Embed Size (px)
Citation preview

Valvular heart diseaseValvular heart diseaseAortic Valve DiseasesAortic Valve Diseases
Dr. Hussam Al-FalehDr. Hussam Al-Faleh
Med 341 courseMed 341 course

Lecture outline Lecture outline
General principles : General principles : Pressure overload and volume overloadPressure overload and volume overload Heart murmursHeart murmurs Aortic valve diseaseAortic valve disease Mitral valve disease Mitral valve disease

VALVULAR STENOSISVALVULAR STENOSIS
Pressure in upstream chamber Pressure in upstream chamber IS HIGHER thanIS HIGHER than Pressure in downstream chamber Pressure in downstream chamber during time of during time of flowflow (when valve is normally open). (when valve is normally open).
Hemodynamic abnormality = "Hemodynamic abnormality = "PRESSURE GRADIENTPRESSURE GRADIENT""
Upstream Down stream
High pressure low pressure

VALVULAR REGURGITATIONVALVULAR REGURGITATION
Upstream Down stream
Volume overload
Retrograde flow of blood "upstream" during time when valve is normally closed. Hemodynamic abnormality = "VOLUME OVERLOAD"

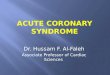
Left Ventricular HypertrophyLeft Ventricular Hypertrophy“Pressure and Volume overload”“Pressure and Volume overload”

LA
RV
RA
LV
VenaCava
AortaPulmArtery
PulmVein

RARA
RV LV
Aortic stenosis
LV
Normal

LA
RV
RA
LV
VenaCava
AortaPulmArtery
PulmVein
AorticInsufficiency

RARA
RV LV↑↑LV
Example: Aortic regurgitation


AI AS

Heart murmurs Heart murmurs

Produced by turbulent blood flowProduced by turbulent blood flow Turbulence is mainly determined by Turbulence is mainly determined by
velocity of blood flow across a structurevelocity of blood flow across a structure Timing of murmurs (either systolic, or Timing of murmurs (either systolic, or
diastolic) can give helpful information diastolic) can give helpful information regarding the valve lesion regarding the valve lesion

Systolic MurmursSystolic Murmurs Aortic stenosisAortic stenosis Mitral insufficiencyMitral insufficiency Mitral valve prolapseMitral valve prolapse Tricuspid insufficiency Tricuspid insufficiency
Diastolic MurmursDiastolic Murmurs Aortic insufficiencyAortic insufficiency Mitral stenosisMitral stenosis
S1 S2 S1
Common Murmurs and Timing

Outline for every valve lesionOutline for every valve lesion
EtiologyEtiology Pathphysiology Pathphysiology Symptoms and signsSymptoms and signs Natural historyNatural history Investigations Investigations ManagementManagement

Aortic stenosisAortic stenosis

EtiologyEtiology
Supra-ValvularSupra-Valvular Valvular Valvular - Congenital- Congenital - Acquired - Acquired Sub-ValvularSub-Valvular - Discreet - Discreet - Tubular- Tubular

Etiology Etiology
Valvular Valvular Congenital Congenital 1. Uni-cusped 1. Uni-cusped -- RareRare - Ages affected 2-30yrs- Ages affected 2-30yrs 2. Bi-cusped 2. Bi-cusped - 2% of the population- 2% of the population - More common in males- More common in males - Associated with coarctation- Associated with coarctation in 6% of patientsin 6% of patients - Ages affected 40-50yrs- Ages affected 40-50yrs


Etiology Etiology
Acquired Acquired 1. Rheumatic1. Rheumatic
- Adhesion and fusion of valve commissures leads to - Adhesion and fusion of valve commissures leads to
stiffening of the free borders as well as calcificationstiffening of the free borders as well as calcification
2. 2. Degenerative (senile)Degenerative (senile)
- Results from mechanical stress- Results from mechanical stress
- Associated with traditional risk factors for - Associated with traditional risk factors for
CAD such as HTN, Dyslipidemia and smoking CAD such as HTN, Dyslipidemia and smoking

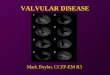
A. Normal Trileaflet AVB. Congenital ASC.Rheumatic ASD.Calcific ASE. Degenerative AS

PathphysiologyPathphysiology


SymptomsSymptoms
Cardinal symptoms:Cardinal symptoms: 1. Chest pain1. Chest pain - Occurs due to ↑ O2 demand- Occurs due to ↑ O2 demand (LV hypertrophy) and ↓ O2 delivery(LV hypertrophy) and ↓ O2 delivery - Is often related to concomitant CAD. - Is often related to concomitant CAD.
2. Presyncope/Syncope2. Presyncope/Syncope - Caused by transient ↓ cerebral blood flow- Caused by transient ↓ cerebral blood flow - May also be related transients VF or AF- May also be related transients VF or AF
3. Dyspnea3. Dyspnea
- Late manifestation of severe AS- Late manifestation of severe AS

SignsSigns Central Pulse :Central Pulse : - Slow rising , low- Slow rising , low volume ( Pulsus Parvus et tardus) volume ( Pulsus Parvus et tardus)
- Coarse systolic vibrations at Carotid artery (Carotid - Coarse systolic vibrations at Carotid artery (Carotid Shudder)Shudder)
JVP:JVP: - Prominent a wave- Prominent a wave Apex:Apex: - Sustained- Sustained - Systolic thrill - Systolic thrill - Displaced (late with LV failure) - Displaced (late with LV failure)

Slow rising pulseAortic pulse

Signs ( Auscultation)Signs ( Auscultation)
S2 may be soft and single S2 may be soft and single Paradoxical splitting of S2 in severe ASParadoxical splitting of S2 in severe AS
S1 S2
Inspiration
Expiration

Signs (Auscultation)Signs (Auscultation)
Aortic ejection sound with Bicuspid AVAortic ejection sound with Bicuspid AV S4 S4
S1EjectionClick S2
S2S4 S1

AuscultationAuscultation
S1 S2
Mild-Moderate
S1 S2
Severe

Natural history Natural history

InvestigationsInvestigations ECG ECG - LAD- LAD
- LVH- LVH

InvestigationsInvestigations
CXRCXR - Aortic Calcification- Aortic Calcification - Post stenotic dilation of Ascending Aorta- Post stenotic dilation of Ascending Aorta Echocardiography Echocardiography - Routinely used to diagnose and estimate the severity of - Routinely used to diagnose and estimate the severity of
ASAS - Peak and mean gradients are measured- Peak and mean gradients are measured - Valve area is measured- Valve area is measured Mild AS (area >1.5 cmMild AS (area >1.5 cm22)) Moderate (area >1.0 to 1.5 cmModerate (area >1.0 to 1.5 cm22)) Severe (area <1.0 cmSevere (area <1.0 cm22) )

ManagementManagement
No place for medical therapy if severe AS No place for medical therapy if severe AS is associated with symptoms.is associated with symptoms.
Surgery is the treatment of choice.Surgery is the treatment of choice. Generally speaking ,if the patient has Generally speaking ,if the patient has
symptoms with severe AS Surgery is symptoms with severe AS Surgery is indicated.indicated.

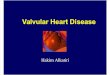
Aortic RegurgitationAortic Regurgitation

Etiology Etiology

Etiology (chronic AR)Etiology (chronic AR)
Two major causes:Two major causes: A. Intrinsic structural valve problemA. Intrinsic structural valve problem 1. Congenital : Bicuspid valve1. Congenital : Bicuspid valve
2. Acquired : - Inflammatory (Rheumatic,2. Acquired : - Inflammatory (Rheumatic,
Connective tissue diseases)Connective tissue diseases)
- Infectious (IE)- Infectious (IE)
- Degenerative - Degenerative

Etiology( chronic AR)Etiology( chronic AR)
B. Abnormality of the Ascending AortaB. Abnormality of the Ascending Aorta 1. Congenital : Marfans disease1. Congenital : Marfans disease
2. Infectious : Syphilis (15-25yr after infection)2. Infectious : Syphilis (15-25yr after infection)
3. Inflammatory : Connective tissue diseases3. Inflammatory : Connective tissue diseases
(RA, AS, GCA)(RA, AS, GCA)
4. Idiopathic : progressive dilation (cystic medial4. Idiopathic : progressive dilation (cystic medial
necrosis)necrosis)

Etiology (Acute AR)Etiology (Acute AR)
TraumaTrauma Aortic dissection Aortic dissection Infective endocarditisInfective endocarditis



Aortic regurgitation
Excess volume to the LV ↑LV end diastolic pressure
Stretching of Myocardium
↑ wall stress
Eccentric LV hypertrophy
↓ effective Stroke volume
↑ Myocardial O2 demand (Ischemia)
LV failure
↓ Myocardial O2 supply
(Ischemia)

Symptoms Symptoms
Gradual development of Dyspnea , Gradual development of Dyspnea , Orthopnea, and PNDOrthopnea, and PND
Angina Angina Palpitations Palpitations With Acute AR , abrupt development of With Acute AR , abrupt development of
dyspnea.dyspnea.

Signs of Chronic ARSigns of Chronic AR
Peripheral signsPeripheral signs - De Musset sign - De Musset sign (head movment with pulse)(head movment with pulse)
- Water hammer pulse- Water hammer pulse (abrupt distention and (abrupt distention and quick collapse)quick collapse)
- Duroziez sign - Duroziez sign - Muller’s sign - Muller’s sign (systolic pulsation of Uvula)(systolic pulsation of Uvula)
- Pistol shot/ Traube sign- Pistol shot/ Traube sign - Quincke sign- Quincke sign - Hill’s sign - Hill’s sign (Popliteal pressure at least 20 mmHg (Popliteal pressure at least 20 mmHg
higher than brachial pressure higher than brachial pressure

Signs of chronic ARSigns of chronic AR
Wide pulse pressureWide pulse pressure Central pulse:Central pulse:
- Large volume pulse- Large volume pulse
- Bisferines pulse- Bisferines pulse
- Corrigan pulse- Corrigan pulse JVP may be normal or elevatedJVP may be normal or elevated Displaced and hyperdynamic apexDisplaced and hyperdynamic apex

Auscultation Auscultation
S2 may be soft or accentuatedS2 may be soft or accentuated S3 indicates severe AIS3 indicates severe AI Ejection clickEjection click High pitched, blowing, decrescendo High pitched, blowing, decrescendo
diastolic murmur at LSB, best heard at diastolic murmur at LSB, best heard at end-expiration & leaning forwardend-expiration & leaning forward

AuscultationAuscultation
Length of murmur correlates with severity.Length of murmur correlates with severity. In Acute AR diastolic murmur is low pitched and In Acute AR diastolic murmur is low pitched and
short.short. Austin-Flint murmur indicates severity Austin-Flint murmur indicates severity (mid to late (mid to late
diastolic murmur)diastolic murmur) Systolic murmur related to high flow stateSystolic murmur related to high flow state
S1 S2 S1

InvestigationsInvestigations ECG – LVH, LADECG – LVH, LAD CXR- may show ↑cardiothoracic ratio, and CXR- may show ↑cardiothoracic ratio, and
dilated aortadilated aorta

Investigations Investigations
AngiographyAngiography: :
- Would aid in diagnosis and grading of - Would aid in diagnosis and grading of severityseverity
Echocardiography:Echocardiography:
- The easiest and fastest way of diagnosing- The easiest and fastest way of diagnosing
and grading the severity of AR.and grading the severity of AR.
- Detection of the underlying mechanism of - Detection of the underlying mechanism of AR.AR.

AsymptomaticAsymptomatic %/Y%/Y Normal LV function (~good prognosis)Normal LV function (~good prognosis)
Progression to symptoms or LV dysfunction Progression to symptoms or LV dysfunction < 6< 6 Progression to asymptomatic LV dysfunction Progression to asymptomatic LV dysfunction < 3.5< 3.5 Sudden death Sudden death < 0.2< 0.2
Abnormal LV functionAbnormal LV functionProgression to cardiac symptoms Progression to cardiac symptoms > 25> 25
SymptomaticSymptomatic (Poor prognosis) (Poor prognosis)
Mortality Mortality > 10> 10
Natural historyNatural history

Management Management
Any patient with severe AR and any of the Any patient with severe AR and any of the following should have aortic valve following should have aortic valve replacement:replacement:
1. Symptomatic patients1. Symptomatic patients
2. Patients without symptoms, but with 2. Patients without symptoms, but with
LV systolic dysfunction (EF<50%), orLV systolic dysfunction (EF<50%), or
marked dilation of the LV.marked dilation of the LV.

Management Management
Vasodilator therapy ( ACE I, or CCB’s) for:Vasodilator therapy ( ACE I, or CCB’s) for:
1. Patients not candidates for surgery1. Patients not candidates for surgery
2. Short term to Improve hemodynamics2. Short term to Improve hemodynamics
3. Treatment of hypertension 3. Treatment of hypertension