Embed Size (px)
Citation preview
Valvular Heart Disease
Health-Related Quality of Life After Transcatheter AorticValve Replacement in Inoperable Patients With Severe
Aortic StenosisMatthew R. Reynolds, MD, MSc; Elizabeth A. Magnuson, ScD; Yang Lei, MSc; Martin B. Leon, MD;
Craig R. Smith, MD; Lars G. Svensson, MD, PhD; John G. Webb, MD; Vasilis C. Babaliaros, MD;Bruce S. Bowers, MD; William F. Fearon, MD; Howard C. Herrmann, MD; Samir Kapadia, MD;
Susheel K. Kodali, MD; Raj R. Makkar, MD; Augusto D. Pichard, MD; David J. Cohen, MD, MSc;for the Placement of Aortic Transcatheter Valves (PARTNER) Investigators
Background—Transcatheter aortic valve replacement (TAVR) has been shown to improve survival compared withstandard therapy in patients with severe aortic stenosis who cannot have surgery. The effects of TAVR on health-relatedquality of life have not been reported from a controlled study.
Methods and Results—The Placement of Aortic Transcatheter Valves (PARTNER) trial randomized patients withsymptomatic, severe aortic stenosis who were not candidates for surgical valve replacement to TAVR (n�179) orstandard therapy (n�179). Health-related quality of life was assessed at baseline and at 1, 6, and 12 months with theKansas City Cardiomyopathy Questionnaire (KCCQ) and the 12-item Short Form-12 General Health Survey (SF-12).The primary end point was the KCCQ overall summary score (range, 0–100; higher�better). At baseline, mean KCCQsummary scores (35�20) and SF-12 physical summary scores (28�7) were markedly depressed. Although the KCCQsummary score improved from baseline in both groups, the extent of improvement was greater after TAVR comparedwith control at 1 month (mean between-group difference, 13 points; 95% confidence interval, 8–19; P�0.001) withlarger benefits at 6 months (mean difference, 21 points; 95% confidence interval, 15–27; P�0.001) and 12 months(mean difference, 26 points; 95% confidence interval, 19–33; P�0.001). At 12 months, TAVR patients also reportedhigher SF-12 physical and mental health scores with mean differences compared with standard care of 5.7 and 6.4points, respectively (P�0.001 for both comparisons).
Conclusions—Among inoperable patients with severe aortic stenosis, compared with standard care, TAVR resulted insignificant improvements in health-related quality of life that were maintained for at least 1 year.
Clinical Trials Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00530894.(Circulation. 2011;124:1964-1972.)
Key Words: aortic valve stenosis � heart valves � quality of life
Aortic stenosis is a common condition among the elderlyand is associated with poor survival without surgery
once symptoms develop.1,2 In addition, patients with severeaortic stenosis experience progressive symptoms and reducedfunctional status and quality of life. Despite the success ofsurgical valve replacement at alleviating symptoms, improv-ing functional status, and extending survival,3,4 a substantialminority of patients with severe aortic stenosis go untreatedbecause of comorbid medical conditions and cardiovascularabnormalities that result in prohibitive surgical risk.5,6 One-
year mortality rates may be as high as 50% to 60% in thesepatients.1,7,8
Clinical Perspective on p 1972
After the first human report in 2002,9 transcatheter aorticvalve replacement (TAVR) has emerged as a less invasivetreatment option for patients with aortic stenosis and high orunacceptable surgical risk.10–12 Recently, the Placement ofAortic Transcatheter Valves (PARTNER) trial demonstratedthat for patients who are not suitable candidates for surgery,
Continuing medical education (CME) credit is available for this article. Go to http://cme.ahajournals.org to take the quiz.Received April 24, 2011; accepted August 24, 2011.From the Harvard Clinical Research Institute, Boston VA Healthcare System, Boston, MA (M.R.R.); Columbia–Presbyterian Hospital, New York, NY
(M.B.L.,C.R.S., S.K..K); Cleveland Clinic, Cleveland, OH (L.G.S., S.K.); St. Paul’s Hospital, Vancouver, BC, Canada (J.G.W.); Emory UniversityHospital, Atlanta, GA (V.C.B.); Medical City Dallas, Dallas, TX (B.S.B.); Stanford University, Stanford, CA (W.F.F.); University of Pennsylvania,Philadelphia (H.C.H.); Cedars-Sinai Heart Institute, Los Angeles, CA (R.R.M.); Washington Hospital Center, Washington, DC (A.D.P.); and Saint Luke’sMid America Heart and Vascular Institute, University of Missouri–Kansas City (E.A.M., Y.L., D.J.C.).
Correspondence to David J. Cohen, MD, MSc, Saint Luke’s Mid America Heart Institute, University of Missouri–Kansas City School of Medicine,4401 Wornall Rd, Kansas City, MO 64111. E-mail [email protected]
© 2011 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.111.040022
1964
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from
TAVR led to a 20% absolute reduction in all-cause mortalityat 1 year compared with standard therapy but also to anincrease in the incidence of major strokes and vascularcomplications.8
For patients with severe heart failure and the elderly ingeneral, improvements in symptoms, functional status, andquality of life may be even more important than improve-ments in longevity.13 Thus, a full characterization of theimpact of TAVR on patients with severe aortic stenosisrequires an understanding of the effects of the intervention onpatients’ health status.14 We therefore performed a prospec-tive quality-of-life substudy among patients enrolled in thePARTNER trial and present here the results for the cohort ofpatients who were not candidates for surgical valve replace-ment and were therefore randomized to TAVR or standardtherapy.
MethodsStudy DesignThe design and initial results of the PARTNER trial (cohort B) havebeen published previously.8 In brief, the PARTNER program en-rolled patients with severe aortic stenosis; New York Heart Associ-ation class II, III, or IV heart failure symptoms; and high surgical riskbased on the Society for Thoracic Surgeons (STS) risk score andqualified physician assessments. Patients included in the presentstudy were not considered to be suitable candidates for cardiacsurgery owing to coexisting medical conditions associated with apredicted probability of death or permanent disability �50% asdetermined by at least 2 surgical investigators and reaffirmed by thestudy’s executive committee. These patients were then randomizedto TAVR with the Edwards SAPIEN heart valve system (EdwardsLifesciences, Irvine, CA) or to standard medical care, which oftenincluded balloon aortic valvuloplasty at the discretion of the inves-tigators. The study was approved by the institutional review board ateach participating site, and all patients provided written informedconsent.
Measurement of Health StatusHealth status, which includes symptoms, functional status, andquality of life,15 was evaluated with standardized written question-naires at baseline and 1, 6, and 12 months after randomization. Thebaseline questionnaires were administered before randomization.Follow-up questionnaires were administered during in-person visitsto the enrolling centers or by mail. Linguistically and culturallyvalidated translations of the original questionnaires were provided tonon–English speakers enrolled at 4 non-US sites (1 in Germany and3 in Canada).
Disease-specific health status was assessed from the patient’sperspective with the Kansas City Cardiomyopathy Questionnaire(KCCQ).16 The KCCQ consists of 23 questions addressing 5 healthdomains pertaining to heart failure: symptoms, physical limitation,social limitation, self-efficacy, and quality of life. These individualscales are combined into an overall summary scale with valuesranging from 0 to 100; higher scores indicate lesser symptoms andbetter quality of life. Previous studies have suggested that KCCQsummary scores correlate roughly with New York Heart Associationfunctional class as follows: class I is roughly equal to KCCQsummary score of 75 to 100; class II, to a score of 60 to 74; class III,to a score of 45 to 59; and class IV, to a score of 0 to 44.17 TheKCCQ has undergone extensive validation and has been shown toindependently predict mortality and healthcare costs in heart failurepopulations.18,19 Among outpatients with heart failure, small, mod-erate, or large clinical improvements as rated by treating physicianscorresponded with changes in the KCCQ summary score of �5, 10,and 20 points, respectively.17
Generic health status was evaluated with the Medical OutcomesStudy Short-Form 12 (SF-12) Health Survey.20 The SF-12 wasderived from the original SF-36 health survey by selecting thoseitems having the greatest explanatory power. The physical andmental summary scores for the SF-12 have been shown to correlatehighly with the same summary scores from the SF-36. They arescaled to overall population norms of 50 and SDs of 10; higherscores are better. Multiple groups have agreed that the minimalclinically important changes in the mental and physical summaryscores are roughly 2 to 2.5 points.21,22
Statistical AnalysisSummary scores for each of the SF-12 and KCCQ scales weregenerated according to the scoring algorithms published by theirdevelopers.16,23 The KCCQ overall summary score was prespecifiedas the primary end point of the quality-of-life study. All other endpoints were considered secondary. For baseline characteristics andquality-of-life scores, between-group comparisons were performedwith the �2 test for categorical variables and 2-sample t tests forcontinuous variables.
Mean changes from baseline within each of the treatment groupsat 1, 6, and 12 months were estimated for each of the health statusmeasures for patients with available quality-of-life data and testedfor significance with paired t tests. Although these analyses do notprovide formal between-group comparisons, they have the advantageof testing each patient against his or her own baseline value (thuscorrecting for any potential survivor bias introduced by the attritionof sicker patients over time).
Table 1. Baseline Patient Characteristics andQuality-of-Life Scores
TAVR(n�179)
Control(n�179) P
Age, y 83�9 83�8 0.95
Female sex,% 54.2 54.1 0.92
White race, % 92 91 0.57
STS risk score 11.2�5.8 12.1�6.1 0.14
STS score �15, % 21.2 24.6 0.45
Prior MI, % 18.6 26.4 0.10
Prior CABG, % 37.4 45.6 0.17
Cerebrovascular disease, % 27.4 27.5 1.00
COPD (oxygen dependent), % 21.2 25.7 0.38
Creatinine �2.0 mg/dL, % 5.6 9.6 0.23
Quality-of-life measures
KCCQ overall summary 36.2�20.5 34.4�20.1 0.44
75–100, % 4.1 3.8 0.70
60–74, % 10.6 7.0
45–59, % 15.9 17.8
0–45, % 69.4 71.3
KCCQ symptoms 47.7�22.6 46.0�24.0 0.52
KCCQ physical limitation 34.6�25.7 30.7�24.9 0.19
KCCQ social limitation 27.8�26.9 26.6�25.7 0.70
KCCQ quality of life 33.6�21.7 32.8�22.9 0.74
SF-12 physical 28.2�7.7 27.7�6.9 0.54
SF-12 mental 44.5�12.2 45.2�11.0 0.57
TAVR indicates transcatheter aortic valve replacement; STS, Society ofThoracic Surgery; MI, myocardial infarction; CABG, coronary artery bypassgrafting; COPD, chronic obstructive pulmonary disease; KCCQ, Kansas CityCardiomyopathy Questionnaire; and SF-12, Short Form-12 General HealthSurvey.
Reynolds et al Quality of Life After TAVR 1965
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from
Differences between TAVR and control group scores at eachfollow-up time point were estimated from longitudinal random-effect growth curve models24 that were fit to the repeated measure-ments for each health status outcome. These longitudinal analysesused all available quality-of-life data, including data from patientswho subsequently died, withdrew, or were lost to follow-up, andaccommodate missing data under the missing at random assump-tion.25 Variables included in the models were treatment assignment,prespecified patient characteristics (age, sex, oxygen-dependentchronic obstructive pulmonary disease), follow-up time (linear,quadratic, and cubic effects of time were considered), and interac-tions between treatment and time. Starting with the highest-ordertime-by-treatment interaction, variables were retained in the model ifP�0.10. The intercept and linear time effects were estimated withboth fixed and random effects, whereas quadratic and cubic effectsof time were modeled as fixed effects to avoid overparameterization.These models were used to calculate mean between-group differ-ences for the KCCQ summary score and the individual subscales ateach follow-up time point, as well as the associated 95% confidenceintervals (CIs) and P values.
To examine the potential impact of missing data, which, given theillness severity of the trial population, would most likely not be
missing at random, we repeated our growth curve analyses afterimputing missing scores among surviving patients as the lowestreported score among respondents within each treatment group foreach respective time point. We also examined the magnitude ofpotential survivor bias by comparing the mean baseline scoresbetween treatment groups for the subgroups of patients with avail-able quality-of-life data at each successive follow-up time point.
To estimate the proportion of patients in each group who achievedmeaningful improvements in health status, we also carried out aseries of categorical analyses on the primary end point. At each timepoint, we categorized patients according to whether their extent ofimprovement on the KCCQ summary scale compared with baselinewas moderately large (�10 points) or very large (�20 points); thedenominator for these analyses was the number of patients withavailable quality-of-life data at that particular time point. In addition,we further defined favorable and excellent outcomes for each groupby calculating the proportion of patients at each time point who werealive with at least a 10-point or 20-point improvement, respectively,in the KCCQ summary score compared with baseline. The denom-inator for these analyses was all randomized patients who had notwithdrawn from the study at the particular time point (includingpatients who died). Thus, these latter metrics considered death to be
Table 2. Mean Follow-up Scores and Within-Group Changes in Disease-Specific and Generic Health Status Measures ComparedWith Baseline on the Basis of Paired t Tests
TAVR Group Control Group
Scale/Time PointMean
(�SD) ValueMean �
vs Baseline 95% CI P*Mean
(�SD) ValueMean � vs
Baseline 95% CI P*
KCCQ summary
1 mo 61.6�26.2 24.8 20.2 to 29.3 �0.001 49.2�24.3 10.4 6.0 to 14.8 �0.001
6 mo 70.7�23.0 33.5 28.9 to 38.1 �0.001 50.5�26.1 11.7 6.1 to 17.2 �0.001
12 mo 69.4�25.3 31.8 26.4 to 37.2 �0.001 47.0�24.6 4.1 �2.2 to 10.5 0.20
KCCQ total symptoms
1 mo 69.4�23.3 20.8 16.3 to 25.4 �0.001 60.0�25.0 10.2 6.0 to 14.5 �0.001
6 mo 77.2�18.9 29.2 24.4 to 34.1 �0.001 59.3�25.1 9.2 3.5 to 14.9 0.002
12 mo 75.3�22.8 26.2 21.0 to 31.5 �0.001 58.9�26.0 5.0 �1.6 to 11.5 0.13
KCCQ physical limitations
1 mo 53.3�31.5 15.2 9.0 to 21.2 �0.001 42.1�27.9 6.7 1.7 to 11.7 0.009
6 mo 57.4�30.8 20.3 13.6 to 267.0 �0.001 42.0�28.6 8.5 2.0 to 14.9 0.01
12 mo 56.4�33.2 16.8 10.4 to 23.3 �0.001 39.9�27.4 �1.9 �9.4 to 5.6 0.62
KCCQ social limitation
1 mo 55.7�36.7 26.0 18.6 to 33.5 �0.001 40.7�31.2 9.3 3.4 to 15.2 0.002
6 mo 68.5�32.7 36.2 28.4 to 44.1 �0.001 41.1�33.4 10.8 2.2 to 19.4 0.01
12 mo 64.7�33.2 34.2 25.9 to 42.6 �0.001 50.5�26.1 3.1 �5.7 to 12.0 0.48
KCCQ quality of life
1 mo 65.0�27.9 31.4 26.5 to 36.4 �0.001 50.5�27.6 14.8 9.6 to 19.9 �0.001
6 mo 76.6�24.7 41.9 36.8 to 47.0 �0.001 51.8�27.6 16.2 9.5 to 22.9 �0.001
12 mo 75.9�27.6 41.2 34.7 to 47.6 �0.001 47.6�27.9 6.8 �1.1 to 14.6 0.09
SF-12 physical
1 mo 34.6�10.3 6.3 4.4 to 8.2 �0.001 30.2�7.3 2.0 0.6 to 3.4 0.006
6 mo 36.0�10.6 7.7 5.4 to 9.9 �0.001 30.5�8.2 2.9 0.7 to 5.0 0.01
12 mo 34.9�11.1 6.6 4.3 to 8.9 �0.001 29.7�8.5 2.0 �0.5 to 4.6 0.11
SF-12 mental
1 mo 47.9�11.0 2.8 0.2 to 5.4 0.03 48.5�10.9 2.0 �0.1 to 4.1 0.06
6 mo 36.0�10.6 5.9 3.5 to 8.3 �0.001 46.7�11.8 2.1 �0.6 to 4.8 0.13
12 mo 53.3�10.0 7.0 4.2 to 9.7 �0.001 46.6�11.7 1.0 �2.2 to 4.1 0.53
CI indicates confidence interval; KCCQ, Kansas City Cardiomyopathy Questionnaire; and SF-12, Short Form-12 General Health Survey.*P value derived from paired t tests comparing follow-up score and baseline within the specific treatment group.
1966 Circulation November 1, 2011
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from
equivalent to failure to improve by the specified amount. Theseproportions were compared between groups at each time point with�2 tests.
Finally, we examined potential subgroup effects with respect tothe 6- and 12-month outcomes using the growth curve modelsthrough the introduction of interaction terms between prespecifiedcovariates and treatment assignment. These prespecified subgroupsincluded age �85 versus �85 years; male versus female sex;STS-predicted 30-day mortality rates26 (categorized as �10%, 10%–15%, or �15%); aortic valve gradient �40 versus �40 mm Hg;oxygen-dependent chronic obstructive pulmonary disease versus nooxygen-dependent chronic obstructive pulmonary disease; left ven-tricular ejection fraction �55% versus �55%; and aortic valve areaindex �0.35 versus �0.35 cm2/m2. With the exception of the STSrisk score, each of the cut points for continuous variables was basedon the approximate median value in the study population.
All analyses were performed on an intention-to-treat basis. A2-tailed P value �0.05 was considered statistically significant for allanalyses of between-group differences. No statistical adjustmentswere made for multiple secondary comparisons. All analyses wereperformed with SAS for Windows version 9.2 (SAS Institute, Inc,Cary, NC).
Role of the Funding SourceThe PARTNER trial was funded by Edwards Lifesciences anddesigned collaboratively by the Steering Committee and the sponsor.
The present analysis was carried out by academic investigators at theHarvard Clinical Research Institute (Boston, MA) and the HealthEconomics and Technology Assessment Group at Saint Luke’s MidAmerica Heart and Vascular Institute (Kansas City, MO). Theauthors had unrestricted access to the study data, drafted themanuscript, made the decision to submit for publication, and vouchfor the veracity and completeness of its content.
ResultsPatient Population and Baseline Health StatusAs previously reported, a total of 358 patients with severe,symptomatic aortic stenosis who were not candidates forsurgery were randomized at 21 centers to TAVR (n�179) orstandard therapy (n�179). Nine patients assigned to TAVRdid not have a valve implanted. A total of 140 of the controlgroup patients (78%) underwent balloon aortic valvuloplastyduring follow-up (114 within 1 month of randomization). The12-month mortality rates were 30.7% in the TAVR arm and50.7% in the standard therapy arm.
The baseline characteristics of the 2 study groups weresimilar, and there were no clinically relevant differencesbetween groups in baseline quality-of-life scores (Table 1).
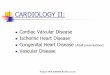
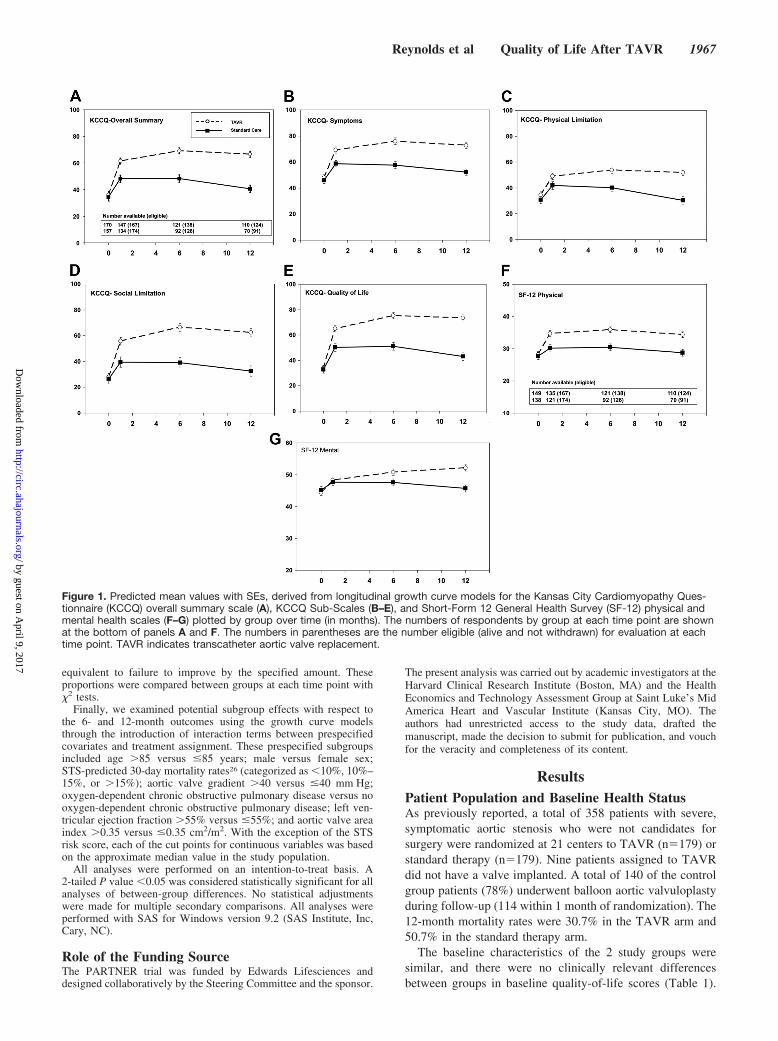
Figure 1. Predicted mean values with SEs, derived from longitudinal growth curve models for the Kansas City Cardiomyopathy Ques-tionnaire (KCCQ) overall summary scale (A), KCCQ Sub-Scales (B–E), and Short-Form 12 General Health Survey (SF-12) physical andmental health scales (F–G) plotted by group over time (in months). The numbers of respondents by group at each time point are shownat the bottom of panels A and F. The numbers in parentheses are the number eligible (alive and not withdrawn) for evaluation at eachtime point. TAVR indicates transcatheter aortic valve replacement.
Reynolds et al Quality of Life After TAVR 1967
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from
The patient population was elderly with a high burden ofchronic medical conditions. The mean physical summaryscores for the SF-12 at baseline were �2 SDs below thepopulation norm for the United States, and the mean baselineKCCQ overall summary scores were in a range previouslyshown to correspond with New York Heart Association classIII and IV functional status.
Within-Group ComparisonsAmong surviving patients, quality-of-life questionnaires werecompleted for �80% of subjects at each time point (baseline,91%; 1 month, 82%; 6 months, 81%; 12 months, 84%), witha slightly higher completion rate among TAVR patients (88%across follow-up time points versus 76% for the controlgroup). Given the high mortality rate in the trial, 12-monthquality-of-life outcome measures were available for only61% of the originally randomized TAVR patients and 39% ofthe originally randomized control group patients.
Mean follow-up scores and the mean change from baselineat each follow-up time point are summarized separately foreach treatment group in Table 2. Although mean quality-of-life scores improved over time for both treatment groups,comparison of the mean within-patient changes from baselinerevealed different patterns of improvement for the TAVR andcontrol patients. For the TAVR group, the mean change frombaseline in the KCCQ overall summary score was 25 pointsat 1 month and increased over time to 34 and 32 points at 6and 12 months, respectively (P�0.001 for all comparisons).In contrast, for the control group, scores were significantlyimproved compared with baseline at both 1 and 6 months(mean changes of 10 and 12 points, respectively; P�0.001for both comparisons), but the change was no longer signif-icantly different from baseline at 12 months (mean change of4 points; P�0.20). Similar patterns of within-group changesover time were noted for each of the KCCQ subscales and theSF-12 summary scales (Table 2).
The difference between the temporal patterns for theoverall group means and the within-group paired compari-sons is explained at least partly by differences in missing data(mainly related to death) between the 2 groups. For thecontrol group, the mean baseline KCCQ overall summaryscores among the subsets of patients who completed ques-tionnaires at each follow-up time point were progressivelyhigher (37, 39, and 43 points for 1-, 6-, and 12-monthrespondents, respectively) than for all baseline respondentscombined (34 points). There was no such trend for the TAVRgroup, however, with mean baseline scores of 37, 37, and 38points for 1-, 6-, and 12-month respondents compared with 36points for all baseline respondents. Thus, the appearance ofsustained improvement in health status at 12 months in thecontrol group relates predominantly to attrition of the sickestpatients over time.
Between-Group ComparisonsPredicted mean scores from the longitudinal growth curvemodels grouped by treatment assignment for each of thequality-of-life scales over the 12-month follow-up period aredisplayed in Figure 1, and the resulting between-groupcomparisons are summarized in Table 3. At 1 month, the
KCCQ summary score had increased to a greater extent in theTAVR group than in the standard therapy group (meandifference, 13.3 points; 95% CI, 7.6–19.0; P�0.001). Thedifference between treatment groups in KCCQ summaryscores became even larger at 6 months (mean difference, 20.8points; 95% CI, 14.7–27.0; P�0.001) and 12 months (meandifference, 26.0 points; 95% CI, 18.7–33.3; P�0.001). Re-sults were similar for each of the individual KCCQ scales.
Changes in the SF-12 physical summary score followed apattern similar to those of the KCCQ summary score, withstatistically significant between-group differences in meanscores of 4.5 to 5.7 points at 1, 6, and 12 months (Figure 1 andTable 3). There was no difference in SF-12 mental compo-nent summary scores at 1 month, but between-group differ-ences in mean scores of 3.2 and 6.4 points in favor of TAVRwere seen at 6 and 12 months.
Table 3. Adjusted Effect of Transcatheter Aortic ValveReplacement Versus Control Therapy on Disease-Specific andGeneric Health Status Measures According to LongitudinalRandom-Effect Growth Curve Models
Scale
Between-GroupDifference
(TAVR-Control)* 95% CI P
KCCQ summary
1 mo 13.3 7.6 to 19.0 �0.001
6 mo 20.8 14.7 to 27.0 �0.001
12 mo 26.0 18.7 to 33.3 �0.001
KCCQ total symptoms
1 mo 10.5 5.1 to 15.9 �0.001
6 mo 18.2 12.5 to 23.9 �0.001
12 mo 20.6 13.6 to 27.6 �0.001
KCCQ physical limitations
1 mo 7.2 2.1 to 12.2 0.006
6 mo 13.8 8.0 to 19.6 �0.001
12 mo 21.7 13.0 to 30.4 �0.001
KCCQ social limitation
1 mo 16.1 8.1 to 24.1 �0.001
6 mo 27.5 18.5 to 36.6 �0.001
12 mo 30.0 20.2 to 39.8 �0.001
KCCQ quality of life
1 mo 14.8 8.6 to 21.0 �0.001
6 mo 24.2 17.4 to 31.0 �0.001
12 mo 30.5 22.3 to 38.7 �0.001
SF-12 physical
1 mo 4.5 2.5 to 6.6 �0.001
6 mo 5.5 3.0–7.9 �0.001
12 mo 5.7 2.8–8.5 �0.001
SF-12 mental
1 mo 0.6 �1.6 to 2.6 0.61
6 mo 3.2 1.1 to 5.3 0.003
12 mo 6.4 3.5 to 9.4 �0.001
CI indicates confidence interval; KCCQ, Kansas City Cardiomyopathy Ques-tionnaire; and SF-12, Short Form-12 General Health Survey.
*Positive values indicate better health status with TAVR.
1968 Circulation November 1, 2011
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from
In sensitivity analyses in which missing KCCQ summaryscores for surviving patients were imputed as the lowestobserved values for each respective time point, the between-group differences became larger than in our primary analysis,with mean differences of 17.9 points (95% CI, 11.6–24.2),25.8 points (95% CI, 18.2–33.3), and 28.9 points (95% CI,20.7–37.0) at 1, 6, and 12 months, respectively (P�0.001 forall comparisons).
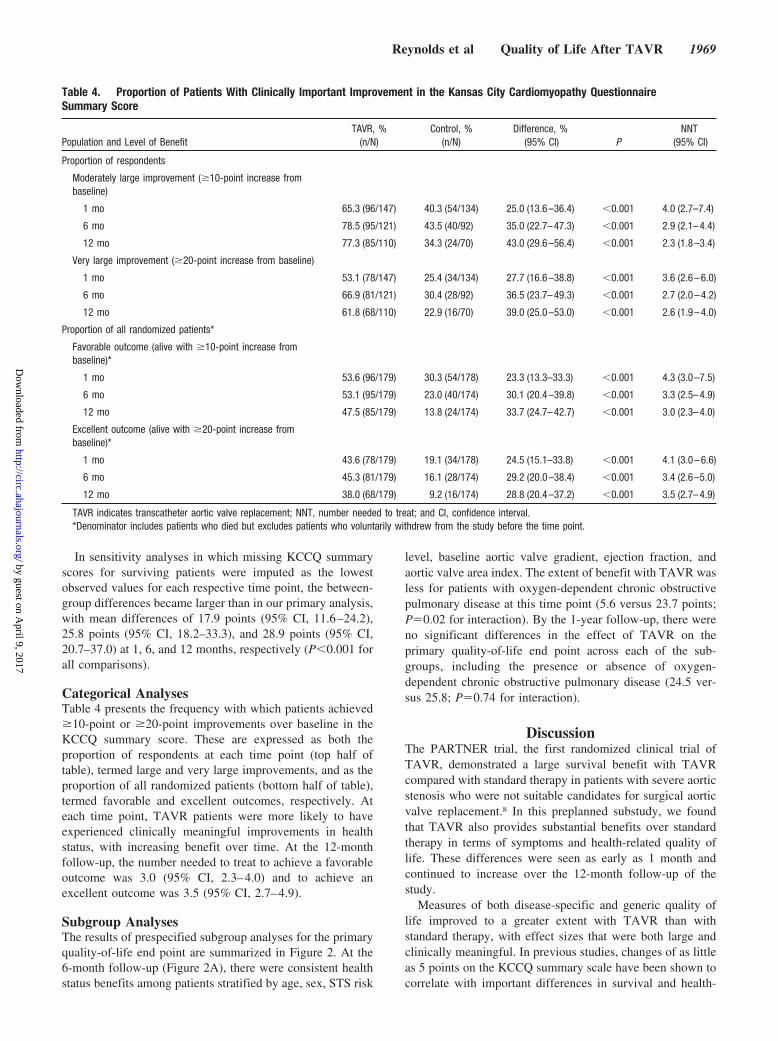
Categorical AnalysesTable 4 presents the frequency with which patients achieved�10-point or �20-point improvements over baseline in theKCCQ summary score. These are expressed as both theproportion of respondents at each time point (top half oftable), termed large and very large improvements, and as theproportion of all randomized patients (bottom half of table),termed favorable and excellent outcomes, respectively. Ateach time point, TAVR patients were more likely to haveexperienced clinically meaningful improvements in healthstatus, with increasing benefit over time. At the 12-monthfollow-up, the number needed to treat to achieve a favorableoutcome was 3.0 (95% CI, 2.3–4.0) and to achieve anexcellent outcome was 3.5 (95% CI, 2.7–4.9).
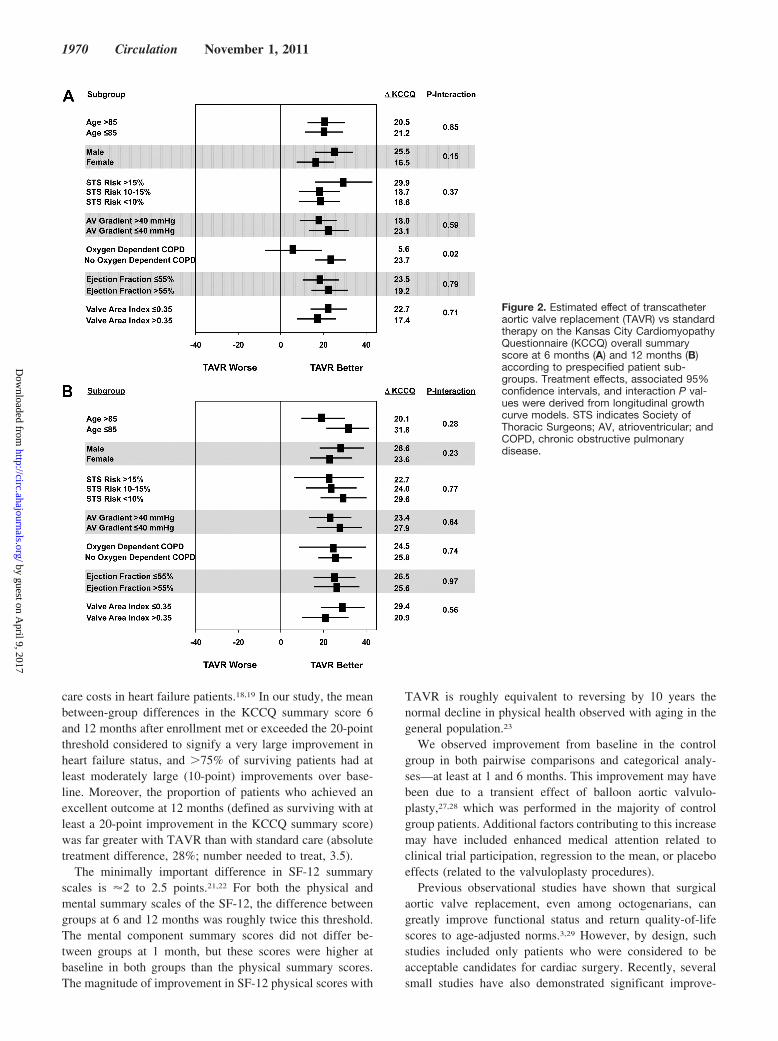
Subgroup AnalysesThe results of prespecified subgroup analyses for the primaryquality-of-life end point are summarized in Figure 2. At the6-month follow-up (Figure 2A), there were consistent healthstatus benefits among patients stratified by age, sex, STS risk
level, baseline aortic valve gradient, ejection fraction, andaortic valve area index. The extent of benefit with TAVR wasless for patients with oxygen-dependent chronic obstructivepulmonary disease at this time point (5.6 versus 23.7 points;P�0.02 for interaction). By the 1-year follow-up, there wereno significant differences in the effect of TAVR on theprimary quality-of-life end point across each of the sub-groups, including the presence or absence of oxygen-dependent chronic obstructive pulmonary disease (24.5 ver-sus 25.8; P�0.74 for interaction).
DiscussionThe PARTNER trial, the first randomized clinical trial ofTAVR, demonstrated a large survival benefit with TAVRcompared with standard therapy in patients with severe aorticstenosis who were not suitable candidates for surgical aorticvalve replacement.8 In this preplanned substudy, we foundthat TAVR also provides substantial benefits over standardtherapy in terms of symptoms and health-related quality oflife. These differences were seen as early as 1 month andcontinued to increase over the 12-month follow-up of thestudy.
Measures of both disease-specific and generic quality oflife improved to a greater extent with TAVR than withstandard therapy, with effect sizes that were both large andclinically meaningful. In previous studies, changes of as littleas 5 points on the KCCQ summary scale have been shown tocorrelate with important differences in survival and health-
Table 4. Proportion of Patients With Clinically Important Improvement in the Kansas City Cardiomyopathy QuestionnaireSummary Score
Population and Level of BenefitTAVR, %
(n/N)Control, %
(n/N)Difference, %
(95% CI) PNNT
(95% CI)
Proportion of respondents
Moderately large improvement (�10-point increase frombaseline)
1 mo 65.3 (96/147) 40.3 (54/134) 25.0 (13.6–36.4) �0.001 4.0 (2.7–7.4)
6 mo 78.5 (95/121) 43.5 (40/92) 35.0 (22.7–47.3) �0.001 2.9 (2.1–4.4)
12 mo 77.3 (85/110) 34.3 (24/70) 43.0 (29.6–56.4) �0.001 2.3 (1.8–3.4)
Very large improvement (�20-point increase from baseline)
1 mo 53.1 (78/147) 25.4 (34/134) 27.7 (16.6–38.8) �0.001 3.6 (2.6–6.0)
6 mo 66.9 (81/121) 30.4 (28/92) 36.5 (23.7–49.3) �0.001 2.7 (2.0–4.2)
12 mo 61.8 (68/110) 22.9 (16/70) 39.0 (25.0–53.0) �0.001 2.6 (1.9–4.0)
Proportion of all randomized patients*
Favorable outcome (alive with �10-point increase frombaseline)*
1 mo 53.6 (96/179) 30.3 (54/178) 23.3 (13.3–33.3) �0.001 4.3 (3.0–7.5)
6 mo 53.1 (95/179) 23.0 (40/174) 30.1 (20.4–39.8) �0.001 3.3 (2.5–4.9)
12 mo 47.5 (85/179) 13.8 (24/174) 33.7 (24.7–42.7) �0.001 3.0 (2.3–4.0)
Excellent outcome (alive with �20-point increase frombaseline)*
1 mo 43.6 (78/179) 19.1 (34/178) 24.5 (15.1–33.8) �0.001 4.1 (3.0–6.6)
6 mo 45.3 (81/179) 16.1 (28/174) 29.2 (20.0–38.4) �0.001 3.4 (2.6–5.0)
12 mo 38.0 (68/179) 9.2 (16/174) 28.8 (20.4–37.2) �0.001 3.5 (2.7–4.9)
TAVR indicates transcatheter aortic valve replacement; NNT, number needed to treat; and CI, confidence interval.*Denominator includes patients who died but excludes patients who voluntarily withdrew from the study before the time point.
Reynolds et al Quality of Life After TAVR 1969
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from
care costs in heart failure patients.18,19 In our study, the meanbetween-group differences in the KCCQ summary score 6and 12 months after enrollment met or exceeded the 20-pointthreshold considered to signify a very large improvement inheart failure status, and �75% of surviving patients had atleast moderately large (10-point) improvements over base-line. Moreover, the proportion of patients who achieved anexcellent outcome at 12 months (defined as surviving with atleast a 20-point improvement in the KCCQ summary score)was far greater with TAVR than with standard care (absolutetreatment difference, 28%; number needed to treat, 3.5).
The minimally important difference in SF-12 summaryscales is �2 to 2.5 points.21,22 For both the physical andmental summary scales of the SF-12, the difference betweengroups at 6 and 12 months was roughly twice this threshold.The mental component summary scores did not differ be-tween groups at 1 month, but these scores were higher atbaseline in both groups than the physical summary scores.The magnitude of improvement in SF-12 physical scores with
TAVR is roughly equivalent to reversing by 10 years thenormal decline in physical health observed with aging in thegeneral population.23
We observed improvement from baseline in the controlgroup in both pairwise comparisons and categorical analy-ses—at least at 1 and 6 months. This improvement may havebeen due to a transient effect of balloon aortic valvulo-plasty,27,28 which was performed in the majority of controlgroup patients. Additional factors contributing to this increasemay have included enhanced medical attention related toclinical trial participation, regression to the mean, or placeboeffects (related to the valvuloplasty procedures).
Previous observational studies have shown that surgicalaortic valve replacement, even among octogenarians, cangreatly improve functional status and return quality-of-lifescores to age-adjusted norms.3,29 However, by design, suchstudies included only patients who were considered to beacceptable candidates for cardiac surgery. Recently, severalsmall studies have also demonstrated significant improve-
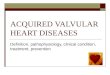
Figure 2. Estimated effect of transcatheteraortic valve replacement (TAVR) vs standardtherapy on the Kansas City CardiomyopathyQuestionnaire (KCCQ) overall summaryscore at 6 months (A) and 12 months (B)according to prespecified patient sub-groups. Treatment effects, associated 95%confidence intervals, and interaction P val-ues were derived from longitudinal growthcurve models. STS indicates Society ofThoracic Surgeons; AV, atrioventricular; andCOPD, chronic obstructive pulmonarydisease.
1970 Circulation November 1, 2011
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from

ment in health status after TAVR,30–33 but none of thesestudies included a parallel control group.
Given the advanced age and poor general health of thepatients enrolled in the PARTNER trial, it is important toestablish how TAVR, a relatively new procedure with distinctrisks and limitations, affects health status compared with thebest alternative therapy. Health-related quality-of-life endpoints are particularly relevant in this setting, given theincreased risks of both stroke and major vascular complica-tions that were observed with TAVR in the PARTNER trial.Our results suggest that despite multiple comorbid conditionsand advanced age, patients similar to those enrolled in thistrial can expect very meaningful improvements in symptoms,functional status, and quality of life after TAVR.
Our study has several limitations. Most important, theproportion of patients with available data diminished overtime as a result of deaths and nonresponses of survivingpatients, both of which were more common in the controlgroup. To supplement our primary analysis based on longi-tudinal growth curve models, we used several analytic ap-proaches to address the potential bias introduced by missingdata, including the imputation of “worst case” values tosurviving patients with missing data, the creation of categor-ical variables (“favorable” and “excellent” outcomes) thattreated missing data for any reason (including death) as“treatment failures, ” and comparisons of within-patientchanges from baseline at individual follow-up time pointsbased on patients with available quality-of-life measure-ments. Each of these supplemental analyses demonstratedbenefits of TAVR that were comparable to or in some caseslarger than those seen in our primary analysis. We thereforebelieve it is unlikely that the magnitude of differencesbetween groups seen in our primary analyses was overesti-mated as a result of biases caused by missing data.
The PARTNER trial was unblinded; therefore, we cannotexclude the possibility that some of the observed benefit ofTAVR was related to a placebo-like effect. However, it isnoteworthy that we also observed trends toward improvedquality of life in the standard therapy group, particularly inthe first 6 months, but these trends diminished by 12 months,whereas health status measures in the TAVR group continuedto improve.
These results encompass only 1 year of follow-up. Thus,the longer-term durability of the observed improvements inquality of life after TAVR remains unknown. Finally, thecurrent data are uninformative regarding how changes inquality of life after TAVR may compare with those aftersurgical aortic valve replacement in lower-risk patients. Thisis the subject of ongoing investigation.
ConclusionsFor patients with severe aortic stenosis who were not surgicalcandidates, TAVR resulted in marked improvements in healthstatus and quality of life compared with standard therapyover 1 year of follow-up. Taken together with previouslyreported benefits on both survival and rehospitalization,these findings further support the notion that TAVR shouldbe considered a valuable therapeutic option for patients
with severe aortic stenosis who are not candidates forvalve replacement surgery.
Sources of FundingThis work was supported by Edwards Lifesciences, Inc. (http://www.clinicaltrials.gov; unique identifier: NCT00530894).
DisclosuresDr Reynolds has received research support from Edwards Life-sciences, Biosense Webster, and Sanofi-aventis and consultingincome from Biosense Webster, Sanofi-aventis, and St. Jude Medi-cal. Dr Magnuson has received grant support from Eli Lilly, DaiichiSankyo, Sanofi-aventis, and Bristol-Myers Squibb. Dr Leon hasreceived consulting fees from Medtronic and has stock options inSadra Medical. Dr Webb has received research support from Ed-wards Lifesciences, Embrella Cardiovascular, Guided Delivery Sys-tems, and Siemens and consulting income from Edwards Life-sciences, Embrella Cardiovascular, Guided Delivery Systems,Philips, St. Jude Medical, Siemens, and Valtech Cardio. Dr Ba-baliaros has been a consultant for Symetis and Direct Flow Medical.Dr Bowers has received consulting fees or speaking honoraria fromCordis, St. Jude Medical, Lilly Pharmaceuticals, Daiichi-SanyoPharmaceuticals, Abbott Vascular, Medtronic, and Access Closure.Dr Fearon has received research support from the National Institutesof Health and St. Jude Medical and consulting fees from TrytonMedical. Dr Herrmann has received research support from EdwardsLifesciences, Abbott, St. Jude Medical, Gore, Johnson & Johnson,Boston Scientific, and Medtronic; speaking honoraria from EdwardsLifesciences and Schering Plough; and consulting fees from Gore,Merck, Astra-Zeneca; Dr Herrmann also has equity in Endovalve,Inc. Dr Kodali has received consulting income from EdwardsLifesciences, Medtronic, and theHeart.org. Dr Makkar has receivedconsulting fees, grant support, and lectures fees from Abbott,Medtronic, and Lilly; consulting fees and grant support fromJohnson & Johnson and Daiichi Sankyo; and grant support from St.Jude Medical and Edwards Lifesciences. Dr Pichard has receivedconsulting income from Edwards Lifesciences and speaking hono-raria from St. Jude Medical. Dr Cohen has received research supportfrom Edwards Lifesciences, Medtronic, Boston Scientific, AbbottVascular, MedRad, Merck/Schering-Plough, and Eli Lilly-DaiichiSankyo; consulting income from Schering-Plough, Eli Lilly,Medtronic, and Cordis; and speaking honoraria from Eli Lilly, TheMedicines Company, and St. Jude Medical. The other authors reportno conflicts.
References1. Ross J, Braunwald E. Aortic stenosis. Circulation. 1968;38:61–67.2. Davies SW, Gershlick AH, Balcon R. Progression of valvular aortic
stenosis: a long-term retrospective study. Eur Heart J. 1991;12:10–14.3. Sundt TM, Bailey MS, Moon MR, Mendeloff EN, Huddleston CB,
Pasque MK, Barner HB, Gay WA Jr. Quality of life after aortic valvereplacement at the age of �80 years. Circulation. 2000;102(suppl):III-70–III-74.
4. Schwarz F, Baumann P, Manthey J, Hoffmann M, Schuler G, MehmelHC, Schmitz W, Kubler W. The effect of aortic valve replacement onsurvival. Circulation. 1982;66:1105–1110.
5. Bach DS, Siao D, Girard SE, Duvernoy C, McCallister BD Jr, GualanoSK. Evaluation of patients with severe symptomatic aortic stenosis whodo not undergo aortic valve replacement: the potential role of subjectivelyoverestimated operative risk. Circ Cardiovasc Qual Outcomes. 2009;2:533–539.
6. Iung B, Cachier A, Baron G, Messika-Zeitoun D, Delahaye F, Tornos P,Gohlke-Barwolf C, Boersma E, Ravaud P, Vahanian A. Decision-makingin elderly patients with severe aortic stenosis: why are so many deniedsurgery? Eur Heart J. 2005;26:2714–2720.
7. Ben-Dor I, Pichard AD, Gonzalez MA, Weissman G, Li Y, Goldstein SA,Okubagzi P, Syed AI, Maluenda G, Collins SD, Delhaye C, WakabayashiK, Gaglia MA Jr, Torguson R, Xue Z, Satler LF, Suddath WO, Kent KM,Lindsay J, Waksman R. Correlates and causes of death in patients withsevere symptomatic aortic stenosis who are not eligible to participate in
Reynolds et al Quality of Life After TAVR 1971
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from

a clinical trial of transcatheter aortic valve implantation. Circulation.2010;122:S37–S42.
8. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG,Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC,Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS,Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S. Transcatheteraortic-valve implantation for aortic stenosis in patients who cannotundergo surgery. N Engl J Med. 2010;363:1597–1607.
9. Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F,Derumeaux G, Anselme F, Laborde F, Leon MB. Percutaneous transcath-eter implantation of an aortic valve prosthesis for calcific aortic stenosis:first human case description. Circulation. 2002;106:3006–3008.
10. Thomas M, Schymik G, Walther T, Himbert D, Lefevre T, Treede H,Eggebrecht H, Rubino P, Michev I, Lange R, Anderson WN, Wendler O.Thirty-day results of the Sapien aortic bioprosthesis European outcome(SOURCE) registry: a European registry of transcatheter aortic valveimplantation using the Edwards Sapien valve. Circulation. 2010;122:62–69.
11. Rodes-Cabau J, Webb JG, Cheung A, Ye J, Dumont E, Feindel CM,Osten M, Natarajan MK, Velianou JL, Martucci G, DeVarennes B,Chisholm R, Peterson MD, Lichtenstein SV, Nietlispach F, Doyle D,DeLarochelliere R, Teoh K, Chu V, Dancea A, Lachapelle K, Cheema A,Latter D, Horlick E. Transcatheter aortic valve implantation for thetreatment of severe symptomatic aortic stenosis in patients at very high orprohibitive surgical risk: acute and late outcomes of the multicenterCanadian experience. J Am Coll Cardiol. 2010;55:1080–1090.
12. Gurvitch R, Wood DA, Tay EL, Leipsic J, Ye J, Lichtenstein SV,Thompson CR, Carere RG, Wijesinghe N, Nietlispach F, Boone RH,Lauck S, Cheung A, Webb JG. Transcatheter aortic valve implantation:durability of clinical and hemodynamic outcomes beyond 3 years in alarge patient cohort. Circulation. 2010;122:1319–1327.
13. Lewis EF, Johnson PA, Johnson W, Collins C, Griffin L, Stevenson LW.Preferences for quality of life or survival expressed by patients with heartfailure. J Heart Lung Transplant. 2001;20:1016–1024.
14. Lazar HL. Transcatheter aortic valves: where do we go from here? N EnglJ Med. 2010;363:1667–1668.
15. Spertus JA, Tooley J, Jones P, et al. Expanding the outcomes in clinicaltrials of heart failure: the quality of life and economic components of theEPHESUS (EPlerenone’s neuroHormonal Efficacy and Survival Study).Am Heart J. 2002;143:636–642.
16. Green CP, Porter CB, Bresnahan DR, Spertus JA. Development andevaluation of the Kansas City Cardiomyopathy Questionnaire: a newhealth status measure for heart failure. J Am Coll Cardiol. 2000;35:1245–1255.
17. Spertus J, Peterson E, Conard MW, Heidenreich PA, Krumholz HM,Jones P, McCullough PA, Pina I, Tooley J, Weintraub WS, Rumsfeld JS.Monitoring clinical changes in patients with heart failure: a comparison ofmethods. Am Heart J. 2005;150:707–715.
18. Soto GE, Jones P, Weintraub WS, Krumholz HM, Spertus JA. Prognosticvalue of health status in patients with heart failure after acute myocardialinfarction. Circulation. 2004;110:546–551.
19. Chan PS, Soto G, Jones PG, Nallamothu BK, Zhang Z, Weintraub WS,Spertus JA. Patient health status and costs in heart failure: insights fromthe Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacyand Survival Study (EPHESUS). Circulation. 2009;119:398–407.
20. Ware J, Kosinski M, Keller SD. A 12-item short-form health survey:construction of scales and preliminary tests of reliability and validity.Med Care. 1996;34:220–233.
21. Wyrwich KW, Spertus JA, Kroenke K, Tierney WM, Babu AN,Wolinsky FD. Clinically important differences in health status for patientswith heart disease: an expert consensus panel report. Am Heart J. 2004;147:615–622.
22. Ware J, Kosinski M, Bjorner JB, Turner-Bowker DM, Gandek B,Maruish ME. Determining important differences in scores. User’sManual for the SF-36v2 Health Survey. Lincoln, RI: Quality Metric Inc;2007.
23. Ware JE Jr, Kosinski M, Turner-Bowker DM, Gandek B. How to ScoreVersion 2 of the SF-12 Health Survey (With a Supplement DocumentingVersion 1). Lincoln, RI: Quality Metric Incorporated; 2002.
24. Jennrich RI, Schluchter MD. Unbalanced repeated-measures models withstructured covariance matrices. Biometrics. 1986;42:805–820.
25. Rubin DB. Inference and missing data. Biometrika. 1976;63:581–592.26. Shroyer AL, Coombs LP, Peterson ED, Eiken MC, DeLong ER, Chen A,
Ferguson TB Jr, Grover FL, Edwards FH; Society of Thoracic Surgeons.The Society of Thoracic Surgeons: 30-day operative mortality and mor-bidity risk models. Ann Thorac Surg. 2003;75:1856–1864.
27. Dodek A, Hooper RO, Kiess M. Percutaneous balloon valvuloplasty foraortic stenosis: improved quality of life for elderly patients. CanJ Cardiol. 1988;4:223–227.
28. Feldman T. Proceedings of the TCT: balloon aortic valvuloplasty appro-priate for elderly valve patients. J Interv Cardiol. 2006;19:276–279.
29. Khan JH, McElhinney DB, Hall TS, Merrick SH. Cardiac valve surgeryin octogenarians: improving quality of life and functional status. ArchSurg. 1998;133:887–893.
30. Gotzmann M, Hehen T, Germing A, Lindstaedt M, Yazar A, LaczkovicsA, Mumme A, Mugge A, Bojara W. Short-term effects of transcatheteraortic valve implantation on neurohormonal activation, quality of life and6-minute walk test in severe and symptomatic aortic stenosis. Heart.2010;96:1102–1106.
31. Bekeredjian R, Krumsdorf U, Chorianopoulos E, Kallenbach K, Karck M,Katus HA, Rottbauer W. Usefulness of percutaneous aortic valve implan-tation to improve quality of life in patients �80 years of age. Am JCardiol. 2010;106:1777–1781.
32. Ussia GP, Mule M, Barbanti M, Cammalleri V, Scarabelli M, Imme S,Capodanno D, Ciriminna S, Tamburino C. Quality of life assessment afterpercutaneous aortic valve implantation. Eur Heart J. 2009;30:1790–1796.
33. Svensson LG, Dewey T, Kapadia S, Roselli EE, Stewart A, Williams M,Anderson WN, Brown D, Leon M, Lytle B, Moses J, Mack M, Tuzcu M,Smith C. United States feasibility study of transcatheter insertion of astented aortic valve by the left ventricular apex. Ann Thorac Surg.2008;86:46–54.
CLINICAL PERSPECTIVEMany patients with severe aortic stenosis do not undergo surgical valve replacement because of prohibitive operative risk.In a cohort of such patients, the Placement of Aortic Transcatheter Valves (PARTNER) trial recently showed thattranscatheter aortic valve replacement increased 12-month survival by an absolute margin of 20% but was associated withincreased risks of vascular complications and stroke compared with standard therapy, which included balloon aorticvalvuloplasty in the majority of subjects. In this trial, quality of life was assessed prospectively with the Kansas CityCardiomyopathy Questionnaire and the Short Form-12 General Health Survey. We found that the overall summary scoreof the Kansas City Cardiomyopathy Questionnaire, the primary quality-of-life end point, improved 20 to 30 points on a100-point scale 1, 6, and 12 months after transcatheter aortic valve replacement, whereas the improvement in the controlgroup was 10 to 12 points at 1 and 6 months and only 4 points at 12 months. Similar patterns were observed for the otherquality-of-life measures. Thus, during the first year after intervention, quality of life was substantially better in thetranscatheter aortic valve replacement group than in the control group in this clinical trial population.
Go to http://cme.ahajournals.org to take the CME quiz for this article.
1972 Circulation November 1, 2011
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from
InvestigatorsDavid J. Cohen and for the Placement of Aortic Transcatheter Valves (PARTNER) Howard C. Herrmann, Samir Kapadia, Susheel K. Kodali, Raj R. Makkar, Augusto D. Pichard,
G. Svensson, John G. Webb, Vasilis C. Babaliaros, Bruce S. Bowers, William F. Fearon, Matthew R. Reynolds, Elizabeth A. Magnuson, Yang Lei, Martin B. Leon, Craig R. Smith, Lars
Inoperable Patients With Severe Aortic StenosisHealth-Related Quality of Life After Transcatheter Aortic Valve Replacement in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2011 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.111.040022
2011;124:1964-1972; originally published online October 3, 2011;Circulation.
http://circ.ahajournals.org/content/124/18/1964World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on April 9, 2017
http://circ.ahajournals.org/D
ownloaded from