Embed Size (px)
Citation preview

To the Editor,
Choriocarcinoma is a rapidly growing and widelymetastatic epithelial neoplasm, derived from eit-her trophoblastic or totipotential germ cells (1).Choriocarcinoma may also occur as a primary ne-oplasm of the ovary or testis. It has been rarely re-ported in non-gestational, extragonadal organssuch as the lung, liver, breast, prostate, urinarybladder, nose, and gastrointestinal tract (2). Pri-mary gastric choriocarcinoma (PGC) is extremelyrare, and most such cases are not diagnosed cor-rectly before operation (1). Most PGCs have beenreported to possess an adenocarcinoma componentof variable extent, and pure PGC is especially ra-re (3).
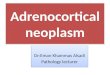
A 72-year-old male admitted to the hospital becau-se of epigastric pain. His physical examinationswere normal. Initial laboratory evaluation confir-med the anemia and hypoalbuminemia. The tu-mor markers were within normal limits. Compu-ted tomography (CT) scan showed a 2.5 cm nodu-lar lesion in the corpus of the stomach, which ex-tended to the gastric serosa and had directly inva-ded the pancreas. There were multiple masses inthe liver consistent with metastatic disease. Insubtotal gastrectomy material, the tumor measu-red 4.3 cm, was irregularly shaped, and had ulce-rative growth pattern and some bleeding areas.Microscopically, the tumor had two components.The first component was a well-differentiated ade-nocarcinoma, accounting for approximately 30% ofthe entire tumor. In hemorrhagic areas, the re-maining 70% of the tumor was a pleomorphic car-cinoma with several ‘syncytiotrophoblast’-likecells with bizarre nuclei; the histological featuresof this component were very suggestive of chori-ocarcinoma. Immunohistochemically, ‘syncytiot-rophoblast’-like cells strongly stained with beta-human chorionic gonadotropin (HCG). However,
the adenocarcinomatous component stained withCEA (Figure 1).
Germ cell-type tumors can occur in the stomach,the two most common forms being choriocarcino-ma and yolk sac tumor. Either can present in a pu-re form, admixed with each other, or associatedwith conventional adenocarcinoma. The choriocar-cinomas show immunohistochemical evidence ofHCG production and can be associated with eleva-ted serum levels of this marker.
The pathogenesis of development of choriocarcino-mas in the stomach is not clear. Hartz and Rami-rez (4) believed that this rare tumor developedfrom a gastric teratoma. Davidson described thefirst case of PGC in 1905, and while several theori-es, based mostly on clinical or histologic informa-tion, have been proposed to explain its pathogene-sis, it remains to be elucidated. He postulated thatthis tumor arises from displaced gonadal anlagewithin the abdomen (2). If this is correct, non-trop-hoblastic gonadal tissue should be found in associ-ation with choriocarcinoma, such as PGC withyolk sac tumor, as reported by Garcia and Ghali(5). However, the most plausible explanation forthe pathogenesis of gastric choriocarcinoma isthat proposed by Krulewski (6) based on his obser-vations that, in many cases, PGC coexists withadenocarcinoma and sometimes appears in a tran-sitional form between adenocarcinoma and chori-ocarcinoma. The author proposed that the trop-hoblastic elements found in the PGC develop fromthe dedifferentiation of the adenocarcinoma tissu-e (6). In coexistent adenocarcinoma and choriocar-cinoma, cytologic analyses may show morphologictransitional forms of cells, so that a sequence oftransition from carcinoma to choriocarcinoma canbe traced. This dedifferentiation theory is also
Manuscript received: 30.06.2010 Accepted: 23.01.2011
Turk J Gastroenterol 2011; 22 (4): 437-448doi: 10.4318/tjg.2011.0291
Address for correspondence: Hatice ÜNVERD‹Etlik ‹htisas Education and Research Hospital, Department of Pathology, Ankara, TurkeyPhone: + 90 312 287 34 11E-mail: [email protected]
Unusual tumor: Primary gastric choriocarcinoma
LETTERS TO THE EDITOR
Nadir bir tümör: Primer gastrik koryokarsinoma

supported by the epidemiologic nature of this tu-mor. In addition, the mean age, male-to-female ra-tio, and geographic frequency distribution of thistumor all parallel the data associated with pri-mary adenocarcinoma of the stomach (7).
Although many investigators accepted the dediffe-rentiation theory, many puzzling questions rema-in, such as the role of HCG-producing cells nor-mally present in the gastric mucosa (3). Possibly,normal gastric cells with the ability to produceHCG directly may develop into a gastric choriocar-cinoma in certain cases (3). In a report by Yakeis-hi et al. (7), immunohistochemical studies showedHCG-positive cells in the normal gastric mucosa,carcinomas and choriocarcinomas at variable per-centages and intensities. Because somatic cells re-tain the entire genome for an organism, with dif-ferentiation depending on repression or expressi-on of various groups of genes, it is conceivable
that, under the profound changes that occur du-ring carcinogenesis, the gastric mucosal cells di-rectly develop the morphologic and functional cha-racteristic of a choriocarcinoma (3,7). However,adenocarcinomas can easily spread through thelymphatic system to regional lymph nodes, where-as choriocarcinomas can hematogenously metas-tasize to the lung and liver (7).
Primary gastric choriocarcinoma (PGC) is a high-ly aggressive tumor that is often associated withliver metastasis. Curative resection, appropriatechemotherapy and the absence of synchronous li-ver metastasis are favorable prognostic factors forpatients with PGC. The report of this case of PGCis important to add data to the literature regar-ding this rare condition, to better understand itshistopathogenesis, to help others in its diagnosisand management, and eventually to improve pati-ent treatment and prognosis.
438
FFiigguurree 11.. AA.. Adenocarcinomatous component in the tumor, BB.. ‘Syncytiotrophoblast’-like cells in the choriocarcinomatous areas, CC..beta HCG positivity in the choriocarcinomatous component, and DD.. CEA positivity in the adenocarcinomatous component.

REFERENCES1. Noguchi T, Takeno S, Sato T, et al. A patient with primary
gastric choriocarcinoma who received a correct preoperati-ve diagnosis and achieved prolonged survival. Gastric Can-cer 2002; 5: 112-7.
2. Wurzel J, Brooks JJ. Primary gastric choriocarcinoma: im-munohistochemistry, postmortem documentation, and hor-monal effects in a postmenopausal female. Cancer 1981;48: 2756-61.
3. Mori H, Soeda O, Kamano T, et al. Choriocarcinomatouschange with immunocytochemically HCG-positive cells inthe gastric carcinoma of the males. Virchows Arch A PatholAnat Histol 1982; 396: 141-53.
4. Hartz PH, Ramirez CA. Coexistence of carcinoma and cho-rioepithelioma in the stomach of a young man. Cancer1953; 6: 319-26.
5. Garcia RL, Ghali VS. Gastric choriocarcinoma and yolk sactumor in a man: observations about its possible origin.Hum Pathol 1985; 16: 955-8.
6. Krulewski T, Cohen LB. Choriocarcinoma of the stomach:pathogenesis and clinical characteristics. Am J Gastroente-rol 1988; 83: 1172-5.
7. Yakeishi Y, Mori M, Enjoji M. Distribution of beta-humanchorionic gonadotropin-positive cells in noncancerous gas-tric mucosa and in malignant gastric tumors. Cancer 1990;66: 695-701.
Letters to the editor
439
Hatice ÜNVERD‹1, Berna SAVAfi2, Arzu ENSAR‹2,Hikmet AKGÜL3
Department of 1Pathology, Etlik ‹htisas Education andResearch Hospital, AnkaraDepartments of 2Pathology and 3Surgical Oncology, AnkaraUniversity School of Medicine, Ankara
Manuscript received: 13.10.2010 Accepted: 06.01.2011
doi: 10.4318/tjg.2011.0299
Address for correspondence: Akif ALTINBAfiD›flkap› Y›ld›r›m Beyaz›t Education and Research Hospital,Department of Gastroenterology, Ankara, TurkeyE-mail: [email protected]
Endoscopic removal of an ingested toothpick fromthe prepyloric antrum in an adult woman
Eriflkin bir kad›nda prepilorik antruma saplanm›fl kürdan›n endoskopik olarak ç›kar›lmas›
To the Editor,
Accidental ingestion of foreign bodies in adults isusually attributed to underlying psychiatric disor-ders or mental retardation (1). Sharp and long ob-jects present a higher risk for gastrointestinaltract perforation. Thus, obtaining a diagnosis be-fore any complication in the case of toothpick in-gestion becomes important (2). Here, we report aconscious adult woman in whom an ingested to-othpick had migrated to the prepyloric antrum.
A 48-year-old female was admitted to our clinicwith epigastric pain for the past three days. Physi-cal examination and routine laboratory investiga-tion were unremarkable. She denied any alcoholconsumption or use of any other legal or illegalmedications. She was a non-smoker. Upper gas-trointestinal endoscopy revealed an impacted, ri-gid, white, 3-4 mm, undetermined object in theprepyloric antrum (Figure 1). The object, whichwas removed with biopsy forceps, was a broken to-
othpick that had migrated through the gastric mu-cosa (Figures 2, 3). Subsequently, the patient re-called the possibility of ingestion of a toothpickthree days before while eating Turkish kebab. Oneweek after the successful procedure, the patientremained symptom-free.
The ingestion of foreign bodies, especially sharpones, and localization of the objects in the esopha-gus or intestine usually result in some complicati-ons (2-4). Perforation of the gastrointestinal sys-tem tract anywhere from the esophagus to the ter-minal ileum resulting in peritonitis or abscess isthe main fatal complication. Despite declining ourrecommendation of assessment by computed to-mography (CT) even after the successful removalof the toothpick to check for the presence of abs-cess formation, our patient did not face any comp-lication during the endoscopic examination or thefollow-up period as an outpatient (5). It is neces-













![Choriocarcinoma syndrome complicating a mixed testicular ...choriocarcinoma are very rare (0, 3% of all GCT) [8]. βHCG is always secreted by choriocarcinoma and plays an important](https://img.pdfslide.us/doc/110x75/5e366cd2a1f24370d80dcb00/choriocarcinoma-syndrome-complicating-a-mixed-testicular-choriocarcinoma-are.jpg)