Reader ResponsePERSPECTIVES encourages counselors torespond to discussion questions presented ineach issue. Replies may help in planningfuture issues. Share your thoughts related tothe questions by writing: Editor, HIVCounselor PERSPECTIVES, UCSF AIDSHealth Project, Box 0884, San Francisco, CA94143.
Volume 3 Number 4 August 1993Using PERSPECTIVES
PERSPECTIVES is aneasy-to-read educationalresource for HIY testcounselors and otherhealth professionals.
Each issue explores a single topic. A ResearchUpdate reviews recentresearch related to thetopic. Implications forCounseling applies theresearch to the counseling session. Also included are a Case Study, andtwo sets of questions Forreview and discussion.
HIV Counselor PERSPECTIVES
Writer and Editor: John TigheWriter and Researcher: Peter ChiraClinical Consultants: JD Benson, MFCC; Marcia
Quackenbush, MFCC; Jaklyn Brookman, MFCCProduction: Leslie SamuelsAdministrative Support: Roger Scroggs
PERSPECTIVES is an educational publication of the CaliforniaDepartment of Health Services, Office of AIDS, written and produced by the AIDS Health Project of the Universily of CaliforniaSon Francisco. Reprint permission is granted, provided acknowledgment is given to the Deportment of Health Services.
PERSPECTIVES is based largely on input from antibody test counselors and other health professionals. Among those who had asignificant influence on this issue: Nikki Baumrind, Brian Louie,Mike Ascher and Barbara Adler.
AiDSHEALTHPROJECT
Director: James W. Dilley, MDPublications Manager: Robert MarksDesigner: Soul Rosenfield
DE!partment of Health Services,Ottice of AIDS, P. O. Box 942732,Sacramento, CA 94234, (916)445-0553.UCSF AIDS Health Project, Box 0884,San Francisco, CA 94143-0884,{415l476-6430.
Printed on recycled paper.
Recommended