Embed Size (px)
Citation preview
Central JSM Clinical Oncology and Research
Cite this article: Atjimakul T, Hanprasertpong J, Saeaib N (2014) Choriocarcinoma with Spinal Metastasis: A Case Report and Literature Review. JSM Clin Oncol Res 2(3): 1019.
*Corresponding authorJitti Hanprasertpong, Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, Faculty of Medicine, Prince of Songkla University, Songkhla 90110, Thailand; Tel: 6674429617; Fax: 6674429617; Email:
Submitted: 22 January 2014
Accepted: 05 March 2014
Published: 02 April 2014
Copyright© 2014 Hanprasertpong et al.
OPEN ACCESS
Case Report
Choriocarcinoma with Spinal Metastasis: A Case Report and Literature ReviewThiti Atjimakul, Jitti Hanprasertpong* and Nungrutai SaeaibDivision of Gynecologic Oncology, Department of Obstetrics and Gynecology, Thailand
INTRODUCTIONChoriocarcinoma is a malignant disease characterized by the
secretion of human chorionic gonadotropin (hCG). It is highly malignant form of gestational trophoblastic neoplasia (GTN), arising in any type of pregnancy and is more common in patients with a history of hydatidiform mole [1,2]. Choriocarcinoma is composed of abnormal cytotrophoblast and syncytiotrophoblast with hyperplasia and anaplasia, and characterized by absence of chorionic villi, hemorrhage, and necrosis. The direct invasion into the myometrium and vascular invasion resulting in spread of choriocarcinoma into distant sites, most commonly to the lungs, vagina, brain and liver [1-3].
The occurrence of choriocarcinoma with spinal metastasis is extremely rare [4-8]. We present a rare case of a patient who primarily presented with symptoms of spinal compression caused by lumbar spinal metastasis of choriocarcinoma. The patient was then successfully treated with a surgery followed by multi-agent. We also present a review of the literature with particular emphasis on the diagnostic and therapeutic issues related to the choriocarcinoma.
CASE PRESENTATIONA 34-year-old woman came to the provincial hospital with
a 2 month history of having difficulty in walking, progressive weakness and numbness in the bilateral lower extremities within a month after the onset of backache (3 months before admitted to the provincial hospital).
The patient was gravida 3, para 2. The first and second pregnancies were delivered spontaneously at term. In year 2010, the third pregnancy was found to be partial hydatidiform mole. Curettage was done at our institute, Songklanagarind hospital. Post surgery, she reported intermittent vaginal bleeding but she did not return back for the follow up.
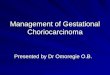
Three years later she returned back to hospital with a history of having difficulty in walking, progressive weakness and numbness in bilateral lower extremities. At the provincial hospital, an initial examination revealed paraplegia, an impaired sensation below the level of thoracic 12 (T12). Urinary incontinence had resulted from loss of urinary bladder sphincter control. A myelography discovered complete the cal sac blockage at L1-L2 vertebra. Then, she underwent a laminectomy to remove the extradurally located tumor mass, which was causing compression of the spinal cord. Pathological examination revealed blackish brown colored tumor mass consisting of multinuclear syncytiotrophoblastic cells with large eosinophilic cytoplasm around the mononuclear cytotrophoblastic cells (Figure 1). These findings were consistent with choriocarcinoma. A computed tomography (CT) scan of the chest showed multiple variable size nodules, about 2-5 mm, in both lungs that were most likely metastases. The CT scans of the brain and abdomen were normal. Postoperative laboratory investigation revealed β-hCG level of 695,257 mIU/ml with other normal blood studies. After surgery the neurological condition did not change.
The patient was then transferred to our institute. During
Keywords•Choriocarcinoma•Spine metastasis
Abstract
Spinal metastasis of choriocarcinoma is very rare. We present a case of metastatic choriocarcinoma in the lumbar spine. A 34-year-old woman was admitted to the hospital with complaints of progressive weakness and numbness in the bilateral lower extremities for 3 months. Three years earlier, she had undergone curettage for a partial hydatidiform mole. A myelography showed complete thecal sac blockage at L1-L2 vertebra. Surgical resection was performed by laminectomy to remove the vertebral lesion. Choriocarcinoma was diagnosed after histological examination. After surgery and six courses of adjuvant chemotherapy and physiotherapy, she was able to walk again. Ten months after diagnosis and treatment, she is now healthy without any evidence of disease.
Conclusion: Choriocarcinoma with spinal metastasis is an unusual phenomenon. Spine surgery plus chemotherapy is highly effective for treatment of this condition.
Central
Hanprasertpong et al. (2014)Email:
JSM Clin Oncol Res 2(3): 1019 (2014) 2/4
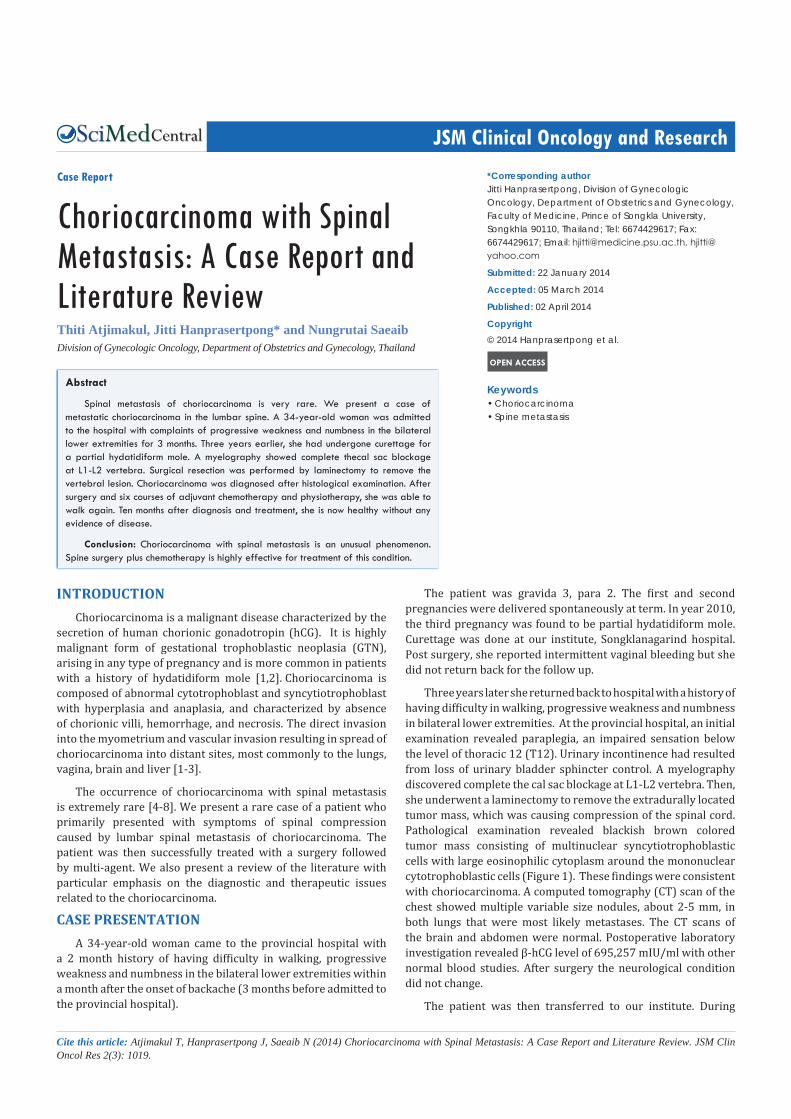
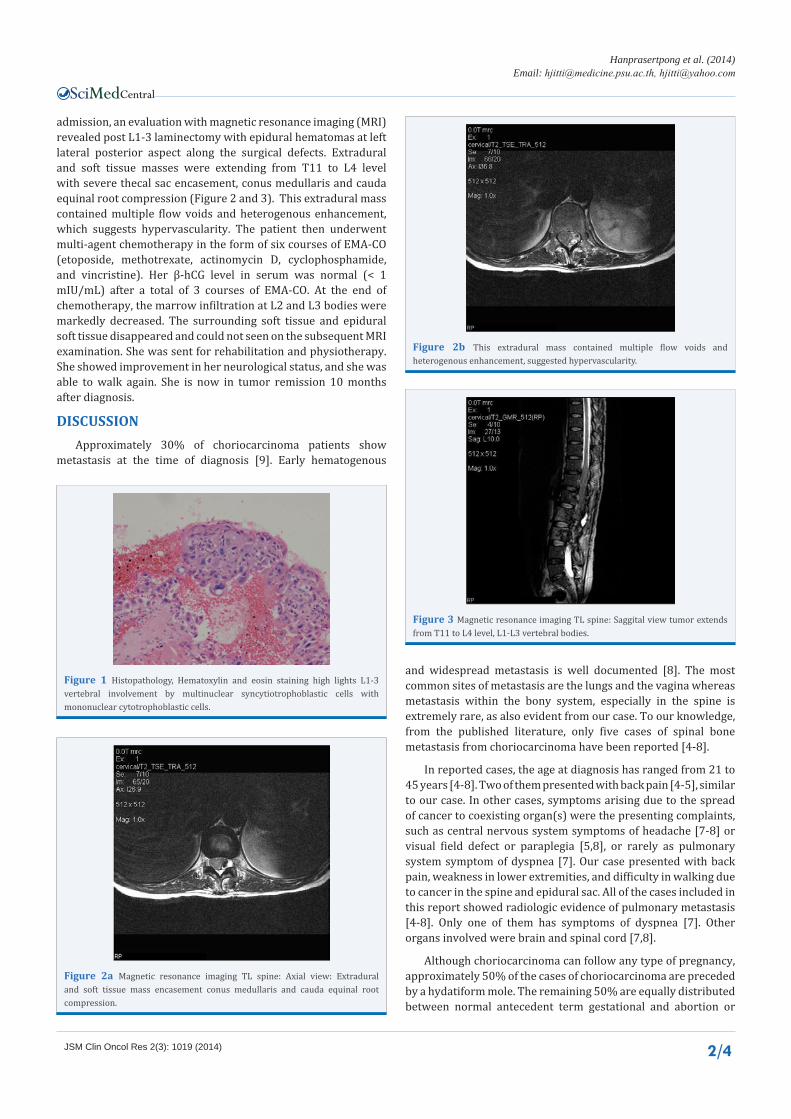
admission, an evaluation with magnetic resonance imaging (MRI) revealed post L1-3 laminectomy with epidural hematomas at left lateral posterior aspect along the surgical defects. Extradural and soft tissue masses were extending from T11 to L4 level with severe thecal sac encasement, conus medullaris and cauda equinal root compression (Figure 2 and 3). This extradural mass contained multiple flow voids and heterogenous enhancement, which suggests hypervascularity. The patient then underwent multi-agent chemotherapy in the form of six courses of EMA-CO (etoposide, methotrexate, actinomycin D, cyclophosphamide, and vincristine). Her β-hCG level in serum was normal (< 1 mIU/mL) after a total of 3 courses of EMA-CO. At the end of chemotherapy, the marrow infiltration at L2 and L3 bodies were markedly decreased. The surrounding soft tissue and epidural soft tissue disappeared and could not seen on the subsequent MRI examination. She was sent for rehabilitation and physiotherapy. She showed improvement in her neurological status, and she was able to walk again. She is now in tumor remission 10 months after diagnosis.
DISCUSSIONApproximately 30% of choriocarcinoma patients show
metastasis at the time of diagnosis [9]. Early hematogenous
Figure 1 Histopathology, Hematoxylin and eosin staining high lights L1-3 vertebral involvement by multinuclear syncytiotrophoblastic cells with mononuclear cytotrophoblastic cells.
Figure 2a Magnetic resonance imaging TL spine: Axial view: Extradural and soft tissue mass encasement conus medullaris and cauda equinal root compression.
Figure 2b This extradural mass contained multiple flow voids and heterogenous enhancement, suggested hypervascularity.
Figure 3 Magnetic resonance imaging TL spine: Saggital view tumor extends from T11 to L4 level, L1-L3 vertebral bodies.
and widespread metastasis is well documented [8]. The most common sites of metastasis are the lungs and the vagina whereas metastasis within the bony system, especially in the spine is extremely rare, as also evident from our case. To our knowledge, from the published literature, only five cases of spinal bone metastasis from choriocarcinoma have been reported [4-8].
In reported cases, the age at diagnosis has ranged from 21 to 45 years [4-8]. Two of them presented with back pain [4-5], similar to our case. In other cases, symptoms arising due to the spread of cancer to coexisting organ(s) were the presenting complaints, such as central nervous system symptoms of headache [7-8] or visual field defect or paraplegia [5,8], or rarely as pulmonary system symptom of dyspnea [7]. Our case presented with back pain, weakness in lower extremities, and difficulty in walking due to cancer in the spine and epidural sac. All of the cases included in this report showed radiologic evidence of pulmonary metastasis [4-8]. Only one of them has symptoms of dyspnea [7]. Other organs involved were brain and spinal cord [7,8].
Although choriocarcinoma can follow any type of pregnancy, approximately 50% of the cases of choriocarcinoma are preceded by a hydatiform mole. The remaining 50% are equally distributed between normal antecedent term gestational and abortion or
Central
Hanprasertpong et al. (2014)Email:
JSM Clin Oncol Res 2(3): 1019 (2014) 3/4
ectopic pregnancy [1-3,6]. Among 5 reported cases, 3 cases are preceded by term pregnancy [4,6-7] and 2 cases are preceded by hydatidiform mole [5,8]. In our case, the patient was diagnosed with choriocarcinoma following partial mole.
The diagnosis was made by clinical history, imaging, hCG level, and histopathologic examination [4-8]. Imaging such as myelography, CT scan or MRI is useful in diagnosis and planning of surgery [4-8]. A myelography in our case revealed a complete the cal sac blockage at L1-L2 vertebra. The MRI also revealed epidural hematomas at the left lateral posterior aspect along the surgical defects. Extradural and soft tissue masses were extending from T11 to L4 level with severe thecal sac encasement, conus medullaris, and cauda equinal root compression. Lumbar level is the most common site of spinal metastasis of choriocarcinoma [5-8]. At the time of diagnosis, serum hCG levels are usually elevated, like in our case, levels ranged from 15,000 to more than 100,000 mIU/Ml (Table 1) [4-8].
Choriocarcinoma is one of the malignant tumors that is most sensitive to chemotherapy [2,10]. A patient with spine metastasis, as our case, is classified as “high risk” and is improbable to response to single chemotherapy. Naito found that a choriocarcinoma patient who has spine and lung metastasis did not respond to 3 courses
of methotrexate. However, the patient was successfully treated by total en bloc spondylectomy and radiotherapy [6]. To date it is agreed that patients with high risk GTN should be treated initially with multiagent chemotherapy especially EMA-CO with or without adjuvant surgery or radiotherapy. Cure rates for high risk GTN of 80-90% are now achievable with intensive multimodality [2,10]. However, the best treatment for patients with spinal metastasis has not been established because of its rarity.
There have been two reported cases of spine metastasis of choriocarcinoma treated with multiagent chemotherapy with radiation [4-5]. Vani reported a poor response to 12 courses of multiagent chemotherapy in a choriocarcinoma patient with spine and lung metastasis. After treatment the patients received palliative radiotherapy [4]. Manegaz reported a choriocarcinoma patient with spine and lung metastasis who responded well to 7 courses of EMA-CO and radiotherapy. However, the patient died from sepsis caused by febrile neutropenia [5].
Surgery for a case of spinal metastasis of choriocarcinoma was firstly reported by Naito et al. in 2009 [6]. Surgery is indicated when a massive mass effect is due to tumor mass or hematoma. In this situation, spine surgery such as spondylectomy or laminectomy is required to provide acute decompression or
Author (year)
Age Symptom (s)
Dura-tion of symp-
tom
Method of Di-
agnosis
Ante-ced-ent
preg-nancy inter-
val
hCG level
(mIU/ml)
Location of spine me-tastasis
Other organ
(s) me-
tasta-sis
Treatment Status of lastFollow up
Sur-gery Chemotherapy
Radia-tion
Se-quence
of treat-ment
Vani [4] 27 Back pain 1 week CT and
hCG
4 yearafter term
30,000 S5 vertebral body Lung - MTX + ActD + Chlorambucil + VP-16 x12 course
Pal-liative radio-thera-
py
CR Loss follow-up
Men-egaz [5]
45Pain,
paraplegialower limb
4 month
MRI andhCG
2 yearafter mole
22,400L3 vertebralbody, L2-S1
epidural spaceLung - EMACO x 7 cycle
45 Gy5
weeks
CR Died (5 months after diagno-
sis)
Naito [6] 38
Abnormal uter-ine bleeding,
PersistedhCG level
6 month
PET/CT and his-tology
6 monthafter term
15,793 L2 vertebral body,lumbar epidural space Lung
Total en bloc
spond-ylec-tomy
MTX 20mg/d 5d x 3 coursesRadio-thera-
pyCSR
Died (6 months after diagno-
sis)
Lee [7] 33
Headache,dyspnea,
hemoptysis 2 weekHistol-
ogy and MRI
2 weekafter term
> 100,000
L3 vertebral body,lumbar epidural space
Lung,brain
Emboli-zation
and lami-nec-tomy
EMA-CO - SCRemission (10
months after operation)
Ko [8] 21
Headache,nausea,
visual field defect
SuddenHistol-
ogy and MRI
10 monthafter mole
> 100,000 L2 vertebral body
Lung, tho-racic
spinal cord, brain
Crani-otomy
Multi-agentchemotherapy
Radio-thera-
pySCR
Died (13 months after
diagnosis)
This case 34
Back pain, weak-ness in lower extremities,difficulty in
walking
3 month
Myelog-raphy, Histol-
ogy and MRI
3 year after
partial mole
695,257 L1-L2 vertebral bodiesT11-L4 epidural space Lung
Lami-nec-tomy
EMACO x 6 cycle - SCRemission (10
months after diagnosis)
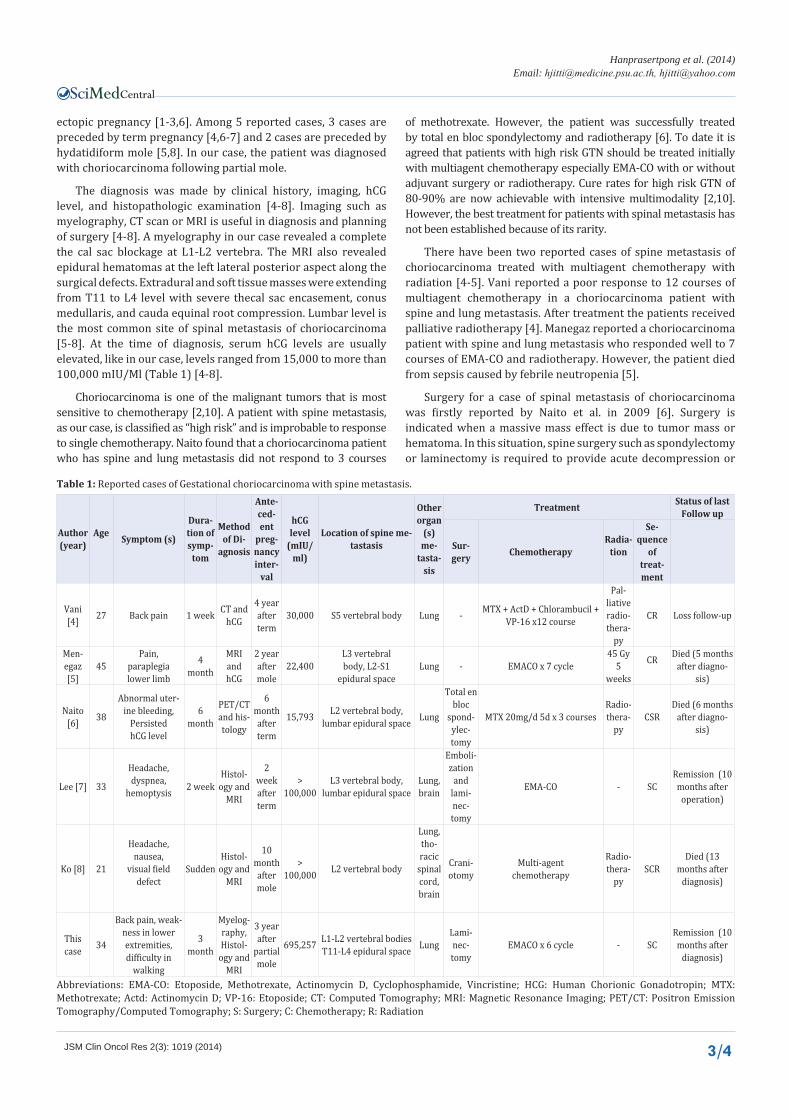
Table 1: Reported cases of Gestational choriocarcinoma with spine metastasis.
Abbreviations: EMA-CO: Etoposide, Methotrexate, Actinomycin D, Cyclophosphamide, Vincristine; HCG: Human Chorionic Gonadotropin; MTX: Methotrexate; Actd: Actinomycin D; VP-16: Etoposide; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; PET/CT: Positron Emission Tomography/Computed Tomography; S: Surgery; C: Chemotherapy; R: Radiation

Central
Hanprasertpong et al. (2014)Email:
JSM Clin Oncol Res 2(3): 1019 (2014) 4/4
Atjimakul T, Hanprasertpong J, Saeaib N (2014) Choriocarcinoma with Spinal Metastasis: A Case Report and Literature Review. JSM Clin Oncol Res 2(3): 1019.
Cite this article
to control bleeding [6-7]. Because choriocarcinoma is extremely hemorrhagic, it is quite possible the surgical procedures may have exacerbated the invasive and metastatic potential of this tumor. Thus, preoperative angiographic embolization, or at least angiography of the tumor should be used to reducing perioperative hemorrhages and evaluate vascularity of the tumor site, respectively [6-7]. Lee reported a good course for choriocarcinoma with a patient with spine, epidural, lung and brain metastasis who was managed successfully by embolization of the lesion of the lumbar spine, followed by an injection of polymethymethacrylate in the L3 vertebral body, total laminectomy of L3, subtotal removal of the epidural mass, screw fixation of L2 and L4, and multiagent chemotherapy (EMA-CO) [7].
When central nervous system metastases are present, radiotherapy (whole brain irradiation) is usually given simultaneously with the initiation of systemic chemotherapy [2,10]. Radiotherapy was performed as adjuvant treatment in four previous cases of spine metastasis of choriocarcinoma [4-6,8]. This therapy can also be utilized when spine metastasis are present [5-6,8]. In our case, the patient was successfully treated by 6 courses of EMA-CO after laminectomy without radiotherapy.
Despite improvements in treatment modality and the use of combined modality treatment with chemotherapy, surgery and radiation, the prognosis for these choriocarcinoma cases with spinal metastasis is unfavorable. The longest reported survivor lived for 13 months after diagnosis [8]. Earlier diagnosis and multimodality treatment is crucial for significant reduction in mortality.
In conclusion, we have reported an uncommon case of metastasic choriocarcinoma to the lumbar spine and lung, which was successfully treated by laminectomy with multiagent chemotherapy. The neurological symptoms,history of a hydatidiform mole, and the possibility of metastatic GTN should always be considered especially in fertile females. In our case, the diagnosis was made by clinical history, imaging, and hCG levels. The treatment involved multiagent chemotherapy with or without surgery or radiotherapy.
ACKNOWLEDGEMENTWe wish to thank Dr.Winyou Mitarnun for performing and
confirming the pathologic diagnosis in this case and Dr.Teeravut Tubtawee for performing and confirming the radiologic diagnosis.
REFERENCES1. Scott JR, Di Saia PJ, Hammond CB. Gestational trophoblastic neoplasms.
8th edn. In: Scott JR, DiSaia PJ, Hammond, editors. Danforth’s Obstetrics and Gynecology. Philadelphia, PA: Lippincott Williams & Wilkins. 1999: 927-937.
2. Seckl MJ, Sebire NJ, Berkowitz RS. Gestational trophoblastic disease. Lancet. 2010; 376: 717-729.
3. Lurain JR. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Am J Obstet Gynecol. 2010; 203: 531-539.
4. Vani R, Kuntal R, Koteshwar RK. Choriocarcinoma following term pregnancy with bone metastasis. Int J Gynaecol Obstet. 1993; 40: 252-253.
5. Menegaz RA, Resende AD, da Silva CS, Barcelos AC, Murta EF. Metastasis of choriocarcinoma to lumbar and sacral column. Eur J Obstet Gynecol Reprod Biol. 2004; 113: 110-113.
6. Naito Y, Akeda K, Kasai Y, Matsumine A, Tabata T, Nagao K, et al. Lumbar metastasis of choriocarcinoma. Spine (Phila Pa 1976). 2009; 34: E538-543.
7. Lee JH, Park CW, Chung DH, Kim WK. A case of lumbar metastasis of choriocarcinoma masquerading as an extraosseous extension of vertebral hemangioma. J Korean Neurosurg Soc. 2010; 47: 143-147.
8. Ko JK, Cha SH, Lee JH, Choi CH. Intramedullary spinal cord metastasis of choriocarcinoma. J Korean Neurosurg Soc. 2012; 51: 141-143.
9. Sierra-Bergua B, Sánchez-Marteles M, Cabrerizo-García JL, Sanjoaquin-Conde I. Choriocarcinoma with pulmonary and cerebral metastases. Singapore Med J. 2008; 49: e286-288.
10. Lurain JR. Gestational trophoblastic disease II: classification and management of gestational trophoblastic neoplasia. Am J Obstet Gynecol. 2011; 204: 11-18.




![Choriocarcinoma syndrome complicating a mixed testicular ...choriocarcinoma are very rare (0, 3% of all GCT) [8]. βHCG is always secreted by choriocarcinoma and plays an important](https://img.pdfslide.us/doc/110x75/5e366cd2a1f24370d80dcb00/choriocarcinoma-syndrome-complicating-a-mixed-testicular-choriocarcinoma-are.jpg)
















![Spinal Metastasis of Medulloblastoma in Adults: A Case Report · 2015. 1. 6. · systemic metastasis [1]. Our patient had neither tumor recurrence in the posterior fossa nor systemic](https://img.pdfslide.us/doc/110x75/5fda06f185061512a942751d/spinal-metastasis-of-medulloblastoma-in-adults-a-case-2015-1-6-systemic-metastasis.jpg)