Embed Size (px)
Citation preview

Grand Rounds Vol 10 pages 46–50
Specialities: Histopathology; Urology
Article Type: Case Report
DOI: 10.1102/1470-5206.2010.0011
� 2010 e-MED Ltd
Horseshoe kidney and primary renal
carcinoid tumour: a case report
of a rare entity
Jonathon Peter de Hoog, Spencer Murray and Wayne Chou
Royal Hobart Hospital, 48 Liverpool Street, Hobart, Tasmania, 7000, Australia
Corresponding address: Dr Jonathon de Hoog, c/o Royal Hobart Hospital,
48 Liverpool Street, Hobart, Tasmania, 7000, Australia.
Email: [email protected]
Date accepted for publication 6 May 2010
Abstract
Carcinoid tumours are unique neuroendocrine neoplasms, displaying low-grade malignant
potential and arising frequently within the gastrointestinal tract and respiratory tree. Primary
carcinoid arising within the renal system is uncommon, whilst carcinoid tumour arising within a
horseshoe kidney is rare. We describe a case of primary renal carcinoid occurring within a
horseshoe kidney.
Keywords
Carcinoid; renal; kidney; neoplasm.
Case report
A 51-year-old man was found to have a mass in a previously unknown horseshoe kidney whilst
undergoing computed tomography (CT) lumbar spine investigation for lumbar back pain and
sciatica. History and examination were unremarkable for carcinoid syndrome or urinary tract
symptoms. Full blood analysis, biochemistry, and urinalysis were within normal parameters.
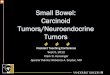
Staging CT chest, abdomen and pelvis revealed a horseshoe kidney containing a solid,
heterogeneous, enhancing, 60�42�35mm mass involving the right lower pole and extending
up to the site of lower pole fusion, with areas of focal calcification. There was no evidence of
metastatic spread (Fig. 1). An uncomplicated tumour resection occurred through a midline
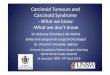
laparotomy with partial nephrectomy and resection of the horseshoe isthmus. A 40�50�35mm
specimen was resected, containing a well-circumscribed pale tumour, measuring 30�25�20mm
(Fig. 2). The patient recovered well and 1 year postoperatively an octreotide study with single
photon emission-computed tomography/CT images demonstrated no evidence of metastatic
tumour.
Diagnosis
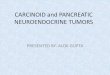
Histopathology demonstrated a solid mass composed of tightly packed trabeculae, in a
background of minimal sclerotic stroma. The tumour cells showed uniform round to ovoid
This paper is available online at http://www.grandrounds-e-med.com. In the event of a change in the URL
address, please use the DOI provided to locate the paper.

nuclei with characteristic fine stippled chromatin. These cells appeared in parallel to each other
forming trabecula and ribbons. There was no evidence of tumour necrosis and no increase in
mitotic activity (Fig. 3).
Immunohistochemical staining was positive for neuroendocrine markers including chromo-
granian, synaptophysin and neuron-specific enolase, confirming the diagnosis of carcinoid.
The cells stained negative for TTF-1, WT-1, and CK-20, ruling out lung and bowel primary sources
(Fig. 4).
Discussion
Carcinoid tumours are a well described, but rare entity arising from neuroendocrine cells. First
described over 100 years ago by Lubarsch, they tend to behave in a more indolent progression
than adenocarcinomas[1].
Fig. 1. CT abdomen. The tumour arises within the horseshoe kidney and is heterogeneous in nature.
Fig. 2. Renal isthmus-containing tumour. The black ink and blue ink display left and right surgical margin, respectively. Awell-circumscribed pale tumour can be seen superiorly with normal renal parenchyma inferiorly.
Horseshoe kidney and primary renal carcinoid tumour 47

Primary carcinoid arising in the kidney is rare (51%), being first described in 1966 by Resnick
and colleagues. Lane et al.[2] recently studied primary neuroendocrine tumours of the kidney and
found only 56 published case reports of primary renal carcinoid, 10 of which arose within
horseshoe kidneys. Our literature review revealed 12 articles (including the above) identifying
17 patients with a primary renal carcinoid arising in the setting of a horseshoe kidney. Carcinoid
appear over-represented in horseshoe kidneys compared with normal renal anatomy[3,4].
Carcinoid tumours arise from neuroendocrine cells but because neuroendocrine cells are not
identified within the kidney or renal pelvis, the precise pathogenesis of these lesions remains
unclear. Current hypotheses suggest that these tumours derive from interspersed neuroendocrine
cells associated with acquired and/or congenital abnormalities. Hypotheses currently include
1. Metaplasia of the urothelium induced by chronic inflammation
2. Metastasis from an unknown primary
3. Abnormal migration of neural crest cells
4. Concurrent congenital renal abnormalities, most commonly arising in the setting of a
teratomatous respiratory or gastrointestinal epithelium within the kidney.
The final hypothesis receives the most support, given that there has been coexistence of
congenital renal abnormalities (horseshoe kidney) and teratoma in several of the previously
reported case studies, suggesting a role for predisposing embryological factors[3,5,6].
The diagnosis of carcinoid tumours of the kidney is often made incidentally and patients are
usually asymptomatic at time of diagnosis. Common presenting symptoms are similar to that of
other renal tumours, including abdominal, back or flank pain, hematuria, constipation and fever.
Up to a quarter of patients have a palpable abdominal mass. The carcinoid syndrome,
Fig. 3. Microscopic imaging of carcinoid tumour demonstrating tightly packed trabeculae of carcinoid cells with abackground minimal sclerotic stroma. Note the uniform nuclei with fine stippled chromatin.
Fig. 4. Immunohistochemical staining with synaptophysin. The cells display strong affinity to synaptophysin asdemonstrated by the intense pink staining.
48 J.P. de Hoog et al.

characterised by skin flushing and telangiectasia, diarrhoea and abdominal pain, cardiac valvular
lesions, and bronchoconstriction, has not been reported to occur within a tumour arising in the
setting of a horseshoe kidney[2].
Carcinoids display slow growth and remain clinically undetected despite being present for
many years. Commonly observed at a mean age of 50 years, they appear to have no predilection
for gender. Their size at diagnosis is large; the retroperitoneum is able to expand with relatively
little impedance before becoming symptomatic and thus the average size at diagnosis of primary
renal carcinoid has been reported to be 8cm. Fourteen of 17 horseshoe kidney carcinoids were
greater than 5 cm at diagnosis[1].
The most common finding at radiologic imaging are solid, circumscribed lesions, often
appearing heterogeneous on CT and ultrasound with minimal enhancement on contrast CT, thus
making differentiating renal carcinoid from renal cell carcinoma unreliable on imaging alone[7].
Newer methods for characterising carcinoid include the use of octreotide scintigraphy. Around
80% of carcinoid tumours express somatostatin receptors, and somatostatin receptor scintigraphy
with radiolabelled octreotide shows an 85% sensitivity for disease. This method of imaging has
advantages in detecting carcinoid lesions before CT and magnetic resonance imaging detection.
Its disadvantage occurs within the kidneys; octreotide’s main elimination is via the renal system,
and this may obscure suspicious lesions within the kidney[8]. All patients should receive
somatostatin scintigraphy as part of their disease staging and follow-up process.
Microscopically, renal carcinoids are characterised by tightly packed cords and trabeculae of
neoplastic cells appearing eosinophilic with a granular cytoplasm and nuclei containing fine
stippled chromatin. These impart a ribbon-like appearance, with minimal stroma often composed
of fibrous tissue. Calcifications are present in around 25% of cases, and frequent mitosis (42 per
10 HPFs) are characteristically absent[2,9].
Immunohistochemical stains are utilised in the diagnosis and exclude other sites as a primary
lesion. Nearly all lesions reported are positive for synaptophysin and chromogranin. Staining for
vimentin and CAM 5.2 has been more variable. These stains detect the intracytoplasmic secretory
granules of neuroendocrine tumours. Other important immunochemical markers are TTF-1 and
WT-1, markers for lung carcinoid and Wilms tumour, respectively. These are common differentials
in a carcinoid arising within the kidney[1].
The mainstay of treatment for primary renal carcinoid is resection, because it is the only
treatment known to cure patients of their primary disease. Procedures include partial
nephrectomy, surgical excision of isthmus tumours to total nephrouretectomy. There is no
consensus on which technique is favoured, and patients should be assessed on a case by case
basis.
Chemotherapeutic regimes in the management of primary renal carcinoid have been utilised,
but little evidence exists that this improves survival. To date, there is no published material
specifically dealing with chemotherapy for renal carcinoids. Somatostatin analogues, most notably
octreotide, are used in reducing the symptoms of the carcinoid syndrome but where this is
absent, they have no role in therapy[10].
Because extended follow-up periods have been previously observed, and during this time new
metastatic disease has been identified, it is important to continue to monitor patients for
evidence of recurrence[4]. Octreotide scintigraphy is the most valuable imaging investigation and
the monitoring of serum chromogranin and urinary 5-hydroxyindoleacetic acid provides a
valuable biochemical marker (when present) for detecting disease progression or recurrence after
treatment. The frequency of imaging and biochemical monitoring should be tailored to the
individual patient; there are few data to suggest exactly within which time frame this should
occur; previous authors have suggested 6-monthly and 12-monthly biochemical and imaging
screening, respectively. It is important that patients are reviewed over the long-term, and new
disease presentations are managed accordingly.
Teaching point
Although rare, carcinoid tumour arising within the kidney is a well-defined entity. The diagnosis
is confirmed by immunohistochemistry, and surgical excision provides the only definitive
treatment modality to date. Metastases are described but are infrequent and the incidence of
carcinoid syndrome accompanying a renal carcinoid is very rare. Imaging of choice involves CT
scanning and octreotide scintigraphy. Follow-up is essential in the long-term, as these lesions
have recurred.
Horseshoe kidney and primary renal carcinoid tumour 49

References
1. Romero FR, Rais-Bahrami S, Permpongkosol S, Fine SW, Kohanim S, Jarrett TW. Primary
carcinoid tumours of the kidney. J Urol 2006; 176: 2359–66. doi:10.1016/j.juro.2006.07.129.
PMid:17085102.
2. Lane BR, Chery F, Jour G, et al. Renal neroendocrine tumours: a clinicopathological study. BJU
Int 2007; 100: 1030–5.
3. Krishnan B, Truong LD, Saleh G, Sirbasku DM, Slawin KM. Horseshoe kidney is associated with
an increased relative risk of primary renal carcinoid tumor. J Urol 1997; 157: 2059–66.
doi:10.1016/S0022-5347(01)64674-3.
4. Shurtleff BT, Shvarts O, Rajfer J. Carcinoid tumor of the kidney: case report and review of the
literature. Rev Urol 2005; 7: 229–33.
5. Begin LR, Guy L, Jacobson SA, Aprikian AG. Renal carcinoid and horseshoe kidney: a frequent
association of two rare entities – a case report and review of the literature. J Surg Oncol 1998;
68: 113–19. doi:10.1002/(SICI)1096-9098(199806)68:25113::AID-JSO843.0.CO;2-9.
6. Isobe H, Takashima H, Higashi N, et al. Primary carcinoid tumor in a horseshoe kidney. Int J
Urol 2000; 7: 184–8. doi:10.1046/j.1442-2042.2000.00160.x. PMid:10830826.
7. Jensen RT, Gibril F. Somatostatin receptor scintigraphy in gastrinomas. Ital J Gastroenterol
Hepatol 1999; 31(Suppl 2): s179–85.
8. Mufarrij P, Varkarakis IM, Studeman KD, Jarrett TW. Primary renal carcinoid tumor with liver
metastases detected with somatostatin receptor imaging. Urology 2005; 65: 1002e19–21.
9. Hansel DE, Epstein J, Berbescu E, Fine SW, Young RH, Chevill JC. Renal carcinoid tumor:
a Clinicopathologic study of 21 cases. Am J Surg Pathol 2007; 31: 1539–44.
10. Hulke MH, Mayer RJ. Carcinoid tumors. N Engl J Med 1999; 340: 858–67.
50 J.P. de Hoog et al.