Embed Size (px)
DESCRIPTION
Â
Citation preview
Research www.AJOG.org
OBSTETRICS
Misoprostol to reduce intraoperative and postoperativehemorrhage during cesarean delivery: a systematicreview and metaanalysisAgustın Conde-Agudelo, MD, MPH, PhD; Anıbal Nieto, MD, PhD; Anyeli Rosas-Bermudez, BA;Roberto Romero, MD, DMedSci
OBJECTIVE: To evaluate the efficacy and safety of prophylactic (relative risk, 0.33; 95% confidence interval, 0.18e0.62). Compared
misoprostol use at cesarean delivery for reducing intraoperative andpostoperative hemorrhage.STUDY DESIGN: Systematic review and metaanalysis of randomizedcontrolled trials.
RESULTS: Seventeen studies (3174 women) were included of which 7evaluated misoprostol vs oxytocin and 8 evaluated misoprostol plusoxytocin vs oxytocin alone. Overall, there were no significant differ-ences in intraoperative and postoperative hemorrhage between sub-lingual or oral misoprostol and oxytocin. Rectal misoprostol, comparedwith oxytocin, was associated with a significant reduction in intra-operative and postoperative hemorrhage. The combined use of sub-lingual misoprostol and oxytocin, compared with the use of oxytocinalone, was associated with a significant reduction in the meandecrease in hematocrit (mean difference, e2.1%; 95% confidenceinterval, e3.4 to e0.8) and use of additional uterotonic agents
From the Perinatology Research Branch, Eunice Kennedy Shriver National InHealth and Human Development, National Institutes of Health, Department oServices, Bethesda, MD, and Detroit, MI (Drs Conde-Agudelo and Romero);Obstetrics and Gynecology, Universidad de Murcia, Murcia, Spain (Dr Nieto)Organization Collaborating Center in Human Reproduction, Universidad del(Dr Rosas-Bermudez).
Received Jan. 10, 2013; revised Feb. 26, 2013; accepted March 13, 2013.
This research was supported, in part, by the Intramural Research Program, ENational Institute of Child Health and Human Development, National Institutesof Health and Human Services.
The authors report no conflict of interest.
Reprints not available from the authors.
0002-9378/$36.00 � ª 2013 Mosby, Inc. All rights reserved. � http://dx.doi.org/10.1
40.e1 American Journal of Obstetrics & Gynecology JULY 2013
with oxytocin alone, buccal misoprostol plus oxytocin reduced the useof additional uterotonic agents; rectal misoprostol plus oxytocindecreased intraoperative and postoperative blood loss, mean fall inhematocrit, and use of additional uterotonic agents; and intrauterinemisoprostol plus oxytocin reduced the mean fall in hemoglobin andhematocrit. Women receiving misoprostol, alone or combined withoxytocin, had a higher risk of shivering and pyrexia.
CONCLUSION:Misoprostol combined with oxytocin appears to be moreeffective than oxytocin alone in reducing intraoperative and post-operative hemorrhage during cesarean section. There were no sig-nificant differences in intraoperative and postoperative hemorrhagewhen misoprostol was compared to oxytocin. However, these findingswere based on a few trials with methodological limitations.
Key words: blood loss, oxytocin, postpartum hemorrhage, pregnancy,uterotonics
Cite this article as: Conde-Agudelo A, Nieto A, Rosas-Bermudez A, et al. Misoprostol to reduce intraoperative and postoperative hemorrhage during cesarean delivery:a systematic review and metaanalysis. Am J Obstet Gynecol 2013;209:40.e1-17.
esarean delivery is the most com-
C mon major surgical procedureperformed on women worldwide and itsrates continue to rise steadily in bothdeveloped and developing countries.1-8In 2007, the global cesarean deliveryrate was estimated to be 15%.9 Postpar-tum hemorrhage is a major contributor
to maternal mortality, mainly in devel-oping countries.10 Recent studies fromdeveloped countries report an increasein the rate of postpartum hemorrhage,which has been attributed (at least inpart) to a rise in the rate of cesareandelivery.11-14 Large population- andhospital-based cohort studies have
stitute of Childf Health and Humanthe Department of; and World HealthValle, Cali, Colombia
unice Kennedy Shriverof Health, Department
016/j.ajog.2013.03.015
attributed this to uterine atony aftervaginal or cesarean deliveries.11,13,14
Cesarean delivery, often performedbecause of “dystocia,” may predispose apatient to uterine atony. This has beentraditionally attributed to either myo-metrial fatigue or impaired contractilityat the site of the uterine incision.
Postpartum hemorrhage following acesarean delivery has been defined asblood loss>1000 mL,15 based on a studyfrom the early 1960s.16 Recent studieshave estimated that the prevalence ofpostpartum hemorrhage after cesareandelivery ranges from 0.6e6.4% (median,3%), although the frequency depends onthe criteria used to define this conditionand the method used to calculate bloodloss.17-26
The efficacy of routine administrationof uterotonic agents, mainly oxytocin,to reduce the frequency of postpartumhemorrhage after vaginal birth is well

www.AJOG.org Obstetrics Research
established.27 It has been assumed thatthe benefits of injectable uterotonicagents observed for vaginal births alsoapply to cesarean deliveries; yet, this hasnot been rigorously demonstrated. Anupdated guideline of the Royal Collegeof Obstetricians and Gynecologists oncesarean delivery recommends a slowintravenous bolus dose of 5 IU ofoxytocin after delivery of the neonate toensure adequate uterine contractility,minimize delay in the delivery of theplacenta, reduce intraoperative bloodloss, and prevent postpartum hemor-rhage.28 In contrast, in the UnitedStates, the practice is to use an oxytocininfusion instead of a bolus dose.29
Regardless of the mode of administra-tion, oxytocin use in the setting ofcesarean delivery may result in maternaladverse effects, such as hypotension andtachycardia.30
Misoprostol, a prostaglandin E1 ana-logue with strong uterotonic properties,has been suggested as an alternativeto injectable uterotonic agents for pre-venting postpartum hemorrhage fol-lowing vaginal or cesarean deliveries. Arecent Cochrane review found that oralmisoprostol was associated with a higherrisk of severe postpartum hemorrhageand use of additional uterotonics aftervaginal birth when compared to con-ventional uterotonic agents.31 However,oral or sublingual misoprostol wasfound to be more effective than placeboin reducing severe postpartum hemor-rhage and blood transfusion after vaginalbirth. The use of misoprostol duringcesarean delivery to prevent hemorrhageattributable to uterine atony has receivedless attention and its effectiveness hasnot been systematically evaluated.
We conducted a systematic reviewand metaanalysis of all available ran-domized controlled trials (RCTs) toassess the efficacy and safety of prophy-lactic misoprostol use at cesarean de-livery for reducing intraoperative andpostoperative hemorrhage.
MATERIALS AND METHODS
The study was conducted using a pro-spectively prepared protocol, and isreported using the Preferred ReportingItems for Systematic Reviews and
Metaanalyses (PRISMA) guidelines formetaanalyses of RCTs.32
Data sources and searchesWe searched Medline, Embase, Cinahl,and Lilacs (all from inception throughMarch 31, 2013); the CochraneCentral Register of Controlled Trials(http://www.mrw.interscience.wiley.com/cochrane/cochrane_clcentral_articles_fs.html) (1960 through March 31, 2013);ISI Web of Science (http://www.isiknowledge.com) (1960 through March31, 2013); research registers of ongoingtrials (http://www.clinicaltrials.gov, http://www.controlled-trials.com, http://www.centerwatch.com, http://www.anzctr.org.au, http://www.nihr.ac.uk, and http://www.umin.ac.jp/ctr); and Google Scholarusing a combination of key words and textwords related to misoprostol, cesareandelivery, and hemorrhage. Congress pro-ceedings of international society meetingsof maternal-fetal and reproductive medi-cine and international meetings on post-partum hemorrhage or cesarean delivery,reference lists of identified studies, text-books, previously published systematicreviews, and review articles were alsosearched. Experts in the field were con-tacted to identify further studies. No lan-guage restriction was applied.
Study selectionWe included RCTs in which misoprostol(alone or in combination) was usedto reduce perioperative hemorrhage inwomen undergoing cesarean deliverycompared with either another utero-tonic agent or placebo/no uterotonicagent. Studies were included irrespectiveof women’s risk status for postpartumhemorrhage, dose, and route of admin-istration. Trials were excluded if theywere quasirandomized or if they evalu-ated only the effect of misoprostol onintestinal motility after cesarean delivery.Published abstracts alone were excludedif additional information on methodo-logical issues and results could not beobtained.Two investigators (A.C-A. and A.N.)
independently reviewed all potentiallyrelevant articles for eligibility. Disagree-ments regarding trial eligibility wereresolved by consensus.
JULY 2013 Ame
Outcome measuresThe prespecified primary outcome mea-sures were the mean intraoperativeand postoperative blood loss, and themean decrease in hemoglobin andhematocrit (difference between preop-erative and postoperative levels). Inaddition, we also chose the use of addi-tional uterotonic agents as a primaryoutcome because obstetricians are likelyto intervene (when uterine atony doesnot respond to therapy) by employingadditional agents. Secondary outcomemeasures included blood loss >500 and>1000 mL, blood transfusion, meanpostoperative hemoglobin and hemato-crit, shivering, pyrexia (�38�C), nausea,vomiting, diarrhea, abdominal pain,headache, any side effect, neonatal out-comes, and costs.
Assessment of risk of biasWe assessed the risk of bias using thecriteria outlined in the CochraneHandbook for Systematic Reviews ofInterventions.33 Seven domains relatedto risk of bias were assessed in eachtrial since there is evidence that theseissues are associated with biased esti-mates of treatment effect: (1) randomsequence generation; (2) allocationconcealment; (3) blinding of participantsand personnel; (4) blinding of outcomeassessment; (5) incomplete outcomedata; (6) selective reporting; and (7)other bias. The assessments were classi-fied as “low,” “high,” or “unclear” risk ofbias. In addition, we evaluated the tech-nique of assessment of blood loss used ineach study and classified it as objective,subjective, unmeasured, or unreported.The risk of bias in each trial includedwas assessed individually by 2 reviewers(A.C-A. and A.N.). Any differences ofopinion regarding assessment of risk ofbias were resolved by discussion.
Data extractionTwo reviewers (A.C-A. and A.N.) inde-pendently extracted data from eacheligible study using a standardized dataabstraction form. There was no blindingof authorship. From each article, re-viewers extracted data on participants(inclusion and exclusion criteria, num-ber of women randomized, baseline
rican Journal of Obstetrics & Gynecology 40.e2

Research Obstetrics www.AJOG.org
characteristics, and country and dateof recruitment); study characteristics(randomization procedure, concealmentallocation method, blinding of clini-cians, women and outcome assessors,completeness of outcome data for eachoutcomeeincluding attrition and ex-clusions from analysis, intention-to-treat analysis, anesthesia used, andmethod of assessment of blood lossused); details of interventions (aim,loading and maintenance dose, route,duration of treatment, and use of alter-native uterotonic agents); and outcomes(definitions used, number of outcomeevents/total number, and mean� SD foreach outcome). In an attempt to obtainadditional data, we contacted 7 authorsby e-mail of whom 2 responded. Dis-agreements in extracted data wereresolved by discussion among reviewers.
Statistical analysisAll statistical analyses were performedaccording to the guidelines of theCochrane Collaboration.34 We analyzedoutcomes on an intention-to-treat basis.If this was not clear from the originalarticle, we then carried out a reanalysiswhen possible. If we found no evidenceof a substantial difference in studypopulations, interventions, or outcomemeasurements, we performed a meta-analysis. For dichotomous data, wecalculated the summary relative risk(RR) with 95% confidence interval (CI).For continuous data, we used the meandifference if outcomes were measuredin the same way among trials, or stan-dardized mean difference if the sameoutcome was measured in a varietyof ways, with 95% CI. Analyses werestratified by route of misoprostol ad-ministration, irrespective of dose used,as follows: sublingual, oral, buccal, rectal,and intrauterine. Further subgroupanalyses were planned to assess primaryoutcomes according to risk statusfor intraoperative/postoperative hemor-rhage, gestational age at cesareandelivery,type of anesthesia, whether the cesareandelivery was unplanned, method ofassessment of blood loss, and dose ofmisoprostol but these analyses were notundertaken due to the small number oftrials included in each comparison.
40.e3 American Journal of Obstetrics & Gynecolo
Heterogeneity of the results amongstudies was tested with the quantity I2,which describes the percentage of totalvariation across studies that is due toheterogeneity rather than chance.35 Avalue of 0% indicates no observed het-erogeneity, whereas I2 values of �50%indicate a substantial level of heteroge-neity. A fixed effects model was used ifsubstantial statistical heterogeneity wasnot detected. If there was substantialstatistical heterogeneity, a random ef-fects model was used to pool data acrossstudies if causes of heterogeneity couldnot be determined and the averagetreatment effect was considered clini-cally meaningful. One of the mostimportant sources of bias in the conductof clinical trials evaluating the efficacyof misoprostol to reduce hemorrhageat cesareandelivery is the lackof blinding,which is likely to influence the mea-surement of intraoperative and post-operative blood loss and use of additionaluterotonic agents. We performed a pre-defined sensitivity analysis to explore theimpact of study quality on the effect sizefor the primary outcomes by includingonly trials with adequate concealmentallocation that were double-masked.Thenumberneeded to treat (NNT) for
benefit or harm with 95% CI was calcu-lated for the outcomes for which therewas a statistically significant reduction orincrease in risk difference based on con-trol event rates in the included trials.36
We planned to assess publication andrelated biases,37 but this was not per-formedbecause of paucity of trials in eachcomparison. Analyses were performedwith the Review Manager (RevMan),version 5.1.7 (Nordic Cochrane Centre,Copenhagen, Denmark).
RESULTS
Study selection, details, and qualityThe searches yielded 1899 citations, ofwhich 26 were considered to be poten-tially eligible (Figure 1). Nine studieswere excluded. Three of these studiesevaluated only the effect of misoprostolon intestinal motility after cesareandelivery, 3 provided very little informa-tion on the methodology, 2 were non-RCTs, and the remainder was availableonly in abstract form with insufficient
gy JULY 2013
information on methods and results.The list of studies excluded is availablefrom the authors upon request. Seven-teen studies,38-54 including 3174 women,fulfilled the inclusion criteria of which7 evaluated misoprostol vs oxytocin(n ¼ 700),39,40,42,45,47,49,54 one evaluatedmisoprostol vs ergometrine (n¼ 374),51
8 evaluated misoprostol plus oxytocin vsoxytocin (n ¼ 1918),41,43,44,46,48,50,52,53
and one 3-arm trial evaluated miso-prostol vs oxytocin vs misoprostol plusoxytocin (n ¼ 182).38
The main characteristics of studiesincluded in the review are shown inTable 1. Thirteen trials were conductedin developing countries (3 in India,2 in Egypt, and 1 each in China, Iran,Thailand, Pakistan, Nigeria, Tunisia,Mexico, and Ecuador), 2 in the UnitedKingdom, and 1 each in the UnitedStates and Switzerland. Seven studiesincluded women undergoing electivecesarean delivery and 10 includedwomen undergoing both elective andemergency cesarean delivery. Regionalanesthesia was used in 15 studies andgeneral anesthesia in 2 studies. Twelvestudies excluded women with any riskfactors associated with an increased riskof intraoperative or postoperative hem-orrhage, 3 excluded women with somerisk factors, and 4 did not report onexclusion criteria. The sample sizeranged from 40e400 (median, 174). Ofthe 17 trials included in the review, 8evaluated misoprostol using the sublin-gual route, 4 using the oral route, 3 usingthe rectal route, and 1 each used buccaland intrauterine routes in doses of200 mg (2 studies), 400 mg (9 studies),500 mg (1 study), 600 mg (1 study), and800 mg (4 studies). The most commondose used in studies evaluating the sub-lingual route was 400 mg, and 800 mg instudies that evaluated the rectal and in-trauterine routes. Misoprostol was usedafter delivery of the neonate in 12 studiesand before delivery of the neonate in 5studies (orally38 or rectally47 at the timeof peritoneal incision, rectally just beforeonset of cesarean section51 or after uri-nary catheter placement,52 and sub-lingually after tracheal intubation53). Itshould be noted that in 7 studies thatcompared misoprostol with placebo, all
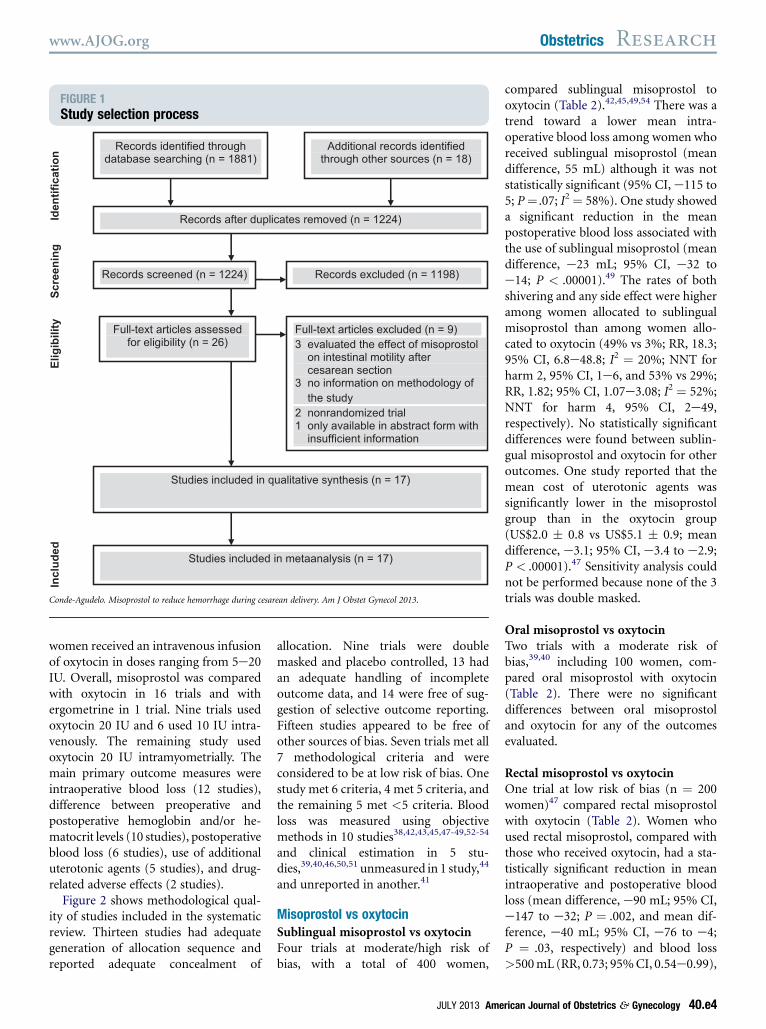
FIGURE 1Study selection process
Records identified through database searching (n = 1881)
Additional records identified through other sources (n = 18)
Records after duplicates removed (n = 1224)
Records screened (n = 1224) Records excluded (n = 1198)
Full-text articles assessed for eligibility (n = 26)
Studies included in qualitative synthesis (n = 17)
Full-text articles excluded (n = 9) 3 evaluated the effect of misoprostol on intestinal motility after cesarean section 3 no information on methodology of the study 2 nonrandomized trial 1 only available in abstract form with insufficient information
Studies included in metaanalysis (n = 17)
Id
en
tificatio
nS
cre
en
in
gE
lig
ib
ility
In
clu
de
d
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013.
www.AJOG.org Obstetrics Research
women received an intravenous infusionof oxytocin in doses ranging from 5e20IU. Overall, misoprostol was comparedwith oxytocin in 16 trials and withergometrine in 1 trial. Nine trials usedoxytocin 20 IU and 6 used 10 IU intra-venously. The remaining study usedoxytocin 20 IU intramyometrially. Themain primary outcome measures wereintraoperative blood loss (12 studies),difference between preoperative andpostoperative hemoglobin and/or he-matocrit levels (10 studies), postoperativeblood loss (6 studies), use of additionaluterotonic agents (5 studies), and drug-related adverse effects (2 studies).
Figure 2 shows methodological qual-ity of studies included in the systematicreview. Thirteen studies had adequategeneration of allocation sequence andreported adequate concealment of
allocation. Nine trials were doublemasked and placebo controlled, 13 hadan adequate handling of incompleteoutcome data, and 14 were free of sug-gestion of selective outcome reporting.Fifteen studies appeared to be free ofother sources of bias. Seven trials met all7 methodological criteria and wereconsidered to be at low risk of bias. Onestudy met 6 criteria, 4 met 5 criteria, andthe remaining 5 met <5 criteria. Bloodloss was measured using objectivemethods in 10 studies38,42,43,45,47-49,52-54
and clinical estimation in 5 stu-dies,39,40,46,50,51 unmeasured in 1 study,44
and unreported in another.41
Misoprostol vs oxytocinSublingual misoprostol vs oxytocinFour trials at moderate/high risk ofbias, with a total of 400 women,
JULY 2013 Ame
compared sublingual misoprostol tooxytocin (Table 2).42,45,49,54 There was atrend toward a lower mean intra-operative blood loss among women whoreceived sublingual misoprostol (meandifference, 55 mL) although it was notstatistically significant (95% CI, e115 to5; P¼ .07; I2¼ 58%). One study showeda significant reduction in the meanpostoperative blood loss associated withthe use of sublingual misoprostol (meandifference, e23 mL; 95% CI, e32 toe14; P < .00001).49 The rates of bothshivering and any side effect were higheramong women allocated to sublingualmisoprostol than among women allo-cated to oxytocin (49% vs 3%; RR, 18.3;95% CI, 6.8e48.8; I2 ¼ 20%; NNT forharm 2, 95% CI, 1e6, and 53% vs 29%;RR, 1.82; 95% CI, 1.07e3.08; I2 ¼ 52%;NNT for harm 4, 95% CI, 2e49,respectively). No statistically significantdifferences were found between sublin-gual misoprostol and oxytocin for otheroutcomes. One study reported that themean cost of uterotonic agents wassignificantly lower in the misoprostolgroup than in the oxytocin group(US$2.0 � 0.8 vs US$5.1 � 0.9; meandifference, e3.1; 95% CI, e3.4 to e2.9;P < .00001).47 Sensitivity analysis couldnot be performed because none of the 3trials was double masked.
Oral misoprostol vs oxytocinTwo trials with a moderate risk ofbias,39,40 including 100 women, com-pared oral misoprostol with oxytocin(Table 2). There were no significantdifferences between oral misoprostoland oxytocin for any of the outcomesevaluated.
Rectal misoprostol vs oxytocinOne trial at low risk of bias (n ¼ 200women)47 compared rectal misoprostolwith oxytocin (Table 2). Women whoused rectal misoprostol, compared withthose who received oxytocin, had a sta-tistically significant reduction in meanintraoperative and postoperative bloodloss (mean difference, e90 mL; 95% CI,e147 to e32; P ¼ .002, and mean dif-ference, e40 mL; 95% CI, e76 to e4;P ¼ .03, respectively) and blood loss>500mL (RR, 0.73; 95%CI, 0.54e0.99),
rican Journal of Obstetrics & Gynecology 40.e4
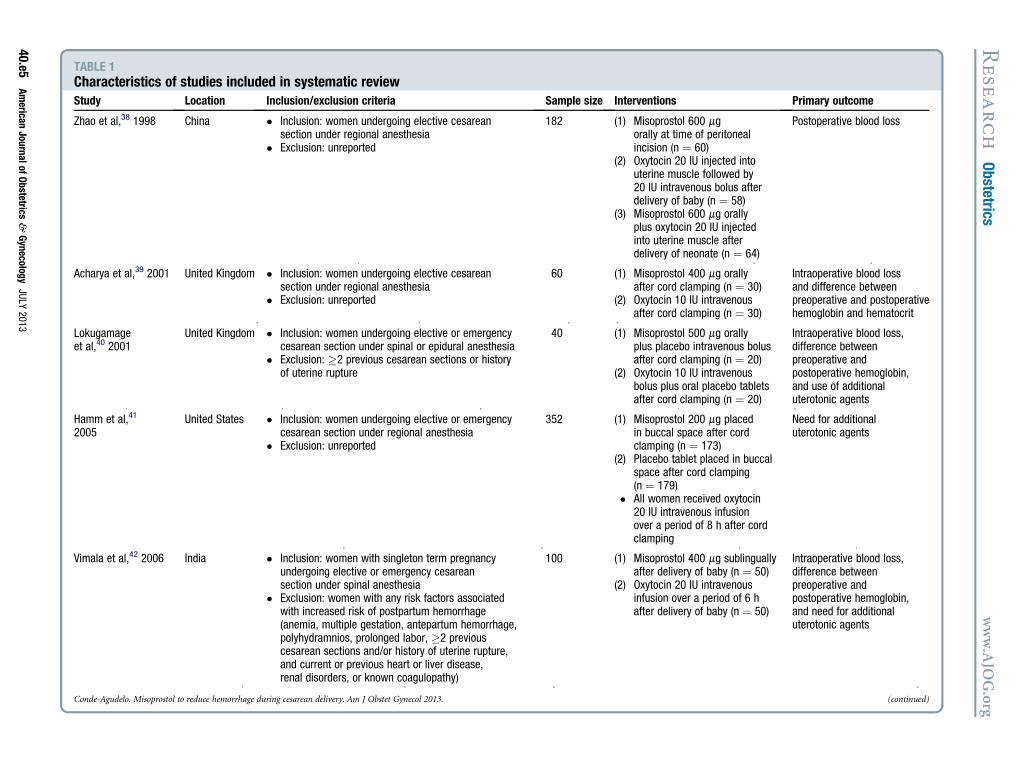
TABLE 1Characteristics of studies included in systematic reviewStudy Location Inclusion/exclusion criteria Sample size Interventions Primary outcome
Zhao et al,38 1998 China � Inclusion: women undergoing elective cesareansection under regional anesthesia
� Exclusion: unreported
182 (1) Misoprostol 600orally at time of p itonealincision (n ¼ 60)
(2) Oxytocin 20 IU in ted intouterine muscle fo wed by20 IU intravenous lus afterdelivery of baby ( 58)
(3) Misoprostol 600 orallyplus oxytocin 20 injectedinto uterine musc afterdelivery of neona (n ¼ 64)
Postoperative blood loss
Acharya et al,39 2001 United Kingdom � Inclusion: women undergoing elective cesareansection under regional anesthesia
� Exclusion: unreported
60 (1) Misoprostol 400 orallyafter cord clampi (n ¼ 30)
(2) Oxytocin 10 IU in venousafter cord clampi (n ¼ 30)
Intraoperative blood lossand difference betweenpreoperative and postoperativehemoglobin and hematocrit
Lokugamageet al,40 2001
United Kingdom � Inclusion: women undergoing elective or emergencycesarean section under spinal or epidural anesthesia
� Exclusion: �2 previous cesarean sections or historyof uterine rupture
40 (1) Misoprostol 500 orallyplus placebo intra nous bolusafter cord clampi (n ¼ 20)
(2) Oxytocin 10 IU in venousbolus plus oral pl bo tabletsafter cord clampi (n ¼ 20)
Intraoperative blood loss,difference betweenpreoperative andpostoperative hemoglobin,and use of additionaluterotonic agents
Hamm et al,41
2005United States � Inclusion: women undergoing elective or emergency
cesarean section under regional anesthesia� Exclusion: unreported
352 (1) Misoprostol 200 placedin buccal space a r cordclamping (n ¼ 17
(2) Placebo tablet pl d in buccalspace after cord mping(n ¼ 179)
� All women receiv oxytocin20 IU intravenous fusionover a period of 8 after cordclamping
Need for additionaluterotonic agents
Vimala et al,42 2006 India � Inclusion: women with singleton term pregnancyundergoing elective or emergency cesareansection under spinal anesthesia
� Exclusion: women with any risk factors associatedwith increased risk of postpartum hemorrhage(anemia, multiple gestation, antepartum hemorrhage,polyhydramnios, prolonged labor, �2 previouscesarean sections and/or history of uterine rupture,and current or previous heart or liver disease,renal disorders, or known coagulopathy)
100 (1) Misoprostol 400 sublinguallyafter delivery of b y (n ¼ 50)
(2) Oxytocin 20 IU in venousinfusion over a p d of 6 hafter delivery of b y (n ¼ 50)
Intraoperative blood loss,difference betweenpreoperative andpostoperative hemoglobin,and need for additionaluterotonic agents
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013. (continued)
Resea
rch
Obstetrics
www.AJO
G.org
40.e5American
JournalofObstetrics
&Gynecology
JULY
2013
mger
jecllobon ¼mgIUlete
mgngtrang
mgvengtraaceng
mgfte3)acecla
edinh
mgabtraerioab
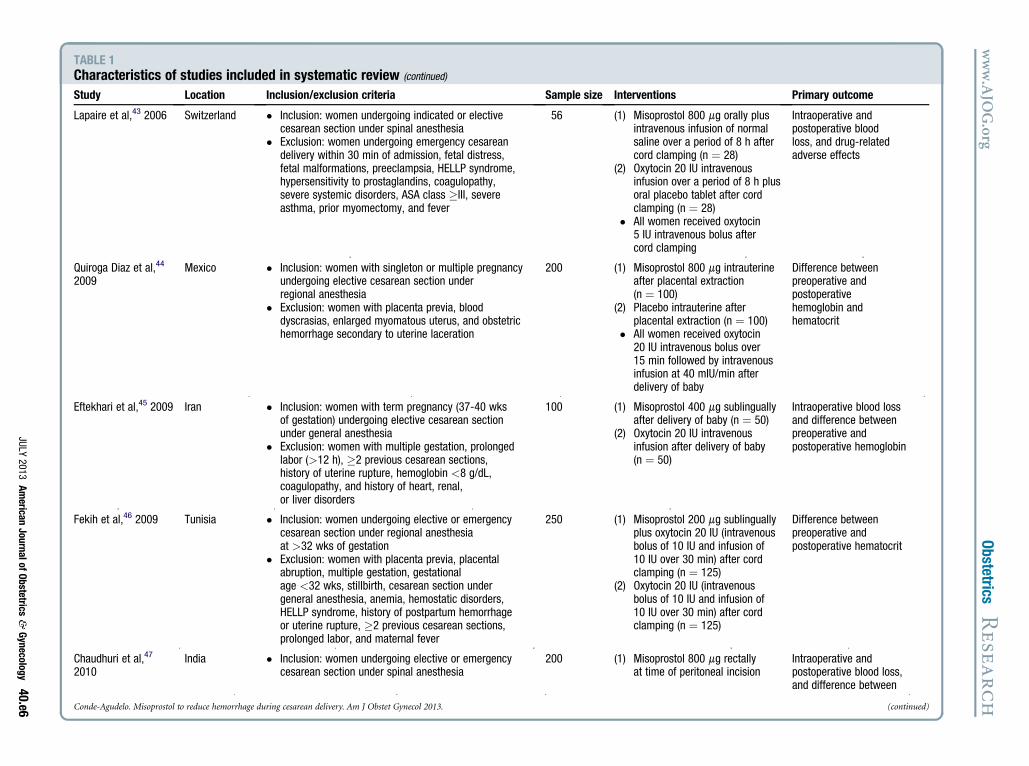
TABLE 1Characteristics of studies included in systematic review (continued)
Study Location Inclusion/exclusion criteria Sample size Interventions Primary outcome
Lapaire et al,43 2006 Switzerland � Inclusion: women undergoing indicated or electivecesarean section under spinal anesthesia
� Exclusion: women undergoing emergency cesareandelivery within 30 min of admission, fetal distress,fetal malformations, preeclampsia, HELLP syndrome,hypersensitivity to prostaglandins, coagulopathy,severe systemic disorders, ASA class �III, severeasthma, prior myomectomy, and fever
56 (1) Misoprostol 800 mg orally plusintravenous infusion of normalsaline over a period of 8 h aftercord clamping (n ¼ 28)
(2) Oxytocin 20 IU intravenousinfusion over a period of 8 h plusoral placebo tablet after cordclamping (n ¼ 28)
� All women received oxytocin5 IU intravenous bolus aftercord clamping
Intraoperative andpostoperative bloodloss, and drug-relatedadverse effects
Quiroga Diaz et al,44
2009Mexico � Inclusion: women with singleton or multiple pregnancy
undergoing elective cesarean section underregional anesthesia
� Exclusion: women with placenta previa, blooddyscrasias, enlarged myomatous uterus, and obstetrichemorrhage secondary to uterine laceration
200 (1) Misoprostol 800 mg intrauterineafter placental extraction(n ¼ 100)
(2) Placebo intrauterine afterplacental extraction (n ¼ 100)
� All women received oxytocin20 IU intravenous bolus over15 min followed by intravenousinfusion at 40 mIU/min afterdelivery of baby
Difference betweenpreoperative andpostoperativehemoglobin andhematocrit
Eftekhari et al,45 2009 Iran � Inclusion: women with term pregnancy (37-40 wksof gestation) undergoing elective cesarean sectionunder general anesthesia
� Exclusion: women with multiple gestation, prolongedlabor (>12 h), �2 previous cesarean sections,history of uterine rupture, hemoglobin <8 g/dL,coagulopathy, and history of heart, renal,or liver disorders
100 (1) Misoprostol 400 mg sublinguallyafter delivery of baby (n ¼ 50)
(2) Oxytocin 20 IU intravenousinfusion after delivery of baby(n ¼ 50)
Intraoperative blood lossand difference betweenpreoperative andpostoperative hemoglobin
Fekih et al,46 2009 Tunisia � Inclusion: women undergoing elective or emergencycesarean section under regional anesthesiaat >32 wks of gestation
� Exclusion: women with placenta previa, placentalabruption, multiple gestation, gestationalage <32 wks, stillbirth, cesarean section undergeneral anesthesia, anemia, hemostatic disorders,HELLP syndrome, history of postpartum hemorrhageor uterine rupture, �2 previous cesarean sections,prolonged labor, and maternal fever
250 (1) Misoprostol 200 mg sublinguallyplus oxytocin 20 IU (intravenousbolus of 10 IU and infusion of10 IU over 30 min) after cordclamping (n ¼ 125)
(2) Oxytocin 20 IU (intravenousbolus of 10 IU and infusion of10 IU over 30 min) after cordclamping (n ¼ 125)
Difference betweenpreoperative andpostoperative hematocrit
Chaudhuri et al,47
2010India � Inclusion: women undergoing elective or emergency
cesarean section under spinal anesthesia200 (1) Misoprostol 800 mg rectally
at time of peritoneal incisionIntraoperative andpostoperative blood loss,and difference between
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013. (continued)
www.AJO
G.org
Obstetrics
Resea
rch
JULY
2013American
JournalofObstetrics
&Gynecology
40.e6
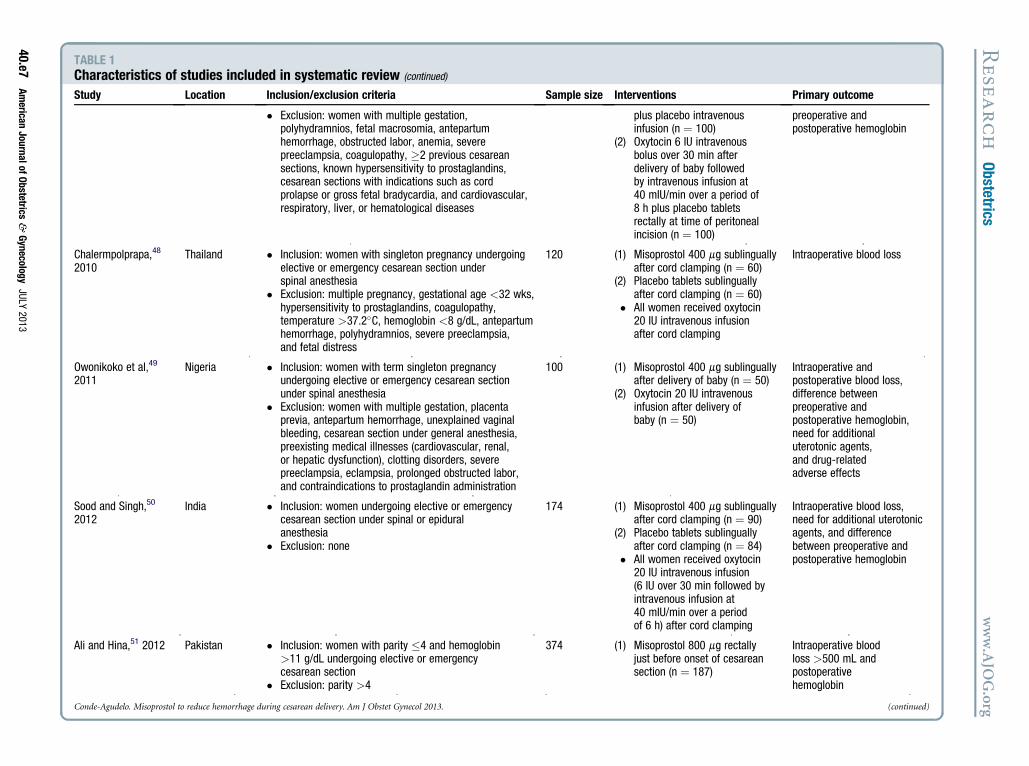
TABLE 1Characteristics of studies included in systematic review (continued)
Study Location Inclusion/exclusion criteria Sample size Interventions Primary outcome
� Exclusion: women with multiple gestation,polyhydramnios, fetal macrosomia, antepartumhemorrhage, obstructed labor, anemia, severepreeclampsia, coagulopathy, �2 previous cesareansections, known hypersensitivity to prostaglandins,cesarean sections with indications such as cordprolapse or gross fetal bradycardia, and cardiovascular,respiratory, liver, or hematological diseases
plus placebo intravenousinfusion (n ¼ 100)
(2) Oxytocin 6 IU intravenousbolus over 30 min afterdelivery of baby followedby intravenous infusion at40 mIU/min over a period of8 h plus placebo tabletsrectally at time of peritonealincision (n ¼ 100)
preoperative andpostoperative hemoglobin
Chalermpolprapa,48
2010Thailand � Inclusion: women with singleton pregnancy undergoing
elective or emergency cesarean section underspinal anesthesia
� Exclusion: multiple pregnancy, gestational age <32 wks,hypersensitivity to prostaglandins, coagulopathy,temperature >37.2�C, hemoglobin <8 g/dL, antepartumhemorrhage, polyhydramnios, severe preeclampsia,and fetal distress
120 (1) Misoprostol 400 mg sublinguallyafter cord clamping (n ¼ 60)
(2) Placebo tablets sublinguallyafter cord clamping (n ¼ 60)
� All women received oxytocin20 IU intravenous infusionafter cord clamping
Intraoperative blood loss
Owonikoko et al,49
2011Nigeria � Inclusion: women with term singleton pregnancy
undergoing elective or emergency cesarean sectionunder spinal anesthesia
� Exclusion: women with multiple gestation, placentaprevia, antepartum hemorrhage, unexplained vaginalbleeding, cesarean section under general anesthesia,preexisting medical illnesses (cardiovascular, renal,or hepatic dysfunction), clotting disorders, severepreeclampsia, eclampsia, prolonged obstructed labor,and contraindications to prostaglandin administration
100 (1) Misoprostol 400 mg sublinguallyafter delivery of baby (n ¼ 50)
(2) Oxytocin 20 IU intravenousinfusion after delivery ofbaby (n ¼ 50)
Intraoperative andpostoperative blood loss,difference betweenpreoperative andpostoperative hemoglobin,need for additionaluterotonic agents,and drug-relatedadverse effects
Sood and Singh,50
2012India � Inclusion: women undergoing elective or emergency
cesarean section under spinal or epiduralanesthesia
� Exclusion: none
174 (1) Misoprostol 400 mg sublinguallyafter cord clamping (n ¼ 90)
(2) Placebo tablets sublinguallyafter cord clamping (n ¼ 84)
� All women received oxytocin20 IU intravenous infusion(6 IU over 30 min followed byintravenous infusion at40 mIU/min over a periodof 6 h) after cord clamping
Intraoperative blood loss,need for additional uterotonicagents, and differencebetween preoperative andpostoperative hemoglobin
Ali and Hina,51 2012 Pakistan � Inclusion: women with parity �4 and hemoglobin>11 g/dL undergoing elective or emergencycesarean section
� Exclusion: parity >4
374 (1) Misoprostol 800 mg rectallyjust before onset of cesareansection (n ¼ 187)
Intraoperative bloodloss >500 mL andpostoperativehemoglobin
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013. (continued)
Resea
rch
Obstetrics
www.AJO
G.org
40.e7American
JournalofObstetrics
&Gynecology
JULY
2013
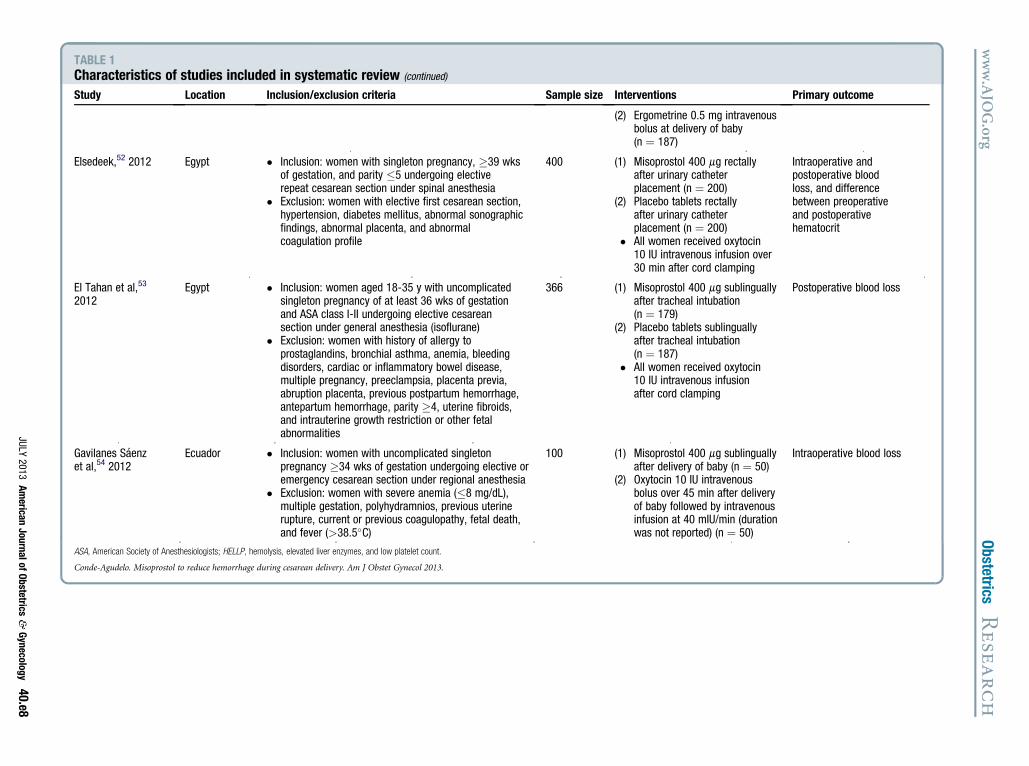
TABLE 1Characteristics of studies included in systematic review (continued)
Study Location Inclusion/exclusion criteria Sample size Interventions Primary outcome
(2) Ergometrine 0.5 mg intravenousbolus at delivery of baby(n ¼ 187)
Elsedeek,52 2012 Egypt � Inclusion: women with singleton pregnancy, �39 wksof gestation, and parity �5 undergoing electiverepeat cesarean section under spinal anesthesia
� Exclusion: women with elective first cesarean section,hypertension, diabetes mellitus, abnormal sonographicfindings, abnormal placenta, and abnormalcoagulation profile
400 (1) Misoprostol 400 mg rectallyafter urinary catheterplacement (n ¼ 200)
(2) Placebo tablets rectallyafter urinary catheterplacement (n ¼ 200)
� All women received oxytocin10 IU intravenous infusion over30 min after cord clamping
Intraoperative andpostoperative bloodloss, and differencebetween preoperativeand postoperativehematocrit
El Tahan et al,53
2012Egypt � Inclusion: women aged 18-35 y with uncomplicated
singleton pregnancy of at least 36 wks of gestationand ASA class I-II undergoing elective cesareansection under general anesthesia (isoflurane)
� Exclusion: women with history of allergy toprostaglandins, bronchial asthma, anemia, bleedingdisorders, cardiac or inflammatory bowel disease,multiple pregnancy, preeclampsia, placenta previa,abruption placenta, previous postpartum hemorrhage,antepartum hemorrhage, parity �4, uterine fibroids,and intrauterine growth restriction or other fetalabnormalities
366 (1) Misoprostol 400 mg sublinguallyafter tracheal intubation(n ¼ 179)
(2) Placebo tablets sublinguallyafter tracheal intubation(n ¼ 187)
� All women received oxytocin10 IU intravenous infusionafter cord clamping
Postoperative blood loss
Gavilanes Saenzet al,54 2012
Ecuador � Inclusion: women with uncomplicated singletonpregnancy �34 wks of gestation undergoing elective oremergency cesarean section under regional anesthesia
� Exclusion: women with severe anemia (�8 mg/dL),multiple gestation, polyhydramnios, previous uterinerupture, current or previous coagulopathy, fetal death,and fever (>38.5�C)
100 (1) Misoprostol 400 mg sublinguallyafter delivery of baby (n ¼ 50)
(2) Oxytocin 10 IU intravenousbolus over 45 min after deliveryof baby followed by intravenousinfusion at 40 mIU/min (durationwas not reported) (n ¼ 50)
Intraoperative blood loss
ASA, American Society of Anesthesiologists; HELLP, hemolysis, elevated liver enzymes, and low platelet count.
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013.
www.AJO
G.org
Obstetrics
Resea
rch
JULY
2013American
JournalofObstetrics
&Gynecology
40.e8
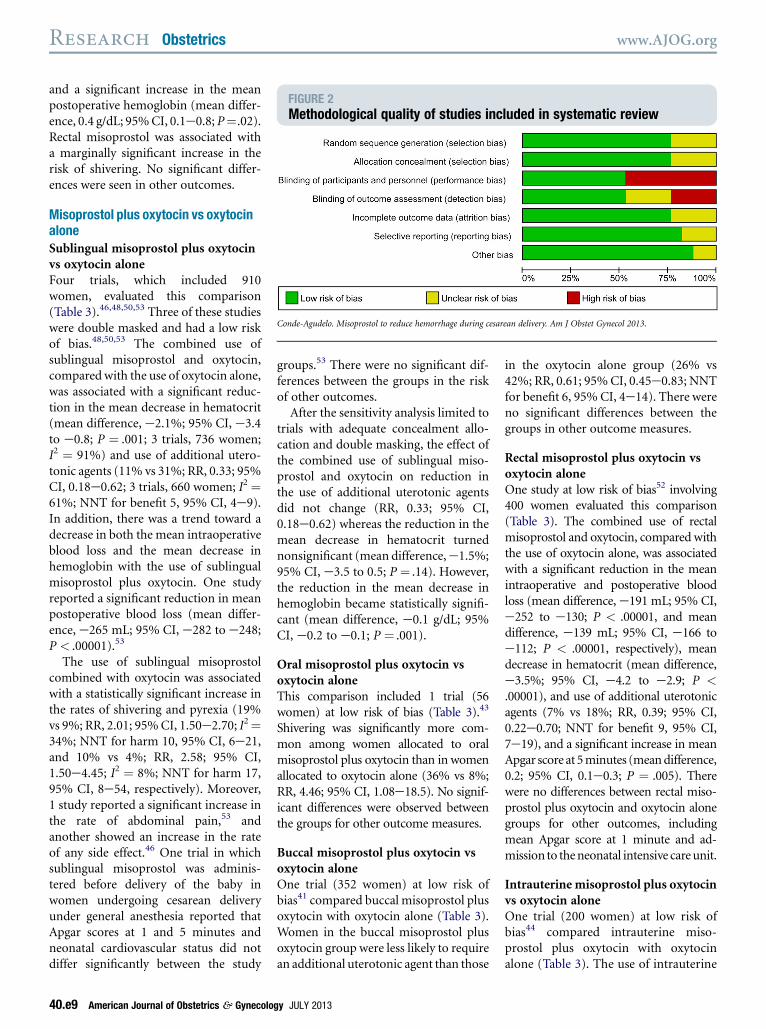
FIGURE 2Methodological quality of studies included in systematic review
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013.
Research Obstetrics www.AJOG.org
and a significant increase in the meanpostoperative hemoglobin (mean differ-ence, 0.4 g/dL; 95%CI, 0.1e0.8; P¼.02).Rectal misoprostol was associated witha marginally significant increase in therisk of shivering. No significant differ-ences were seen in other outcomes.
Misoprostol plus oxytocin vs oxytocinaloneSublingual misoprostol plus oxytocinvs oxytocin aloneFour trials, which included 910women, evaluated this comparison(Table 3).46,48,50,53 Three of these studieswere double masked and had a low riskof bias.48,50,53 The combined use ofsublingual misoprostol and oxytocin,compared with the use of oxytocin alone,was associated with a significant reduc-tion in the mean decrease in hematocrit(mean difference, e2.1%; 95% CI, e3.4to e0.8; P ¼ .001; 3 trials, 736 women;I2 ¼ 91%) and use of additional utero-tonic agents (11% vs 31%; RR, 0.33; 95%CI, 0.18e0.62; 3 trials, 660 women; I2 ¼61%; NNT for benefit 5, 95% CI, 4e9).In addition, there was a trend toward adecrease in both the mean intraoperativeblood loss and the mean decrease inhemoglobin with the use of sublingualmisoprostol plus oxytocin. One studyreported a significant reduction in meanpostoperative blood loss (mean differ-ence, e265 mL; 95% CI, e282 to e248;P < .00001).53
The use of sublingual misoprostolcombined with oxytocin was associatedwith a statistically significant increase inthe rates of shivering and pyrexia (19%vs 9%; RR, 2.01; 95%CI, 1.50e2.70; I2¼34%; NNT for harm 10, 95% CI, 6e21,and 10% vs 4%; RR, 2.58; 95% CI,1.50e4.45; I2 ¼ 8%; NNT for harm 17,95% CI, 8e54, respectively). Moreover,1 study reported a significant increase inthe rate of abdominal pain,53 andanother showed an increase in the rateof any side effect.46 One trial in whichsublingual misoprostol was adminis-tered before delivery of the baby inwomen undergoing cesarean deliveryunder general anesthesia reported thatApgar scores at 1 and 5 minutes andneonatal cardiovascular status did notdiffer significantly between the study
40.e9 American Journal of Obstetrics & Gynecolo
groups.53 There were no significant dif-ferences between the groups in the riskof other outcomes.After the sensitivity analysis limited to
trials with adequate concealment allo-cation and double masking, the effect ofthe combined use of sublingual miso-prostol and oxytocin on reduction inthe use of additional uterotonic agentsdid not change (RR, 0.33; 95% CI,0.18e0.62) whereas the reduction in themean decrease in hematocrit turnednonsignificant (mean difference,e1.5%;95% CI, e3.5 to 0.5; P ¼ .14). However,the reduction in the mean decrease inhemoglobin became statistically signifi-cant (mean difference, e0.1 g/dL; 95%CI, e0.2 to e0.1; P ¼ .001).
Oral misoprostol plus oxytocin vsoxytocin aloneThis comparison included 1 trial (56women) at low risk of bias (Table 3).43
Shivering was significantly more com-mon among women allocated to oralmisoprostol plus oxytocin than in womenallocated to oxytocin alone (36% vs 8%;RR, 4.46; 95% CI, 1.08e18.5). No signif-icant differences were observed betweenthe groups for other outcome measures.
Buccal misoprostol plus oxytocin vsoxytocin aloneOne trial (352 women) at low risk ofbias41 compared buccal misoprostol plusoxytocin with oxytocin alone (Table 3).Women in the buccal misoprostol plusoxytocin group were less likely to requirean additional uterotonic agent than those
gy JULY 2013
in the oxytocin alone group (26% vs42%; RR, 0.61; 95%CI, 0.45e0.83; NNTfor benefit 6, 95% CI, 4e14). There wereno significant differences between thegroups in other outcome measures.
Rectal misoprostol plus oxytocin vsoxytocin aloneOne study at low risk of bias52 involving400 women evaluated this comparison(Table 3). The combined use of rectalmisoprostol and oxytocin, compared withthe use of oxytocin alone, was associatedwith a significant reduction in the meanintraoperative and postoperative bloodloss (mean difference,e191 mL; 95% CI,e252 to e130; P < .00001, and meandifference, e139 mL; 95% CI, e166 toe112; P < .00001, respectively), meandecrease in hematocrit (mean difference,e3.5%; 95% CI, e4.2 to e2.9; P <.00001), and use of additional uterotonicagents (7% vs 18%; RR, 0.39; 95% CI,0.22e0.70; NNT for benefit 9, 95% CI,7e19), and a significant increase in meanApgar score at 5minutes (meandifference,0.2; 95% CI, 0.1e0.3; P ¼ .005). Therewere no differences between rectal miso-prostol plus oxytocin and oxytocin alonegroups for other outcomes, includingmean Apgar score at 1 minute and ad-mission to theneonatal intensive careunit.
Intrauterine misoprostol plus oxytocinvs oxytocin aloneOne trial (200 women) at low risk ofbias44 compared intrauterine miso-prostol plus oxytocin with oxytocinalone (Table 3). The use of intrauterine
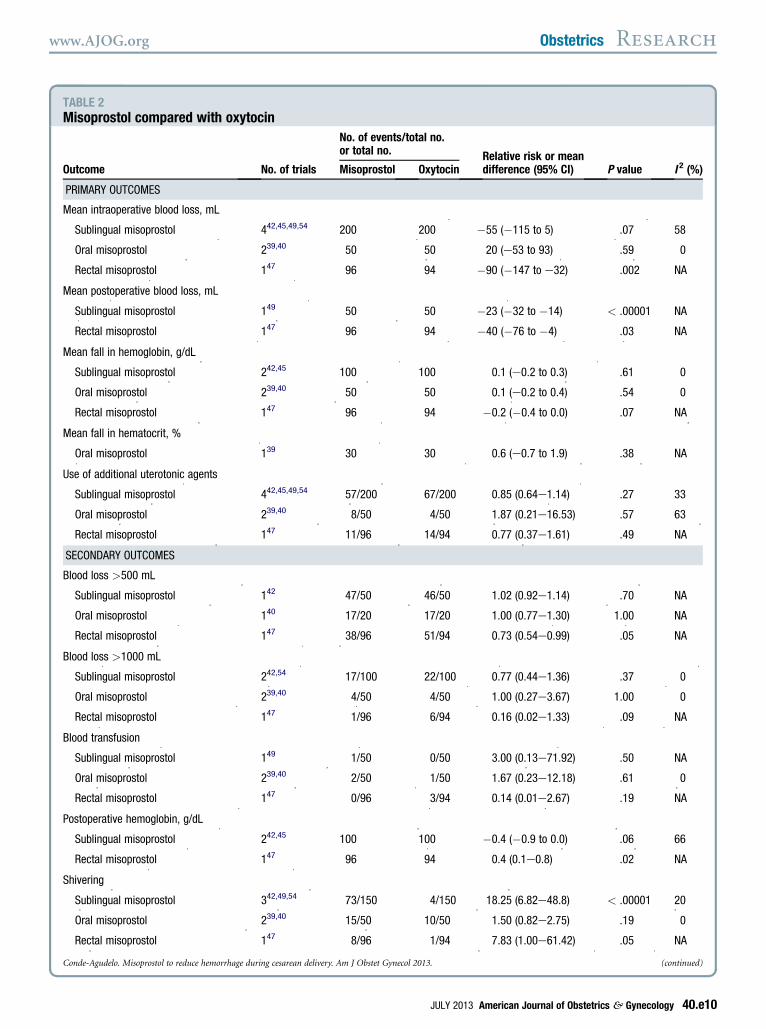
TABLE 2Misoprostol compared with oxytocin
Outcome No. of trials
No. of events/total no.or total no. Relative risk or mean
difference (95% CI) P value I 2 (%)Misoprostol Oxytocin
PRIMARY OUTCOMES
Mean intraoperative blood loss, mL
Sublingual misoprostol 442,45,49,54 200 200 �55 (�115 to 5) .07 58
Oral misoprostol 239,40 50 50 20 (e53 to 93) .59 0
Rectal misoprostol 147 96 94 �90 (�147 to e32) .002 NA
Mean postoperative blood loss, mL
Sublingual misoprostol 149 50 50 �23 (�32 to �14) < .00001 NA
Rectal misoprostol 147 96 94 �40 (�76 to �4) .03 NA
Mean fall in hemoglobin, g/dL
Sublingual misoprostol 242,45 100 100 0.1 (e0.2 to 0.3) .61 0
Oral misoprostol 239,40 50 50 0.1 (e0.2 to 0.4) .54 0
Rectal misoprostol 147 96 94 �0.2 (�0.4 to 0.0) .07 NA
Mean fall in hematocrit, %
Oral misoprostol 139 30 30 0.6 (e0.7 to 1.9) .38 NA
Use of additional uterotonic agents
Sublingual misoprostol 442,45,49,54 57/200 67/200 0.85 (0.64e1.14) .27 33
Oral misoprostol 239,40 8/50 4/50 1.87 (0.21e16.53) .57 63
Rectal misoprostol 147 11/96 14/94 0.77 (0.37e1.61) .49 NA
SECONDARY OUTCOMES
Blood loss >500 mL
Sublingual misoprostol 142 47/50 46/50 1.02 (0.92e1.14) .70 NA
Oral misoprostol 140 17/20 17/20 1.00 (0.77e1.30) 1.00 NA
Rectal misoprostol 147 38/96 51/94 0.73 (0.54e0.99) .05 NA
Blood loss >1000 mL
Sublingual misoprostol 242,54 17/100 22/100 0.77 (0.44e1.36) .37 0
Oral misoprostol 239,40 4/50 4/50 1.00 (0.27e3.67) 1.00 0
Rectal misoprostol 147 1/96 6/94 0.16 (0.02e1.33) .09 NA
Blood transfusion
Sublingual misoprostol 149 1/50 0/50 3.00 (0.13e71.92) .50 NA
Oral misoprostol 239,40 2/50 1/50 1.67 (0.23e12.18) .61 0
Rectal misoprostol 147 0/96 3/94 0.14 (0.01e2.67) .19 NA
Postoperative hemoglobin, g/dL
Sublingual misoprostol 242,45 100 100 �0.4 (�0.9 to 0.0) .06 66
Rectal misoprostol 147 96 94 0.4 (0.1e0.8) .02 NA
Shivering
Sublingual misoprostol 342,49,54 73/150 4/150 18.25 (6.82e48.8) < .00001 20
Oral misoprostol 239,40 15/50 10/50 1.50 (0.82e2.75) .19 0
Rectal misoprostol 147 8/96 1/94 7.83 (1.00e61.42) .05 NA
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013. (continued)
www.AJOG.org Obstetrics Research
JULY 2013 American Journal of Obstetrics & Gynecology 40.e10
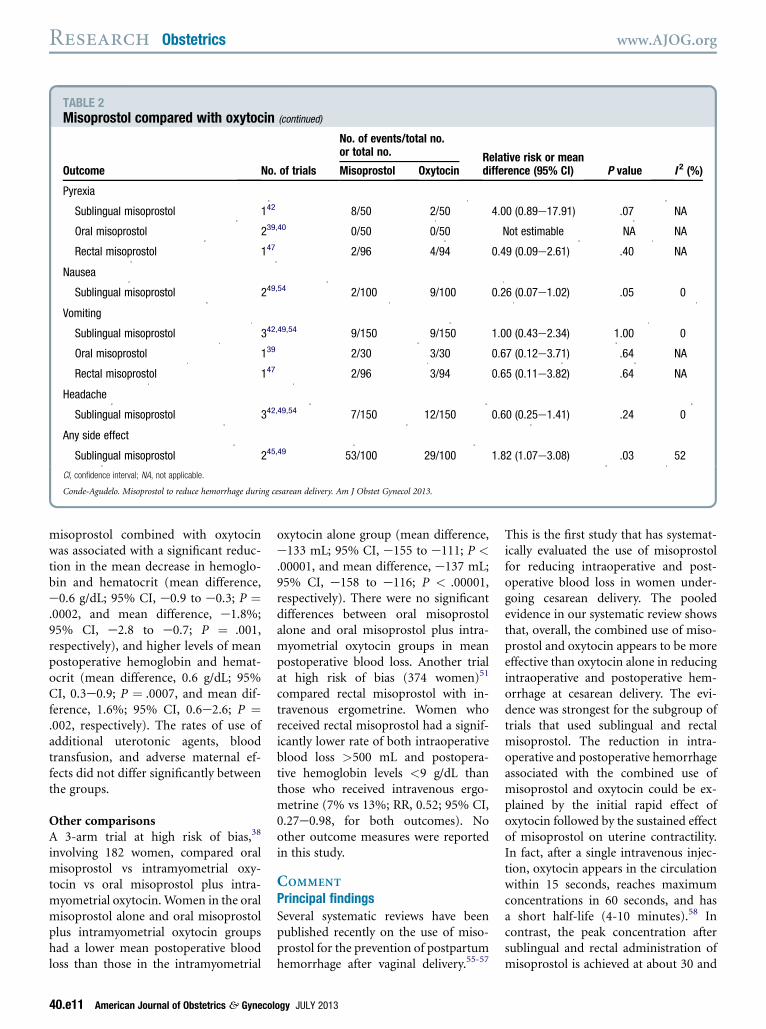
TABLE 2Misoprostol compared with oxytocin (continued)
Outcome No. of trials
No. of events/total no.or total no. Relative risk or mean
difference (95% CI) P value I 2 (%)Misoprostol Oxytocin
Pyrexia
Sublingual misoprostol 142 8/50 2/50 4.00 (0.89e17.91) .07 NA
Oral misoprostol 239,40 0/50 0/50 Not estimable NA NA
Rectal misoprostol 147 2/96 4/94 0.49 (0.09e2.61) .40 NA
Nausea
Sublingual misoprostol 249,54 2/100 9/100 0.26 (0.07e1.02) .05 0
Vomiting
Sublingual misoprostol 342,49,54 9/150 9/150 1.00 (0.43e2.34) 1.00 0
Oral misoprostol 139 2/30 3/30 0.67 (0.12e3.71) .64 NA
Rectal misoprostol 147 2/96 3/94 0.65 (0.11e3.82) .64 NA
Headache
Sublingual misoprostol 342,49,54 7/150 12/150 0.60 (0.25e1.41) .24 0
Any side effect
Sublingual misoprostol 245,49 53/100 29/100 1.82 (1.07e3.08) .03 52
CI, confidence interval; NA, not applicable.
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013.
Research Obstetrics www.AJOG.org
misoprostol combined with oxytocinwas associated with a significant reduc-tion in the mean decrease in hemoglo-bin and hematocrit (mean difference,e0.6 g/dL; 95% CI, e0.9 to e0.3; P ¼.0002, and mean difference, e1.8%;95% CI, e2.8 to e0.7; P ¼ .001,respectively), and higher levels of meanpostoperative hemoglobin and hemat-ocrit (mean difference, 0.6 g/dL; 95%CI, 0.3e0.9; P ¼ .0007, and mean dif-ference, 1.6%; 95% CI, 0.6e2.6; P ¼.002, respectively). The rates of use ofadditional uterotonic agents, bloodtransfusion, and adverse maternal ef-fects did not differ significantly betweenthe groups.
Other comparisonsA 3-arm trial at high risk of bias,38
involving 182 women, compared oralmisoprostol vs intramyometrial oxy-tocin vs oral misoprostol plus intra-myometrial oxytocin. Women in the oralmisoprostol alone and oral misoprostolplus intramyometrial oxytocin groupshad a lower mean postoperative bloodloss than those in the intramyometrial
40.e11 American Journal of Obstetrics & Gynecol
oxytocin alone group (mean difference,e133 mL; 95% CI, e155 to e111; P <.00001, and mean difference, e137 mL;95% CI, e158 to e116; P < .00001,respectively). There were no significantdifferences between oral misoprostolalone and oral misoprostol plus intra-myometrial oxytocin groups in meanpostoperative blood loss. Another trialat high risk of bias (374 women)51
compared rectal misoprostol with in-travenous ergometrine. Women whoreceived rectal misoprostol had a signif-icantly lower rate of both intraoperativeblood loss >500 mL and postopera-tive hemoglobin levels <9 g/dL thanthose who received intravenous ergo-metrine (7% vs 13%; RR, 0.52; 95% CI,0.27e0.98, for both outcomes). Noother outcome measures were reportedin this study.
COMMENT
Principal findingsSeveral systematic reviews have beenpublished recently on the use of miso-prostol for the prevention of postpartumhemorrhage after vaginal delivery.55-57
ogy JULY 2013
This is the first study that has systemat-ically evaluated the use of misoprostolfor reducing intraoperative and post-operative blood loss in women under-going cesarean delivery. The pooledevidence in our systematic review showsthat, overall, the combined use of miso-prostol and oxytocin appears to be moreeffective than oxytocin alone in reducingintraoperative and postoperative hem-orrhage at cesarean delivery. The evi-dence was strongest for the subgroup oftrials that used sublingual and rectalmisoprostol. The reduction in intra-operative and postoperative hemorrhageassociated with the combined use ofmisoprostol and oxytocin could be ex-plained by the initial rapid effect ofoxytocin followed by the sustained effectof misoprostol on uterine contractility.In fact, after a single intravenous injec-tion, oxytocin appears in the circulationwithin 15 seconds, reaches maximumconcentrations in 60 seconds, and hasa short half-life (4-10 minutes).58 Incontrast, the peak concentration aftersublingual and rectal administration ofmisoprostol is achieved at about 30 and
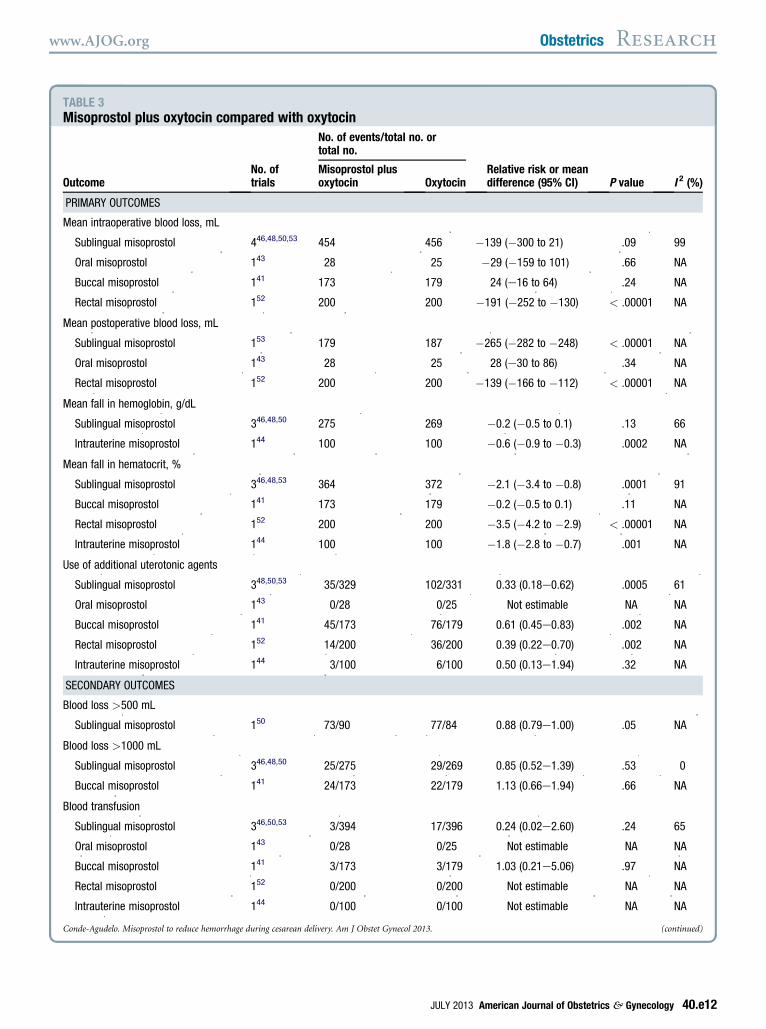
TABLE 3Misoprostol plus oxytocin compared with oxytocin
OutcomeNo. oftrials
No. of events/total no. ortotal no.
Relative risk or meandifference (95% CI) P value I 2 (%)
Misoprostol plusoxytocin Oxytocin
PRIMARY OUTCOMES
Mean intraoperative blood loss, mL
Sublingual misoprostol 446,48,50,53 454 456 �139 (�300 to 21) .09 99
Oral misoprostol 143 28 25 �29 (�159 to 101) .66 NA
Buccal misoprostol 141 173 179 24 (e16 to 64) .24 NA
Rectal misoprostol 152 200 200 �191 (�252 to �130) < .00001 NA
Mean postoperative blood loss, mL
Sublingual misoprostol 153 179 187 �265 (�282 to �248) < .00001 NA
Oral misoprostol 143 28 25 28 (e30 to 86) .34 NA
Rectal misoprostol 152 200 200 �139 (�166 to �112) < .00001 NA
Mean fall in hemoglobin, g/dL
Sublingual misoprostol 346,48,50 275 269 �0.2 (�0.5 to 0.1) .13 66
Intrauterine misoprostol 144 100 100 �0.6 (�0.9 to �0.3) .0002 NA
Mean fall in hematocrit, %
Sublingual misoprostol 346,48,53 364 372 �2.1 (�3.4 to �0.8) .0001 91
Buccal misoprostol 141 173 179 �0.2 (�0.5 to 0.1) .11 NA
Rectal misoprostol 152 200 200 �3.5 (�4.2 to �2.9) < .00001 NA
Intrauterine misoprostol 144 100 100 �1.8 (�2.8 to �0.7) .001 NA
Use of additional uterotonic agents
Sublingual misoprostol 348,50,53 35/329 102/331 0.33 (0.18e0.62) .0005 61
Oral misoprostol 143 0/28 0/25 Not estimable NA NA
Buccal misoprostol 141 45/173 76/179 0.61 (0.45e0.83) .002 NA
Rectal misoprostol 152 14/200 36/200 0.39 (0.22e0.70) .002 NA
Intrauterine misoprostol 144 3/100 6/100 0.50 (0.13e1.94) .32 NA
SECONDARY OUTCOMES
Blood loss >500 mL
Sublingual misoprostol 150 73/90 77/84 0.88 (0.79e1.00) .05 NA
Blood loss >1000 mL
Sublingual misoprostol 346,48,50 25/275 29/269 0.85 (0.52e1.39) .53 0
Buccal misoprostol 141 24/173 22/179 1.13 (0.66e1.94) .66 NA
Blood transfusion
Sublingual misoprostol 346,50,53 3/394 17/396 0.24 (0.02e2.60) .24 65
Oral misoprostol 143 0/28 0/25 Not estimable NA NA
Buccal misoprostol 141 3/173 3/179 1.03 (0.21e5.06) .97 NA
Rectal misoprostol 152 0/200 0/200 Not estimable NA NA
Intrauterine misoprostol 144 0/100 0/100 Not estimable NA NA
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013. (continued)
www.AJOG.org Obstetrics Research
JULY 2013 American Journal of Obstetrics & Gynecology 40.e12
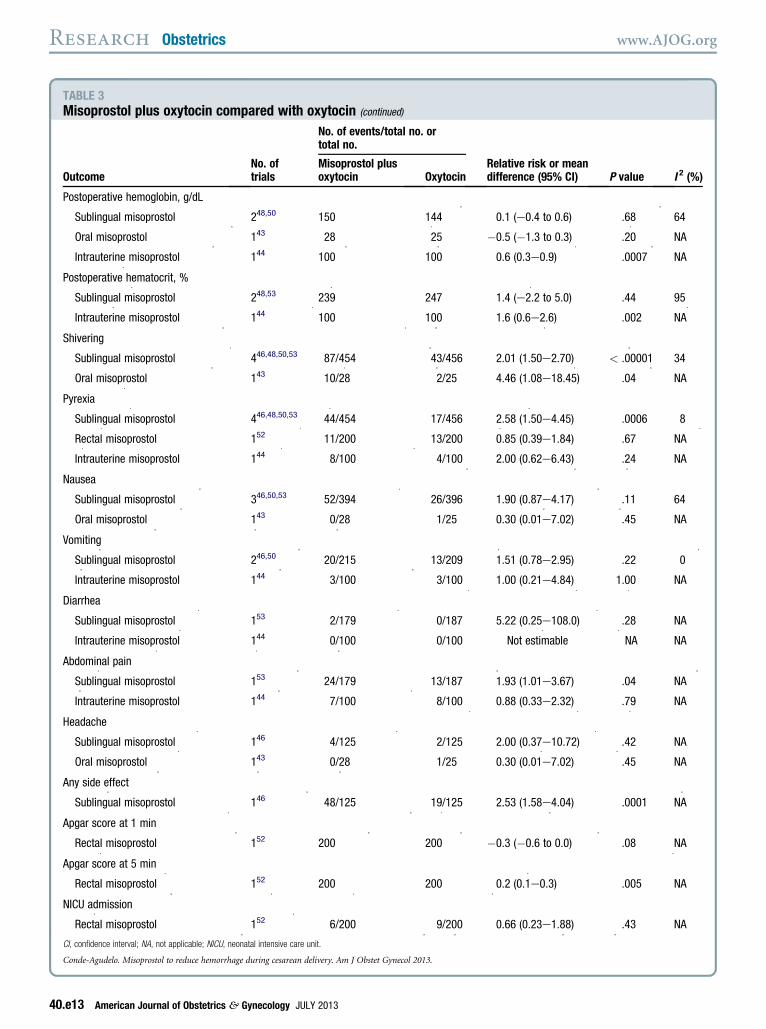
TABLE 3Misoprostol plus oxytocin compared with oxytocin (continued)
OutcomeNo. oftrials
No. of events/total no. ortotal no.
Relative risk or meandifference (95% CI) P value I 2 (%)
Misoprostol plusoxytocin Oxytocin
Postoperative hemoglobin, g/dL
Sublingual misoprostol 248,50 150 144 0.1 (e0.4 to 0.6) .68 64
Oral misoprostol 143 28 25 �0.5 (�1.3 to 0.3) .20 NA
Intrauterine misoprostol 144 100 100 0.6 (0.3e0.9) .0007 NA
Postoperative hematocrit, %
Sublingual misoprostol 248,53 239 247 1.4 (e2.2 to 5.0) .44 95
Intrauterine misoprostol 144 100 100 1.6 (0.6e2.6) .002 NA
Shivering
Sublingual misoprostol 446,48,50,53 87/454 43/456 2.01 (1.50e2.70) < .00001 34
Oral misoprostol 143 10/28 2/25 4.46 (1.08e18.45) .04 NA
Pyrexia
Sublingual misoprostol 446,48,50,53 44/454 17/456 2.58 (1.50e4.45) .0006 8
Rectal misoprostol 152 11/200 13/200 0.85 (0.39e1.84) .67 NA
Intrauterine misoprostol 144 8/100 4/100 2.00 (0.62e6.43) .24 NA
Nausea
Sublingual misoprostol 346,50,53 52/394 26/396 1.90 (0.87e4.17) .11 64
Oral misoprostol 143 0/28 1/25 0.30 (0.01e7.02) .45 NA
Vomiting
Sublingual misoprostol 246,50 20/215 13/209 1.51 (0.78e2.95) .22 0
Intrauterine misoprostol 144 3/100 3/100 1.00 (0.21e4.84) 1.00 NA
Diarrhea
Sublingual misoprostol 153 2/179 0/187 5.22 (0.25e108.0) .28 NA
Intrauterine misoprostol 144 0/100 0/100 Not estimable NA NA
Abdominal pain
Sublingual misoprostol 153 24/179 13/187 1.93 (1.01e3.67) .04 NA
Intrauterine misoprostol 144 7/100 8/100 0.88 (0.33e2.32) .79 NA
Headache
Sublingual misoprostol 146 4/125 2/125 2.00 (0.37e10.72) .42 NA
Oral misoprostol 143 0/28 1/25 0.30 (0.01e7.02) .45 NA
Any side effect
Sublingual misoprostol 146 48/125 19/125 2.53 (1.58e4.04) .0001 NA
Apgar score at 1 min
Rectal misoprostol 152 200 200 �0.3 (�0.6 to 0.0) .08 NA
Apgar score at 5 min
Rectal misoprostol 152 200 200 0.2 (0.1e0.3) .005 NA
NICU admission
Rectal misoprostol 152 6/200 9/200 0.66 (0.23e1.88) .43 NA
CI, confidence interval; NA, not applicable; NICU, neonatal intensive care unit.
Conde-Agudelo. Misoprostol to reduce hemorrhage during cesarean delivery. Am J Obstet Gynecol 2013.
Research Obstetrics www.AJOG.org
40.e13 American Journal of Obstetrics & Gynecology JULY 2013

www.AJOG.org Obstetrics Research
40-65 minutes, respectively, with aduration of action of about 3 and 4hours, respectively.59
In addition, we found no statisticallysignificant differences between miso-prostol and oxytocin in reducing intra-operative and postoperative hemorrhageat cesarean delivery. Nevertheless, it isnoteworthy that this finding is basedon a few small trials with methodo-logical limitations, mainly lack of doublemasking. Trials comparing misoprostolwith oxytocin should be consideredequivalence or noninferiority trials de-signed to evaluate whether misoprostolis not superior but equivalent to ornot inferior to oxytocin.60 None of thetrials that compared misoprostol withoxytocin were planned or had the sta-tistical power to evaluate equivalence ornoninferiority between the 2 agents.Therefore, the lack of statistical signifi-cance between misoprostol and oxytocinfound in our review does not imply thatthese drugs have the same efficacy inreducing perioperative hemorrhage atcesarean delivery. Overall, the rates ofside effects, mainly shivering and py-rexia, were higher among women whoreceived misoprostol alone or combinedwith oxytocin than among women whoreceived oxytocin alone. The increasedrisk of side effects was more apparent intrials that used sublingual misoprostolthan in trials that used other routesof misoprostol administration. Therewere no significant differences in Apgarscores at 1 and 5 minutes and admissionto the neonatal intensive care unit be-tween misoprostol and oxytocin groups,although these outcomes were reportedin only 2 of the 5 trials that used miso-prostol before delivery of the neonate.
Strengths and limitations of the studyThe reliability and robustness of ourresults are supported by the use of themost rigorous methodology for per-forming a systematic review and meta-analysis of RCTs, the comprehensiveliterature search without language re-strictions and including the gray litera-ture and conference proceedings thatidentified studies published in English,Spanish, French, Chinese, and Thai; theinclusion of a relatively large number of
studies in the systematic review, mostof which were published in recentyears; the strict assessment of methodo-logical quality of included trials; thequantitative summary of the evidence;the performance of subgroup analysesaccording to route of administrationof misoprostol and combined use ofoxytocin; and the sensitivity analysisrestricted to trials at low risk of bias.Some limitations of this study should
be acknowledged. First, there was sub-stantial statistical heterogeneity in sev-eral of the metaanalyses performed;therefore, our findings should be inter-preted in this context. Nevertheless, inmost of the comparisons, the estimatesshowed the same direction of effect,which could suggest the absence ofclinical heterogeneity among the studies.We used random effects models to pooldata across studies to attempt to incor-porate any heterogeneity and exploredpossible sources of heterogeneity such asstudy quality. In addition, we stratifiedanalyses by route of misoprostol ad-ministration and the combined use ofoxytocin. Despite this, we could notexplain most of the heterogeneity, whichmay be due to differences in studypopulation, doses of misoprostol andoxytocin, cesarean delivery technique,surgical experience, method of assess-ment of blood loss, or trial imple-mentation. Second, some subgroupanalyses were based on small numbers ofpatients. As a result, our analysis waslimited in its power to estimate effectswithin these subgroups and to detectdifferences, if any exist, among womenin predetermined subgroups. Third,several studies did not report results ofimportant primary outcome measuresincluded in our review, such as post-operative blood loss and decrease inhematocrit in trials comparing miso-prostol and oxytocin, and postoperativeblood loss and decrease in hemoglobinin trials comparing misoprostol plusoxytocin and oxytocin alone. Thus, ourmetaanalysis may be underpowered forsuch outcomes. It is possible that, if theseresults were reported more consistently,effect sizes might be different. Finally,like any systematic review, ours is limitedby the quality of original data. Only
JULY 2013 Ameri
about half of the trials included in themetaanalyses were considered to be atlow risk of bias. Nevertheless, sensitivityanalyses restricted to high-quality trialscomparing misoprostol plus oxytocinand oxytocin alone upheld most resultsobtained with the overall metaanalyses.
Thus far, no systematic review onthe prophylactic use of misoprostol atcesarean delivery for reducing intra-operative and postoperative hemorrhagehas been published. A recent Cochranereview assessed the effectiveness of pro-phylactic prostaglandin use as part of theroutine management of the third stage oflabor for the prevention of postpartumhemorrhage.31 A total of 57 trials thatevaluated misoprostol were includedin this review. Only 7 trials included inour review were also included in theCochrane review.40-46 Data provided bythese studies were pooled with data fromstudies that evaluated misoprostol inwomen after vaginal delivery. This re-view found that oral or sublingualmisoprostol, compared with placebo,significantly reduced the risk of severepostpartum hemorrhage and bloodtransfusion. Nevertheless, when com-pared with oxytocin, oral misoprostolwas associated with a significant increasein the risk of severe postpartum hem-orrhage and use of additional uterotonicagents, but with a trend toward fewerblood transfusions. Overall, misoprostolwas associated with an increased risk ofshivering and pyrexia compared withboth placebo and oxytocin. No resultswere reported for women receivingmisoprostol at cesarean delivery.
Carbetocin, a synthetic analogue ofhuman oxytocin with structural modifi-cations that increase its half-life (therebyprolonging its pharmacological effects),has been proposed for the preventionof postpartum hemorrhage followingcesarean delivery. A recent Cochranereview reported that carbetocin de-creased significantly the use of additionaluterotonic agents in women undergoingcesarean delivery when compared tooxytocin (RR, 0.64; 95% CI, 0.51e0.81;4 trials, 1173 women).61 There wereno differences between carbetocin andoxytocin in postpartum hemorrhage>500 and >1000 mL, intraoperative
can Journal of Obstetrics & Gynecology 40.e14

Research Obstetrics www.AJOG.org
blood loss, blood transfusion, decreasein hemoglobin, and adverse effects.Our systematic review and metaanalysisshowed that the combined use of sub-lingual misoprostol and oxytocin wassuperior to oxytocin alone, because thecombination significantly reduced theneed for additional uterotonic agents by67% (RR, 0.33; 95% CI, 0.18e0.62).Moreover, the use of combined sub-lingual misoprostol and oxytocin wasassociated with a significant reduction inthe mean decrease in hematocrit and atrend toward a decrease in both themeanintraoperative blood loss and the meandecrease in hemoglobin. It should benoted that the Society of Obstetriciansand Gynecologists of Canada recom-mends the use of carbetocin instead ofoxytocin in elective cesarean delivery forthe prevention of postpartum hemor-rhage and to decrease the need for addi-tional uterotonic agents.62
Implications for practiceCurrently, there is insufficient evidenceto establish equivalence between miso-prostol and oxytocin in the controlof intraoperative and postoperativehemorrhage during cesarean delivery.Moreover, misoprostol is associated withincreased rates of side effects. Therefore,misoprostol by itself cannot be recom-mended to replace oxytocin as a first-lineprophylactic uterotonic agent for thecontrol of blood loss at cesarean delivery.If future equivalence or noninferioritytrials show that misoprostol is as effica-cious as oxytocin in the reduction ofperioperative hemorrhage at cesareandelivery, then misoprostol could beconsidered as an option in settings inwhich the use of oxytocin is not feasible.
The results of our review show thatmisoprostol as an adjunct to oxytocinis more effective than oxytocin alone forreducing intraoperative and postopera-tive blood loss during cesarean delivery.Hence, the use of misoprostol, possibly400 mg sublingually after cord clamp-ing, in addition to oxytocin, shouldbe considered in women undergoingelective or emergency cesarean deliveryunder regional or general anesthesia.This prophylactic strategy could beespecially useful in women undergoing
40.e15 American Journal of Obstetrics & Gynecol
emergency cesarean delivery or undergeneral anesthesia, which are well-known risk factors for postpartumhemorrhage associated with this surgicalprocedure.17,22,23,63 Some trials have re-ported that misoprostol has the addi-tional effect of increasing intestinalmotility after cesarean delivery andallowing early oral feeding, which couldreduce the risk of postoperative ileusand shortened hospital stay length,and allow early breast-feeding.64-66 Thiseffect has been reported in trials thatadministered misoprostol rectally aftersurgery, but it is unclear if similar effectscan be obtained if the drug is adminis-tered sublingually.Finally, it should be noted that
although 13 of 17 studies were con-ducted in developing countries, the re-sults of this systematic review andmetaanalysis are very likely applicable toindustrialized ones. In fact, the medianmean intraoperative blood loss andmean duration of surgery in the controlgroup of the 4 studies conducted indeveloped countries was very similar tothat in the control group of the 13studies conducted in developing coun-tries (650 vs 651 mL, and 42 vs 43minutes, respectively). Moreover, thecesarean section technique used was verysimilar in all 17 studies included in thereview.
Implications for researchEquivalence or noninferiority RCTsare needed to compare the efficacy ofmisoprostol and oxytocin in reducingperioperative hemorrhage at cesareandelivery. Such trials should have suffi-cient statistical power to establishequivalence or noninferiority betweenthe 2 drugs, be double masked to mini-mize the risk of bias in the assessmentof the outcomes, and measure intra-operative and postoperative blood loss asobjectively and accurately as possible.Further research on the combined
use of misoprostol and oxytocin couldfocus on determining the best routeof administration and the optimal doseof misoprostol for reducing periopera-tive hemorrhage at cesarean delivery,the cost-effectiveness of this interven-tion, and the short- and long-term
ogy JULY 2013
consequences of infants exposed tomisoprostol in utero. Moreover, trialscomparing misoprostol plus oxytocin vscarbetocin would be justified. -
REFERENCES
1. Gibbons L, Belizan JM, Lauer JA, Betran AP,Merialdi M, Althabe F. Inequities in the use ofcesarean section deliveries in the world. Am JObstet Gynecol 2012;206:331.e1-331.e19.2. AnanthCV, Vintzileos AM. Trends in cesareandelivery at preterm gestation and associationwith perinatal mortality. Am J Obstet Gynecol2011;204:505.e1-8.3. Zhang J, Troendle J, Reddy UM, et al.Contemporary cesarean delivery practice in theUnited States. Am J Obstet Gynecol 2010;203:326.e1-10.4. Klemetti R, Che X, Gao Y, et al. Cesareansection delivery among primiparous women inrural China: an emerging epidemic. Am J ObstetGynecol 2010;202:65.e1-6.5. Getahun D, Strickland D, Lawrence JM,Fassett MJ, Koebnick C, Jacobsen SJ. Racialand ethnic disparities in the trends in primarycesarean delivery based on indications. Am JObstet Gynecol 2009;201:422.e1-7.6. Brennan DJ, Robson MS, Murphy M,O’Herlihy C. Comparative analysis of interna-tional cesarean delivery rates using 10-groupclassification identifies significant variation inspontaneous labor. Am J Obstet Gynecol2009;201:308.e1-8.7. Tang S, Li X, Wu Z. Rising cesarean deliveryrate in primiparous women in urban China:evidence from three nationwide householdhealth surveys. Am J Obstet Gynecol 2006;195:1527-32.8. Bailit JL, Love TE, Mercer B. Rising cesareanrates: are patients sicker? Am J Obstet Gynecol2004;191:800-3.9. Betrán AP, Merialdi M, Lauer JA, et al. Ratesof cesarean section: analysis of global, regionaland national estimates. Paediatr Perinat Epi-demiol 2007;21:98-113.10. Khan KS, Wojdyla D, Say L,Gülmezoglu AM, Van Look PF. WHO analysis ofcauses of maternal death: a systematic review.Lancet 2006;367:1066-74.11. Joseph KS, Rouleau J, Kramer MS,Young DC, Liston RM, Baskett TF. Investigationof an increase in postpartum hemorrhage inCanada. BJOG 2007;114:751-9.12. Ford JB, Roberts CL, Simpson JM,Vaughan J, CameronCA. Increased postpartumhemorrhage rates in Australia. Int J GynaecolObstet 2007;98:237-43.13. CallaghanWM, Kuklina EV, Berg CJ. Trendsin postpartum hemorrhage: United States,1994-2006. Am J Obstet Gynecol 2010;202:353.e1-6.14. Bateman BT, Berman MF, Riley LE,Leffert LR. The epidemiology of postpartumhemorrhage in a large, nationwide sample ofdeliveries. Anesth Analg 2010;110:1368-73.

www.AJOG.org Obstetrics Research
15. American College of Obstetricians andGynecologists. ACOG practice bulletin: clini-cal management guidelines for obstetrician-gynecologists no. 76; postpartum hemorrhage.Obstet Gynecol 2006;108:1039-47.16. Pritchard JA, Baldwin RM, Dickey JC,Wiggins KM, Reed GP, Bruce DM. Blood vol-ume changes in pregnancy and the puerperium,II: red blood cell loss and changes in apparentblood volume during and following vaginal de-livery, cesarean section, and cesarean plus totalhysterectomy. Am J Obstet Gynecol 1962;84:1271-82.17. Magann EF, Evans S, Hutchinson M,Collins R, Lanneau G, Morrison JC. Postpartumhemorrhage after cesarean delivery: an analysisof risk factors. South Med J 2005;98:681-5.18. Al-Zirqi I, Vangen S, Forsén L, Stray-Pedersen B. Effects of onset of labor andmode of delivery on severe postpartum hemor-rhage. Am J Obstet Gynecol 2009;201:273.e1-9.19. Carroli G, Cuesta C, Abalos E,Gulmezoglu AM. Epidemiology of postpartumhemorrhage: a systematic review. Best PractRes Clin Obstet Gynaecol 2008;22:999-1012.20. Kolås T, Øian P, Skjeldestad FE. Risks forperoperative excessive blood loss in cesareandelivery. Acta Obstet Gynecol Scand 2010;89:658-63.21. Kramer MS, Dahhou M, Vallerand D,Liston R, Joseph KS. Risk factors for post-partum hemorrhage: can we explain the recenttemporal increase? J Obstet Gynaecol Can2011;33:810-9.22. Chang CC, Wang IT, Chen YH, Lin HC.Anesthetic management as a risk factor forpostpartum hemorrhage after cesarean de-liveries. Am J Obstet Gynecol 2011;205:462.e1-7.23. Skjeldestad FE, Oian P. Blood loss aftercesarean delivery: a registry-based study inNorway, 1999-2008. Am J Obstet Gynecol2012;206:76.e1-7.24. Larsson C, Saltvedt S, Wiklund I, Pahlen S,Andolf E. Estimation of blood loss after cesareansection and vaginal delivery has low validitywith a tendency to exaggeration. Acta ObstetGynecol Scand 2006;85:1448-52.25. Stafford I, Dildy GA, Clark SL, Belfort MA.Visually estimated and calculated blood loss invaginal and cesarean delivery. Am J ObstetGynecol 2008;199:519.e1-7.26. Toledo P, McCarthy RJ, Burke CA, Goetz K,Wong CA, Grobman WA. The effect of liveand web-based education on the accuracy ofblood-loss estimation in simulated obstetricscenarios. Am J Obstet Gynecol 2010;202:400.e1-5.27. Begley CM, Gyte GM, Devane D,McGuire W, Weeks A. Active versus expectantmanagement for women in the third stage oflabor. Cochrane Database Syst Rev 2011;11:CD007412.28. National Collaborating Center for Women’sand Children’s Health. Cesarean section: NICEclinical guideline. London: RCOG Press; 2011.
29. Bonanno C, Gaddipati S. Mechanisms ofhemostasis at cesarean delivery. Clin Perinatol2008;35:531-47.30. Dyer RA, Butwick AJ, Carvalho B. Oxytocinfor labor and cesarean delivery: implications forthe anesthesiologist. Curr Opin Anaesthesiol2011;24:255-61.31. Tunçalp Ö, Hofmeyr GJ, Gülmezoglu AM.Prostaglandins for preventing postpartumhemorrhage. Cochrane Database Syst Rev2012;8:CD000494.32. Liberati A, Altman DG, Tetzlaff J, et al. ThePRISMA statement for reporting systematicreviews and meta-analyses of studies thatevaluate healthcare interventions: explanationand elaboration. Ann Intern Med 2009;151:W65-94.33. Higgins JPT, Altman DG, Sterne JAC.Assessing risk of bias in included studies. In:Higgins JPT, Green S, eds. Cochrane handbookfor systematic reviews of interventions. Version5.1.0 (updated March 2011). CochraneCollaboration; 2011.34. Deeks JJ, Higgins JPT, Altman DG.Analyzing data and undertaking meta-analyses.In: Higgins JPT, Green S, eds. Cochrane hand-book for systematic reviews of interventions.Version 5.1.0 (updated March 2011). CochraneCollaboration; 2011.35. Higgins JP, Thompson SG, Deeks JJ,Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557-60.36. Altman DG. Confidence intervals for thenumber needed to treat. BMJ 1998;317:1309-12.37. Egger M, Davey Smith G, Schneider M,Minder C. Bias in meta-analyses detectedby a simple graphical test. BMJ 1997;315:629-34.38. Zhao Y, Li X, Peng Y. Clinical study onreduction of postpartum bleeding in cesareansection by misoprostol [in Chinese]. ZhonghuaFu Chan Ke Za Zhi 1998;33:403-5.39. Acharya G, Al-Sammarai MT, Patel N,Al-Habib A, Kiserud T. A randomized, controlledtrial comparing effect of oral misoprostol andintravenous syntocinon on intra-operative bloodloss during cesarean section. Acta ObstetGynecol Scand 2001;80:245-50.40. Lokugamage AU, Paine M, Bassaw-Balroop K, Sullivan KR, Refaey HE, Rodeck CH.Active management of the third stage at cesar-ean section: a randomized controlled trial ofmisoprostol versus syntocinon. Aust N Z JObstet Gynaecol 2001;41:411-4.41. Hamm J, Russell Z, Botha T, Carlan SJ,Richichi K. Buccal misoprostol to preventhemorrhage at cesarean delivery: a random-ized study. Am J Obstet Gynecol 2005;192:1404-6.42. Vimala N, Mittal S, Kumar S. Sublingualmisoprostol versus oxytocin infusion to reduceblood loss at cesarean section. Int J GynaecolObstet 2006;92:106-10.43. Lapaire O, Schneider MC, Stotz M,Surbek DV, Holzgreve W, Hoesli IM. Oral miso-prostol vs intravenous oxytocin in reducing
JULY 2013 Ameri
blood loss after emergency cesarean delivery.Int J Gynaecol Obstet 2006;95:2-7.44. Quiroga Díaz R, Cantú Mata R, TelloGutiérrez HE, Puente Villalobos M, MontemayorGarza R, Martínez Mendoza A. Intrauterinemisoprostol for the prevention of bleedingcesarean [in Spanish]. Ginecol Obstet Mex2009;77:469-74.45. Eftekhari N, Doroodian M, Lashkarizadeh R.The effect of sublingual misoprostol versusintravenous oxytocin in reducing bleeding aftercesarean section. J Obstet Gynaecol 2009;29:633-6.46. Fekih M, Jnifene A, Fathallah K, et al.Benefit of misoprostol for prevention ofpostpartum hemorrhage in cesarean section:a randomized controlled trial [in French].J Gynecol Obstet Biol Reprod (Paris) 2009;38:588-93.47. Chaudhuri P, Banerjee GB, Mandal A.Rectally administered misoprostol versus intra-venous oxytocin infusion during cesarean de-livery to reduce intraoperative and postoperativeblood loss. Int J Gynaecol Obstet 2010;109:25-9.48. Chalermpolprapa MD. Efficacy of sublingualmisoprostol in prevention of postpartum hem-orrhage in cesarean section: a randomizeddouble-blinded, placebo-controlled trial [in Thai].Reg 4-5 Med J 2010;29:325-35.49. OwonikokoKM,ArowojoluAO,OkunlolaMA.Effect of sublingual misoprostol versus intra-venous oxytocin on reducing blood loss atcesarean section in Nigeria: a randomizedcontrolled trial. J Obstet Gynaecol Res 2011;37:715-21.50. Sood AK, Singh S. Sublingual misoprostolto reduce blood loss at cesarean delivery.J Obstet Gynecol India 2012;62:162-7.51. Ali R, Hina F. Postpartum hemorrhage:comparison of efficacy of ergometrine withmisoprostol in prophylaxis in cesarean section.Prof Med J 2012;19:86-90.52. Elsedeek MS. Impact of preoperative rectalmisoprostol on blood loss during and afterelective cesarean delivery. Int J Gynaecol Obstet2012;118:149-52.53. El Tahan MR, Warda OM, Rashad A, et al.Effects of preoperative sublingual misoprostolon uterine tone during isoflurane anesthesia forcesarean section. Rev Bras Anestesiol 2012;62:625-35.54. Gavilanes Sáenz VP, Morales Carrasco MF,Velasco Jácome SM. Comparison of theefficacy between misoprostol and oxytocinin the prevention of hemorrhage duringcesarean section in pregnant women at �34weeks’ gestation in the gynecological andobstetrical hospital “Isidro Ayora,” 2011-2012[postgraduate thesis] [in Spanish]. Quito(Ecuador): Universidad Central del Ecuador;2012. Available at: http://www.dspace.uce.edu.ec/bitstream/25000/634/1/T-UCE-0006-18.pdf.Accessed Feb. 6, 2013.55. Chu CS, Brhlikova P, Pollock AM.Rethinking WHO guidance: review of evidencefor misoprostol use in the prevention of
can Journal of Obstetrics & Gynecology 40.e16

Research Obstetrics www.AJOG.org
postpartum hemorrhage. J R Soc Med2012;105:336-47.56. Oladapo OT, Fawole B, Blum J, Abalos E.Advance misoprostol distribution for pre-venting and treating postpartum hemorrhage.Cochrane Database Syst Rev 2012;2:CD009336.57. Chelmow D. Postpartum hemorrhage: pre-vention. Clin Evid (Online) 2011;2011.58. Gibbens D, Boyd NR, Crocker S,Baumber S, Chard T. The circulating levels ofoxytocin following intravenous and intramus-cular administration of Syntometrine. J ObstetGynaecol Br Commonw 1972;79:644-6.59. Tang OS, Gemzell-Danielsson K, Ho PC.Misoprostol: pharmacokinetic profiles, effects
40.e17 American Journal of Obstetrics & Gynecol
on the uterus and side effects. Int J GynaecolObstet 2007;99(Suppl):S160-7.60. Treadwell J, Uhl S, Tipton K, et al. Assessingequivalence and noninferiority: AHRQ publica-tion no. 12-EHC045-EF. Rockville, MD: Agencyfor Healthcare Research and Quality; 2012.61. Su LL, Chong YS, Samuel M. Carbetocin forpreventing postpartum hemorrhage. CochraneDatabase Syst Rev 2012;4:CD005457.62. Leduc D, Senikas V, Lalonde AB, et al.Active management of the third stage of labor:prevention and treatment of postpartum hem-orrhage. J Obstet Gynaecol Can 2009;31:980-93.63. Häger RM, Daltveit AK, Hofoss D, et al.Complications of cesarean deliveries: rates and
ogy JULY 2013
risk factors. Am J Obstet Gynecol 2004;190:428-34.64. Hu BM, Liu X, Chen ZY. Effect of miso-prostol on gastrointestinal peristalsis after ce-sarean section [in Chinese]. Chin J Prim MedPharm 2008;15:1297-8.65. Çayan F, Doruk A, Sungur MA, Dilek S.Comparison of the different dosages of rectalmisoprostol on intestinal motility and pain scorein high risk cesarean delivery. Turkiye Klinikleri JMed Sci 2010;30:1154-9.66. Adanikin AI, Orji EO, Fasubaa OB,Onwudiegwu U, Ijarotimi OA, Olaniyan O. Theeffect of post-cesarean rectal misoprostolon intestinal motility. Int J Gynaecol Obstet2012;119:159-62.





























