Embed Size (px)
Citation preview

Pediatr Blood Cancer 2006;46:465–471
Wilms Tumour Experience in a South African Centre
Alan Davidson, MBChB, FCP Paed,1* Patricia Hartley, MBChB, FCP Paed,1 Farieda Desai, MBChB, FCP Paed,1
John Daubenton, MD, FCP Paed,1 Heinz Rode, MBChB, MMed, FCS, FRCS,2
and Alastair Millar, MBChB, FRCS, FRACS2
INTRODUCTION
There are few reported series of Wilms tumour from
Africa. Hadley et al. [1] reported on 78 black South African
children from KwaZulu-Natal with Wilms tumour. They
noted a high proportion of advanced local and metastatic
disease (53%were stages III and IV) aswell as generally poor
outcomes. In addition, treatment was compromised by a high
incidence of nutritional and infective co-morbidity. Of the 78
children, 8 declined treatment or absconded and 16 died
during or prior to pre-operative chemotherapy. Only 54
(69%) came to nephrectomy, 31 primarily and 23 after
chemotherapy with or without radiotherapy. Long-term
survival of this group was not reported. Zaghloul et al. [2]
more recently confirmed a high proportion of advanced
disease (51% were stages III and IV) in a series of 112
children in Egypt, but reported good results for non-
metastatic tumours (10 year actuarial survival of 94% for
stage I, 86% for stage II and 71% for stage III). We have
utilised primary surgery followed by chemotherapy in a
South African setting for many years and this study presents
our results.
METHODS
The study was a retrospective analysis of all patients
diagnosed with unilateral Wilms tumour at Red Cross
Children’s Hospital between January 1979 and December
2003. Twenty patients who presented with bilateral Wilms
tumour and 11 who presented with clear cell sarcoma of the
kidney were excluded from analysis. Details of presentation,
histology and management were extracted from patient
records.
Red Cross Children’s Hospital is an academic referral
hospital attached to the University of Cape Town. The
oncology unit treats children from the Eastern and Western
Cape provinces, a combined area of almost 300,000 sq. km
with a population of 10.9 million [3]. About half the patients
come from outside the greater Cape Town area, many from
under-resourced rural areas. The Western Cape, and in
particular the greater Cape Town area (population 3.1
million), has undergone considerable change in its demo-
graphy in recent years. Recent census figures show that
around 54% of the population is mixed race and about 20%
white, with an increasing number of black residents—
currently 26% [3]. There is considerable poverty—33% of
households live at or below the poverty line of $300 month
[4].
The hospital is state-funded, and fees are based on
parental income, with most families paying only nominal
sums, and a few with sufficient income or medical insurance
paying on a fee for service basis—15% of the Wilms tumour
patients in this series had medical insurance.
The oncology unit is staffed by three full time consultants,
and has a reliable supply of all necessary chemotherapeutic
agents and access to appropriate supportive care in the form
of a paediatric intensive care unit, safe blood products and
modern broad-spectrum antibiotics. Surgery is performed by
a small team of highly experienced surgeons, and radio-
therapy is administered by qualified radiation oncologists.
Background. In Africa, Wilms tumour frequently presents withadvanced disease. This study reports our results over 25 years using theNational Wilms Tumour Study Group (NWTSG) approach of primarysurgery followed by chemotherapy. Procedure. A retrospectiveanalysis was performed on all patients diagnosed with unilateralWilms tumour between January 1979 and December 2003. Results.The records of 188 childrenwith newly diagnosedWilms tumour wereexamined. Of these 57 (30.3%) were stage I, 33 (17.6%) were stage II,60 (31.9%) were stage III and 38 (20.2%) were stage IV. Twenty-fourpatients (12.8%) had unfavourable histology (UFH). The estimated 5-year overall survival (OS) for the whole group was 80.5% (84.8% for
favourable histology (FH) and 51.6% for UFH). Among those with FH,estimated 5-year OS was 94.4% for stage I, 96.2% for stage II, 84.9%for stage III and 54.2% for stage IV. There was no difference in OSbetween those FH stage III tumours that were operable and thosedeemed inoperable. Intra-operative spillage was uncommon (8%),and did not increase local relapse rate. Conclusions. National WilmsTumour Study Group protocols employed in an African setting withhighly competent and experienced surgical care, produced results fornon-metastatic FHWilms tumour comparable to those of the NWTSG.Pediatr Blood Cancer 2006;46:465–471. � 2005 Wiley-Liss, Inc.
Key words: chemotherapy; histology; stage; surgery; Wilms tumour
� 2005 Wiley-Liss, Inc.DOI 10.1002/pbc.20388
——————1Haematology-Oncology Service, Red Cross Children’s Hospital,
School of Child and Adolescent Health, University of Cape Town,
Cape Town, South Africa; 2Department of Paediatric Surgery, Red
Cross Children’s Hospital, School of Child and Adolescent Health,
University of Cape Town, Cape Town, South Africa
*Correspondence to: Alan Davidson, Ward G1, Red Cross Children’s
War Memorial Hospital, Private Bag Rondebosch, Cape Town 7700,
South Africa. E-mail: [email protected]
Received 7 June 2004; Accepted 24 January 2005

Standard practice throughout this period was that patients
were assessed at diagnosis and primary surgery was under-
taken where possible. All patients were staged radio-
graphically with chest X-ray and ultrasound abdomen, and
since 1986, computed tomography of the abdomen and chest.
For tumours deemed inoperable, pre-operative chemother-
apy was given after fine needle aspiration biopsy. These
tumours were regarded as stage III.
Chemotherapy protocols changed over time with treat-
ment duration varying from 15 months initially to 18 weeks
(all stage I and favourable histology (FH) stage II) and
24 weeks (all other stages) currently. All patients received
vincristine and actinomycin. Patients with stage III and IV
tumours also received doxorubicin—300 mg/m2 until 1998,
and 5 mg/kg (equivalent to 150 mg/m2) since 1999. Before
1989, stages I–IV received 20 Gray renal bed irradiation.
Subsequently, only those with local stage III received renal
bed irradiation (currently 1,080 cGray in six fractions), and
those with pulmonary metastases received pulmonary
irradiation (currently 1,200 cGray in eight fractions).
From the outset, all patients with unfavourable histology
(UFH) received vincristine, actinomycin, doxorubicin
(300 mg/m2) and cyclophosphamide. Stage I patients with
UFH were excluded from this in 1989 and now receive only
vincristine and actinomycin. Since 1999, stage II–IV
tumours with diffuse anaplastic histology have been treated
with vincristine, actinomycin, doxorubicin (7.5 mg/kg
equivalent to 225 mg/m2), cyclophosphamide and etoposide.
Stage II–IV tumours with focal anaplasia have been treated
with vincristine, actinomycin and doxorubicin (5 mg/kg
equivalent to 150 mg/m2).
Relapse was treated with surgery, local and pulmonary
radiotherapy (depending on site), as well as a variety of
chemotherapeutic regimes including vincristine, actinomy-
cin, doxorubicin, cyclophosphamide, ifosfamide, etoposide
and carboplatin. Relapse-free survival (RFS) and overall
survival (OS) were estimated by the method of Kaplan and
Meier. Survival analysis was performed using Statistica 6.1
(Statsoft, Inc. 1984–2003).
RESULTS
Patient Characteristics
One hundred eighty-eight children were diagnosed with
Wilms tumour during the 25-year study period. There were
77 males and 111 females representing a male: female ratio
of 2:3. Age at diagnosis ranged from 0.24 to 12.87 years. The
median age at presentation was 39.2 months. There were 24
white patients (12.8%), 85 mixed-race patients (45.2%) and
79 black patients (42%).
Most presented with an abdominal mass or distension
(77%). Abdominal pain occurred in 48 patients (25.5%) and
macroscopic haematuria in 18 (9.6%). Thirty-two patients
(17%) were hypertensive at diagnosis and two of these
presented in cardiac failure.Weight was below the 3rd centile
of weight for age in 39 patients (20.7%). Therewere only two
cases of renal failure; onewith creatinine>2.5mg/dl and one
with a massive tumour, raised urea and normal creatinine,
and oliguria (urine output <0.5 ml/kg/hr).
Thirteen patients had associated abnormalities. These
included five with urogenital abnormalities, four with
hemihypertrophy, three with aniridia and one with Beck-
with–Wiedemann syndrome. One patient with no associated
physical abnormalities, whose sibling had a Wilms tumour
and renal dysplasia, was found to have a deletion of
chromosome 11. There were four patients with unrelated
syndromes (alagille syndrome, moebius syndrome, chron-
drodysplasia punctata and ectodermal dysplasia).
Fifty-seven childrenwere stage I (30.3%), 33were stage II
(17.6%), 60 were stage III (31.9%) and 38 were stage IV
(20.2%). Stage IV disease constituted 8.3% of the tumours
among white patients, 17.6% of the tumours among mixed-
race patients and 26.6% of the tumours among black patients.
Of those with metastatic disease, 34 (89.4%) had lung
metastases. Six of these 34 patients also had liver metastases,
and three others had isolated liver metastases. One had
central nervous systemmetastases. Inferior vena cava tumour
thrombus was present at diagnosis in 11 cases (5.9%), five
with extension into the right atrium. Characteristics of the
study population are shown in Table I, and those of the stage
IV patients are shown in Table II.
Of the 137 tumours operable at diagnosis, 118 were
weighed. Seventy-five (63.6%)weighedmore than 550 g and
of these, 24 (20.3%) weighed more than 1 kg. In order to
make comparison with NWTS-3, 79 (66.9%) had tumours
larger than 500 g. Of the 28 operable stage III tumours that
were weighed, 23 (82.1%) exceeded 550 g and of these, 10
(35.7%) were more than 1 kg.
There were 24 patients (12.8%) with UFH. Thirteen
(6.9%) had diffuse anaplasia and 11 had focal anaplasia.
Fifty-fivepercent of the patientswith focal anaplasia and23%
of those with diffuse anaplasia had stage IV disease. UFH
was seen in 29.2% of white patients, 8.2% of mixed-race
patients and 12.7% of black patients. Twenty-four patients
(12.8%) had nephroblastomatosis. Rhabdomyomatous ele-
ments were noted in the histology of 20 cases (10.6%).
Patient Outcomes
Length of follow-up varied from 4.1 to 303.8 months with
amean of 117.5months. Of the 142 patients that are alive and
disease free, 106 are now more than 5 years from diagnosis.
Eight were lost to follow-up less than 5 years from diagnosis.
Thirty-eight patients have died, 34 as a result of disease,
2 due to treatment-related complications (anthracycline-
induced cardiomyopathy and undiagnosed intestinal obstruc-
tion) and 2 from infection (gastroenteritis and adenoviral
pneumonia).
Estimated 5-year OS for the whole group was 80.5%,
84.8% for FH tumours and 51.6% for UFH tumours.
Pediatr Blood Cancer DOI 10.1002/pbc
466 Davidson et al.

Estimated 5-year RFS for thewhole groupwas 74.8%, 78.9%
for FH tumours and 47.1% for UFH tumours.
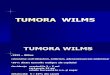
Estimated 5-year OS for FH tumours by stage was 94.4%
for stage I, 96.2% for stage II, 84.9% for stage III and 54.2%
for stage IV. Kaplan–Meier curves are shown in Figure 1.
When stage IV FH patients were analysed in cohorts, the
estimated 5-yearOS for 1984–1993was 62.9%, compared to
49% for 1994–2003 (log-rank P value¼ 0.43). The esti-
mated 5-year RFS by stage for FH tumours was 86.3% for
stage I, 84.7% for stage II, 83.6% for stage III and 51.6% for
stage V.
In the group of patients with FH stage III tumours, the
estimated 5-year OS was 84.9% for those that had primary
surgery, compared to 84.4% for those that were deemed
inoperable and had pre-operative chemotherapy (log-rank P
value¼ 0.83).
Three of the 11 patients with inferior vena cava tumour
thrombus had primary surgery. Eight were deemed inoper-
able and received chemotherapy initially. Two patients, one
from each group, died early as a result of thromboembolus
and vascular decompensation. Successful surgery was
carried out in nine cases, three of these on cardiopulmonary
TABLE I. Patient Characteristics and Outcome by Stage
Total Stage I Stage II Stage III Stage IV
Patients (%) 188 57 (30.3) 33 (17.6) 60 (31.9) 38 (20.2)
Black (% of total) 79 17 (21.5) 10 (12.7) 31 (39.2) 21 (26.6)
Mixed-race (% of total) 85 32 (37.6) 15 (17.6) 23 (27.1) 15 (17.6)
White (% of total) 24 8 (33.3) 8 (33.3) 6 (25) 2 (8.3)
Tumour weight
Inoperable 41 0 0 23 18
Operable 137 57 33 37 10
Operable (weighed) 118 49 31 28 10
Weight <550 g 22 15 5 1
Weight 550-999 g 22 10 13 6
Weight >1,000 g 5 6 10 3
Histology
Favourable histology 164 56 28 51 29
Focal anaplasia 11 1 1 3 6
Diffuse anaplasia 13 0 4 6 3
Outcome
Achieved remission 175 57 33 57 28
Relapse 32 7 6 9 10
Local 8 3 1 1 3
Lung 17 2 3 6 6
Liver 2 1 0 1 0
Multiple 5 1 2 1 1
Alive disease free (%) 142 (75.5) 52 (91.2) 28 (84.8) 44 (73.3) 18 (47.4)
Died of disease 34 3 2 11 18
Lost/unrelated death 12 2 3 5 2
TABLE II. Characteristics of the Stage IV Wilms Tumour Patients
Total Black Mixed race White
Histology
Favourable 29 (14) 16 (7) 13 (7) 0
Focal anaplasia 6 (2) 4 (0) 0 2 (2)
Diffuse anaplasia 3 (0) 1 (0) 2 (0) 0
Stage IV WT by race 38 21 15 2
All WT by race 188 79 85 24
Percentage of stage IV WT by race 20.2% 26.6% 17.6% 8.3%
Cohort
1979–1983 1 0 1 0
1984–1993 18 11 7 0
1994–2003 19 10 7 2
Site Lung Lung and liver Liver Brain
Metastases 28 6 3 1
Entries within parenthesis are alive disease free.
Pediatr Blood Cancer DOI 10.1002/pbc
Wilms Tumour Experience in South Africa 467

bypass. Six are alive and disease free, and three died of
progressive disease or following relapse.
Thirteen of the 29 FH stage IV tumours did poorly. Six
failed to achieve remission and seven patients relapsed. Only
one of the children who relapsed has survived.
Neither rhabdomyomatous histology nor nephro-
blastomatosis conferred a poorer outcome, with estimated
5-year OS of 82.6% and 82.6%, respectively. Of the
20 patients with rhabdomyomatous histology, 40%
were inoperable with a 75% response rate to primary chemo-
therapy. This is comparable to the 81.6% response rate seen
among FH tumours that were inoperable at diagnosis.
Considering the small group of patients with UFH, those
with focal anaplasia fared as poorly as those with diffuse
anaplasia; estimated 5-year OS of 54.6% compared to 50.4%
(log-rank P value¼ 0.65). Six of the 11 patients in the focal
anaplasia group were stage IV compared to only 3 of the
13 patients with diffuse anaplasia. Four of the five deaths in
those with focal anaplasia occurred in the six stage IV
tumours.
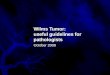
When the patients were analysed by race, there is a trend
that does not achieve statistical significance for white
patients to do better than mixed-race and black patients.
Estimated 5-year OS was 91.1%, 84.0% and 72.9%,
respectively (Chi-square P value¼ 0.13). However, when
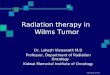
metastatic disease was excluded, there was no difference
between the groups—estimated 5-year OS was 90.2%,
89.5% and 86.9% (Chi-square P value¼ 0.92). Kaplan–
Meier curves are shown in Figures 2 and 3. Table II
shows that a higher proportion of black children (26.6%)
had metastatic disease compared to mixed-race (17.6%)
or white children (8.3%), and that nearly one quarter
(23.8%) of black stage IV patients had UFH. Estimated 5-
year OS for black children with stage IV disease was
35.9% compared to 59.3% for mixed-race children (log-
rank P value¼ 0.16). Notably, when UFH tumours were
excluded from analysis, the estimated 5-year OS was still
lower for black FH stage IV patients at 49.1% compared
to 60.6% for mixed-race FH stage IV patients (log-rank
P value¼ 0.45). Both thewhite childrenwho presentedwith
stage IV disease had focal anaplasia and are alive and
disease free.
Relapse
Relapse occurred in 32 children of whom 20 were
still receiving chemotherapy. The remaining 12 relapsed
2 months–3.5 years after completing therapy. Of the
175 patients who achieved remission, the rate of relapse by
stage was as follows: stage I 12.3%, stage II 18.2%, stage III
15.8%, stage IV 35.7%. The number of relapses by stage is
shown in Table I. The commonest site of relapse was
pulmonary, occurring in 17 cases. There were eight local
relapses, two liver relapses and five relapses at multiple sites.
Eight patients (25%) had UFH and two patients (6.3%) had
nephroblastomatosis.
Fig. 1. Estimated 5-year overall survival (OS) Favourable histology Wilms tumour 1979–2003. [Color figure can be viewed in the online issue,
which is available at www.interscience.wiley.com.]
Pediatr Blood Cancer DOI 10.1002/pbc
468 Davidson et al.

Salvage was good for stage I and II (8 survivors out of 13)
but poor for stage III and IV (2 survivors out of 19). Salvage
was better for pulmonary relapse (6 survivors out of 17) than
for local relapse (2 survivors out of 8). Only one of the eight
patients with UFH survived. Five of those 12 (41.7%) who
relapsed off treatment are alive and disease free. By contrast
only 5 of the 20 (25%) who relapsed on treatment were
survivors.
Fig. 2. Estimated 5-year OS by race Stage I–IVWilms tumour 1979–2003. [Color figure can be viewed in the online issue, which is available at
www.interscience.wiley.com.]
Fig. 3. Estimated 5-year OS by race Stage I–III Wilms tumour 1979–2003. [Color figure can be viewed in the online issue, which is available at
www.interscience.wiley.com.]
Pediatr Blood Cancer DOI 10.1002/pbc
Wilms Tumour Experience in South Africa 469

Complications of Treatment
Complications of treatment were relatively few. One
hundred twelve patients received anthracyclines initially or
at relapse, the cumulative dose ranging from 90 to 440 mg/
m2. Of these, 77 received a cumulative dose of over 250 mg/
m2, two of whom received over 350 mg/m2. Two of the
112 (1.8%) patients developed cardiomyopathy. One
received 430 mg/m2 as well as pulmonary radiotherapy and
died of cardiomyopathy. The other received 300mg/m2 and is
alive on antifailure treatment.
Eleven patients received ifosfamide for resistant disease or
at relapse, the cumulative dose ranging from 18 to 72 g/m2.
One patient developed nephrogenic diabetes insipidus and
Fanconi’s syndrome after 36 g/m2 and subsequently died of
disease. There are only three survivors, 66.1–105.9 months
from diagnosis, all with normal renal tubular reabsorption of
phosphate.
One patient developed veno-occlusive disease after
dactinomycin, and one infant suffered a brief unexplained
apnoea after vincristine and dactinomycin. There are no
secondary malignancies to date.
Complications of surgery occurred in 41 (21.8%) patients.
There was rupture or spillage as defined by the NWTSG
(beyond the flank) in 12, and local spillage in five.
Considering only the 137 operable tumours there were 11
with NWTSG-defined spillage (8%). All were treated with
vincristine, actinomycin and doxorubicin as well as renal bed
irradiation (10–20 Gray). Of the 122 FH tumours that were
operable, 10 had NWTSG-defined spillage. In this group
there were no local relapses but two pulmonary relapses, and
no difference in estimated RFS between those with spill
(80%) and those without (84.4%) (log-rank P value¼ 0.64).
Of interest is that of the five patients who experienced local
spillage—all were treated with vincristine and actinomycin,
and one before 1989 with renal bed radiotherapy—there were
three relapses, one local and two pulmonary. The patient with
local relapse was salvaged with three drugs and renal bed
irradiation.
Post-operative small bowel obstruction occurred in
17 cases (9%) and wound sepsis in three. There were two
cases of wound dehiscence and one patient had major
bleeding during surgery (defined as more than 50 ml/kg of
blood loss). This patient was not tested for acquired von
Willebrand disease. Routine partial thromboplastin time
(PTT) testing has been undertaken for several years. Only one
child had a prolonged PTTandwas found to have normal von
Willebrand factor activity.
DISCUSSION
How does our group compare with larger reported series
such as those of the NWTSG? The mild predominance of
female patients is unusual, but the age distribution is typical
with a median of 39.2 months-median age of presentation in
NWTSG is 36.5 months for boys and 42.5 months for girls
[5]. Poor nutrition was a common problem, and our figure of
20.7% below the 3rd centile of weight for age is conservative
in a series where 20.3% of the tumours weighed more than
1,000 g. Renal failure was extremely uncommon, consistent
with the 0.25% reported by NWTSG for unilateral Wilms
tumours [6].
More patients had advanced disease than those on
NWTSG studies; 31.9% of our patients were stage III and
20.2% stage IV compared to 21% and 11%, respectively of
NWTS-3 [7]. There were also larger tumours; 66.9% of our
patients had tumours larger than 500 g compared to 49% of
the patients on NWTS-3 [8]. Moreover, 63.6% were more
than 550 g, aweight belowwhich tumours are associatedwith
a good prognosis especially in children younger than 2 years
of age [9]. There were more anaplastic tumours (12.8%) in
our series than in NWTS-3 (3.9%) [7]. IVC thrombosis was
comparable to the 4% rate reported by the NWTSG [10].
NWTSG currently reports a 4-year OS for patients with
FHWilms tumour that approaches 90% [5]. Four-year OS for
stage I through IV reported by NWTS-3 were 95.6%, 91.1%,
90.9%, and 80.9%, respectively [11]. Hence, our results are
comparable for non-metastatic Wilms tumour, but disap-
pointing for patients with stage IV disease. Significantly,
recent stage IV patients (1994–2003) did no better than those
in earlier years (1984–1993). Our stage III patients fared
equally well regardless of their amenability to surgery at
diagnosis. Notably, tumour size was not an obstacle to
resection with 35.7% exceeding 1,000 g.
The results of our UFH are surprising in that focal
anaplasia fared as poorly as diffuse anaplasia. NWTS-3 and -
4 reported a 4-yearOS of 52.2% for stage II–IV tumourswith
diffuse anaplasia [12]. There was a small group of children
with focal anaplasia with a 100%OS. In our series, the larger
number of stage IV tumours among those with focal
anaplasia (54.5%) probably accounts for their poor outcome.
Hadley [1] pointed to a poor prognosis for black patients in
SouthAfricawithWilms tumour, and noted a high proportion
of advanced local and metastatic disease, as well as
nutritional and infective co-morbidity. Our results show
that black patients with non-metastatic disease do as well as
other patients. Metastatic disease was seen relatively more
frequently in black patients and conferred a very poor
prognosis. In part this is explained by a higher proportion of
stage IV tumours with UFH, but even black children with FH
metastatic disease fared worse than their mixed-race
counterparts.
There is an approximately 15% risk of recurrence in
Wilms tumour [13]. Lungs, liver, contralateral kidney and
renal bed are the commonest sites, and risk factors include
stage, histology, advanced age at diagnosis, tumour size, and
lymph node involvement. In addition, spillage or pre-
operative rupture has been demonstrated to be a risk factor
for local recurrence [14], and nephroblastomatosis has been
cited as an independent risk factor for both relapse [15] and
contralateral disease [16]. In our series, UFH and high stage
Pediatr Blood Cancer DOI 10.1002/pbc
470 Davidson et al.

were associatedwith increased relapse.Nephroblastomatosis
occurredmore frequently in our series than the 4.5% reported
in the literature [8], but did not confer additional risk of
relapse. Spill or rupture was also not associated with
increased risk of local relapse.
Post-relapse survival on NWTS-2 and -3 was best for
tumours of low stage and FH, pulmonary relapse and those
relapses occurring more than 12 months after diagnosis [17],
and this was what we experienced. In the literature,
rhabdomyomatous change is associated with a poor response
to chemotherapy [18], but a generally favourable outcome
when treated by surgery [19]. However, the response rate in
our serieswas nopoorer among thosewith rhabdomyomatous
histology than other FH Wilms tumours.
The rate of surgical complications was low in our series.
NWTSG-defined intra-operative spillage or rupture occurred
in 8%; much less frequently than the 20% reported by
NWTS-4 [20]. At 9%, the frequency of small bowel
obstruction was comparable to the 6.9% reported by
NWTS-3. All other complications were negligible.
NationalWilmsTumourStudyGroup protocols employed
in an African setting with appropriate surgical expertise,
produced results for non-metastatic favourable histology
Wilms tumour comparable to the NWTSG. Results for
metastatic disease and UFH tumours were poor. A recent
review of Wilms tumour treatment concluded that there is
very little to choose between primary surgery and pre-
operative chemotherapy in the face of modern, expert care
[20]. Early surgery is recommended where circumstances
allow; our results show that this approach is possible outside a
developed world setting.
REFERENCES
1. HadleyGP, JacobsC. The clinical presentation ofWilms’ tumour in
black children. S Afr Med J 1990;77:565–567.
2. Zaghloul MS, Hussein MH, Koutbey ME. Wilms’ tumor: Long-
term results from a single institution. J SurgOncol 1994;56:25–31.
3. Southall HA, Mthembu TZ, Dorrington R, et al. Census 2001.
Online at http://www.statssa.gov.za. Accessed 8 December 2004.
4. Edes D. Background Report: Cape Town Economic Trends and
Analysis: 1980–2000. Online at http://www.capetown.gov.za.
econstats. Accessed 8 December 2004.
5. NevilleH,RitcheyM.Wilms’ tumor:OverviewofNationalWilms’
Tumor Study Group results. Urol Clin North Am 2000;27:435–
442.
6. Ritchey ML, Green DM, Thomas PRM, et al. Renal failure in
Wilms’ tumor patients: A report from the National Wilms’ Tumor
Study Group. Med Pediatr Oncol 1996;26:75–80.
7. Green DM, Breslow NE, Beckwith JB, et al. Effect of duration of
treatment on treatment outcome and cost of treatment for Wilms’
tumor: A report from the National Wilms’ Tumor Study Group.
J Clin Oncol 1998;16:3744–3751.
8. Breslow NE, Sharples K, Beckwith JB, et al. Prognostic factors in
nonmetastatic, favourable histology Wilms’ tumor. Cancer 1991;
68:2345–2353.
9. Green DM. The treatment of stages I–IV favorable histology
Wilms’ tumor. J Clin Oncol 2004;22:1366–1372.
10. National Wilms’ Tumor Study Committee. Wilms’ tumor: Status
report, 1990. J Clin Oncol 1991;9:877–887.
11. Green DM, Thomas PRM, Shochat S. The treatment of Wilms’
tumor: Results of the National Wilms Tumor Studies. Hematol/
Oncol Clin North Am 1995;9:1267–1274.
12. Green DM, Beckwith JB, Breslow NE, et al. Treatment of children
with stages II to IV anaplastic Wilms’ tumor: A report from the
NationalWilms’ Tumor StudyGroup. J ClinOncol 1994;12:2126–
2131.
13. Farhat W, McLorie G, Capolicchio G. Wilms’ tumor: Surgical
considerations and controversies. Urol Clin North Am 2000;27:
455–462.
14. Shamberger RC, Guthrie KA, Ritchey ML, et al. Surgery-related
factors and local recurrence of Wilms Tumor in National Wilms
Tumor Study 4. Ann Surg 1999;229:292–297.
15. Bergeron C, Iliescu C, Thiesse P, et al. Does nephroblastomatosis
influence the natural history and relapse rate in Wilms’ tumour? A
single centre experience over 11 years. Eur J Cancer 2001;37:385–391.
16. Coppes MJ, Arnold M, Beckwith JB, et al. Factors affecting the
risk of contralateral Wilms tumor development. Cancer 1999;85:
1616–1625.
17. Grundy P, Breslow NE, Green DM, et al. Prognostic factors for
children with recurrentWilms’ tumor: Results from the second and
third National Wilms’ Tumor Study. J Clin Oncol 1989;7:638–
647.
18. Pollono D, Drut R, Tomarchio S, et al. Fetal rhabdomyomatous
nephroblastoma: Report of 14 cases confirming chemotherapy
resistance. J Pediatr Hematol Oncol 2003;25:640–643.
19. Maes Ph, Delemarre J, de Kraker J, Ninane J. Fetal rhabdomyo-
matous nephroblastoma: A tumour of good prognosis but resistant
to chemotherapy. Eur J Cancer 1999;35:1356–1360.
20. D’Angio GJ. Pre- or post-operative treatment for Wilms tumor?
Who, what, when, where, how, why, and which.Med Pediatr Oncol
2003;41:545–549.
Pediatr Blood Cancer DOI 10.1002/pbc
Wilms Tumour Experience in South Africa 471